bernard nordlinger m.d. hôpital ambroise paré – boulogne assistance publique hôpitaux de paris
DESCRIPTION
The multimodal treatment of liver metastases : FREQUENTLY ASKED QUESTIONS. Bernard NORDLINGER M.D. Hôpital Ambroise Paré – Boulogne Assistance Publique Hôpitaux de Paris. Questions. What is resectable ? Chemotherapy before or after resection ? Indications for immediate surgery ? - PowerPoint PPT PresentationTRANSCRIPT
Bernard NORDLINGER M.D.
Hôpital Ambroise Paré – BoulogneAssistance Publique Hôpitaux de Paris
The multimodal treatment of liver metastases:
FREQUENTLY ASKED QUESTIONS
Questions
What is resectable?Chemotherapy before or after resection?Indications for immediate surgery?How to manage metastases which disappear from imaging?Does neoadjuvant chemotherapy increase the risks of surgery?Targeted agents before surgery for liver metastases ? Should all patients with liver metastases be considered for resection?
What is a resectable metastasis?
Question
A resectable metastasis: a principle
Complete resection of tumor is feasible Free resection clearance: R0 Preservation of hepatic vein(s) and portal pedicle to remnant
liver Remnant liver parenchyma 25 % Resectability does not depend on the number of metastases
Resectable metastases
Categories: - Easily resectable
- More difficult to resect; need for specific skills
- Resectable + RFA
- Potentially resectable after response to chemotherapy
- Unresectable and unlikely to ever be resected Do not deny the potential benefit of major liver resection; if local surgeon does not have the expertise,refer to an expert institution
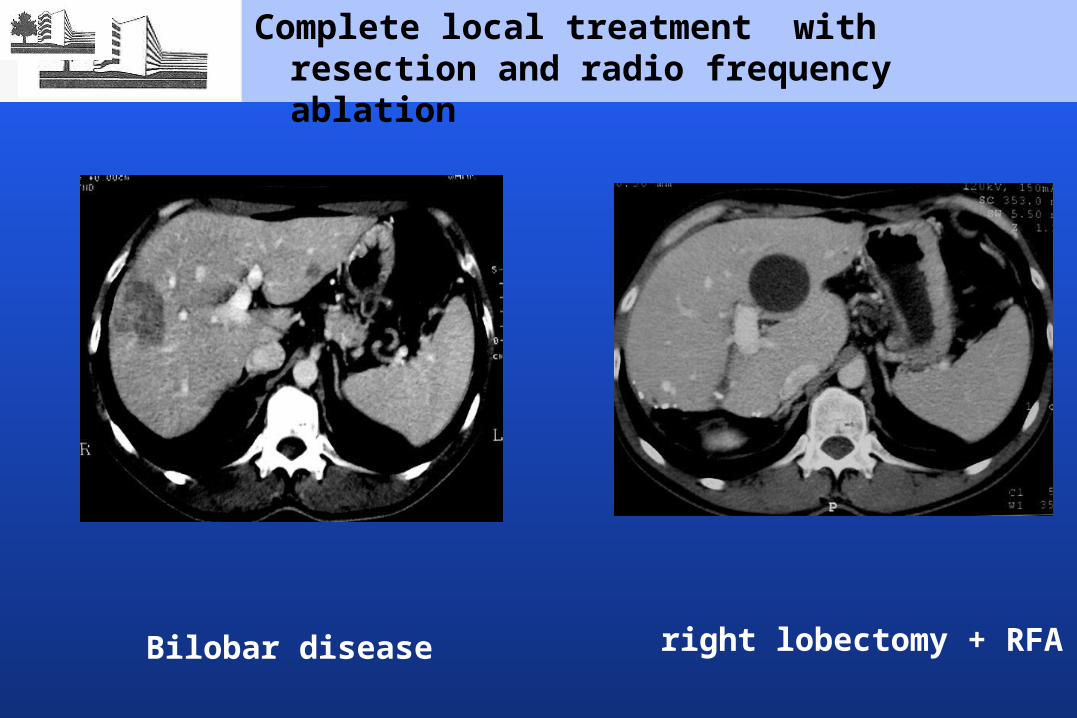
Bilobar disease right lobectomy + RFA
Complete local treatment with resection and radio frequency ablation
Message:
Discuss all cases in multidisciplinary meetings
Question:
Chemotherapy combined with surgery for resectable metastases: before or after?
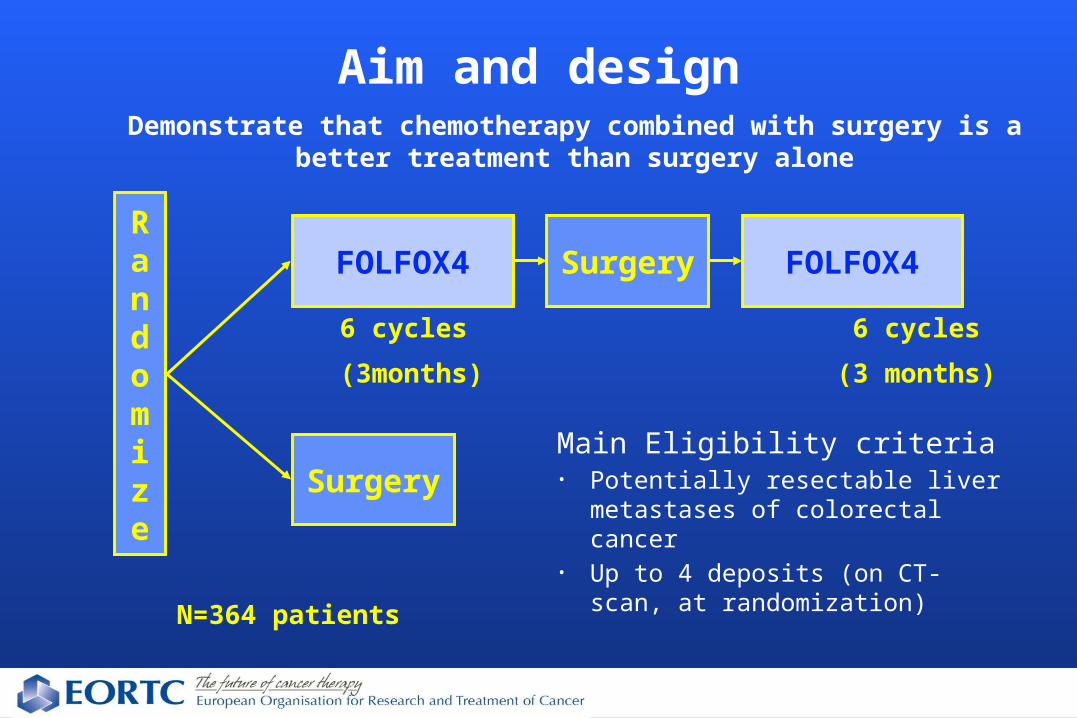
Aim and designDemonstrate that chemotherapy combined with surgery is a better
treatment than surgery alone
Randomize
SurgeryFOLFOX4
Surgery
6 cycles (3months)
N=364 patients
6 cycles(3 months)
FOLFOX4
Main Eligibility criteria• Potentially resectable liver
metastases of colorectal cancer• Up to 4 deposits (on CT-scan, at
randomization)
(years)
0 1 2 3 4 5 6
0
10
20
30
40
50
60
70
80
90
100
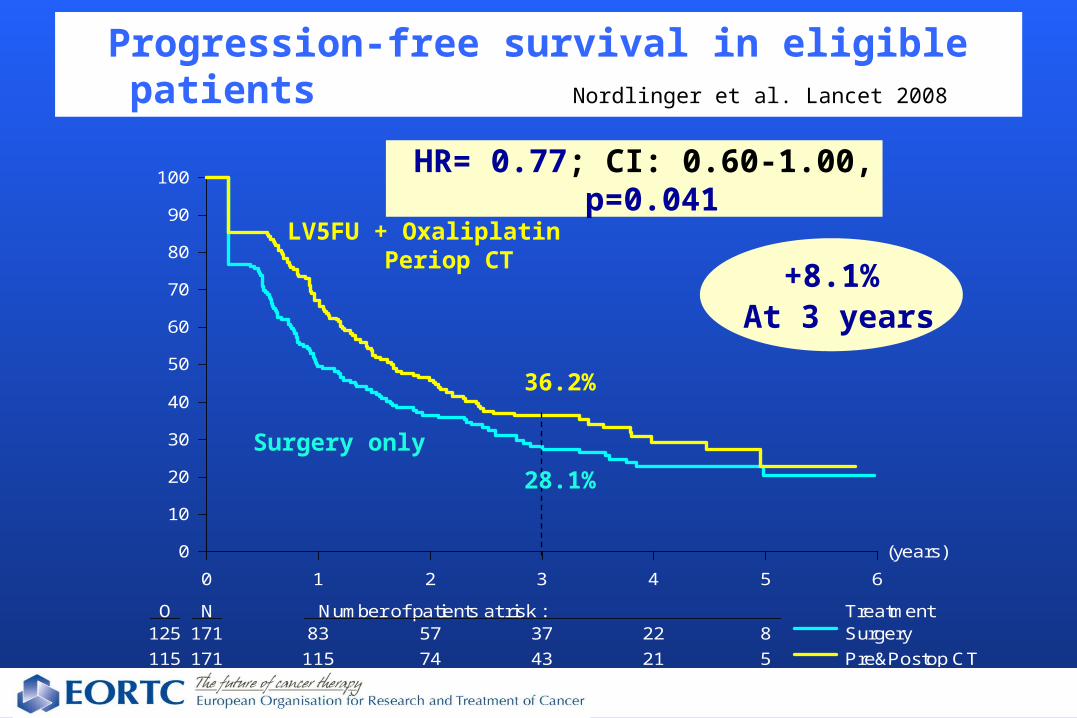
O N Number of patients at risk : Treatment125 171 83 57 37 22 8115 171 115 74 43 21 5
SurgeryPre&Postop CT
Progression-free survival in eligible patients Nordlinger et al. Lancet 2008
HR= 0.77; CI: 0.60-1.00, p=0.041
LV5FU + Oxaliplatin Periop CT
28.1%
36.2%
+8.1%At 3 years
Surgery only
(years)
0 2 4 6 8 10 12
0
10
20
30
40
50
60
70
80
90
100
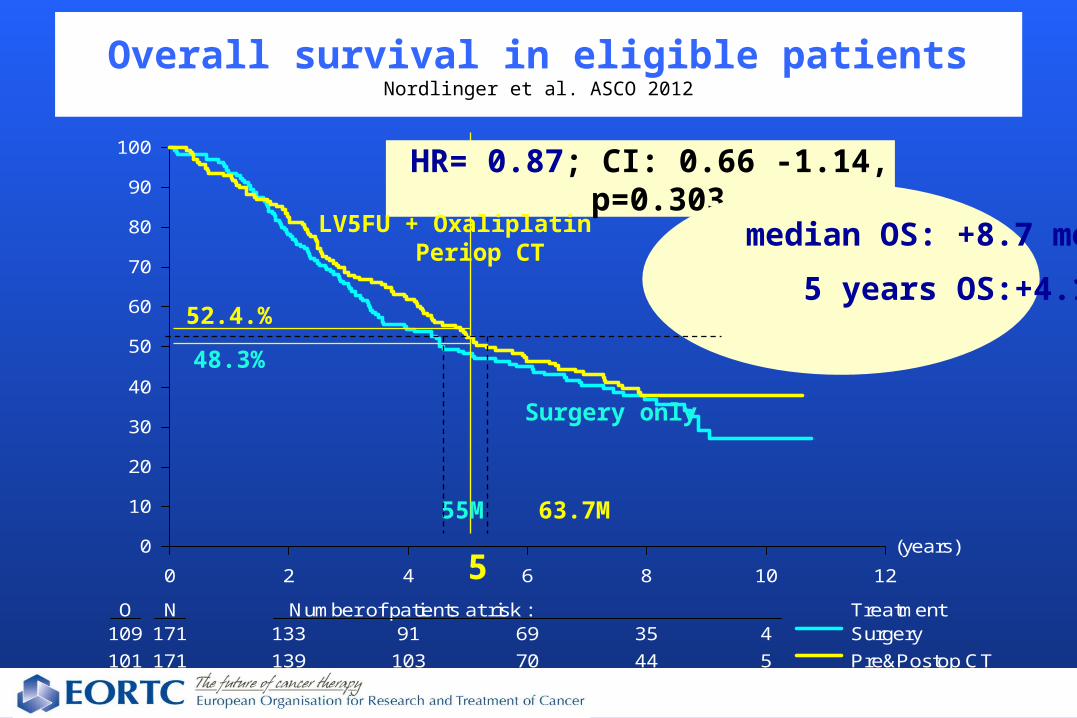
O N Number of patients at risk : Treatment109 171 133 91 69 35 4101 171 139 103 70 44 5
SurgeryPre&Postop CT
Overall survival in eligible patientsNordlinger et al. ASCO 2012
HR= 0.87; CI: 0.66 -1.14, p=0.303
LV5FU + Oxaliplatin Periop CT median OS: +8.7 months
5 years OS:+4.1 %
Surgery only
63.7M55M
52.4.%
48.3%
5
Message:
Peri-operative chemotherapy with FOLFOX considered the treatment of reference in patients with resectable metastases
Question:
• Are there indications for immediate surgery of resectable metastases?
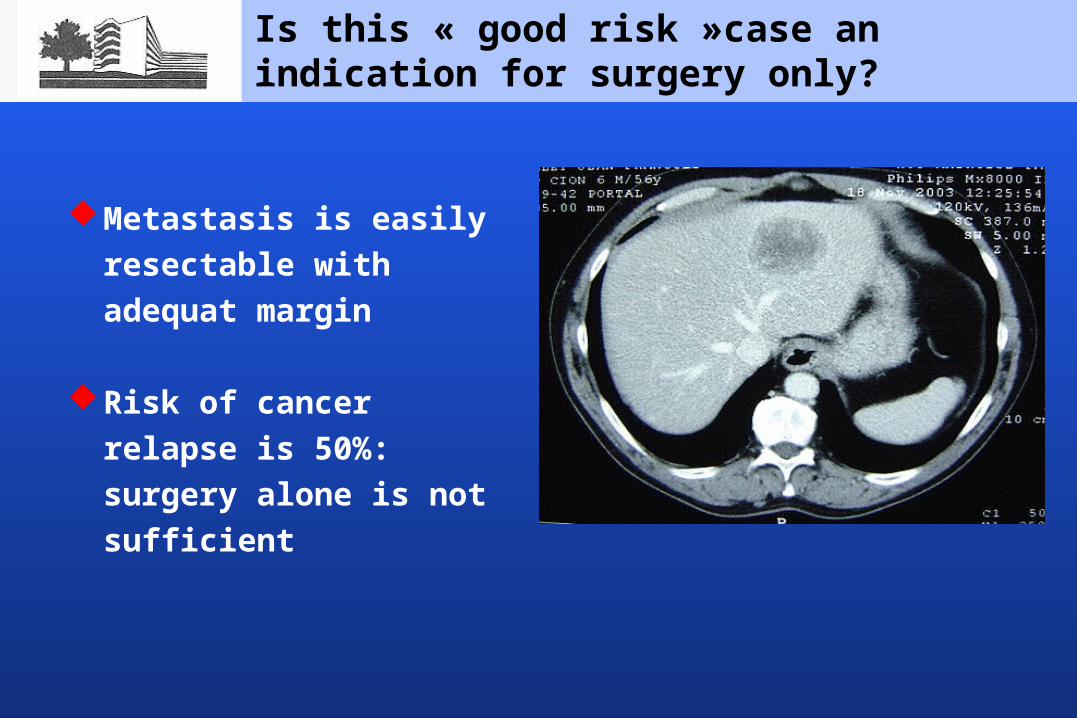
Is this « good risk »case an indication for surgery only?
Metastasis is easily resectable with adequat margin
Risk of cancer relapse is
50%: surgery alone is not sufficient
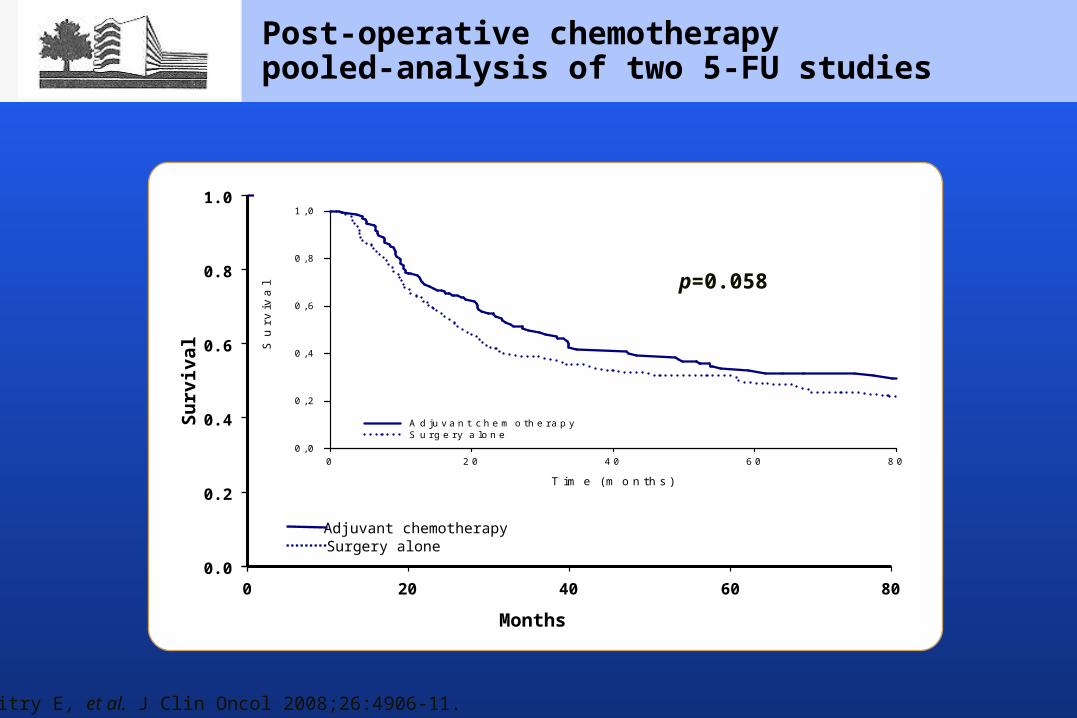
Post-operative chemotherapypooled-analysis of two 5-FU studies
Months0 20 40 60 80
Surv
ival
Adjuvant chemotherapySurgery alone
0.0
0.2
0.4
0.6
0.8
1.0
Time (months)
0 20 40 60 80
Sur
viva
l
0,0
0,2
0,4
0,6
0,8
1,0
Adjuvant chemotherapySurgery alone
Mitry E, et al. J Clin Oncol 2008;26:4906-11.
p=0.058
Post-operative chemotherapy only?
- No sufficient evidence to be standard treatment at the moment
- 1/3 patients do not receive planned post-op treatment, although almost all can receive pre-op treatment ( EORTC study )
- No trials available comparing pre vs post- Post-operative chemotherapy is an option in patients who
did not receive peri-operative chemotherapy:
- Small and poorly located metastasis which may disappear after chemotherapy
- Small synchronous metastasis with indication to resect the primary
Question:
How to manage metastases which disappear from imaging during chemotherapy?
« Complete response » on imaging
Complete response does not mean cure in up to 80% of cases
It is preferable to resect liver metastases before complete response when surgeons can see them, and not overtreat patients with chemotherapy
1Benoist et al. JCO 20062Tan et al. J GastroIntest Surg 20073Adam et al. JCO 20084Elias et al. Ann Surg Oncol 2007
« Complete response » on imaging: looking for lost metastases
Try other imaging methods: - MRI - FDG Pet scan probably unhelpful ( Tan, J Gastrointest Surg 2007 Covas ASCO 2008) - Contrast Enhanced US
If they are no longer visible - resect the site
- hepatic artery infusion
- follow up for recurrence
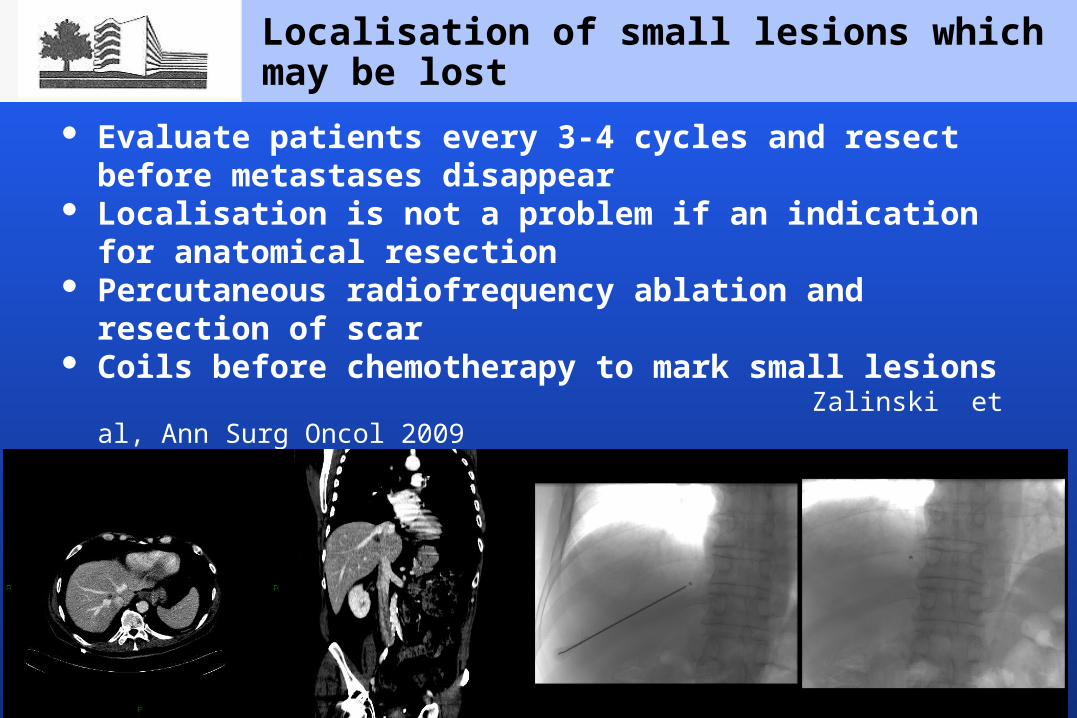
Localisation of small lesions which may be lost
Evaluate patients every 3-4 cycles and resect before metastases disappear
Localisation is not a problem if an indication for anatomical resection
Percutaneous radiofrequency ablation and resection of scar Coils before chemotherapy to mark small lesions Zalinski et al, Ann Surg Oncol 2009
Question:
Does neoadjuvant chemotherapy increase the morbidity or mortality of surgery?
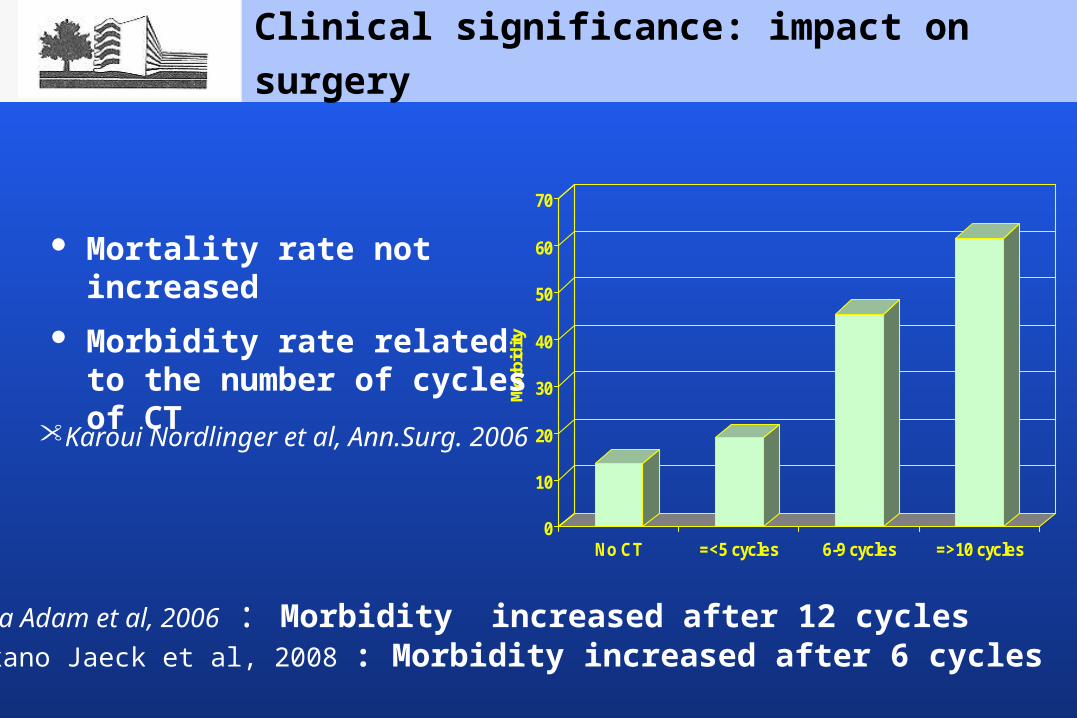
Clinical significance: impact on surgery
• Karoui Nordlinger et al, Ann.Surg. 2006
0
10
20
30
40
50
60
70
Mor
bidi
ty
No CT =<5 cycles 6-9 cycles =>10 cycles
• Aloia Adam et al, 2006 : Morbidity increased after 12 cycles • Nakano Jaeck et al, 2008 : Morbidity increased after 6 cycles
Mortality rate not increased Morbidity rate related to the
number of cycles of CT
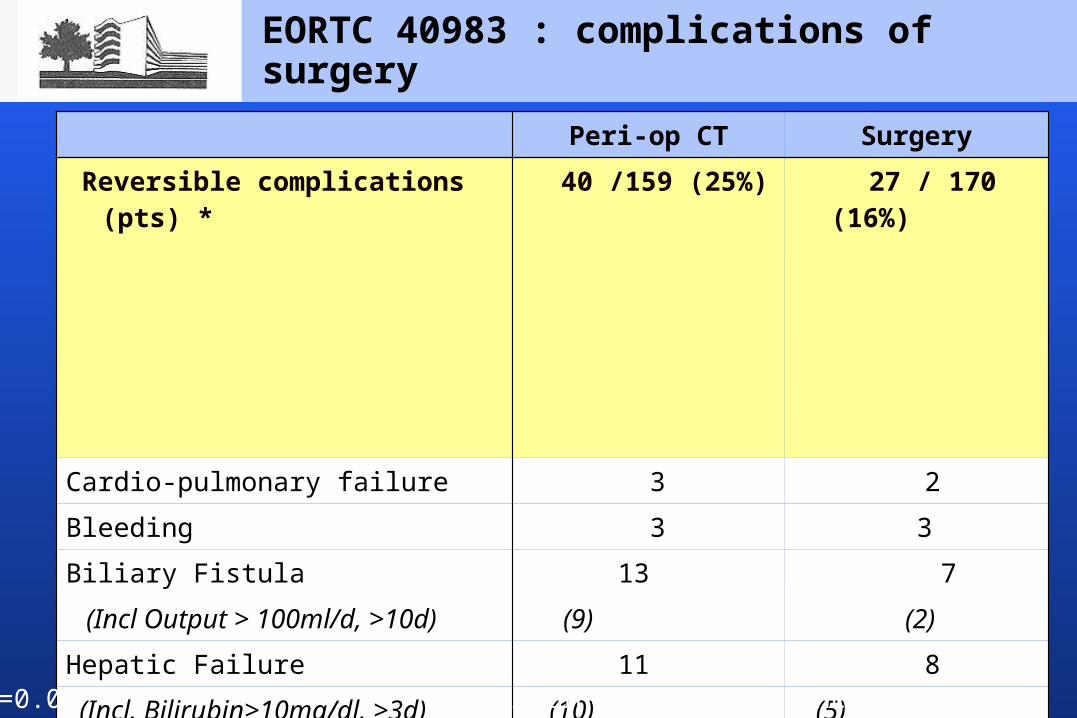
EORTC 40983 : complications of surgery
Peri-op CT Surgery Reversible complications (pts) *
40 /159 (25%)
27 / 170 (16%)
Cardio-pulmonary failure 3 2 Bleeding 3 3 Biliary Fistula 13 7 (Incl Output > 100ml/d, >10d) (9) (2) Hepatic Failure 11 8 (Incl. Bilirubin>10mg/dl, >3d) (10) (5)
Wound infection 5 4 Intra-abdominal infection 11 4 Need for reoperation 5 3 Other (lung, urinary, ascites, etc…) 20
10
Post-operative deaths 1 patient 2 patients
*P=0.04 Nordlinger et al., Lancet 2008
Risks of surgery depend on the number of cycles
Message:
Optimal duration of pre-operative chemotherapy?
Question:
Different
- when metastases are resectable - when metastases are not resectable
Optimal duration of pre-operative chemotherapy
- 6 cycles according to EORTC 40983
- Could fewer cycles be sufficient?
Duration of pre-operative chemotherapy in resectable metastases
Duration of pre-operative chemotherapy in initially unresectable metastases?
• Aim: convert patients to resection with a hope for cure
• Chemotherapy should be discontinued when metastases have become resectable and not given until best response is observed
• Overtreatment can damage the liver and preclude surgery
Question:
If resectable metastases progress during pre-operative chemotherapy?
Progression during pre-operative CT
A biological marker for poor prognosis No surgery if metastases progress Change chemotherapy,
Question:
Targeted agents before liver surgery for metastases ?
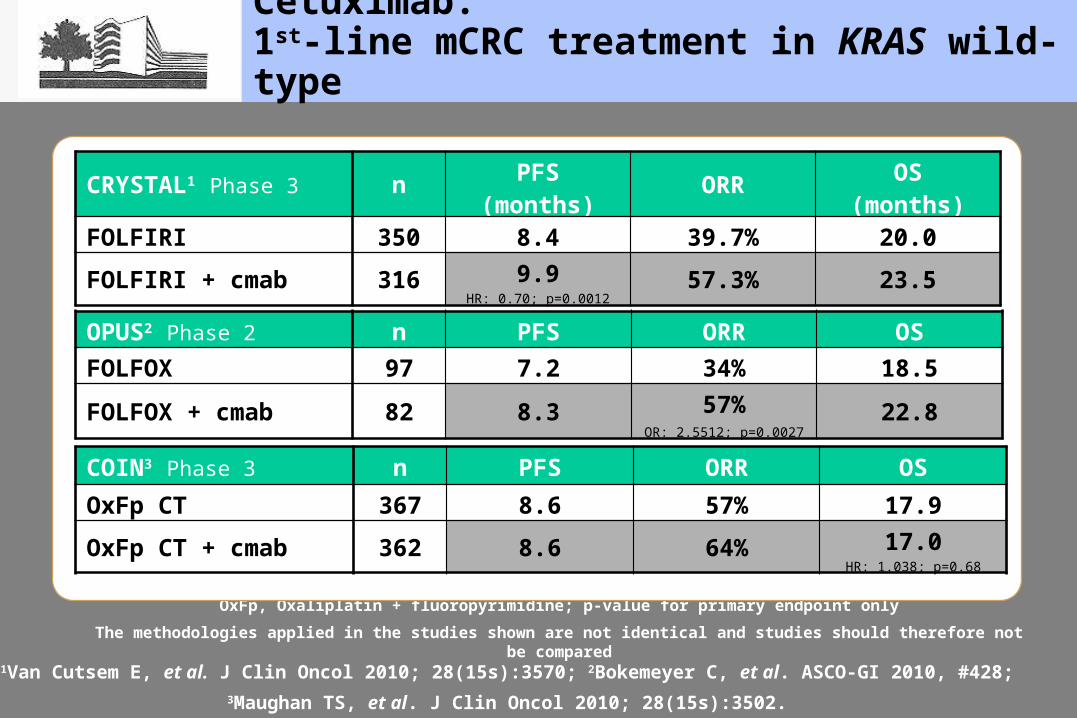
Cetuximab:1st-line mCRC treatment in KRAS wild-type
OxFp, Oxaliplatin + fluoropyrimidine; p-value for primary endpoint onlyThe methodologies applied in the studies shown are not identical and studies should therefore not be compared
1Van Cutsem E, et al. J Clin Oncol 2010; 28(15s):3570; 2Bokemeyer C, et al. ASCO-GI 2010, #428; 3Maughan TS, et al. J Clin Oncol 2010; 28(15s):3502.
CRYSTAL1 Phase 3 n PFS(months) ORR OS
(months)FOLFIRI 350 8.4 39.7% 20.0
FOLFIRI + cmab 316 9.9HR: 0.70; p=0.0012
57.3% 23.5
OPUS2 Phase 2 n PFS ORR OSFOLFOX 97 7.2 34% 18.5
FOLFOX + cmab 82 8.3 57%OR: 2.5512; p=0.0027
22.8
COIN3 Phase 3 n PFS ORR OSOxFp CT 367 8.6 57% 17.9
OxFp CT + cmab 362 8.6 64% 17.0HR: 1.038; p=0.68
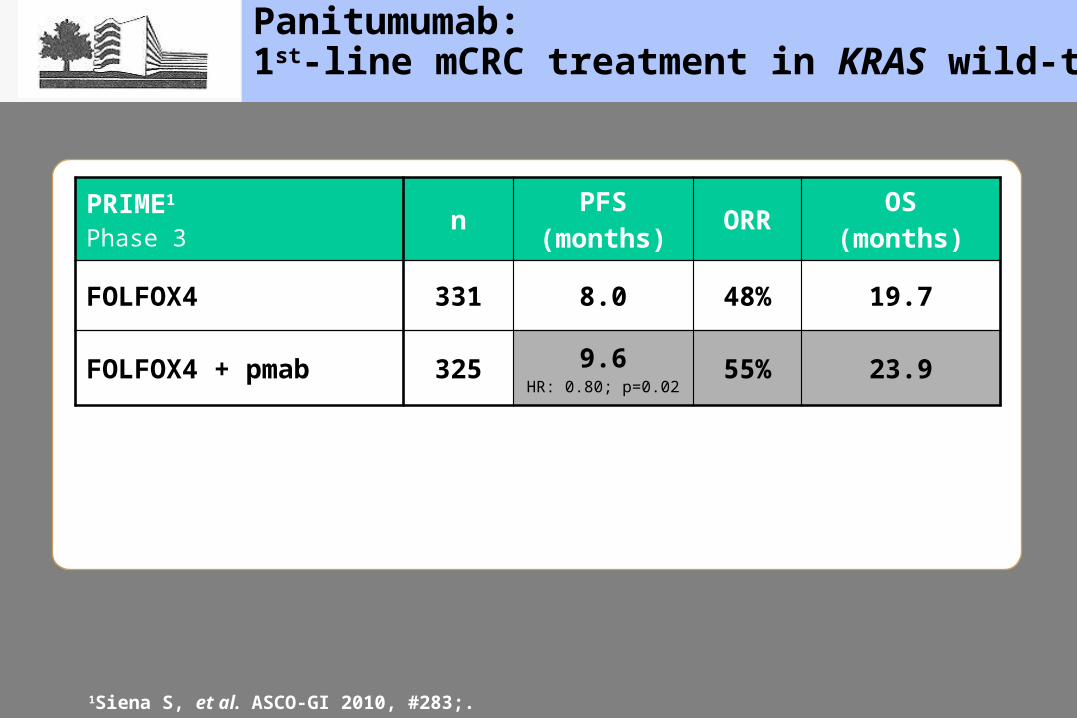
Panitumumab:1st-line mCRC treatment in KRAS wild-type
PRIME1
Phase 3 n PFS(months) ORR OS
(months)
FOLFOX4 331 8.0 48% 19.7
FOLFOX4 + pmab 325 9.6HR: 0.80; p=0.02
55% 23.9
1Siena S, et al. ASCO-GI 2010, #283;.
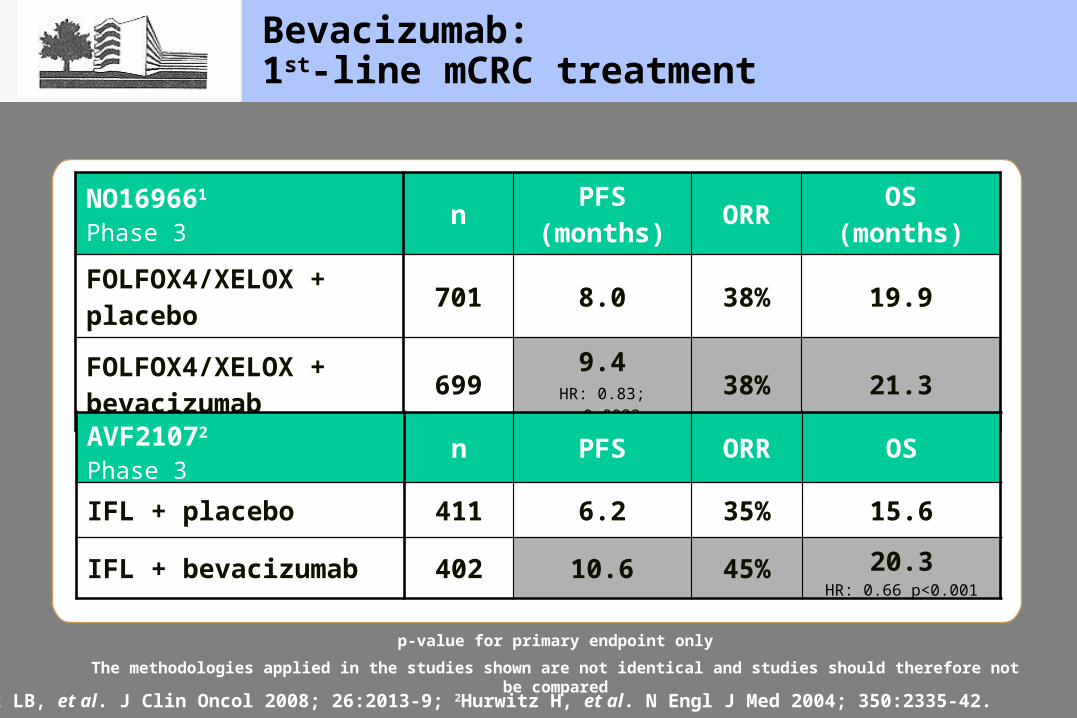
Bevacizumab:1st-line mCRC treatment
NO169661
Phase 3 n PFS(months) ORR OS
(months)FOLFOX4/XELOX + placebo 701 8.0 38% 19.9
FOLFOX4/XELOX + bevacizumab 699 9.4
HR: 0.83; p=0.002338% 21.3
1Saltz LB, et al. J Clin Oncol 2008; 26:2013-9; 2Hurwitz H, et al. N Engl J Med 2004; 350:2335-42.
p-value for primary endpoint onlyThe methodologies applied in the studies shown are not identical and studies should therefore not be compared
AVF21072
Phase 3 n PFS ORR OS
IFL + placebo 411 6.2 35% 15.6
IFL + bevacizumab 402 10.6 45% 20.3HR: 0.66 p<0.001
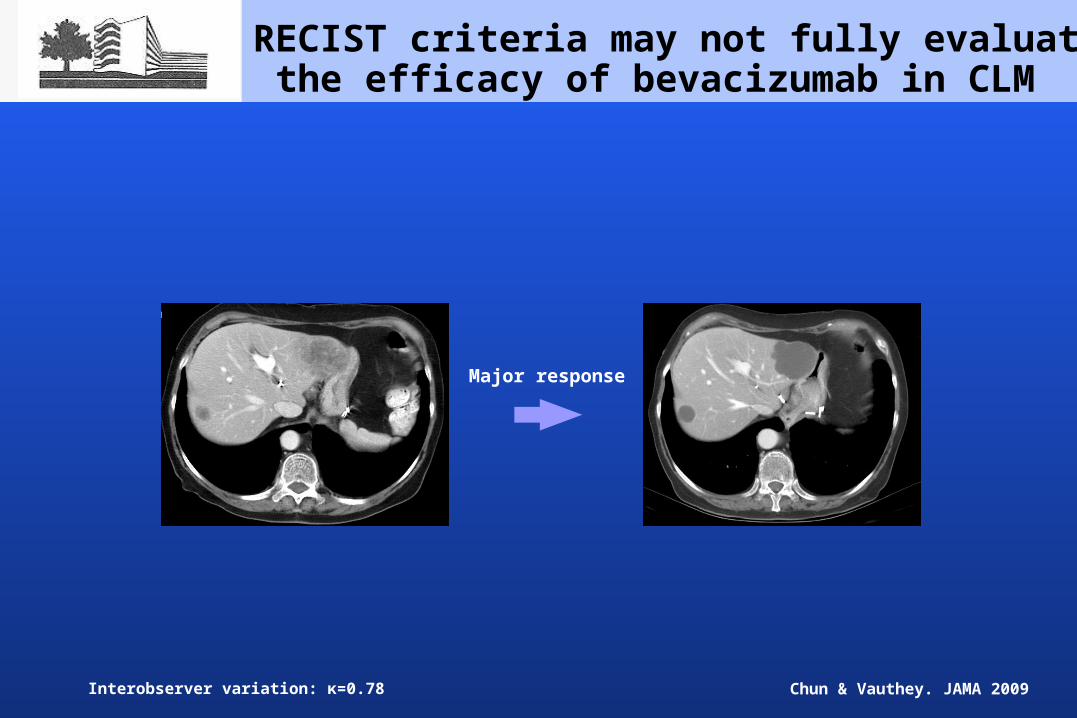
RECIST criteria may not fully evaluate the efficacy of bevacizumab in CLM
Major response
Interobserver variation: κ=0.78 Chun & Vauthey. JAMA 2009
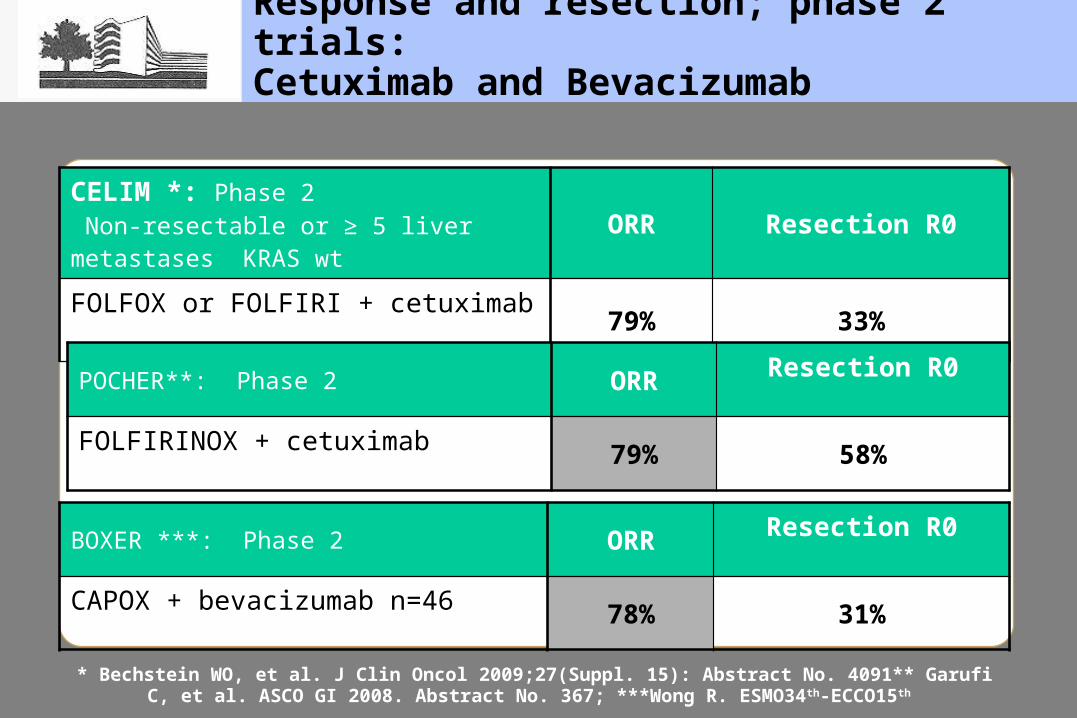
Response and resection; phase 2 trials:Cetuximab and Bevacizumab
CELIM *: Phase 2 Non-resectable or ≥ 5 liver metastases KRAS wt
ORR Resection R0
FOLFOX or FOLFIRI + cetuximab 79% 33%
* Bechstein WO, et al. J Clin Oncol 2009;27(Suppl. 15): Abstract No. 4091** Garufi C, et al. ASCO GI 2008. Abstract No. 367; ***Wong R. ESMO34th-ECCO15th
POCHER**: Phase 2 ORR Resection R0
FOLFIRINOX + cetuximab 79% 58%
BOXER ***: Phase 2 ORR Resection R0
CAPOX + bevacizumab n=46 78% 31%
Targeted therapies and risk of surgical complications
- EGFR blockers: no interference with surgery
- VEGF inhibitors: surgery delayed 6 – 8 weeks
Targeted agents in resectable metastases
Standard treatment is FOLFOX4 Should we extrapolate that « the most effective
regimen » is the best? Which reference? Metastatic or adjuvant
treatment?
Ongoing and future trials in resectable metastasis
CRUK 06/031: FOLFOX ± cetuximab in KRAS WT
EORTC: 2 trials
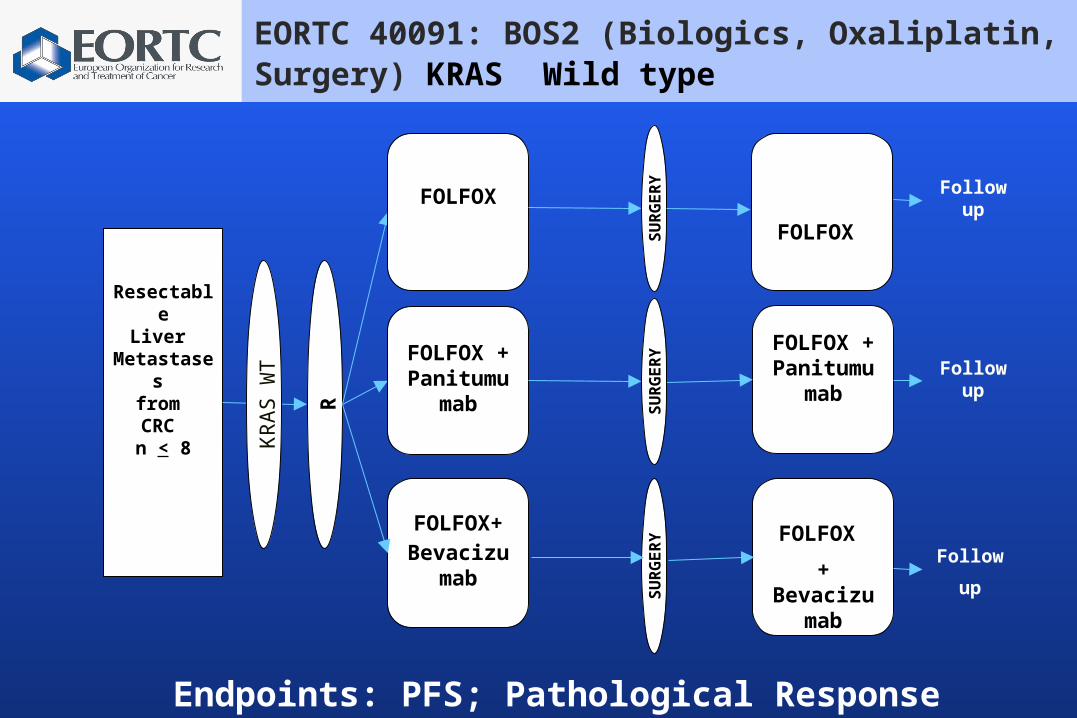
FOLFOX + Panitumu
mabRResectable
Liver Metastases
from CRC n < 8
FOLFOX
FOLFOX + Panitumu
mab
FOLFOX Follow
up
Follow up
SUR
GER
YSU
RG
ERY
FOLFOX+Bevacizum
ab
SUR
GER
Y
FOLFOX + Bevacizu
mabFollow
up
KR
AS
WT
EORTC 40091: BOS2 (Biologics, Oxaliplatin, Surgery) KRAS Wild type
Endpoints: PFS; Pathological Response
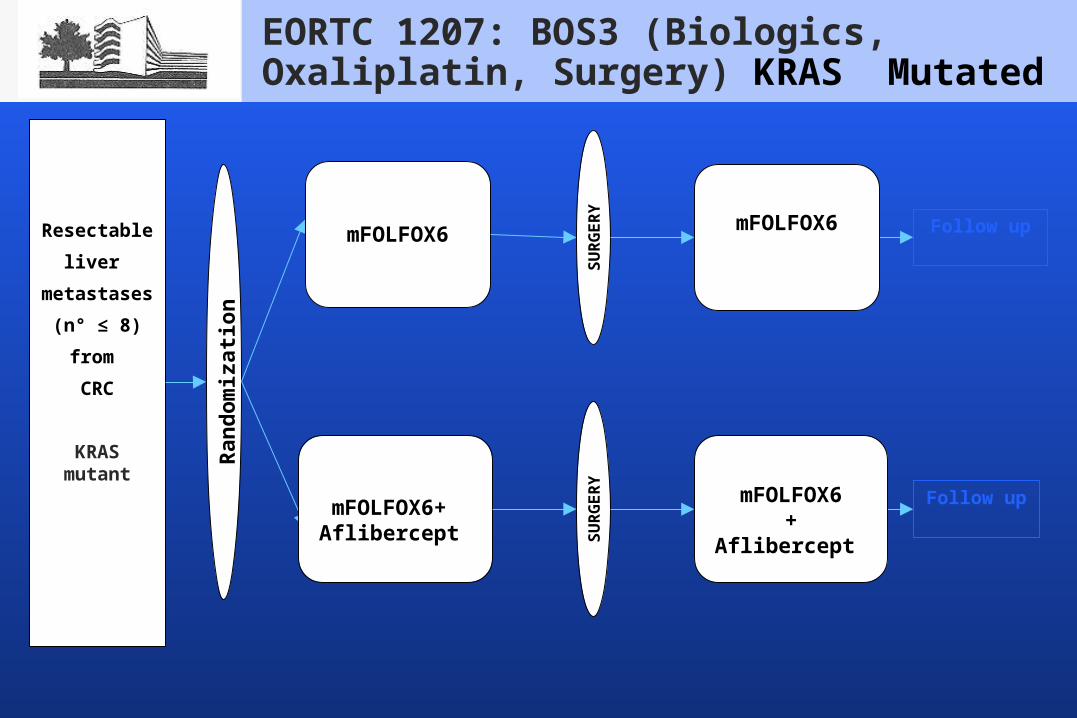
EORTC 1207: BOS3 (Biologics, Oxaliplatin, Surgery) KRAS Mutated
Ran
dom
izat
ion
Resectableliver
metastases (n° ≤ 8)from CRC
KRAS mutant
mFOLFOX6 Follow up
SUR
GER
Y
mFOLFOX6
mFOLFOX6+ Aflibercept SU
RG
ERY
mFOLFOX6+ Aflibercept
Follow up
Targeted agents in unresectable metastases
Aim is resection Regimen with high response rate - intensified chemotherapy - addition of biologics to chemotherapy
Question:
Should all patients presenting with liver metastases be considered for resection?
Patients usually divided in 3 groups:- Resectable- Never resectable- Potentially resectable in case of good response
to chemotherapy
Some patients have such a major response to chemotherapy that it allows to consider surgery although not expected initially
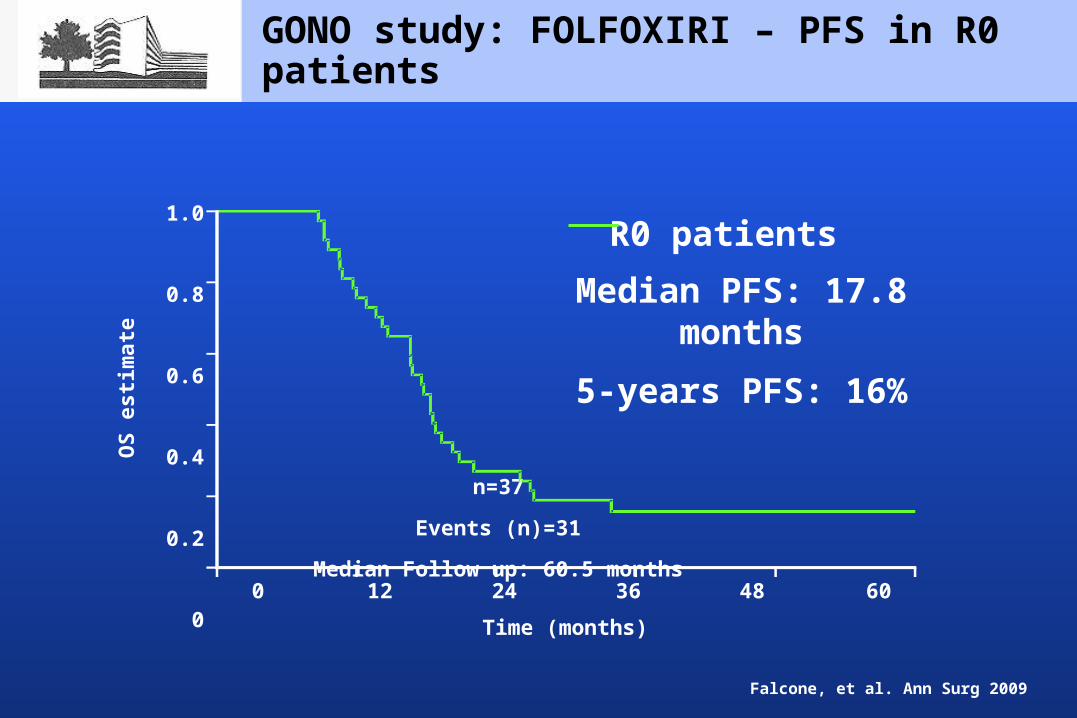
Falcone, et al. Ann Surg 2009
GONO study: FOLFOXIRI – PFS in R0 patients
Median PFS: 17.8 months
5-years PFS: 16%
Time (months)0 12 24 36 48 60
1.0
0.8
0.6
0.4
0.2
0
R0 patients
OS
estim
ate
n=37
Events (n)=31
Median Follow up: 60.5 months
Resection after chemotherapy
Resection after chemotherapy: Never say never; keep eyes open Be aware that resection does not solve all the
problems Discuss all patients in multidisciplinary meetings
Any other question?