beta-blocker use and morbidity from chronic lung disease in patients ... · ii beta-blocker use and...
TRANSCRIPT

Beta-Blocker Use and Morbidity from Chronic Lung Disease in Patients Undertaking Pulmonary
Rehabilitation
by
Robert Gabriel Varadi
A thesis submitted in conformity with the requirements for the degree of Master of Science (Clinical Epidemiology)
Graduate Department of Health Policy, Management and Evaluation University of Toronto
© Copyright by Robert Gabriel Varadi 2014

ii
Beta-Blocker Use and Morbidity from Chronic Lung Disease in
Patients Undertaking Pulmonary Rehabilitation
Robert Gabriel Varadi
Master of Science
Graduate Department of Health Policy, Management and Evaluation
University of Toronto
2014
Abstract
Cardiovascular diseases are common in patients with chronic lung diseases. Beta-blockers
reduce their morbidity, but are underutilized because of concerns over pulmonary side effects.
In this retrospective cohort study, we evaluated the association of beta-blocker use with
survival in elderly patients enrolled in pulmonary rehabilitation between 1996-2008. Patient
characteristics were abstracted from hospital charts and linked to administrative health
databases. Primary outcome was time to death or first hospitalization. Matching on propensity
score was used to account for potential confounding. No significant increase was seen in the
hazard of death or hospitalization in beta-blocker users. In patients with obstructive lung
disease, survival was non-significantly longer among beta-blocker users. Residual imbalance
in important confounders remained despite repeated refinement of the propensity-score.
Survival to death or hospitalization was not significantly associated with beta-blocker use.
Beta-blockers should not be withheld from patients with lung disease who have clinical
indications for them.

iii
Acknowledgments
Firstly, to my supervisor, Dr. Matthew Stanbrook, and to the members of my thesis committee,
Dr. Roger Goldstein and Dr. Don Redelmeier, for their unfailing support, dedication,
mentorship and education through all stages of the Master’s program.
To Dr. Rachael Evans, my one-time office mate, for her invaluable assistance in data collection
and verification, and her appreciation for the wit of Eddie Izzard.
To the clinical and administrative staff at West Park Healthcare Centre, for their
encouragement, good cheer, and their help in locating lost charts and data scattered throughout
the hospital.
To Brandon Zagorski and the IT group at ICES, for guidance in SAS and troubleshooting in
data analysis.
To Amber Gertzbein and Errin Barker, for helping me navigate the SGS maze.
To my family and friends, for putting up with my erratic hours and absentmindedness, and for
always being in my corner. And most of all, to my wife Mariana and my sons, for always
being the best possible reasons to close the computer.

iv
Table of Contents
Acknowledgments ......................................................................................................................... iii
Table of Contents............................................................................................................................iv
List of Tables ..................................................................................................................................vi
List of Figures................................................................................................................................vii
Chapter 1 : Background ...................................................................................................................1
Chapter 2 : Methods.........................................................................................................................5
1 Design .........................................................................................................................................5
2 Population ...................................................................................................................................5
3 Administrative data sources........................................................................................................6
4 Exposure .....................................................................................................................................6
5 Outcome......................................................................................................................................7
6 Baseline characteristics and potential confounders ....................................................................8
7 Data verification .........................................................................................................................9
8 Analysis ......................................................................................................................................9
9 Sample size / Power..................................................................................................................12
Chapter 3 : Results.........................................................................................................................13
1 Cohort creation .........................................................................................................................13
2 Data verification .......................................................................................................................13
3 Validity .....................................................................................................................................14
4 Baseline characteristics.............................................................................................................14
5 Unadjusted analysis ..................................................................................................................15
6 Propensity score matching ........................................................................................................16
7 Adjusted analysis ......................................................................................................................17
v
8 Obstructive lung disease subgroup ...........................................................................................17
Chapter 4 : Discussion ...................................................................................................................19
1 Comparison to existing literature..............................................................................................19
2 Analysis ....................................................................................................................................20
3 Issues in study design ...............................................................................................................23
4 Future directions .......................................................................................................................26
Chapter 5 : Conclusion ..................................................................................................................27
References......................................................................................................................................28
Tables.............................................................................................................................................36
Figures ...........................................................................................................................................59

vi
List of Tables
1. Definition of medication classes.
2. Comorbidities.
3. Cardiorespiratory diagnostic codes.
4. Standardised differences.
5. Missing data.
6. Beta-blocker use by year of entry to study.
7. Baseline characteristics, entire cohort.
8. Baseline characteristics, matched sample, using primary propensity score model.
9. Baseline characteristics, matched sample, using secondary propensity score model.
10. Baseline characteristics, moderate obstructive lung disease subgroup.
11. Baseline characteristics, moderate obstructive lung disease subgroup, matched sample.
12. Survival analysis
a. Whole cohort, unadjusted.
b. Matched cohort, primary propensity score model.
c. Matched cohort, secondary propensity score model.
d. Moderate obstructive lung disease subgroup, unadjusted.
e. Moderate obstructive lung disease subgroup, matched.

vii
List of Figures
1. Power plots.

1
Chapter 1 : Background
Heart disease frequently coexists or develops in patients with chronic lung diseases.
Investigators have attributed this association to common risk factors such as advanced age and
cigarette smoking, to common pathophysiology such as systemic inflammation, and to
medication toxicity [1, 2]. Coronary artery disease (CAD) has been described in 10-20% of
patients with chronic obstructive pulmonary disease (COPD) [3, 4], while angiographic
evidence of CAD has been found in nearly 30% of transplant-listed patients with idiopathic
pulmonary fibrosis (IPF) [5-7]. Similarly, up to a third of patients with congestive heart failure
(CHF) carry a diagnosis of COPD [8]. The coincidence of both lung and heart disease
portends a poorer prognosis than the presence of either in isolation [9-11]. In large cohorts,
decreased lung function has been shown to predict increased cardiovascular mortality [12-15].
Cardiovascular complications account for up to a quarter of deaths in COPD [16] and for 10-
30% in interstitial lung diseases [17-19]. As such, management of chronic lung diseases must
include concurrent strategies to manage coexistent cardiac disease.
Beta-adrenergic receptor inhibiting agents, or beta-blockers, reduce mortality and morbidity
associated with a wide variety of cardiac diseases, including acute coronary syndromes and
myocardial infarction (MI) [20, 21]; stable angina pectoris [22, 23]; congestive heart failure
(CHF) [24]; hypertension [25]; and arrhythmias [26-28]. They have also been shown to
reduce cardiac morbidity in the perioperative period [29, 30]. There has long been concern that
non-selective beta-blockade in patients with obstructive lung diseases would inhibit beta-2-
receptor-mediated bronchodilatation, resulting in bronchoconstriction and clinical deterioration
[31, 32]. Because of this concern, patients with lung diseases were excluded from many
clinical trials of beta-blockers [33-37], while practice guidelines and review articles have listed
asthma and COPD as contraindications to beta-blocker use [38-40].
The first generation of beta-blockers were non-selective agents that inhibited both major beta-
adrenergic receptor subtypes. The subclass of beta-1 receptor blockers are considered
cardioselective, as they have a 20-fold greater affinity for the beta-1 adrenergic receptor that
predominate in cardiac tissue. With a lower affinity for beta-2 receptors, they carry a lower

2
theoretical risk of bronchoconstriction [41]. Meta-analyses of trials of short-term
administration of cardioselective beta-blockers in patients with obstructive lung diseases have
showed no significant effect on lung function compared to placebo, nor any loss of sensitivity
to the bronchodilating effects of short-acting beta-2 agonists (SABA) [42-44]. Though the
results are reassuring, the pooled studies were small and focused on surrogate physiologic, not
clinical, endpoints. Moreover, deleterious effects on exercise performance, such as increased
dynamic hyperinflation in COPD, and on symptoms may be seen without deterioration in static
lung function [45].
No clinical trial has yet prospectively tested the effects of long-term beta-blocker use in
chronic lung disease. A number of investigators have shown good clinical outcomes in
observational studies of patients with chronic lung diseases treated with BB.
Mortality was reduced in patients with COPD or asthma treated with beta-blockers following
an acute MI, compared to those in whom beta-blockers were withheld [46, 47]. Though not
statistically significant, lower hospital readmission rates for COPD or asthma were also seen in
the beta-blocker users [46]. Since respiratory disease parameters such as pulmonary function
were not available, these studies were unable to adequately adjust for confounding by severity
of lung disease. It is possible that those treated with beta-blockers had, on average, less severe
lung disease and thus better survival. Moreover, cardiac disease is the most common causes of
death in the immediate period after acute MI, and accounts for the majority of deaths over the
1-2 years of follow-up. This may have biased the studies in favour of beta-blockers and
masked any deleterious respiratory effects.
Chronic use of beta-blockers has been shown to reduce mortality in patients with COPD and
hypertension, compared to other antihypertensives [48], and to blunt the apparent cardiac
toxicity of SABA [49]. COPD in this study was defined by self-report, which is susceptible to
misclassification. Frequency of exacerbations was used to adjust for disease severity, but
pulmonary function and other respiratory parameters were not measured.
Patients with coexistent COPD and CHF treated with carvedilol, a combined alpha- and non-
selective beta-blocker, have shown improvements in cardiovascular function without notable
pulmonary complications [50].

3
Among patients admitted for acute exacerbations of COPD, in which heart disease frequently
contributes to mortality, those treated with beta-blockers were found to have lower in-hospital
mortality than those not so treated, irrespective of their indication [3]. This study was unique
in focusing on a population whose risk of morbidity was most strongly related to pulmonary as
opposed to cardiac disease. However, as only short-term outcomes were considered and
follow-up not extended beyond hospital discharge, conclusions about long-term safety and
efficacy cannot be drawn. Similar to previous studies, pulmonary function data was not
included in the analysis.
Owing in part to these studies’ weaknesses, clinical practice has not been significantly
impacted, and studies continue to find beta-blockers are underutilised in chronic lung diseases
[51-55]. For instance, in one retrospective study of patients hospitalised for an acute coronary
syndrome, only 16% of those diagnosed with lung disease were discharged on beta-blockers
[54].
Pulmonary rehabilitation may provide a unique setting in which to investigate the role of beta-
blockers in treating the pulmonary patient. Pulmonary rehabilitation is recognized as a central
component in the management of chronic lung diseases [56, 57]. In COPD, strong evidence
supports the benefits of pulmonary rehabilitation in reducing dyspnea, improving exercise
capacity and quality of life, and reducing hospital and ER admissions and possibly all-cause
mortality. An increasing body of literature also supports the value of pulmonary rehabilitation
in other lung diseases [58, 59]. Patients enrolling in pulmonary rehabilitation are well
characterised at baseline, providing a wealth of variables that may be important potential
confounders, including pulmonary function and exercise capacity. Since the patients entering
pulmonary rehabilitation generally have more severe disease, heart disease is more prevalent in
this population [60, 61]. This should result in a higher rate of cardiac events over time and
provide greater power to detect a protective effect of beta-blockers. Access to pulmonary
rehabilitation in Canada is limited: it is estimated that rehabilitation program capacity exists
for only 1.2% of the eligible population with COPD [62]. Appropriate referral to pulmonary
rehabilitation may thus be considered a marker of better quality of respiratory care. As
pulmonary rehabilitation demands a major investment of time and effort, patients enrolling are
likely more highly motivated and more health-conscious than the general population with lung
4
disease [63-65]. Finally, a major goal of pulmonary rehabilitation is to increase patients’
physical activity in day-to-day life. In one study, over 80% of subjects reported adherence to a
home exercise program for 6 months after completing pulmonary rehabilitation, and over 50%
maintained adherence through one year’s follow-up [66]. These habits are likely to reduce the
potential for confounding by behavioural and social factors, and strengthen the conclusions
drawn on the effects of beta-blockers.
We therefore sought to assess the impact of beta-blocker use on morbidity from chronic lung
disease, as reflected by death and hospitalization, in patients undertaking pulmonary
rehabilitation. We hypothesized that, in patients enrolling in inpatient pulmonary
rehabilitation, use of beta-blockers will be associated with longer time to death or first
hospitalization for cardiac or respiratory condition.

5
Chapter 2 : Methods
1 Design
This was a retrospective cohort study, in which data from primary chart abstraction was
supplemented by administrative data sources.
2 Population
West Park Healthcare Centre (WPHC) provides a program of pulmonary rehabilitation in both
inpatient and outpatient settings. The rehabilitation centre is served by an experienced
multidisciplinary team, and all patients are assessed by a respiratory physician prior to
enrolment. Potential participants must have quit smoking prior to enrolment. The standard
inpatient pulmonary rehabilitation course is of 6-weeks’ duration. Patients undergo
individualized exercise training including aerobic exercise at least 3 days per week, according
to established practice guidelines [56, 57]. Activities include treadmill, cycling, interval
training (alternating high and low power exercise), upper-extremity weight training, and leisure
walking. Patients experiencing exercise-induced oxygen desaturation are trained with
supplemental oxygen according to routine practice. Other components of the program include
education and self-management, nutritional counselling, and psychosocial support. Adverse
events arising during rehabilitation are assessed by the attending respirologist. Since WPHC
does not have acute care facilities, inpatients suffering any potentially serious complications
are discharged from WPHC and transferred to nearby acute care hospitals.
Eligible patients were adults with any chronic lung disease, aged at least 66 years on the date
of admission to inpatient pulmonary rehabilitation at WPHC. Patients must have undertaken at
least one exercise test or exercise training session following admission to be included in the
study. A baseline value for the forced expiratory volume in 1 second (FEV1) was required for
inclusion. The inception cohort consisted of all eligible patients enrolled between January 1,
1996 and December 31, 2008. Patients with COPD were identified as those meeting Canadian
Thoracic Society criteria [67], including: 1) compatible chronic respiratory symptoms; 2)
FEV1 < 80% of predicted normal; 3) FEV1/FVC ≤ 0.7; 4) incomplete bronchodilator

6
reversibility of FEV1 and FEV1/FVC (if results available). A subgroup of patients with
moderate-to-severe obstructive lung disease was identified as having FEV1 < 80% of predicted
normal and FEV1/FVC ≤ 0.7, regardless of the underlying diagnosis. The date of admission
served as the index date for analysis. Inpatient admission records were used to identify
potential study patients, and individual charts were manually reviewed for eligibility. In the
event of multiple pulmonary rehabilitation admissions for the same subject, only the first
eligible admission was included.
3 Administrative data sources
Administrative data sources were used to define the patients’ exposure to medications,
supplement baseline characteristics, and assess outcomes. The Canadian Institute for Health
Information – Discharge Abstract Database (CIHI-DAD) contains demographic and clinical
data on all hospital admissions in Ontario from 1988 through the last update of March 2011.
Coverage is exhaustive, with fewer than 0.01% of values missing for variables containing
demographic data, dates of admission, disposition, and main diagnosis [68]. The Registered
Persons Database (RPDB) contains the vital status of all persons issued a health insurance
number in Ontario since 1990. Date of death is gleaned from multiple sources and considered
accurate through the date of last CIHI-DAD update. The Ontario Drug Benefits (ODB)
program provides publicly-funded coverage for prescription medications to all insured Ontario
residents over the age of 65. The ODB database provides records of all drug claims (dispensed
prescriptions) paid through the ODB since April 1990, including name, date and quantity of
medication dispensed. Coding of ODB records has been validated against original
prescriptions, with an error rate of less than 1% [69]. All physician services billed to the
provincial public health insurance plan are captured in the Ontario Health Insurance Plan
(OHIP) database. Records include the date, setting, and type of service provided. Each
individual Ontario resident’s records are linked across all these databases using a unique
identification number based on the encrypted health insurance number.
4 Exposure
The exposure of interest was use of beta-blockers prior to enrolment in pulmonary
rehabilitation. Beta-blocker use was determined based on records of beta-blockers

7
prescriptions in the ODB database. Since direct evidence of medication use was not possible
in this study design, drug exposure is defined as two or more prescriptions for beta-blockers
dispensed within the year prior to admission to pulmonary rehabilitation; at least one
prescription must have been filled within 100 days prior to admission, the maximum supply a
pharmacy will dispense at a single visit. The practice in the pulmonary rehabilitation program
at WPHC is to continue prescribing all non-respiratory medications that an incoming patient
had been receiving, unless there is a strong clinical indication to do otherwise. Therefore,
patient receiving beta-blockers prior to enrolment would routinely have continued to receive
them upon completion of the program.
The following beta-blockers are listed for coverage on the ODB formulary: beta-1-selective
agents, including atenolol, bisoprolol, metoprolol, acebutolol; nonselective agents, including
nadolol, oxprenolol, pindolol, propranolol, timolol; and the combined alpha-/beta-blockers
carvedilol and labetalol. Because of its distinct indication as an antidysrrhythmic, prescriptions
for sotalol were not considered beta-blocker use.
5 Outcome
All outcome data were derived from administrative databases. The primary outcome was the
combined endpoint of death or first acute care hospital admission for any cardiac or respiratory
diagnosis. Since all patients transferred to an acute care centre from the inpatient pulmonary
rehabilitation unit are considered discharged from WPHC, this definition includes those
patients experiencing a serious adverse event during the rehabilitation course. Secondary
endpoints include all-cause hospitalisation, and cardiac and respiratory admissions considered
separately, and death alone. Admission for COPD exacerbation were also considered as a
distinct endpoint.
5.1 Death
The final study date was March 31, 2011, which was the date of the final update of the CIHI-
DAD database for the year 2010. Vital status for all patients was determined by linkage to the
RPDB. A subject was considered to have died if there was a recorded date of death falling on
or before March 31, 2011.

8
5.2 Hospital admission
Acute-care hospitalisations were identified by linkage to CIHI-DAD. The database contains
validated fields for dates of admission and discharge, most responsible diagnosis (MRD), and
procedures. An admission episode may include multiple consecutive hospital admissions, each
of which is assigned a separate MRD. In such cases, the listed MRD for the first admission
within an episode was retained. Diagnoses in CIHI-DAD are classified according to the ICD-9
and -10 systems, depending on the era. Table 3 lists the ICD-9 and -10 diagnosis codes we
used to identify admissions as cardiac or respiratory.
5.3 Lung transplantation
Patients who undergo lung transplantation have a risk of morbidity and mortality that is unique
and substantially different from the general population of patients with chronic lung disease.
As such, study patients who received a lung transplant had their outcome data censored at the
time of admission for transplant. The following lung transplant procedure codes were
identified: 4550 or 4560 under the Canadian Classification of Diagnostic, Therapeutic and
Surgical Procedures [CCP]; 1GR85, 1GT85, or 1HY85 under the Canadian Classification of
Health Interventions [CCI]. If, in the course of a single admission episode, a subject admitted
to a first acute-care institution had subsequently been transferred to a second for the purpose of
lung transplantation, the initial non-transplant admission was included in the outcome
assessment, while the second was excluded and further data censored.
6 Baseline characteristics and potential confounders
Demographic and anthropomorphic data; measures of static pulmonary function, exercise
capacity, and gas exchange; and comorbidities were obtained by primary chart abstraction.
Primary and secondary respiratory diagnoses were determined from the attending
respirologist’s diagnosis, supplemented by the available clinical materials. Cardiovascular and
metabolic comorbidities were determined based on prespecified criteria (table 2). The
Charlson index was used to summarize the total burden of comorbidities [70].
Health care utilization was reflected by the quantity of acute care visits made within the two
years prior to the index date. The number of acute care hospitalizations and cumulative length

9
of stay in hospital was calculated from CIHI-DAD records. OHIP billing records were used to
compute the number of Emergency Department visits.
Use of non-beta-blocker medications was determined by linkage to ODB records (table 1).
Patients were considered users of a particular class of medication if they had filled at least one
prescription in that class within the year prior to the index date. Respiratory medications
included inhaled short- and long-acting anticholenergics, inhaled short- and long-acting beta-
agonists, inhaled corticosteroids, leukotriene antagonists, and methylxanthines. Cardiovascular
medications included angiotensin pathway inhibitors, HMG-CoA-reductase inhibitors
(‘statins’), antiplatelet agents, diuretics, nitrates, digoxin, calcium-channel blockers, and
vasodilators. Other potentially important medications included alpha-adrenergic blockers and
ophthalmic beta-blockers preparations. Since aspirin is also available for over-the-counter
purchase without a prescription, ODB records may not accurately reflect aspirin use in the
population.
7 Data verification
Average (mean and median), maximum and minimum values for all abstracted data were
reviewed; records whose values appeared improbably extreme were re-abstracted. A second
investigator, a practicing respirologist, independently abstracted the respiratory diagnoses from
48 patients’ charts selected at random. The primary and, if applicable, secondary diagnoses
were assigned to one of 7 lung disease groupings: COPD; other obstructive diseases;
interstitial lung diseases; extraparenchymal restrictive diseases; pulmonary hypertension; lung
resection; and other conditions. Concordance between the two investigators was assessed
using the unweighted Kappa score [71, 72].
8 Analysis
Event-free survival was computed between the index date and date of endpoint. Survival for
the patients who were alive and did not have a recorded hospitalisation by the final study date
was censored either at the final study date or at the date of last contact recorded in RPDB,
whichever was earliest.

10
Baseline characteristics were summarized with descriptive statistics. Crude unadjusted
estimates of survival among beta-blocker users and non-users were generated by Kaplan-Meier
method accounting for censoring. Multivariable analysis was performed to account for
possible confounding. Statistical analysis was performed using SAS (SAS 9.2 for Windows,
SAS Institute Inc., Cary, NC, USA). The level of significance for all tests was 0.05.
8.1 Propensity score matching
In circumstances in which the number of outcome events is small relative to the number of
variables analysed, survival analysis by multivariable regression modeling may produce results
that are biased and unreliable [73, 74]. Adjustment based on the propensity score does not
suffer from this limitation [75]. The propensity score is defined as the conditional probability
of having received an intervention, given a set of covariates. This probability provides a single
number as summary of a set of measured covariates [76, 77]. However, it does not necessarily
balance important confounders that are unmeasured or not included in the propensity score
model [78]. Propensity score can be estimated using a logistic regression model:
( ) jjXβ̂ˆ
ˆ1
ˆloglogit 0 +=
−= β
i
i
e
ePS
where ie)
is the estimated propensity score for an individual patient, representing in this study
the probability of beta-blocker use; and ββββjXj is the vector of covariates and their regression
coefficients. All potentially important covariates were included in the initial propensity score
model as main effects. Based on residual imbalances between beta-blocker users and non-
users, the model was then refined using an iterative approach, allowing for interaction terms,
and quadratic and cubic terms for continuous variables [79].
Three techniques are commonly employed to reduce confounding using the propensity score:
matching, stratification, and covariate adjustment; more recently a new technique, inverse
probability of treatment weighting, has been introduced. Covariate adjustment methods may
be less reliable, and are sensitive to inaccurate modeling of the propensity score in the final
regression model [76, 80]. Matching and stratification techniques are not dependent on correct
model specification, and are therefore preferred. From studies on stratification by a single
11
continuous variable, it has been demonstrated that stratifying on quintiles of propensity score
should similarly remove 90% of the bias due to imbalance in all measured covariates used in
the construction of propensity score [79] [81]. The stratified analysis may use data from a
greater proportion of eligible patients, while the matched analysis discards untreated patients
who are dissimilar to treated patients. However, stratification may result in a greater
imbalance in covariates than is seen with matching [80]. As such, matching was chosen as the
primary analytic method.
A 1:1 matching ratio was employed in a “greedy” matching strategy, using a standard
technique. A random beta-blocker user was selected and paired with the non-beta-blocker user
who had the closest match on the logit of the propensity score, within a caliper width of 0.2
times the standard deviation of the logit of the propensity score [82]. Matching was performed
without replacement; once matched, the non-beta-blocker user was removed from the sample
and could not serve as match for any of the following beta-blocker users. Matching continued
until all beta-blocker users had been matched, or until no satisfactory match was identified. An
“optimal” matching algorithm, by contrast, would select the best non-user matches so as to
minimize the total within-pair differences in propensity score across the entire matched cohort.
Such an algorithm is computationally very demanding, and may not provide a significant
benefit to balance [102].
The success of balancing measured covariates was assessed numerically by computing
standardised differences for each measured covariate (table 4). It has been suggested that a
standardised difference of more than 10% represents meaningful imbalance in a covariate [83].
It was expected that many patients would be missing values for some important covariates
abstracted by chart review. A propensity score model based solely on patients with complete
data would exclude patients with any missing data and thus restrict the sample size. Missing
values were imputed using the SAS Multiple Imputation procedure, with 20 imputed data sets
created. Their estimates were pooled in order to develop the propensity score model. At this
point, the imputed data were discarded; assessment of covariate balance and analysis of
treatment effect was performed on the original data set containing actual, not imputed, data.

12
Cox proportional-hazard modelling was used to estimate the effect of beta-blocker use on
event-free survival, stratified on matched-pair. Analysis was performed for the primary and
secondary endpoints.
A planned subgroup analysis was performed in patients with moderate obstructive lung
disease. Matching was done using the same primary propensity score model as for the primary
cohort.
9 Sample size / Power
An estimated 1200 eligible elderly patients (120 patients admitted each year, 75% over age 65)
have enrolled in pulmonary rehabilitation at the study centre over the 13 year accrual period;
10-20% of these were expected to be beta-blocker users. Patients have a high morbidity
following completion of pulmonary rehabilitation. The literature suggests that 35-40% of
patients with severe disease are admitted to hospital within one year after discharge from a
program [84, 85], and approximately 5% die within one year [61, 86]. In experimental and
observational studies of patients with acute MI, chronic CHF or hypertension, treatment with
beta-blockers has been associated with relative reductions of 15-40% in the risk of death and
hospitalization, even in patients with COPD [46-48, 87, 88]. Given the lower baseline cardiac
risk in the population in pulmonary rehabilitation, a more conservative estimate of risk
reduction of 10-20% was expected.
In estimating the required sample size, a median event-free survival time of 24 months was
assumed for the non-beta-blocker user group. With 900 patients accrued over 13 years, 20% of
whom were beta-blocker users, the study would have at least 80% power to detect a hazard
ratio of 0.78, or a reduction in hazard of death or hospitalisation of at least 22% (two-sided
alpha=0.05) (figure 1, upper panel). With the same sample size of 900 patients, the smallest
detectable HR would range from 0.83 to 0.74, if median survival fell in the range of 12-36
months (figure 1, lower panel).

13
Chapter 3 : Results
1 Cohort creation
Administrative records at West Park Healthcare Centre identified 3800 admissions to the
inpatient respiratory unit over the inception period from January 1, 1996, through December
31, 2008. 1906 admissions involved patients aged at least 66 years. Excluding 735 repeat
admissions, 1171 individual patient admission records were identified for full review. Data
were abstracted from several discrete sources, including the primary hospital chart, the
outpatient Respiratory Medicine clinic chart, the pulmonary function laboratory, and the
departments of Respiratory Therapy and of Physiotherapy. 132 patients were excluded after
chart review: 33 were missing value for the FEV1; 32 had a permanent tracheostomy; 34 were
admitted for mechanical ventilation assessment only; 22 were admitted for but did not
participate in pulmonary rehabilitation; and 11 charts could not be located. 1039 patients were
included in the final cohort.
The cohort was then linked to provincial administrative databases held at the Institute for
Clinical Evaluative Sciences. For each subject, linkage was performed using a unique
identification number based on the encrypted health insurance number. All 1039 (100%)
patients in the cohort were successfully linked to the administrative databases.
2 Data verification
Data were reviewed to identify outliers with improbable values; these variables were then
reabstracted from the original source. Only 4 errors required correction. No errors were
identified in variables considered important potential confounders.
Variables for which data were incomplete are listed in table 5. Complete data were available
for all demographic, comorbidity, medication, and health care utilization variables. Fewer than
10% of values for gas exchange and exercise capacity variables were missing. MRC dyspnea
score was not provided or could not be accurately computed for 17% of patients. The Chronic

14
Respiratory Questionnaire health status score was not available for over 50% of patients; as
such, this parameter was not included in the analysis.
Event dates recorded in the Registered Persons Database were compared against similar dates
recorded in Discharge Abstracts Database. In no instance did a hospital admission date fall
after the recorded date of death or date of last contact.
3 Validity
There was substantial agreement between the independent data abstractors on the respiratory
diagnosis considered primary (Kappa=0.74). There was very strong agreement on the presence
of a respiratory diagnosis, irrespective of its being considered primary or secondary
(Kappa=0.89). Agreement was similarly very strong when the primary diagnosis was
dichotomized as COPD or other (Kappa=0.82).
4 Baseline characteristics
53 (5.1%) patients met the criteria for beta-blocker use, having filled a total of 365
prescriptions for beta-blockers in the year prior to the index date. The majority of patients
received beta-1-selective agents including metoprolol (20 patients [34%]), atenolol (18 [31%]),
and bisoprolol (13 [22%]). Other beta-blockers agents included carvedilol (4 [7%]), acebutolol
(3 [5%]), and propranolol (1 [2%]). 6 patients had filled prescriptions for two distinct beta-
blockers. One subject prescribed bisoprolol had also filled 4 prescriptions for sotalol in the
year prior to index date.
Beta-blocker use varied with era of study, with a greater proportion of beta-blocker use seen in
patients entering the cohort in later years (table 6). Beta-blocker users accounted for only 1.6%
of patients entering the cohort between 1996-2003, but 13.4% of patients entering between
2004-2008. Among beta-blocker users, the median year of entry to the cohort was 2006, as
compared to 2001 among non-beta-blocker users. Overall, patients in the more recent era were
more likely to have a non-COPD diagnosis, more frequently had cardiac comorbidities, and
had greater use of cardiac and long-acting respiratory medications.

15
Baseline characteristics of beta-blocker and non-beta-blocker users are presented in table 7.
Beta-blocker users were on average older, less likely to be married, and residing in more
affluent neighbourhoods. There was no significant difference in use of acute medical care in
the 2 years prior to index date. A greater proportion of beta-blocker users did not have a
diagnosis of COPD, and had reported never smoking. Pulmonary function was on average
severely impaired in the cohort. Spirometric values and total lung capacity in beta-blocker
users were less severely perturbed, though this may also reflect the greater proportion of non-
obstructive lung diseases. The diffusing capacity was severely reduced to a similar degree in
both groups. Self-reported dyspnea, as measured by both the MRC score and the CRQ
dyspnea subscale, was more severe in beta-blocker users, and exercise capacity and resting
oxygen levels were poorer.
Overall, 653 (62.8%) patients in the cohort had a diagnosis of at least one cardiovascular or
metabolic disease, while 597 (57.5%) patients had at least one diagnosis considered an
indication for beta-blockers. Beta-blocker users had a greater burden of comorbidities, as
measured by the Charlson Comorbidity Index, and individual cardiovascular and metabolic
comorbidities were more common in beta-blocker users. The mean number of distinct
medications used in the past year was significantly greater in beta-blocker users. A greater
proportion of beta-blocker users had filled prescriptions for important cardiac medications.
The pattern of use of respiratory medications between the groups was mixed: significantly
more beta-blocker users were prescribed inhaled long-acting anticholenergic and beta-agonist
agents, while prescriptions for inhaled corticosteroids, short-acting bronchodilators, and
methylxanthines were significantly less common in this group.
5 Unadjusted analysis
There were 4067 hospital admission episodes among all 1039 patients during the follow-up
period. Among the 53 beta-blocker users, there were 129 admissions: 64 (50%) for a
respiratory diagnosis, 50 (39%) for COPD, and 16 (12%) for a cardiac diagnosis. Among the
986 non-beta-blocker users, there were 3938 admissions: 2565 (65%) for a respiratory
diagnosis, 2149 (55%) for COPD, and 225 (6%) for a cardiac diagnosis. 97 patients, including

16
5 (9.4%) beta-blocker users and 92 (9.3%) non-beta-blocker users, did not have a record of
death or hospital admission after the index date.
In unadjusted analysis including all 1039 patients, there was no significant difference in
survival between all beta-blocker users and non-users to the primary combined endpoint of
death or cardiorespiratory hospitalization (table 12a). No significant difference was detected in
survival to combined death or all-cause hospitalization. 798 (77%) patients died during the
follow-up period, with a median survival from index date of 47.5 months. There were 38
deaths among beta-blocker users, and 760 among non-beta-blocker users. The Kaplan-Meier
estimate of median survival to death was significantly shorter in beta-blocker users (33 vs 50
months, HR 1.40, 95% CI 1.01-1.94). Beta-blocker users had a significantly increased hazard
of death or hospitalisation for cardiac disease only (HR 1.57, 95% CI 1.15-2.14), but non-
significantly longer survival to combined death or hospitalisation for respiratory disease (HR
0.85, 95% CI 0.63-1.16).
6 Propensity score matching
Despite repeated refinements to the propensity score model, there remained significant residual
imbalance in important covariates between matched beta-blocker users and non-users. A
primary propensity score model was chosen to achieve balance in the greatest number of
important cardiovascular and respiratory covariates. 31 of 53 (58%) beta-blocker users were
successfully matched to non-beta-blocker user controls (table 8). Matched cases and controls
were well balanced on cardiovascular, respiratory and metabolic comorbidities. Among
important medications, matched beta-blocker users were less commonly prescribed angiotensin
antagonists, calcium-channel blockers and nitrates, but more commonly prescribed long-acting
inhaled anticholinergics. Matched beta-blocker users had lower baseline 6MWD and diffusing
capacity, and were more likely to have smoked; they less commonly reported severe dyspnea
and were less likely to experience exertional desaturation. Though the number of hospital
admissions were similar between the two groups, matched beta-blocker users spent fewer days
in hospital over the 2 years prior to index date.
A secondary propensity score model was then designed to achieve balance in important
respiratory parameters; with this model, 35 (66%) beta-blocker users were successfully

17
matched to controls (table 9). As expected, the groups demonstrated balance on baseline
6MWD, MRC dyspnea, oxygenation measures, respiratory medication use, and smoking
status; however, mean FEV1 was greater in matched beta-blocker users than in non-users.
There was residual imbalance in comorbidities, with matched beta-blocker users having a
higher mean Charlson comorbidity score, and a greater proportion of beta-blocker users having
a diagnosis of CAD and CHF. The main difference in this model was the removal of a term for
era from the secondary propensity score model.
7 Adjusted analysis
The primary adjusted analysis was performed with 62 patients matched on the primary
propensity score (31 each beta-blocker users and non-users). No significant difference was
detected between the matched groups in survival to the combined endpoint of death or
cardiorespiratory (table 12b). Similarly, no significant association was seen between beta-
blocker use and survival to death alone or any of the combined endpoints. The point estimates
of the hazard ratio were closer to unity in all of the primary matched analyses, as compared to
the unadjusted estimates.
The secondary adjusted analysis was performed with 70 patients matched on the secondary
propensity score (35 each beta-blocker users and non-users). No significant difference in
survival was detected for the primary endpoint. A significant decrease in survival to death
alone remained among beta-blocker users, with a point estimate of effect that was higher than
in the unadjusted analysis (HR 2.22, 95% CI 1.01-4.88) (table 12c).
8 Obstructive lung disease subgroup
864 patients met criteria for at-least moderate obstructive lung disease (FEV1/FVC < 0.7, and
FEV1 < 80% of predicted normal), of whom 29 (3.4%) were beta-blocker users. COPD was
the primary diagnosis in 95% of patients. Baseline characteristics are presented in table 10.
While FEV1 was less impaired on average in beta-blocker users, exercise capacity and dyspnea
were more severely limited. As expected, beta-blocker users were more likely to have a
cardiac comorbidity and to be receiving cardiac medications. Long-acting bronchodilators
were more commonly used among beta-blocker users.

18
18 (62%) beta-blocker users were successfully matched to non-beta-blocker controls. The
matched groups were generally well balanced on important comorbidities and cardiorespiratory
medication use. Matched beta-blocker users had a tendency to milder lung disease, with a
higher mean baseline 6MWD and less severe dyspnea than non-beta-blocker users (table 11).
In unadjusted analysis of all 864 patients, no significant difference was detected between the
exposure groups in survival to any endpoint (table 12d). In the matched analysis including 36
patients (18 each beta-blocker users and non-users), no significant differences were found
between the groups in survival to any endpoint (table 12e). The point estimates for effect were
lower for all endpoints than in the unadjusted analysis, and nealy all favoured a survival
advantage among beta-blocker users, though without achieving statistical significance.

19
Chapter 4 : Discussion
1 Comparison to existing literature
Historical concerns about the deleterious effects of beta-blockers may no longer be as relevant.
Many early reports of BB-induced bronchoconstriction, reduced sensitivity to inhaled beta-
agonists, and increased respiratory symptoms, involved small series of patients exposed to non-
selective beta-blockers such as propranolol [89-91]. These agents have largely been replaced
by the cardioselective BB, which have much lower affinity for the beta-2 adrenergic receptor in
the lungs. In a meta-analysis of 20 studies including 278 patients with obstructive lung
diseases, cardioselective beta-blockers were not found to have significant impact on lung
function or symptoms [42]. Similarly, combined alpha/beta-blockers such as carvedilol may
not produce an important decline in lung function [50, 92]. 86% of beta-blockers prescriptions
in our study were for beta-1 selective agents, and only 1 patient received propranolol. Our
study design did not permit identifying patients who had previously suffered adverse effects of
beta-blockers.
There is a growing body of evidence that beta-blockers are safe for use in patients with chronic
lung disease. While our results are consistent with this, we did not demonstrate an
improvement in mortality or hospitalization. Our study included patients with any chronic
lung disease, while previous research centered on COPD and asthma. 23% of beta-blocker
users in our cohort had a primary diagnosis of an interstitial lung disease, often pulmonary
fibrosis, for which prognosis is poor and no effective treatment is available [93]. This may
have reduced our ability to detect a treatment effect. When the analysis was restricted to those
patients with obstructive disease of at least moderate severity, we found estimates of mortality
and hospitalization reduction in line with previous research, though not achieving statistical
significance. Previous studies on beta-blocker use have selected populations whose
cardiovascular risk is highest, such as following MI [46, 47] or vascular surgery [94], in
chronic CHF [95, 96] or in chronic hypertension [48]. Our study selected a population with
more severe lung disease and therefore greater pulmonary risk, as evidenced by the
preponderance of hospitalizations for respiratory diagnoses. Two studies have observed lower

20
in-hospital mortality among beta-blocker users who were hospitalized with COPD
exacerbation; however, follow-up was not extended after hospital discharge [3, 97].
Moreover, by defining medication use by in-hospital prescriptions, these studies were
vulnerable to immortal time bias.
Two recent large population-based studies of beta-blocker use in COPD have yielded
conflicting results. Short and colleagues retrospectively analysed a patient registry in
Scotland, and found that patients using beta-blockers had 22% lower mortality than non-users
over a 10-year span, irrespective of respiratory medication use [98]. This cohort was well-
characterized and accounted for FEV1 in the analysis. In a prospective study, Ekstrom and
colleagues evaluated patients with severe COPD upon initiation of home oxygen therapy [99].
They incorporated a time-dependent analysis to account for continuity of medication exposure
throughout the study period. Beta-blocker use was associated with a statistically significant
19% increase in mortality over 4 years follow-up, while other cardiac medications such as
angiotensin-pathway antagonists and statins were associated with non-significant mortality
reduction. In addition to the difference in analytic techniques, the conflicting results may in
part be attributable to severity of illness. Ekstrom et al included only severely impaired
patients with chronic hypoxemic respiratory failure, whose mean FEV1 was severely reduced
at less than 40% of predicted normal. This severity of illness more closely matches that seen in
our study. Short et al included a broader range of range of patients, only 30% of whom had
spirometrically severe COPD. It is possible that beta-blockers have differential effects based
on severity of disease. Our small number of beta-blocker users did not permit additional
analysis of this potential interaction.
2 Analysis
2.1 Choice of analytic technique
In non-randomized studies, it is important to account for differences in baseline characteristics
that may confound the relationship between treatment and outcome. Multivariable regression
modeling is commonly used to adjust for potential confounding. However, regression
modeling has been shown to be unreliable when the number of confounders is large relative to
the sample size. It has been shown that when there are fewer than 10 outcome events in the

21
smallest of the primary exposure groups for each variable analysed (generally referred to as
“events per variable”), the model proves unreliable, with excessively biased estimates of effect
and questionable validity of significance testing [73, 100, 101]. This finding has been
described in both logistic and Cox proportional hazard regression. The problems associated
with few events per variable may be more pronounced when the association between the
primary exposure and the outcome is weak, and when the sample size is small [74]. In our
study, the number of outcome events among beta-blocker users was small (at most 53); the
number of potential confounders large (as many as 50); and the association between beta-
blocker use and morbidity weak (hazard ratios no larger than 2). As such, simple multivariable
regression adjustment was not an appropriate method to account for confounding.
The propensity score provides a single summary of a set of known confounders, and may be
estimated as the probability of having received the treatment of interest based on measured
baseline characteristics. The propensity score is a balancing score, such that after conditioning
on the propensity score, the distribution of measured characteristics is similar between treated
and untreated patients. There are a number of advantages posited to propensity score methods
over multivariable regression methods alone [102]. Firstly, propensity score methods have
greater flexibility in accounting for confounders when outcomes are few, and may provide
correct estimates of treatment effect when sample size is small [103]. For instance, a
simulation study with binary outcome showed less bias and smaller standard errors in the
estimate of treatment effect using stratification on the propensity score as compared to logistic
regression, when the number of outcome events was small [75]. Secondly, it is easier and
more explicit to assess the success of propensity score methods in achieving balance of
baseline characteristics by direct comparison, than to assess residual confounding and
appropriateness of model specification in regression modeling. Thirdly, propensity score
methods separate the balancing of treatment groups with respect to potential confounders, from
the analysis of treatment effect on outcome. Since these steps are combined in regression
modeling, a concern has been raised that adjustment of the regression model may be continued
in an effort to further address confounding, until a desired or expected treatment effect on
outcome is seen [102].

22
A principal limitation of all propensity score techniques is that they are unable to address
confounding by hidden or unmeasured characteristics.
2.2 Comparison of propensity score methods
There are four common methods by which propensity score can be used to reduce
confounding: matching on propensity score; stratifying by propensity score; covariate
adjustment using propensity score in a regression model; and inverse probability of treatment
weighting (IPTW) using the propensity score.
We employed propensity score matching methods. Observational and simulation studies have
shown that propensity score matching generally achieves a greater balance in baseline
characteristics than either stratification or covariate adjustment, and does at least as well as
IPTW [80, 104]. Propensity score matching and stratification may be less sensitive to
inaccuracies in the model estimating the propensity score [105]. Covariate adjustment using
the propensity score may be a less reliable method, as the analysis depends both on accurate
estimation of the propensity score, and on correctly specifying the relationship between
propensity score and the outcome [102].
In exchange for improved balance in baseline characteristics, propensity score matching
sacrifices sample size, with treated and untreated patients who are markedly dissimilar being
excluded from analysis. In our study, the primary matched analysis included only 58% (31/53)
of beta-blocker users and 3% (31/986) of non-beta-blocker users. Stratification on the
propensity score may similarly exclude a large proportion of the cohort whose characteristics
are dissimilar. IPTW methods allow for inclusion of all patients in the analysis. However, the
weights may be inaccurate for patients with a very low estimated probability of being treated,
as was the case for a large proportion of non-beta-blocker users in our cohort [102].
Matching on a caliper width of 0.2 times the standard deviation of the logit of the propensity
score has been shown to optimize the reduction in bias in the estimate of treatment effect [106].
In our study, increasing the caliper width did not improve the balance of baseline
characteristics in the matched sample, nor did it significantly increase the number of successful
matches.

23
2.3 Propensity score estimation
There is no consensus on which variables to include in the propensity score model. It has been
suggested that the best propensity score model would include only variables that are true
confounders or are associated with the outcome. Including variables associated solely with
treatment assignment has been shown to increase the variance without improving the accuracy
of the estimate of effect [107, 108]. Moreover, models including such variables have been
shown to result in fewer matched pairs than those including only true or potential confounders
[109]. However, it is often difficult in practice to determine which variables are not associated
with outcome. In our study, after deriving our primary propensity score model, we repeated
our iterative propensity score building using a restricted set of variables in order to create a
second propensity score model. While the latter model increased the number of matched pairs
from 31 to 35, there were greater imbalances between treatment groups in important
cardiovascular comorbidities and medication use.
The inclusion of an era term in the propensity score model is controversial. We included date
of enrolment in the primary propensity score model, as a significant era effect was anticipated.
The accrual window spanned 13 years, during which time numerous advances were made in
the management of respiratory and cardiovascular diseases, including the introduction of new
medications. Significantly lower mortality rates have been reported in patients with COPD in
the 2000’s as compared to the 1990’s, both in small cohorts and at the population level [110-
112]. We found a similar era effect in our cohort, with significantly longer survival to
combined death or hospitalization seen in the latter 5 years of accrual. Pulmonary
rehabilitation indications also changed over time, with greater number of non-COPD disease
being considered grounds for enrolment. Thus, era was a true confounder and should be
included in the propensity score model.
3 Issues in study design
3.1 Setting
The study sample was enrolled from a single centre specializing in rehabilitation and complex
care. The cohort was well characterized and included patients with a range of severe chronic
lung diseases. At the same time, this unique setting may limit generalizability to the general

24
population of patients with chronic lung disease who are not participating in pulmonary
rehabilitation. The study included only patients older than 65 years and may not be
generalizable to younger patients.
3.2 Baseline characteristics
Diagnoses of lung disease and comorbidities were based on primary chart abstraction, which
increases their validity. Pulmonary diagnoses were independently assessed by a second
abstractor in a random sample of patients, and the level of agreement was very strong. It is the
standard practice as part of pulmonary rehabilitation assessment to request supporting
documentation from the referring physicians when a patient has a potentially important
comorbidity. Most patients referred to WPHC have primary care and specialist follow-up at
another centre, and we did not have access to the complete medical records held elsewhere.
Beta-blocker users are likely to have had cardiovascular comorbidities of greater severity than
non-users and may therefore be less susceptible to misclassification.
Patients in the cohort were generally well-characterized. In addition to pulmonary function
tests, important data on exercise testing, symptoms and gas exchange were also obtained.
There was incomplete data available for certain potentially important variables. In building the
propensity score model, we used multiple imputation methods for variables missing a small
proportion of values. The imputed values were used only to permit propensity score
estimation, and only measured values were used in assessing balance achieved. For certain
variables like the subscales of the Chronic Respiratory Questionnaire, a very large proportion
of values was missing and the variables were therefore not included in the analysis.
Data on hospitalizations and vital status were obtained from provincial administrative health
records which provide comprehensive coverage of all residents of Ontario, and therefore
improves the completeness of follow-up for outcomes.
Use of beta-blockers and other medications was determined from prescription records in the
ODB database. This approach has an advantage over chart review, since patients often forget
to report medications they have used in the past year. However, the ODB records can only
verify that a medication was purchased, not taken. Moreover, our methodology classified

25
patients as medication users or non-users at baseline only. We did not assess continuity of
medication use through the follow-up period. Finally, we were unable to assess whether
patients had stopped using beta-blockers due to side effects.
We did not include prior use of oral corticosteroids in our analysis. They are frequently used
in intermittent courses of varying duration for acute exacerbations of lung disease, and it would
therefore be difficult to distinguish acute from chronic use. Severe exacerbations would likely
result in visit to ER or in hospitalization, both of which were captured in our data. While mild
exacerbations may be treated as an outpatient with oral corticosteroids alone, these are less
likely to act as a significant confounder to the association between beta-blockers and
hospitalization or death.
3.3 Sample size
Our study suffered a lack of power due to a smaller-than-expected number of beta-blocker
users. Based on our recent clinical experience, the prevalence of beta-blocker use was
estimated at 10-20%. 13% of patients in the subgroup enrolled from 2004-2008 were indeed
beta-blocker users; however, among the larger group enrolled between 1996-2003, the
prevalence of beta-blocker use was less than 2%. This is unlikely to reflect a selection bias in
the pulmonary rehabilitation program. There was no formal change in the enrollment criteria
for pulmonary rehabilitation at West Park Healthcare Centre in the corresponding time frame.
The same two academic respirologists were responsible for patient assessment and clearance
for the rehabilitation program during these 13 years. Medication use has not been a deciding
factor in enrolment. Practice patterns in pulmonary rehabilitation have changed over these 13
years. A greater proportion of patients in the recent era had a primary diagnosis other than
COPD (26% vs 16%), in keeping with new literature supporting the benefits of pulmonary
rehabilitation to patients with non-COPD lung diseases [58, 59]. As the concerns about beta-
blockers have centred on obstructive lung diseases, these patients may have been more likely to
receive a prescription for beta-blockers. There has also been a trend to increased complexity of
the cases referred to pulmonary rehabilitation, as reflected by the greater burden of
comorbidities among patients in the recent era. These patients may also have been more likely
to receive a beta-blockers prescription. We cannot fully explain the low prevalence of beta-
blocker use in the early era.

26
The sample of beta-blocker users was too small to explore interactions between beta-blockers
and other cardiovascular medications such as angiotensin antagonists, or inhaled
bronchodilators.
4 Future directions
All observational studies of beta-blocker use in chronic lung disease are vulnerable to
confounding by indication and by disease severity. Our study adds to the existing literature in
having an extensive set of respiratory parameters to better characterize the nature and severity
of patients’ lung disease. We incorporated an analysis designed to account for differences in a
large number of characteristics; nonetheless, residual confounding persisted. The effects of
beta-blockers in patients with chronic lung disease has still not been resolved. A prospective
randomized controlled trial is therefore needed to provide a robust and reliable answer to this
important clinical question. Such design would enable an assessment of effect modification by
type of lung disease, especially COPD versus non-obstructive diseases, and by disease severity.
27
Chapter 5 : Conclusion
After matching on the propensity score, we failed to demonstrate a significant difference in
survival to death or hospitalization between beta-blocker users and non-users, among elderly
patients with chronic lung disease enrolled in pulmonary rehabilitation. In the subgroup of
patients with at least moderate obstructive disease, we similarly failed to detect a significant
difference in the hazard of death or hospitalization in beta-blocker users. Beta-blockers should
not be withheld from elderly patients with chronic lung disease, who would otherwise have an
indication for this class of medication.

28
References
1. Gan, W.Q., et al., Association between chronic obstructive pulmonary disease and systemic
inflammation: a systematic review and a meta-analysis. Thorax, 2004. 59(7): p. 574-580.
2. Au, D.H., et al., The risk of myocardial infarction associated with inhaled beta-adrenoceptor
agonists. Am J Respir Crit Care Med, 2000. 161(3 Pt 1): p. 827-830.
3. Dransfield, M.T., et al., Use of beta blockers and the risk of death in hospitalised patients with
acute exacerbations of COPD. Thorax, 2008. 63(4): p. 301-305.
4. Antonelli Incalzi, R., et al., Co-morbidity contributes to predict mortality of patients with
chronic obstructive pulmonary disease. Eur Respir J, 1997. 10(12): p. 2794-2800.
5. Izbicki, G., et al., The prevalence of coronary artery disease in end-stage pulmonary disease: is
pulmonary fibrosis a risk factor? Respir Med, 2009. 103(9): p. 1346-9.
6. Kizer, J.R., et al., Association between pulmonary fibrosis and coronary artery disease.
Archives of Internal Medicine, 2004. 164(5): p. 551-6.
7. Nathan, S.D., et al., Prevalence and impact of coronary artery disease in idiopathic pulmonary
fibrosis. Respir Med, 2010. 104(7): p. 1035-41.
8. Sirak, T.E., S. Jelic, and T.H. Le Jemtel, Therapeutic update: non-selective beta- and alpha-
adrenergic blockade in patients with coexistent chronic obstructive pulmonary disease and
chronic heart failure. J Am Coll Cardiol, 2004. 44(3): p. 497-502.
9. Curkendall, S.M., et al., Cardiovascular disease in patients with chronic obstructive pulmonary
disease, Saskatchewan Canada: cardiovascular disease in COPD patients. Ann Epidemiol,
2006. 16(1): p. 63-70.
10. Curkendall, S.M., et al., Chronic obstructive pulmonary disease severity and cardiovascular
outcomes. Eur J Epidemiol, 2006. 21(11): p. 803-813.
11. Berger, J.S., et al., Effect of chronic obstructive pulmonary disease on survival of patients with
coronary heart disease having percutaneous coronary intervention. Am J Cardiol, 2004. 94(5):
p. 649-651.
12. Ebi-Kryston, K.L., et al., Breathlessness, chronic bronchitis and reduced pulmonary function
as predictors of cardiovascular disease mortality among men in England, Scotland and the
United States. Int J Epidemiol, 1989. 18(1): p. 84-88.
13. Sin, D.D., L. Wu, and S.F. Man, The relationship between reduced lung function and
cardiovascular mortality: a population-based study and a systematic review of the literature.
Chest, 2005. 127(6): p. 1952-1959.
14. Sorlie, P.D., W.B. Kannel, and G. O'Connor, Mortality associated with respiratory function
and symptoms in advanced age. The Framingham Study. Am Rev Respir Dis, 1989. 140(2): p.
379-384.

29
15. Persson, C., et al., Peak expiratory flow and risk of cardiovascular disease and death. A 12-
year follow-up of participants in the population study of women in Gothenburg, Sweden. Am J
Epidemiol, 1986. 124(6): p. 942-948.
16. Sin, D.D., et al., Mortality in COPD: Role of comorbidities. Eur Respir J, 2006. 28(6): p. 1245-
1257.
17. Coultas, D.B. and M.P. Hughes, Accuracy of mortality data for interstitial lung diseases in New
Mexico, USA. Thorax, 1996. 51(7): p. 717-20.
18. Olson, A.L., et al., Mortality from pulmonary fibrosis increased in the United States from 1992
to 2003. Am J Respir Crit Care Med, 2007. 176(3): p. 277-84.
19. Mannino, D.M., R.A. Etzel, and R.G. Parrish, Pulmonary fibrosis deaths in the United States,
1979-1991. An analysis of multiple-cause mortality data. Am J Respir Crit Care Med, 1996.
153(5): p. 1548-52.
20. Anderson, J.L., et al., ACC/AHA 2007 guidelines for the management of patients with unstable
angina/non-ST-elevation myocardial infarction. J Am Coll Cardiol, 2007. 50(7): p. e1-e157.
21. Antman, E.M., et al., 2007 Focused Update of the ACC/AHA 2004 Guidelines for the
Management of Patients With ST-Elevation Myocardial Infarction. Circulation, 2008. 117(2):
p. 296-329.
22. Fox, K., et al., Guidelines on the management of stable angina pectoris: executive summary:
the Task Force on the Management of Stable Angina Pectoris of the European Society of
Cardiology. Eur Heart J, 2006. 27(11): p. 1341-1381.
23. Gibbons, R.J., et al., ACC/AHA 2002 guideline update for the management of patients with
chronic stable angina--summary article. J Am Coll Cardiol, 2003. 41(1): p. 159-168.
24. Hunt, S.A., et al., ACC/AHA 2005 Guideline Update for the Diagnosis and Management of
Chronic Heart Failure in the Adult. Circulation, 2005. 112(12): p. e154-235.
25. Chobanian, A.V., et al., The Seventh Report of the Joint National Committee on Prevention,
Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA, 2003.
289(19): p. 2560-2572.
26. Blomstrom-Lundqvist, C., et al., ACC/AHA/ESC guidelines for the management of patients
with supraventricular arrhythmias. J Am Coll Cardiol, 2003. 42(8): p. 1493-1531.
27. Zipes, D.P., et al., ACC/AHA/ESC 2006 guidelines for management of patients with ventricular
arrhythmias and the prevention of sudden cardiac death. J Am Coll Cardiol, 2006. 48(5): p.
e247-346.
28. Fuster, V., et al., ACC/AHA/ESC 2006 Guidelines for the Management of Patients with Atrial
Fibrillation. Circulation, 2006. 114(7): p. e257-354.
29. Fleisher, L.A., et al., ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation
and care for noncardiac surgery. J Am Coll Cardiol, 2007. 50(17): p. e159-241.

30
30. POISE Study Group, et al., Effects of extended-release metoprolol succinate in patients
undergoing non-cardiac surgery (POISE trial): a randomised controlled trial. Lancet, 2008.
371(9627): p. 1839-1847.
31. van der Woude, H.J., et al., Detrimental effects of beta-blockers in COPD: a concern for
nonselective beta-blockers. Chest, 2005. 127(3): p. 818-824.
32. Butland, R.J., J.A. Pang, and D.M. Geddes, Effect of beta-adrenergic blockade on
hyperventilation and exercise tolerance in emphysema. J Appl Physiol, 1983. 54(5): p. 1368-
1373.
33. Committees, C.-I.I.a., The Cardiac Insufficiency Bisoprolol Study II (CIBIS-II): a randomised
trial. Lancet, 1999. 353(9146): p. 9-13.
34. Poole-Wilson, P.A., et al., Comparison of carvedilol and metoprolol on clinical outcomes in
patients with chronic heart failure in the Carvedilol Or Metoprolol European Trial (COMET):
randomised controlled trial. Lancet, 2003. 362(9377): p. 7-13.
35. Savonitto, S., et al., Combination therapy with metoprolol and nifedipine versus monotherapy
in patients with stable angina pectoris. Results of the International Multicenter Angina
Exercise (IMAGE) Study. J Am Coll Cardiol, 1996. 27(2): p. 311-316.
36. Chadda, K., et al., Effect of propranolol after acute myocardial infarction in patients with
congestive heart failure. Circulation, 1986. 73(3): p. 503-510.
37. Metoprolol in acute myocardial infarction. Patients and methods. The MIAMI Trial Research
Group. The American journal of cardiology, 1985. 56(14): p. 3G-9G.
38. The sixth report of the Joint National Committee on prevention, detection, evaluation, and
treatment of high blood pressure. Arch Intern Med, 1997. 157(21): p. 2413-2446.
39. O'Malley, K., J.P. Cox, and E. O'Brien, Choice of drug treatment for elderly hypertensive
patients. Am J Med, 1991. 90(3A): p. 27S-33S.
40. Fallen, E.L., et al., Report of the Canadian Cardiovascular Society's consensus conference on
the Management of the Postmyocardial Infarction Patient. CMAJ, 1991. 144(8): p. 1015-1025.
41. Wellstein, A., et al., Reduction of exercise tachycardia in man after propranolol, atenolol and
bisoprolol in comparison to beta-adrenoceptor occupancy. Eur Heart J, 1987. 8 Suppl M: p. 3-
8.
42. Salpeter, S., T. Ormiston, and E. Salpeter, Cardioselective beta-blockers for chronic obstructive
pulmonary disease.[see comment][update of Cochrane Database Syst Rev.
2002;(2):CD003566; PMID: 12076486]. Cochrane Database Syst Rev, 2005(4).
43. Salpeter, S.R., T.M. Ormiston, and E.E. Salpeter, Cardioselective beta-blockers in patients with
reactive airway disease: a meta-analysis. Ann Intern Med, 2002. 137(9): p. 715-725.
44. Salpeter, S.R., et al., Cardioselective beta-blockers for chronic obstructive pulmonary disease:
a meta-analysis. Respir Med, 2003. 97(10): p. 1094-1101.

31
45. Mainguy, V., et al., Effect of bisoprolol on respiratory function and exercise capacity in
chronic obstructive pulmonary disease. The American journal of cardiology, 2012. 110(2): p.
258-63.
46. Chen, J., et al., Effectiveness of beta-blocker therapy after acute myocardial infarction in
elderly patients with chronic obstructive pulmonary disease or asthma. J Am Coll Cardiol,
2001. 37(7): p. 1950-1956.
47. Gottlieb, S.S., R.J. McCarter, and R.A. Vogel, Effect of beta-blockade on mortality among
high-risk and low-risk patients after myocardial infarction. N Engl J Med, 1998. 339(8): p.
489-497.
48. Au, D.H., et al., Beta-blockers as single-agent therapy for hypertension and the risk of
mortality among patients with chronic obstructive pulmonary disease. Am J Med, 2004.
117(12): p. 925-931.
49. Au, D.H., et al., Association between inhaled beta-agonists and the risk of unstable angina and
myocardial infarction. Chest, 2002. 121(3): p. 846-851.
50. Kotlyar, E., et al., Tolerability of carvedilol in patients with heart failure and concomitant
chronic obstructive pulmonary disease or asthma. J Heart Lung Transplant, 2002. 21(12): p.
1290-1295.
51. Heller, D.A., F.M. Ahern, and M. Kozak, Changes in rates of beta-blocker use between 1994
and 1997 among elderly survivors of acute myocardial infarction. Am Heart J, 2000. 140(4): p.
663-671.
52. Chafin, C.C., et al., Beta-blockers after myocardial infarction: do benefits ever outweigh risks
in asthma? Cardiology, 1999. 92(2): p. 99-105.
53. Viskin, S. and H.V. Barron, Beta blockers prevent cardiac death following a myocardial
infarction: so why are so many infarct survivors discharged without beta blockers? Am J
Cardiol, 1996. 78(7): p. 821-822.
54. Egred, M., et al., Under-use of beta-blockers in patients with ischaemic heart disease and
concomitant chronic obstructive pulmonary disease. QJM, 2005. 98(7): p. 493-497.
55. Stefan, M.S., et al., The impact of COPD on management and outcomes of patients hospitalized
with acute myocardial infarction: a 10-year retrospective observational study. Chest, 2012.
141(6): p. 1441-8.
56. Ries, A.L., et al., Pulmonary Rehabilitation: Joint ACCP/AACVPR Evidence-Based Clinical
Practice Guidelines. Chest, 2007. 131(5 Suppl): p. 4S-42S.
57. Nici, L., et al., American Thoracic Society/European Respiratory Society statement on
pulmonary rehabilitation. Am J Respir Crit Care Med, 2006. 173(12): p. 1390-1413.
58. Holland, A.E., et al., Short term improvement in exercise capacity and symptoms following
exercise training in interstitial lung disease. Thorax, 2008. 63(6): p. 549-554.

32
59. Mereles, D., et al., Exercise and respiratory training improve exercise capacity and quality of
life in patients with severe chronic pulmonary hypertension. Circulation, 2006. 114(14): p.
1482-9.
60. Crisafulli, E., et al., Role of comorbidities in a cohort of patients with COPD undergoing
pulmonary rehabilitation. Thorax, 2008. 63(6): p. 487-492.
61. Gerardi, D.A., et al., Variables related to increased mortality following out-patient pulmonary
rehabilitation. Eur Respir J, 1996. 9(3): p. 431-435.
62. Brooks, D., et al., Characterization of pulmonary rehabilitation programs in Canada in 2005.
Can Respir J, 2007. 14(2): p. 87-92.
63. Arnold, E., A. Bruton, and C. Ellis-Hill, Adherence to pulmonary rehabilitation: A qualitative
study. Respir Med, 2006. 100(10): p. 1716-1723.
64. Young, P., et al., Respiratory rehabilitation in chronic obstructive pulmonary disease:
predictors of nonadherence. Eur Respir J, 1999. 13(4): p. 855-859.
65. Garrod, R., et al., Predictors of success and failure in pulmonary rehabilitation. Eur Respir J,
2006. 27(4): p. 788-794.
66. Brooks, D., et al., The effect of postrehabilitation programmes among individuals with chronic
obstructive pulmonary disease. Eur Respir J, 2002. 20(1): p. 20-29.
67. O'Donnell, D.E., et al., State of the Art Compendium: Canadian Thoracic Society
recommendations for the management of chronic obstructive pulmonary disease. Can Respir J,
2004. 11 Suppl B: p. 7B-59B.
68. Executive Summary: data quality documentation, Discharge Abstract Database, 2006–2007.
2007 [cited Accessed at http://www.cihi.ca.
69. Levy, A.R., et al., Coding accuracy of administrative drug claims in the Ontario Drug Benefit
database. Can J Clin Pharmacol, 2003. 10(2): p. 67-71.
70. Charlson, M.E., et al., A new method of classifying prognostic comorbidity in longitudinal
studies: development and validation. J Chronic Dis, 1987. 40(5): p. 373-383.
71. Cohen, J., A coefficient of agreement for nominal scales. Educ Psychol Meas, 1960. 20(1): p.
37-46.
72. McGinn, T., et al., Tips for learners of evidence-based medicine: 3. Measures of observer
variability (kappa statistic). CMAJ : Canadian Medical Association journal = journal de
l'Association medicale canadienne, 2004. 171(11): p. 1369-73.
73. Peduzzi, P., et al., A simulation study of the number of events per variable in logistic regression
analysis. J Clin Epidemiol, 1996. 49(12): p. 1373-1379.
74. Vittinghoff, E. and C.E. McCulloch, Relaxing the rule of ten events per variable in logistic and
Cox regression. Am J Epidemiol, 2007. 165(6): p. 710-718.

33
75. Cepeda, M.S., et al., Comparison of logistic regression versus propensity score when the
number of events is low and there are multiple confounders. Am J Epidemiol, 2003. 158(3): p.
280-287.
76. D'Agostino, R.B., Jr, Propensity score methods for bias reduction in the comparison of a
treatment to a non-randomized control group. Stat Med, 1998. 17(19): p. 2265-2281.
77. Rosenbaum, P.R. and D.R. Rubin, The central role of the propensity score in observational
studies for causal effects. Biometrika, 1983. 70: p. 41-55.
78. Austin, P.C., et al., The use of the propensity score for estimating treatment effects:
administrative versus clinical data. Stat Med, 2005. 24(10): p. 1563-1578.
79. Rosenbaum, P.R. and D.R. Rubin, Reducing bias in observational studies using
subclassification on the propensity score. J Am Stat Assoc, 1984. 79(387): p. 516-524.
80. Austin, P.C. and M.M. Mamdani, A comparison of propensity score methods: a case-study
estimating the effectiveness of post-AMI statin use. Stat Med, 2006. 25(12): p. 2084-2106.
81. Cochran, W.G., The effectiveness of adjustment by subclassification in removing bias in
observational studies. Biometrics, 1968. 24(2): p. 295-313.
82. Rosenbaum, P.R. and D.B. Rubin, Constructing a control group using multivariate matched
sampling methods that incorporate the propensity score. Am Stat, 1985. 39(1): p. 33-38.
83. Normand, S.T., et al., Validating recommendations for coronary angiography following acute
myocardial infarction in the elderly: a matched analysis using propensity scores. J Clin
Epidemiol, 2001. 54(4): p. 387-398.
84. Griffiths, T.L., et al., Results at 1 year of outpatient multidisciplinary pulmonary rehabilitation:
a randomised controlled trial. Lancet, 2000. 355(9201): p. 362-368.
85. Man, W.D., et al., Community pulmonary rehabilitation after hospitalisation for acute
exacerbations of chronic obstructive pulmonary disease: randomised controlled study. BMJ,
2004. 329(7476): p. 1209.
86. Bowen, J.B., et al., Functional status and survival following pulmonary rehabilitation. Chest,
2000. 118(3): p. 697-703.
87. Foody, J.M., M.H. Farrell, and H.M. Krumholz, beta-Blocker therapy in heart failure: scientific
review. JAMA, 2002. 287(7): p. 883-889.
88. Tandon, P., et al., The use of beta-blockers in a tertiary care heart failure clinic: dosing,
tolerance, and outcomes. Arch Intern Med, 2004. 164(7): p. 769-774.
89. Sinclair, D.J., Comparison of effects of propranolol and metoprolol on airways obstruction in
chronic bronchitis. British medical journal, 1979. 1(6157): p. 168.
90. Skinner, C., J. Gaddie, and K.N. Palmer, Comparison of effects of metoprolol and propranolol
on asthmatic airway obstruction. British medical journal, 1976. 1(6008): p. 504.

34
91. Gayrard, P., et al., Beta-adrenergic function in airways of healthy and asthmatic subjects.
Thorax, 1975. 30(6): p. 657-62.
92. Jabbour, A., et al., Differences between beta-blockers in patients with chronic heart failure and
chronic obstructive pulmonary disease: a randomized crossover trial. Journal of the American
College of Cardiology, 2010. 55(17): p. 1780-7.
93. Raghu, G., et al., An official ATS/ERS/JRS/ALAT statement: idiopathic pulmonary fibrosis:
evidence-based guidelines for diagnosis and management. Am J Resp Crit Care Med, 2011.
183(6): p. 788-824.
94. van Gestel, Y.R., et al., Impact of cardioselective beta-blockers on mortality in patients with
chronic obstructive pulmonary disease and atherosclerosis. Am J Resp Crit Care Med, 2008.
178(7): p. 695-700.
95. Hawkins, N.M., et al., Bisoprolol in patients with heart failure and moderate to severe chronic
obstructive pulmonary disease: a randomized controlled trial. European journal of heart
failure, 2009. 11(7): p. 684-90.
96. Mascarenhas, J., et al., Chronic obstructive pulmonary disease in heart failure. Prevalence,
therapeutic and prognostic implications. Am Heart J, 2008. 155(3): p. 521-525.
97. Stefan, M.S., et al., Association between beta-blocker therapy and outcomes in patients
hospitalised with acute exacerbations of chronic obstructive lung disease with underlying
ischaemic heart disease, heart failure or hypertension. Thorax, 2012. 67(11): p. 977-84.
98. Short, P.M., et al., Effect of beta blockers in treatment of chronic obstructive pulmonary
disease: a retrospective cohort study. BMJ, 2011. 342: p. d2549.
99. Ekstrom, M.P., A.B. Hermansson, and K.E. Strom, Effects of cardiovascular drugs on mortality
in severe chronic obstructive pulmonary disease. Am J Resp Crit Care Med, 2013. 187(7): p.
715-20.
100. Concato, J., et al., Importance of events per independent variable in proportional hazards
analysis. I. Background, goals, and general strategy. Journal of clinical epidemiology, 1995.
48(12): p. 1495-501.
101. Peduzzi, P., et al., Importance of events per independent variable in proportional hazards
regression analysis. II. Accuracy and precision of regression estimates. Journal of clinical
epidemiology, 1995. 48(12): p. 1503-10.
102. Austin, P.C., An Introduction to Propensity Score Methods for Reducing the Effects of
Confounding in Observational Studies. Multivariate behavioral research, 2011. 46(3): p. 399-
424.
103. Pirracchio, R., M. Resche-Rigon, and S. Chevret, Evaluation of the propensity score methods
for estimating marginal odds ratios in case of small sample size. BMC medical research
methodology, 2012. 12: p. 70.

35
104. Austin, P.C., Type I error rates, coverage of confidence intervals, and variance estimation in
propensity-score matched analyses. The international journal of biostatistics, 2009. 5(1): p.
Article 13.
105. Rubin, D.B., On principles for modeling propensity scores in medical research.
Pharmacoepidemiology and drug safety, 2004. 13(12): p. 855-7.
106. Austin, P.C., Optimal caliper widths for propensity-score matching when estimating differences
in means and differences in proportions in observational studies. Pharmaceutical statistics,
2011. 10(2): p. 150-61.
107. Brookhart, M.A., et al., Variable selection for propensity score models. American journal of
epidemiology, 2006. 163(12): p. 1149-56.
108. Rubin, D.B. and N. Thomas, Matching using estimated propensity scores: relating theory to
practice. Biometrics, 1996. 52(1): p. 249-64.
109. Austin, P.C., P. Grootendorst, and G.M. Anderson, A comparison of the ability of different
propensity score models to balance measured variables between treated and untreated
subjects: a Monte Carlo study. Statistics in medicine, 2007. 26(4): p. 734-53.
110. Kaboli, P.J., et al., Associations between reduced hospital length of stay and 30-day
readmission rate and mortality: 14-year experience in 129 Veterans Affairs hospitals. Annals
of internal medicine, 2012. 157(12): p. 837-45.
111. Gershon, A.S., et al., Trends in chronic obstructive pulmonary disease prevalence, incidence,
and mortality in ontario, Canada, 1996 to 2007: a population-based study. Archives of internal
medicine, 2010. 170(6): p. 560-5.
112. Almagro, P., et al., Recent improvement in long-term survival after a COPD hospitalisation.
Thorax, 2010. 65(4): p. 298-302.

36
Tables
Table 1. Definition of medication classes.
Medication class Definition
Beta-blocker • Drug subclass name = 'BETA-BLOCKERS' or 'BETA-BLOCKERS
COMBINATION'
Angiotensin antagonist • Drug subclass name = 'ACE INHIBITORS’ or 'ACE INHIBITORS
COMBINATION', or
• Drug subclass name = 'ANGIOTENSIN II ANTAGONIST' or
'ANGIOTENSIN II COMBINATION'
Alpha-adrenergic
blocker • Drug subclass name = 'ALPHA ADRENERGIC BLOCKING
AGENTS'
Calcium channel blocker • Drug subclass name = 'CALCIUM BLOCKERS' or 'CALCIUM
BLOCKERS ANTILIPEMIC COMBINATIONS', or
• Drug name = 'FELODIPINE & METOPROLOL' or 'FELODIPINE &
RAMIPRIL' or 'VERAPAMIL HCL & TRANDOLAPRIL'
Digoxin • Drug subclass name = 'DIGITALIS PREPARATIONS'
Diuretic • Drug subclass name = 'DIURETICS' or 'DIURETICS (POTASSIUM-
SPARING)', or
• Drug name contains 'HYDROCHLOROTHIAZIDE' or
'CHLORTHALIDONE' or 'FUROSEMIDE', or
• Drug name = 'ACETAZOLAMIDE'
Statin • Drug subclass name = 'ANTILIPEMIC: STATINS' or 'CALCIUM
BLOCKERS ANTILIPEMIC COMBINATIONS'
Nitrate • Drug name = 'NITROGLYCERIN' or 'ISOSORBIDE DINITRATE' or
'ISOSORBIDE-5-MONONITRATE'
Antiplatelet agent • Drug name = 'ASA' or 'TICLOPIDINE HCL' or 'ASA &
DIPYRIDAMOLE' or 'CLOPIDOGREL BISULFATE'
Vasodilator • Drug name = 'DIAZOXIDE' or 'HYDRALAZINE HCL' or
'MINOXIDIL' or 'PHENOXYBENZAMINE'
Optic beta-blocker
preparation • Drug subclass name = 'BETA BLOCKING AGENTS'
Inhaled corticosteroid • Drug subclass name = 'BRONCHODILATOR AND ANTI-
INFLAMMATORY COMBINATION', or
• Drug name = 'FORMOTEROL FUMARATE DIHYDRATE &
MOMETASONE FUROATE', or
• Drug subclass name = 'INHALED CORTICOSTEROIDS' and route of
administration is not nasal
Inhaled long-acting beta-
agonist • Drug name contains 'FORMOTEROL' or 'SALMETEROL'

37
Inhaled long-acting
anticholenergic • Drug name = 'TIOTROPIUM BROMIDE MONOHYDRATE'
Inhaled short-acting
beta-agonist • Drug subclass name = 'ADRENERGIC AND ANTICHOLINERGIC
BRONCHODILATORS', or
• Drug subclass name = 'SELECTIVE BETA2-ADRENERGIC
AGONISTS', and drug name does not contain 'FORMOTEROL' or
'SALMETEROL'
Inhaled short-acting
anticholenergic • Drug subclass name = 'ADRENERGIC AND ANTICHOLINERGIC
BRONCHODILATORS', or
• Drug name = 'IPRATROPIUM BROMIDE', and drug subclass name =
'ANTI-CHOLINERGICS', and route of administration is not nasal
Leukotriene receptor
antagonist • Drug subclass name = 'LEUKOTRIENE RECEPTOR
ANTAGONISTS'
Methyxanthine • Drug name = 'AMINOPHYLLINE' or 'OXTRIPHYLLINE' or
'THEOPHYLLINE' or 'THEOPHYLLINE & POTASSIUM'
Drug names and drug subclass names are presented as listed in the Ontario Drug Benefits database.

38
Table 2. Comorbidities.
Comorbidity Criteria
Coronary artery disease • Coronary artery stenosis demonstrated on angiography or on
noninvasive testing; or
• Prior coronary revascularization procedure; or
• Clinical history of stable exertional angina.
Congestive heart failure • Left ventricular ejection fraction < 50%; or
• Clinical history of pulmonary edema from left ventricular failure.
Arrhythmia • Atrial or ventricular tachyarrhythmia.
Hypertension • Clinical history of hypertension.
Diabetes • Clinical history of diabetes mellitus with or without microvascular
complications.
Cerebrovascular disease • Clinical history of transient ischaemic attack; or
• History of or imaging demonstrating ischaemic or haemorrhagic stroke.
Chronic renal failure • Estimated creatinine clearance less than 50 mL/min; or
• Need for renal replacement therapy.
Peripheral vascular
disease • Peripheral arterial stenosis demonstrated on angiography or noninvasive
testing; or
• Revascularization procedure; or
• Clinical history of vascular claudication; or
• Abdominal aortic aneurysm with diameter greater than 5 cm, or history
of surgical repair.

39
Table 3. Cardiorespiratory diagnostic codes.
Diagnosis ICD-9 code ICD-10 code
Cardiac
Hypertension and hypertensive heart disease 401-402 I10-I11
Ischaemic heart disease 410-414 I20-I25
Cardiomyopathy and heart failure 425, 428 I42-I43, I50
Conduction disorders and dysrhythmias 426-427 I44-I49
Other cardiac disease 429 I51
Respiratory
Respiratory tuberculosis 010-012 A15-A16
Non-tuberculous mycobacterial infection 031 A31
Sarcoidosis 135 D86
Late effects of tuberculosis or poliomyelitis 137-138 B90-B91
Sleep disordered breathing 327 G47
Pulmonary vascular disease 416-417 I27-I28
Acute lower respiratory tract infection 466, 480-488 J09-J22
Chronic obstructive pulmonary disease 491-492, 496 J41-J44
Other lower respiratory tract disease 490-519 J40-J99
Legend: ICD, International Classification of Disease.

40
Table 4. Standardised differences.
For continuous variables For dichotomous variables
( )2
unexposed
2
exposed21
unexposedexposed
ss
xxd
+
−=
( )unexposedunexposedexposedexposed21
unexposedexposed
QPQP
PPd
+
−=
Legend: d, standardised difference; x , mean; s2, variance; P, proportion with characteristic; Q,
proportion without characteristic.

41
Table 5. Missing data.
Variable Beta-blocker users
(N=53)
Non-beta-blocker users
(N=986)
Lung disease
Smoking status 0 3 (0.3%)
Quantity smoked 0 24 (2.4%)
Pulmonary function
FEV1 0 0
FEV1/FVC 0 2 (0.2%)
TLC 5 (9.4%) 209 (21.2%)
IC 3 (5.7%) 206 (20.9%)
RV 5 (9.4%) 211 (21.4%)
DLCO 11 (20.8%) 203 (20.6%)
MIP 19 (35.8%) 531 (53.9%)
Exercise / gas exchange
6MWD 2 (3.8%) 54 (5.5%)
Resting oxygen saturation 0 3 (0.3%)
PaO2 0 25 (2.5%)
PaCO2 0 25 (2.5%)
Exertional desaturation 0 10 (1.0%)
Endurance walk time 8 (15.1%) 122 (12.4%)
MRC dyspnea score 11 (20.8%) 165 (16.7%)
CRQ-dyspnea score 37 (69.8%) 533 (54.1%)
CRQ-emotional score 37 (69.8%) 531 (53.9%)
CRQ-mastery score 37 (69.8%) 531 (53.9%)
CRQ-fatigue score 37 (69.8%) 532 (54.0%)
Legend: FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; TLC,
total lung capacity; IC, inspiratory capacity; RV, residual volume; DLCO, diffusing
capacity for carbon monoxide; MIP, maximal inspiratory capacity; 6MWD, 6-minute
walk distance; PaO2, partial pressure of oxygen; PaCO2, partial pressure of carbon
dioxide; MRC, Medical Research Council; CRQ, Chronic Respiratory Questionnaire.

42
Table 6. Beta-blocker use by year of entry to study.
Year Patients enrolled Beta-blocker users enrolled
1996 111 0
1997 95 0
1998 109 3 (2.8%)
1999 93 2 (2.2%)
2000 74 0
2001 89 1 (1.1%)
2002 93 3 (3.2%)
2003 69 3 (4.3%)
2004 58 4 (6.9%)
2005 65 8 (12.3%)
2006 52 7 (13.5%)
2007 71 14 (19.7%)
2008 60 8 (13.3%)
Total 1039 53 (5.4%)

43
Table 7. Baseline characteristics, entire cohort
Variable Beta-blocker
users
(N=53)
Non-beta-blocker
users
(N=986)
Standardised
Difference of
the Mean
P-
Value
Demographic / Anthropomorphic
Age, yr 74.96 (5.23) 73.25 (4.99) 0.34 0.015
Male 27 (50.9%) 493 (50.0%) 0.02 0.894
Body Mass Index, kg/m2 26.41 (6.53) 24.93 (5.99) 0.25 0.08
Married 22 (41.5%) 497 (50.4%) 0.18 0.207
Income quintile 2.77 (1.44) 2.98 (1.47) 0.14 0.308
Index date (year of admission to
pulmonary rehabilitation)
2005 (2.8) 2001 (3.7) 1.11 <.001
Health care utilization
Hospitalisations in past 2 years 1.57 (2.01) 1.69 (2.06) 0.06 0.662
Cumulative length of stay in hospital
in past 2 years, days
17.21 (27.13) 18.03 (29.43) 0.03 0.843
Emergency Department visits in past
2 years
2.85 (4.87) 3.00 (3.79) 0.04 0.786
Lung disease
Primary lung diagnosis by type 0.53 <.001
COPD 29 (54.7%) 815 (82.7%)
Other obstructive lung disease 2 (3.8%) 48 (4.9%)
Interstitial lung disease 12 (22.6%) 49 (5.0%)
Neuromuscular disease 7 (13.2%) 27 (2.7%)
Pulmonary hypertension 1 (1.9%) 1 (0.1%)
Lung resection 1 (1.9%) 30 (3.0%)
Other 1 (1.9%) 16 (1.6%)
Primary lung diagnosis is COPD 29 (54.7%) 815 (82.7%) 0.72 <.001
Any diagnosis of COPD 32 (60.4%) 849 (86.1%) 0.72 <.001
Smoking status: 0.28 0.26
Never 8 (15.1%) 82 (8.3%)
Former 45 (84.9%) 881 (89.4%)
Current 0 20 (2.0%)
Quantity smoked, pack-years 41.87 (38.05) 45.91 (26.69) 0.15 0.295

44
Pulmonary function
FEV1, L 1.21 (0.48) 0.93 (0.43) 0.65 <.001
FEV1 % pred 48.66 (18.37) 36.64 (16.48) 0.73 <.001
FEV/FVC ratio, % 59.68 (21.04) 43.89 (17.33) 0.9 <.001
TLC % pred 90.71 (27.20) 111.33 (26.77) 0.77 <.001
IC % pred 56.76 (19.90) 58.35 (18.02) 0.09 0.549
DLCO % pred 38.93 (19.04) 37.36 (16.40) 0.09 0.55
Exercise / gas exchange
6MWD, m 234.94 (110.18) 292.42 (112.96) 0.51 <.001
Resting oxygen saturation, % 88.87 (7.40) 91.10 (5.48) 0.4 0.005
PaO2, mmHg 61.00 (15.83) 64.86 (12.67) 0.3 0.033
PaCO2, mmHg 42.62 (6.91) 44.63 (8.75) 0.23 0.101
Exertional desaturation 28 (52.8%) 498 (50.5%) 0.04 0.738
Endurance walk time, minutes 8.28 (6.84) 11.89 (9.87) 0.37 0.016
MRC dyspnea score: 0.7 <.001
1 (mild) 0 2 (0.2%)
2 0 39 (4.0%)
3 6 (11.3%) 223 (22.6%)
4 13 (24.5%) 385 (39.0%)
5 (severe) 23 (43.4%) 172 (17.4%)
CRQ-dyspnea score 2.74 (0.75) 3.14 (1.01) 0.4 0.113
CRQ-emotional score 4.54 (1.06) 4.27 (1.19) 0.23 0.359
CRQ-fatigue score 3.33 (1.39) 3.28 (1.24) 0.04 0.873
CRQ-mastery score 4.34 (1.30) 4.13 (1.29) 0.16 0.525
Comorbidities
Atrial fibrillation 17 (32.1%) 117 (11.9%) 0.61 <.001
Coronary artery disease 26 (49.1%) 195 (19.8%) 0.72 <.001
Congestive heart failure 8 (15.1%) 70 (7.1%) 0.3 0.031
Hypertension 35 (66.0%) 379 (38.4%) 0.57 <.001
Chronic renal failure 10 (18.9%) 23 (2.3%) 0.96 <.001
Cerebrovascular disease 11 (20.8%) 72 (7.3%) 0.5 <.001
Diabetes 14 (26.4%) 97 (9.8%) 0.54 <.001
Peripheral vascular disease 2 (3.8%) 63 (6.4%) 0.11 0.444
Charlson Comorbidity Index score 1.58 (1.18) 0.83 (1.17) 0.65 <.001

45
Medications
Number of discrete medications used
in previous year
16.66 (6.58) 13.38 (6.13) 0.53 <.001
Angiotensin antagonist 35 (66.0%) 298 (30.2%) 0.78 <.001
Calcium-channel blocker 27 (50.9%) 283 (28.7%) 0.49 <.001
Digoxin 9 (17.0%) 108 (11.0%) 0.19 0.176
Diuretic 38 (71.7%) 451 (45.7%) 0.52 <.001
Nitrate 19 (35.8%) 156 (15.8%) 0.54 <.001
Ophthalmic beta-blocker 3 (5.7%) 36 (3.7%) 0.11 0.453
Anti-platelet 23 (43.4%) 166 (16.8%) 0.7 <.001
Statin 28 (52.8%) 189 (19.2%) 0.84 <.001
Inhaled corticosteroid 32 (60.4%) 814 (82.6%) 0.57 <.001
Tiotropium 24 (45.3%) 212 (21.5%) 0.57 <.001
Long-acting inhaled beta-agonist 29 (54.7%) 459 (46.6%) 0.16 0.246
Short-acting inhaled anticholenergic 19 (35.8%) 731 (74.1%) 0.87 <.001
Short-acting inhaled beta-agonist 32 (60.4%) 863 (87.5%) 0.8 <.001
Methylxanthine 7 (13.2%) 397 (40.3%) 0.56 <.001
Data are presented as mean (standard deviation) or number (%), as appropriate.
Legend: COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second;
FVC, forced vital capacity; TLC, total lung capacity; IC, inspiratory capacity; DLCO, diffusing capacity
for carbon monoxide; 6MWD, 6-minute walk distance; PaO2, partial pressure of oxygen; PaCO2,
partial pressure of carbon dioxide; MRC, Medical Research Council; CRQ, Chronic Respiratory
Questionnaire.

46
Table 8. Baseline characteristics, matched sample, using primary propensity score model
Variable Beta-blocker users
(N=31)
Non-beta-blocker
users
(N=31)
Standardised
Difference of the
Mean
Demographic / Anthropomorphic
Age, yr 73.84 (4.99) 74.06 (5.25) 0.04
Male 17 (54.8%) 17 (54.8%) 0.00
Body Mass Index, kg/m2 24.52 (6.15) 25.06 (5.53) 0.09
Married 11 (35.5%) 14 (45.2%) 0.20
Income quintile 2.90 (1.42) 2.61 (1.38) 0.21
Index date (year of admission to
pulmonary rehabilitation)
2004 (3.1) 2004 (3.3) 0.01
Health care utilization
Hospitalisations in past 2 years 1.77 (2.43) 1.84 (2.49) 0.03
Cumulative length of stay in hospital in
past 2 years, days
15.45 (25.90) 24.13 (36.12) 0.28
Emergency Department visits in past 2
years
3.45 (6.19) 3.45 (4.59) 0.00
Lung disease
Primary lung diagnosis by type 0.08
COPD 22 (71.0%) 22 (71.0%)
Other obstructive lung disease 1 (3.2%) 2 (6.5%)
Interstitial lung disease 5 (16.1%) 3 (9.7%)
Neuromuscular disease 3 (9.7%) 2 (6.5%)
Pulmonary hypertension 0 1 (3.2%)
Lung resection 0 1 (3.2%)
Other 0 0
Primary lung diagnosis is COPD 22 (71.0%) 22 (71.0%) 0.00
Any diagnosis of COPD 23 (74.2%) 23 (74.2%) 0.00
Current or former smoker 28 (90.3%) 26 (83.9%) 0.19
Quantity smoked, pack-years 47.58 (41.03) 36.57 (22.98) 0.33
Pulmonary function
FEV1, % predicted 43.03 (16.27) 41.65 (15.69) 0.09
FEV1/FVC ratio, % 53.87 (21.08) 53.65 (21.32) 0.01
DLCO, % predicted 36.64 (15.90) 40.04 (17.37) 0.20
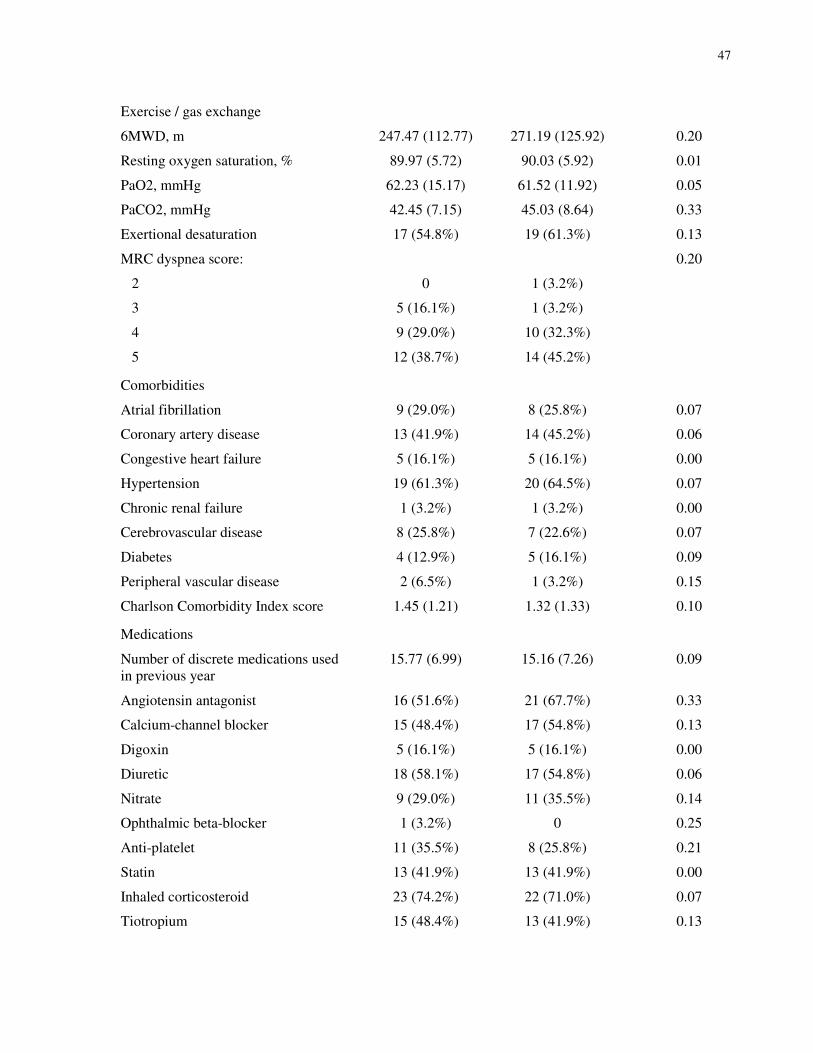
47
Exercise / gas exchange
6MWD, m 247.47 (112.77) 271.19 (125.92) 0.20
Resting oxygen saturation, % 89.97 (5.72) 90.03 (5.92) 0.01
PaO2, mmHg 62.23 (15.17) 61.52 (11.92) 0.05
PaCO2, mmHg 42.45 (7.15) 45.03 (8.64) 0.33
Exertional desaturation 17 (54.8%) 19 (61.3%) 0.13
MRC dyspnea score: 0.20
2 0 1 (3.2%)
3 5 (16.1%) 1 (3.2%)
4 9 (29.0%) 10 (32.3%)
5 12 (38.7%) 14 (45.2%)
Comorbidities
Atrial fibrillation 9 (29.0%) 8 (25.8%) 0.07
Coronary artery disease 13 (41.9%) 14 (45.2%) 0.06
Congestive heart failure 5 (16.1%) 5 (16.1%) 0.00
Hypertension 19 (61.3%) 20 (64.5%) 0.07
Chronic renal failure 1 (3.2%) 1 (3.2%) 0.00
Cerebrovascular disease 8 (25.8%) 7 (22.6%) 0.07
Diabetes 4 (12.9%) 5 (16.1%) 0.09
Peripheral vascular disease 2 (6.5%) 1 (3.2%) 0.15
Charlson Comorbidity Index score 1.45 (1.21) 1.32 (1.33) 0.10
Medications
Number of discrete medications used
in previous year
15.77 (6.99) 15.16 (7.26) 0.09
Angiotensin antagonist 16 (51.6%) 21 (67.7%) 0.33
Calcium-channel blocker 15 (48.4%) 17 (54.8%) 0.13
Digoxin 5 (16.1%) 5 (16.1%) 0.00
Diuretic 18 (58.1%) 17 (54.8%) 0.06
Nitrate 9 (29.0%) 11 (35.5%) 0.14
Ophthalmic beta-blocker 1 (3.2%) 0 0.25
Anti-platelet 11 (35.5%) 8 (25.8%) 0.21
Statin 13 (41.9%) 13 (41.9%) 0.00
Inhaled corticosteroid 23 (74.2%) 22 (71.0%) 0.07
Tiotropium 15 (48.4%) 13 (41.9%) 0.13

48
Long-acting inhaled beta-agonist 20 (64.5%) 20 (64.5%) 0.00
Short-acting inhaled anticholenergic 15 (48.4%) 17 (54.8%) 0.13
Short-acting inhaled beta-agonist 22 (71.0%) 22 (71.0%) 0.00
Methylxanthine 6 (19.4%) 7 (22.6%) 0.08
Data are presented as mean (standard deviation) or number (%), as appropriate.
Legend: COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second;
FVC, forced vital capacity; DLCO, diffusing capacity for carbon monoxide; 6MWD, 6-minute walk
distance; PaO2, partial pressure of oxygen; PaCO2, partial pressure of carbon dioxide; MRC, Medical
Research Council.

49
Table 9. Baseline characteristics, matched sample, using secondary propensity score model
Variable Beta-blocker users
(N=35)
Non-beta-blocker
users
(N=35)
Standardised
Difference of the
Mean
Demographic / Anthropomorphic
Age, yr 74.57 (4.94) 74.60 (4.65) 0.01
Male 18 (51.4%) 18 (51.4%) 0.00
Body Mass Index, kg/m2 26.35 (6.96) 26.17 (7.31) 0.03
Married 14 (40.0%) 17 (48.6%) 0.17
Income quintile 2.77 (1.46) 3.03 (1.36) 0.18
Index date (year of admission to
pulmonary rehabilitation)
2005 (3.0) 2003 (3.3) 0.36
Health care utilization
Hospitalisations in past 2 years 1.80 (2.37) 1.26 (1.48) 0.27
Cumulative length of stay in hospital
in past 2 years, days
17.60 (28.96) 20.51 (33.52) 0.09
Emergency Department visits in past 2
years
3.29 (5.85) 2.46 (3.28) 0.17
Lung disease
Primary lung diagnosis by type 0.14
COPD 22 (62.9%) 23 (65.7%)
Other obstructive lung disease 0 3 (8.6%)
Interstitial lung disease 6 (17.1%) 4 (11.4%)
Neuromuscular disease 6 (17.1%) 3 (8.6%)
Pulmonary hypertension 0 1 (2.9%)
Lung resection 0 1 (2.9%)
Other 1 (2.9%) 0
Primary lung diagnosis is COPD 22 (62.9%) 23 (65.7%) 0.06
Any diagnosis of COPD 24 (68.6%) 24 (68.6%) 0.00
Current or former smoker 32 (91.4%) 30 (85.7%) 0.08
Quantity smoked, pack-years 44.97 (39.76) 41.26 (29.69) 0.11
Pulmonary function
FEV1, % predicted 49.74 (18.89) 46.37 (17.18) 0.19
FEV1/FVC ratio, % 58.29 (21.26) 54.63 (19.88) 0.18
DLCO, % predicted 40.27 (19.39) 41.97 (18.32) 0.09

50
Exercise / gas exchange
6MWD, m 251.26 (106.78) 260.42 (88.54) 0.09
Resting oxygen saturation, % 90.43 (5.54) 90.57 (5.35) 0.03
PaO2, mmHg 63.91 (15.92) 62.26 (11.19) 0.12
PaCO2, mmHg 41.77 (6.87) 44.00 (7.80) 0.30
Exertional desaturation 17 (48.6%) 18 (51.4%) 0.06
MRC dyspnea score: 0.01
3 6 (17.1%) 3 (8.6%)
4 10 (28.6%) 17 (48.6%)
5 12 (34.3%) 9 (25.7%)
Comorbidities
Atrial fibrillation 11 (31.4%) 12 (34.3%) 0.06
Coronary artery disease 17 (48.6%) 14 (40.0%) 0.17
Congestive heart failure 6 (17.1%) 3 (8.6%) 0.25
Hypertension 22 (62.9%) 22 (62.9%) 0.00
Chronic renal failure 4 (11.4%) 4 (11.4%) 0.00
Cerebrovascular disease 7 (20.0%) 8 (22.9%) 0.07
Diabetes 8 (22.9%) 5 (14.3%) 0.22
Peripheral vascular disease 2 (5.7%) 2 (5.7%) 0.00
Charlson Comorbidity Index score 1.63 (1.21) 1.31 (0.96) 0.29
Medications
Number of discrete medications used
in previous year
16.80 (7.57) 16.11 (7.68) 0.09
Angiotensin antagonist 21 (60.0%) 19 (54.3%) 0.11
Calcium-channel blocker 18 (51.4%) 21 (60.0%) 0.17
Digoxin 6 (17.1%) 9 (25.7%) 0.21
Diuretic 21 (60.0%) 22 (62.9%) 0.06
Nitrate 14 (40.0%) 10 (28.6%) 0.24
Ophthalmic beta-blocker 1 (2.9%) 2 (5.7%) 0.14
Anti-platelet 14 (40.0%) 12 (34.3%) 0.12
Statin 16 (45.7%) 15 (42.9%) 0.06
Inhaled corticosteroid 25 (71.4%) 24 (68.6%) 0.06
Tiotropium 14 (40.0%) 14 (40.0%) 0.00
Long-acting inhaled beta-agonist 20 (57.1%) 21 (60.0%) 0.06

51
Short-acting inhaled anticholenergic 16 (45.7%) 19 (54.3%) 0.17
Short-acting inhaled beta-agonist 25 (71.4%) 25 (71.4%) 0.00
Methylxanthine 7 (20.0%) 3 (8.6%) 0.33
Data are presented as mean (standard deviation) or number (%), as appropriate.
Legend: COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second;
FVC, forced vital capacity; DLCO, diffusing capacity for carbon monoxide; 6MWD, 6-minute walk
distance; PaO2, partial pressure of oxygen; PaCO2, partial pressure of carbon dioxide; MRC, Medical
Research Council.

52
Table 10. Baseline characteristics, moderate obstructive lung disease subgroup
Variable Beta-blocker users
(N=29)
Non-beta-blocker
users
(N=835)
Standardised
Difference of the
Mean
Demographic / Anthropomorphic
Age, yr 75.31 (4.83) 73.02 (4.88) 0.47
Male 15 (51.7%) 422 (50.5%) 0.02
Body Mass Index, kg/m2 25.65 (7.10) 24.64 (5.62) 0.18
Married 7 (24.1%) 421 (50.4%) 0.53
Income quintile 2.86 (1.60) 2.94 (1.46) 0.05
Index date (year of admission to
pulmonary rehabilitation)
2005 (2.7) 2001 (3.6) 1.15
Health care utilization
Hospitalisations in past 2 years 1.80 (2.37) 1.26 (1.48) 0.27
Cumulative length of stay in hospital in
past 2 years, days
17.60 (28.96) 20.51 (33.52) 0.09
Emergency Department visits in past 2
years
3.29 (5.85) 2.46 (3.28) 0.17
Lung disease
Primary lung diagnosis is COPD 28 (96.6%) 797 (95.4%) 0.05
Any diagnosis of COPD 28 (96.6%) 802 (96.0%) 0.03
Current or former smoker 28 (96.6%) 804 (96.3%) 0.07
Quantity smoked, pack-years 54.48 (40.36) 49.29 (24.92) 0.2
Pulmonary function
FEV1, % predicted 42.41 (15.04) 33.17 (12.49) 0.73
FEV1/FVC ratio, % 43.79 (12.70) 38.39 (10.85) 0.49
DLCO, % predicted 38.38 (17.20) 36.50 (15.65) 0.12
Exercise / gas exchange
6MWD, m 260.69 (107.05) 295.46 (110.54) 0.31
Resting oxygen saturation, % 90.93 (4.74) 91.21 (5.30) 0.05
PaO2, mmHg 63.69 (13.07) 65.02 (12.48) 0.11
PaCO2, mmHg 42.14 (6.24) 44.53 (8.48) 0.28
Exertional desaturation 15 (51.7%) 417 (49.9%) 0.03

53
MRC dyspnea score: 0.55
1 0 1 (0.1%)
2 0 30 (3.6%)
3 5 (17.2%) 189 (22.6%)
4 8 (27.6%) 340 (40.7%)
5 12 (41.4%) 142 (17.0%)
Comorbidities
Atrial fibrillation 10 (34.5%) 91 (10.9%) 0.74
Coronary artery disease 11 (37.9%) 171 (20.5%) 0.43
Congestive heart failure 3 (10.3%) 56 (6.7%) 0.14
Hypertension 20 (69.0%) 310 (37.1%) 0.66
Chronic renal failure 4 (13.8%) 14 (1.7%) 0.85
Cerebrovascular disease 9 (31.0%) 57 (6.8%) 0.92
Diabetes 6 (20.7%) 70 (8.4%) 0.44
Peripheral vascular disease 2 (6.9%) 51 (6.1%) 0.03
Charlson Comorbidity Index score 1.41 (1.02) 0.76 (1.12) 0.59
Medications
Number of discrete medications used
in previous year
17.14 (6.20) 13.51 (5.90) 0.61
Angiotensin antagonist 17 (58.6%) 241 (28.9%) 0.65
Calcium-channel blocker 16 (55.2%) 230 (27.5%) 0.62
Digoxin 7 (24.1%) 98 (11.7%) 0.38
Diuretic 19 (65.5%) 378 (45.3%) 0.41
Nitrate 10 (34.5%) 137 (16.4%) 0.48
Ophthalmic beta-blocker 2 (6.9%) 26 (3.1%) 0.21
Anti-platelet 11 (37.9%) 143 (17.1%) 0.55
Statin 15 (51.7%) 150 (18.0%) 0.87
Inhaled corticosteroid 23 (79.3%) 729 (87.3%) 0.24
Tiotropium 21 (72.4%) 189 (22.6%) 1.19
Long-acting inhaled beta-agonist 24 (82.8%) 415 (49.7%) 0.67

54
Short-acting inhaled anticholenergic 23 (79.3%) 779 (93.3%) 0.54
Short-acting inhaled beta-agonist 16 (55.2%) 677 (81.1%) 0.65
Methylxanthine 7 (24.1%) 380 (45.5%) 0.43
Data are presented as mean (standard deviation) or number (%), as appropriate.
Legend: COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second;
FVC, forced vital capacity; DLCO, diffusing capacity for carbon monoxide; 6MWD, 6-minute walk
distance; PaO2, partial pressure of oxygen; PaCO2, partial pressure of carbon dioxide; MRC, Medical
Research Council.

55
Table 11. Baseline characteristics, moderate obstructive lung disease subgroup, matched sample
Variable Beta-blocker users
(N=18)
Non-beta-blocker
users
(N=18)
Standardised
Difference of the
Mean
Demographic / Anthropomorphic
Age, yr 74.39 (5.23) 74.28 (5.12) 0.02
Male 10 (55.6%) 10 (55.6%) 0.00
Body Mass Index, kg/m2 24.22 (6.87) 24.53 (6.01) 0.05
Married 5 (27.8%) 8 (44.4%) 0.34
Income quintile 3.17 (1.62) 3.17 (1.34) 0.00
Index date (year of admission to
pulmonary rehabilitation)
2004 (3.1) 2003 (3.0) 0.31
Health care utilization
Hospitalisations in past 2 years 1.83 (2.71) 2.11 (2.42) 0.11
Cumulative length of stay in hospital
in past 2 years, days
12.94 (29.60) 27.67 (33.30) 0.47
Emergency Department visits in past 2
years
3.83 (7.12) 4.94 (7.06) 0.16
Lung disease
Primary lung diagnosis is COPD 17 (94.4%) 17 (94.4%) 0.00
Any diagnosis of COPD 17 (94.4%) 18 (100.0%) 0.33
Current or former smoker 17 (94.4%) 18 (100.0%) 0.33
Quantity smoked, pack-years 61.67 (49.53) 48.33 (21.56) 0.35
Pulmonary function
FEV1, % predicted 37.39 (10.56) 38.50 (14.33) 0.09
FEV1/FVC ratio, % 39.94 (10.99) 43.94 (11.10) 0.36
DLCO, % predicted 38.59 (16.88) 35.46 (12.78) 0.21
Exercise / gas exchange
6MWD, m 293.06 (107.19) 227.82 (84.26) 0.67
Resting oxygen saturation, % 90.89 (4.74) 91.44 (4.53) 0.12
PaO2, mmHg 64.22 (14.48) 64.00 (12.00) 0.02
PaCO2, mmHg 43.06 (5.68) 41.94 (8.21) 0.16
Exertional desaturation 11 (61.1%) 11 (61.1%) 0.00

56
MRC dyspnea score: 0.36
3 5 (27.8%) 1 (5.6%)
4 5 (27.8%) 8 (44.4%)
5 6 (33.3%) 6 (33.3%)
Comorbidities
Atrial fibrillation 4 (22.2%) 4 (22.2%) 0.00
Coronary artery disease 6 (33.3%) 5 (27.8%) 0.12
Congestive heart failure 1 (5.6%) 3 (16.7%) 0.35
Hypertension 12 (66.7%) 15 (83.3%) 0.38
Chronic renal failure 0 0 .
Cerebrovascular disease 2 (11.1%) 1 (5.6%) 0.20
Diabetes 2 (11.1%) 1 (5.6%) 0.20
Peripheral vascular disease 1 (5.6%) 0 0.33
Charlson Comorbidity Index score 1.06 (0.87) 0.94 (0.87) 0.13
Medications
Number of discrete medications used
in previous year
17.00 (6.66) 15.72 (6.06) 0.20
Angiotensin antagonist 10 (55.6%) 12 (66.7%) 0.22
Calcium-channel blocker 10 (55.6%) 8 (44.4%) 0.22
Digoxin 4 (22.2%) 5 (27.8%) 0.12
Diuretic 10 (55.6%) 10 (55.6%) 0.00
Nitrate 4 (22.2%) 4 (22.2%) 0.00
Ophthalmic beta-blocker 0 0 .
Anti-platelet 6 (33.3%) 7 (38.9%) 0.11
Statin 7 (38.9%) 7 (38.9%) 0.00
Inhaled corticosteroid 16 (88.9%) 16 (88.9%) 0.00
Tiotropium 11 (61.1%) 11 (61.1%) 0.00
Long-acting inhaled beta-agonist 15 (83.3%) 14 (77.8%) 0.14
Short-acting inhaled anticholenergic 12 (66.7%) 12 (66.7%) 0.00
Short-acting inhaled beta-agonist 17 (94.4%) 15 (83.3%) 0.35
Methylxanthine 6 (33.3%) 7 (38.9%) 0.11
Data are presented as mean (standard deviation) or number (%), as appropriate.
Legend: COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second;
FVC, forced vital capacity; DLCO, diffusing capacity for carbon monoxide; 6MWD, 6-minute walk
distance; PaO2, partial pressure of oxygen; PaCO2, partial pressure of carbon dioxide; MRC, Medical
Research Council.

57
Table 12a. Survival analysis, whole cohort (N=1039), unadjusted.
Outcome Hazard Ratio 95% CI
Death / all-cause hospitalisation 1.07 0.81 - 1.42
Death / cardiorespiratory hospitalisation 0.95 0.71 - 1.28
Death alone 1.40 1.01 - 1.94
Death / cardiac hospitalisation 1.57 1.15 - 2.14
Death / respiratory hospitalisation 0.85 0.63 - 1.16
Table 12b. Survival analysis, matched cohort (N=62), primary propensity score model.
Outcome Hazard Ratio 95% CI
Death / all-cause hospitalisation 1.07 0.53 - 2.16
Death / cardiorespiratory hospitalisation 1.00 0.49 - 2.05
Death alone 1.25 0.59 - 2.67
Death / cardiac hospitalisation 1.07 0.52 - 2.22
Death / respiratory hospitalisation 1.14 0.56 - 2.34
Table 12c. Survival analysis, matched cohort (N=70), secondary propensity score model.
Outcome Hazard Ratio 95% CI
Death / all-cause hospitalisation 1.33 0.68 - 2.60
Death / cardiorespiratory hospitalisation 1.06 0.55 - 2.05
Death alone 2.22 1.01 - 4.88
Death / cardiac hospitalisation 2.10 0.99 - 4.46
Death / respiratory hospitalisation 0.89 0.45 - 1.74
Table 12d. Survival analysis, moderate obstructive lung disease subgroup, unadjusted
(N=864).
Outcome Hazard Ratio 95% CI
Death / all-cause hospitalisation 1.03 0.71 - 1.50
Death / cardiorespiratory hospitalisation 0.87 0.59 - 1.29
Death alone 1.13 0.72 - 1.77
Death / cardiac hospitalisation 1.32 0.86 - 2.02
Death / respiratory hospitalisation 0.77 0.51 - 1.15
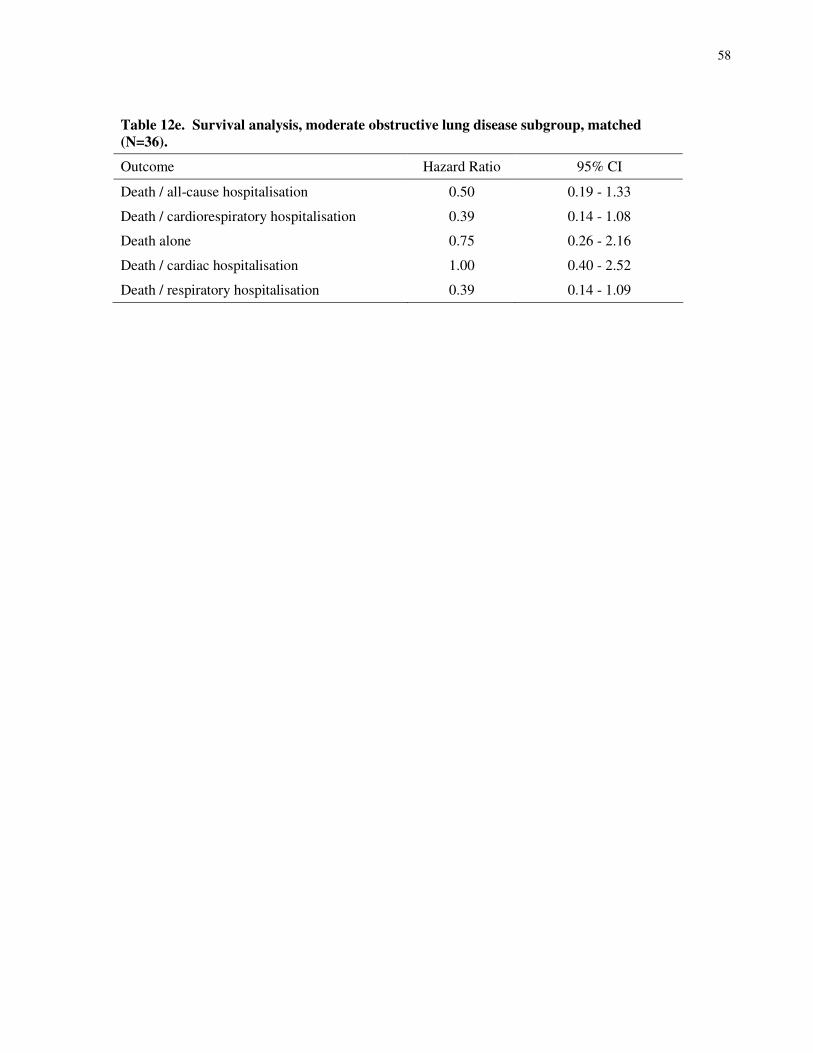
58
Table 12e. Survival analysis, moderate obstructive lung disease subgroup, matched
(N=36).
Outcome Hazard Ratio 95% CI
Death / all-cause hospitalisation 0.50 0.19 - 1.33
Death / cardiorespiratory hospitalisation 0.39 0.14 - 1.08
Death alone 0.75 0.26 - 2.16
Death / cardiac hospitalisation 1.00 0.40 - 2.52
Death / respiratory hospitalisation 0.39 0.14 - 1.09

59
Figures
Figure 1. Power plots.
0
0.2
0.4
0.6
0.8
1
0.6 0.7 0.8 0.9
Detectable HR
1300
1100
900
0
0.2
0.4
0.6
0.8
1
0.6 0.7 0.8 0.9
Detectable HR
12
24
36
Legend: HR, hazard ratio.