bevacizumab in metastatic breast cancer (mbc) · pdf filebevacizumab in metastatic breast...
TRANSCRIPT

Bevacizumab in Metastatic Breast Cancer (MBC)
Sandra M. Swain, M.D.Medical Director, Washington Cancer Institute

APPROVED AGENTS IN MBC

Agent Type of Approval
Approval Endpoint
Trastuzumab + paclitaxel (1998)
Regular Overall Survival (OS)
Gemcitabine + paclitaxel (2004)
Regular Time to Progression (TTP); OS (trend)
Bevacizumab + paclitaxel (2008)
Accelerated Progression Free Survival (PFS)
Lapatinib + letrozole (2010)
Accelerated PFS; OS data still immature
FDA approvals for 1st line MBC

FDA approvals for 2nd line MBC
Agent Type of Approval Approval Endpoint
Paclitaxel (1994) Regular
Docetaxel (1998) Regular OSNab-paclitaxel (2005) Regular Target Lesion Response Rate
(TLRR)Ixabepilone (2007) Regular ORR
Lapatinib + cape (2007) RegularCape + docetaxel (2001) Regular OSEribulin (2010) Regular OS
ANTIANGIOGENIC AGENTS

Adapted from Gerber H and Ferrara N. Cancer Research 2005;65:671-680
Antiangiogenic Agents

sorafenib
bevacizumab
sorafenibsunitinib
Antiangiogenic Agents
Adapted from Gerber H and Ferrara N. Cancer Research 2005;65:671-680

BEVACIZUMAB

Bevacizumab• Avastin®, Genentech• A recombinant human monoclonal anti-VEGF
antibody that binds to and neutralizes all biologically active isoforms of VEGF
• The first antiangiogenic drug to demonstrate a survival benefit in cancer patients
• Initially approved by the Food and Drug Administration (FDA) in 2004 as first line treatment for metastatic colon cancer

MILESTONE TRIALS IN BEVACIZUMAB AND MBC

Metastatic breast cancer • Measurable disease• Prior anthracycline + taxane
therapy required• HER2+ or HER2–
Primary endpoint• PFS by IRF
Stratification• ECOG performance status• Number of prior chemotherapy regimens
Capecitabine2500 mg/m2 q day × 14q 3 wk
Capecitabine2500 mg/m2 q day × 14Avastin 15 mg/kgq 3 wk
N = 450
RANDOMIZE
1:1From Genentech slides, 2007Miller et al. J Clin Oncol 2005;23
AVF2119g: Study Design

AVF2119g Study: PFS
Slides from ODAC meeting, Dec 2007Miller et al. J Clin Oncol 2005;23

AVF2119g Study: PFS
Slides from ODAC meeting, Dec 2007Miller et al. J Clin Oncol 2005;23

Treatment group: CAP CAP+AVF ---
AVF2119g Study: OS
Slides from ODAC meeting, Dec 2007Miller et al. J Clin Oncol 2005;23

Treatment group: CAP CAP+AVF ---
AVF2119g Study: OS
Slides from ODAC meeting, Dec 2007Miller et al. J Clin Oncol 2005;23

AE known to occur with bevacizumab
Slides from ODAC meeting, Dec 2007Miller et al. J Clin Oncol 2005;23

AE known to occur with bevacizumab
Slides from ODAC meeting, Dec 2007Miller et al. J Clin Oncol 2005;23

AVF2119g: capecitabine + bev in MBC
• Negative study• PFS benefit of 0.69 months (p=0.86) and OS
benefit of 0.60 months (p=1.0)• Adverse Events: bleeding more than 2x than in
placebo group; hypertension more than 9x than in placebo group
• IRF and investigator disagreed in the definition of disease progression in 22% of patients
Miller et al. J Clin Oncol 2005;23

MBC not previously treated with
chemotherapy(N = 685)
Stratification- Disease-free interval- Adjuvant therapy- ER+, ER–, unknown- Number of metastatic
Sites (< 3 vs. ≥ 3)
Paclitaxel: 90 mg/m2 IV infusion over 1 hr every wk for 3 wk followed by 1 wk of restAvastin: 10 mg/kg following paclitaxel treatment on Wk 1 and 3 of every cycle
RANDOMIZED
Paclitaxel: 90 mg/m2 IV infusion over 1 hr every wk for 3 wk followed by 1 wk of rest
TREAT
UNTIL
PD
E2100: Study Design
Adapted from Genentech slides 2007Miller K et al. N Engl J Med 2007;357:2666-76

E2100: Study Design
• Open label study
• Primary endpoint: PFS
• Secondary endpoints: OSORRToxicityQuality of life
Miller K et al. N Engl J Med 2007;357:2666-76

E2100: Patients characteristicsDemographic / Tumor characteristics Total (N=722)Female (%) 99.2Age 55 (27-85)Post menopausal (%) 55.3Metastatic disease (%) 98.3HER2 negative (%) 98.9
Common sites of involvement (%)Bone 54.5Liver 41.7Lung 41.5
ER status (%) Positive 38.2Negative 61.8
No measurable disease at baseline (%) 27.3Miller K et al. N Engl J Med 2007;357:2666-76

E2100: Prior Cancer Therapy
Adapted from FDA slides 2007Miller K et al. N Engl J Med 2007;357:2666-76
Prior Cancer Therapy Total (N=722)Hormonal therapy (Adjuvant or Metastatic setting)
61%
Adjuvant Chemotherapy 66%
Prior taxane 20%
Prior anthracycline 50%

All PatientsAge < 40 yrAge 40 - 64 yrAge ≥ 65 yr< 3 Metastatic sites≥ 3 Metastatic sitesMeasurable disease at baselineNon-measurable disease at baselineNo prior adjuvant chemotherapyPrior adjuvant chemotherapy
Prior adjuvant TAXANE therapyER+
ER–
Paclitaxel betterPaclitaxel + Avastin better
0.50.2 521Hazard ratio
E2100: PFS Consistent Across Subgroups
Adapted from Genentech slides 2007
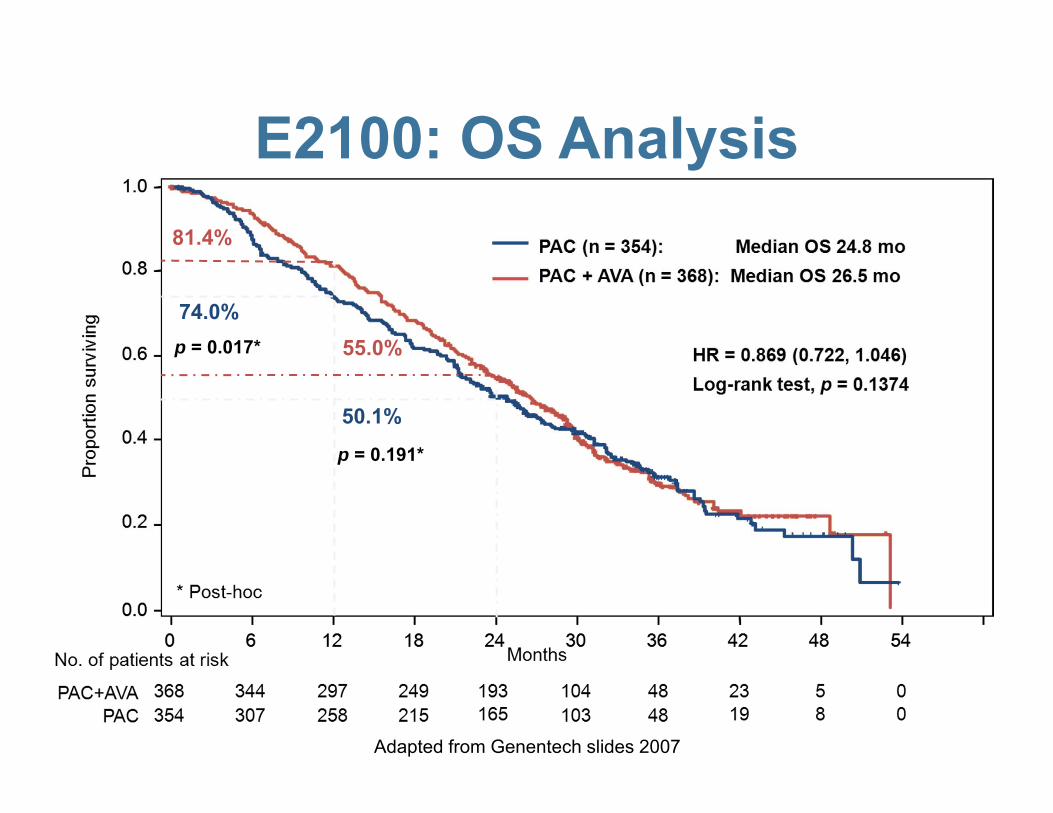
p = 0.017*
74.0%
81.4%
50.1%
55.0%
p = 0.191*
E2100: OS Analysis
Adapted from Genentech slides 2007

AE Grade 3-5 known to occur with bev
PACN=348 (%)
PAC/BVN=363 (%)
Hypertension 5 (1.4) 57 (15.7)Proteinuria 0 10 (2.8)Arterial Thromboembolic Events
Cerebrovascular ischemiaCardiac ischemia
000
10 (2.8)7 (1.9)3 (0.8)
Venous Thromboembolic Events 15 (4.3) 9 (2.5)
Bleeding/Hemorrhage 1 (0.3) 6 (1.7)Congestive Heart Failure 1 (0.3) 5 (1.4)GI perforation/fistula 0 3 (0.9)Neutropenia/infection 28 (8) 62 (17.1)
Adapted from FDA slides 2007

Additional Adverse Events Grade 3-4
Adapted from FDA slides 2007
PAC % (N=348)
PAC/BV % (N=363)
Sensory neuropathy 18 24VomitingDiarrheaDehydration
211
653
Fatigue 5 11Pain 10 16

Adapted from Genentech slides – Public Hearing 2011
Reasons for Treatment Discontinuation
Status and reason for discontinuation Paclitaxel(n = 354)
(%)
Paclitaxel + Avastin(n = 368)
(%)
Total(N = 722)
(%)Not treated 2.3 0.5 1.4
Treatment ongoing 2 11 7
Discontinued protocol therapy 96 89 92
Disease progression 55 45 50
Toxicity/side effects/complications 19 20 20
Death 1.4 1.6 1.5
Other 20 22 21
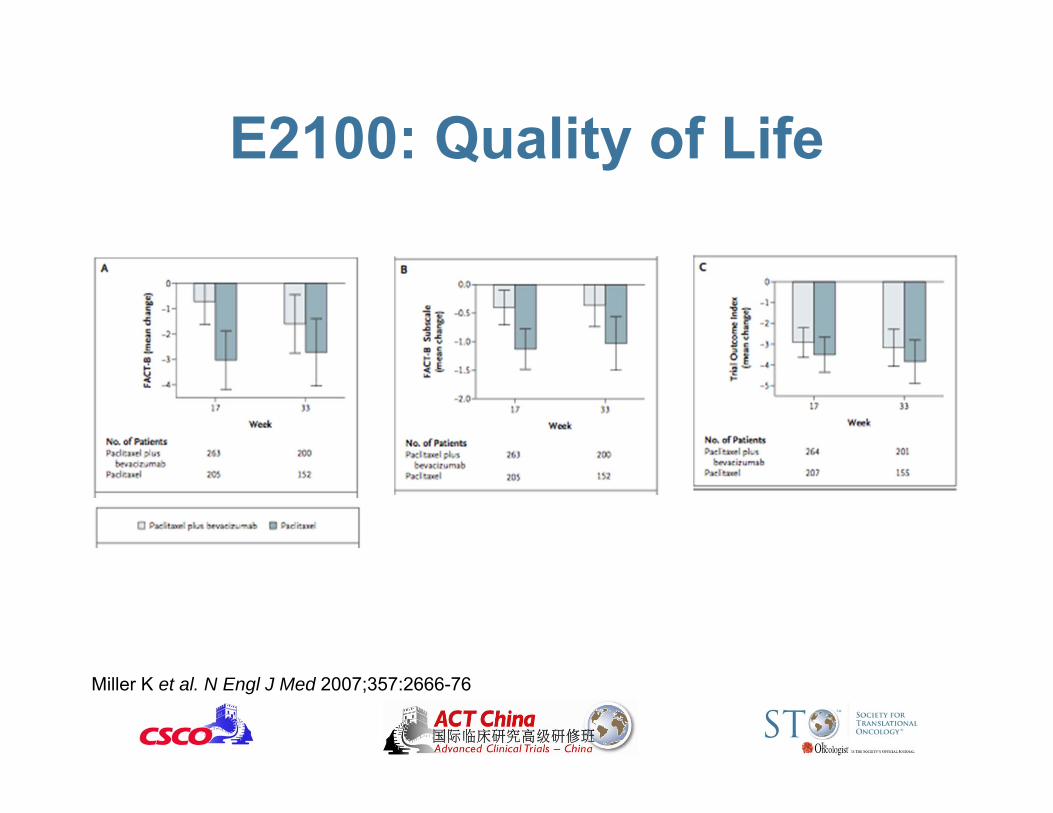
E2100: Quality of Life
Miller K et al. N Engl J Med 2007;357:2666-76

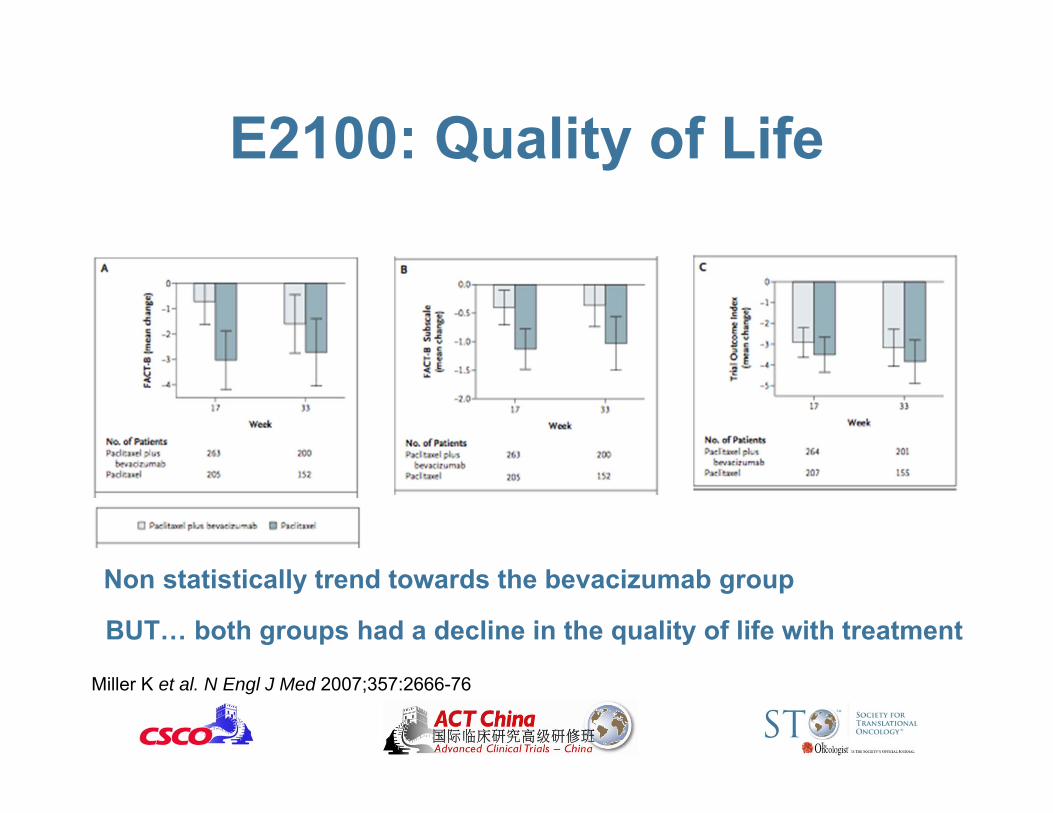
E2100: Quality of Life
Miller K et al. N Engl J Med 2007;357:2666-76
Non statistically trend towards the bevacizumab group
Non statistically trend towards the bevacizumab group
BUT… both groups had a decline in the quality of life with treatment
E2100: Quality of Life
Miller K et al. N Engl J Med 2007;357:2666-76

E2100: Quality of Life
Miller KD presentation to ODAC 2007

E2100: Quality of Life
Miller KD presentation to ODAC 2007
Non placebo trial…

E2100: Paclitaxel + Bevacizumab in MBC
• PFS benefit that did not translate into a OS benefit:– ∆ PFS 5.5 months and ∆ OS 1.7 months
• No improvement in the quality of life, with decline in both groups from the beginning
• Increased incidence of hypertension (11x), bleeding (6x), CHF (5x) and neutropenia (2x) in the bevacizumab arm
Miller K et al. N Engl J Med 2007;357:2666-76

E2100 and AVF2119g: Treatment Summary
E2100 AVF2119
PAC(n = 348)
PAC + AVA(n = 363)
Cape(n = 215)
Cape + AVA(n = 229)
Median number of cycles administered
6 10 4 6
4-wk cycles 3-wk cycles
Discontinuation due to toxicity, %
19 20 12 10
Treatment-related deaths, %
Not assessable by Genentech 1.7* 0.9 0.4
Comprehensive Genentech clinical review, 2007

ODAC Meeting December 2007
• Concerns that the E2100 study had shortcomings and inconsistencies such as data collection and imaging discordance.
• Committee members agreed that PFS is a clinically meaningful endpoint but had issues with how best to measure it. If PFS is the endpoint, the study must be powered for survival.
• Are the data provided sufficient to establish a favorable risk/benefit analysis for the use of bevacizumab plus paclitaxel for first-line treatment of patients with MBC ?
5 No 4 Yes

OS PFS
Pros Gold standard endpoint of clinical trials in oncology
Provides results at an earlier endpoint
Cons Requires elevated number of patients
Greater degree of subjectivity
Results affected by subsequent treatment choices
Difficult to establish what is a robust result, especially when it does not translate into a OS benefit
OS vs. PFS

Definition of SPP (Survival Post-Progression)
OS = PFS + SPPIf the progression eventis death, then SPP = 0
Broglio KR & Berry DA, JNCI 2009

Res
pons
e R
ate
Progression-free Survival
In breast cancer (as in other cancers), RR correlates with PFS
Adapted from Tito Fojo

Res
pons
e R
ate
Progression-free Survival
In breast cancer RR correlates with PFS: exception paclitaxel + bevacizumab
Adapted from Tito Fojo
Paclitaxel +Bevacizumab

FDA February 2008 Study Design
• Accelerated approval of bevacizumab used in conjunction with paclitaxel as first line therapy for patients with MBC.
• This approval required further trials to confirm the perceived clinical benefit.

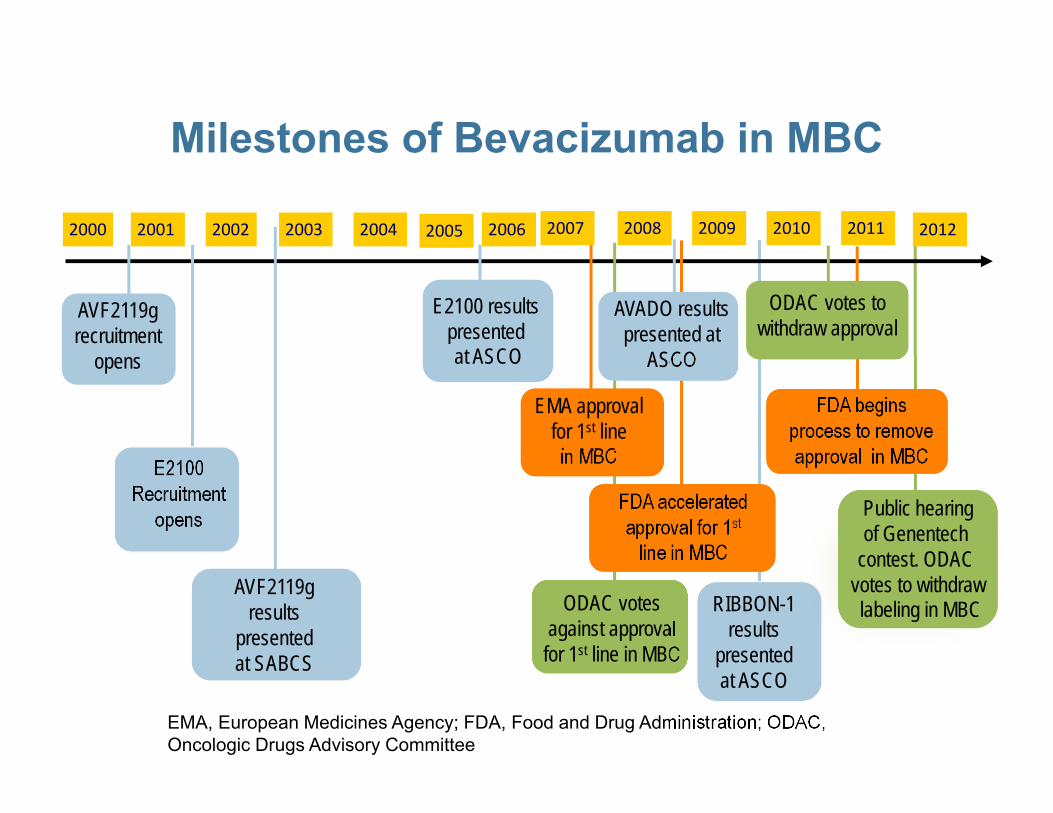
Milestones of Bevacizumab in MBC
AVF2119g recruitment
opens
E2100 Recruitment
opens
AVADO results presented at
ASCO
AVF2119g results
presented at SABCS
FDA acceleratedapproval for 1st
line in MBC
EMA approval for 1st line in MBC
2001 20032000 2002
ODAC votes against approval for 1st line in MBC
FDA begins process to remove approval in MBC
ODAC votes to withdraw approval
2004 2005 2006 2007 2008 2009 2010 2011 2012
E2100 results presented at ASCO
Public hearing of Genentech
contest. ODAC votes to withdraw labeling in MBC RIBBON-1
resultspresented at ASCO
EMA, European Medicines Agency; FDA, Food and Drug Administration; ODAC, Oncologic Drugs Advisory Committee

Accrual: 736 Docetaxel 100 mg/m2
+ Placebo q3w x 9 *
Docetaxel 100 mg/m2
+ bevacizumab 7.5 mg/kg q3w x 9 *
Docetaxel 100 mg/m2
+ bevacizumab 15 mg/kg q3w x 9 *
*Bevacizumab or placebo administered until disease progression
Eligibility1st-line locallyrecurrent or mBC
HER2-negative
No prior chemotherapyfor locally recurrent or mBC, unless relapse is>6 months since last dose (>12 months if taxane-based)
R
AVADO: Study Design
Miles DW et al. SABCS 2009;Abstract 41.

1.0
0.8
0.6
0.4
0.2
00 6 12 18 24 30 36
PFSestimate
Time (months)
9.0a,b
a 8.2b 8.1
Placebo + docetaxel (n=241)Bevacizumab 7.5 mg/kg q3w + docetaxel (n=248)
Intent-to-treat analysis; *p values are of exploratory nature‡Censored for non-protocol therapy prior to progressive disease; a unstratified; b stratified
Unstratified HR=0.86 (0.72–1.04), p=0.1163*Stratified HR‡=0.80 (0.65–1.00), p=0.0450*
AVADO: PFS Analysis (Bev 7.5mg/kg dose)
Miles DW et al. SABCS 2009;Abstract 41.

Unstratified HR=0.77 (0.64–0.93), p=0.0061*Stratified HR‡=0.67 (0.54–0.83), p=0.0002*
10.1a
10.0ba 8.2b 8.1
Placebo + docetaxel (n=241)Bevacizumab 15 mg/kg q3w + docetaxel (n=247)
1.0
0.8
0.6
0.4
0.2
00 6 12 18 24 30 36
PFSestimate
Time (months)
Intent-to-treat analysis; *p values are of exploratory nature‡Censored for non-protocol therapy prior to progressive disease; a unstratified; b stratified
AVADO: PFS Analysis (Bev 15mg/kg dose)
Miles DW et al. SABCS 2009;Abstract 41.

AVADO: Efficacy Analysis
BV, 7.5 mg/kg + docetaxel(n = 248)
BV, 15 mg/kg + docetaxel(n = 247)
Placebo + docetaxel(n = 241)
Median PFSHR (vs placebo)p-value (vs placebo)
9.0 mos0.80*
0.0450†
10.0 mos0.67*
0.0002†
8.1 mos——
Median OSHR (vs placebo)p-value (vs placebo)
30.8 mos1.05
0.7198†
30.2 mos1.03
0.8528†
31.9 mos——
*Stratified; † p values are of exploratory nature.
Miles DW et al. SABCS 2009;Abstract 41.

AVADO: Efficacy Analysis (continued)
Patients with measurable disease at baseline
BV, 7.5 mg/kg + docetaxel(n = 201)
BV, 15 mg/kg + docetaxel(n = 206)
Placebo + docetaxel(n = 207)
Overall response rate (ORR)p-value (vs control)†
55.2%0.0739
64.1%0.0003
46.4%—
Intent to treat population (n = 248) (n = 247) (n = 241)
1-year survival ratep-value (vs control)†
81%0.198
84%0.02
76%—
Patients still at risk (n) 195 201 178
† p values are of exploratory nature.
Miles DW et al. SABCS 2009;Abstract 41.
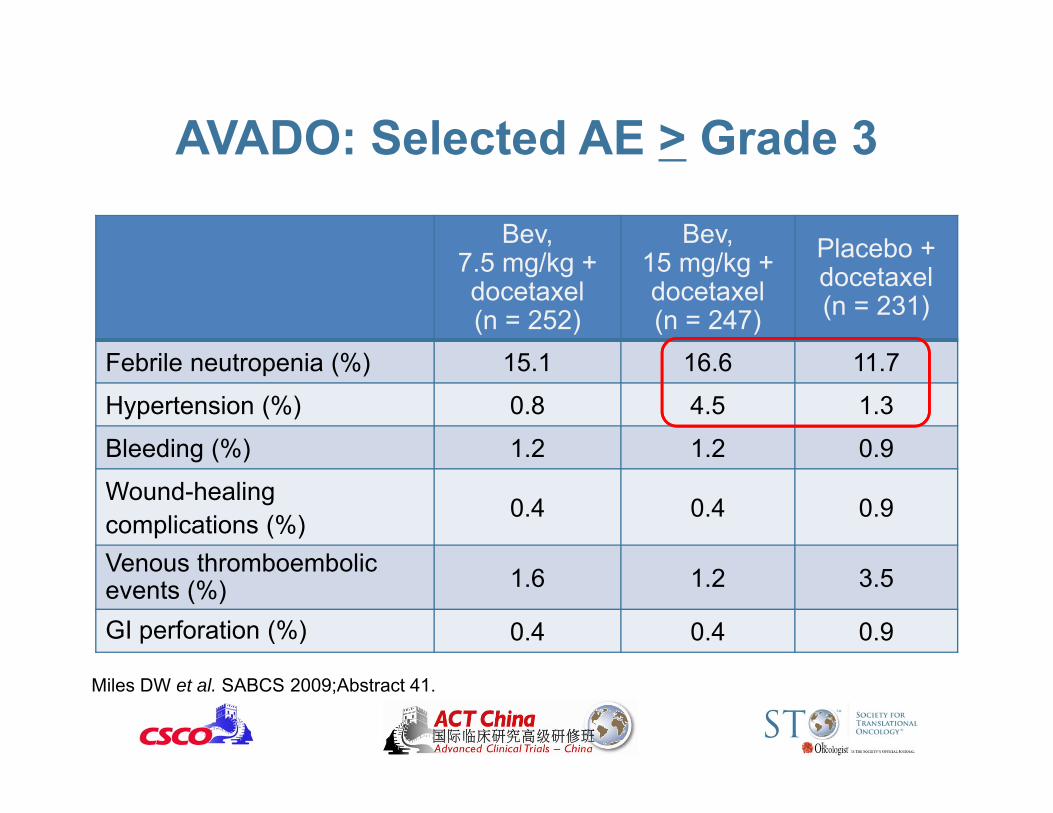
AVADO: Selected AE > Grade 3
Bev,7.5 mg/kg + docetaxel(n = 252)
Bev,15 mg/kg + docetaxel(n = 247)
Placebo + docetaxel(n = 231)
Febrile neutropenia (%) 15.1 16.6 11.7
Hypertension (%) 0.8 4.5 1.3
Bleeding (%) 1.2 1.2 0.9
Wound-healing complications (%) 0.4 0.4 0.9
Venous thromboembolic events (%) 1.6 1.2 3.5
GI perforation (%) 0.4 0.4 0.9
Miles DW et al. SABCS 2009;Abstract 41.

AVADO: Docetaxel +/- Bev• Blinded study • Confirms results of E2100 but smaller amplitude:
first-line BV 15 mg/kg plus docetaxel significantly improves PFS (10.0 months vs. 8.1 months) compared to docetaxel alone in patients with HER2- MBC.
• No difference in OS was observed between the study arms
• Lower frequencies of grade 3 and 4 AE than in E2100• Scarce data on quality of life
Miles D et al. J Clin Oncol 2010;28
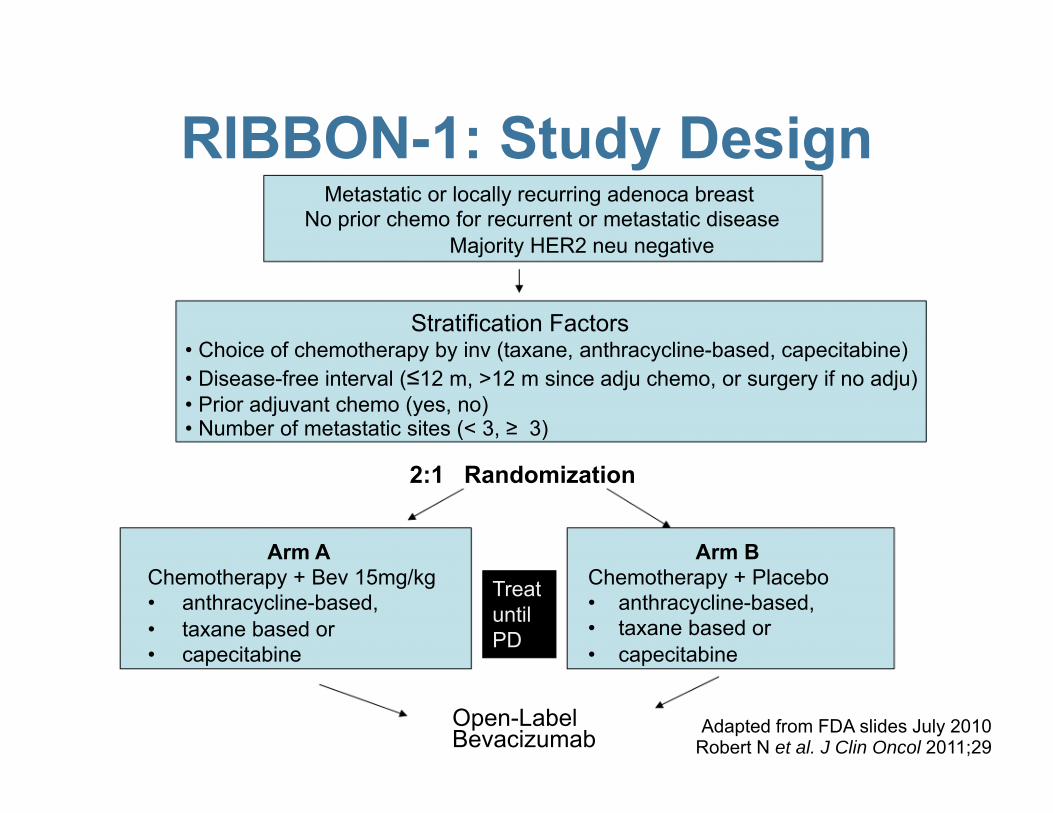
Metastatic or locally recurring adenoca breastNo prior chemo for recurrent or metastatic disease
Majority HER2 neu negative
Stratification Factors• Choice of chemotherapy by inv (taxane, anthracycline-based, capecitabine)• Disease-free interval (≤12 m, >12 m since adju chemo, or surgery if no adju)• Prior adjuvant chemo (yes, no)• Number of metastatic sites (< 3, ≥ 3)
2:1 Randomization
Arm A Arm BChemotherapy + Bev 15mg/kg Chemotherapy + Placebo• anthracycline-based, • anthracycline-based,• taxane based or • taxane based or• capecitabine • capecitabine
Open-Label Bevacizumab Robert N et al. J Clin Oncol 2011;29
Adapted from FDA slides July 2010
Treat until PD
RIBBON-1: Study Design

Robert N et al. J Clin Oncol 2011;29
RIBBON-1: Study Design• Primary endpoint: PFS (by inv)• Secondary endpoints: OS, ORR, PFS (by
IRC), safety• Allowed chemotherapy regimens:
– Anthracycline-based (AC, EC, FAC, FEC)– Taxane (docetaxel or protein bound paclitaxel)– Capecitabine
• Paclitaxel was not considered a chemotherapy option!

PFS KM Curves -Taxane/Anthracycline Cohort
Bevacizumab
HR 0.64 (0.52, 0.80) Placebo

RIBBON-1: PFS
T/Anth + PI207
T/Anth + Bev415
No. with an event (%)Disease progressionDeath
160 (77.3)14911
249 (60.0)21732
Median (month)(95% CI)
8.0(6.7, 8.4)
9.2(8.6, 10.1)
Hazard ratio(95% CI)
0.64(0.52, 0.80)
p-value <0.0001Adapted from FDA slides July 2010Robert N et al. J Clin Oncol 2011;29
Taxane/Anthracycline Cohort

OS KM Curves -
HR 1.1 (0.86, 1.43)
Taxane/Anthracycline Cohort
Placebo
Bevacizumab
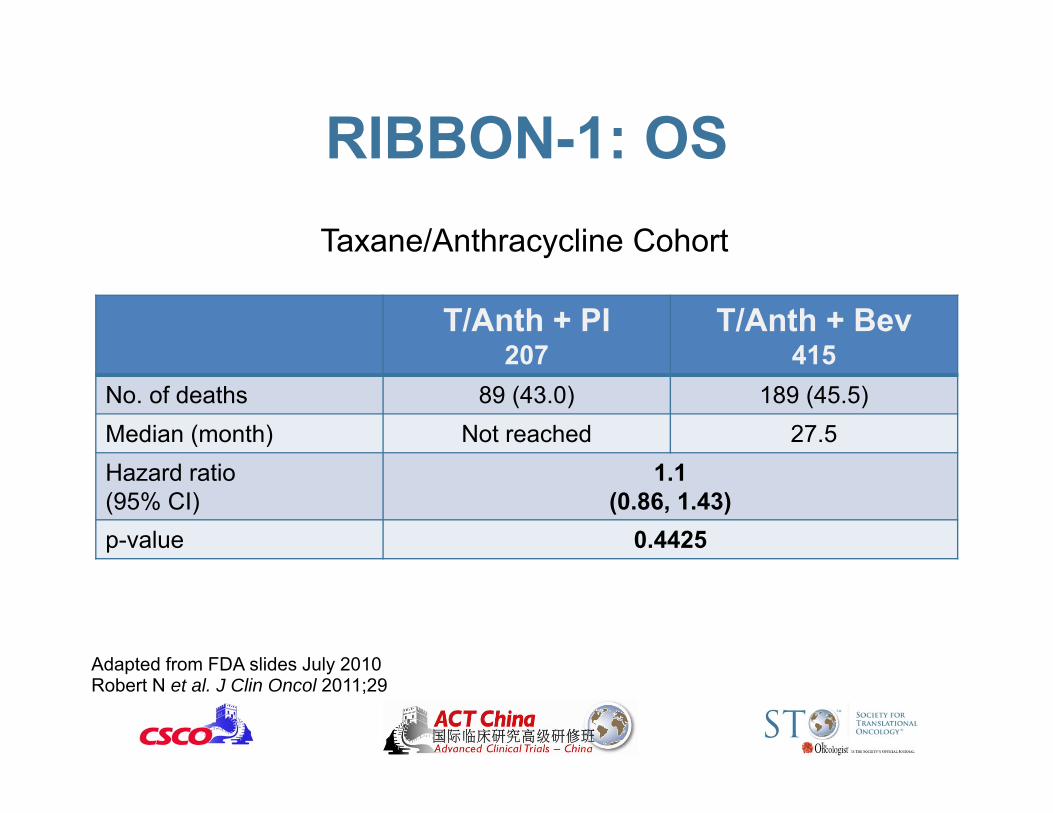
RIBBON-1: OS
T/Anth + PI207
T/Anth + Bev415
No. of deaths 89 (43.0) 189 (45.5)Median (month) Not reached 27.5Hazard ratio(95% CI)
1.1(0.86, 1.43)
p-value 0.4425
Taxane/Anthracycline Cohort
Adapted from FDA slides July 2010Robert N et al. J Clin Oncol 2011;29
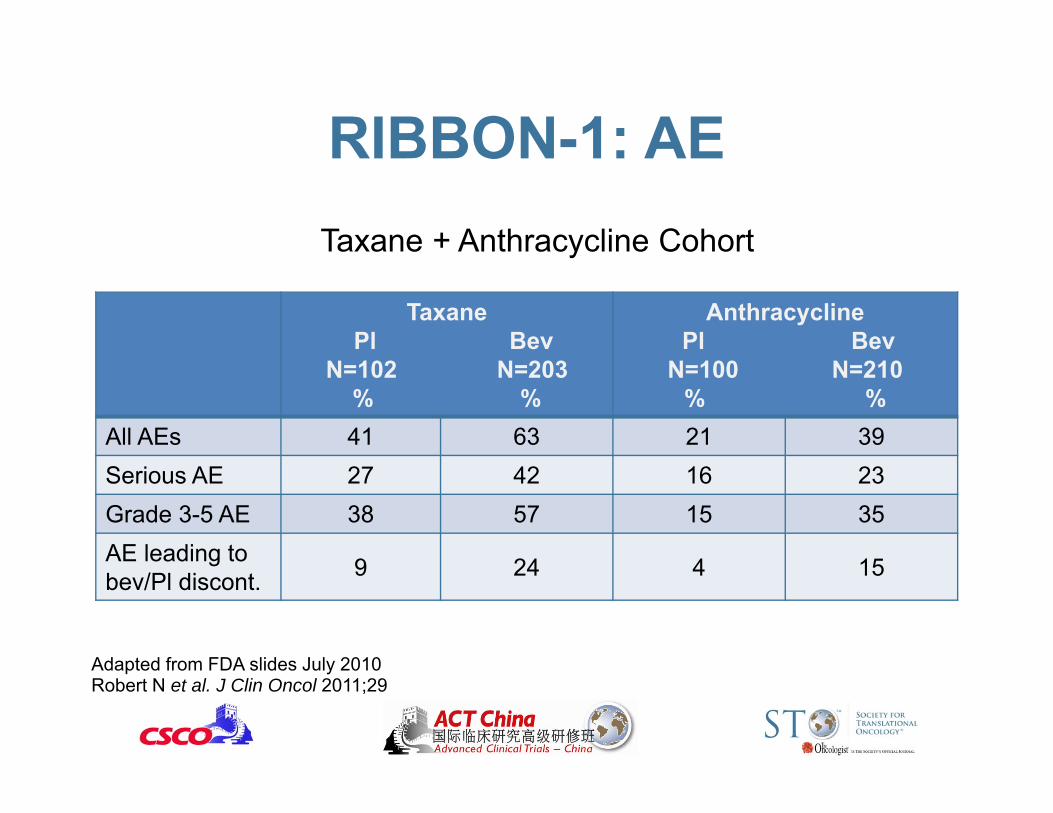
RIBBON-1: AE
TaxanePl Bev
N=102 N=203% %
AnthracyclinePl Bev
N=100 N=210% %
All AEs 41 63 21 39Serious AE 27 42 16 23Grade 3-5 AE 38 57 15 35AE leading to bev/Pl discont. 9 24 4 15
Taxane + Anthracycline Cohort
Adapted from FDA slides July 2010Robert N et al. J Clin Oncol 2011;29

RIBBON-1: AE Grade > 3-5
TaxanePl Bev
N=102 N=203% %
AnthracyclinePl Bev
N=100 N=210% %
Hypertension 2.0 9.4 0 10Febrile Neutropenia 2.0 7.9 5.0 3.8Bleeding/hemorrhage 0 5.4 0 0Proteinuria 0 3.9 0 1.9LV systolic dysfunction 0 2.0 0 2.9
Taxane + Anthracycline Cohort
Cut off – Feb 23, 2009Adapted from FDA slides July 2010Robert N et al. J Clin Oncol 2011;29

PFS KM Curves -Capecitabine Cohort
Bevacizumab
Placebo
HR 0.69 (0.56, 0.84)

RIBBON-1: PFS
Cap + PI206
Cap + Bev409
No. with an event (%)Disease progressionDeath
162 (78.6)14913
291 (71.1)26625
Median (month) 5.7 8.6Hazard ratio(95% CI)
0.69(0.56, 0.84)
p-value <0.0001
Capecitabine Cohort
Adapted from FDA slides July 2010Robert N et al. J Clin Oncol 2011;29

OS KM Curves -Capecitabine Cohort
Bevacizumab
Placebo
HR 0.88 (0.69, 1.13)P = 0.329
6
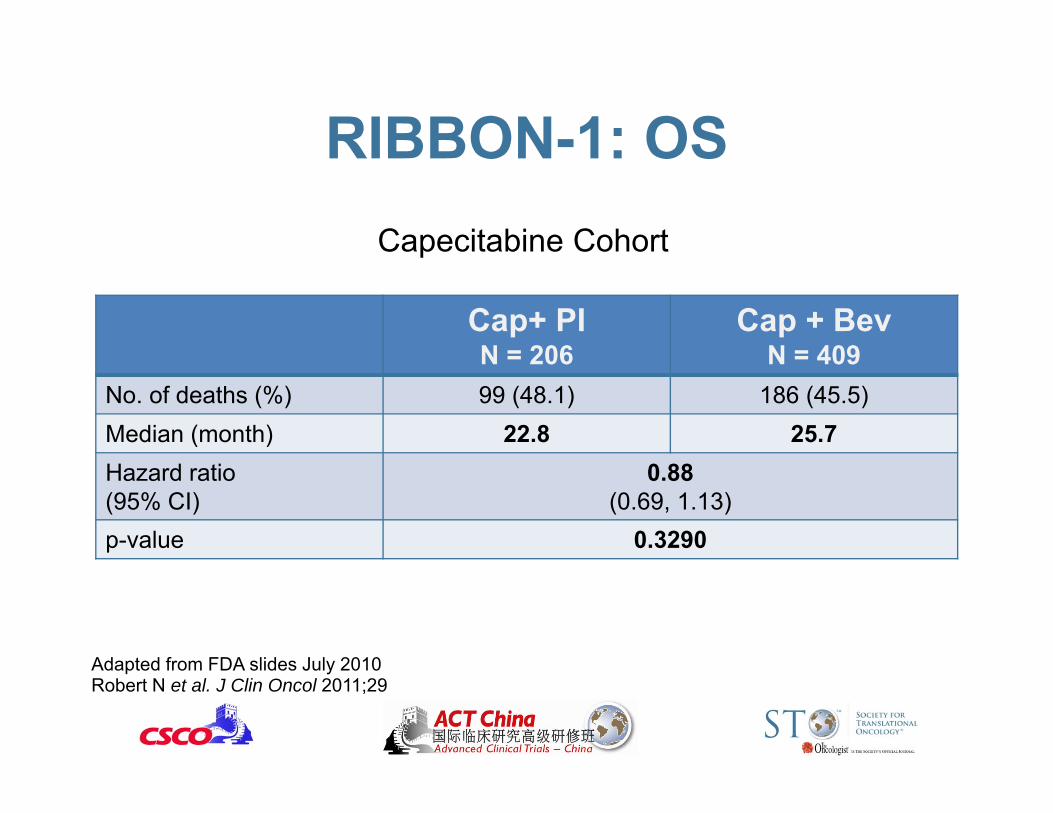
RIBBON-1: OS
Cap+ PIN = 206
Cap + BevN = 409
No. of deaths (%) 99 (48.1) 186 (45.5)Median (month) 22.8 25.7Hazard ratio(95% CI)
0.88(0.69, 1.13)
p-value 0.3290
Capecitabine Cohort
Adapted from FDA slides July 2010Robert N et al. J Clin Oncol 2011;29

RIBBON-1: AE
CapecitabinePlacebo BevacizumabN=201 N=404
% %Any (collected) AEs* 27 40Serious AE 20 25Grade 3-5 AE 23 37AD leading to bev/pldiscont. 12 13
* Only selected AEs collected
Capecitabine Cohort
Adapted from FDA slides July 2010Robert N et al. J Clin Oncol 2011;29
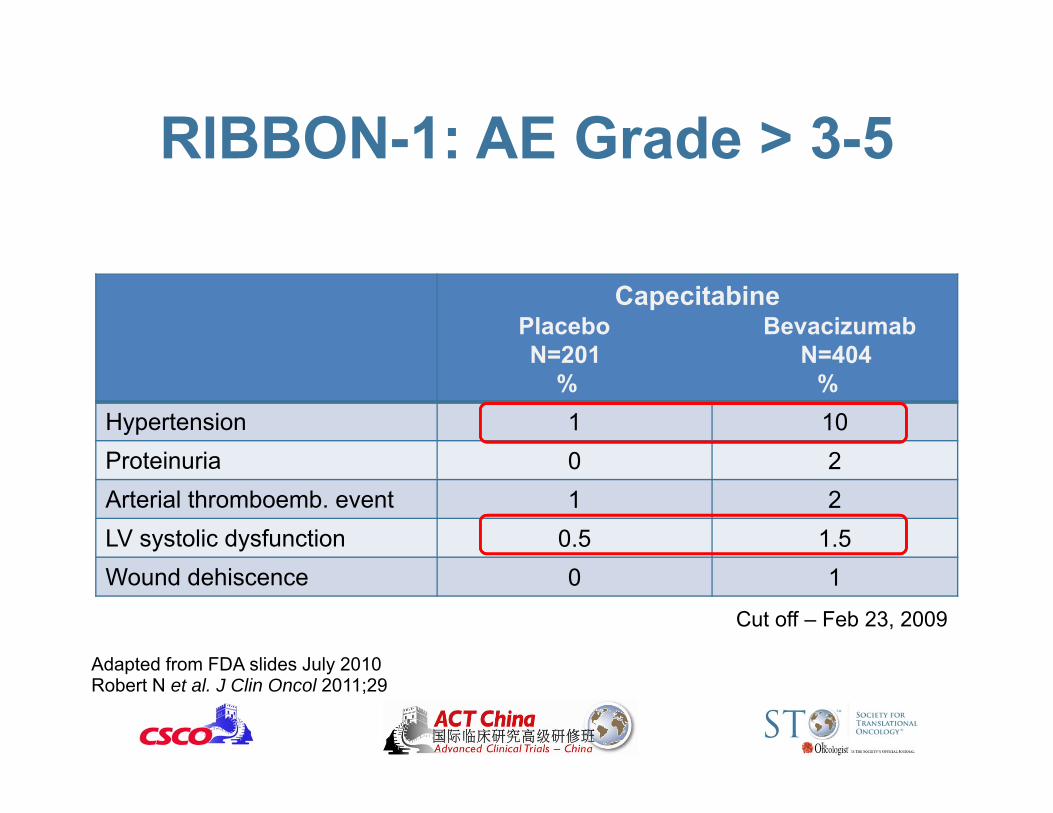
RIBBON-1: AE Grade > 3-5
CapecitabinePlacebo BevacizumabN=201 N=404
% %Hypertension 1 10Proteinuria 0 2Arterial thromboemb. event 1 2LV systolic dysfunction 0.5 1.5Wound dehiscence 0 1
Cut off – Feb 23, 2009
Adapted from FDA slides July 2010Robert N et al. J Clin Oncol 2011;29

RIBBON1: Different chemo regimens +/- bev
• Two independently powered cohorts that confirm PFS benefit seen in E2100 study but with lower amplitude of response: – ∆ PFS (cape + bev) = 2.9 months– ∆ PFS (tax/anthra + bev) = 1.2 months
• No improvement in OS • Increase in bleeding events with bev+tax
(5x), and increased risk of hypertension (10X) and LV systolic dysfunction (2-3x) across all subgroups
Robert N et al. J Clin Oncol 2011;29

* Independent Review Facility
Summary: Studies Design Study design E2100 AVADO Ribbon-1
Capecitabine
Ribbon-1Anth/Tax
Placebo controlled
No Yes Yes Yes
Chemotherapy Weekly paclitaxel
Q3w docetaxel
Capecitabine Q3w doc/nabPAC/FAC/EC/FEC
Dose of bevacizumab
10 mg/kg q2w
7.5 or 15 mg/kg q3w
15 mg/kg q3w
15 mg/kg q3w
Treat until PD Yes No Yes Yes
IRF* review Retrospective Yes Yes Yes

Treatment regimen (s)
HR for PFS Difference in Median PFS
HR for OS Difference in median OS
Paclitaxel +/-bev 15 mg/kg 0.48 + 5.5 months 0.87 +1.7 months
Docetaxel +/-bev 7.5 mg/kg 0.70 +0.8 months 1.103 -1.1 months
Docetaxel +/-bev 15 mg/kg 0.62 + 0.9 months 1.003 -1.7 months
Taxane/Ant +/-bev 15 mg/kg 0.64 +1.2 months 1.1 +1.4 months
Capecitabine +/-bev 15 mg/kg 0.69 + 2.9 months 0.88 +2.9 months
E2100
AVADO
RIBBON1
Adapted from FDA slides July 2010
Summary: PFS and OS

Milestones of Bevacizumab in MBC
AVF2119g recruitment
opens
E2100 Recruitment
opens
AVADO results presented at
ASCO
AVF2119g results
presented at SABCS
FDA acceleratedapproval for 1st
line in MBC
EMA approval for 1st line in MBC
2001 20032000 2002
ODAC votes against approval for 1st line in MBC
FDA begins process to remove approval in MBC
ODAC votes to withdraw approval
EMA, European Medicines Agency; FDA, Food and Drug Administration; ODAC, Oncologic Drugs Advisory Committee
2004 2005 2006 2007 2008 2009 2010 2011 2012
E2100 results presented at ASCO
Public hearing of Genentech
contest. ODAC votes to withdraw labeling in MBC RIBBON-1
resultspresented at ASCO

ODAC Meeting July 2010• No improvement in overall survival: HR favors placebo arm in
AVADO and RIBBON 1 (Taxane/Anthracycline cohort)• Addition of bevacizumab to taxanes, anthracycline and
capecitabine resulted in an overall ↑ in serious AEs and grade 3-5 AEs
• Toxicities attributed to bevacizumab:– Hypertension – Proteinuria – Bleeding/hemorrhage– Gastrointestinal perforation/fistulas – Arterial and venous thromboembolic events – Wound healing complications– 0.8 – 1.2 % bevacizumab related death

ODAC Meeting July 2010• Question 1: (AVADO study) Does the addition
of bevacizumab to docetaxel represent a favorable risk/benefit analysis for the initial treatment of patients with MBC?Yes 0 No 13
• Question 2: (RIBBON1 study) Does the addition of bevacizumab to taxanes, anthracyclines or capecitabine represent a favorable risk/benefit analysis for the initial treatment of patients with MBC?Yes 1 No 12

ODAC Meeting July 2010• Question 3: Taking into consideration the totality of
findings, and the responses to Questions 1 and 2 above, do the AVADO and RIBBON1 results provide confirmatory evidence of clinical benefit of bevacizumab in combination with paclitaxel for the initial treatment of MBC?Yes 0 No 13
• Question 4: Should the indication for treatment of MBC be removed from the Avastin label?Yes 12 No 1
FDA December 16, 2010
• Proposal to withdraw marketing approval of the breast cancer indication for bevacizumab.
• Postmarketing trials required as a condition of this approval have failed to verify the clinical benefit.
• Notice of opportunity for a Hearing.

FDA December 16, 2010• Proposal to withdraw marketing approval of
the breast cancer indication for bevacizumab.• Postmarketing trials required as a condition
of this approval have failed to verify the clinical benefit.
• Notice of opportunity for a Hearing
Genentech January 2011• Genentech request for a Notice of
Opportunity for a Hearing

Genentech Public Hearing• Genentech: “Benefit from E2100 study was
demonstrated in the confirmatory trials but of a lesser magnitude. The differences in the study design may have reflected unforeseen limitations in the trial design rather than clear evidence of a lack of clinical benefit”.
• Genentech proposed to conduct a new confirmatory trial of bevacizumab with weekly paclitaxel. One of the endpoints would be to determine biomarkers of outcome.
• Indication should be kept for patients with TNBC as they have less options (Dr. O’Shaughnessy).

TrialBev+ chemo (%)
Chemo alone (%)
∆ PFSfor TNBCPatients(months)
∆ PFSfor allpatients(months)
E2100 122 (33) 110 (31) + 5.3 + 5.9AVADO 58 (23) 52 (22) + 2.0 + 1.9RIBBON-1 (taxane/anthracycline)
96 (23) 46 (22) + 0.3 + 1.2
RIBBON-1 (capecitabine)
87 (21) 50 (24) + 1.9 + 2.9
Adapted from O’Shaughnessy J, et al. Poster P6-12-03. SABCS 2010
Patients with TNBC
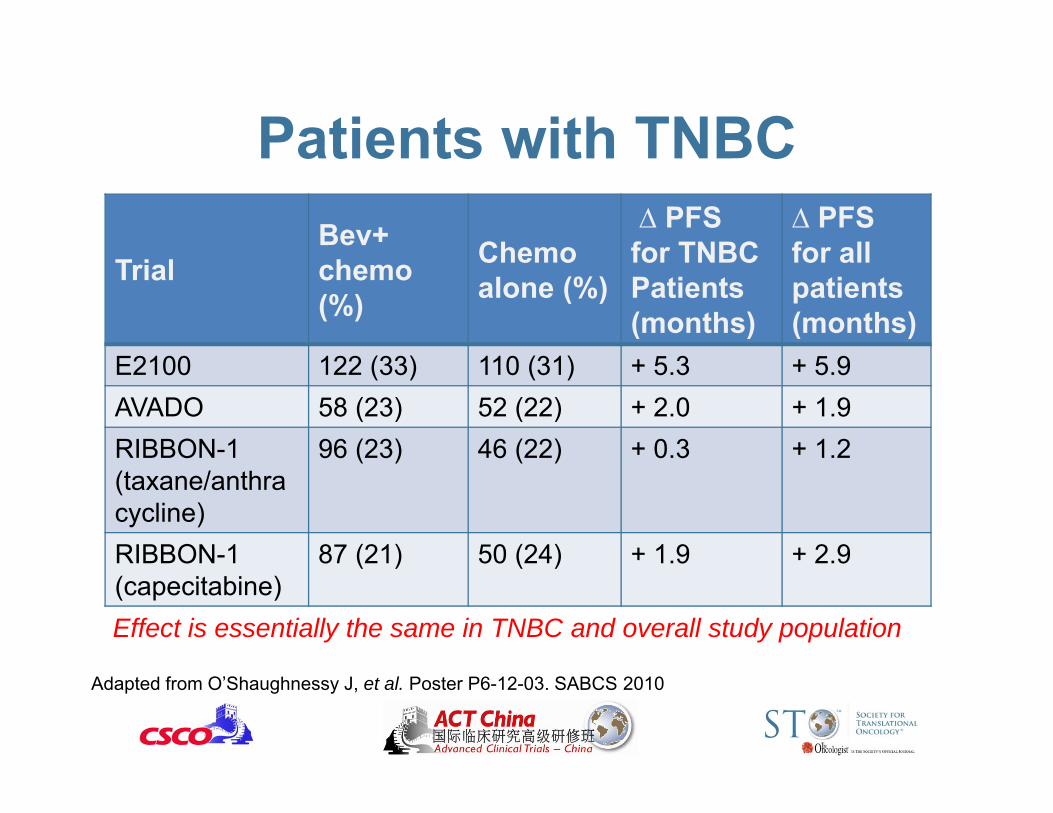
TrialBev+ chemo (%)
Chemo alone (%)
∆ PFSfor TNBCPatients(months)
∆ PFSfor allpatients(months)
E2100 122 (33) 110 (31) + 5.3 + 5.9AVADO 58 (23) 52 (22) + 2.0 + 1.9RIBBON-1 (taxane/anthracycline)
96 (23) 46 (22) + 0.3 + 1.2
RIBBON-1 (capecitabine)
87 (21) 50 (24) + 1.9 + 2.9
Effect is essentially the same in TNBC and overall study population
Patients with TNBC
Adapted from O’Shaughnessy J, et al. Poster P6-12-03. SABCS 2010

ODAC Meeting June 2011 (at the end of Genentech public hearing)
• Question 1: AVADO and RIBBON-1 trials failed to verify the clinical benefit of Avastin for the breast cancer indication?Yes: 6 No: 0
• Question 2: Does the available evidence on Avastin demonstrate that the drug has not been shown to be effective for the breast cancer indication for which it was approved and that Avastin has not been shown to present a clinical benefit that justifies the risk associated with use of the product for this indication?Yes: 6 No: 0

ODAC Meeting June 2011 (at the end of Genentech public hearing)
• Question 3. If the Commissioner agrees with the grounds for withdrawal set out in Issue 1 or Issue 2, should FDA nevertheless continue the approval of the breast cancer indication while the sponsor designs and conducts additional studies intended to verify the drug’s clinical benefit?Yes: 0 No: 6
Milestones of Bevacizumab in MBC
AVF2119g recruitment
opens
E2100 Recruitment
opens
AVADO results presented at
ASCO
AVF2119g results
presented at SABCS
FDA acceleratedapproval for 1st
line in MBC
EMA approval for 1st line in MBC
2001 20032000 2002
ODAC votes against approval for 1st line in MBC
FDA begins process to remove approval in MBC
ODAC votes to withdraw approval
EMA, European Medicines Agency; FDA, Food and Drug Administration; ODAC, Oncologic Drugs Advisory Committee
2004 2005 2006 2007 2008 2009 2010 2011 2012
E2100 results presented at ASCO
Public hearing of Genentech
contest. ODAC votes to withdraw labeling in MBC RIBBON-1
resultspresented at ASCO

QUESTIONS STILL NOT ANSWERED…

Patients with HER-2 positive MBC
• Preclinical studies suggest that VEGF is a downstream target of HER-2 activation and thus patients could benefit from synergism of drugs that act on both targets [1]
• This patient population was rarely included in the previous trials
• Two new studies: – E1105: discontinued due to slow accrual – AVEREL: currently closed, results awaited.
[1] Finkenzeller G, Weindel K, Zimmermann W, et al. Angiogenesis 2004;7:59-68

[1] Miles DW, et al. Cancer Res 2010;70:235s; [2] Yang SX, et al. Clin Cancer Res 2008;14:5893-9; [3] Schneider BP, et al. J Clin Oncol 2008;28:4672-8; [4] Etienne-Grimaldi MC, et al. Br J Clin Pharmacol 2010;71:921-8
Possible Biomarkers of Outcome
• Circulating VEGF concentration [1]• Tumor measurement of VEGF-A [2]• Genetic polymorphisms in components of the
VEGF pathway, particularly VEGF-A polymorphisms – E2100 trial: VEGF-2578AA, VEGF-1154AA
associated with improved OS in the bev group, but not with PFS [3]
– Findings not confirmed in the ATHENA study [4]

“There may be utility of a drug that slows tumor progression but does not prolong survival, but only in one situation: There must also be good evidence that that drug also improves quality of
life, evidence that was lacking for Avastin”
Dr. Wilson, ODAC member – June 2011