beyond p450: pgp transport and cns drug...
TRANSCRIPT
Handout for the Neuroscience Education Institute (NEI) online activity:
Beyond P450: PGP Transport and CNS Drug Response

Objectives
• Analyze the genetics, function, and aliases (!) of the transporter P-glycoprotein
• Assess how PGP affinity is assayed and how to interpret in vivo studies
• Evaluate the literature on PGP–drug interactions
• Compare the clinical literature on PGP polymorphisms and psychotropic drug response
Pretest Question 1
Which of the following statements is true about P-glycoprotein?
1. It functions to import substrates into cells (i.e., influx)2. In humans, it is present only at the blood-brain barrier
(BBB)3. PGP substrates and inhibitors often overlap with those
of cytochrome P450 3A44. Due to its importance at the BBB, there is limited
genetic variation in humans

Case: 55-Year-Old White Man With Treatment-Resistant Depression
Date Amlodipine Aripiprazole Atenolol Clonazepam L-thyroxine Lithium Nortriptyline Omeprazole Prazosin Venlafaxine
03/08/13 5 mg hs 25 mg od 3 mg/d 0.175 mg/d 600 mg hs 100 mg hs 20 mg od 2 mg hs 150 mg od
04/19/13 10 mg hs 25 mg od 3 mg/d 0.175 mg/d 600 mg hs 100 mg hs 20 mg od 2 mg hs 150 mg od
06/14/13 20 mg hs 25 mg od 3 mg/d 0.175 mg/d 600 mg hs 100 mg hs 20 mg od 2 mg hs 150 mg od
11/15/13 20 mg hs 25 mg od 2 mg/d 0.175 mg/d 600 mg hs 100 mg hs 20 mg od 2 mg hs 150 mg od
03/07/14 20 mg hs 25 mg od 1 mg hs 0.250 mg/d D/C 100 mg hs 20 mg od 2 mg hs 75 mg od
07/01/14 20 mg hs 25 mg od 1 mg hs 0.200 mg/d 100 mg hs 20 mg bid D/C 75 mg od
08/08/14 2.5 mg od 20 mg hs D/C 1 mg hs 0.200 mg/d 50 mg hs 20 mg bid 150 mg od
08/22/14 2.5 mg od 10 mg hs 1 mg hs 0.200 mg/d 25 mg hs 20 mg bid 150 mg od
09/19/14 2.5 mg od 7.5 mg hs 1 mg hs 0.200 mg/d D/C 20 mg bid 150 mg od
12/11/14 2.5 mg od 5 mg hs 1 mg hs 0.200 mg/d 20 mg bid 150 mg od
Issue: started complaining of sedation in August 2014Relevant labs TSH values: 02/14/2014: 9.02 (H); 03/20/2014: 12.67 (H);
06/11/2014: <0.05 (L); 07/18/2014: 0.337 (L)
PSYCHOTROPIC DOSE MAY NOT CORRELATE WITH CNS DRUG RESPONSE
3 Variables That Determine Response to Any Drug
Affinity for × Drug concentration × Underlying biologysite of action at site of action of patient
Absorption* GeneticsDistribution AgeMetabolism DiseaseElimination Environment
* Rarely an issue with most psychiatric medications; ziprasidone, lurasidone, and asenapine are the major exceptions
Clinical response is the net result of:
WHAT IS A SIGNIFICANT INTERACTION?Typically ± 50%, but depends on therapeutic index of the victim drug

Example: Factors Influencing Lurasidone Plasma Levels: Food and CYP 3A4 Effects
Potkin SG et al. CNS Spectrums. 2014; 19(2): 176-181.
Impact on LurasidoneExposure Examples
Strong CYP 3A4 inhibitors
Increase lurasidone AUC 9-fold Ketoconazole, clarithromycin, indinavir, nelfinavir, ritonavir
Moderate CYP 3A4inhibitors
Increase lurasidone AUC 2-fold Verapamil, diltiazem, fluconazole, erythromycin,grapefruit juice
Strong CYP 3A4 inducers
Decrease lurasidone AUC 80% Carbamazepine, phenytoin, rifampin
Food 350 Kcal increases lurasidoneAUC 2-fold
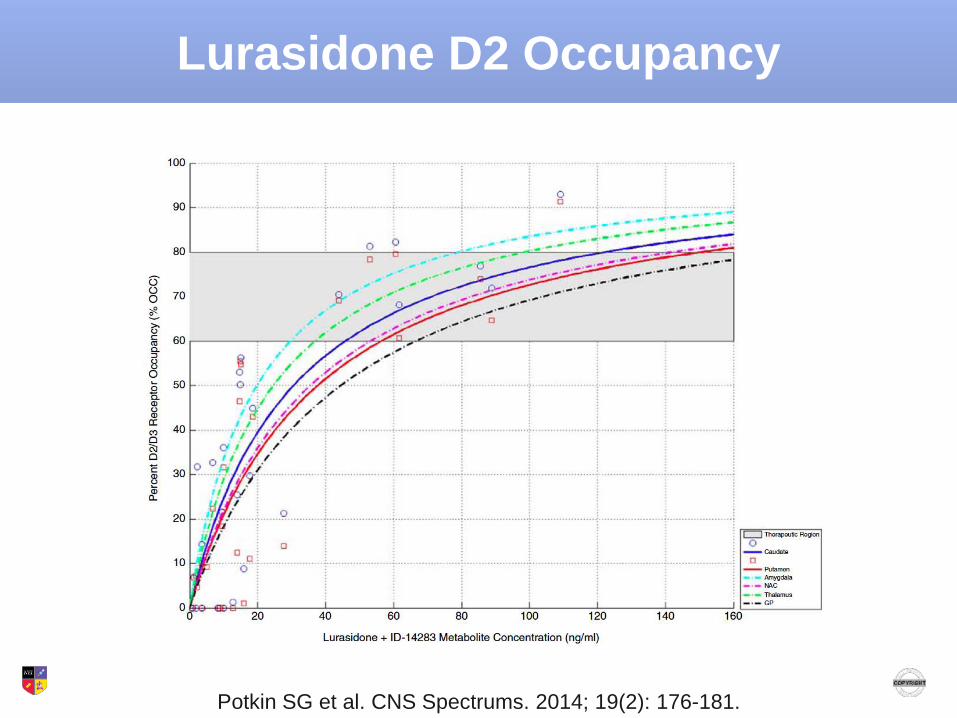
Lurasidone D2 Occupancy
Potkin SG et al. CNS Spectrums. 2014; 19(2): 176-181.
Conclusion from PET Study: D2 occupancy correlates poorly with dose,
but very well with plasma level of the active moiety
Lurasidone D2 Occupancy
Potkin SG et al. CNS Spectrums. 2014; 19(2): 176-181.

Mechanisms Mediating Kinetic Drug Interactions
• Protein binding• Phase I enzymes*
– CYPs and non-CYPs• Phase II enzymes• Nuclear receptors• TRANSPORTERS
– ABC (ATP-binding cassette) transporters (e.g., PGP transporters: efflux)
– OATPs (organic anion transporting polypeptides: influx)
* The main mechanism underlying clinically important DDIs
Levy RH et al. In: Metabolic Drug Interactions. 2000.
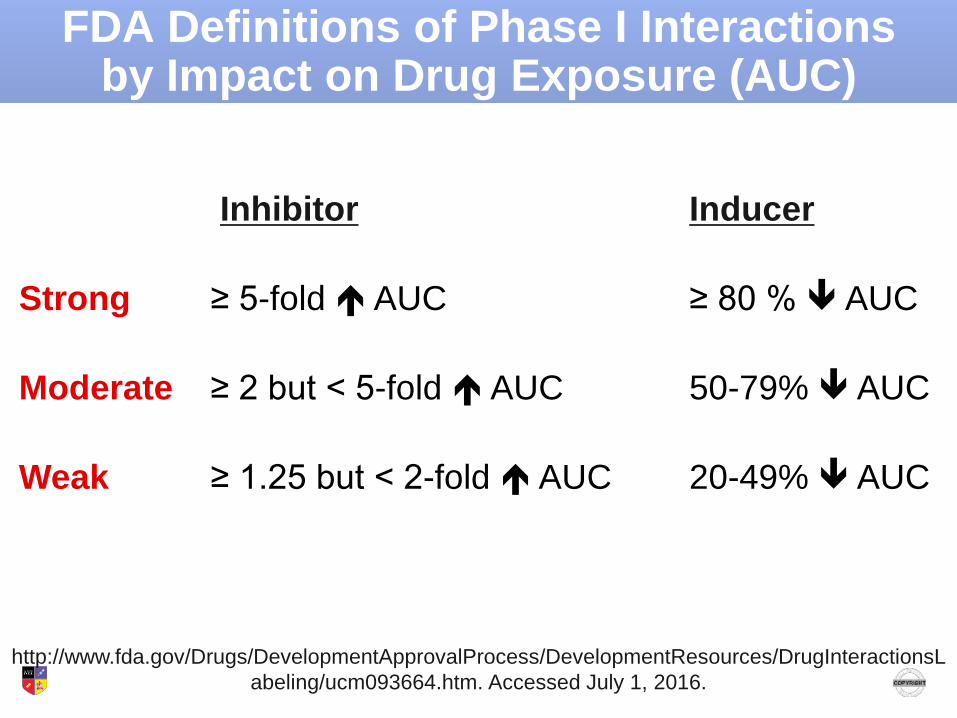
FDA Definitions of Phase I Interactions by Impact on Drug Exposure (AUC)
Inhibitor Inducer
Strong ≥ 5-fold AUC ≥ 80 % AUC
Moderate ≥ 2 but < 5-fold AUC 50-79% AUC
Weak ≥ 1.25 but < 2-fold AUC 20-49% AUC
http://www.fda.gov/Drugs/DevelopmentApprovalProcess/DevelopmentResources/DrugInteractionsLabeling/ucm093664.htm. Accessed July 1, 2016.
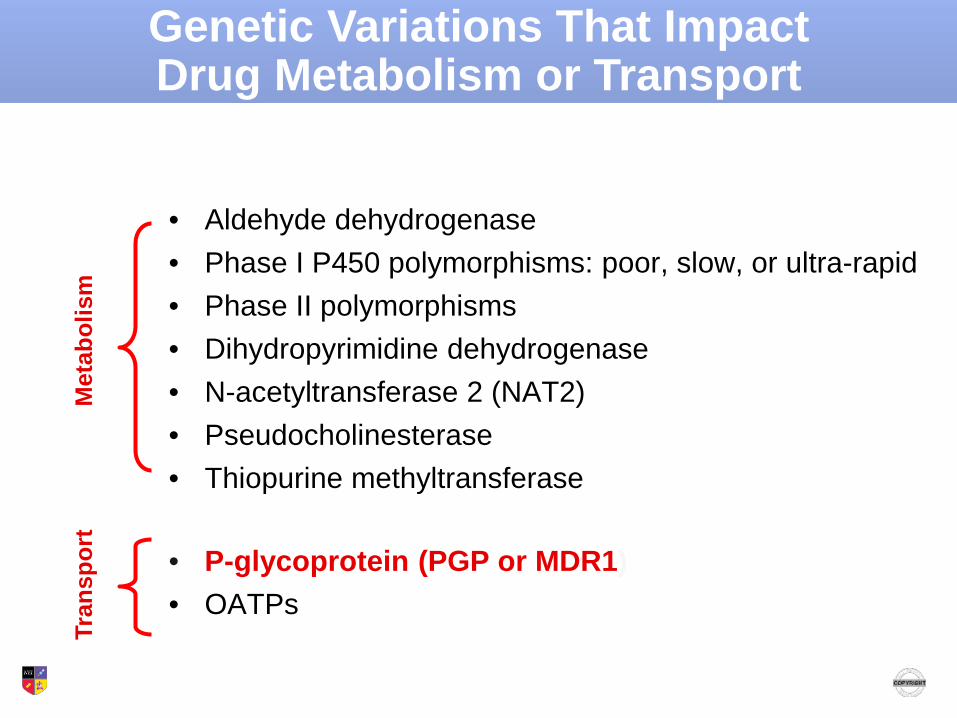
• Aldehyde dehydrogenase• Phase I P450 polymorphisms: poor, slow, or ultra-rapid• Phase II polymorphisms • Dihydropyrimidine dehydrogenase• N-acetyltransferase 2 (NAT2)• Pseudocholinesterase• Thiopurine methyltransferase
• P-glycoprotein (PGP or MDR1)• OATPs
Met
abol
ism
Tran
spor
t
Genetic Variations That Impact Drug Metabolism or Transport

EFFLUX PROTEINS: DISCOVERY AND FUNCTION

Cancer and Drug Resistance
• 1940s: first cancer chemotherapy trials begin
• 1970s: mammalian cells resistant to specific antitumor agents frequently exhibited cross-resistance to drugs dissimilar in structure and mode of action– Multidrug resistance was a major problem in cancer chemotherapy
because it involved resistance to some of the most commonly used anticancer drugs
• 1982: multidrug resistance was shown in most cases to result from decreased intracellular drug accumulation, apparently as a result of alterations in the plasma membrane– In many multidrug-resistant cell lines, the resistance was found to
correlate with overexpression of a 170-kDa membrane glycoprotein
Roninson IB. PNAS 1986;83:4538-42.

A Few Facts About P-glycoprotein (PGP)• 1280 amino acid transmembrane protein whose role is to "bounce" molecules
out of the cell (efflux transporter)• Because of its historical role in chemotherapy resistance, it is also called
multidrug resistance protein 1 (MDR1)• PGP/MDR1 requires ATP to function and is therefore also called ATP-binding
cassette subfamily B member 1; encoded by the ABCB1 gene• Exists at permeability barriers; transports hydrophobic agents back into gut
lumen, bile, and urine (renal proximal tubules) and out of the CNS and gonads
Ozdemir V, Godard B. Psychiatr Times. 2007; 8(8):1051-62.
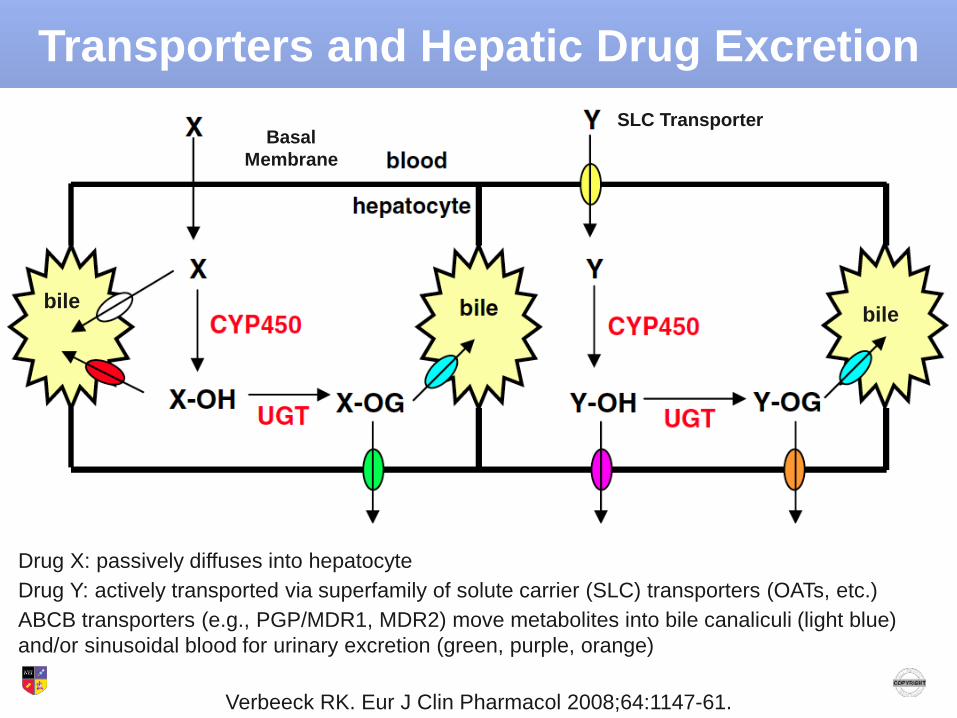
Verbeeck RK. Eur J Clin Pharmacol 2008;64:1147-61.
Drug X: passively diffuses into hepatocyteDrug Y: actively transported via superfamily of solute carrier (SLC) transporters (OATs, etc.)ABCB transporters (e.g., PGP/MDR1, MDR2) move metabolites into bile canaliculi (light blue) and/or sinusoidal blood for urinary excretion (green, purple, orange)
SLC TransporterBasal
Membrane
bilebile
Transporters and Hepatic Drug Excretion
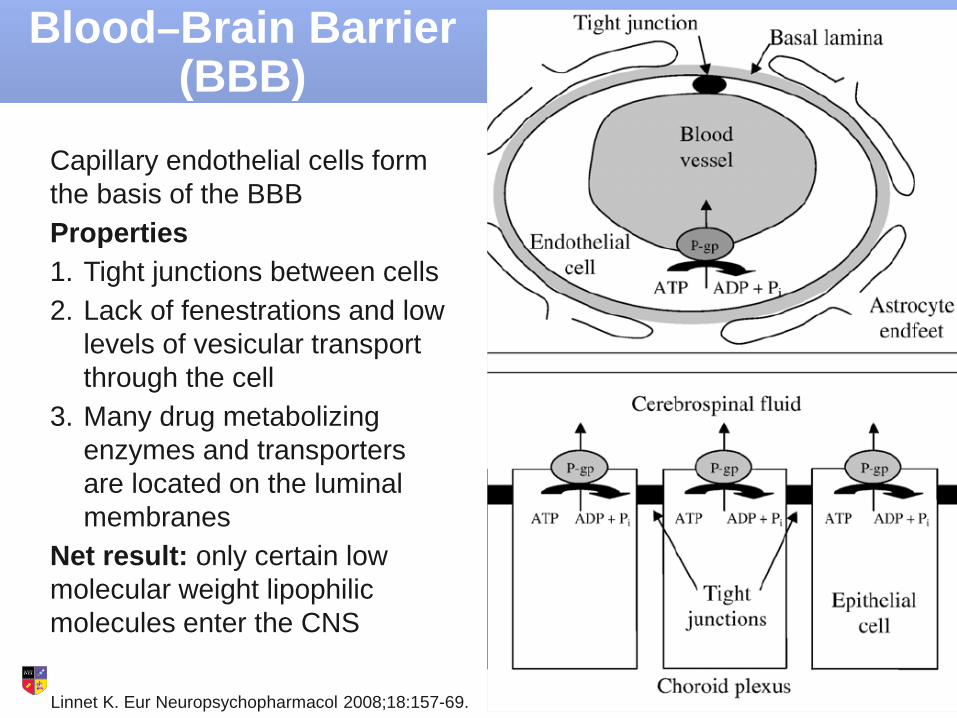
Linnet K. Eur Neuropsychopharmacol 2008;18:157-69.
Capillary endothelial cells form the basis of the BBBProperties1. Tight junctions between cells2. Lack of fenestrations and low
levels of vesicular transport through the cell
3. Many drug metabolizing enzymes and transporters are located on the luminal membranes
Net result: only certain low molecular weight lipophilic molecules enter the CNS
Blood–Brain Barrier (BBB)

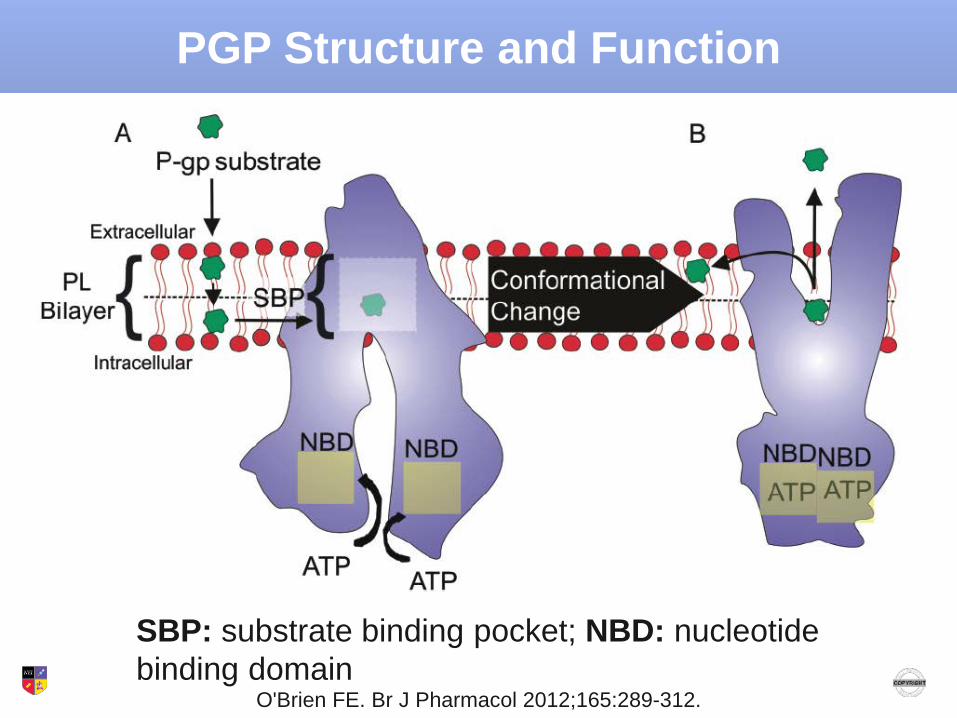
O'Brien FE. Br J Pharmacol 2012;165:289-312.
• PGP/MDR1: encoded by ABCB1
• BCRP: breast cancer resistance protein; encoded by ABCG2
• MRPs: multidrug resistance-associated proteins; encoded by ABCC4 and 5
BBB Efflux Transporters
O'Brien FE. Br J Pharmacol 2012;165:289-312.
SBP: substrate binding pocket; NBD: nucleotide binding domain
PGP Structure and Function

• Binds a wide range of structurally unrelated compounds but prefers hydrophobic molecules
• No obvious chemical structure or characteristic distinguishes substrates with high PGP affinity from those with low PGP affinity
• Significant overlap between substrates of PGP and those of certain cytochrome P450 enzymes, especially 3A4– Net result: drugs that escape PGP might still be metabolized by
enzymes
3 Classes of Interacting Molecules1. Substrates: high affinity for binding site2. Modulators: allosterically modulate PGP to interfere with binding3. Inhibitors: interfere with substrate (or ATP) binding
O'Brien FE. Br J Pharmacol 2012;165:289-312.
PGP Mechanism of Action

PGP Substrates and Inhibitors
O'Brien FE. Br J Pharmacol 2012;165:289-312.

Overlap Between 3A4 and PGP Inhibitors
Wang E. Chem Res Toxicol 2001;14(12):1596-603.
PGP IC50 (μm) 3A4 IC50 (μm)BothCyclosporine A 1.4 4Itraconazole 1.7 1.2Verapamil 4.2 24Carvedilol 4.6 6.83A4 SelectiveNifedipine 113 10PGP SelectiveN-Norverapamil 0.9 62Clarithromycin 4.6 49Fluphenazine 6.5 76

Overlap Between 3A4 and PGP Inducers
Owen A. Br J Clin Pharmacol 2006;62(2):237-42.
• Carbamazepine (CBZ) and rifampin (RIF) are known 3A4 inducers and are thought to share similar properties at PGP– PGP expression was assessed using lymphocytes incubated with
therapeutic concentrations of CBZ and RIF as a positive control; binding to DR-4 elements in the MDR1 promoter region was also assessed
• CBZ increased MDR1 mRNA expression at 6 hrs by 3.7-fold and increased PGP expression at 72 hrs by 7.6-fold
• A 2.1-fold level of increased binding to the DR-4 element was seen with CBZ and was associated with activation of the DR-4 element
• RIF had similar effects in all experiments

PET Imaging of BBB PGP Function
Eyal S. Clin Pharmacol Ther 2010;87(5);579-85.
Method: compare the amount of [11C]-verapamil entering the CNS prior to and during infusion with the potent PGP inhibitor cyclosporine A (CsA)

Distribution of Radioactivity From [11C]-Verapamil Before and During Cyclosporine Infusion
Eyal S. Clin Pharmacol Ther 2010;87(5);579-85.
before during
PSYCHOTROPIC PGP AFFINITY
In Vitro Methods for Calculating PGP Affinity for Psychotropics
• Use of tissues rich in PGP (e.g., placenta)• High throughput assays that examine ATP hydrolysis in PGP-
containing membranes• Issue: the data often did not correlate with findings in animal
models• Gold standard: cell lines to examine bidirectional transport
across a cellular monolayer – Caco-2 cell line derived from human epithelial colorectal adenocarcinoma cells
that express PGP
– Madin-Darby canine kidney cells that can be stably transfected to express PGP
• Cell lines can be used with PGP inhibitors to examine affinity and with known substrates to study PGP inhibitors– Problems: labor intensive, time consuming
Doran A et al. Drug Metab Dispos 2005;33:165-74; Rahi M. J Psychopharmacol 2007;21(7):751-6.

In Vivo Models for Calculating PGP BBB Interactions
• Avoids problems related to passive diffusion that can occur in vitro due to use of high drug concentrations
• Mice have 2 analogous genes (abcb1a and abcb1b) that have similar distribution and substrate specificity to human PGP
Method: use normal (wild-type) and PGP knockout mice and look at differences in CNS drug penetration• At several time points after IV infusion, the brain (or CSF)
concentration/serum concentration ratio is calculated for wild-type (WT) mice
• Using the same method, the brain/serum ratio is calculated for PGP knockout (KO) mice (also known as abcb1ab -/-)
• The 2 ratios are divided: KO/WT – Values ~1.0 imply no PGP effect on CNS drug penetration
Karlsson L. Eur Neuropsychopharmacol 2010;20:632-40.
Limitations of Knockout Mouse Models
• Mice have different distributions of other transporters than humans
• The abcb1ab knockout may result in the upregulation of other transporters
• Studies are done with single IV infusions and do not test the effects of chronic exposure, which better mimics the clinical use of psychotropics
O'Brien FE. Br J Pharmacol 2012;165:289-312.

Calculating PGP Affinity for Venlafaxine (VEN) and O-Desmethylvenlafaxine (ODM)
Karlsson L. Eur Neuropsychopharmacol 2010;20:632-40.
ABCB1ab (+/+) WT(nmol/L)
ABCB1ab (-/-) KO(nmol/L)
KO/WT Ratio
Brain Serum B/S Ratio Brain Serum B/S Ratio
VEN 1 hr 3731 918 4.06 8797 983 8.95 2.20
VEN 3 hr 266 61.7 4.29 837 113 7.41 1.73
VEN 9 hr 9.1 2.3 3.96 10.0 2.1 4.76 1.20
Value reported in literature for VEN AUC 1.80
ODM 1 hr 169 97.5 1.73 421 108 3.90 2.25
ODM 3 hr 73.5 14.7 5.00 295 24.5 12.04 2.41
ODM 9 hr 7.9 1.5 5.27 49.3 3.1 15.9 3.02
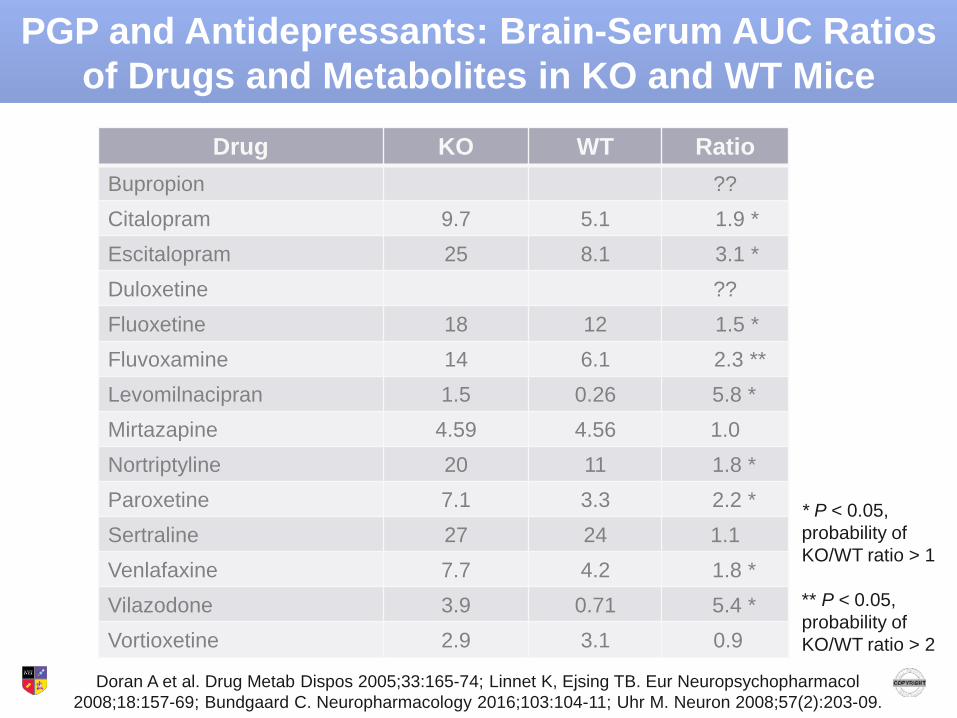
Drug KO WT RatioBupropion ??Citalopram 9.7 5.1 1.9 *Escitalopram 25 8.1 3.1 *Duloxetine ??Fluoxetine 18 12 1.5 *Fluvoxamine 14 6.1 2.3 **Levomilnacipran 1.5 0.26 5.8 *Mirtazapine 4.59 4.56 1.0Nortriptyline 20 11 1.8 *Paroxetine 7.1 3.3 2.2 *Sertraline 27 24 1.1Venlafaxine 7.7 4.2 1.8 *Vilazodone 3.9 0.71 5.4 *Vortioxetine 2.9 3.1 0.9
Doran A et al. Drug Metab Dispos 2005;33:165-74; Linnet K, Ejsing TB. Eur Neuropsychopharmacol2008;18:157-69; Bundgaard C. Neuropharmacology 2016;103:104-11; Uhr M. Neuron 2008;57(2):203-09.
* P < 0.05, probability of KO/WT ratio > 1
** P < 0.05, probability of KO/WT ratio > 2
PGP and Antidepressants: Brain-Serum AUC Ratios of Drugs and Metabolites in KO and WT Mice
The Mystery of Sertraline
• KO/WT ratio 1.1; however, using in vitro assays, sertraline and its metabolite have high PGP affinity1
• Sertraline increases the brain AUC of risperidone and 9-OH risperidone 1.5-fold (P < 0.05) and 5-fold (P < 0.01), respectively2
• Question: is sertraline a PGP inhibitor?
1. Wang JS. Biol Pharm Bull 2008;31(2):231-4.2. Wang JS. Psychopharmacology (Berl) 2006;183(4):490-9.

Drug KO WT Ratio
Aripiprazole 7.46 2.44 3.1 **Dehydroaripiprazole 6.16 1.47 4.2 **Chlorpromazine 29 23 1.3 *Clozapine 6.6 4.1 1.6 *Haloperidol 18 13 1.4 *Olanzapine 2.0 0.9 2.6 *Risperidone 8.0 0.78 10 **9-OH Risperidone 1.0 0.06 17 **
Doran A et al. Drug Metab Dispos 2005;33:165-74; Kirschbaum KM et al. Neuropharmacology 2010;59:474-9; Linnet K, Ejsing TB. Eur Neuropsychopharmacol 2008;18:157-69.
* P < 0.05, probability of KO/WT ratio > 1** P < 0.05, probability of KO/WT ratio > 2
PGP and Antipsychotics: Brain-Serum AUC Ratios of Drugs and Metabolites in KO and WT Mice

Case: 55-Year-Old White Man With Treatment-Resistant Depression
Date Amlodipine Aripiprazole Atenolol Clonazepam L-thyroxine Lithium Nortriptyline Omeprazole Prazosin Venlafaxine
03/08/13 5 mg hs 25 mg od 3 mg/d 0.175 mg/d 600 mg hs 100 mg hs 20 mg od 2 mg hs 150 mg od
04/19/13 10 mg hs 25 mg od 3 mg/d 0.175 mg/d 600 mg hs 100 mg hs 20 mg od 2 mg hs 150 mg od
06/14/13 20 mg hs 25 mg od 3 mg/d 0.175 mg/d 600 mg hs 100 mg hs 20 mg od 2 mg hs 150 mg od
11/15/13 20 mg hs 25 mg od 2 mg/d 0.175 mg/d 600 mg hs 100 mg hs 20 mg od 2 mg hs 150 mg od
03/07/14 20 mg hs 25 mg od 1 mg hs 0.250 mg/d D/C 100 mg hs 20 mg od 2 mg hs 75 mg od
07/01/14 20 mg hs 25 mg od 1 mg hs 0.200 mg/d 100 mg hs 20 mg bid D/C 75 mg od
08/08/14 2.5 mg od 20 mg hs D/C 1 mg hs 0.200 mg/d 50 mg hs 20 mg bid 150 mg od
08/22/14 2.5 mg od 10 mg hs 1 mg hs 0.200 mg/d 25 mg hs 20 mg bid 150 mg od
09/19/14 2.5 mg od 7.5 mg hs 1 mg hs 0.200 mg/d D/C 20 mg bid 150 mg od
12/11/14 2.5 mg od 5 mg hs 1 mg hs 0.200 mg/d 20 mg bid 150 mg od
Issue: started complaining of sedation in August 2014Relevant labs TSH values: 02/14/2014: 9.02 (H); 03/20/2014: 12.67 (H);
06/11/2014: <0.05 (L); 07/18/2014: 0.337 (L)

PGP and Omeprazole
• Inhibits PGP using in vitro cell lines with the IC50value of 17.7 μmol/L
• In extensive metabolizers of CYP2C19, the 20-mg dose will result in maximum plasma levels of 1.5–3.5 μmol/L
• However, the use of higher doses might result in levels much closer to the IC50 values
Pauli-Magnus C. Naunyn-Schmiedeberg's Arch Pharmacol 2001;364:551-7.
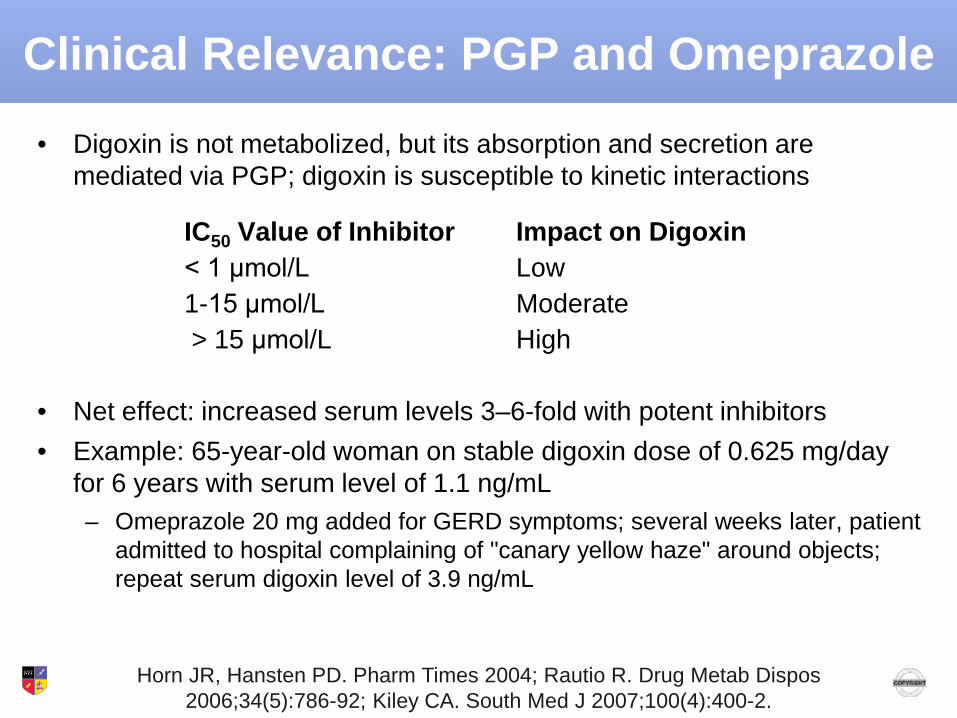
Clinical Relevance: PGP and Omeprazole• Digoxin is not metabolized, but its absorption and secretion are
mediated via PGP; digoxin is susceptible to kinetic interactions
IC50 Value of Inhibitor Impact on Digoxin< 1 μmol/L Low1-15 μmol/L Moderate> 15 μmol/L High
• Net effect: increased serum levels 3–6-fold with potent inhibitors• Example: 65-year-old woman on stable digoxin dose of 0.625 mg/day
for 6 years with serum level of 1.1 ng/mL– Omeprazole 20 mg added for GERD symptoms; several weeks later, patient
admitted to hospital complaining of "canary yellow haze" around objects; repeat serum digoxin level of 3.9 ng/mL
Horn JR, Hansten PD. Pharm Times 2004; Rautio R. Drug Metab Dispos2006;34(5):786-92; Kiley CA. South Med J 2007;100(4):400-2.

Pretest Question 2
Individuals who have genetic polymorphisms associated with decreased PGP expression or function have demonstrated in clinical studies increased response to which of the following psychotropics?
1. 3-OH benzodiazepines (lorazepam, oxazepam)2. Citalopram3. Olanzapine4. 1 and 35. 2 and 36. 1, 2, and 3

CLINICAL ISSUES: GENETICS AND RESPONSE
PGP Genetics
• Product of the polymorphic ABCB1 gene (ATP-binding cassette subfamily B member 1, also known as the MDR1 gene), located on chromosome 7q21
• Strong overlap with 3A4 in terms of genetics (also encoded on ch 7) and locations
– Promoter binding elements that result in induction of expression have common substrates (e.g., rifampin)
Lin Y-C et al. Therapeutic Drug Monitoring 2006;28(5):668-72.

PGP Polymorphisms
• Several single nucleotide polymorphisms (SNPs) linked to PGP expression and function – rs2032582 G>T variant: 40% (G2677T)
G>A variant: 3% (G2677A) • Located in the exon, results in a change of alanine to
threonine– rs2032583 T>C variant: 12%– rs2235015 G>T variant: 18%– rs1128503 C>T variant: 46% (C1236T) – rs1045642 C>T variant: 50% (C3435T)– rs10245483 G>T variant: 47%
Lin Y-C et al. Therapeutic Drug Monitoring 2006;28(5):668-72;Breitenstein B. J Psychiatr Res 2016;73:86-95.
Intr
onic
Retrospective Study: Impact of PGP Polymorphisms on Antidepressant Response
Methods• Retrospective analysis of data on 1,257 antidepressant
users with known ABCB1 genotypes (rs1128503 C/T, rs2032582 G/T, rs1045642 C/T) in the population-based Rotterdam Study of health outcomes
Results• In a model adjusted for age and gender, homozygotes of the
more functional, wild-type allele (T/T at each allele) had an increased risk of switching (OR 4.22; 95% CI 1.30–13.7; P = 0.017) and discontinuation (OR 1.47; 95% CI 0.98–2.22; P = 0.063)
Noordam R. J Clin Psychopharmacol 2013;33(4):546-50.

PGP Polymorphisms and Remission
Methods• 133 adults with unipolar MDD were genotyped for various PGP
SNPs; remission rates were examined based on 2 factors:– Whether the patients were treated with a PGP substrate
(citalopram, paroxetine, amitriptyline, venlafaxine) or nonsubstrate (mirtazapine)
– Whether those treated with PGP substrates had functional PGP polymorphisms
Results• For those on non-PGP substrates, there was no difference in
the genotype distribution between remitters and nonremitters• In the group of patients with PGP genetic variations, the
corrected P value over all SNPs was 0.00016 for remission
Uhr M. Neuron 2008;57:203-9.

Non-remission Rates for Those on PGP Substrates Based on rs2032583 Allele
Uhr M. Neuron 2008;57:203-9.
Non
-rem
issi
on %
Impact of PGP Polymorphisms on Antidepressant Dose and Remission
Methods• 113 adults with unipolar MDD were treated with escitalopram or
venlafaxine for 8 weeks; response rates were analyzed based on the presence of 1 PGP SNP (rs1045642)– P450 status and 5HTTLPR (5HT transporter-linked promoter region)
genotype were controlled for
ResultsEscitalopram: carriers of rs1045642 TT needed mean 11 mg to remit, whereas TC and CC carriers required 24 mg and 19 mg, respectively (P < 0.0001)Venlafaxine: 73.3% of TT carriers remitted compared to 12.5% of CC carriers (odds ratio: 6.69; 95% confidence interval: 1.72–25.9, P < 0.006)
Singh AB. Translational Psychiatry 2012;2:e198.

Impact of PGP Polymorphisms on Antidepressant Response
Methods• Genotyped 10 ABCB1 SNPs in 683 patients with MDD treated for at
least 2 weeks; 576 patients completed 8 weeks of treatment with escitalopram, sertraline, or venlafaxine XR
Schatzberg AF. Am J Psychiatry 2015;172(8):751-9.

PGP Polymorphisms and Antidepressant Response
Results• rs10245483 status was associated with outcome; T alleles PGP function
– GG (common) homozygotes responded better and had fewer side effects with escitalopram and sertraline
– TT homozygotes responded better and had fewer side effects with venlafaxine (unexpected)
Schatzberg AF. Am J Psychiatry 2015;172(8):751-9.
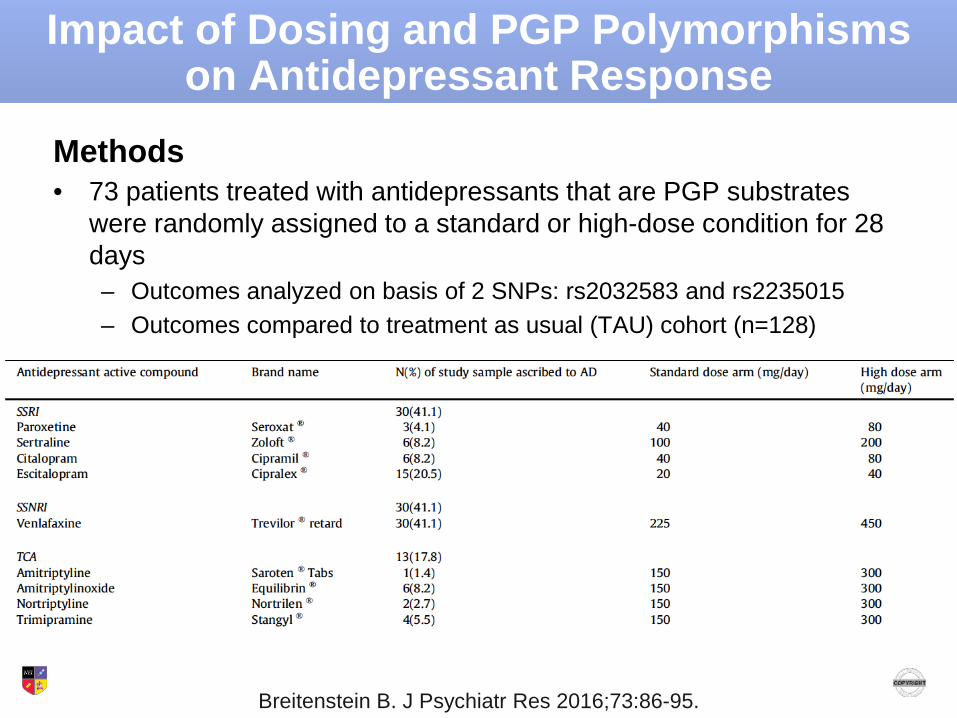
Impact of Dosing and PGP Polymorphisms on Antidepressant Response
Methods• 73 patients treated with antidepressants that are PGP substrates
were randomly assigned to a standard or high-dose condition for 28 days– Outcomes analyzed on basis of 2 SNPs: rs2032583 and rs2235015– Outcomes compared to treatment as usual (TAU) cohort (n=128)
Breitenstein B. J Psychiatr Res 2016;73:86-95.
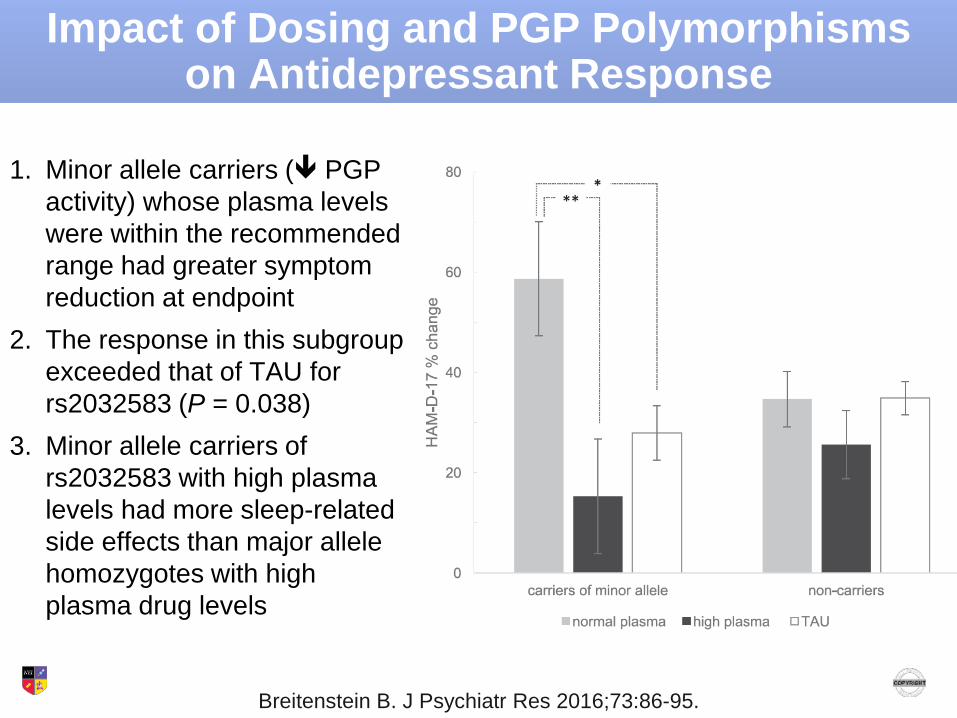
Impact of Dosing and PGP Polymorphisms on Antidepressant Response
1. Minor allele carriers ( PGP activity) whose plasma levels were within the recommended range had greater symptom reduction at endpoint
2. The response in this subgroup exceeded that of TAU for rs2032583 (P = 0.038)
3. Minor allele carriers of rs2032583 with high plasma levels had more sleep-related side effects than major allele homozygotes with high plasma drug levels
Breitenstein B. J Psychiatr Res 2016;73:86-95.

Using PGP Polymorphisms to Tailor Antidepressant Therapy
2 cases of patients who were TT homozygotes at the PGP SNP rs2032583; TT is associated with decreased likelihood of response; C alleles are associated with greater response• Case 1: 2D6 extensive metabolizer who failed to respond
to 375 mg/day venlafaxine – Plasma levels: VEN 655 ng/mL; ODM 420 ng/mL (lab ref ranges: VEN
200–400 ng/mL; ODM 200–400 ng/mL)– Dose increased to 600 mg with response; dose tolerated by patient
• Case 2: 2D6 extensive metabolizer who failed to respond to venlafaxine with plasma levels of VEN 385 ng/mL and ODM 320 ng/mL – Because this patient was experiencing sexual side effects, the decision
was made to try meds with limited PGP affinity; patient responded to the combination of bupropion + mirtazapine
Rosenhagen M. J Clin Psychopharmacol 2010;30(2):209-10.

Impact of PGP Polymorphisms on Antipsychotic Response
Olanzapine trial with outcomes analyzed based on the PGP rs1045642 SNP (also known as 3435 C>T)
• For carriers of at least 1 T allele, the plasma olanzapine level was positively associated with percent change in BPRS score (P = 0.02)
• This relationship was not seen in the group of CC homozygotes (P = 0.583)
Lin Y-C et al. Therapeutic Drug Monitoring 2006;28(5):668-72.
• The goal of psychopharmacology is effective drug concentrations in the CNS
• PGP not only mediates drug absorption and excretion, but also plays an important role at the blood-brain barrier
• Our understanding of PGP corresponds to developments in the cytochrome P450 literature– Improved characterization of PGP in vivo affinities and the
impact of inhibitors or modulators– Better definition of the relationship between genetic
variations and drug outcomes– Hope: better genetic predictors of treatment outcomes
Summary
Resources
• Understanding SNP terminologyhttp://www.snpedia.com/index.php/SNPedia
• Understanding the differences between in vitro and in vivo data on psychotropicsO'Brien FE et al. Interactions between antidepressants and P-glycoprotein at the blood–brain barrier: clinical significance of in vitro and in vivo findings. Br J Pharmacol 2012;165:289-312.
• PGP psychotropic table: KO/WT values Linnet K, Ejsing TB. A review of the impact of P-glycoprotein on the penetration of drugs into the brain. Focus on psychotropic drugs. Eur Neuropsychopharmacol 2008;18:157-69.