beyond the basics: the art and science of tracing ... 3- july 25.pdf · { resume oxytocin at half...
TRANSCRIPT

Beyond the Basics: The Art and Science of Tracing Interpretation
Session 3:
July 25, 2018
2018 Fetal Monitoring Lunch & Learn Series

Wisconsin Association for Perinatal Care (WAPC)

Planners
• Sara Bronson, MSN, RN, CNL
• Julie Bulgrin, BSN, RNC-OB, C-EFM
• Eva Fassbinder Brummel, MPH
• Ann E. Conway, MS, MPA, RN
• Anne Kuschel, RN, BSN
• Janice McIntosh, BSN, RNC-OB, C-EFM
• Jeanne Rosendale, MSN, RNC-Inpatient OB, C-EFM
• Chris Van Mullem, MS, RNC, C-EFM
No conflicts to disclose.
3

Faculty
Sara Bronson, MSN, RN, CNL
Nursing Practice Specialist
ThedaCare Regional Medical Center
Appleton, Berlin, Neenah, New London,
Shawano, Waupaca, WI
4

Notice of disclosures
• Notice of requirements for successful completion – Registrants must attend full session and complete evaluation to receive
contact hours
• Conflicts of Interest – None to report
• Financial Disclosures – None
• Sponsorship or commercial support – None
• Non-endorsement of products – The speaker does not endorse the use of any particular medications or
products as part of this educational session
• Off-label use – The speaker may discuss the off-label use of misoprostol and terbutaline as
they relate to labor and delivery.
5

Before we begin…
• Listen-only mode • Questions – please ask, please answer!
– Raise your hand – Type into the Question Pane – Out of time? Email [email protected]
• Technical problems: Call Jenee Jerome/Barb
Wienholtz at 608-285-5858, ext. 201
6

Before we begin… The content presented today is a case study. Components of this case were chosen based on their applicability to achieve learning objectives for this presentation. Do not assume the patient featured in the case was cared for by the instructor or at the facility at which the instructor is employed. The discussion will focus on interpretation of the electronic fetal monitoring (EFM) tracings for the purpose of education. At times, the discussion may lead to the care decisions made based on EFM interpretation. IF the instructor shares details regarding actual or potential care decisions, please note those decisions do not necessarily reflect the opinions of the instructor, a particular provider, the standard of care for any particular institution or facility, or of WAPC.
7

Objectives
At the conclusion of the session, participants will be able to:
1. Systematically review the fetal monitoring data to identify the fetal heart rate pattern classification (category).
2. Discuss interventions/management of the fetal heart rate patterns based on their pathophysiology.
8
Learning Outcome
• Identify required actions correctly to manage patients with abnormal fetal heart rate patterns.
9

2008 NICHD Report The 2008 National Institute of Child Health
and Human Development (NICHD)
Report of Fetal Heart Rate Monitoring
• Defined standard fetal heart rate nomenclature
• Identified three categories for fetal heart rate interpretation
• Proposed future research
10

2008 NICHD Report
• Report endorsed by:
– ACOG (2009) Practice Bulletin #106 "Intrapartum Fetal Heart Rate Monitoring: Nomenclature, Interpretation and General Management Principles”
– AWHONN-endorsed and incorporated in fetal monitoring
curriculum – American College of Nurse Midwives – American Academy of Family Practice
American College of Obstetricians and Gynecologists (2009, July). ACOG Practice Bulletin #106: Intrapartum Fetal Heart Rate Monitoring: Nomenclature, Interpretation, and General Management Principles. Washington, D.C.: Author
11

ACOG Practice Bulletin #116 (2010)
"Management of Intrapartum Fetal Heart Rate Tracings"
• Reviewed: – Nomenclature – Fetal Heart Rate Interpretation (categories)
• Provided framework for evaluation and management of intrapartum patterns based on categories
• Assessment algorithm for fetal heart rate patterns
• Intrapartum resuscitative measures
• Management of uterine tachysystole American College of Obstetricians and Gynecologists (2009, July). ACOG Practice Bulletin #106: Intrapartum Fetal Heart Rate Monitoring: Nomenclature, Interpretation, and General Management Principles. Washington, D.C.: Author
12

Systematic Review of Case Studies
The following questions are used to evaluate every tracing, followed by specific questions:
1. What is the contraction pattern? (interval,
duration, resting tone if appropriate) 2. What is the baseline fetal heart rate? 3. What is the baseline variability? 4. Are there any periodic changes present? 5. Are there any episodic changes present? 6. What are the probable causes of the changes
present? 7. When was the last time there was either moderate
variability or an acceleration?
13

Strip Review Discussion
• Interpretation
• Interventions/Communication
• Documentation in chart
14

Intervention/Communication
• SBAR
– Situation
– Background
– Assessment
– Recommendation
15

Case #1

Case history
• 26 years old
• G1P0
• 37 + 5 days
• Presented with SROM
• GBS –
• Prenatal course uncomplicated, no risk factors
• NKDA

Tracing 1

Tracing 2
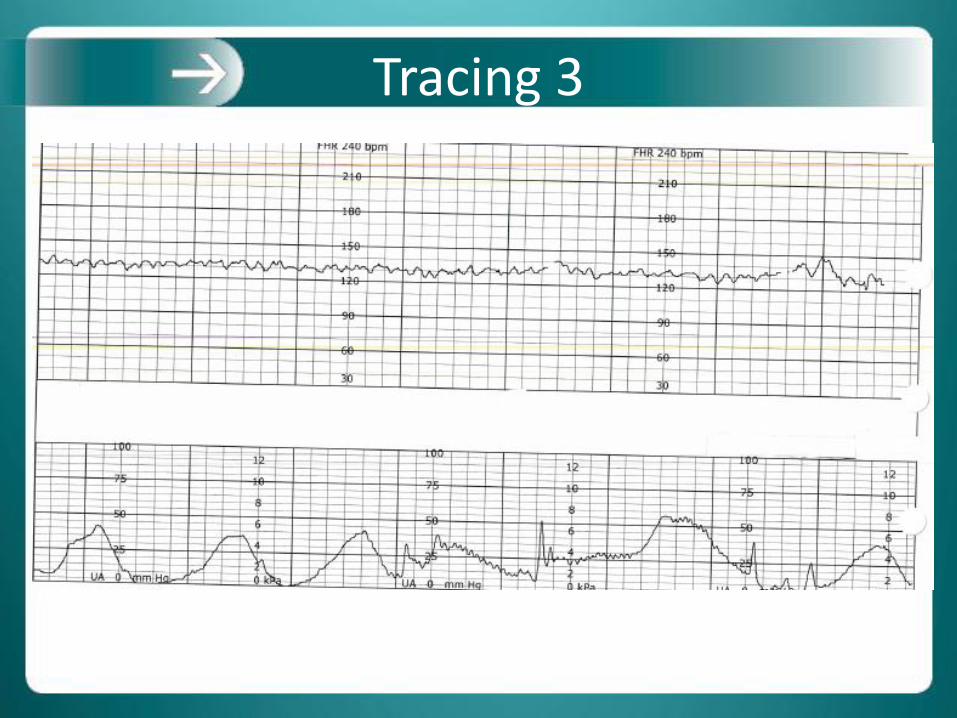
Tracing 3

Poll question #1
When asked to increase oxytocin for a patient with tachysystole, an appropriate response from the nurse is to: a) Increase the oxytocin because there is an
acceleration in the fetal heart rate b) Refuse to increase the oxytocin c) Collaborate with the provider about fetal
oxygenation and potential hypoxia and discuss decreasing the oxytocin.
d) Call another provider to get their opinion about this.

Tachysystole Algorithm Tachysystole: > 5 contractions in a 10 minute period, averaged over 30 minutes. Tachysystole is further qualified by the presence
or absence of associated FHT decelerations
OXYTOCIN-INDUCED TACHYSYSTOLE Category I FHR
Give IV fluid bolus of 500ml Lactated Ringer's solution unless fluid restricted
If tachysystole has not resolved in 15 minutes, decrease oxytocin rate by half
Notify Provider
If tachysystole has not resolved in 15 more minutes, discontinue oxytocin until uterine
activity is less than 6 contractions in 10 minutes
If oxytocin has been discontinued for less than 30 minutes, you have a category I FHR tracing, and no tachysystole:
• Resume oxytocin at half the rate that caused the tachysystole and increase per orders
If the oxytocin is discontinued for more than 30 minutes:
•Resume oxytocin at the initial dose ordered and increase per orders.
OXYTOCIN-INDUCED TACHYSYSTOLE Category II or III FHR
Discontinue oxytocin
Assist the mother to a lateral position
Give IV fluid bolus of 500ml Lactated Ringer's solution if not fluid restricted
Administer oxygen at 10L/min via mask (discontinue as soon as posisible based on the
FHR pattern)
Notify provider
If no response, consider 0.25 mg terbutaline SQ per provider order
If oxytocin has been discontinued for less than 30 minutes, you have a category 1 FHR tracing, and no tachysystole:
• Resume oxytocin at half the rate that caused the tachysystole and increase per orders
If the oxytocin is discontinued for more than 30 minutes:
•Resume oxytocin at the initial dose ordered and increase per orders.

Tracing 4

Tracing 5

Poll question #2
Which of the following statements given during an SBAR reflect assessment (the A in SBAR)?
a) “The fetal heart rate tracing is indeterminate and do not resolve with position change”
b) “I have turned her from side to side and the decelerations continue”
c) “I need you to come to the bedside”
d) “The baseline FHR is 120”

Tracing 6 and 7

Poll question #3
The indication for an amnio-infusion is particulate meconium.
a) True
b) False

Case 1 Outcome
• Apgars 2/4/7/8
• The baby required 4 minutes of PPV
• Cord pH 7.1
• Baby did well and was discharged to home on Day 3

Case #2

Case history #2
• 38 years old
• G4P1
• 38 +4 days
• Admitted for decreased fetal movement
• GBS –
• Pregnancy complicated by gestational diabetes and preeclampsia without severe features
• NKDA

Tracing 8

Tracing 9

Tracing 10
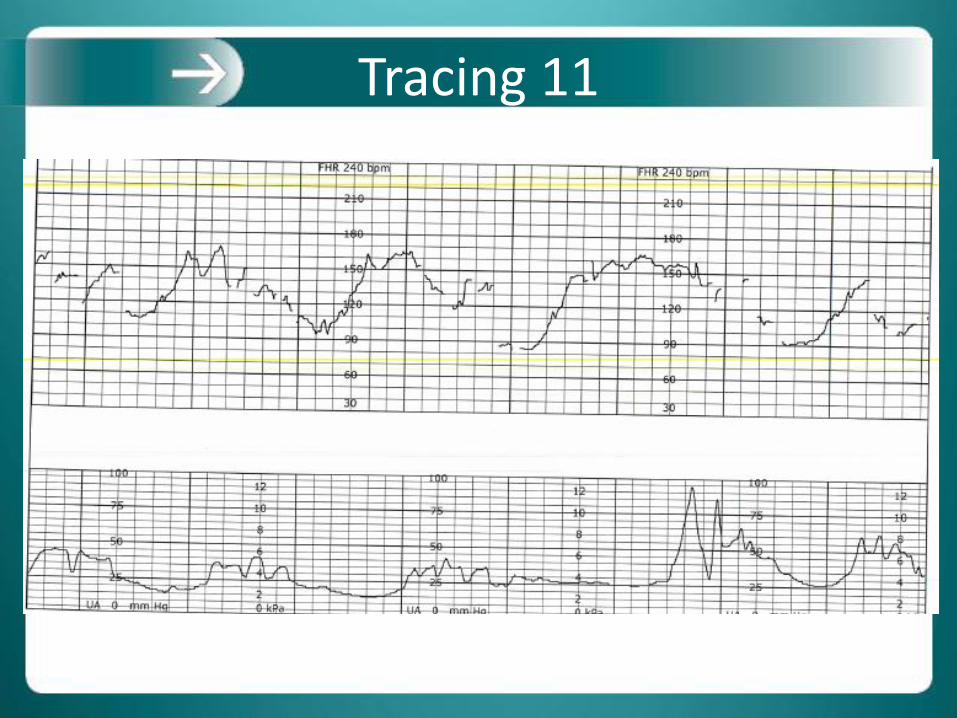
Tracing 11

Poll Question #4
Which of the following can result in the production of oxygen- free radicals in the newborn?
a) Hypoxia
b) Hyperoxia
c) Both hypoxia and hyperoxia
d) Neither hypoxia and hyperoxia

Tracing 12

Tracing 13

Tracing 14

Tracing 15

Tracing 16

Tracing 17

Poll question #5
Which of the following along with temperature is part of the diagnosis of an intra-amniotic infection?
a) Minimal variability
b) Prolonged decelerations
c) Fetal tachycardia

Tracing 18

Tracing 19

Tracing 20

Poll Question #6
What Category is this tracing?
a) Category 1
b) Category 2
c) Category 3
Poll question #7
Guess the Agars
a) 1/3/5
b) 1/1/4
c) 2/5/6
d) 3/4/5

Case 2 Outcome
• Baby to NICU for intraamniotic infection
• Home with family at 2 weeks and is doing well
References
ACOG Committee Opinion Number 712. (2017, August). Intrapartum management of intraamniotic infection. AWHONN Maternal Fetal Triage Index Miller, L., Miller, D., Cypher, R. (2017). Mosby’s pocket guide to fetal monitoring: A multidisciplinary approach. Elsevier: St. Louis. Pettker, C.M. & Funai, E.F. (2014) Patient Safety in Obstetrics from Creasy and Resnik's Maternal-Fetal Medicine: Principles and Practice, 49, 785-794.e3 Raghuraman, N., Temming, L.A., Stout, M.J., Macones, g.A., Cahill, A;G., Tuuli, M.G. (2017). Intrauterine hyperoxemia and riks of neonatal morbidity. Obstetrics & Gynecology, 0 (0), pp. 1-6.

Discussion
Questions?
Comments?

Remember
• Fax or email attendance list to WAPC – fax: 608-285-5004
– email: [email protected]
• Evaluation will be sent via email from WAPC. Please complete to receive Continuing Education Credit.
• Continuing Education Certificate will be sent via email upon completion of evaluation.
• Archived version
• Become a member of WAPC! Join online: https://www.perinatalweb.org/n-pay/membership.asp
• Don’t miss the next session: September 27, 2018

Thank-you