beyond the threshold: an etiological bridge between hypoxia and immunity in preeclampsia
TRANSCRIPT
Journal of Reproductive Immunology 85 (2010) 112–116
Contents lists available at ScienceDirect
Journal of Reproductive Immunology
journa l homepage: www.e lsev ier .com/ locate / j repr imm
Review
Beyond the threshold: an etiological bridge between hypoxia andimmunity in preeclampsia
Surendra Sharma ∗, Wendy E. Norris, Satyan KalkunteDepartment of Pediatrics, Women and Infants Hospital-Warren Alpert Medical School of Brown University, Providence, RI, USA
a r t i c l e i n f o
Article history:Received 10 September 2009Received in revised form 15 January 2010Accepted 22 January 2010
Keywords:PreeclampsiaHypoxiaIL-10 deficiencyAngiogenesisApoptosis
a b s t r a c t
Taking a cue from the recent workshop ‘Preeclampsia—A Pressing Problem’ sponsoredby the National Institutes of Child Health and Human Development, this review articletakes a fresh look at hypoxia and a dysfunctional immune system as the key contributorsto the etiology of preeclampsia and the mechanisms involved therein. In the context ofepidemiological research on the intricate and multifactorial nature of preeclampsia, wefocus on hypoxia as an upstream regulator of preeclampsia and its consequences in amodel compromised by a deficiency in key pregnancy compatible immune modulators.It has been proposed that placental hypoxia releases cytotoxic factors produced at thematernal–fetal interface into the circulation to manifest the maternal symptoms associatedwith preeclampsia. However, it is not clear how this mechanism is empowered in pregnantwomen. Does systemic hypoxia exert preeclampsia-like effects on pregnancy? Are theseeffects further manifested by intrinsic inflammation in the absence of key immune modu-
lators such as IL-10? Thus, it is of paramount importance that in vivo models be developedwherein the role of systemic hypoxia can be evaluated for preeclampsia-causing events.We present a discussion on whether prolonged exposure to hypoxia can lead to a perpetualcycle of compartmentalized uteroplacental tissue damage, release of anti-angiogenic andvasoconstrictive factors that impair trophoblast invasion and promote systemic vascularg in the
resistance resultin1. Introduction
Preeclampsia is a syndrome diagnosed by hypertensionand proteinuria after 20 weeks of gestation with mild tosevere microangiopathy of various target organs includ-ing kidney, liver, brain and placenta (ACOG Committeeon Practice Bulletins—Obstetrics, 2002). The fact that
placental tissue but not the fetus is necessary for thedevelopment of this disease and that the disease itself isalways cured after delivery of the placenta underscores itsindispensable role in the pathophysiology of preeclamp-∗ Corresponding author at: Department of Pediatrics, Women andInfants Hospital, 101 Dudley Street, Providence, RI 02905, USA.Tel.: +1 401 274 1122x8004; fax: +1 401 277 3617.
E-mail address: [email protected] (S. Sharma).
0165-0378/$ – see front matter © 2010 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.jri.2010.01.002
maternal syndrome.© 2010 Elsevier Ireland Ltd. All rights reserved.
sia (Moore-Maxwell and Robboy, 2004). The consensusreached at a recent NICHD/NIH sponsored workshop isthat preeclampsia is a multifactorial disease whose patho-genesis is not solely vascular, genetic, immunologic, orenvironmental but a complex combination of factors (Ilekiset al., 2007). Moreover, the heterogeneity of the disease issuggested by diverse clinical manifestations such as mildor severe preeclampsia, early onset (<34 weeks) or lateonset (>34 weeks) of the disease and presence or absence ofintra-uterine growth restriction (IUGR) with preeclampsia(Dekker and Sibai, 2001). One may wonder if these distinctclinical presentations have common underlying mecha-
nistic underpinnings that simply manifest differentiallybased on contribution from predisposing maternal factors.Indeed, women with asthma, obesity, maternal infections,insulin resistance or adverse lipid metabolic profile all havean increased incidence of preeclampsia (Sibai et al., 2005).
ductive
dnmpectsewe2sfmp
2
bttrpsnicdmgaprspriMap
ptfsratIcgr2pb1Bp
S. Sharma et al. / Journal of Repro
Nevertheless, the consequence is that this multisystemisorder occurs in about 5–8% of all live birth preg-ancies in the United States and is a leading cause ofaternal and fetal mortality and morbidity. Moreover, a
opulation-based cohort study suggests that women witharly-onset preeclampsia are at greater risk of cardiovas-ular disease later in life (Irgens et al., 2001). Importantly,he hallmark pathological features of preeclampsia arehallow trophoblast invasion and poor spiral artery remod-ling resulting in placental hypoperfusion, although not allomen with reduced blood flow to the placenta experi-
nce preeclampsia (Roberts and Hubel, 1999; Burton et al.,009). It is then possible that a second hit in terms of intrin-ic or induced dysregulation of a pregnancy compatibleactor(s) or inflammation at the maternal–fetal interface
ay culminate in full spectrum of symptoms as seen inreeclampsia.
. Etiological factors associated with preeclampsia
Pregnancy is a physiological state that is characterizedy an active dialog between maternal and extraembryonicissues. The in utero milieu instructs developmental cueso the placenta which lead to the remodeling of deliveryoute for nutrients to the fetus. As a consequence, cytotro-hoblasts efficiently invade the decidua and the maternalpiral arteries, a critical process that ensures supply ofutrients to the developing fetus. The outcome of this
nvasion is transformation of the resistant and small mus-ular blood vessels to large, vascular channels with highegree of plasticity and low resistance created by replace-ent of musculoelastic wall with fibrinoid material, thus
reatly enhancing blood flow to the placenta (De Wolf etl., 1982; Pijnenborg et al., 2006). Although the preciseeriod when the trophoblast invasion ceases is unclear, theemodeling is believed to occur during the first and earlyecond trimester. On the contrary in preeclampsia, cytotro-hoblasts fail to invade the spiral arteries deeply enough,esulting in poor transformation of these blood vessels andnsufficient blood flow to the placenta (Brosens et al., 1977;
eekins et al., 1994). Normal trophoblast differentiationnd invasion are associated with integral events in normalregnancy (Zhou et al., 1997).
Why then do third trimester trophoblasts not serve thisurpose in preeclampsia? We have recently demonstratedhat unlike first trimester trophoblasts, term trophoblastsail to interact with endothelial cells due to high expres-ion of E-cadherin and poor expression of VEGF-C and VEGFeceptor (Kalkunte et al., 2008). Impaired differentiationnd transition of trophoblasts may contribute to defectiverophoblast invasion and placentation (Zhou et al., 1993).n this regard, empowerment of uterine natural killer (uNK)ells that uniquely home to the pregnant uterus with angio-enic features not only promote tolerance through VEGF-Celease, but also facilitate angiogenesis (Kalkunte et al.,009). In both mouse and human models, uNK cells further
romote trophoblast invasion and spiral artery remodelingy secreting IFN-�, chemokines and modulators such as IP-0, IL-8 and CXCL12 (Ashkar et al., 2000; Hanna et al., 2006).ecause of concurrent co-onset of maternal symptoms andlacental pathology, it is now well appreciated that fac-Immunology 85 (2010) 112–116 113
tors released from the placenta and found in the maternalcirculation cause systemic endothelial dysfunction.
Similar to tumor growth, a balance of proangiogenic fac-tors such as vascular endothelial growth factor (VEGF) andplacenta growth factor (PlGF) and anti-angiogenic factorsincluding soluble fms-like tyrosone kinase-1 (sFlt-1) andsoluble endoglin (sEng) is established in the developingplacenta. A number of studies have shown that increasedproduction of sFlt-1 and sEng coupled with reduced VEGFand PlGF levels in preeclamptic women seem to corre-late positively with the severity of the disease (Levine etal., 2004; Thadhani et al., 2004; Romero et al., 2008). Itis important to point out that not all women with highsFlt-1 levels acquire preeclampsia and not all preeclampticwomen have high sFlt-1 levels, again confirming the het-erogeneity of the disease. Although the source of sFlt-1seems to be the placenta, the symptoms of hyperten-sion and proteinuria observed in non-pregnant mice implythat upstream factors are involved in the placental injuryleading to multifold production and release of sFlt-1 andsEng into maternal circulation (Karumanchi and Stillman,2006). These molecules would then sequester VEGF in tar-get organs such as the kidney. The upstream factors that arelikely to trigger production of anti-vascular factors at thematernal–fetal interface are poorly understood, but mayinclude hypoxia/ischemia.
3. Is hypoxia an upstream regulator in thepathogenesis of preeclampsia?
Oxygen is a vital regulator of placentation. Embryonicand placental development during early pregnancy occursin a predominantly low oxygen milieu, at least in part,choreographed by hypoxia signaling pathways (Fig. 1).Studies have shown that low oxygen tension can regu-late differentiation of trophoblast stem cells dependenton hypoxia-induced factor-1� (HIF1�) signaling path-ways (Maltepe et al., 2005). Recent studies have elegantlydemonstrated in vivo that exposure of pregnant ratsfrom gestation day 6.5 through day 13.5 to hypobarichypoxia (11% oxygen) stimulated changes in the uter-ine mesometrial vasculature. This was associated withdramatic increase in vascularity and vessel diameter aswell as increased endovascular trophoblast invasion andreplacement of the endothelium. In these experiments, theanimals were intermittently exposed to normoxia, whichmay create a hypoxia–reperfusion scenario. Under theseconditions, hypoxia hastens the appearance of the invasiveendovascular trophoblast (day 13.5) in the mesometrialregions as compared to normoxia (day 14.5), promptingthe authors to suggest a possible window of “sensitivityand timing” to hypoxia that facilitates either early matura-tion of trophoblast or removal of maternal barrier (Rosarioet al., 2008).
Nevertheless, systemic hypoxia is an effective stimuluseliciting adaptations at the maternal–fetal interface, addi-
tionally determining the depth of trophoblast cell invasion.It is then pertinent to contemplate if there is a window of“tolerance” to hypoxia and oxygen levels. Can prolongedexposure to severe systemic hypoxia beyond a thresholdinitiate placental pathology, placental ischemia, inhibition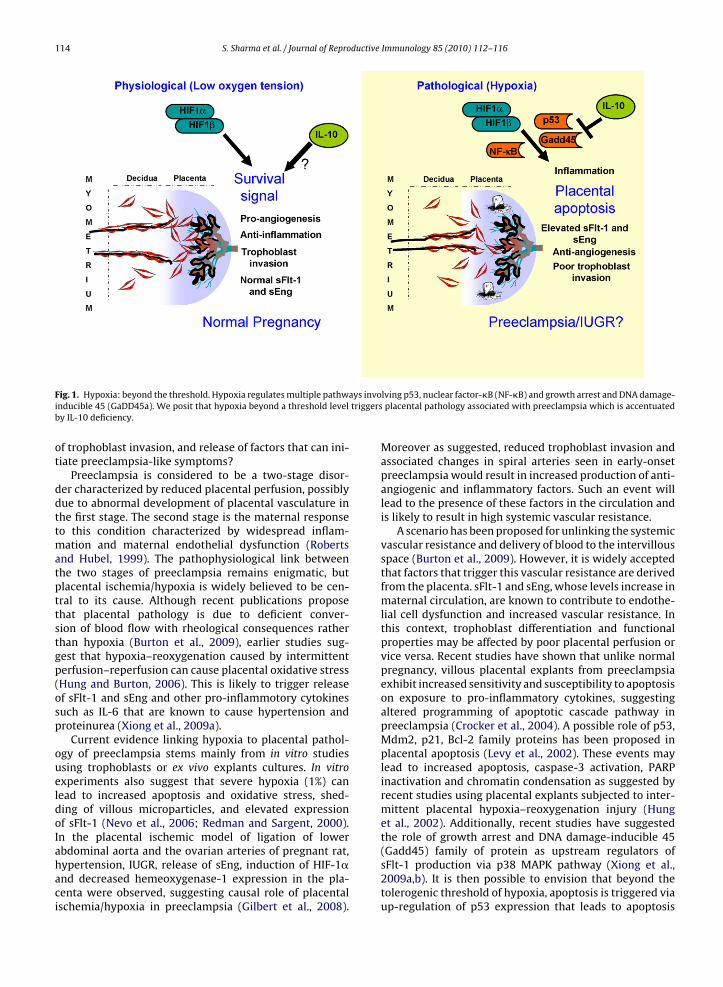
114 S. Sharma et al. / Journal of Reproductive Immunology 85 (2010) 112–116
ays invotriggers
Fig. 1. Hypoxia: beyond the threshold. Hypoxia regulates multiple pathwinducible 45 (GaDD45a). We posit that hypoxia beyond a threshold levelby IL-10 deficiency.
of trophoblast invasion, and release of factors that can ini-tiate preeclampsia-like symptoms?
Preeclampsia is considered to be a two-stage disor-der characterized by reduced placental perfusion, possiblydue to abnormal development of placental vasculature inthe first stage. The second stage is the maternal responseto this condition characterized by widespread inflam-mation and maternal endothelial dysfunction (Robertsand Hubel, 1999). The pathophysiological link betweenthe two stages of preeclampsia remains enigmatic, butplacental ischemia/hypoxia is widely believed to be cen-tral to its cause. Although recent publications proposethat placental pathology is due to deficient conver-sion of blood flow with rheological consequences ratherthan hypoxia (Burton et al., 2009), earlier studies sug-gest that hypoxia–reoxygenation caused by intermittentperfusion–reperfusion can cause placental oxidative stress(Hung and Burton, 2006). This is likely to trigger releaseof sFlt-1 and sEng and other pro-inflammotory cytokinessuch as IL-6 that are known to cause hypertension andproteinurea (Xiong et al., 2009a).
Current evidence linking hypoxia to placental pathol-ogy of preeclampsia stems mainly from in vitro studiesusing trophoblasts or ex vivo explants cultures. In vitroexperiments also suggest that severe hypoxia (1%) canlead to increased apoptosis and oxidative stress, shed-ding of villous microparticles, and elevated expressionof sFlt-1 (Nevo et al., 2006; Redman and Sargent, 2000).In the placental ischemic model of ligation of lower
abdominal aorta and the ovarian arteries of pregnant rat,hypertension, IUGR, release of sEng, induction of HIF-1�and decreased hemeoxygenase-1 expression in the pla-centa were observed, suggesting causal role of placentalischemia/hypoxia in preeclampsia (Gilbert et al., 2008).lving p53, nuclear factor-�B (NF-�B) and growth arrest and DNA damage-placental pathology associated with preeclampsia which is accentuated
Moreover as suggested, reduced trophoblast invasion andassociated changes in spiral arteries seen in early-onsetpreeclampsia would result in increased production of anti-angiogenic and inflammatory factors. Such an event willlead to the presence of these factors in the circulation andis likely to result in high systemic vascular resistance.
A scenario has been proposed for unlinking the systemicvascular resistance and delivery of blood to the intervillousspace (Burton et al., 2009). However, it is widely acceptedthat factors that trigger this vascular resistance are derivedfrom the placenta. sFlt-1 and sEng, whose levels increase inmaternal circulation, are known to contribute to endothe-lial cell dysfunction and increased vascular resistance. Inthis context, trophoblast differentiation and functionalproperties may be affected by poor placental perfusion orvice versa. Recent studies have shown that unlike normalpregnancy, villous placental explants from preeclampsiaexhibit increased sensitivity and susceptibility to apoptosison exposure to pro-inflammatory cytokines, suggestingaltered programming of apoptotic cascade pathway inpreeclampsia (Crocker et al., 2004). A possible role of p53,Mdm2, p21, Bcl-2 family proteins has been proposed inplacental apoptosis (Levy et al., 2002). These events maylead to increased apoptosis, caspase-3 activation, PARPinactivation and chromatin condensation as suggested byrecent studies using placental explants subjected to inter-mittent placental hypoxia–reoxygenation injury (Hunget al., 2002). Additionally, recent studies have suggestedthe role of growth arrest and DNA damage-inducible 45
(Gadd45) family of protein as upstream regulators ofsFlt-1 production via p38 MAPK pathway (Xiong et al.,2009a,b). It is then possible to envision that beyond thetolerogenic threshold of hypoxia, apoptosis is triggered viaup-regulation of p53 expression that leads to apoptosis
ductive
cesa
4
bisccicdq
tfInmfue12Ilpddaiagismae
plseTnth2sp
pac(hi
S. Sharma et al. / Journal of Repro
ausing signaling cascade (Fig. 1). However, a direct in vivovidence of the hypoxia-sFlt1-sEng-placental pathology-ystemic vascular resistance axis is currently notvailable.
. Hypoxia and immunity
NF-�B is a crucial regulator of post-transcriptional sta-ilization and accumulation of HIF1� protein in innate
mmune cells, particularly macrophages which encounterevere hypoxia at the site of injury or infection. Under theseonditions, HIF promotes release of pro-inflammatoryytokines and VEGF, up-regulates TLR expression andnduces iNOS expression (Nizet and Johnson, 2009). In thisontext, it is possible that intra-uterine cytokine milieuisplays a vital regulatory role in hypoxia-driven conse-uences during placentation and preeclampsia (Fig. 1).
Among immuno-regulatory cytokines, IL-10 is thoughto play a critical role at the maternal–fetal inter-ace because of its potent anti-inflammatory activities.L-10 is expressed in a gestational age-dependent man-er and is down regulated in the placental–decidualicroenvironment as part of “the normal mechanism”
or the onset of labor (Hanna et al., 2000). Further, innexplained spontaneous pregnancy loss compared tolective terminations, there is poor expression of IL-0 in placental and decidual tissues (Plevyak et al.,002). Importantly, mice with a null mutation in the
l10 gene are more sensitive to very low doses of toll-ike receptor ligands such as lipopolysaccharide (LPS),oly I:C or CpG which cause fetal demise, prematureelivery, and IUGR depending on the route and win-ow of administration. Pregnancy incompatible effectsppear to be associated with cytotoxic activation of uter-ne immune cells (Murphy et al., 2005, 2009; Thaxton etl., 2009). More recently, it was shown that adenoviralene transfer of recombinant human IL-10 amelioratedschemia–reperfusion injury by decreasing hepatic necro-is and apoptosis by inhibiting caspase-3 activity anditochondrial cytochrome c release, and up-regulating
nti-apoptotic (Bcl-2) and antioxidant (HO-1) molecules (Lit al., 2009).
Preliminary studies from our laboratory suggest thatregnant mice exposed to hypoxia (9.5% O2) for pro-
onged period (gd 7.5–15) experience preeclampsia-likeymptoms with elevated sFlt-1 and sEng, providing directvidence of systemic hypoxia in initiating preeclampsia.he effect of hypoxia was severe particularly in IL-10ull mutant mice as compared to their wild type coun-erparts. Moreover, placental pathology seems to implyypoxia-driven apoptosis due to perturbed p53–Bax–Bcl-–caspase-3 axis. Taken together, our studies seem touggest that IL-10 may blunt the severe hypoxia-inducedlacental injury and apoptosis.
It is then possible that IL-10 deficiency in a subset of theopulation could be a predisposing factor to preeclampsia
nd may define its severity. As understanding of an intri-ate link between hypoxia and innate immunity emergesNizet and Johnson, 2009), future studies on the impact ofypoxia on uNK cell homoeostasis and functions, responsen the settings of infections and inflammation, and effect
Immunology 85 (2010) 112–116 115
on endovascular activity at the maternal–fetal interface arehighly warranted.
5. Conclusions
Preeclampsia is a heterogeneous disease. The mecha-nistic understanding of preeclampsia as understood todayresembles an airline flight map converging on one des-tination, making it a multifactorial disorder. We positthat beyond the threshold hypoxic challenge during preg-nancy is a crucial upstream trigger that leads to perpetualcycle of placental pathology, release of anti-angiogenic andvasoconstrictive factors that promote systemic vascularresistance leading to manifestation of the maternal syn-drome.
Acknowledgements
This work was supported in part by the Rhode IslandResearch Alliance Collaborative Research Award 2009-28.We thank the members of the Sharma laboratory for theircritical reading of the manuscript.
References
ACOG Committee on Practice Bulletins—Obstetrics, 2002. ACOG practicebulletin. Diagnosis and management of preeclampsia and eclampsia.Obstet. Gynecol. 99, 159–167.
Ashkar, A.A., Di Santo, J.P., Croy, B.A., 2000. Interferon � contributes to initi-ation of uterine vascular modification, decidual integrity, and uterinenatural killer cell maturation during normal murine pregnancy. J. Exp.Med. 192, 259–269.
Brosens, I., Dixon, H.G., Robertson, W.B., 1977. Fetal growth retardationand the arteries of the placental bed. Br. J. Obstet. Gynaecol. 84,656–663.
Burton, G.J., Woods, A.W., Jauniaux, E., Kingdom, J.C., 2009. Rheologicaland physiological consequences of conversion of the maternal spi-ral arteries for uteroplacental blood flow during human pregnancy.Placenta 30, 473–482.
Crocker, I.P., Cooper, S., Ong, S.C., Baker, P.N., 2004. Altered cell kinet-ics in cultured placental villous explants in pregnancies complicatedby preeclampsia and intra-uterine growth restriction. J. Pathol. 204,11–18.
Dekker, G., Sibai, B., 2001. Primary, secondary and tertiary prevention ofpre-eclampsia. Lancet 357, 209–215.
De Wolf, F., Brosens, I., Robertson, W.B., 1982. Ultrastructure of uteropla-cental arteries. Contrib. Gynecol. Obstet. 9, 86–99.
Gilbert, J.S., Ryan, M.J., LaMarca, B.B., Sedeek, M., Murphy, S.R., Granger, J.P.,2008. Pathophysiology of hypertension during preeclampsia: linkingplacental ischemia with endothelial dysfunction. Am. J. Physiol. HeartCirc. Physiol. 294, 541–550.
Hanna, J., Goldman-Wohl, D., Hamani, Y., Avraham, I., Greenfield, C.,Natanson-Yaron, S., Prus, D., Cohen-Daniel, L., Arnon, T.I., Manaster, I.,Gazit, R., Yutkin, V., Benharroch, D., Porgador, A., Keshet, E., Yagel, S.,Mandelboim, O., 2006. Decidual NK cells regulate key developmen-tal processes at the human fetal–maternal interface. Nat. Med. 12,1065–1074.
Hanna, N., Hanna, I., Hleb, M., Wagner, E., Dougherty, J., Balkundi, D., Pad-bury, J., Sharma, S., 2000. Gestational age-dependent expression ofIL-10 and its receptor in human placental tissues and isolated cytotro-phoblasts. J. Immunol. 164, 5721–5728.
Hung, T.H., Skepper, J.N., Charnock-Jones, S.D., Burton, G.J., 2002. Hypoxiareoxygenation. A potent inducer of apoptotic changes in the humanplacenta and possible etiological factor in preeclampsia. Circ. Res. 90,1274–1281.
Hung, T.H., Burton, G.J., 2006. Hypoxia and reoxygenation: a possiblemechanism for placental oxidative stress in preeclampsia. Taiwan J.Obstet. Gynecol. 45, 189–200.
Ilekis, J., Reddy, U.M., Roberts, J.M., 2007. Preeclampsia—a pressing prob-lem: an executive summary of a National Institute of Child Health andHuman Development workshop. Reprod. Sci. 14, 508–523.
ductive
116 S. Sharma et al. / Journal of ReproIrgens, H.U., Reisaeter, L., Irgens, L.M., Lie, R.T., 2001. Long term mortalityof mothers and fathers after preeclampsia: population based cohortstudy. Br. Med. J. 323, 1213–1217.
Kalkunte, S., Lai, Z., Tewari, N., Chichester, C., Romero, R., Padbury, J.,Sharma, S., 2008. In vitro and in vivo evidence for lack of endovascularremodeling by third trimester trophoblasts. Placenta 29, 871–878.
Kalkunte, S., Mselle, T.F., Norris, W.E., Wira, C.R., Sentman, C.L., Sharma, S.,2009. VEGF C facilitates immune tolerance and endovascular activityof human uterine NK cells at the maternal–fetal interface. J. Immunol.182, 4085–4092.
Karumanchi, S.A., Stillman, I.E., 2006. In vivo rat model of preeclampsia.Methods Mol. Med. 122, 393–399.
Levine, R.J., Maynard, S.E., Qian, C., Lim, K.H., England, L.J., Yu, K.F., Schister-man, E.F., Thadhani, R., Sachs, B.P., Epstein, F.H., Sibai, B.M., Sukhatme,V.P., Karumanchi, S.A., 2004. Circulating angiogenic factors and therisk of preeclampsia. N. Engl. J. Med. 350, 672–683.
Levy, R., Smith, S.D., Yusuf, K., Huettner, P.C., Kraus, F.T., Sadovsky, Y.,Nelson, D.M., 2002. Trophoblasts apoptosis from pregnancies com-plicated by fetal growth restriction is associated with enhanced p53expression. Am. J. Obstet. Gynecol. 186, 1056–1061.
Li, J.Q., Qi, H.Z., He, Z.J., Hu, W., Si, Z.Z., Li, Y.N., Li, D.B., 2009. Cytoprotectiveeffects of human interleukin-10 gene transfer against necrosis andapoptosis induced by hepatic cold ischemia/reperfusion injury. J. Surg.Res. 157, e71–e78.
Maltepe, E., Krampitz, G.W., Okazaki, K.M., Red-Horse, K., Mak, W., Simon,M.C., Fisher, S.J., 2005. Hypoxia-inducible factor-dependent histonedeacetylase activity determines stem cell fate in the placenta. Devel-opment 32, 3393–3403.
Meekins, J.W., Pijnenborg, R., Hanssens, M., McFadyen, I.R., van Asshe, A.,1994. A study of placental bed spiral arteries and trophoblast inva-sion in normal and severe pre-eclamptic pregnancies. Br. J. Obstet.Gynaecol. 101, 669–674.
Moore-Maxwell, C.A., Robboy, S.J., 2004. Placental site trophoblastictumor arising from antecedent molar pregnancy. Gynecol. Oncol. 92,708–712.
Murphy, S.P., Fast, L.D., Hanna, N.N., Sharma, S., 2005. Uterine NK cellsmediate inflammation-induced fetal demise in IL-10-null mice. J.Immunol. 175, 4084–4090.
Murphy, S.P., Hanna, N.N., Fast, L.D., Shaw, S., Berg, G., Padbury, J.F.,Romero, R., Sharma, S., 2009. Evidence for participation of uterinenatural killer cells in the mechanisms responsible for spontaneouspreterm labor and delivery. Am. J. Obstet. Gynecol. 200 (308), e1–e9.
Nevo, O., Soleymanlou, N., Wu, Y., Xu, J., Kingdom, J., Many, A., Zamudio,S., Caniggia, I., 2006. Increased expression of sFlt-1 in in vivo and invitro models of human placental hypoxia is mediated by HIF-1. Am. J.Physiol. Regul. Integr. Comp. Physiol. 355, 992–1005.
Nizet, V., Johnson, R.S., 2009. Interdependence of hypoxic and innateimmune responses. Nat. Rev. Immunol. 9, 609–617.
Immunology 85 (2010) 112–116
Pijnenborg, R., Vercruysse, L., Hanssens, M., 2006. The uterine spiralarteries in human pregnancy: facts and controversies. Placenta 27,939–958.
Plevyak, M., Hanna, N., Mayer, S., Murphy, S., Pinar, H., Fast, L., Ekerfelt,C., Ernerudh, J., Berg, G., Matthiesen, L., Sharma, S., 2002. Deficiency ofdecidual IL-10 in first trimester missed abortion: a lack of correlationwith the decidual immune cell profile. Am. J. Reprod. Immunol. 47,242–250.
Redman, C.W.G., Sargent, I.L., 2000. Placental debris, oxidative stress andpreeclampsia. Placenta 21, 597–602.
Roberts, J.M., Hubel, C.A., 1999. Is oxidative stress the link in the two-stagemodel of preeclampsia. Lancet 354, 788–789.
Romero, R., Nien, J.K., Espinoza, J., Todem, D., Fu, W., Chung, H.,Kusanovic, J.P., Gotsch, F., Erez, O., Mazaki-Tovi, S., Gomez, R.,Edwin, S., Chaiworapongsa, T., Levine, R.J., Karumanchi, S.A., 2008.A longitudinal study of angiogenic (placental growth factor) andanti-angiogenic (soluble endoglin and soluble vascular endothe-lial growth factor receptor-1) factors in normal pregnancy andpatients destined to develop preeclampsia and deliver a smallfor gestational age neonate. J. Matern. Fetal Neonatal Med. 21,9–23.
Rosario, G.X., Konno, T., Soares, M.J., 2008. Maternal hypoxia activatesendovascular trophoblast cell invasion. Dev. Biol. 314, 362–375.
Sibai, B., Dekker, G., Kupferminic, M., 2005. Preeclampsia. Lancet 353,785–799.
Thadhani, R., Mutter, W.P., Wolf, M., Levine, R.J., Taylor, R.N., Sukhatme,V.P., Ecker, J., Karumanchi, S.A., 2004. First trimester placental growthfactor and soluble fms-like tyrosine kinase 1 and risk for preeclampsia.J. Clin. Endocrinol. Metab. 89, 770–775.
Thaxton, J.E., Romero, R., Sharma, S., 2009. TLR9 activation coupled to IL-10 deficiency induces adverse pregnancy outcomes. J. Immunol. 183,1144–1154.
Xiong, Y., Liebermann, D.A., Tront, J.S., Holtzman, E.J., Huang, Y., Hoff-man, B., Geifman-Holtzman, O., 2009a. Gadd45a stress signalingregulates sFlt-1 expression in preeclampsia. J. Cell Physiol. 220,632–639.
Xiong, Y., Liebermann, D.A., Holtzman, E.J., Hoffman, B., Geifman-Holtzman, O., 2009b. Hypoxia regulates sFlt-1 secretion viaGadd45a-p38 stress response pathway. Am. J. Obstet. Gynecol. 199,S204.
Zhou, Y., Fisher, S.J., Janatpor, M., Genbacev, O., Dejana, E., Wheelock, M.,Damsky, C.H., 1997. Human cytotrophoblasts adopt a vascular phe-
notype as they differentiate. A strategy for successful endovascularinvasion. J. Clin. Invest. 99, 2139–2151.Zhou, Y., Damsky, C.H., Chiu, K., Roberts, J.M., Fisher, S.J., 1993.Preeclampsia is associated with abnormal expression of adhe-sion molecules by invasive cytotrophoblasts. J. Clin. Invest. 91,950–960.