bilateral central scotomata due to intracranial...
TRANSCRIPT
British Journal of Ophthalmology, 1984, 68, 449-457
Bilateral central scotomata due to intracranial tumourN. G. R. PAGE AND M. D. SANDERS
From the National Hospitals for Nervous Diseases, Queen Square, London WC]
SUMMARY Bilateral centrocaecal scotomata have been recognised as a sign of intrinsic optic nervedisease, usually associated with hereditary optic neuropathy, and nutritional or toxic amblyopias.This report describes four patients with central scotomata due to intracranial masses, three ofwhom recovered after surgical intervention. The clinician should be alerted to the association inpatients with headaches, other neurological signs, and central visual loss.
A central scotoma is characteristic of optic nervedisease and found concomitantly with reduced visualacuity, reduced colour vision, an afferent pupil defect,and pallor of the optic disc. Macular disease maycause a central field defect which may be presentbilaterally, but metamorphopsia, abnormal photo-stress, and normal pupils in conjunction with fundusdetails seen on fluorescein angiography will usuallyallow an accurate diagnosis.When central visual loss is unilateral, painless, and
progressive, a compressive optic neuropathy will besuspected. However, the vast majority of bilateraloptic neuropathies are due to 'toxic,' 'inflammatory,'or hereditary causes, and compression is not usuallysuspected. Typically, compressive lesions of theanterior visual pathways are unilateral or, if bilateral,very asymmetric, with late involvement of the secondeye, and then signs of chiasmal involvement. Thediagnosis of a toxic or nutritional amblyopia may bepresumptive, particularly with a reticent patient inwhom field charting may, with difficulty, revealdiscrete symmetrical centrocaecal scotomata.We have recently seen four patients presenting
with visual failure and bilateral central scotomata. Ineach case this was caused by an expanding intracranialtumour.
Case reports
CASE 1A 65-year-old woman was admitted for investigationof bilateral visual loss. Initially she had noted pro-gressive blurring of vision in the right eye for a year,and during that period a small horseshoe retinal tear
Correspondence to Dr N. G. R. Page, MRC Ncuro-Otology Unit,Institute of Neurology, National Hospital, Queen Square, LondonWC1N 3BG.
in the periphery was repaired. In the weeks beforeadmission she had noticed increasing central mistinessin the left eye, with inability to read a newspaper.There was no ocular pain or headache and no otherspecific complaints, but on questioning she admittedto loss of smell for about a year. She was a non-smoker, did not consume alcohol, and had anadequate diet.She was fit and alert, with abnormalities confined
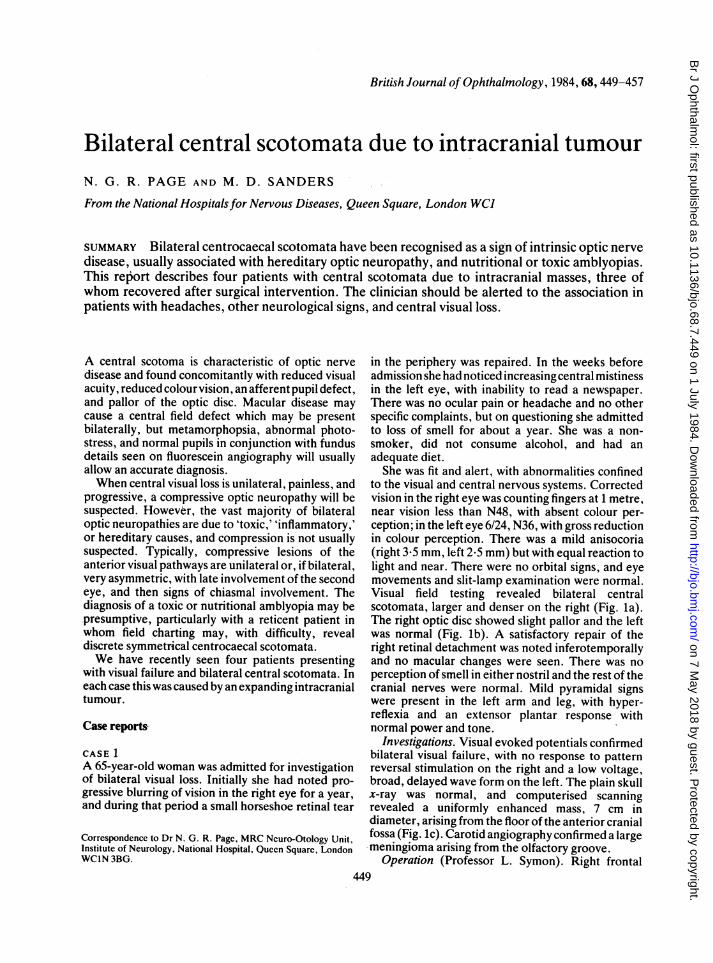
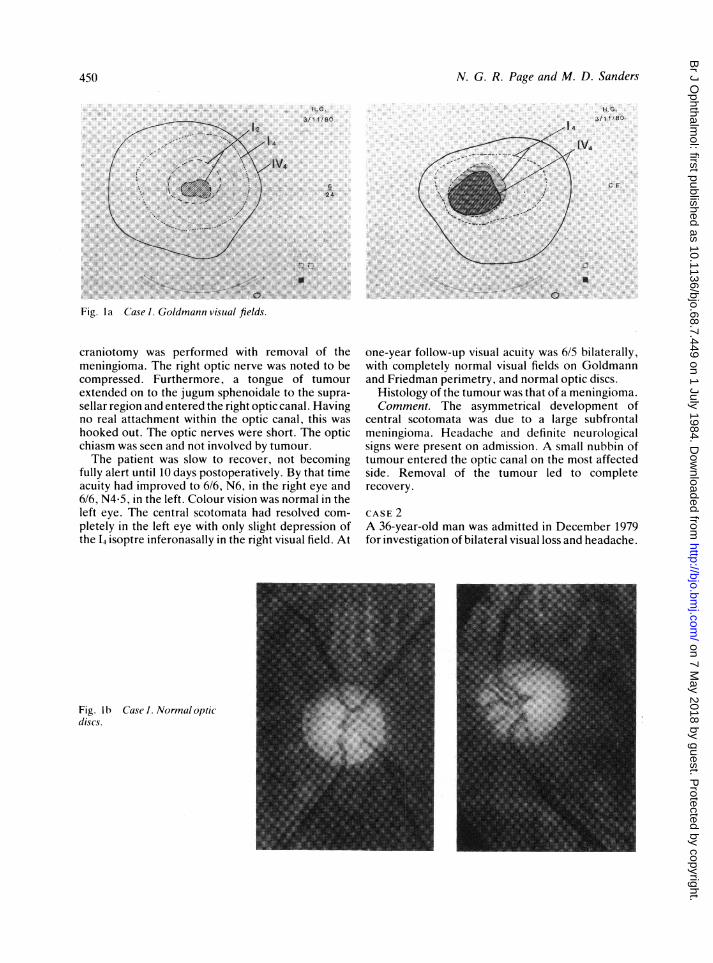
to the visual and central nervous systems. Correctedvision in the right eye was counting fingers at 1 metre,near vision less than N48, with absent colour per-ception; in the left eye 6/24, N36, with gross reductionin colour perception. There was a mild anisocoria(right 3*5 mm, left 2-5 mm) but with equal reaction tolight and near. There were no orbital signs, and eyemovements and slit-lamp examination were normal.Visual field testing revealed bilateral centralscotomata, larger and denser on the right (Fig. la).The right optic disc showed slight pallor and the leftwas normal (Fig. lb). A satisfactory repair of theright retinal detachment was noted inferotemporallyand no macular changes were seen. There was noperception of smell in either nostril and the rest of thecranial nerves were normal. Mild pyramidal signswere present in the left arm and leg, with hyper-reflexia and an extensor plantar response withnormal power and tone.
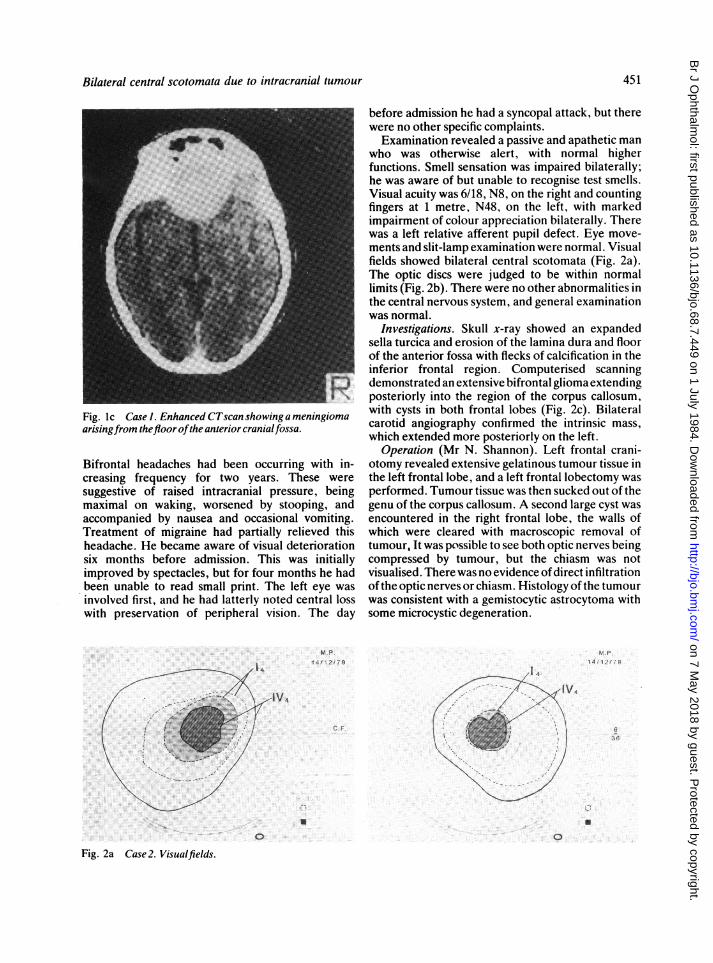
Investigations. Visual evoked potentials confirmedbilateral visual failure, with no response to patternreversal stimulation on the right and a low voltage,broad, delayed wave form on the left. The plain skullx-ray was normal, and computerised scanningrevealed a uniformly enhanced mass, 7 cm indiameter, arising from the floor of the anterior cranialfossa (Fig. lc). Carotid angiography confirmed a largemeningioma arising from the olfactory groove.
Operation (Professor L. Symon). Right frontal449
on 7 May 2018 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.68.7.449 on 1 July 1984. D
ownloaded from
N. G. R. Page and M. D. Sanders
..........
. :..
*I *'sS \s Z/{ s ) :~~~~~~~~~~....
.. .
, ......:.. .:. ::.~~~~~~~.Fig la Cas Godmn viua fields.
H.
Sf, F,8
craniotomy was performed with removal of themeningioma. The right optic nerve was noted to becompressed. Furthermore, a tongue of tumourextended on to the jugum sphenoidale to the supra-sellar region and entered the right optic canal. Havingno real attachment within the optic canal, this washooked out. The optic nerves were short. The opticchiasm was seen and not involved by tumour.The patient was slow to recover, not becoming
fully alert until 10 days postoperatively. By that timeacuity had improved to 6/6, N6, in the right eye and6/6, N4-5, in the left. Colour vision was normal in theleft eye. The central scotomata had resolved com-pletely in the left eye with only slight depression ofthe L isoptre inferonasally in the right visual field. At
one-year follow-up visual acuity was 6/5 bilaterally,with completely normal visual fields on Goldmannand Friedman perimetry, and normal optic discs.
Histology of the tumour was that of a meningioma.Comment. The asymmetrical development of
central scotomata was due to a large subfrontalmeningioma. Headache and definite neurologicalsigns were present on admission. A small nubbin oftumour entered the optic canal on the most affectedside. Removal of the tumour led to completerecovery.
CASE 2A 36-year-old man was admitted in December 1979for investigation of bilateral visual loss and headache.
Fig. lb Case Normal opticdiscs.
450
on 7 May 2018 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.68.7.449 on 1 July 1984. D
ownloaded from
Bilateral central scotomata due to intracranial tumour
Fig. Ic Case 1. Enhanced CTscan showing a meningiomaarisingfrom thefloor ofthe anterior cranialfossa.
Bifrontal headaches had been occurring with in-creasing frequency for two years. These weresuggestive of raised intracranial pressure, beingmaximal on waking, worsened by stooping, andaccompanied by nausea and occasional vomiting.Treatment of migraine had partially relieved thisheadache. He became aware of visual deteriorationsix months before admission. This was initiallyimproved by spectacles, but for four months he hadbeen unable to read small print. The left eye wasinvolved first, and he had latterly noted central losswith preservation of peripheral vision. The day
-1 4
before admission he had a syncopal attack, but therewere no other specific complaints.
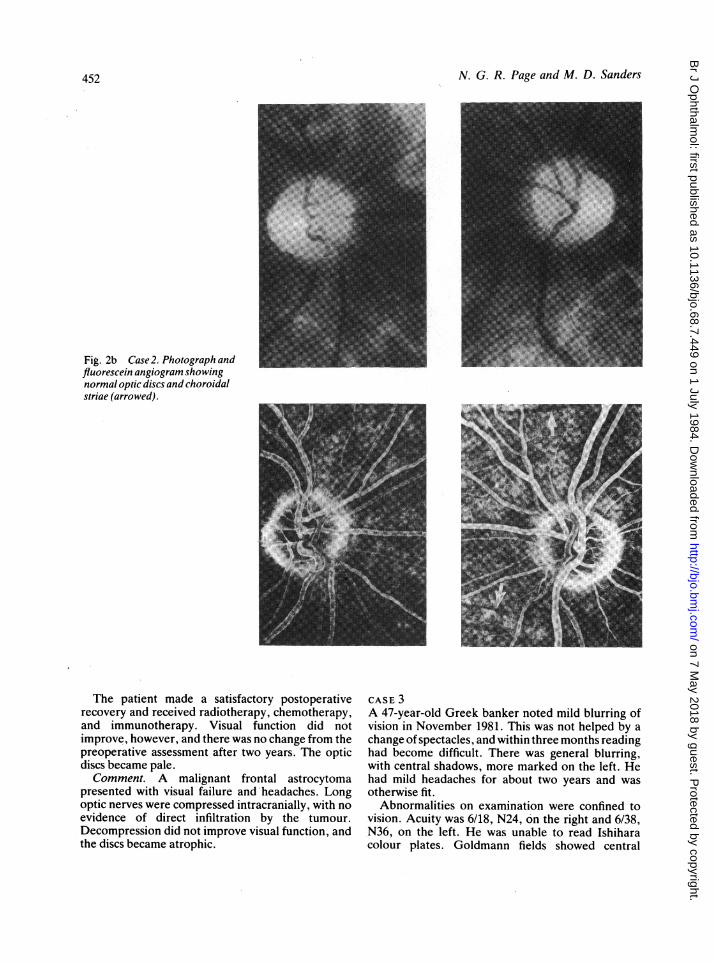
Examination revealed a passive and apathetic manwho was otherwise alert, with normal higherfunctions. Smell sensation was impaired bilaterally;he was aware of but unable to recognise test smells.Visual acuity was 6/18, N8, on the right and countingfingers at 1 metre, N48, on the left, with markedimpairment of colour appreciation bilaterally. Therewas a left relative afferent pupil defect. Eye move-ments and slit-lamp examination were normal. Visualfields showed bilateral central scotomata (Fig. 2a).The optic discs were judged to be within normallimits (Fig. 2b). There were no other abnormalities inthe central nervous system, and general examinationwas normal.
Investigations. Skull x-ray showed an expandedsella turcica and erosion of the lamina dura and floorof the anterior fossa with flecks of calcification in theinferior frontal region. Computerised scanningdemonstrated an extensive bifrontal glioma extendingposteriorly into the region of the corpus callosum,with cysts in both frontal lobes (Fig. 2c). Bilateralcarotid angiography confirmed the intrinsic mass,which extended more posteriorly on the left.
Operation (Mr N. Shannon). Left frontal crani-otomy revealed extensive gelatinous tumour tissue inthe left frontal lobe, and a left frontal lobectomy wasperformed. Tumour tissue was then sucked out of thegenu of the corpus callosum. A second large cyst wasencountered in the right frontal lobe, the walls ofwhich were cleared with macroscopic removal oftumour, It was possible to see both optic nerves beingcompressed by tumour, but the chiasm was notvisualised. There was no evidence ofdirect infiltrationofthe optic nerves or chiasm. Histology of the tumourwas consistent with a gemistocytic astrocytoma withsome microcystic degeneration.
M P.14/12/79
1f 4
M r4/ :2 7
-IV4
C.F.
U
0
a
0
Fig. 2a Case2. Visualfields.
451
on 7 May 2018 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.68.7.449 on 1 July 1984. D
ownloaded from
N. G. R. Page and M. D. Sanders452
Fig. 2b Case 2. Photograph andfluorescein angiogram showingnormal optic discs and choroidalstriae (arrowed).
The patient made a satisfactory postoperativerecovery and received radiotherapy, chemotherapy,and immunotherapy. Visual function did notimprove, however, and there was no change from thepreoperative assessment after two years. The opticdiscs became pale.Comment. A malignant frontal astrocytoma
presented with visual failure and headaches. Longoptic nerves were compressed intracranially, with noevidence of direct infiltration by the tumour.Decompression did not improve visual function, andthe discs became atrophic.
CASE 3A 47-year-old Greek banker noted mild blurring ofvision in November 1981. This was not helped by achange of spectacles, and within three months readinghad become difficult. There was general blurring,with central shadows, more marked on the left. Hehad mild headaches for about two years and wasotherwise fit.
Abnormalities on examination were confined tovision. Acuity was 6/18, N24, on the right and 6/38,N36, on the left. He was unable to read Ishiharacolour plates. Goldmann fields showed central
on 7 May 2018 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.68.7.449 on 1 July 1984. D
ownloaded from
Bilateral central scotomata due to intracranial tumour
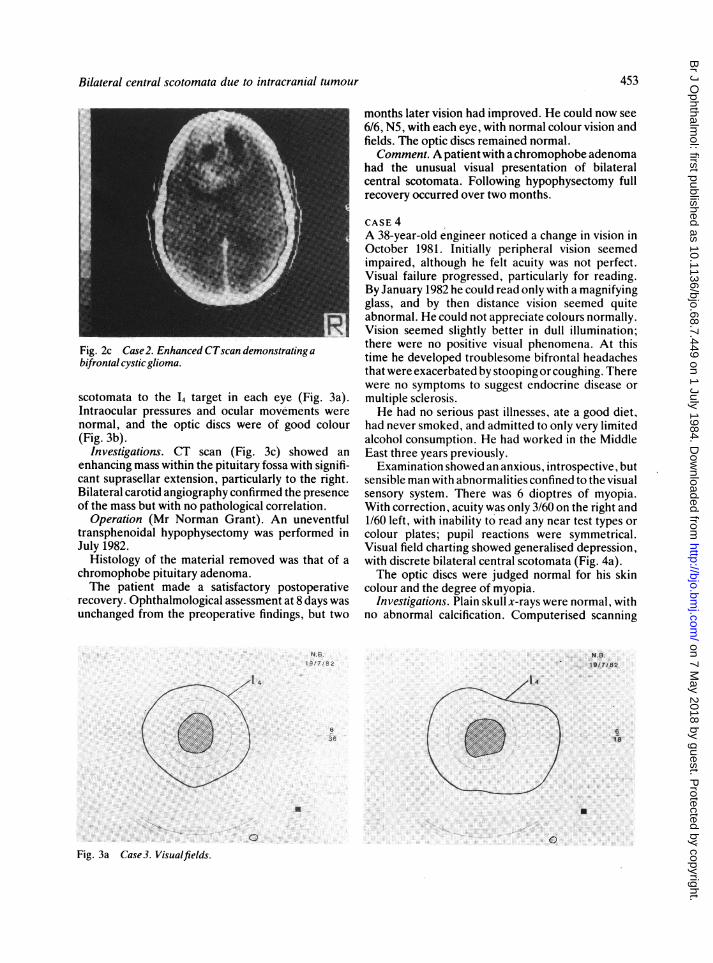
Fig. 2c Case2. Enhanced CTscan demonstrating abifrontalcysticglioma.
scotomata to the 14 target in each eye (Fig. 3a).Intraocular pressures and ocular movements werenormal, and the optic discs were of good colour(Fig. 3b).
Investigations. CT scan (Fig. 3c) showed anenhancing mass within the pituitary fossa with signifi-cant suprasellar extension, particularly to the right.Bilateral carotid angiography confirmed the presenceof the mass but with no pathological correlation.
Operation (Mr Norman Grant). An uneventfultransphenoidal hypophysectomy was performed inJuly 1982.
Histology of the material removed was that of achromophobe pituitary adenoma.The patient made a satisfactory postoperative
recovery. Ophthalmological assessment at 8 days wasunchanged from the preoperative findings, but two
months later vision had improved. He could now see6/6, N5, with each eye, with normal colour vision andfields. The optic discs remained normal.Comment. A patient with a chromophobe adenoma
had the unusual visual presentation of bilateralcentral scotomata. Following hypophysectomy fullrecovery occurred over two months.
CASE 4A 38-year-old engineer noticed a change in vision inOctober 1981. Initially peripheral vision seemedimpaired, although he felt acuity was not perfect.Visual failure progressed, particularly for reading.By January 1982 he could read only with a magnifyingglass, and by then distance vision seemed quiteabnormal. He could not appreciate colours normally.Vision seemed slightly better in dull illumination;there were no positive visual phenomena. At thistime he developed troublesome bifrontal headachesthat were exacerbated by stooping or coughing. Therewere no symptoms to suggest endocrine disease ormultiple sclerosis.He had no serious past illnesses, ate a good diet,
had never smoked, and admitted to only very limitedalcohol consumption. He had worked in the MiddleEast three years previously.Examination showed an anxious, introspective, but
sensible man with abnormalities confined to the visualsensory system. There was 6 dioptres of myopia.With correction, acuity was only 3/60 on the right and1/60 left, with inability to read any near test types orcolour plates; pupil reactions were symmetrical.Visual field charting showed generalised depression,with discrete bilateral central scotomata (Fig. 4a).The optic discs were judged normal for his skin
colour and the degree of myopia.Investigations. Plain skull x-rays were normal, with
no abnormal calcification. Computerised scanning
N.S.19XJ/82
N.B-. 19M8i2
4
636
U U
0 0Fig. 3a Case3. Visualfields.
453
on 7 May 2018 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.68.7.449 on 1 July 1984. D
ownloaded from
N. G. R. Page and M. D. Sanders
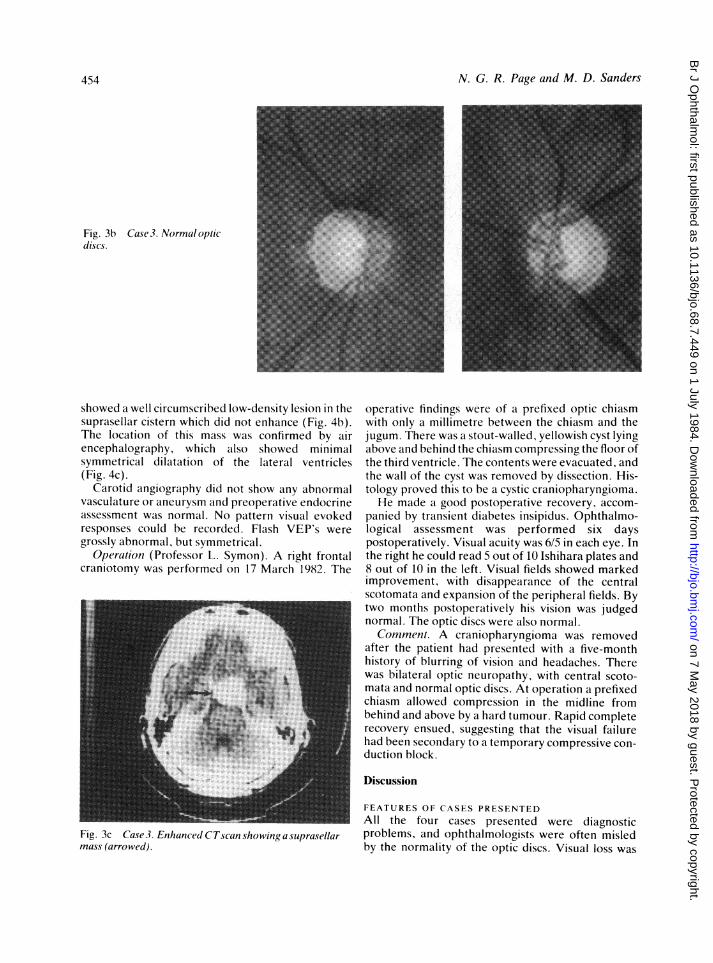
Fig. 3b Case 3. Normal opticdiscs.
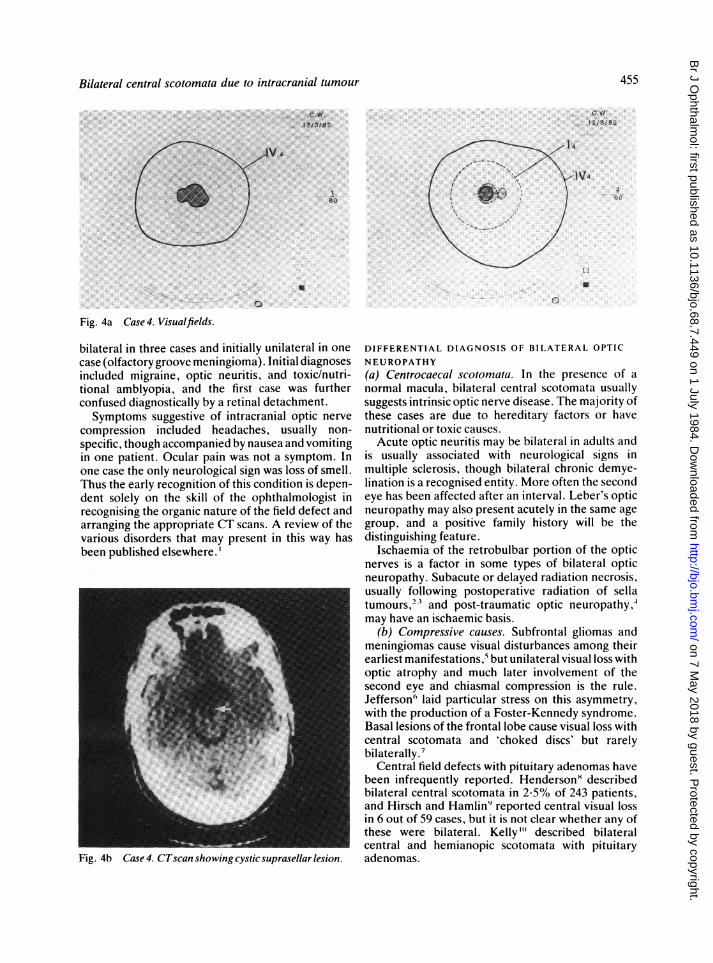
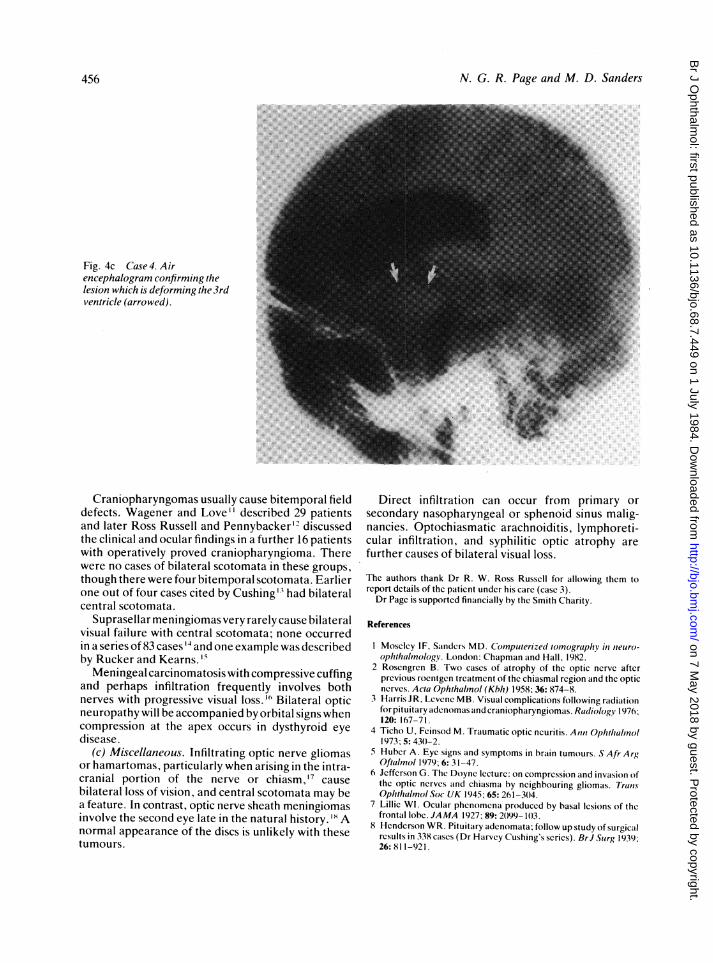
showed a well circumscribed low-density lesion in thesuprasellar cistern which did not enhance (Fig. 4b).The location of this mass was confirmed by airencephalography, which also showed minimalsymmetrical dilatation of the lateral ventricles(Fig. 4c).
Carotid angiography did not show any abnormalvasculature or aneurysm and preoperative endocrineassessment was normal. No pattern visual evokedresponses could be recorded. Flash VEP's weregrossly abnormal, but symmetrical.
Operation (Professor L. Symon). A right frontalcraniotomy was performed on 17 March 1982. The
Fig. 3c Case 3. Enhanced CTscan showingasuprasellarmass (arrowed).
operative findings were of a prefixed optic chiasmwith only a millimetre between the chiasm and thejugum. There was a stout-walled, yellowish cyst lyingabove and behind the chiasm compressing the floor ofthe third ventricle. The contents were evacuated, andthe wall of the cyst was removed by dissection. His-tology proved this to be a cystic craniopharyngioma.He made a good postoperative recovery, accom-
panied by transient diabetes insipidus. Ophthalmo-logical assessment was performed six dayspostoperatively. Visual acuity was 6/5 in each eye. Inthe right he could read 5 out of 10 Ishihara plates and8 out of 10 in the left. Visual fields showed markedimprovement, with disappearance of the centralscotomata and expansion of the peripheral fields. Bytwo months postoperatively his vision was judgednormal. The optic discs were also normal.Comment. A craniopharyngioma was removed
after the patient had presented with a five-monthhistory of blurring of vision and headaches. Therewas bilateral optic neuropathy, with central scoto-mata and normal optic discs. At operation a prefixedchiasm allowed compression in the midline frombehind and above by a hard tumour. Rapid completerecovery ensued, suggesting that the visual failurehad been secondary to a temporary compressive con-duction block.
Discussion
FEATURES OF CASES PRESENTEDAll the four cases presented were diagnosticproblems, and ophthalmologists were often misledby the normality of the optic discs. Visual loss was
454
on 7 May 2018 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.68.7.449 on 1 July 1984. D
ownloaded from
Bilateral central scotomata due to intracranial tumour
c-w,12/3182
*::~~ ~ ~ ~ ~...3: 2lV 4.
*:. 6
:.~~~~~~~i
a U
00
Fig. 4a Case 4. Visualfields.
bilateral in three cases and initially unilateral in onecase (olfactory groove meningioma). Initial diagnosesincluded migraine, optic neuritis, and toxic/nutri-tional amblyopia, and the first case was furtherconfused diagnostically by a retinal detachment.Symptoms suggestive of intracranial optic nerve
compression included headaches, usually non-specific, though accompanied by nausea and vomitingin one patient. Ocular pain was not a symptom. Inone case the only neurological sign was loss of smell.Thus the early recognition of this condition is depen-dent solely on the skill of the ophthalmologist inrecognising the organic nature of the field defect andarranging the appropriate CT scans. A review of thevarious disorders that may present in this way hasbeen published elsewhere.
Fig. 4b Case 4. CTscan showing cystic suprasellar lesion.
DIFFERENTIAL DIAGNOSIS OF BILATERAL OPTIC
NEUROPATHY(a) Centrocaecal scotomata. In the presence of anormal macula, bilateral central scotomata usuallysuggests intrinsic optic nerve disease. The majority ofthese cases are due to hereditary factors or havenutritional or toxic causes.Acute optic neuritis may be bilateral in adults and
is usually associated with neurological signs inmultiple sclerosis, though bilateral chronic demye-lination is a recognised entity. More often the secondeye has been affected after an interval. Leber's opticneuropathy may also present acutely in the same agegroup, and a positive family history will be thedistinguishing feature.
Ischaemia of the retrobulbar portion of the opticnerves is a factor in some types of bilateral opticneuropathy. Subacute or delayed radiation necrosis,usually following postoperative radiation of sellatumours,23 and post-traumatic optic neuropathy,4may have an ischaemic basis.
(b) Compressive causes. Subfrontal gliomas andmeningiomas cause visual disturbances among theirearliest manifestations,5 but unilateral visual loss withoptic atrophy and much later involvement of thesecond eye and chiasmal compression is the rule.Jefferson" laid particular stress on this asymmetry,with the production of a Foster-Kennedy syndrome.Basal lesions of the frontal lobe cause visual loss withcentral scotomata and 'choked discs' but rarelybilaterally.7
Central field defects with pituitary adenomas havebeen infrequently reported. Hendersonx describedbilateral central scotomata in 2-5% of 243 patients,and Hirsch and Hamlin' reported central visual lossin 6 out of 59 cases, but it is not clear whether any ofthese were bilateral. Kelly "' described bilateralcentral and hemianopic scotomata with pituitaryadenomas.
455
on 7 May 2018 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.68.7.449 on 1 July 1984. D
ownloaded from
N. G. R. Page and M. D. Sanders
Fig. 4c Case 4. Airencephalogram confirming thelesion which is deforming the 3rdventricle (arrowed).
Craniopharyngomas usually cause bitemporal fielddefects. Wagener and Love" described 29 patientsand later Ross Russell and Pennybacker'' discussedthe clinical and ocular findings in a further 16 patientswith operatively proved craniopharyngioma. Therewere no cases of bilateral scotomata in these groups,though there were four bitemporal scotomata. Earlierone out of four cases cited by Cushing"' had bilateralcentral scotomata.
Suprasellar meningiomas very rarely cause bilateralvisual failure with central scotomata; none occurredin a series of 83 cases '4 and one example was describedby Rucker and Kearns.' 5Meningeal carcinomatosis with compressive cuffing
and perhaps infiltration frequently involves bothnerves with progressive visual loss." Bilateral opticneuropathy will be accompanied by orbital signs whencompression at the apex occurs in dysthyroid eyedisease.
(c) Miscellaneous. Infiltrating optic nerve gliomasor hamartomas, particularly when arising in the intra-cranial portion of the nerve or chiasm, 7 causebilateral loss of vision, and central scotomata may bea feature. In contrast, optic nerve sheath meningiomasinvolve the second eye late in the natural history. '8 Anormal appearance of the discs is unlikely with thesetumours.
Direct infiltration can occur from primary orsecondary nasopharyngeal or sphenoid sinus malig-nancies. Optochiasmatic arachnoiditis, lymphoreti-cular infiltration, and syphilitic optic atrophy arefurther causes of bilateral visual loss.
The authors thank Dr R. W. Ross Russcll for allowing them toreport details of the paticnt undcr his carc (case 3).Dr Page is supported financially hy the Smith Charity.
References
I Moscicy IF, Sainders MD. Comnputerized tomographyl in nieuro-ophthalmnology. London: Chapmian ind Haill, 1982.
2 Rosengren B. Two cascs of atrophy of the optic nervc afterprevious roentgen treatmcnt of the chiasmal region and the opticncrves. Acta Ophthaltnol (Kbh) 1958; 36: 874-8.
3 Hairris JR, Lcvene MB. Visual complications following radiationfor pituitary adenomats and crainiopharyngiomas. Radiology 1976;120: 167-71.
4 Ticho U, Fcinsod M. Traumatic optic ncuritis. Annti Ophthalinol1973; 5: 43()-2.
5 Hubcr A. Eye signs and symptoms in hrain tumours. S Afr ArgOftialnol 1979; 6: 31-47.
6 Jeffcrson G. The Doync lecturc: on comprcssion and invaision ofthe optic ncrvcs and chiasma hy neighhouring gliomas. TranisOphthalmnol Soc UK 1945; 65: 261-30)4.
7 Lillic WI. Ocular phcnomcna produced hy basal lcsions of thefrontail lobe. JAMA 1927; 89: 2)99-10)3.
8 Hcnderson WR. Pituitary adenomata; follow up study of surgicalrcsults in 338 cases (Dr Harvey Cushing's scrics). BrJ Surg 1939;26: 81 -92 1.
456
on 7 May 2018 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.68.7.449 on 1 July 1984. D
ownloaded from

Bilateral central scotomata due to intracranial tumour
9 Hirsch 0, H-amlin H. Faitc of visuail ficids and optic discs inpituitary tumours. A ]nJ Opihthlmnol 1954; 37: 880-5.
Il) Kcily RE. Lcsions of the optic chilasm duc to comprcssion. TransOphtialnol Soc UK 1962; 83: 149-64.
11 Wagencr HP, Lovc JG. Ficlds of vision in cases of tumour ofRathkc's pouch. Archi Ophtlhahnol 1943; 29: 873-87.
12 Russcll RWR, Pcnnyhaickcr JB. Craniopharyngioma in thecldcrly. J Neurot Neurosl(rg P.yhiatrs 1961; 24: 1-13.
13 Cushing H. The chiasmail syndromc of primary optic atrophy andhitemporal ficid dcfccts in adults with normail scila turcica. ArchOphthalnot 193t); 3: 5115-51, 704-35.
14 Finn JE, Mount LA. Meningiomais of the tubcrculum scilac and
plainum sphenoidailc: a revicw of 83 cascs. Arcli Ophthahlol1974; 92: 23-7.
15 Rucker CW, Kcarns TP. Mistaikcn diagnoscs in somc catscs ofmcningiomat. A ]nJ Ophthalmot 1961; 51: 15-9.
16 Tcrry TL, Dunphy EB. Mctastaitic circinomi in hoth optic ncrvcssimulaiting rctrobulhar ncuritis. Arc/i Ophiliahimol 1933; 10:611-4.
17 Spoor TC, Kcnncrdell JS, Miartinez AJ, Zoruh D. Mailignaintgliomais of the optic ncrvc pathways. Tratis Ain Oplitlimienol Soc1972; 70: 490)-528.
18 Hairt WM Jr, Burdc RM, Klingclc TG, Pcrlmuttcr JC. Bilatcraloptic ncrvc shcith mcningiomais. Arc/i Ophtha/ino/l 19801); 98:149-5 1.
457
on 7 May 2018 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.68.7.449 on 1 July 1984. D
ownloaded from