bilateral macular dysplasia ('colobomata') and … · bilateral scleral ectasia with a...
TRANSCRIPT

British Journal of Ophthalmology, 1985, 69, 691-699
Bilateral macular dysplasia ('colobomata') andcongenital 'retinal dystrophyA T MOORE, D S TAYLOR, AND ANN HARDEN
From the Hospitalfor Sick Children, Great Ormond Street, London WCIN3JH
SUMMARY Three unrelated patients with bilateral macular dysplasia ('colobomata') with norelevant family history were found to have- absent or substantially abnormal electroretinograms,implying that there was an associated retinal dystrophy. This may suggest that the macular lesionsare associated with a global failure of retinal development, with a regional preponderance ratherthan a purely localised cause such as an intrauterine infection. It is important to distinguishbetween congenital infections such as toxoplasmosis and developmental macular colobomata,which have a somewhat similar ophthalmoscopic appearance as a cause of bilateral macularabnormalities seen in young children, since they have different implications for genetic advice andfuture ophthalmic care.
Until intrauterine infection with Toxoplasma gondiiwas recognised as a cause of certain congenitalmacular abnormalities and serological tests for toxo-plasmosis became available, many macular lesionswhich are now more readily diagnosed as those ofcongenital toxoplasmosis were classified as con-genital macular 'colobomata.' Ida Mann pointed outthat not only were most of these cases due tointrauterine infection, but the term macular'coloboma' is itself a misnomer, as it does not resultfrom a defect in closure of the fetal fissure. ' The termmacular dysplasia may be preferable. There is,however, a group of patients with bilateral macular'colobomata' or dysplasia, in whom the defect isthought to result from an abnormality of develop-ment of the macula unrelated to fetal fissure closuredefects. A developmental mechanism is likely inthose cases with a family history, or when there areother systemic abnormalities which form part of arecognisable syndrome. It may not be possible todistinguish between inflammatory and develop-mental aetiology on clinical appearance alone.2
Bilateral macular 'colobomata' have been des-cribed in sibs' and in two or more successivegenerations,2""' and have been reported in associa-tion with two different systemic abnormalities. Suchan association has been proposed as evidence ofprimary developmental aetiology for the macularCorrespondence to Mr D S Taylor, FRCS.
lesions. Sorsby2 described a family group consistingof a mother and five children all of whom hadbilateral pigmented 'colobomata' in association witha rare skeletal abnormality-apical dystrophy of thehands and feet. Bilateral macular 'colobomata' havealso been described in idiopathic infantile hyper-calcuria." 2 This condition may be inherited in anautosomal recessive manner, as it has been reportedin two sibs from a consanguineous marriage."A third group of patients with macular
'colobomata' have electrophysiological evidence of amore widespread retinal dystrophy. An absent orabnormal electroretinogram has been reported inassociation with familial macular 'colobomata'" andin 'colobomata' associated with idiopathic infantilehypercalcuria." Macular 'colobomata' and an absentelectroretinogram have also been reported in Leber'samaurosis'3'4 and retinitis pigmentosa.'1 6 Not allfamilial cases have abnormal electrodiagnostic tests,however. Tamaki et al.'" found a normal electro-retinogram, electroculogram, and dark adaptometryin all affected family members in their pedigreeof autosomal dominantly inherited macular'colobomata.'We present here three cases of bilateral macular
dysplasia with abnormal electrodiagnostic findings,in whom the macular lesions are likely to be develop-mental in origin rather than secondary to intrauterineinfection.
691
copyright. on 20 S
eptember 2018 by guest. P
rotected byhttp://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.69.9.691 on 1 S
eptember 1985. D
ownloaded from

A TMoore, D S Taylor, andAnn Harden
Case reports
CASE 1This female infant was first seen at the Hospital forSick Children at 13 months, of age. She was thesecond child born to unrelated parents, and there wasno relevant family history. The mother had twoupper respiratory tract infections during pregnancyat three and eight months, but the pregnancy wasotherwise uneventful. There was a normal delivery atterm. At birth the infant was noted to have an extrathumb on the right hand (Fig. 1), but initial examina-tion was otherwise normal. The extra digit wasexcised at 11 months. At 4 weeks the parents hadnoticed that the child had 'wobbly eyes' and that hervision appeared very poor. She was seen by a localophthalmologist, who found poor visual attention,nystagmus, and bilateral macular abnormalities.When the child was first examined at the Hospital
for Sick Children she showed no response to light;there were 'roving eye movements' and absent pupil-lary responses to light. The anterior segments werenormal, but both fundi showed similar abnormalappearances (Fig. 2). Both discs were pale, and theretinal blood vessels were attenuated. There werescattered peripheral retinal pigmentation andbilateral non-pigmented macular 'colobomata.' Inthe right eye there was an excavated, non-pigmented'coloboma' with ectatic sclera at the base. A few largechoroidal blood vessels were visible at the base, butno retinal vessels crossed the defect. In the left eye
rig.2a easel. runauspnotograpnhojrignteyesnowingpolecoloboma, with afew choroidal vessels in the base.
Fig. 1 Case l. Plain x-ray ofright handshowingpolydactylism.
there was a non-ectatic macular 'coloboma' withsmall and medium sized choroidal vessels visible inthe base. Again no retinal vessels crossed the defect.General examination was normal apart from a scar atthe right thumb. Developmental assessment revealedthat she was developing normally for a blind child ofher age. There was no recordable electroretinogramor flash visually evoked potential on two occasions(Fig. 3). X-ray of the hands and feet showed a shortright first metacarpal with an abnormal epiphysis ofthe terminal phalynx, but was otherwise normal. ACT scan showed high density areas in the retina ofboth globes, which may represent calcification in the
thready vessels and a non-pigmented ectatic macular
692
copyright. on 20 S
eptember 2018 by guest. P
rotected byhttp://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.69.9.691 on 1 S
eptember 1985. D
ownloaded from

Bilateral macular dysplasia ('colobomata') and congenital retinal dystrophy
'e was similar to the right, but the coloboma was non-ectatic.
base of the macular 'coloboma' (Fig. 4), but was
otherwise normal. Other investigations includingserum and urinary amino acids, urinary reducingsubstances, urinary calcium excretion, syntheticvasopressin urinary concentration tests, and skullx-ray were normal. Toxoplasma dye test was negativeat 1 in 16 dilution in the mother and baby on twooccasions. Serological tests for cytomegalovirus,rubella, and herpes simplex were negative in motherand child. The fundi of both parents and her oldersibling were examined and found to be normal.
CASE 2
This young girl was first seen at the Hospital for SickChildren at 3 years of age. She is the only child bornto unrelated parents and there is no relevant familyhistory. The mother had severe essential hyperten-sion and depression, and was taking methyldopa,propranolol, and amitriptyline during the pregnancy.She required several admissions during the preg-nancy, because of the raised blood pressure, and thedelivery was at 38 weeks by caesarian section. Birthweight was 2040 g. The placenta was small and therewas slight meconium staining at delivery. At 6 weeksher mother had noticed 'wobbly' eyes and thoughtthat her vision was poor. However, over the follow-ing months her vision appeared to improve. Whenthe girl was first seen at the age of 3 years there washorizontal nystagmus, with an abnormal head pos-ture and a face turn to the left. There was a rightdivergent squint, but ocular movements were full.Both fundi were abnormal (Fig. 5). The discs were
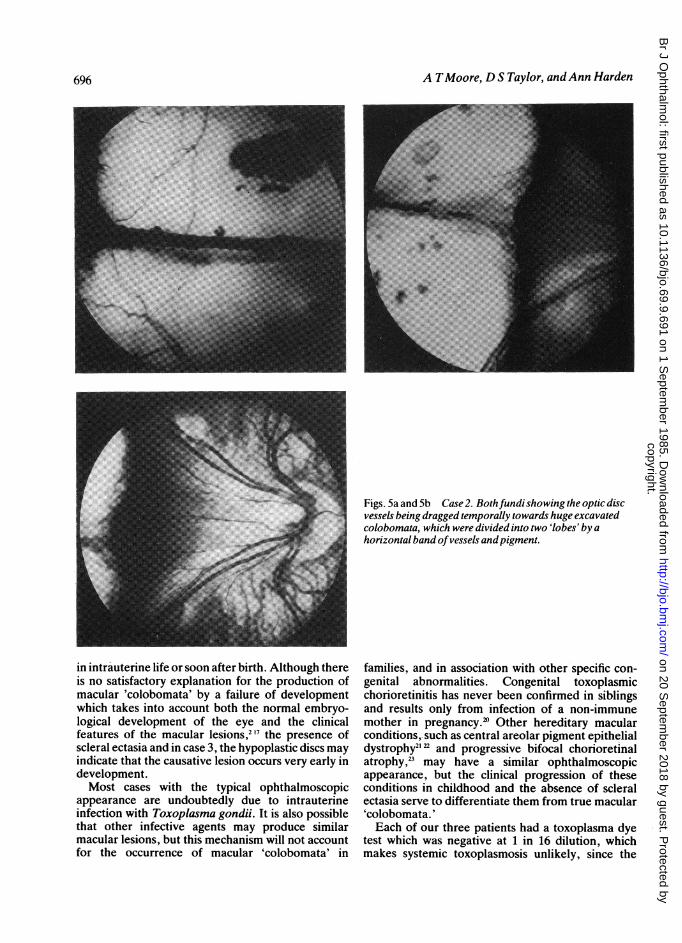
normal, but the vessels, which were of normalcalibre, were dragged temporally to large, deep, non-pigmented macular defects. There was markedbilateral scleral ectasia with a line of pigment andblood vessels stretched across the defect, giving it abilobed appearance. Large choroidal vessels crossedthe base of the 'coloboma' in each eye. Generalexamination had revealed no other systemic abnor-malities. She has shown normal intellectual develop-ment; though she has been investigated on severaloccasions for poor weight gain and short stature, noorganic cause has been found. A toxoplasma dye testcarried out at the age of 6 months was negative at 1 in16 dilution.She was last reviewed in May 1983 at the age of 6,
when she was managing well at a normal school.Distance visual acuity was 6/36 in each eye andbinocular near vision 6/9 on a reduced Snellen chartat 10 cm. There was horizontal nystagmus, anabnormal head posture, with either left or right faceturn, and an alternating divergent squint. Colourvision was normal on testing with Ishihara plates ineach eye. Visual field examination showed bilateralrelative central scotoma with normal peripheralfields. The fundus appearances were unchanged. Theelectroretinogram was of markedly reduced ampli-tude (Fig. 3). The flash visually evoked potential wasof normal latency and wave form, but the major earlycomponent was of reduced amplitude.
CASE 3This Greek boy was first seen at the Hospital for Sick
693
copyright. on 20 S
eptember 2018 by guest. P
rotected byhttp://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.69.9.691 on 1 S
eptember 1985. D
ownloaded from

A TMoore, D S Taylor, andAnn Harden
ERG
Normal control >'
Age 17m
Case 1
Age 15m
Case 2
Age 6y
Case 3
Age 1 5.y
20AJv[
/
VEP
Time marker 25msFig. 3 ERG (recordedfrom bridge ofnose) and VEP (midoccipital) in response toflash stimulus. Eyes open; both eyesstimulated simultaneously at arrow. Note absent or verypoorERG in cases 1, 2, and3 compared with normal control. In caseI no VER is recordable; in case2 the VEP earlier components in thefirst 75 ns are small andpoorly defined compared withnormal. In case3, however, a well defined VEP is seen which issomewhat unusually large, but within normal limits. Thesefindings contrast with cases oftoxoplasmosis retinitis which have notshown gross ERG abnormalities.
Children at the age of 15 years. He had been referredto Professor Otto Wolff for investigation of renal,metabolic, and respiratory problems. He was born tounrelated parents at 28 weeks gestation. The preg-nancy had been normal until that point. Birth weightwas 1500 g, and he required oxygen, withoutmechanical ventilation, for about 30 days. He hadpoor vision and nystagmus from infancy but was ableto attend a normal school, where he was said to be'slow.' He also had hearing problems and had worn ahearing aid from the age of 6. At 10 years he had beennoted to get short of breath very easily, and hisrespiratory difficulties gradually increased, which ledto investigation in Greece. This had revealed poly-cythaemia, interstitial lung disease, and radiologicaland biochemical evidence of rickets.When he was examined in London his visual acuity
was 3/60 right and 6/60 left, with +5-00 sphericaldioptre correction in each eye. Binocular visualacuity was 6/60 for distance and 6/18 Snellen for near.With a low-vision aid he was able to read a 6/6reduced Snellen chart at 10 cm. There was manifesthorizontal nystagmus and an alternating divergentsquint. Ocular movements were full and pupilreactions were normal. Both fundi were abnormal(Fig. 6).
In the right eye there was a deeply excavatedmacular defect with two large choroidal vessels, oneof which appeared to penetrate the sclera in themanner similar to a vortex vein, crossing the base. Athin membrane containing pigment was suspendedacross the defect at the level ofthe normal retina. Theoptic disc was vertically oval and was segmentallyhypoplastic, being deficient in the area of the papillo-
694
copyright. on 20 S
eptember 2018 by guest. P
rotected byhttp://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.69.9.691 on 1 S
eptember 1985. D
ownloaded from

Bilateral macular dysplasia ('colobomata') and congenital retinal dystrophy
rig. 4 uase 1. (- i scun(rcmareas at both posteriorpoles.
macular bundle-resulting in a kidney-shaped disc.In the left eye the optic disc was similar in shape andthere was a large macular defect, but no underlyingscleral ectasia. The retinal pigment epithelium andsmall choroidal vessels were absent in the area of thedefect, but medium and large sized choroidal vesselstraversed the base. A few retinal vessels crossed theperiphery of the lesion. The peripheral retina wasnormal in each eye. The electroretinogram wasreduced in amplitude (Fig. 3). The flash visuallyevoked potential was well formed and of the usuallatency and waveform.
General examination showed that he was belowthe tenth percentile for both height and weight, andthe head circumference was on the third percentile.He was slightly cyanosed, with finger clubbing, butchest examination was normal. He was of subnormalintelligence, had marked genu valgum, but systemicexamination was otherwise normal. Extensiveinvestigations were carried out to elucidate the cause
of his systemic and ocular problems and to try toprovide a single unifying diagnosis. This was notpossible. A chest x-ray showed the appearance ofinterstitial lung disease, and lung function testsconfirmed that there was a diffusion defect. A lungbiopsy, however, was not diagnostic; the histologicalappearances were consistent either with a viral pneu-monia or a disease characterised by circulatingimmune complexes. Renal investigation revealedrenal tubular abnormalities with renal tubular pro-teinuria, aminoaciduria, glycosuria, and an inabilityto acidify or concentrate the urine normally. Renalultrasound and intravenous pyelogram were normal.A renal biopsy showed mild mesangial proliferationand tubular atrophy. There was no interstitial
nephritis, and immunofluorescence tests were nega-tive for IgG, IgA, and IgM. A skeletal survey showedradiological evidence of healing rickets. A CT scanshowed colpocephaly (Fig. 7). An audiogramrevealed bilateral sensorineural hearing loss. A toxo-plasma dye test was negative at 1 in 16 dilution, andvenereal disease reference laboratory (VDRL) andTreponema pallidum haemagglutination (TPHA)tests were negative. Many other investigationsincluding immunological studies and viral serologywere negative. No unifying diagnosis was made. Hewas treated empirically with oral steroids with someimprovement in his respiratory function.
Discussion
Ida Mann' '7 classified macular 'colobomata' intothree types based on their ophthalmoscopic appear-ance. The first and commonest type, the pigmentedmacular 'coloboma,' consists of a circular patch at themacula covered by an irregular mass of pigment,beneath which the choriocapillaris is absent, butsmall patches of bare sclera and a few choroidalvessels may be seen. There is no scleral ectasia, andnormal retinal arterioles pass over the pigmentedarea, indicating that the main lesion is deep to theinner retinal layers at least. The second type, the non-pigmented 'coloboma,' Mann describes as a round oroval patch at the macula with a white base of baresclera which is usually ectatic to some extent. There isoften pigment clumping at the edge of the lesion, andretinal vessels stop at the margin of the coloboma,suggesting that in this type the retina is also involved.A third, rare, type is represented by those cases inwhich the macular 'coloboma' is associated withabnormal vessels which may form an anastomosiswithin the 'coloboma' or run forward from the lesioninto the vitreous.8 19 Not all cases of macular'colobomata' fall clearly into one of these threegroups, and intermediate types do occur. Each of ourthree cases had macular lesions of the non-pigmentedtype, and they also do not represent a completelyhomogeneous group. Mann has speculated that thethree types of lesions are caused by a destructiveprocess affecting the developing macular regionoccurring during the eighth or ninth month, fifth orsixth month, and second or third month of gestationrespectively.The various theories put forward to account for the
production of these macular lesions have beenreviewed by Mann' 17 and Sorsby.2 They fall into twomain groups. Firstly, there may be a failure of normaldevelopment of the eye, giving rise to the macularabnormality; or, secondly, the development of theeye may be initially normal but later become dis-organised by a pathological process, such as infection
695
copyright. on 20 S
eptember 2018 by guest. P
rotected byhttp://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.69.9.691 on 1 S
eptember 1985. D
ownloaded from
A TMoore, D S Taylor, andAnn Harden
Figs. 5a and 5b Case2. Bothfundi showing the optic discvessels being dragged temporally towards huge excavatedcolobomata, which were divided into two 'lobes' by ahorizontal band ofvessels andpigment.
in intrauterine life or soon after birth. Although thereis no satisfactory explanation for the production ofmacular 'colobomata' by a failure of developmentwhich takes into account both the normal embryo-logical development of the eye and the clinicalfeatures of the macular lesions,2'7 the presence ofscleral ectasia and in case 3, the hypoplastic discs mayindicate that the causative lesion occurs very early indevelopment.Most cases with the typical ophthalmoscopic
appearance are undoubtedly due to intrauterineinfection with Toxoplasma gondii. It is also possiblethat other infective agents may produce similarmacular lesions, but this mechanism will not accountfor the occurrence of macular 'colobomata' in
families, and in association with other specific con-genital abnormalities. Congenital toxoplasmicchorioretinitis has never been confirmed in siblingsand results only from infection of a non-immunemother in pregnancy.' Other hereditary macularconditions, such as central areolar pigment epithelialdystrophy2' and progressive bifocal chorioretinalatrophy,' may have a similar ophthalmoscopicappearance, but the clinical progression of theseconditions in childhood and the absence of scleralectasia serve to differentiate them from true macular'colobomata.'Each of our three patients had a toxoplasma dye
test which was negative at 1 in 16 dilution, whichmakes systemic toxoplasmosis unlikely, since the
696
copyright. on 20 S
eptember 2018 by guest. P
rotected byhttp://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.69.9.691 on 1 S
eptember 1985. D
ownloaded from

Bilateral macular dysplasia ('colobomata') and congenital retinal dystrophy
Fig. Sb Legend under Fig. 5a.
toxoplasma titre tends to parallel systemic involve-ment. The serological results do not, however,exclude congenital toxoplasmosis confined to theeye. Zscheile24 has reported a case of ocular toxo-plasmosis confirmed by histopathology in whom thetoxoplasma dye test was positive only in undilutedserum. Any toxoplasma titre may be significant in thepresence of typical chorioretinal lesions.25 However,each case reported here had an absent or substan-
tially abnormal electroretinogram, which cannot beexplained on the basis of a single macular toxoplasmalesion. The fact that the electroretinogram isabnormal in familial macular 'colobomata' and thoseoccurring as part of a recognisable syndrome pointsto a developmental origin for the macular lesions inour patients.Macular dysplasia has been reported in association
with several different skeletal abnormalities.2426
Fig. 6a Case3. The rightfundus shows a hypoplastic optic disc with the temporalsegment being most affected. The maculararea is replaced by a circumscribed ectatic area at the base ofwhich was a large choroidal vessel. A thin membrane containing afewspots ofpigment covered the coloboma at the level ofthe retina.
697
copyright. on 20 S
eptember 2018 by guest. P
rotected byhttp://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.69.9.691 on 1 S
eptember 1985. D
ownloaded from

A TMoore, D S Taylor, andAnn Harden
e leftfundus was similar butshowed betterpreserved choroid vessels andpigment, and there was no scleralectasia.
Case 1 had skeletal abnormalities consisting of anextra digit but showed none of the other features ofapical dystrophy and macular 'colobomata' describedby Sorsby.2 It is interesting that our patient had anextra thumb, as the most constant radiologicalfeature in Sorsby's family was a bifid terminalphalynx of the thumbs and great toes.The third case reported here had several systemic
problems which could not be related to his oculardisease. In addition to the macular lesions both discswere hypoplastic (Fig. 6), the nerve head beingespecially deficient on the temporal side where thepapillomacular bundle normally enters the disc.Optic nerve hypoplasia has not previously beenreported in association with macular dysplasia, andthe presence of the disc abnormalities suggests that inthis case the insult to the developing macular regionoccurred at an early stage in intrauterine develop-ment. The early theories of the pathogenesis of theoptic nerve hypoplasia proposed that there is aprimary failure of ganglion cell differentiation at the13-15 mm stage (6 weeks) or their failure to incor-porate into the optic stalk at the 19 mm stage(7 weeks).27 However, the frequent association ofoptic nerve hypoplasia with central nervous system(CNS) malformations, in particular midline abnor-malities such as absent or anomalous septumpellucidum" 9 or abnormalities of the corpuscallosum or with cerebral atrophy"' and poren-cephaly,3' has led to the suggestion that optic nervehypoplasia may also result from secondary atrophy ofthe optic nerves during intrauterine development,either as a result of transynaptic degeneration or by afailure of normal cortical induction or influence on
optic nerve development.' It is also possible that aninsult causing a CNS abnormality may also simul-taneously damage the developing optic nerve. Theoptic nerve hypoplasia in our patient may have beenrelated to his CNS abnormality (Fig. 7); optic nervehypoplasia has been reported in association withcolpocephaly.32 However, the unusual configurationof the hypoplastic discs, with the main defect beingrelated to the deficient papillomacular bundle sug-gests that the optic nerve hypoplasia in this case isrelated to the macular dysplasia.The implications of an abnormal electroretino-
gram for genetic counselling in a patient withbilateral macular dysplasia is not clear. It is evident
ig. 7 Case3. CTscan showing colpocephaly.
698
copyright. on 20 S
eptember 2018 by guest. P
rotected byhttp://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.69.9.691 on 1 S
eptember 1985. D
ownloaded from

Bilateral macular dysplasia ('colobomata') and congenital retinal dystrophy
that patients with bilateral macular dysplasia form aheterogeneous group; macular 'colobomata'(dysplasia) have been reported to have both domi-nant and recessive modes of inheritance. Dominantlyinherited macular 'colobomata' may occur alone9' orwith a specific skeletal abnormality2; the electro-retinogram may be normal"' or abnormal.9 An auto-somal recessive mode of inheritance is seen withmacular 'colobomata' in association with retinitispigmentosa'3 and Leber's amaurosis'3'4 and is thepossible mode of inheritance in 'colobomata' associ-ated with idiopathic infantile hypercalcuria." Thetwo cases reported by Phillips and Stokoe3 alsooccurred in siblings. All these patients had absent orseverely abnormal electroretinograms. It is difficultto give accurate genetic advice to parents who havehad one child with isolated macular 'colobomata' andno family history, especially since the condition mayhave different aetiologies. If the child has an absentelectroretinogram and has had poor vision andnystagmus from infancy, the condition is more likelyto resemble Leber's amaurosis in being inherited asan autosomal recessive condition.Our three cases also illustrate the variability of
visual acuity in this condition. Case 1 behaved as ablind child, whereas the other two patients achieveduseful vision despite extensive macular lesions and anabsent or abnormal electroretinogram. Thereforewhen a child is seen in infancy with bilateral maculardysplasia it may be better to give the parents acautiously optimistic visual prognosis, as the visionmay later prove to be better than expected from theophthalmoscopic appearance, though the long termcourse of the retinal dystrophy is less certain. IndeedClarke33 in 1927 described a child with bilateralmacular 'colobomata' to whom he gave a 'gloomy'visual prognosis who later went normally throughHarrow School, took a degree at Cambridge, and wasalways good at games, especially tennis. There maybe several interpretations of this achievement.We thank Professor 0 H Wolff for permission to report details ofcase 3 and Martin Johns for taking the fundus photographs. Mr A TMoore received financial support from the TFC Frost CharitableTrust.
References
1 Mann IC. On certain abnormal conditions of the macular regionusually classified as colobomata. Br J Ophthalmol 1927; 11:99-116.
2 Sorsby A. Congenital coloboma of the macula together with anaccount of the familial occurrence of bilateral macular colobo-mata in association with apical dystrophy of the hands and feet.BrJ Ophthalmol 1935; 19: 65-90.
3 Phillips CI, Stokoe NL, Newton M. Macula coloboma andretinal aplasia. Acta Ophthalmol (Kbh) 1981; 59: 894-900.
4 Phillips CI, Griffiths LD. Macula coloboma and skeletal abnor-mality. BrJ Ophthalmol, 1969; 53: 346-9.
5 Schott K. Uber das songenannte Kolobom der Makula. KlinMonastsbl Augenheilkd 1921; 67: 415-24.
6 Evans PJ. Familial macular colobomata. Br J Ophthalmol 1937;21: 503-6.
7 Clausen M. Typisches beiderseitiges hereditares Makula-Kolobom. Klin MonatsblAugenheilkd 1921; 67: 116.
8 Davenport RC. Bilateral 'macular coloboma' in mother and son.Proc R Soc Med 1927; 21: 109- 10.
9 Miller SA, Bresnik G. Familial bilateral macular coloboma. BrJOphthalmol 1978; 62: 261-4.
10 Tamaki S, Garcia CA, Katzmann J. Macular coloboma. InvestOphthalmol Vis Sci (Arvo suppl) 1979; abstr 15, 222.
11 Meier W, Blumberg A, Imahorn W, De Luca F, Wildberger H,Oetliker 0. Idiopathic hypercalcuria with bilateral macularcolobomata: a new variant of oculo-renal syndrome. HelvPaediatrActa 1979; 34: 257-69.
12 Gil-Gilberneau J, Galan A, Callis L, Rodrigo C. Infantileidiopathic hypercalcuria, high congenital myopia and atypicalmacular coloboma: a new oculo-renal syndrome? J PediatrOphthalmol 1982; 19: 7-11.
13 Margolis S, Sher BM, Carr RE. Macular coloboma in Leber'scongenital amaurosis. Am J Ophthalmol 1977; 83: 27-31.
14 Leighton D, Harris R. Retinal aplasia in association withmacular coloboma, keratoconus and cataract. Clin Genet 1973;4:270-4.
15 Heckenlively JR, Garcia CA, Maumenee IH, Shahininian J.Two retinitis pigmentosa syndromes. Invest Ophthalmol Vis Sci(Arvo suppl) 1979; abstr 3, 119.
16 Freedman J, Gombos GM. Bilateral macular coloboma, kera-toconus and retinitis pigmentosa. Ann Ophthalmol 1971; 3:664-6.
17 Mann I. Developmental abnormalities of the eye. 2nd ed.Philadelphia: Lippincott, 1957; 151-70.
18 Beaumont WM. Macular coloboma? Trans Ophthalmol Soc UK1891; 11:221.
19 Silcock QA. Vestigial hyaloid artery starting from a macularcoloboma. Trans Ophthalmol Soc UK, 1900; 20: 188.
20 Perkins ES. Ocular toxoplasmosis. Br J Ophthalmol 1973; 57:1-17.
21 Lefler WH, Wadsworth JAC, Sidbury JB. Hereditary maculardegenerations and amino-aciduria. Am J Ophthalmol 1971; 71:224-30.
22 Hermsen VM, Judisch GM. Central aerolar pigment epithelialdystrophy. Ophthalmologica 1984; 189:69-72.
23 Waheed AA, Wyse CT. Progressive bifocal chorioretinalatrophy. BrJ Ophthalmol 1968; 52: 742-50.
24 Zscheile FP. Recurrent toxoplasmic retinitis with weakly posi-tive methylene blue dye test. Arch Ophthalmol 1964; 71:645-8.
25 Smoling G, O'Connor GR. Toxoplasma dye test in ocularimmunology. Philadelphia: Lea and Febiger, 1981: 83.
26 Smith RD, Fireman RM, Sillence DO, etal. Brief clinical report:congenital macular colobomas and short limbed skeletaldysplasia. Am J Med Genet 1980; 5: 365-71.
27 Anonymous. Editorial: Small optic discs. BrJ Ophthalmol 1978;62:1-2.
28 De Morsier G. Etudes sur les dysraphies cranioencephaliques111. Agenesie du septum lucidum avec malformations duetractus optique la dysplasie septo-optique. Schweiz Arch NeurolNeurochir Pschiatr 1956; 77: 267-92.
29 Hoyt WF, Kaplan SL, Grumbach MM, Glaser JS. Septo-opticdysplasia and pituitary dwarfism. Lancet 1970; ii: 893-4.
30 Rogers GL, Brown D, Gray I, Bremer D. Bilateral optic nervehypoplasia associated with cerebral atrophy. J PediatrOphthalmol 1981; 18:18-21.
31 Greenfield PS, Wilcox LM, Weiter JJ, Adelman L. Hypoplasiaof the optic nerve in association with porencephaly. J PediatrOphthalmol 1980; 17: 75-80.
32 Garg BP. Colpocephaly: an error of morphogenesis? ArchNeurol 1982; 39:243-6.
33 Clarke E. Coloboma at the macula (both eyes). BrJ Ophthalmol1927; 11: 96-9.
699
copyright. on 20 S
eptember 2018 by guest. P
rotected byhttp://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.69.9.691 on 1 S
eptember 1985. D
ownloaded from