bio-medical waste management satish sinha. history of medical waste medical waste tracking act in us...
TRANSCRIPT

Bio-Medical Waste Management
Satish Sinha

History of medical waste
• Medical Waste Tracking Act in US
• I Draft Rules in India–1995• Final Rules in 1998, 2
amendments and 5 guidelines• Evolution of Rules and
Practices through National Experiences
• National Guidelines on BMW, Guidelines on Incineration, CTFs, Immunization Waste and Mercury

Various networks
NGOs• Health Care Without Harm
(HCWH)Injection safety:• SIGN (Safe Injection Global
Network)Anti-incineration: • GAIA (Global Anti Incinerator
Alliance)Mercury• Zero MercuryWorld Health Assembly• Patient safety

Stockholm Convention on Persistent Organic Pollutants
• an international environmental treaty
• aims to eliminate or restrict the production and use of persistent organic pollutants (POPs).
• entered into force on 17 May 2004 with ratification by 128 and 168 signatories.
Basel Convention
• Control of Tran boundary Movement of Hazardous Wastes and Their Disposal
• Minimize hazardous waste generation and dispose it nearest to the point of generation
Environmental Regulations
• Environment Protection Act, 1986• BMW Rules 1998• Municipal Waste (Management and Handling)
Rules, 2000• Atomic Energy Act• Hazardous Wastes (Management & Handling)
Rules, 1989• E-Waste Rules• Batteries (M&H) Rules 2001• Manufacture, Storage and Import of
Hazardous Chemicals rules, 1989

Patient safety and Bio-medical waste management
• In 2002 World Health assembly, passed a resolution calling member states to work for safety of Patients.
• In Oct. 2004, World alliance for Patient safety was formed, who have identified certain challenges in relation to safety of patients. First Challenge is “Clean care is Safer Care” (2005)
• A formal pledge committing to address health care-associated infection in the country was signed by Government of India.
Priority areas for Patient safety
• Safe clinical practices and hand hygiene
• Safe Surgical practices• Blood Safety • Safe Injections Practices • Health Care Waste Management Rules and guidelines are available but
implementation is very poor. Lack of training or poor training is also a factor. It has not been given the due priority by most of the states and dedicated budget is required. All states should focus on this.

Health care associated infections
• Complicate between 5-10% of admissions in acute care hospitals in industrialized countries
• It is estimated that this risk is up to 20 times higher in developing world
• At any given time, 1.4 million people worldwide suffer from HAI, and at least 50% of HCAI are preventable.

Unsafe injections
• India contributes to 25%-30% of the global injections (WHO, 1999)
• Annual injection usage ~ 3 – 6 billion, of this nearly two-thirds (62.9%injections) unsafe India CLEN Study 2002-04

Why Follow Universal Precautions
• The prevalence rate of blood born disease- Hepatitis B 38/1000, HIV 7/1000 (NACO 1993)
• Difficult to test each patient• NSI and other sharp injuries are
the key Canadian health issue, affecting 70000 people per year and costing around dollar 140 million.
• A safety programme at Toronto Hospital achieved 80% reduction in injuries within an year.

What is this concern for?
• Infectious waste (solid and liquid)• Sharps waste• Cytotoxic waste• Pharmaceutical waste• Radioactive waste• Chemicals and disinfectants• Pressurised containers

Headline of presentation to come here (on slide master)
BMW Rules and Key Actors
• Notified in 1998 • Concept of PPP model• Identified technologies and
standards• CPCB• SPCB• Department of Health
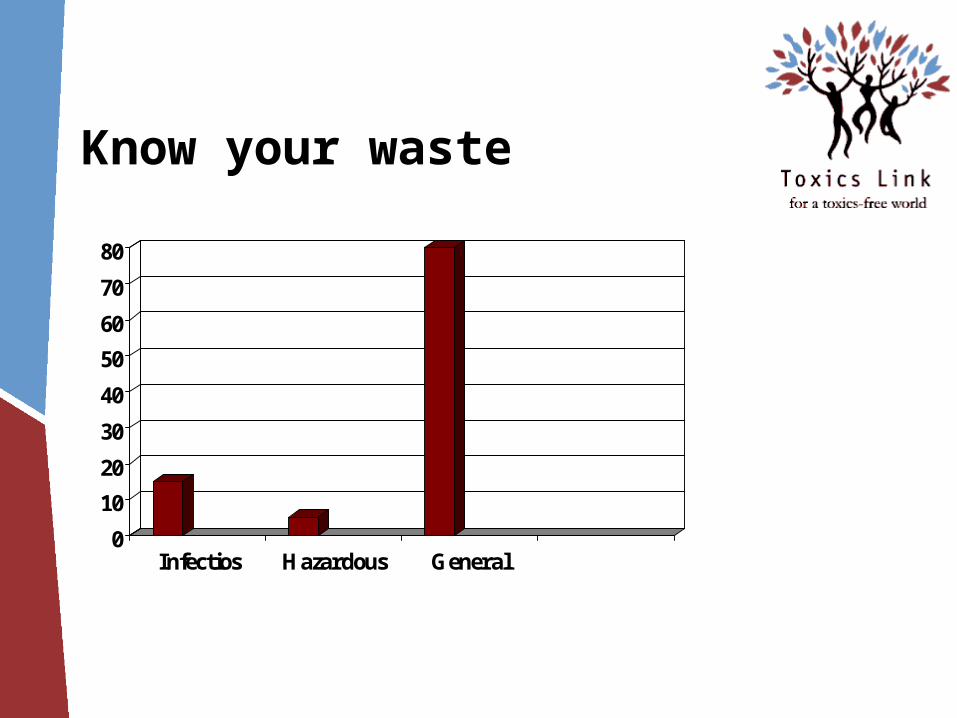
Know your waste
0
10
20
30
40
50
60
70
80
Infectios Hazardous General
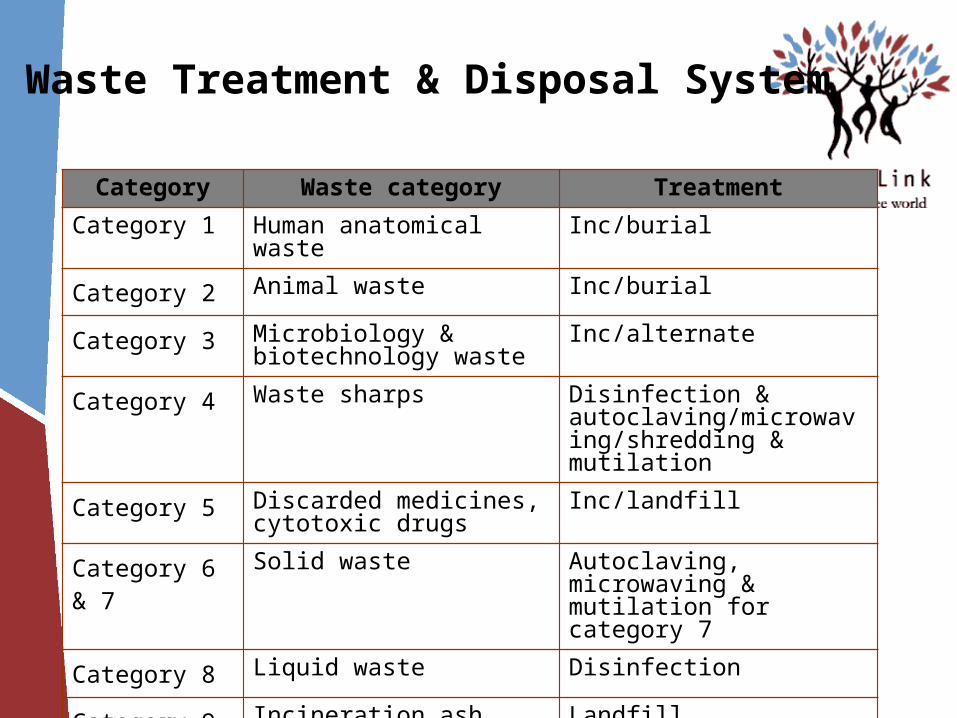
Waste Treatment & Disposal System
Category Waste category Treatment
Category 1 Human anatomical waste Inc/burial
Category 2 Animal waste Inc/burial
Category 3 Microbiology & biotechnology waste
Inc/alternate
Category 4 Waste sharps Disinfection & autoclaving/microwaving/shredding & mutilation
Category 5 Discarded medicines, cytotoxic drugs
Inc/landfill
Category 6 & 7 Solid waste Autoclaving, microwaving & mutilation for category 7
Category 8 Liquid waste Disinfection
Category 9 Incineration ash Landfill
Category 10 Chemical waste Drain/secured landfill after treatment
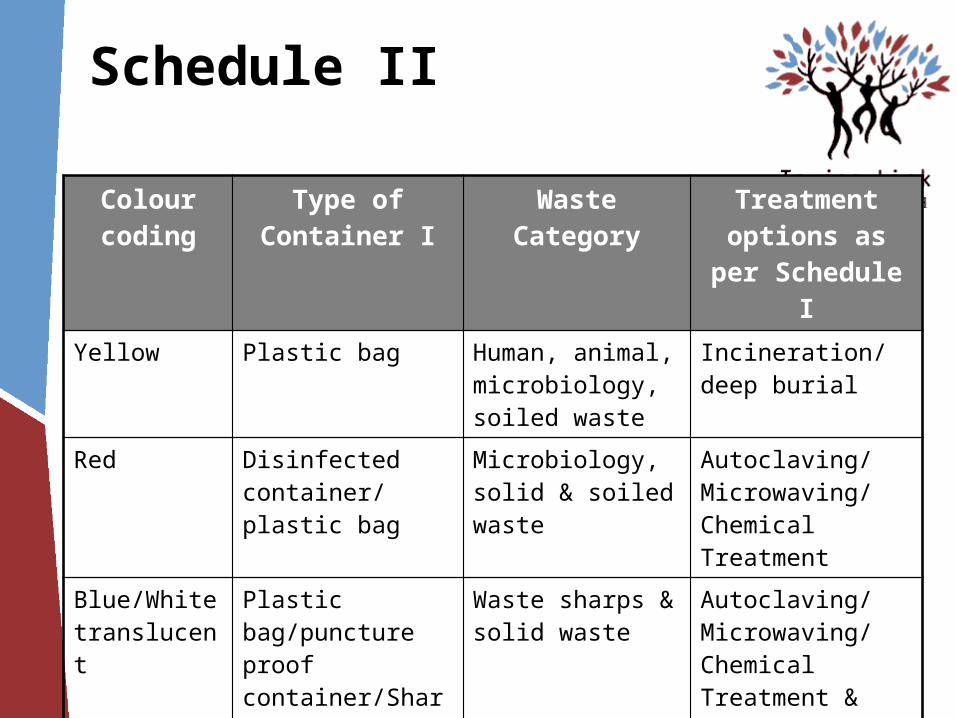
Schedule II
Colour coding
Type of Container I Waste Category Treatment options as per Schedule I
Yellow Plastic bag Human, animal, microbiology, soiled waste
Incineration/deep burial
Red Disinfected container/ plastic bag
Microbiology, solid & soiled waste
Autoclaving/Microwaving/Chemical Treatment
Blue/White translucent
Plastic bag/puncture proof container/Sharps Blaster
Waste sharps & solid waste
Autoclaving/Microwaving/Chemical Treatment & destruction/shredding
Black Plastic bag Discarded medicine, cytotoxic drugs, incineration ash & Chemical waste
Disposal in secured landfill
Bio-medical waste and technology
• Technology is only a fraction of the solution.
• Major components of waste management are:o Segregation of wasteo Waste minimisationo Reducing use of hazardous substances
or processeso Waste Audit

Approved treatment methods
• Autoclave
• Chemical disinfection
• Hydroclave
• Microwave
• Incineration
• Any other technology after CPCB approval
In house management of waste
• 1.Survey
2.Meeting with the heads of all the departments
3.Forming a waste management committee
4.Rounds of wards to see the functioning
5.Creating a model ward
6.Suggest equipment procurement
7.Formal training for all the nursing staff
8.Implementing the system throughout the hospital

Right Technology
Medical waste management is 80% segregation and 20% technology
• Incineration: Pathological Waste and Body Parts , no chlorinated plastics
• Autoclaving: All except body parts and pathological waste
• Microwaving: All except pathological waste and metals
• Chemical: Mainly plastics
Of site management of waste-Centralized Facilities
Draft Guidelines on Common facilities-
• Treatment facilities- 90% non-burn, 10% waste- burn
• Limits incineration to Categories 1&2
• Atleast 1 Km from residential areas. Acceptable in industrial area
• One operator allowed to cater upto 10,000 beds, situated within 150 km radius
• Segregation is the role of generator; operator can report mixing of waste to the prescribed authority
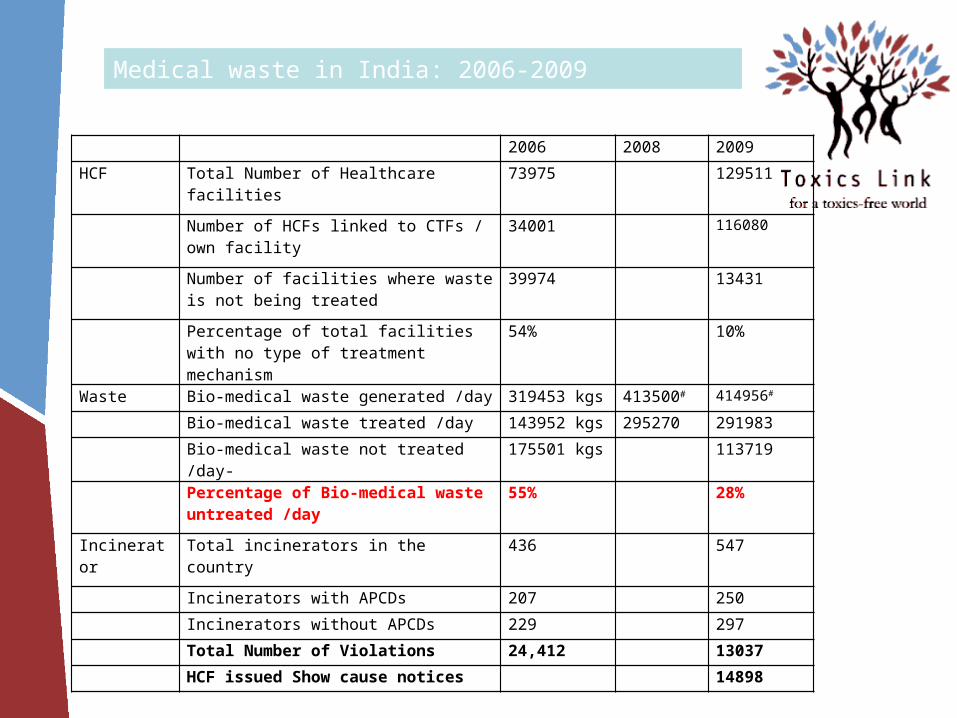
2006 2008 2009
HCF Total Number of Healthcare facilities 73975 129511
Number of HCFs linked to CTFs / own facility 34001 116080
Number of facilities where waste is not being treated
39974 13431
Percentage of total facilities with no type of treatment mechanism
54% 10%
Waste Bio-medical waste generated /day 319453 kgs 413500# 414956#
Bio-medical waste treated /day 143952 kgs 295270 291983
Bio-medical waste not treated /day- 175501 kgs 113719
Percentage of Bio-medical waste untreated /day
55% 28%
Incinerator Total incinerators in the country 436 547
Incinerators with APCDs 207 250
Incinerators without APCDs 229 297
Total Number of Violations 24,412 13037
HCF issued Show cause notices 14898
Medical waste in India: 2006-2009

Hurdles in Implementation Issues of Capacity Low priority Resource Allocation Fixed Mindset Injection safety, chemical safety and
waste management issues yet to find space in development planning

At the SPCB level
Capacity and resource Monitoring and control Transparency of processes Hierarchy of control Independent audits Awareness of community Increasing outreach of centralized
facility to rural areas
At the Hospital level
Mindset issues Involvement of senior
management Resource availability and
prioritising Government Hospitals biggest
defaulters Capacity Building Implementation bottlenecks Responsibility fixing Monitoring and Accreditation Periodic Waste audits wrt
economics

At the CTF level
Untrained Staff Poor maintenance of equipment Effluent Treatment Plants Maintenance of records No power back ups Closed door, non transparent Differential charges Flawed systems Profit driver Need for accreditation
Way Forward
Resource allocation for waste management
Maintaining a pool of trainers at block/ district levels
Stakeholders involvement Incorporation into curricula of medical,
nursing and paramedical colleges Up gradation to latest developments in
BMW management Waste minimizations policy Appropriate technology selection Pro-environment procurement policy

Emerging Issues
Mercury First mercury documentation in
healthcare in 2004: 3 kg/ hospital/year
Public notices by DPCC Mercury phase-out committee
formed by DHS Delhi hospitals to phase out mercury No new mercury equipment
procurement in Delhi government hospitals
HCEs aiming for ISO/ NABH to phase out mercury
Emerging Issues
Injection Safety Increased attention by hospitals Fines on unattended needles No to recapping Reporting of needle stick injury and
follow up
Chemical Safety Monitored use of Glutaraldehyde,
formaldehyde, benzene, cytotoxic drugs etc.
