biochemİcal evaluation of anemia prof.dr.arzu seven
TRANSCRIPT
BIOCHEMİCAL EVALUATION OF ANEMIA
Prof.Dr.Arzu SEVEN



Biochemical evaluation of anemia
• Hemolytic disorders resulting from erythrocytic enzyme abnormalities:
• a)enzymes of Emden-Meyerhof Pathway of anaerobic glycolysis
-hexokinase -glucose phosphate isomerase -phosphofructokinase -triosephosphate isomerase -phosphoglycerate kinase -pyruvate kinase

• b)hexose monophosphate pathway
-transketolase
-glucose 6-phosphate dehydrogenase(G6PD)
• c)glutathione pathway
-GSH peroxidase
-GSH synthetase

• d)purine pyrimidine metabolism
-adenosine triphosphatase
-adenosine deaminase
-pyrimidine-5'-nucleotidase

Pyruvate kinase deficiency
• Most common
• Autosomal recessive
• Mild severe
• İnability to synthesize ATP for RBC metabolism, ion gradients γ cell shape
• 2,3 BPG -O2 affinity
-O2 delivery to muscle γ fetus

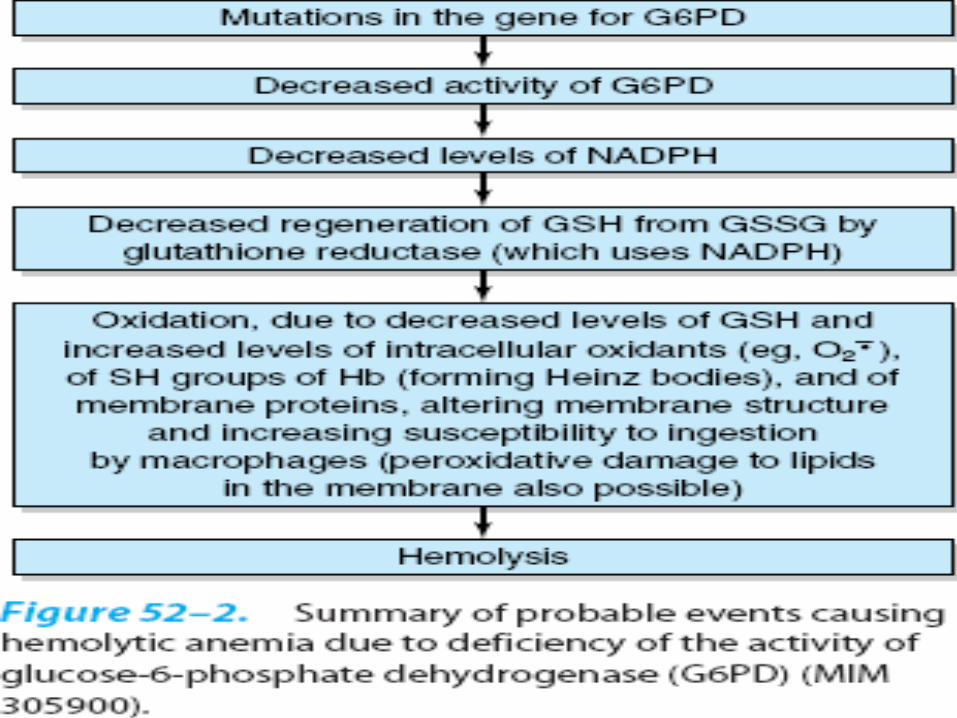
G6PD deficiency
• Genetic
• Mutation
• Common in Mediterenean γ Africo_Carribbean origins
• NADPH
• GSH can not be regenerated from GSSG
• GSSG , H2O2 , radicals

• Oxidative challenge: -oxidants (antimalarial primaquine,
aspirin, sulfonamids) -severe infections -fava beans• Primaquine sensitive hemolytic anemia • Peroxidation of lipids in RBC membrane RBC lysis

Iron deficiency anemia
• A common nutritional problem seen especially in menstruating γ pregnant women
• ♂ 1 mg iron/day
• Mensruating ♀ ~ 2mg iron/day
• Pregnant ♀ ~3mg iron/day
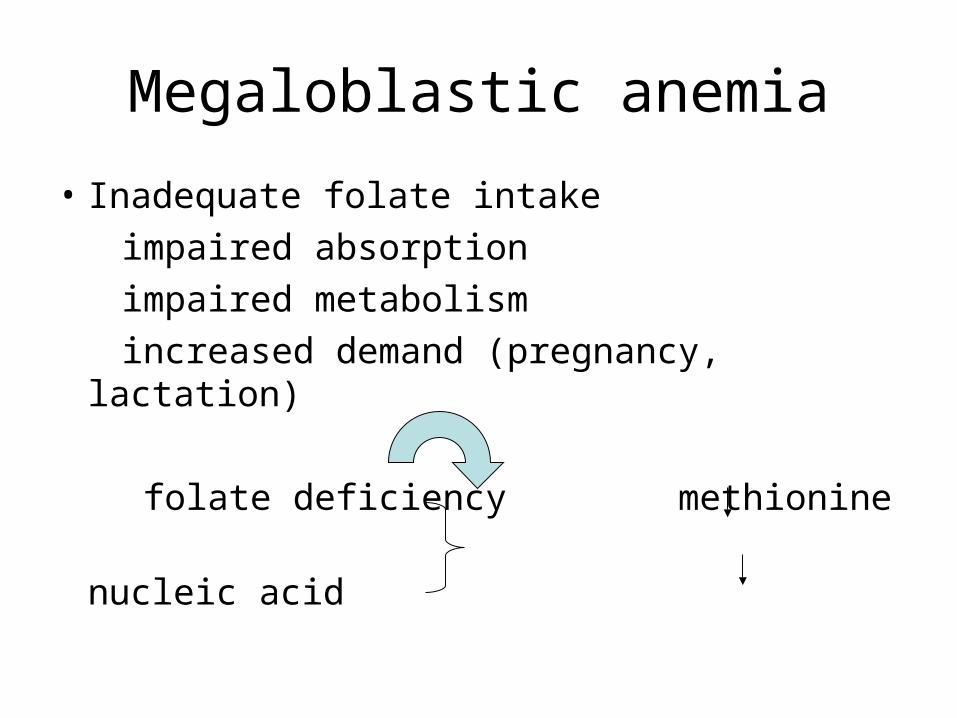
Megaloblastic anemia
• Inadequate folate intake
impaired absorption
impaired metabolism
increased demand (pregnancy, lactation)
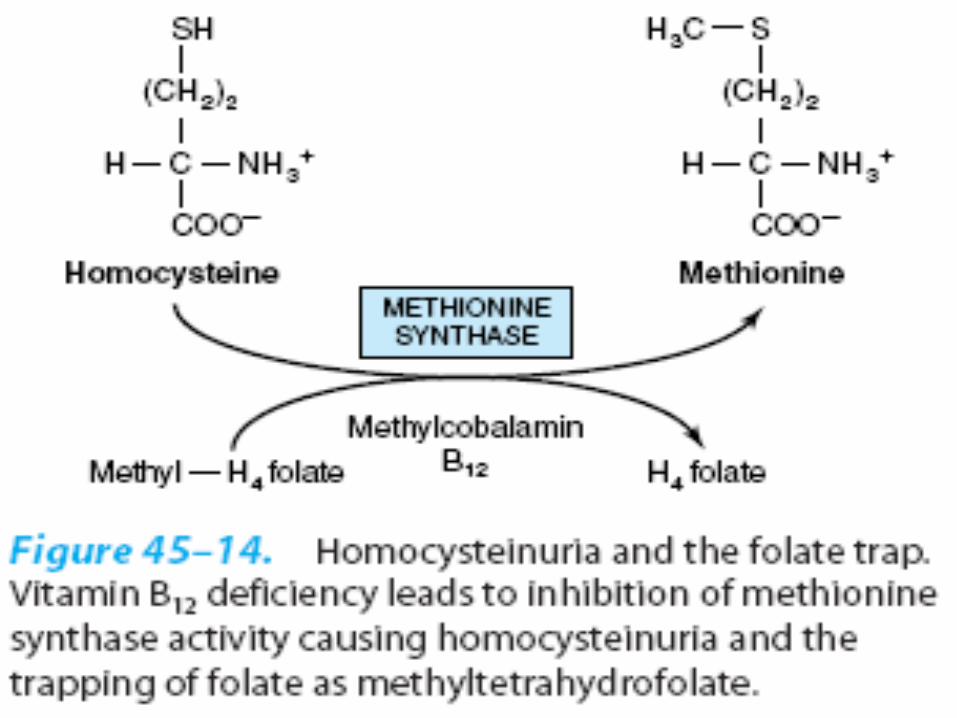
folate deficiency methionine
nucleic acid
• Enlarge blast cells in bone marrow • Macrocytic RBC with fragile membranes
tendency to hemolyze (macrocytic anemia) • Folate supplementation (400 mg/day)
during periconception period (4 weeks before γ 8 weeks after conception) prevents neural tube defects in spina bifida and hyperhomocysteinemia)

Pernicious anemia
• PA is a conditioned nutritional deficiency of cobalamin by failure of gastric mucosa to secrete IF
• Inadequate intake of vit B12 extremely rare• Defective production of IF most common• Genetically determined, but not
manifested until late in life

• vit B12 deficiency folate deficiency• IF deficiency in the stomach prevents
vit B12 absorption in terminal ileum• gastric surgery surgical removal of ileum IF (Crohn's disease)
vegans vit B12

• Gastrointestinal symptoms
(episodic abdominal pain, constipation
γ diarrhea)
• Atrophic gastritis
• Immune abnormalities:
antiparietal cell antibodies
anti-IF antibodies

• Liver disease associated with alcoholism may lead to folate_deficiency megalosblastic anemia
• During the investigation of the cause of megaloblastic anemia, folate must be given together with B12 vit.(to prevent neuropathy)

Correlation of vit.B12 and folate levels with clinical status:three laboratory tests need to separate four clinical situations
Clinical situation
Serum vit.B12 (pg/mL)
Serum folate
(ng/mL)
Red cell folate
(ng/Ml)
normal Normal
(200-900)
Normal(5-16),intermediate(3-5), or low(<3)
Normal(>150)
Vit.B12 deficiency
Low(<100) Normal(5-6) or high(>16)
Low(<150)
Folic acid deficiency
normal low low
Deficiency of both
low low low

Methods for the determination of vitamin B12 and Folic acid
• Microbial assay
• Competitive protein binding assay
• Immunometric assay

Indirect methods for assessment of vitamin B12
deficiency• Methylmalonic acid assay
• Measurement of homocysteine
• Deoxyuridine suppression test
• Vit.B12 absorption (Schilling) test
• Tests for intrinsic factor blocking antibodies

• Because vit.B12 is needed for the conversion of methylmalonic acid to succinic acid , patients deficient in vit.B12 excrete excess amounts of methylmalonic acid in urine

• Homocysteine is increased in the plasma of patients who are deficient in vit.B12 because their cells can not metabolise homocysteine to methionine at a normal rate
• The increase in plasma homocysteine may precede the typical signs of macrocytic anemia and decreased cobalamin

• Schilling test permits differentiation of causes of vit B12 deficiency (pernicious anemia or intestinal malabsorption)
