birgit humpert, ksc dietetic intern 2012-2013. our mission we advance health through research,...
TRANSCRIPT

Clinical Case StudyThe long road back to eating.
Birgit Humpert, KSC Dietetic Intern 2012-2013

Our mission
We advance health through research, education, clinical practice and community partnerships, providing each person the best care, in the right place, at the right time, every time.
Our vision
Achieve the healthiest population possible, leading the transformation of health care in our region and setting the standard for our nation.
Dartmouth-Hitchcock Medical Center

DHMCMary Hitchcock Memorial Hospital Teaching hospital Only Level 1 trauma center in NH 396 inpatient beds Major tertiary-care referral site for the region
Dartmouth-Hitchcock Clinic Geisel School of Medicine at DartmouthVeterans Affairs Center at WRJ, Vermont
Also Children’s Hospital at Dartmouth –CHaDNorris Cotton Cancer Center
Team of 21 Dietitians and Diet Technicians. 4 RD and 3 DT only inpatient 7 in- and outpatient 5 only outpatient 1 employee wellness
Work with other members of the medical team to ensure the best treatment for the patient.
Role of the RDs

Mrs. H. 56 years old married, lived with her husband
Original problem: gallbladder cancer◦ in November laparoscopic
cholecystectomy, ◦ radiation therapy after
Now: new mass, surgery
My patient

Gallbladder
Image: retrieved from National Cancer Institute

1. Cholelithiasis2. Cholecystitis3. Gallbladder cancer
Diseases of the gallbladder

Uncommon Risk factors:
being female Being Native American Patients with large gallstones With extensive gallbladder calcification due to cholecystitis
Signs and symptoms: Jaundice, pain above stomach, N/V, bloating, lumps
Difficult to detect and diagnose Most often adenocarcinom
Gallbladder cancer

Initiation: abnormal cells are formed
Promotion: abnormal cells multiply
Progression: tumor growth
Pathophysiology of Cancer
Excission of the tumor and lymph nodes Gastric antrectomy Antecolic anterior gastrojejunostomy Choledochojejunostomy
Surgery 1/17 DAY 0

http://studynursing.blogspot.com/2011/01/gastrojejunostomy.html

Assessment: Anthropometrics: 80.8 kg, 69.4 kg
(admission), 68-70 kg UBW, 160 cm, BMI 27.1 Pertinent labs: Hgb 9.4, albumin 2,
creatinine 0.39 Meds: pain meds, antibiotics, IV fluids,
metoprolol, fluconazole, heparin, esomeprazole, Reglan, Senna, Dulcolax
Needs: 1400 kcal (20 kcal/kg), 140 g protein (2 g/kg)
First nutrition assessmentDAY 7

Diagnosis: malnutrition in intraabdominal disease, postoperative ileus
PES Statement: NI-5.2 Malnutrition related to alterations in gastrointestinal tract structure/function AEB inability to eat sufficient energy and protein.Intervention: TPN176 g dextrose, 135 g AA, 40 g lipids

Same day: Difficulty breathing, tachicardia, ECG
abnormalitites, transferred to ICU Duodenal stump leak gastrostomy and feeding jejunostomy
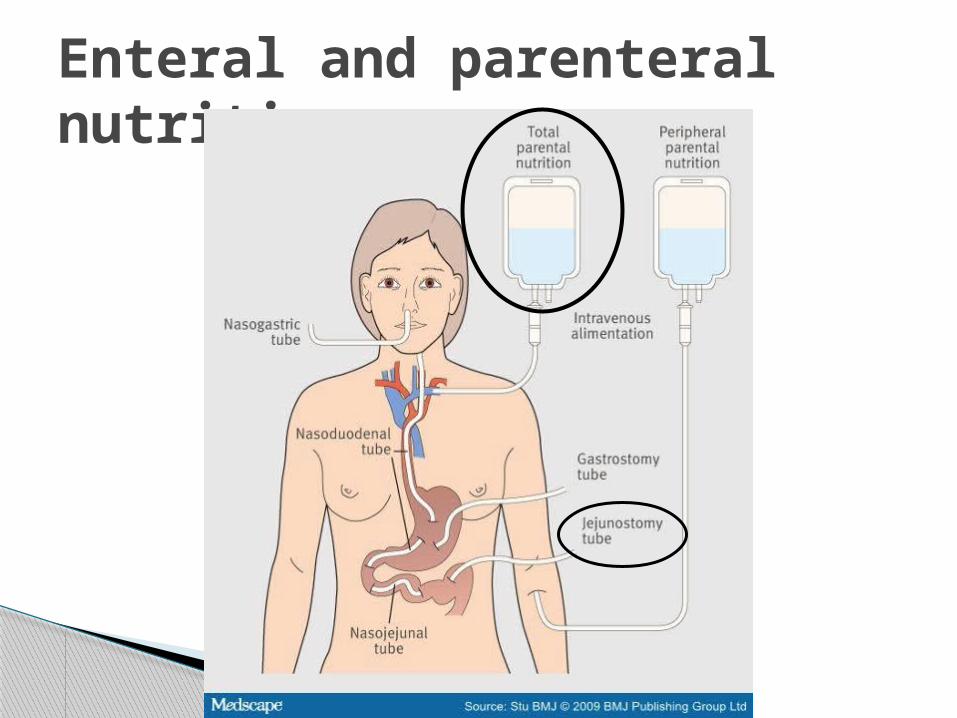
Enteral and parenteral nutrition
Assessment: Anthropometrics: 80.8 kg, 69.4 kg (admission), 160 cm,
BMI 27.1 Labs: Na 137, K 2.4, ch 104, CO2 26, BUN 20, creatinine
0.32, glucose 108, PAB 3 Meds: same + lasix In: 5442 ml, out 3530 ml Needs: 1400 kcal, 140 g protein
Diagnosis: NI-5.2 Malnutrition related to alterations in
gastrointestinal tract structure/function AEB Prealbumin of 3.
Consult for TF recommendationDAY 11

Intervention: Peptamen Bariatric at 56 ml/hr + 3 scoops
protein powder Initiate at 20 ml/h, advance 20 ml/h q 8-12
h as tolerated At goal: 1419 kcal, 143 g protein, 1129 ml
free water, 90% RDA vitamins/minerals
Monitoring/Evalutation: TF rates, tolerance, lab values

Pt complains of bloating and feeling of tightness
Also struggeling with pain control and diarrhea
TF is advanced more slowly 7 days after tube placement up to 30 ml/h,
25% of goal
Still TPN (Clinimix with electrolytes) 1200 ml to provide 853 cal, including 60 g protein
Advancement of TF

Mimics the action of naturally occuring somatostatin
Used to treat severe diarrhea Decreases pancreatic and GI secretion Inhibits gastrin, CCK, secretin, motilin Reduces smooth muscle contractions and
blood flow within the intestine
Octreotide

TF temporarily stopped due to leak from choledochojejunostomy site
Labs: Na 134, creatinine 0.52 Needs: 1750 kcal, 150 g protein, 2400 ml
continously Provided as premixed formula: (1032 cal,
151g protein, 125 g CHO, 0 g lipids)
New TPN assessment DAY 19

Assessment: Weight: 86.9 kg Labs: Na 133, creatinine 0.39, Ca 6.8,
Phos 1.4 In: 3150 ml, Out: 3132 ml Recommendation: Continue TPN Trophic feeding through J-tube Bile reinfusion Assess stool output prior to increasing TF
rate
TF restarted DAY 22
Bile important for absorption of fat and fat soluble vitamins, necessary for micelle formation
95% is recycled daily Loss of bile salt can decrease fat absorption up to 50% 1) reduce fat content of the diet 2) or collect bile and re-infuse
◦ Collect bile, strain with kidney stone strainer◦ Y-site into TF line ◦ 100-200 ml every 4 hours or continuously together with enteral nutrition ◦ via pump, gravity or syringe
Source: Practical GastroenterologyParrish, C.R., Quatrara, B. (2010). Reinfusion of Intestinal Secretions: A viable Option for
Select Patients. Nutrition Issues in Gastroenterology, Series #83, April 2010
Bile reinfusion
Nocturnal TF considered: Peptamen bariatric at 120 ml/hr over 12 hours recommended
Also still gets TPN cyclic (960 ml over 12 h at night) to provide 800 cal from 115 g protein, 100 g CHO, 0 g lipids
Still poor tolerance, feels full and nauseated, can’t exceed 20 ml/h
Preparing for discharge DAY 25
Persistent leak Preperations for discharge ongoing,
teaching of family regarding TF and TPN, rehab considered
Peritoneal fluid collection, drain placed Diarrhea on and off Changed mental status Rehab denied because of TPN
Progress DAY 23-33

Assessment: 78.6 kg Labs: mostly WNL, phos 1.5, albumin 1.5,
BUN 23, creatinine 0.21, prealbumin 5 Meds: zosyn, liquid tylenol, lomotil, zofran,
nexium Needs: 1400-1600 kcal, 140 g proteinRecommendation: Replete at 67 ml/hr x 12 h to provide 50-
60% of needs (804 kcal, 50 g protein, 676 ml free water, 80% RDA for vitamins/minerals
Change in TF DAY 35

S: Why do I have to get so much tube feeding?O: Meds: dulcolax supp. OrderedLabs: phos 1.1A: TF: average daily intake 231 ml (goal 804 ml) with steady increase, 29% Currently TF and TPN combined provide
74% of energy and 92% of protein needsP: TPN increased, phos provided
Evaluation DAY 37

Caused by inadequate intake, excessive loss (diuretics), redistribution
Results in anorexia, weakness, bone pain, dizziness, rhabdomyolysis, red blood cell dysfunction, heart failure, sudden death,
Hypophosphatemia

Blood in gastrostomy tube Fever, blood culture positive for G+ cocci Pneumonia CT scan revealed pyleophlebitis and liver
abcess TPN, TF is running at 20 ml, team does not
want to increase Pt is allowed ice chips
Readmission DAY 48
Labs: Na 131, K 3.4, ALT 555, AST 484, creatinine 0.34, Ca 7.4, PAB 3
Needs: 1650 kcal (25 kcal/kg), 100-135 g protein (1.5-2 g/kg)
Diet order: starting clear liquids today Plan: Cyclic TPN, recommendation for TF
advancement Replete 70 ml/h, to provide 1680 kcal, 105 g protein, 1420 ml free water, 100 % RDA vit/min
Reassessment DAY 51

“It was great to eat, it’s been months. I had cereal for breakfast.”Assessment: Cyclic TPN, TF running at 40 ml/h over 14 h,
pt gets full fast, declines snacks diet order: mechanical softPlan: Replete 65 ml/h over 12 hours to allow 2
more hours off TF, may encourage appetite Encouraged high protein food
Evaluation: DAY 56

TF stopped since she is eating and getting Boost
TPN continued, provides 740 kcal, 100 g protein, 100 g CHO
Reassessment on 3/19: 74 kg, PAB 3
Pt discharged home with VNA
TF stopped/discharge DAY 61

Weight: 68.9 kg Still on TPN, pt wants off Recall: cereal with 2% milk for breakfast,
toast w butter or grilled-cheese sdw with chicken-noodle soup for lunch, ½ Hamburger w potato wedges for dinner, vitamin water
800-900 kcal, 35-40 g proteinNeeds: 1700 kcal, 105 g proteinRecommendations: Add 500 kcal w calorie-dense food and fluids Increase protein
Update DAY 82

Resources:Calandra, T., Marchetti, O. (2004) Clinical Trials of Antifungal Prophylaxis among
Patients Undergoing Surgery. Clin Infect Dis. (2004) 39 (Supplement 4): S185-S192. doi: 10.1086/421955
Charney, P., Malone A.M. (2009). ADA Pocket Guide to Nutrition Assessment. 2nd edition. American Dietetic Association Chicago, IL.
Gallbladder and Bile Duct Disorders (2007). The Merck Manual for Health Care Professionals, retrieved from
www.merckmanuals.com/professional/hepatic_and_biliary_disorder s/gallbladder_and_bile_duct_disorders/tumors_of_the_gallbladder_and_bile_ducts.html?qt=gallbladder%20cancer&alt=shGallbladder Cancer (2011) Retrieved from http://www.mayoclinic.org/medicalprofs/gallbladder-carcinoma-management.htmlGeneral Information about Gallbladder Cancer (2011). Retrieved from http://www.cancer.gov/cancertopics/pdq/treatment/gallbladder/Patient/ page1Insel, P. (2011) Nutrition (4th ed.) Sudbury MA: Jones and BartlettNelms, M., Sucher, K.P., Lacey, K., Roth, S.L. (2011). Nutrition Therapy &
Pathophysiology (2nd ed.). Belmont, CA: WadsworthOctreotide (2012) Mayo Clinic. Drugs and Supplements. Retrieved from http://www.mayoclinic.com/health/drug-information/DR601739Parrish, C.R., Quatrara, B. (2010). Reinfusion of Intestinal Secretions: A viable
Option for Select Patients. Nutrition Issues in Gastroenterology, Series #83, April 2010.
???