bleeding complications during pregnancy - htrs · severe postpartum hemorrhage following an...
TRANSCRIPT

Bleeding Complications During Pregnancy
Keith McCrae, M.D.Cleveland Clinic4/13/2016

Disclosure
I have no relevant personal financial relationship and I have not presented any promotional talks for any pharmaceutical
companies within the past 12 months.

Outline
• Epidemiology and causes of maternal mortality
• Placental structure and relation to hematologic disease in pregnancy
• Maternal mortality/morbidity due to bleeding
• Life threatening bleeding disorders
• Von Willebrand disease in pregnancy




Maternal Mortality: WHO Analysis
Khan et al, Lancet 2006

http://www.cdc.gov/reproductivehealth/MaternalInfantHealth/PMSS.html
Pregnancy-Related Death in the United States

Placentation and the Maternofetal Circulation
Kingdom and Drewlo, Blood 118:4780, 2011

Defective Placentation in Preeclampsia
Normal Preeclampsia
Kingdom and Drewlo, Blood 118:4780, 2011

Q1: Postpartum Hemorrhage
You are called to see a 24 year old woman who has developed severe postpartum hemorrhage following an extended labor and delivery. Her pregnancy had been previously uncomplicated. On further questioning she has had mild epistaxis about once every year or two, usually in the winter. She had previously undergone tonsillectomy as a child and said she bled afterwards but does not recall needing transfusions. She also underwent a laparoscopic appendectomy without excessive bleeding. Her obstetricians want to know whether she has an underlying coagulopathy.


Definitions and Causes of Postpartum Hemorrhage
Abdul-Kadir et al: Transfusion, 2014
Bateman et al: Anesth Analg, 2010

Risk Factors for Postpartum Hemorrhage
Abdul-Kadir et al: Transfusion, 2014

Massive Obstetric Hemorrhage/Disseminated Intravascular Coagulation
• Amniotic fluid embolism
• Placental abruption
• Placenta previa
• Placenta accreta
• Retained products of conception

Causes and Pathogenesis of DIC in Pregnancy
Montagna Sem Thromb Hemost 36:404, 2010

ISTH Scoring System for DIC: Relevance to Pregnancy
Taylor FB et al: JTH, 2001Charbit G; JTH, 2007
Réger et al; Thromb Res 2013

Amniotic Fluid Embolism• Misnomer—“anaphylactoid syndrome of pregnancy”
• Incidence: 1/40,000
• Risk factors--controversial
– No risk factor identified that justifies prospective alterations of clinical practice
• Early clinical signs and symptoms
– Hypotension
– Dyspnea
– Cyanosis
– Loss of consciousness
– Cardiac arrest
• Fulminant coagulopathy (DIC)-diffuse bleeding from uterus, incisions, intravenous sites
• Consequences
– Maternal mortality in 60% if all classic signs and symptoms are present
– If cardiac arrest, mortality increases to 90%
– Severe fetal morbidity/mortality if not delivered urgently

Amniotic Fluid Embolism
https://www.studyblue.com/notes/note/n/vascular-disorders-_atlas-images/deck/8094977
Kanayama and Tamura J Obstet Gynec Res 40: 1507, 2014

Amniotic Fluid Procoagulant Activity/DIC
Clark SL; Obstet Gynec, 2014
Sarig et al; Thromb Res, 2011

Placental Abruption• Partial or complete separation of normally implanted placenta before delivery
• Incidence: 0.4-1.0% of pregnancies
– Highest incidence at 24-26 weeks
• Risk factors
– Advanced maternal age (>35 years)
– Smoking
– Chronic hypertension
– Vaginal bleeding during pregnancy
– PROM/chorioamnionitis
– Obstetrical history (preeclampsia, C-section, stillbirth, abruption)
– Thrombophilia?
• Clinical manifestations
– Hypovolemic shock, renal failure
– Fulminant DIC in severe cases
– Neonatal compromise
– Maternal mortality < 1%
http://umm.edu/health/medical/pregnancy/labor-and-delivery/placenta-abruptio

MRI Placental Abruption
Masselli et al. Radiology 259:222, 2011

Ananth et al. AJOG 272e2, 2016
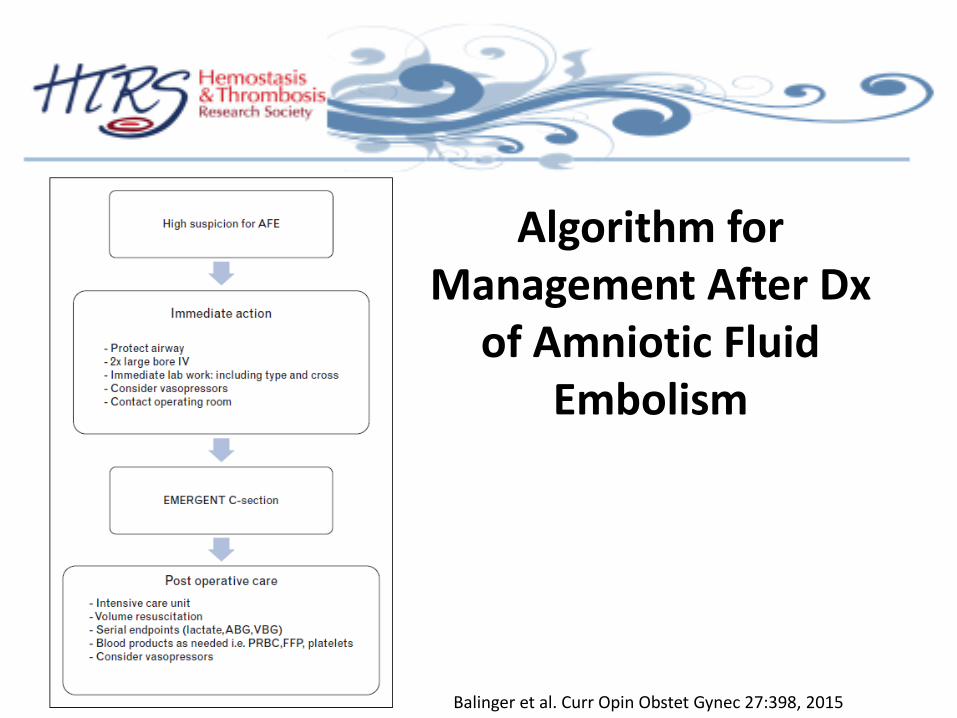
Algorithm for Management After Dx
of Amniotic Fluid Embolism
Balinger et al. Curr Opin Obstet Gynec 27:398, 2015

PPH: French Guidelines
Sentilhes et al; EJOG 198:12, 2016
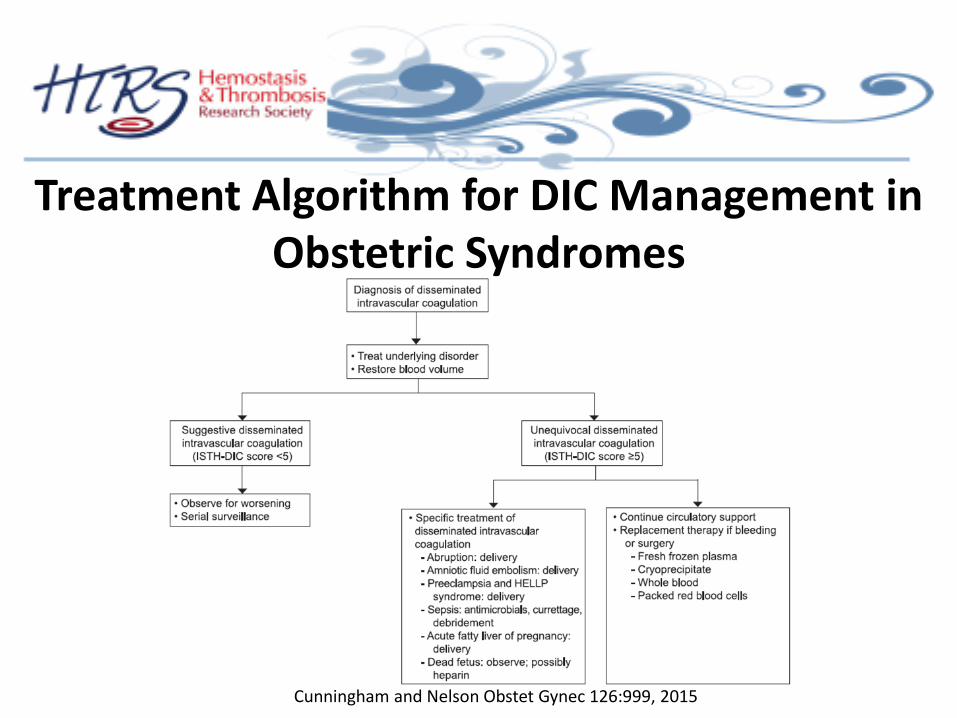
Treatment Algorithm for DIC Management in Obstetric Syndromes
Cunningham and Nelson Obstet Gynec 126:999, 2015

Prevention and Management of PPH
Abdul-Kadir et al: Transfusion, 2014

Management of Severe Postpartum Hemorrhage
• Uterine massage/uterotonics– Syntocinon
– Ergometrine/Syntometrine
– PGF2 alpha/Misoprostol
• Interventional approaches
– Uterine tamponade
– B-lynch suture
– Uterine artery/internal iliac artery embolization
– Hysterectomy
• Aggressive transfusion, platelet, coagulation factor replacement
• Recombinant factor VIIa (rVIIa)
Su et al: Best Prac Clin Res Obstet Gyn, 2012

Massive Transfusion in Obstetrical Bleeding
Pacheco LD et al: Am J Perinatol, 2013
Burtelow M et al: Transfusion, 2007

rVIIa in Obstetrical Hemorrhage
Leighton et al: Anesthesiology, 2011
Kobayashi et al: Int J Hematolol, 2012

Tranexamic Acid in Postpartum Hemorrhage
TXA: 4 gm over 1 hour, then 1 gm/hr infusion, IV Ducloy-Bouthors et al: Crit Care, 2011

Tranexamic Acid in Pregnancies at High Risk for PPH
Sujata et al IJOG, 2016

Effect of TA on Postpartum Blood Loss: Systematic Analysis
Alam and Choi, Transf Med Rev 29:231-241, 2015

Case 2: VWD in Pregnancy
• 32 yo woman with VWD
• Menorrhagia
• Epistaxis, once per year, usually in winter
• Lab• PTT 36 sec (< 32 sec)
• RCOF 31% (>35%)
• CBA 42% (>41%)
• VWF ag 44% (>50%)
• All multimers reduced
• Presents in week 28 of uncomplicated pregnancy


Prophylaxis of Women with Inherited Bleeding Disorders
Abdul-Kadir et al: Transfusion, 2014
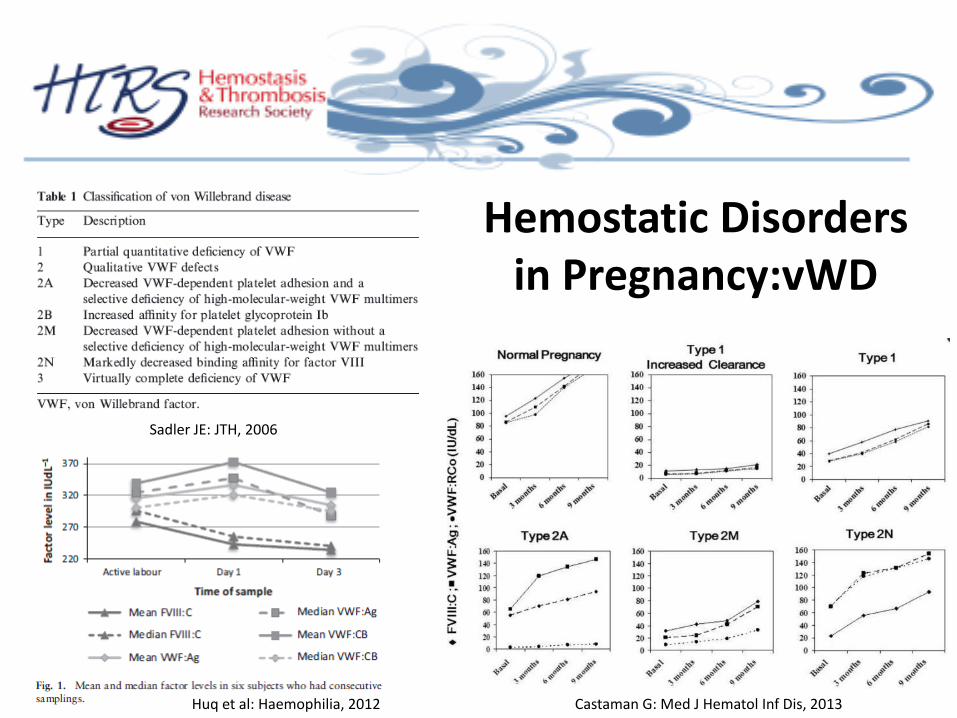
Hemostatic Disorders in Pregnancy:vWD
Sadler JE: JTH, 2006
Castaman G: Med J Hematol Inf Dis, 2013Huq et al: Haemophilia, 2012

Treatment of VWD in Pregnancy
James A. Hemophilia 21:81, 2015

Levels of VWF, Rcof and FVIII Postpartum
James A, Hemophilia 21:81, 2015
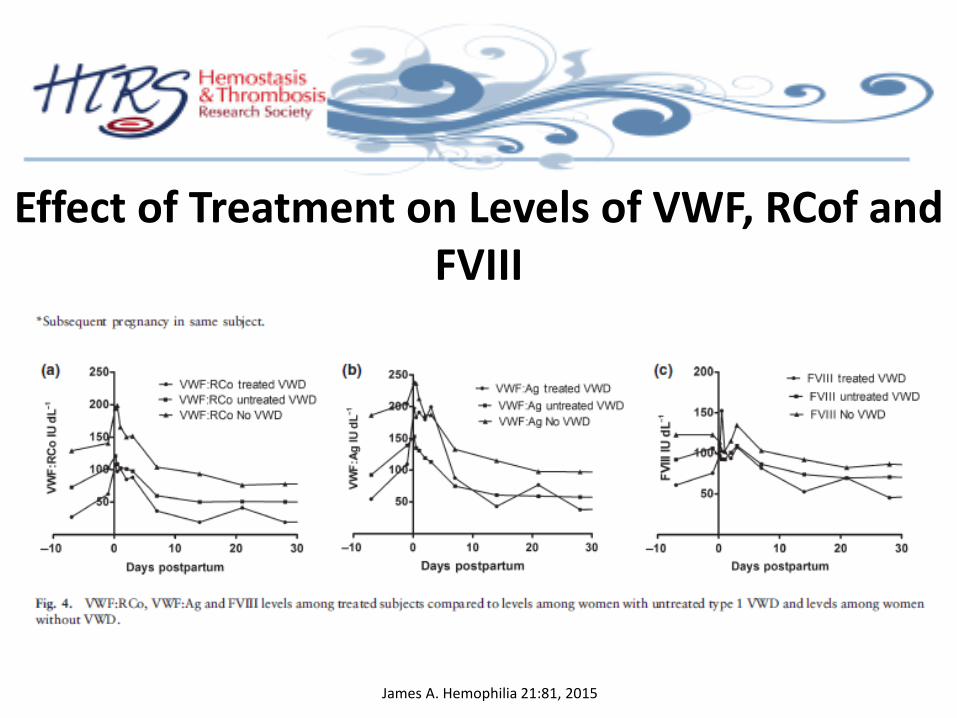
Effect of Treatment on Levels of VWF, RCof and FVIII
James A. Hemophilia 21:81, 2015

Management of Type I VWD at Delivery
• Most patients achieve normal levels of VWF by mid second trimester
• Vaginal or C-section is safe if RCof and FVIII levels are > 50%
• DDAVP can be used in pregnancy if invasive procedures needed before increase in VWF
• VWF levels begin to drop by day 3 and return to baseline by day 14—mean time at presentation for hemorrhage in VWF patients is 15.7 days
• Patient should be counseled to consult physician at any sign of increased bleeding: treatment options include DDAVP, factor concentrates, tranexamic acid
Neff and Sidonio. Am Soc Hematol Educ Prog 2014(1): 536-41

Summary• With respect to coagulation, pregnancy is a closely regulated
state, disruption of which can cause profound derangement of hemostasis
• The most common cause of post-partum bleeding is uterine atony
• Placental abruption is a cytokine/SIRS driven process, in which profound DIC follows the initial insult and may lead to life-threatening hemorrhage
• The normal increases in VWF during pregnancy in patients with Type I VWD are usually sufficient to enable safe delivery, but bleeding can occur in the post-partum period.