blindness kenya: status kenya rural blindness prevention ject · whitfield,...
TRANSCRIPT

Britishlournal ofOphthalmology,1990,74,333-3403
Blindness and eye disease in Kenya: ocular statussurvey results from the Kenya Rural BlindnessPrevention Project
Randolph Whitfield, Larry Schwab, Dennis Ross-Degnan, Paul Steinkuller, Jack Swartwood
AbstractA series of eight regional eye surveys wereconducted in Kenya as part ofthe Kenya RuralBlindness Prevention Project. Each surveyconsisted of clinical examinations of about1800 individuals selected by a random clustersampling technique in geographically distinctand culturally homogeneous rural areas; 13 803examinations were completed in all. Togetherthese surveys provide the basis for nationalestimates of the prevalence and aetiology ofvisual loss and ocular pathology. The resultsshowed that 0-7% ofrural Kenyans are blind inthe better eye byWHO standards, and another2*5% suffer significant visual impairment.Rates ofvisual loss tend to increase five-fold ineach 20-year age cohort. Females have higherprevalence of visual loss than males over age20, and certain geographical areas havemarkedly higher rates. The commonest causeof both blindness and visual impairment iscataract, accounting for 38% of all visual loss.Trachoma (a localised problem), glaucoma,macular degeneration, and severe refractiveerrors follow cataract as leading causes ofblindness in the better eye. Trauma, cornealscars of various causes, phthisis, andstaphyloma are important causes ofmonocularblindness. Nutritional eye disease does notappear to be a problem of any magnitude inrural Kenya.
Royal CommonwealthSociety for the Blind andOperation EyesightUniversal, Nairobi,KenyaR Whitfield
International EyeFoundation, Bethesda,Maryland, USAL Schwab
Department of SocialMedicine, HarvardMedical School, USAD Ross-Degnan
Department ofOphthalmology, BaylorSchool ofMedicine, USAP Steinkuller
Association of CatholicCharities, Silver Spring,Maryland, USAJ SwartwoodCorrespondence to:L Schwab, MD, InternationalEye Foundation, 7801 NorfolkAvenue, Bethesda, Maryland20814, USA.Accepted for publication23 November 1989
Preventable blindness has long been identified asa global public health problem.'2 Approximately28 million people are blind worldwide and overtwo-thirds of them live in developing nations.3Often blindness rates in poor countries are 10 to20 times those in industrialised nations,4 and incertain communities with particular diseaseproblems like onchocerciasis or severe trachomaas much as 30-50% of the population may beaffected, especially among the elderly. Thisoccurs not only because of limited access tohealth services, but also because of environ-mental or climatic stresses, poor hygiene, andother factors associated with a low standard ofliving. Approximately 80% ofthe people who areblind in the developing world suffer from condi-tions which are avoidable in the sense that theirblindness could have been prevented or issurgically correctable.The true consequences of blindness are diffi-
cult to calculate. In addition to the social andpsychological isolation of the blind and thestigma attached to their helplessness, in a situa-tion ofvery limited resources for survival, a blindperson can be a tremendous economic burden.
The presence of high rates of blindness in acommunity implies a significant loss of itsproductivity, not only because the blind oftencannot be productively engaged, but alsobecause others must care for them and generatethe resources needed for their survival.The International Eye Foundation (IEF) has
assisted the Government of Kenya in developingpreventive and therapeutic ophthalmic servicessince 1972, when an IEF ophthalmologist wasposted to a rural provincial hospital as thegovernment eye specialist. Kenya typifies thehealth manpower situation in many Africannations, in that most of the medical facilities,manpower, and resources are concentrated inlarge cities, especially the capital city. Thereare only a few government ophthalmologistsassigned to rural facilities, concentrating theirefforts on the rural population. A pilot ocularsurvey among the rural Samburu people5 con-firmed that most blindness in rural Kenya iseither preventable or curable. For these reasonsthe underlying rural needs are better addressedby training clinical and surgical personnel whoare not ophthalmologists to provide ophthalmiccare, and by eye disease prevention programmes,rather than by the isolated clinical efforts of eyespecialists.
Substantial funding from the United StatesAgency for International Development begin-ning in October 1976 made possible an IEFsponsored Kenya-wide Rural Blindness Preven-tion Project (KRBPP).6 The objectives of thisproject were to strengthen and extend thecapabilities of the established system of thera-peutic rural eye care, and to divert the emphasisin rural eye care away from a purely therapeuticapproach towards prevention of blindnessthrough health education, screening, and treat-ment at the primary care level, and early referralof people in need of specialised care. To planfor these objectives it was necessary to defineaccurately the prevalence and causes ofblindnessamong rural Kenyans.
Material and methods
SAMPLE DESIGNBecause of constraints in time and resources anational statistical sample of the rural populationwas not. organised. Instead advantage was takenof the fact that tribes in Kenya traditionally livein defined geographical regions and have nottended to intermingle in their rural homes asthey have in the cities. Specific rural areas thatrepresented the major population groups, as wellas the ranges of ecological conditions that might
333
on August 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.74.6.333 on 1 June 1990. D
ownloaded from
Whitfield, Schwab, Ross-Degnan, Steinkuller, Swartwood
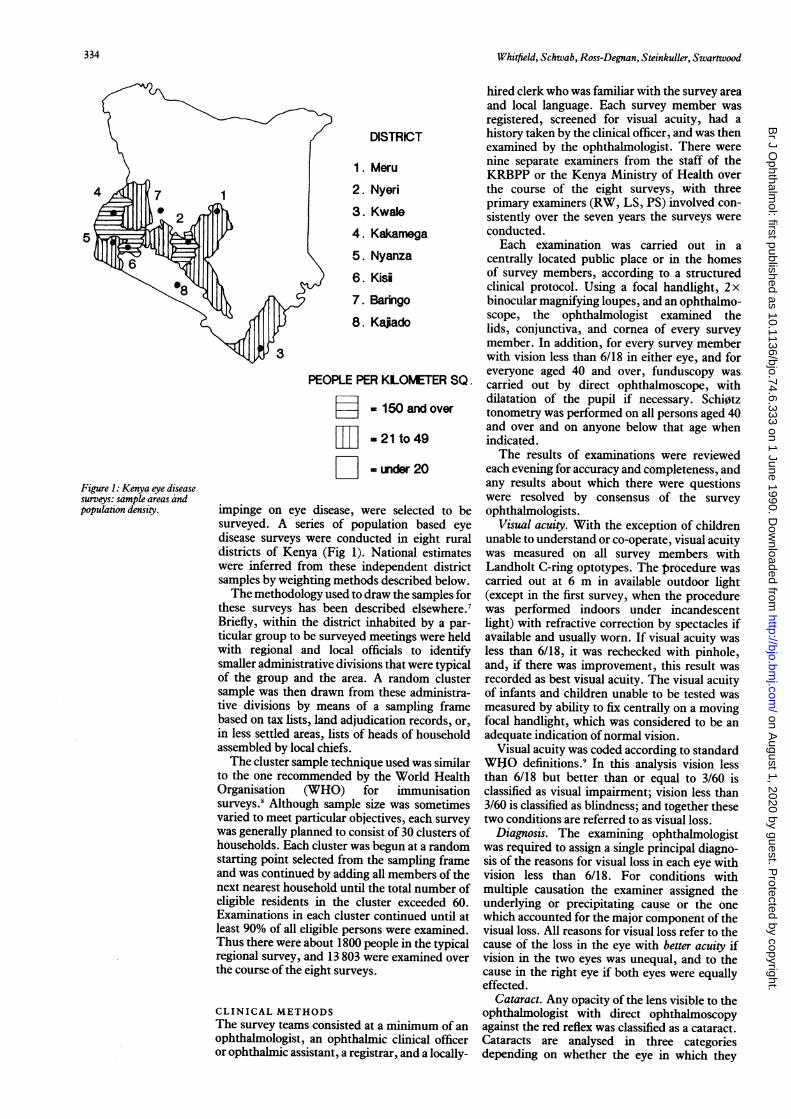
DISTRICT
1. Meru
1 2. Nyeri3. Kwale4. Kakamega5. Nyanza6. Kisi
7. Baringo8. Kajado
3
PEOPLE PER KLOMETER SQ.
- 150 and over
Ljj] - 21 to 49
D = under 20
impinge on eye disease, were selected to besurveyed. A series of population based eyedisease surveys were conducted in eight ruraldistricts of Kenya (Fig 1). National estimateswere inferred from these independent districtsamples by weighting methods described below.The methodology used to draw the samples for
these surveys has been described elsewhere.7Briefly, within the district inhabited by a par-ticular group to be surveyed meetings were heldwith regional and local officials to identifysmaller administrative divisions that were typicalof the group and the area. A random clustersample was then drawn from these administra-tive divisions by means of a sampling framebased on tax lists, land adjudication records, or,in less settled areas, lists of heads of householdassembled by local chiefs.The cluster sample technique used was similar
to the one recommended by the World HealthOrganisation (WHO) for immunisationsurveys.8 Although sample size was sometimesvaried to meet particular objectives, each surveywas generally planned to consist of 30 clusters ofhouseholds. Each cluster was begun at a randomstarting point selected from the sampling frameand was continued by adding all members of thenext nearest household until the total number ofeligible residents in the cluster exceeded 60.Examinations in each cluster continued until atleast 90% of all eligible persons were examined.Thus there were about 1800 people in the typicalregional survey, and 13 803 were examined overthe course of the eight surveys.
CLINICAL METHODSThe survey teams consisted at a minimum of anophthalmologist, an ophthalmic clinical officeror ophthalmic assistant, a registrar, and a locally-
hired clerk who was familiar with the survey areaand local language. Each survey member wasregistered, screened for visual acuity, had ahistory taken by the clinical officer, and was thenexamined by the ophthalmologist. There werenine separate examiners from the staff of theKRBPP or the Kenya Ministry of Health overthe course of the eight surveys, with threeprimary examiners (RW, LS, PS) involved con-sistently over the seven years the surveys wereconducted.Each examination was carried out in a
centrally located public place or in the homesof survey members, according to a structuredclinical protocol. Using a focal handlight, 2 xbinocular magnifying loupes, and an ophthalmo-scope, the ophthalmologist examined thelids, conjunctiva, and cornea of every surveymember. In addition, for every survey memberwith vision less than 6/18 in either eye, and foreveryone aged 40 and over, funduscopy wascarried out by direct ophthalmoscope, withdilatation of the pupil if necessary. Schi0tztonometry was performed on all persons aged 40and over and on anyone below that age whenindicated.The results of examinations were reviewed
each evening for accuracy and completeness, andany results about which there were questionswere resolved by consensus of the surveyophthalmologists.
Visual acuity. With the exception of childrenunable to understand or co-operate, visual acuitywas measured on all survey members withLandholt C-ring optotypes. The procedure wascarried out at 6 m in available outdoor light(except in the first survey, when the procedurewas performed indoors under incandescentlight) with refractive correction by spectacles ifavailable and usually worn. If visual acuity wasless than 6/18, it was rechecked with pinhole,and, if there was improvement, this result wasrecorded as best visual acuity. The visual acuityof infants and children unable to be tested wasmeasured by ability to fix centrally on a movingfocal handlight, which was considered to be anadequate indication of normal vision.
Visual acuity was coded according to standardWHO definitions.9 In this analysis vision lessthan 6/18 but better than or equal to 3/60 isclassified as visual impairment; vision less than3/60 is classified as blindness; and together thesetwo conditions are referred to as visual loss.
Diagnosis. The examining ophthalmologistwas required to assign a single principal diagno-sis of the reasons for visual loss in each eye withvision less than 6/18. For conditions withmultiple causation the examiner assigned theunderlying or precipitating cause or the onewhich accounted for the major component of thevisual loss. All reasons for visual loss refer to thecause of the loss in the eye with better acuity ifvision in the two eyes was unequal, and to thecause in the right eye if both eyes were equallyeffected.
Cataract. Any opacity of the lens visible to theophthalmologist with direct ophthalmoscopyagainst the red reflex was classified as a cataract.Cataracts are analysed in three categoriesdepending on whether the eye in which they
5
Figure 1: Kenya eye diseasesurveys: sample areas andpopulation density.
334
on August 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.74.6.333 on 1 June 1990. D
ownloaded from
Blindness and eye disease in Kenya: ocular status survey resultsfrom theKenya RuralBlindness Prevention Project
TABLE I Regional survey area characteristics
AttributedTribal Sample % ofrural
District group size population Geography Climate and rainfall Economy
Meru Meru 1142 16-1 Nyambene Hills northeast Temperate to hot; moderate Cultivation of miraa (a plantofMt Kenya runoff, rain but high subsistence used as a stimulant)scarce water farming
Nyeri Kikuyu 1825 20-4 Hilly highlands west ofMt Cool temperate, high Coffee and tea farming,Kenya plentiful rainfall, water subsistence farming
Kwale Mijikenda 1342 6-8 Coastal plain and immediate Hot, humid, moderate Fishing, subsistence farming,hinterland rainfall tourism
Kakamega Abaluhya 1651 23-6 Highland plateau west of Temperate to hot, moderate Cotton farming, some coffeeRift Valley reliable water rainfall farming, subsistence
farmingNyanza Luo 1807 11-5 Basin south of Lake Victoria Hot, humid, rainfall Cotton farming, fishing,
moderate but variable subsistence farmingKisii Kisii 1753 6-2 Hilly plateau west of Rift Temperate, high rainfall; Tea and coffee farming,
Valley good water subsistence farmingBaringo Tugen 1182 6-7 Tugen Hills, Lake Baringo Varied; temperate to hot; Coffee and subsistence
Njemps 581 plain, Rift Valley north of moderate to very low farming; livestock herdingPokot 5% lake rainfall in arid areas
Kajiado Masai 1924 8-7 1000 m grassland plateau Hot, arid, semidesert; water Herding cattle, goatseast of Rift Valley scarce
occur had normal visual acuity, visual impair-ment, or blindness.
Trachoma. This paper reports only the basicfindings for visual loss due to trachoma andprevalence of trachoma inflammation. Detailedfindings on the disease and related ocularpathology will be reported elsewhere. Visual losswas determined as being due to trachoma inthree situations: (1) the simultaneous presence ofcorneal opacities, and entropion or trichiasis; (2)the presence of focal corneal opacity due tosecondary bacterial infection or corneal ulcerwhere there were other clinical signs oftrachoma(active inflammation, scarring of the tarsal con-junctiva, corneal or limbal pannus, or Herbert'spits); (3) the presence of trachomatous keratitisthat was believed to affect visual acuity. Thescoring of trachoma inflammation was based onrecommendations'0 of the WHO and coded by asimplified recording system.
Refraction. Formal measurement of the typeand severity of refractive errors was not carriedout. When refractive error was considered to be apossible cause of visual loss, the presence ofrefractive error was confirmed by lens powerreadings from the ophthalmoscope or byobserved improvements in acuity with pinholeexamination.
Glaucoma. Visual field testing could not beperformed during these surveys for logisticreasons. In the absence of such a definitive testfor diagnosis ofglaucoma as a cause of visual lossthe survey protocol required observation of oneof the following: a pathological optic disc(marked pallor of the nerve head, or verticalcupping greater than 0 5) in the presence ofraised intraocular pressure (>21 mmHg);markedly raised intraocular pressure (>26mmHg) without visualisation of a pathologicaldisc; a history ofglaucoma surgery or treatment.
Because of the criteria used for identifying thedisease, glaucoma as a cause ofvisual loss is likelyto be underestimated in the surveys, but there isno way of determining the extent to which thisoccurred. Cases of low-tension glaucoma, andthose where adequate assessment of the opticdisc was not possible (for example, due to thepresence of a cataract), were unlikely to beclassified as glaucoma. Furthermore, becausetonometry and funduscopy were performed
routinely only on persons over 40, early andborderline glaucoma cases in the younger agegroups that were not yet sufficiently advanced toaffect central vision also may have been missed.
Retinal disorders. Age related maculardegeneration and other retinal anomalies werediagnosed on clinical grounds alone, as diagnos-tic laboratory investigations were not feasible.
METHODS OF ANALYSISBecause ofthe great sensitivity ofestimates oftheprevalence and causes of visual loss to thedistribution ofage in a population, a standardisa-tion procedure was carried out to minimise theeffects of random differences in the age distribu-tion of the eight regional survey samples. Eachsurvey population was adjusted to the nationalpopulation age distribution from the 1979 censusby weighting age categories according to whetherthey were over- or undersampled relative to thestandard. This procedure allows more appro-priate regional comparisons and ensures thatnational estimates are less influenced bysampling differences.
Because the surveyed regions, and the loca-tions within them, were not selected randomly,there is no unbiased procedure for estimating thetrue population prevalence of blindness or ofother ocular conditions. Within each region,however, an assumption was made that theparticular locations from which the sample wasrandomly drawn were representative of abroader population group, and that estimates ofrates from the survey sample would apply to theunderlying regional population within reason-able bounds of error.
National estimates were computed by attrib-uting to each regional survey a certain proportionof the national rural population, based onsimilarity in tribal composition, geography, andclimate (Table I). Observations within eachsurvey were appropriately weighted so thatthe national estimates reported reflect theseattributed proportions.For the reasons mentioned, and also because
the sample was drawn in clusters, there is nounbiased procedure for calculating samplingerrors or confidence intervals for the estimates.No standard errors are reported, though it would
335
on August 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.74.6.333 on 1 June 1990. D
ownloaded from

Whitfield, Schwab, Ross-Degnan, Steinkuller, Swartwood
TABLE II Visual impairment and blindness by age by sex:percentage by acuity level*
Age groupAll
0-19 20-39 40-59 60+ Kenya
MaleNormal 99-7 98-5 94'3 66-6 97 3Impaired 0-2 1-0 4-4 26-9 2-1Blind 0-1 0-6 1-2 6'5 0-6Weighted Nt (3925) (1185) (510) (304) (5925)FemaleNormal 99-7 98-0 89-7 61-4 96-4Impaired 0-2 1-7 8-6 29-2 2-8Blind 0-1 03 1-7 9-4 0-8Weighted Nt (4178) (2227) (932) (315) (7653)
*All categories refer to acuity in the better eye with availablecorrection. Normal=6/18 or better; impaired=worse than 6/18but better than or equal to 3/60; blind=worse than 3/60.tWeighted according to the proportion of the national ruralpopulation represented by each survey region and after adjustingto a standard age distribution based on all surveys combined.
be possible to compute rough estimates based onassumptions of simple random sampling fromthe information on sample size presented, and toinflate them by an appropriate factor (perhaps2-4 times) to account for the non-randomiseddesign and clustering.
Results
RATE OF BLINDNESS AND VISUALIMPAIRMENTThe prevalence of blindness and visual impair-ment by age and sex group is presented in TableII. About 0 7% of all rural Kenyans were blind intheir better eye, and another 2'5% had visionwhich was substantially impaired. Femalesexceeded males by slight percentages in boththese categories.As expected, the prevalence of visual loss
showed a very strong relationship with age,increasing by approximately a factor of 5 in each20-year age cohort. In the most severely affectedgroup of rural Kenyans, those over the age of 60,about 1 in 12 were blind, and another 28%suffered from visual impairment. Females had anotably higher prevalence of visual loss over theage of 40, and especially in the 40 to 59 yearcohort, where total prevalence was nearly doublethat of males (10-3% vs 5'6%).There was a fair degree of consistency in the
prevalence of impairment and blindness acrossall the regions surveyed (Table III), with threeexceptions. In the two surveys of pastoralgroups, among the Masai in Kajiado and amongthe Pokot and Njemps in Baringo (not separatedin Table III from the non-pastoral groups inBaringo) a markedly higher total prevalence of
visual loss was found. However, the highestprevalence of blindness was found in Meru,among a settled agricultural group.
REASONS FOR VISUAL LOSS
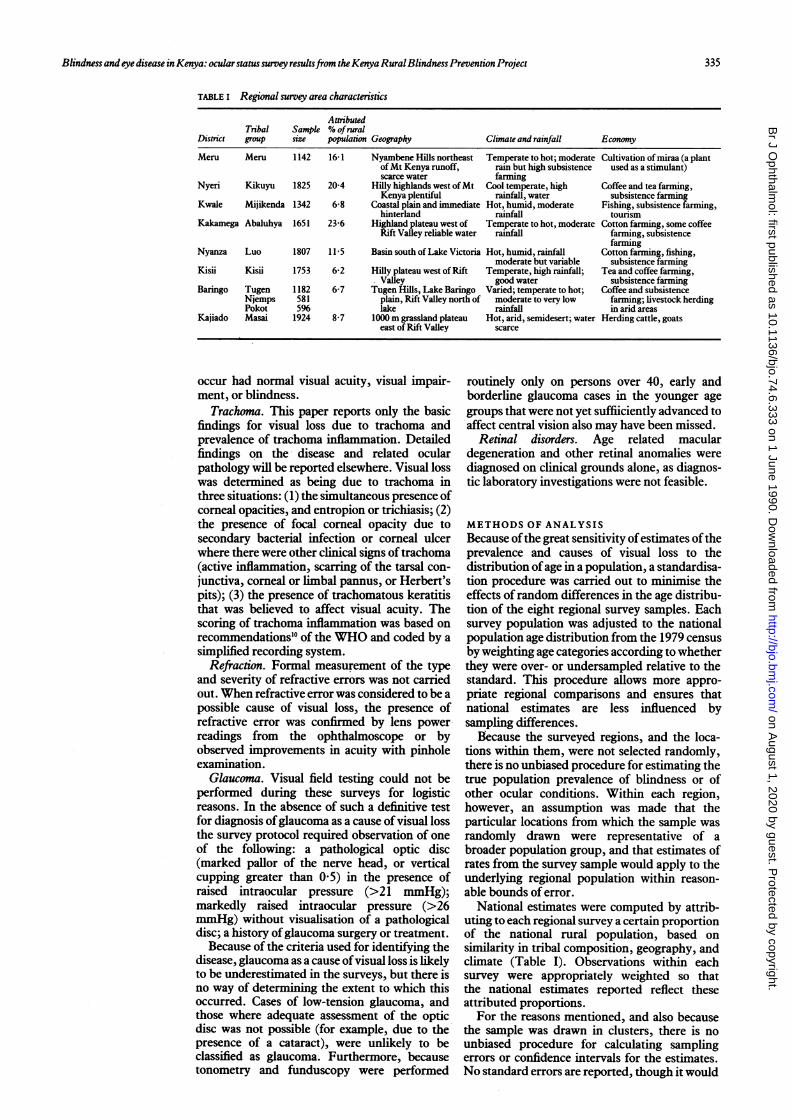
Cataract was the major cause ofblindness in ruralKenya, with a prevalence of 2 5 per 1000,accounting for 36% of all blindness (Fig 2).Following cataract in prevalence were trachoma(1 3/1000), glaucoma (0'6/1000), maculardegeneration (0'5/1000), and severe refractiveerrors or amblyopia (0 4/1000). Blindness due toxerophthalmia - nutritional blindness - was
estimated to occur at a rate of less than 1 per10000 individuals overall in rural Kenya and wasnot found in any person examined under the ageof 20.
Cataracts were also responsible for 39% of allvisual impairment (rate of 10'0/1000). It was themost prevalent cause of visual loss in six of theeight survey areas and was second to refractiveerror in the remaining two (Nyeri and Kisii).Refractive errors and macular degeneration werefound to be equally prevalent (4'5/1000) as
leading causes for visual impairment aftercataract. They were followed in importanceby trachoma (3'3/1000) and corneal scars dueto causes other than trachoma, trauma, or
xerophthalmia (corneal scar/other) (1 2/1000).The prevalence by age group of the causes of
visual impairment (rate of 10'0/1000). It was theFigure 3. Cataract, trachoma, refractive errors,macular degeneration, and glaucoma all showsharp increases in prevalence among those 60and over, while trachoma and cataract stand outin importance as blinding conditions in the twopreceeding decades. The relative prevalence ofthe leading causes of visual loss was found to besimilar for men and women in all age groups,except that visual impairment and blindness dueto trachoma occur more frequently amongwomen beginning at age 40.
PREVALENCE OF OCULAR CONDITIONSOcular pathologies have as their most importantendpoint the inability to see, and the ensuingblindness is not only a health problem but a
major socioeconomic problem as well. From a
public health perspective, therefore, the mostappropriate way to organise diagnoses obtainedthrough prevalence survey is by conditionswhich affect both eyes or the eye with bettervision. However, from the perspective ofmakingdecisions related to training health systempersonnel about common conditions or of public
TABLE III Rates ofvisual impairment and blindness by regional survey: percentage by acuity level*
Regional survey
AllKakamega Meru Nyeri Kwale Nyanza Kisii Baringo Kajiado Kenya
Normal 98'5 94.5 97-6 974 96-8 %-9 96-9 93.3 96-8Impaired 1-0 4'0 2-1 1-8 2-6 2-7 2-5 5-4 2-5Blind 0'5 1-5 0-3 0 7 0-6 0 4 0-6 1-3 0-7Weighted Nt (3174) (2210) (2778) (934) (1576) (842) (902) (1176)
*AJl categories refer to acuity in the better eye with available correction. Normal=6/18 or better; impaired=worse than 6/18 butbetterthan or equal to 3/60; blind=worse than 3/60.tWeighted according to the proportion of the national rural population represented by each survey region, and after adjusting to astandard age distribution based on all surveys combined.
336
on August 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.74.6.333 on 1 June 1990. D
ownloaded from

Blindness and eye disease in Kenya: ocular status survey resultsfrom theKenya RuralBlindness Prevention Project
Figure 2: Conditions causingloss ofvision in the eye withbetter visual acuity
Cataract, aphakia
Refractive errors
Congenital condition
Corneal condition
Corneal condition
Unknown, unspecified
Visual impairmentO (Acuity 6/19 -3/60)
Blindness
| (Acuity <3/60)
0 2 4 6 8 10 12 14
Prevalence per 1000 persons
Blindness (acuity <3/60)
.
D:
.2: E::::
(...
Visual impairment
(acuity 6/19 - 3/60)
40
c1
--- 30
I
0
10 ego
Eo
Age group
0-3e
40-59
60 and over
40
30 9
-20-
10 cT1at | £8
3 LC 88
Figure 3: Reasonsfor loss ofvision by age group.
health education, it is also useful to examine theprevalence of sight affecting conditions in eithereye (Fig 4).From this perspective cataract is again the
major cause of visual loss. Its prevalence as a
blinding condition more than doubles (6 0/1000), since many people have at least one eye
with a dense cataract even if the other stillretained better sight. Trauma, which is mostoften monocular, assumes a position as thesecond most prevalent blinding condition (4 3/1000). It is followed in importance by cornealscar due to non-trachomatous infections (3 5/1000) and trachoma (2-9/1000). Phthisis andstaphyloma of unknown aetiology (1-7/1000),which are also most often monocular, are nearlyequal in prevalence to blinding refractiveproblems (1 8/1000).
Table IV arrays the prevalence by age group ofthe most important ocular diseases and condi-tions from a public health standpoint. Inflam-matory trachoma is the most prevalent oculardisease in rural Kenya, with 18-7% of the entirepopulation, and about 1 in 4 children under theage of 10, affected overall. The prevalence in allage groups, but especially among children,varied dramatically among survey areas. Over80% of those under the age of 10 had activetrachoma in Meru and Kajiado; about 50% hadactive disease among the Pokot in Baringo; 25%in Nyeri and among the Njemps in Baringo; 10%among the Tugen in Baringo; and less than 1% inthe remaining survey regions.The prevalence ofvisual loss due to sequelae of
trachoma varied among survey areas even more
sharply - 1-6% of the population in Meru, 1-4%among the affected groups in Baringo, 1 0% inKajiado, 0-2% in Nyeri, and none in the remain-ing areas.
There is a very low prevalence of signs of
337
Breakdown of corneal causes
( < :2F-TrachomaME Trauma
Corneal impairmentXerophthalmia
M Staphyloma/phthisis
M Other corneal
Corneal blindness
II 1
on August 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.74.6.333 on 1 June 1990. D
ownloaded from

Whitfield, Schwab, Ross-Degnan, Steinkuller, Swartwood
Figure 4: Conditions causingloss ofvision in any eyeexamined.
Cataract, aphakia ..........
:.:....
,, - .:.:.:.:::.:....::: .:.:....:.:.:.::...:
Congenital condition|
Corneal condition E
Retinal condition_
_ Visu~~IIal impairment
. [E1 ~~~(Acuity 6/19 - 3/601)
_ * ~~~~(Acuity 3/601
I~ ~~~~~~~~....
0 2 4 6 8 10 12 14
Prevalence per 1000 persons
potential nutritional eye disease in rural Kenya,especially among children under 5, who are atthe highest risk of a nutritional crisis whichmight precipitate vitamin A deficiency. No cases
TABLE IV Selected ocular conditions by age: percentage with condition in either eye
Age group
0-39 40-59 60+
Lens opacities:With visual acuity >6/18* 0-1 2-3 10-8With visual loss or aphakia 0-1 6-1 32-1Weighted N (10439) (1390) (609)
Corneal and globe conditions:Ulcer ofany origin 0 3 0 4 0-2Dystrophy or degeneration 0-2 2-1 7-1Nebula, macula, or leucoma 2-2 5 8 11-2Phthisis 0-2 0-8 1-9Staphyloma 0-1 0-3 0 5Weighted N (11600) (1449) (628)
Disorders of the optic nerve head or macula:Glaucomatous cupping NAt 1-1 2-8Opticdiskpallor NA 07 1-3Optic atrophy NA 0-6 1-2Macular degeneration NA 3-0 13-9Other macular lesions NA 1-0 10-5Pigmentary degeneration NA 0-1 0-6Other retinal lesion NA 1-5 8-6Weighted N (-) (1360) (568)
Schiotz intraocular pressure:22-25mm NA 2-2 3-126+mm NA 1-5 3-8Weighted N (-) (957) (535)
Age group
0-4 5-9 10-19 20+
Potential nutritional eye disease:Bitot's spots 0-1 0-6 0 3 0-2Conjunctival xerosis <0-1 0 3 0-1 0-1Leucoma from keratomalaci4 <0-1 <0 1 <0-1 <0 1
Conjunctival inflammations:Inflammatory trachoma 27-1 23-8 16-6 14-0Purulentconjunctivitis 3-1 1-3 0-2 0-4Tarsal or limbal vernal 0-1 0-2 0-4 0 3Weighted N (2541) (2223) (3415) (5843)
*An individual with cataracts of both types is counted in both categories.tOphthalmoscopy and intraocular pressure examination performed only if indicated on persons under40.t:No cases of corneal xerosis or active current keratomalacia were found.
of corneal xerosis or active keratomalacia, thetwo least equivocal signs of current vitamin Adeficiency, were found in any of the surveys.Like trachoma, the occurrence of nutritional eyedisease appears very localised. Nine of the 10cases of visual loss due to old xerophthalmia werefound in the Baringo survey, and the other was
among the Masai in Kajiado.Glaucomatous cupping was found in I1-% of
the rural population between 40 and 59 years andin 2-8% of those over 60. In addition optic discpallor or atrophy of the optic nerve, either one ofwhich might indicate the presence of glaucoma,was found in an additional 1-3% of the 40-59-year group and in another 2 5% of those over 60.A raised intraocular pressure (over 21 mmHg) on
Schi0tz tonometry, which may indicate open-angle glaucoma, was found in 3-7% of thosebetween 40 and 59 and 7 0% of those over 60,and about half of these individuals were found tohave very high (over 26 mmHg) pressures.
DiscussionA substantial part of the Kenyan rural popula-tion, particularly in older people, has beenshown to suffer from blinding or visually impair-ing eye disease. However, without a standard ofcomparison it is difficult to evaluate the severityofthe problem. Relevant population estimates ofa similar nature to this one are scarce.
It has been estimated that the prevalenceof blindness in the United States is 0.2%," butthis is based on a more liberal criterion forblindness (visual acuity equal to or less than6/60). Although it is impossible to give an exactcomparison with this figure because of the way inwhich acuities were recorded in this series ofsurveys, it can be estimated that approximately1-7% of rural Kenyans would have been blind by
Breakdown of corneal causes
\ Trachoma
I.::::: :/ ..LI- Trauma
Corneal impairment Xerophthalmia
Staphyloma/phthisis
Other corneal
Corneal blindness
.
338
on August 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.74.6.333 on 1 June 1990. D
ownloaded from

Blindness and eye disease in Kenya: ocular status survey resultsfrom theKenya RuralBlindness Prevention Project
this standard, a figure 8 5 times as large as therate in the USA.There have been two major recent population
based national surveys of eye disease in develop-ing countries, both of which used the sameWHO criterion for blindness employed in thisstudy. In Nepal the Ministry of Health/WHO"2reported a prevalence of 0 9% for blindness and1-9% for visual impairment. In Saudi ArabiaTabbara and Ross-Degnan'3 reported compar-able figures of 1-5% blind and 7-7% visuallyimpaired. In addition to these national studiesChirambo et al4 reported a blindness prevalenceof 13% in the Lower Shire Valley of Malawi.Rural Kenya, with an estimated 0-7% blind and2-5% impaired, is therefore quite similar overallto Nepal and much less severely affected thanSaudi Arabia. However, the two worst regions inthe Kenyan series - Meru and Kajiado - havesimilar prevalences of blindness to those foundnationally in Saudi Arabia, and one mightsuggest that 1-5% is typical of moderate tosevere trachoma environments in the developingworld.
It is not surprising that cataract was theleading cause ofvisual impairment and blindnessin rural Kenya. The WHO reports that it is theleading cause of blindness worldwide,3 despitethe fact that it is no longer a leading cause inindustrialised nations. Given the primacy ofcataract as a cause of visual loss, it is readily seenthat the major thrust ofany blindness preventionprogramme in an environment like Kenyashould be directed at cataract. Because thesupply of ophthalmologists in African countriesis typically very limited, cataract programmesare often most productive when they rely on non-ophthalmologists trained to perform simplifiedcataract extractions by a standardised surgicaltechnique. '5Trachoma was the second leading cause of
blindness overall in rural Kenya, but the preval-ence of both current inflammation and blindingsequelae varied widely among the survey areas.A variety of factors may be responsible for thisvariability, yet it is impossible to separate theirindependent effects because of their tendency tovary together in the areas studied.High in importance in the natural history of
blindness from trachoma would certainly beaccess to adequate supplies of water, since thedisease is easily controlled with adequatepersonal hygiene. People surveyed who live inarid areas of rural Kenya - the Masai in Kajiadoand the Pokot and Njemps in Baringo - tended tohave a higher prevalence of trachoma in all itsmanifestations. However, the first two tribes,and to a certain extent the third, also rely on theherding of livestock for economic livelihood andlive in quite close proximity to their animals.They are therefore exposed to an additionalrisk factor, the persistent eye seeking flies whichhave been implicated in the spread of thedisease.
Visual loss due to trachoma occurred withhighest prevalence not among these arid areagroups, however, but among the Meru. Thesepeople live in an area with rainfall adequate foragriculture, but with porous volcanic soil thatabsorbs water rapidly, passing it directly down to
a deep water table. This makes access to dailysupplies of water for hygiene a problem. How-ever, trachoma inflammation and blindness werealso found in Nyeri, where people enjoy quitegood rainfall, ready access to water and tomedical services, and a relatively high level ofsocioeconomic development for rural Kenya.But trachoma was not found among other ruraltribes living in similar circumstances. One mustconclude that in Nyeri, and to a certain extent inMeru, it is the cultural pattern ofhygiene that is amajor factor in the continuing presence of thedisease.
In addition to trachoma and cataract many ofthe other leading causes of visual loss in ruralKenya are preventable or curable. Some con-ditions are most appropriately addressed byincreasing access to prompt and effective treat-ment by primary care personnel throughout thehealth system. Much of the visual disability dueto trauma and other corneal lesions could beprevented in this manner. In addition, mostvisual impairment from refractive errors couldbe alleviated by access to optometric services andspectacles.A more difficult preventable problem, and an
extremely important one given its status as thirdleading cause of blindness, is that of glaucoma.For the same reasons that open-angle glaucomais underdiagnosed in field surveys it tends to gounnoticed in the general population. The onsetofvisual loss from glaucoma is typically slow andinsidious, and clinical signs are difficult torecognise and identify reliably. Generally neitherthe clinical signs nor loss of central visual acuityare apparent until late in the course of thedisease.The best available prevalence estimate for
glaucoma in a white population, from theFramingham Eye Study,'6 is 1-9% in people aged52 and older, an estimate based on very detailedvisual field examinations. The comparable groupin this age cohort in rural Kenya has a prevalenceof 2- 1% with visible pathologically cupped opticdisc and raised IOP, which represents anextremely conservative estimate of the preval-ence of glaucoma disease in all its stages.One can conclude that glaucoma is probably
considerably more prevalent in the Kenyan ruralpopulation than in Caucasian populations ofindustrialised nations, and that it represents amajor class of preventable blindness for whichthere is not yet any clearly defined strategy fordiagnosis and treatment. More detailed researchon its true prevalence and on the relative efficacyof methods of screening and treatment is clearlyindicated.
In summary, blindness and visual impairmenthave been shown to be much commoner in ruralKenya than in industralised countries. However,except for certain subgroups, rates of visualdisability are lower than those found in theMiddle East. The prevalence or visual loss risessharply with increasing age, and females have ahigher prevalence of visual loss than males,especially due to trachoma. Except for agerelated macular degeneration, the major causesof blindness - cataract, trachoma, glaucoma,refraction, and other corneal opacities - areeither preventable or curable.
339
on August 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.74.6.333 on 1 June 1990. D
ownloaded from

Whitfield, Schwab, Ross-Degnan, Steinkuller, Swartwood
This work was completed with the co-operation, material, andfinancial assistance of the Government of Kenya, the United StatesAgency for International Development, the World HealthOrganisation Programme for the Prevention of Blindness, theKenya Society for the Blind, institutional and private donors to theInternational Eye Foundation, the many dedicated people whoworked in these surveys, and the people of rural Kenya. It isdedicated to the memory of the late Dr John Harry King Jr, thefounder of the International Eye Foundation.
We acknowledge gratefully the assistance of the followingophthalmologists in the project: Niek Bakker, Houdijn Beekhuis,Nico Dekkers, Isao Hoshiwara, Harshvadan Mandalia, RobertMeaders, and Joseph 0 Ochola.
1 World Health Organisation. The prevention of blindness:Report of a WHO Study Group. WHO Tech Rep Ser 1973;518: 5-17.
2 World Health Organisation. The prevention of blindness.WHO Chron 1976; 30: 391-7.
3 WHO Programme Advisory Group on the Prevention ofBlindness. Data on blindness throughout the world. WHOChron 1979; 33: 275-83.
4 Thylefors B. Prevention of blindness: the current focus. WHOChron 1985; 39: 149-54.
5 Whitfield R, Schwab L, Bakker NJA, Bisley GG, Ross-Degnan D. Cataract and corneal opacity are the main causesofblindness in the Samburu tribe ofKenya. Ophthalmic Surg1983; 14: 139-44.
6 Arbuckle RD. The International Eye Foundation/KenyaRural Blindness Prevention Project. Soc Sci Med 1983; 17:1789-92.
7 Ross-Degnan D, Schwab L, Mburu FM. Field methodologyfor ocular surveys in rural Africa. Soc Sci Med 1983; 17:1793-6.
8 Henderson RH, Sundaresan T. Cluster sampling to assessimmunization coverage: a review of experience with asimplified sampling method. Bull WHO 1982; 60: 253-60.
9 World Health Organisation. Methods ofassessment ofavoidableblindness. Geneva: WHO Offset Publication, 1980: 54.
10 Dawson CR, Jones BR, Tarizzo ML. Guide to trachoma controlin programmes for the prevention of blindness. Geneva: WorldHealth Organisation, 1981.
11 National Society to Prevent Blindness. Vision problems in theUS. New York: National Society to Prevent Blindness,1980.
12 Ministry of Health, HM Government of Nepal, and BlindnessPrevention and Control Programme, World HealthOrganisation. The epidemiology ofblindness in Nepal: thefinalreport of the Nepal Blindness Survey. Kathmandu: Govern-ment of Nepal, 1982.
13 Tabbara KF, Ross-Degnan D. Blindness in Saudi Arabia.JAMA 1986; 255: 3378-84.
14 Chirambo MC, Tielsch JM, West KP Jr, et al. Blindness andvisual impairment in southern Malawi. Bull WHO 1986; 64:567-72.
15 Steinkuller P. Cataract: the leading cause of blindness andvision loss in Africa. Soc Sci Med 1983; 17: 1693-702.
16 Leibowitz HM, Kreuger DE, Maunder LR, et al. TheFramingham Eye Study Monograph. Surv Ophthalmol 1980;24 (suppl).
340
on August 1, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.74.6.333 on 1 June 1990. D
ownloaded from