blood pressure limbo how low to go?
TRANSCRIPT
4/16/2018
1
Joseph L. Kummer, MD, FACC
Bryan Heart Spring Conference
April 21st, 2018
Blood Pressure LIMBOHow Low To Go?
• Over a billion people have hypertension
• Major cause of morbidity and mortality, much mediated through cardiovascular disease
• Optimal BP goals are controversial. Need to balance benefits vs side effects, costs, and convenience of therapeutic interventions
Hypertension Epidemiology
• Over 60 million Americans have hypertension, a prevalence of about 3 of 10 adults
• About half of the US adult population older than 65 are hypertensive
• Of these, 70% are aware of their disease, 59% are receiving treatment, and only 34% are adequately treated
Hypertension Epidemiology

4/16/2018
2
• Treating hypertension has been shown to:
• Reduce Stroke by 35-40%
• Reduce Myocardial Infarction by 15-25%
• Reduce Heart Failure by up to 64%
Hypertension Epidemiology
• Goal BP for an otherwise healthy adult
• 140/90 mmHg
• With Diabetes or Renal Insufficiency
• 130/80 mmHg
• Without a compelling indication, start medical therapy with a diuretic. Strongly consider initial therapy with two medications.
JNC-7 Guidelines (2003)
JNC VII Lifestyle Modifications for BP Control
Modification Recommendation SBP Reduction
Weight Reduction Keep BMI 18.5-24.9 kg/m2 5-20 mmHg per 10kg Weight
Loss
DASH Eating Plan Fruits, vegetables, low-fat
dairy; reduced saturated and
total fat
8-14 mmHg
Dietary Sodium Restriction 2.4 gm Na+ (6 gm NaCl) daily 2-8 mmHg
Physical Activity At least 30 minutes aerobic
activity most days of the week
4-9 mmHg
Moderate EtOH Consumption Up to 2 drinks/day for men, 1
for women
2-4 mmHg
Chobanian AV et al. JAMA. 2003;289:2560-2572
4/16/2018
3
• ACCORD-BP1
• Excellent trial design
• 40-79 year olds with Type II DM
• 4377 Subjects, 5 Year follow-up (Released 2010)
• Known CAD (pre-existing or subclinical) or at least two additional CAD risk factors
ACCORD Trial
1 The ACCORD Study Group. NEJM 2010; 362:1575-1585.
• ACCORD-BP
• Compared SBP goal < 120 mmHg to < 140 mmHg in these high risk diabetics
• Several medication combinations used
• Primary end point
• Non-fatal MI, Non-fatal CVA, Cardiovascular Death
ACCORD Trial
• NO difference in major cardiac outcomes
• 40% lower absolute risk of non-fatal stroke
• Higher risk of adverse events in the intensive treatment group
• Hypotension, Renal Dysfunction, Hyperkalemia
• No difference in significant renal failure or ESRD
ACCORD Trial
4/16/2018
4
• Cardiac outcomes no better; fewer strokes offset by more complications, side effects
• Ultimately questioned BP Goals for diabetics and methodology for guidelines
• Less than or equal to 130 mmHg at the time
ACCORD Trial
• Released December, 2013
• Generally Higher (Less Intense) BP Goals
• Broadened initial BP med recommendations to 4 different categories
• Very strict trial criteria; only a handful of trials were included
• “Expert Opinion” was prevalently used
JNC-8
• In the general population ≥ 60 years of age, initiate pharmacologic treatment if SBP is ≥ 150 mmHg or DBP is ≥ 90 mmHg
• Strong Recommendation (Grade A)
Recommendation 1

4/16/2018
5
• There is insufficient evidence to support a SBP less than 140 mmHg compared to a goal SBP below 150 mmHg
• Several panel members dissented and wanted a goal < 140 mmHg based upon Expert Opinion
Recommendation 1
• In the general population < 60 y/o, initiate pharmacologic therapy for DBP ≥ 90 mmHg
• For 30-59 y/o, Strong Recommendation
• For 18-29 y/o, Expert Opinion
Recommendation 2
• In the general population < 60 y/o, initiate pharmacologic therapy for SBP ≥ 140 mmHg
• Expert Opinion (Grade E)
Recommendation 3

4/16/2018
6
• In the general population ≥ 18 y/o with CKD, initiate pharmacologic therapy for SBP ≥ 140 mmHg or DBP ≥ 90 mmHg
• Expert Opinion (Grade E)
Recommendation 4
• In the general population ≥ 18 y/o with DM, initiate pharmacologic therapy for SBP ≥ 140 mmHg or DBP ≥ 90 mmHg
• Expert Opinion (Grade E)
Recommendation 5
4/16/2018
7
• Systolic Blood Pressure Intervention Trial
• A Randomized Trial of Intensive vs. Standard Blood-Pressure Control. The SPRINT Research Group. NEJM. 373;22. Nov 26th, 2015
• https://www.sprinttrial.org
SPRINT Trial
• 9361 Enrolled
• At least 50 years old
• SBP ≥ 130 mmHg and ≤ 180 mmHg
• NOT Diabetic
• Increased Cardiovascular Risk
SPRINT Trial, Inclusion Criteria
• Increased Cardiovascular Risk (1 or more)
• Clinical or subclinical cardiovascular disease other than stroke
• CRI with GFR 20 to 60 ml/min/1.73 m2
• 10-year risk of CAD 15% or higher on Framingham Risk Score
• Age ≥ 75 years
• Not Diabetic
SPRINT Trial, Inclusion Criteria

4/16/2018
8
• Goal SBP ≤ 120 mmHg
OR
• Goal SBP ≤ 140 mmHg
SPRINT Trial, Randomization
• Primary Outcome was a composite of:
• Acute Myocardial Infarction
• Other Acute Coronary Syndromes
• Heart Failure
• Stroke
• Death from Cardiovascular Causes
• Secondary Outcome included Death from any Cause
SPRINT Trial, Primary Outcome
• After one year, Average Systolic BP:
• 121.4 mmHg in Intensive-Treatment group
• 136.2 mmHg in Standard-Treatment group
SPRINT Trial, Results
4/16/2018
9
• After one year, Average Diastolic BP:
• 68.7 mmHg in Intensive-Treatment group
• 76.3 mmHg in Standard-Treatment group
SPRINT Trial, Results
• Trial stopped after mean of 3.26 years of follow-up due to improvement in primary outcome in Intensive-Treatment group
SPRINT Trial, Results
• Event Rates:
• 2.19% in Standard-Treatment group
• 1.65% in Intensive-Treatment group
• HR 0.75. 95% CI [0.64-0.89], P < 0.001
SPRINT Trial, Results
4/16/2018
10
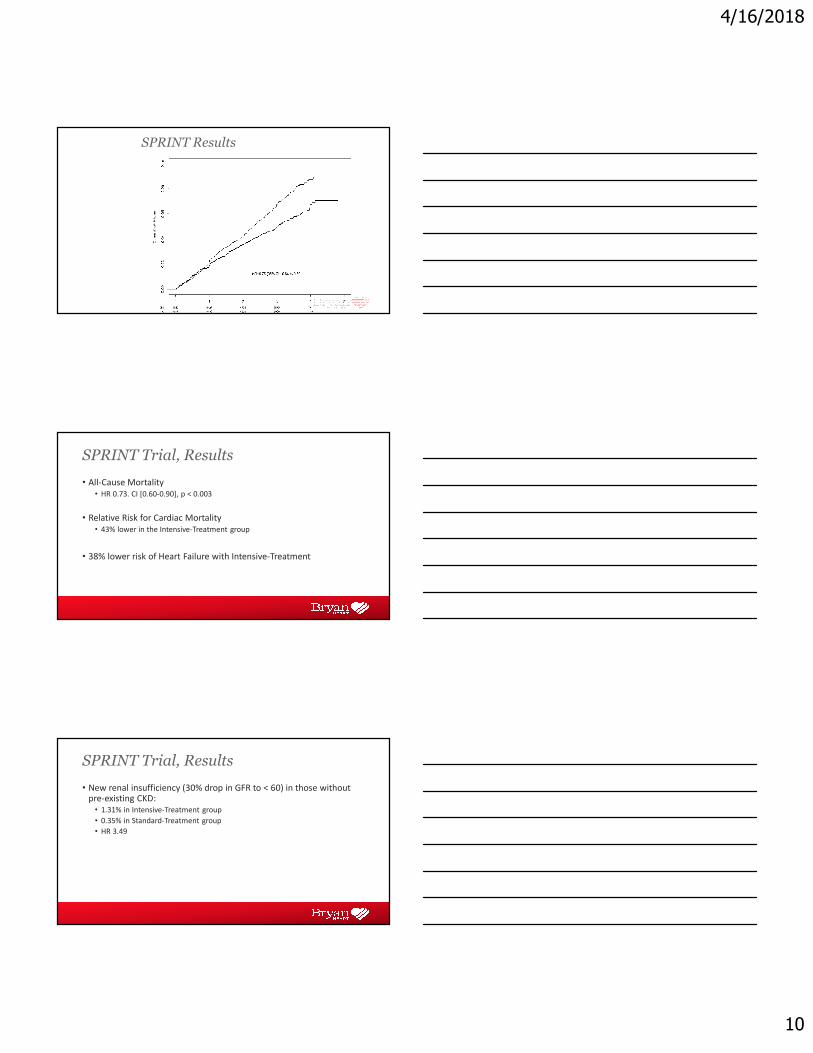
SPRINT Results
• All-Cause Mortality
• HR 0.73. CI [0.60-0.90], p < 0.003
• Relative Risk for Cardiac Mortality
• 43% lower in the Intensive-Treatment group
• 38% lower risk of Heart Failure with Intensive-Treatment
SPRINT Trial, Results
• New renal insufficiency (30% drop in GFR to < 60) in those without pre-existing CKD:
• 1.31% in Intensive-Treatment group
• 0.35% in Standard-Treatment group
• HR 3.49
SPRINT Trial, Results

4/16/2018
11
• Adverse Reactions attributed to the treatment intervention were more common in the Intensive-Treatment group
• Hypotension, Syncope, Electrolyte Abnormalities, Acute Kidney Injury
• 4.7% vs. 2.5%. HR 1.88, p < 0.001
SPRINT Trial, Adverse Reactions
• Adverse Reactions NOT more common in the Intensive-Treatment group included:
• Injurious Falls
• Bradycardia
SPRINT Trial, Adverse Reactions
• Goal SBP < 120 mmHg vs < 140 mmHg in non-diabetic patients at increased risk of CV events showed significant mortality and morbidity benefit with increase in relatively mild adverse events
SPRINT Conclusion

4/16/2018
12
• Non diabetic patients only
• Different than ACCORD (Diabetics, no benefit)
• Minimal to no medication guidelines
Considerations
• 123 studies met criteria; 613,815 subjects
• Every 10 mmHg reduction in BP
• Reduced Major Cardiac Events (RR 0.8)
• Reduced Coronary Events (RR 0.83)
• Reduced Stroke (RR 0.73)
• Reduced CHF (0.72)
• Reduced All-Cause Mortality (RR 0.83)
• NO change in renal failure
The Lancet, Meta-Analysis
• Benefits seems to span across all baseline systolic blood pressures
• Benefit was seen across several baseline co-morbidities (including CAD)
• Exceptions include DM and CKD, where the benefit was less clear
The Lancet, Meta-Analysis

4/16/2018
13
• B-Blockers were inferior to other meds for CAD, CVA, CKD prevention
• Calcium Channel Blockers were worse in CHF but better for CVA prevention
• Diuretics were superior for preventing CHF
The Lancet, Meta-Analysis
• “Blood pressure lowering significantly reduces vascular risk across various baseline blood pressure levels and comorbidities. Our results provide strong support for lowering blood pressure to systolic blood pressures less than 130 mm Hg and providing blood pressure lowering treatment to individuals with a history of cardiovascular disease, coronary heart disease, stroke, diabetes, heart failure, and chronic kidney disease.”
The Lancet, Meta-Analysis
• Authors’ Commentary
• This study calls for BP lowering to a greater extent than recommended in current guidelines
• As there was no lower BP threshold where benefit ceased, they recommended individualizing therapy based upon potential benefit, rather than universal BP goals
The Lancet, Meta-Analysis

4/16/2018
14
• Authors’ Commentary, cont.
• They emphasized the benefit across multiple co-morbidities and in those both with and without vascular disease. Hence, guidelines could be simplified
• Lastly, they emphasized benefits of certain medications over the others based upon risk factors or known diseases
The Lancet, Meta-Analysis
2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood
Pressure in Adults
• http://hyper.ahajournals.org/content/hypertensionaha/early/2017/11/10/HYP.0000000000000065.full.pdf
• Hypertension. 2017; HYP.00000000-00000066, November 13, 2017.
2017 Guidelines

4/16/2018
15
• JNC-7 released December 2003
• JNC-8 released December 2013
• NHLBI develops JNC
• ACC and AHA have had independent guidelines since 1980
Collaboration of Societies
• In 2013, NHLBI (JNC) and ACC/AHA Task Force decided to partner with each other and several other societies to develop unified guidelines
• The present guidelines were formulated as part of the ongoing efforts the AHA/ACC Task Force in collaboration with NHLBI
2107 Guideline Updates
• Comprehensive guideline review/updates every 6 years but also when new significant data arises
• The new guidelines are essentially an update of JNC-8 Guidelines
• SPRINT Trial likely a major reason for the present update
2107 Guideline Updates

4/16/2018
16
Hypertension – Defined
SBP DBP
Normal < 120 mmHg and < 80 mmHg
Elevated 120-129 mmHg and < 80 mmHg
Hypertension
- Stage 1 130-139 mmHg or 80-89 mmHg
- Stage 2 ≥ 140 mmHg or ≥ 90 mmHg
• Increased risk of cardiac events and stroke starts at fairly low blood pressure
• Several meta-analyses of observational data show the following:
• RR of event is 1.1-1.5 for SBP/DBP of 120-129/80-84 mmHg compared to < 120/80 mmHg
• RR of event is 1.5-2.0 for SBP/DBP of 130-139/85-89 mmHg compared to < 120/80 mmHg
Hypertension - Defined
• Severe hypertension is still generally considered to be average BP > 160/100 mmHg
• This was not extensively addressed in the new guidelines
Hypertension - Defined

4/16/2018
17
• SBP ≥ 130 mmHg or DBP ≥ 90 mmHg
• Pharmacologic therapy is indicated for secondary prevention in those with CVD
• Indicated for primary prevention in adults with a 10 year atherosclerotic disease risk of 10% or higher
Medical Therapy
• SBP ≥ 140 mmHg or DBP ≥ 90 mmHg
• Indicated for primary prevention in adults with a 10 year atherosclerotic disease risk of less than 10%
Medical Therapy
• http://www.cvriskcalculator.com
• http://tools.acc.org/ASCVD-Risk-Estimator-Plus/#!/calculate/estimate
ASCVD Risk Calculator
4/16/2018
18
• Product of ACC and AHA
• Estimates 10 year risk of an atherosclerotic event
• Intended for those with LDL < 190 and only for those without known disease (primary prevention)
ASCVD Risk Calculator
• Estimated risk of the following:
• Nonfatal heart attack
• Death from coronary artery disease
• Fatal and nonfatal stroke
ASCVD Risk Calculator
• Demographics
• Age
• Valid for ages 40-79
• Gender (Male/Female)
• Ethnicity
• Caucasian
• African American
• Other
• May under or overestimate for different ethnicities
ASCVD Risk Calculator

4/16/2018
19
• Cholesterol Data
• Total Cholesterol
• HDL
• LDL
• Blood Pressure
• Systolic BP
ASCVD Risk Calculator
• Personal History
• Diabetes
• On Treatment for Hypertension
• Smoker
• Yes, No, Former (When Quit)
• On a statin for high cholesterol
• On aspirin therapy
ASCVD Risk Calculator
• Will estimate risk reduction with:
• Smoking Cessation
• Start or intensify statin therapy
• Initiate blood pressure control medications
• Treat with Aspirin
ASCVD Risk Calculator

4/16/2018
20
• Provides advice on lifestyle and Medical Therapy changes
• Diet and Exercise
• Salt Restriction, Potassium Supplementation
• Smoking Cessation
• Cholesterol/Statin Therapy
• Starting BP Meds
ASCVD Risk Calculator
• Supposedly better than Framingham-based assessment
• Pooled cohort data
• More ethnic diversity
• Includes more outcomes
ASCVD Risk Calculator
• Factors NOT included but may be relevant
• Family History
• (1st Degree Male < 55, Female < 65)
• Elevated hsCRP
• Lifetime CVD Risk
• Coronary Calcium Score
• Ankle-Brachial Index
ASCVD Risk Calculator

4/16/2018
21
• The new AHA/ACA guidelines defining HTN as 130/80 mmHg “raised” the prevalence in the US adult population from 32% to 46%
• In other words, the new definition just “gave” a disease to 50 million Americans
Prevalence
1) Properly prepare the patient
2) Use Proper Technique
3) Take the Proper Measurement
4) Properly Document Accurate Readings
5) Average the Readings
6) Provide BP Readings to the Patient
Measurement of Blood Pressure
• Increase of SBP of greater than 20 mmHg and diastolic greater than 10 mmHg
• This often decreases with familiarity with the clinician as well as throughout the office visit
• It is also less severe with nurses rather than doctors taking the BP reading
White Coat Hypertension

4/16/2018
22
White Coat Hypertension
• Properly Prepare the Patient
• Patient relaxed, sitting in a chair for at least 5 minutes
• Avoid caffeine, smoking, and exercise for 30 minutes prior to assessment
• Ensure the patient has emptied their bladder
Measurement of Blood Pressure
• Properly Prepare the Patient
• Neither patient not observer should talk during the rest period nor during assessment
• Remove all clothing covering the cuff area
• Patient should not be sitting or lying on an exam table
Measurement of Blood Pressure
4/16/2018
23
• Use Proper Technique
• Use validated BP measurement device and make sure it’s calibrated properly
• Support the patient’s arm (resting on a desk)
• Position middle of cuff at level of right atrium (mid-sternum)
Measurement of Blood Pressure
• Use Proper Technique
• Use proper cuff size (80% of bladder encircles the arm)
• Too small of a cuff falsely increases measurement
• Too big falsely lowers the reading
• Use either the bell or diaphragm of the stethoscope
Measurement of Blood Pressure
• Take the Proper Measurement
• At least at first visit, take BP in both arms and use higher reading from then on
• Wait 1-2 minutes between repeat measurement
• For auscultatory measurements use radial artery obliteration first, then inflate 20-30 mmHg above this level
• Deflate cuff by 2 mmHg per second
Measurement of Blood Pressure

4/16/2018
24
• Properly Document Accurate BP Readings
• Record SBP and DBP
• Onset of first Korotkoff sound and disappearance of all Korotkoff sounds
• Note time of administration of last BP medications
Measurement of Blood Pressure
• Average the Readings
• Average of ≥ 2 readings obtained on ≥ 2 different occasions
Measurement of Blood Pressure
• Provide BP Readings to the Patient
• Provide SBP and DBP readings to patient both verbally and in writing
Measurement of Blood Pressure

4/16/2018
25
• ACC/AHA/AAPA/ABC/ACPM/AGS/-APhA/ASH/ASPC/NMA/PCNA
• Notably absent is AAFP
AAFP?
• The American College of Physicians and American Academy of Family Physicians disagree with the ACC/AHA Guidelines
• They released their guidelines 1/17/2017
• Ann Intern Med. 2017;166(6):430-437
ACP and AAFP
• AAFP announced in December 2017 that it does NOT endorse the ACC/AHA Guidelines
• The ACP and AAFP continue to endorse the 2014 JNC-8 Guidelines
• https://www.aafp.org/patient-care/clinical-recommendations/non-endorsed.html
Non-Endorsement
4/16/2018
26
• Guidelines not based upon a sufficient systematic review of the evidence
• Only 4 key questions had a systematic review out of over 100 recommendations
• Harms of lower BP goals not systematically reviewed
Non-Endorsement Rationale
• The systematic review that was provided suggested a small benefit for lower BP goals in cardiac events but not mortality, MI, or renal events
• This review has similar conclusions to that performed for the ACP/AAFP Guidelines
• Therefore, AAFP recommends shared decision-making with some patients about the risks vs benefits of this
Non-Endorsement Rationale
• The recommendation statements included a grade for the strength of evidence, but assessments of the quality of individual studies or systematic reviews were not provided.
Non-Endorsement Rationale
4/16/2018
27
• Substantial weight was given to the SPRINT trial while results from other trials were minimized
• The SPRINT trial was stopped early due to benefit leading to the potential for exaggerated benefits and an under reporting of harms
Non-Endorsement Rationale
• Conflicts of Interest
• The Chair of the SPRINT trial steering committee was commissioned as chair of the guideline panel
• Several other members of the panel also have intellectual conflicts of interest
Non-Endorsement Rationale
• The guideline recommends the use of the ASCVD risk assessment tool to determine whether medications should be initiated for BP control (strong recommendation). This recommendation is not based on evidence that using the tool in this way improves outcomes.
Non-Endorsement Rationale
4/16/2018
28
• Ann Intern Med. 2017;166(6):430-437
• For adults 60 years and older
• Published March 2017
ACP and AAFP Guidelines
• Recommendation #1
• Initiate medical therapy at SBP 150 mmHg with goal < 150 mmHg to reduce mortality, stroke, and cardiovascular events
• Discuss risks/benefits and BP goals with patient first
ACP and AAFP Guidelines
• Recommendation #2
• Consider pharmacologic therapy with a goal of SBP < 140 mmHg for patients with a history of TIA or CVA to reduce risk of stroke
ACP and AAFP Guidelines

4/16/2018
29
• Recommendation #3
• Consider pharmacologic therapy with a goal of SBP < 140 mmHg for patients with high cardiovascular risk, based on individualized assessment, to reduce risk of stroke or cardiac events
ACP and AAFP Guidelines