blood pressure— the driving force stephen hales 1733 blood pressure (hydrostatic pressure) is the...
TRANSCRIPT

Blood Pressure—The driving force Stephen Hales
1733• Blood pressure (hydrostatic pressure) is the force exerted by the blood against any unit area of vessel wall.
• Measured in millimeters of mercury (mmHg). A pressure of 100 mmHg means the force of blood was sufficient to push a column of mercury 100mm high.
• All vessels have it – but we’re usually addressing arteries when we refer to it.

Blood Pressure Profile in the Circulatory System
Systemic Pulmonary
Aor
ta
Lar
ge a
rter
ies
Smal
l art
erie
s
Art
erio
les
Cap
illa
ries
Pre
ssu
re(m
mH
g)
0
20
40
60
80
100
120
Ven
ule
s
Smal
l vie
ns
Lar
ge v
ien
s
Ven
ae c
avae
Pu
lmon
ary
arte
ries
Art
erio
les
Cap
illa
ries
Ven
ule
s
Pu
lmon
ary
vien
s
Circulatory pressure- averages 100mmHg Arterial blood pressure-100-35mmHgCapillary pressure- 35mmHg at beginning and 10-15mmHg at endVenous pressure-15-0mmHg
•Large pressure drop across the arteriolar-capillary junction
Measurement of Blood Pressure
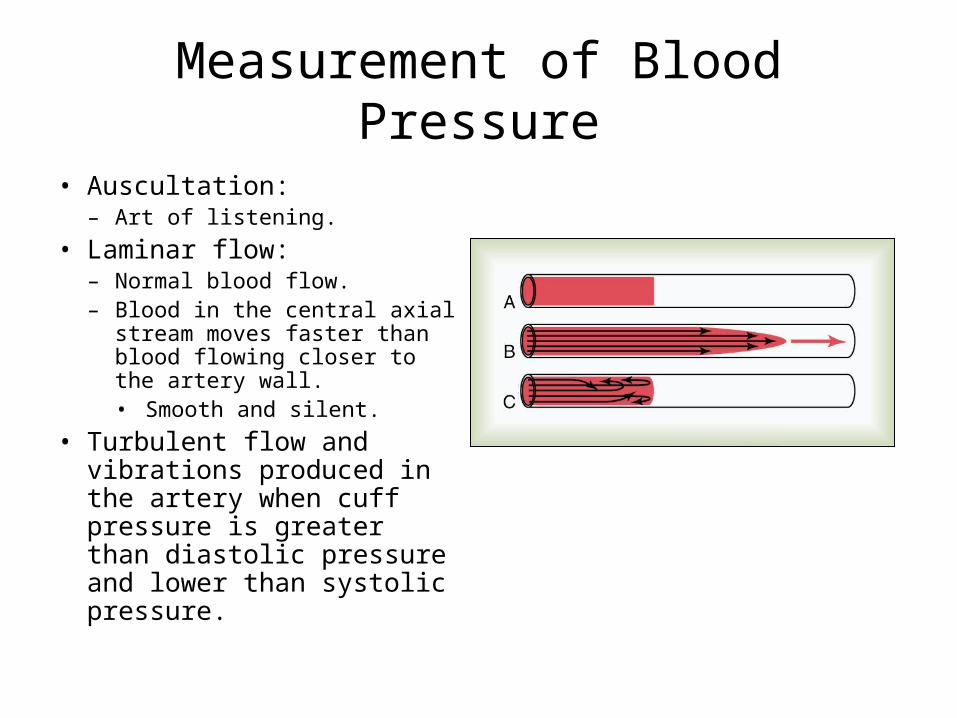
• Auscultation:– Art of listening.
• Laminar flow:– Normal blood flow. – Blood in the central axial
stream moves faster than blood flowing closer to the artery wall.• Smooth and silent.
• Turbulent flow and vibrations produced in the artery when cuff pressure is greater than diastolic pressure and lower than systolic pressure.
Measurement of Blood Pressure (continued)
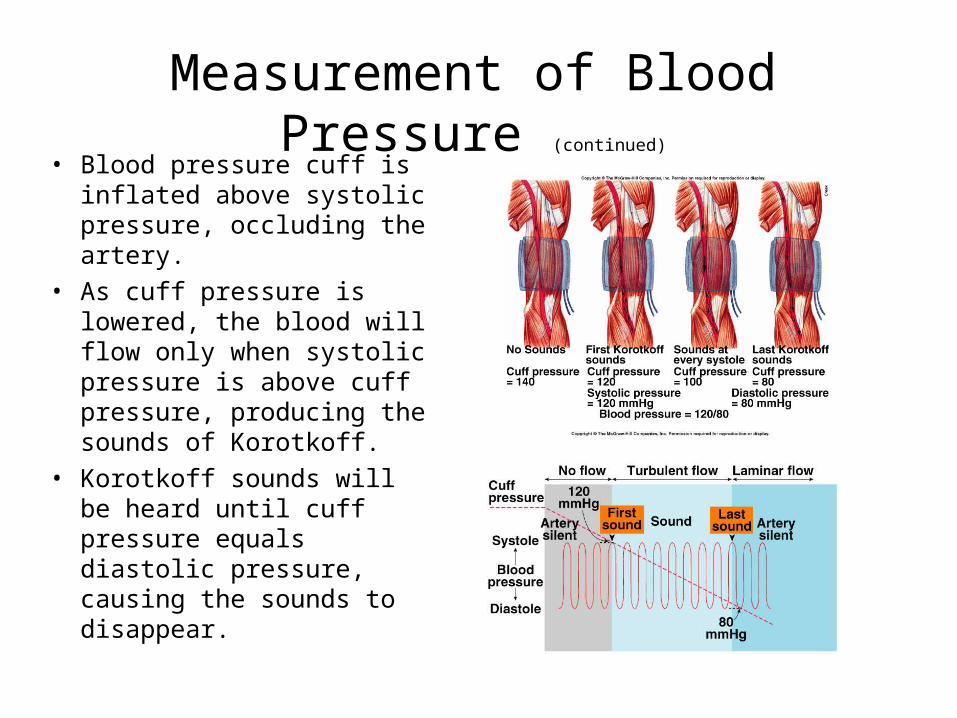
• Blood pressure cuff is inflated above systolic pressure, occluding the artery.
• As cuff pressure is lowered, the blood will flow only when systolic pressure is above cuff pressure, producing the sounds of Korotkoff.
• Korotkoff sounds will be heard until cuff pressure equals diastolic pressure, causing the sounds to disappear.
Measurement of Blood Pressure (continued)
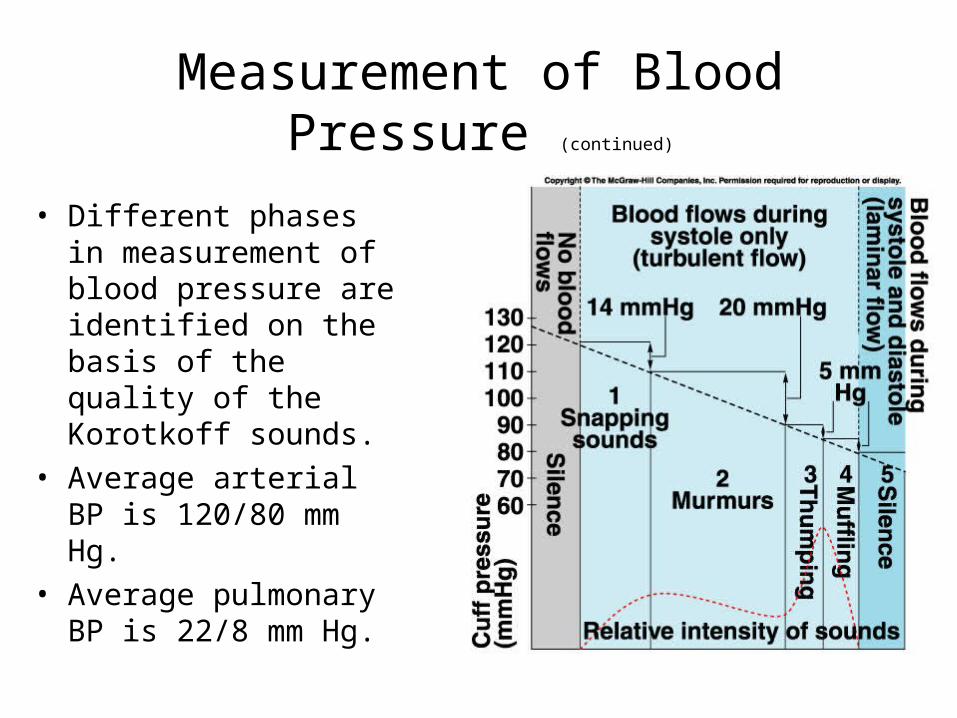
• Different phases in measurement of blood pressure are identified on the basis of the quality of the Korotkoff sounds.
• Average arterial BP is 120/80 mm Hg.
• Average pulmonary BP is 22/8 mm Hg.

Central Venous Pressure• Pressure in the right atrium is called
central venous pressure.
• determined by the balance of the heart pumping blood out of the right atrium and flow of blood from the large veins into the right atrium.
• normally 0 mmHg, but can be as high as 20-30 mmHg.
• More vigorous heart contraction (lower CVP).
• Less heart contraction (higher CVP)• Factors that increase CVP:
- increased blood volume- increased venous tone- dilation of arterioles- decreased cardiac function- Skeletal and respiratory pumps
Figure 15-9; Guyton and Hall

Your lab today and CVP
• Not holding breath—• Raising arm- should
take smaller elevation of arm for the blood in your hand veins to over come the somewhat collapsed veins in arm
Blood pressure here becomes greater and over comes pressure in downstream veins

Your lab today and CVP• Holding valsalva
maneuver —• Increases peripheral
venous pressure (simulating elevated CVP)
• Raising arm- should take a higher elevation of arm for the blood in your hand veins to over come the very collapsed veins in chest
Blood pressure here becomes greater and over comes pressure in downstream veins

A decrease in blood pressure is detected by baroreceptors found in the aortic arch and carotid bodies. Afferent impulses are transmitted through cranial nerve X and IX, respectively toward the medulla oblongata for integration.

In the medulla oblongata the decreased rate of action potentials arriving from cranial nerve X and IX, stimulates the cardioacceleratory and vasomotor centers within the medulla oblongata.

Sympathetic outflow from the medulla oblongata increases and stimulates preganglionic cell bodies found at levels (T1-T6).
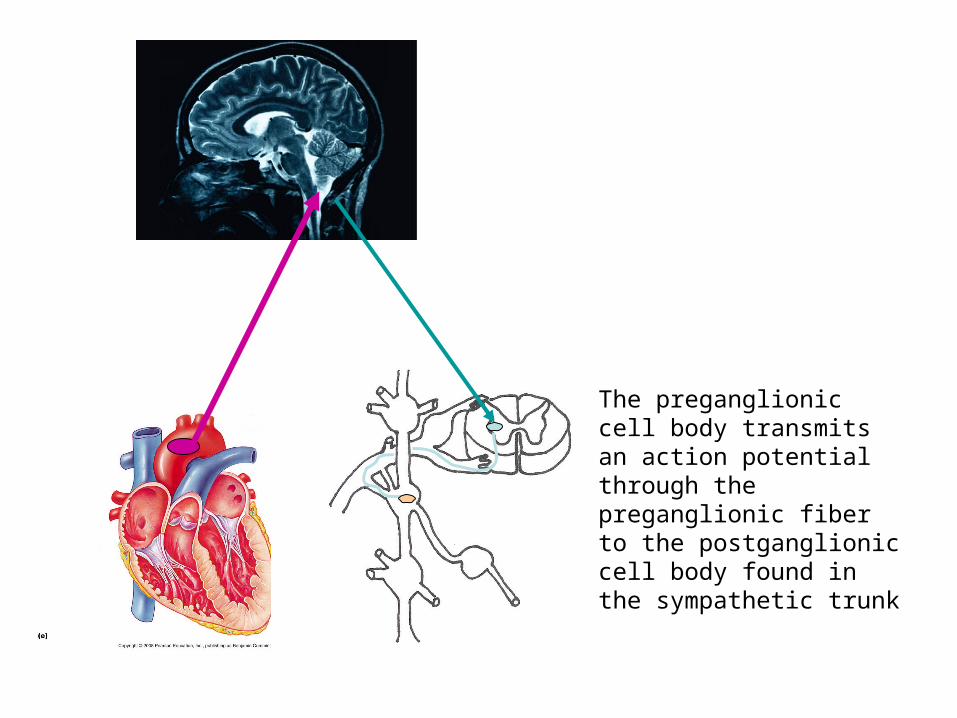
The preganglionic cell body transmits an action potential through the preganglionic fiber to the postganglionic cell body found in the sympathetic trunk

The postganglionic fiber transmits an action potential to the conductive fibers of the heart that leads to increased heart rate and contractility
How is this reflex arc different if too much stroke volume (i.e., too much pressure) is detected?
Valsalva maneuver
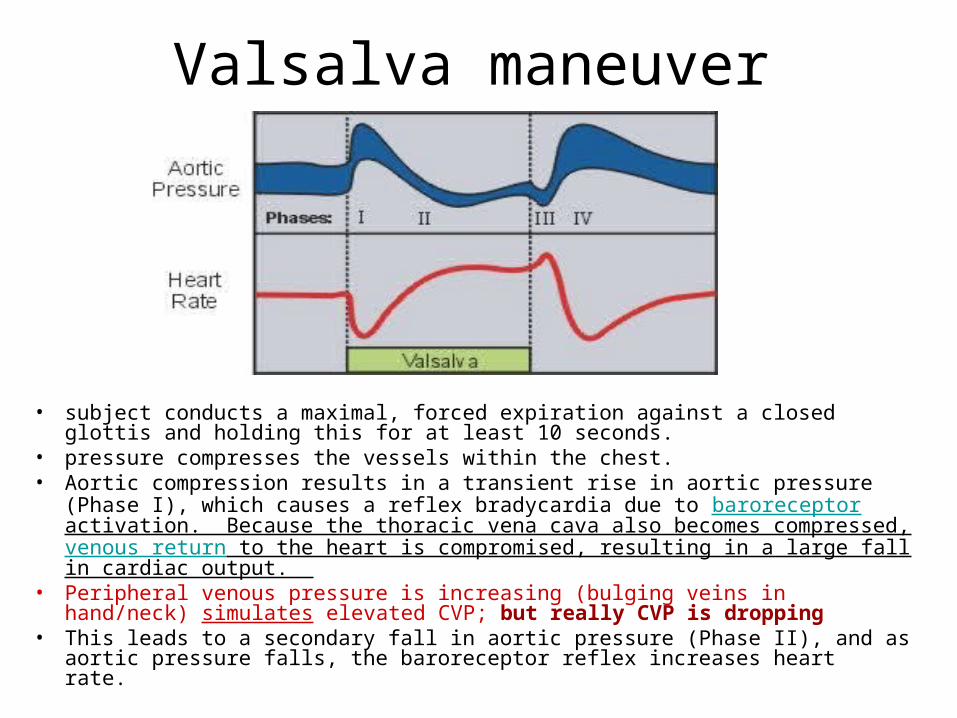
• subject conducts a maximal, forced expiration against a closed glottis and holding this for at least 10 seconds.
• pressure compresses the vessels within the chest. • Aortic compression results in a transient rise in aortic pressure (Phase I), which
causes a reflex bradycardia due to baroreceptor activation. Because the thoracic vena cava also becomes compressed, venous return to the heart is compromised, resulting in a large fall in cardiac output.
• Peripheral venous pressure is increasing (bulging veins in hand/neck) simulates elevated CVP; but really CVP is dropping
• This leads to a secondary fall in aortic pressure (Phase II), and as aortic pressure falls, the baroreceptor reflex increases heart rate.
Valsalva Maneuver
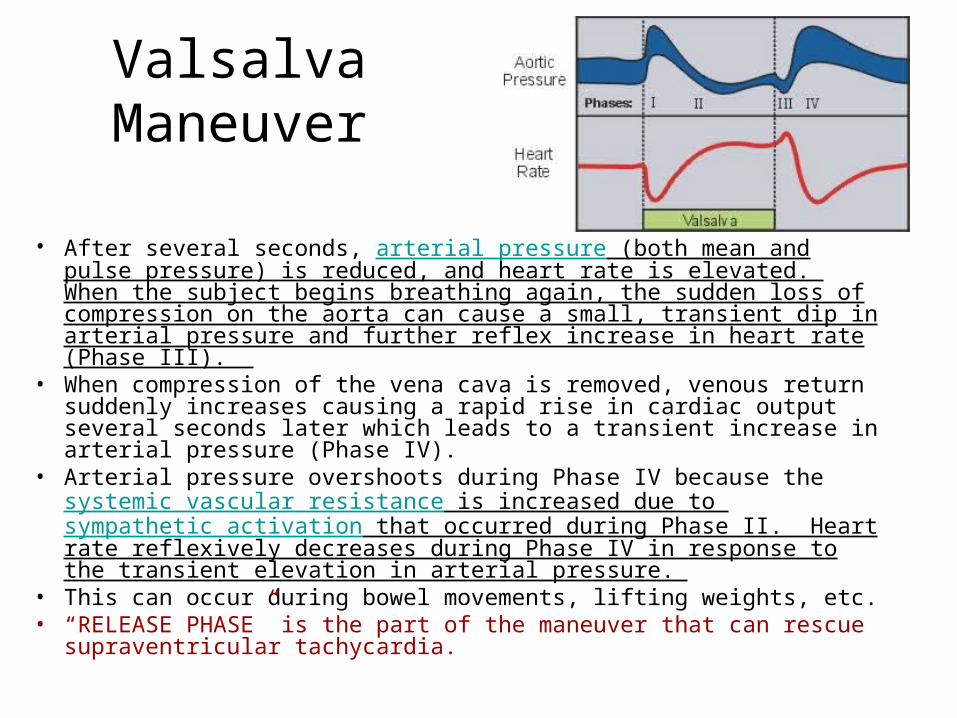
• After several seconds, arterial pressure (both mean and pulse pressure) is reduced, and heart rate is elevated. When the subject begins breathing again, the sudden loss of compression on the aorta can cause a small, transient dip in arterial pressure and further reflex increase in heart rate (Phase III).
• When compression of the vena cava is removed, venous return suddenly increases causing a rapid rise in cardiac output several seconds later which leads to a transient increase in arterial pressure (Phase IV).
• Arterial pressure overshoots during Phase IV because the systemic vascular resistance is increased due to sympathetic activation that occurred during Phase II. Heart rate reflexively decreases during Phase IV in response to the transient elevation in arterial pressure.
• This can occur during bowel movements, lifting weights, etc.• “RELEASE PHASE” is the part of the maneuver that can rescue
supraventricular tachycardia.