blue cross blue shield of michigan is a nonprofit corporation and independent licensee of the blue...
TRANSCRIPT

Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee of the Blue Cross and Blue Shield Association.
Decision Analytic Modeling for Wellness and Care Management
Disease Management ColloquiumMay 20, 2008
Richard E. Ward, MD, MBAVice President, Clinical Programs and Medical Informatics
Blue Cross Blue Shield of Michigan

2
BCBSM MembersBCBSM Members
Effective ProvidersEffective Providers
Car
eR
elat
ions
hip
Basics -Medical Policy-Pre-certification-Utilization Review
Michigan
BCBSM Clinical Programs
Support
Wellness & Care Management

3
BlueHealthConnection components
Medicare DM (Health Dialog)
Medicare DM (Health Dialog)
Complex Case Management
(Internal)
Complex Case Management
(Internal)
Hysterectomy for Benign Uterine
Conditions
Hysterectomy for Benign Uterine
Conditions
Health Risk AppraisalHealth Risk Appraisal
DepressionDepression
Personal Health Record +
Dashboard
Personal Health Record +
Dashboard
24-hour Nurse Line24-hour Nurse Line
Complex Case Management (CareGuide)
Complex Case Management (CareGuide)
Medicare Complex Case Management
(CareGuide)
Medicare Complex Case Management
(CareGuide)
Case Management
(Internal)
Case Management
(Internal)
Medicare Case Management (CareGuide)
Medicare Case Management (CareGuide)
Asthma DMAsthma DM
Hip ReplacementHip Replacement
Knee ReplacementKnee Replacement
Lumbar Back Surgery
Lumbar Back Surgery
Acute/Chronic Back Pain
Acute/Chronic Back Pain
Prostatectomy for Benign Prostate
Enlargement
Prostatectomy for Benign Prostate
Enlargement
Audio LibraryAudio Library
Healthwise Self-Help Book
Healthwise Self-Help Book
Living Health MagazineLiving Health Magazine
Chronic Disease Gaps-in-Care Alert
Chronic Disease Gaps-in-Care Alert
Quit-the-NicQuit-the-Nic
Health FairsHealth Fairs
Biometric MeasurementBiometric Measurement
Wellness Incentive Tracking
Wellness Incentive Tracking
Retrospective Claim Review
Retrospective Claim Review
Consultation about worksite initiatives
Consultation about worksite initiatives
Online Health Managers
(Asthma, Arthritis, Pregnancy)
Online Health Managers
(Asthma, Arthritis, Pregnancy)
Prevention RemindersPrevention Reminders
Medication Treatment Mgmt
Medication Treatment Mgmt
Medical Encyclopedia
Medical Encyclopedia
Drug GuideDrug Guide
Drug Interaction Checker
Drug Interaction Checker
Fitness AssessmentFitness Assessment
(Not a complete list)
Walking WorksWalking Works
Worksite Educ ClassesWorksite Educ Classes
Premium Incentive Tracking
Premium Incentive Tracking
Affinity ProgramsAffinity Programs
Subimo Provider Profiles
Subimo Provider Profiles
Screening for Depression
Screening for Depression
COPD DMCOPD DM
CHD DMCHD DM
CAD DMCAD DM
Diabetes DMDiabetes DM
ChronicConditions
ChronicConditionsWellnessWellness Concerns
& Symptoms
Concerns
& SymptomsAcute
Conditions
Acute Conditions
Preference Sensitive
Conditions
Preference Sensitive
Conditions
Complex Catastrophic Conditions
Complex Catastrophic Conditions
Continuum of member needs

4
Outline
• Consultative Tailoring
• Optimization using Decision Analytic Modeling– Steady State Models
– Dynamic “Ramp Up” Models
– Stochastic Models: Monte Carlo Simulation
• Medical Home-based Coaching
• IT Architecture to support mass customization and multi-party process integration

5
Develop a collection of mix and match wellness & care management componentsDevelop a collection of mix and match wellness & care management components
COPDDiseaseMgmt
IHDDisease Mgmt
DiabetesDiseaseMgmt
CHFDiseaseMgmt
Health Risk Appraisal
Smoking Cessation
AsthmaDiseaseMgmt
DepressionDiseaseMgmt
Back Surg Decision Making
Hip Surgery Decision Making
Incentive Tracking
BUCDecisionMaking
Etc.
CHF Disease MgmtPerformance Characteristics
for this configuration
Yr 2 --------PMPM Cost: $0.07Identify% 0.4%Target % 87%Engage % 36%Admits Avoided 206PMPM Savings: $0.58PMPM Net Savings: $0.51ROI: 7.96
Card Revasc Decision Making
Knee Surg Decision Making
End-of-Life Care Coord
RareConditions
Mgmt
SmokingCessation
WorksiteWellnessConsult
Medicare Case Mgmt
Long Term Care Coord
Intervention Intensity
(Parameters vary by component)
High
80%90%
70%Low
Med
EngagementIncentive Level
40 pts30 pts20 pts
CHF Disease Mgmt Configuration Parameters
TargetPenetration
Consultative Tailoring
6
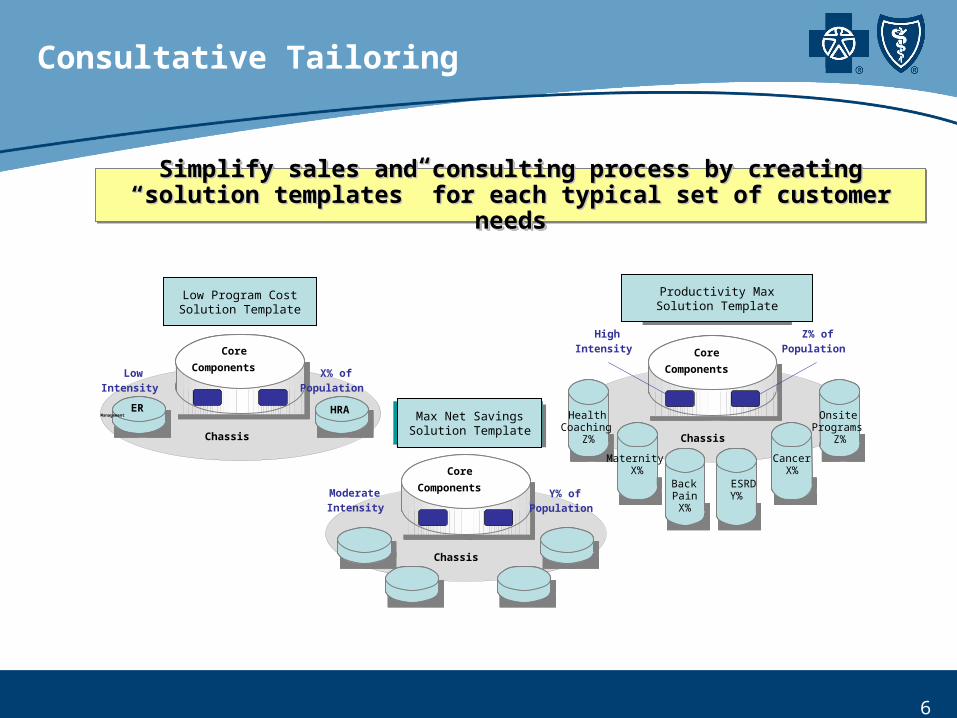
Simplify sales and consulting process by creatingSimplify sales and consulting process by creating““solution templates” for each typical set of customer needssolution templates” for each typical set of customer needs
Simplify sales and consulting process by creatingSimplify sales and consulting process by creating““solution templates” for each typical set of customer needssolution templates” for each typical set of customer needs
Core
Components
Core
Components
HRA
HRA
Chassis
Core
Components
Core
Components
Chassis
ModerateIntensity
Y% ofPopulation
Core
Components
Core
Components
Chassis
HighIntensity
Z% ofPopulation
HealthCoaching
Z%
MaternityX%
BackPainX%
ESRD
Y%
CancerX%
OnsitePrograms
Z%
Targeted Focus
Solution
Targeted Focus
Solution
Robust
Solution
Robust
Solution
Basic
Solution
BasicSolution
LowIntensity
X% ofPopulation
ERManagement
Consultative Tailoring
Low Program CostSolution Template
Max Net SavingsSolution Template
Productivity MaxSolution Template

7
Dedicated wellness & care mgmt
consulting team interacts with
customer and sales team to understand
customer needs
Consultative Tailoring
Consultant identifies solution
template closest to customer’s need
and uses it as basis for making a
proposal to customer
Consultant and sales team interact with customer to
tailor solution to customer
Flexible information technology platform uses business process mgmt / workflow technology to
facilitate efficient delivery of the solution
Enhanced medical informatics
capabilities enable measurement of
activity and outcomes to be
reported to customer
Consultant and sales periodically
interact with customer to provide
reports & to recommend course
corrections
Listen Propose Tailor
DeliverMeasureRevise

8
Wellness & Care Mgmt Analytics
Plausibility of Value as Justification Effect Size -> Power Calcs -> Sample Size
Evidence-based Parameter Assumptions
EVALUATIONRESEARCH
MeasuringOutcomes
Compared toControl Group
DECISIONANALYSIS
ProjectingOutcomes
For AlternativeIntervention
Designs
WhichComesFirst?

9
Decision Analytic Models
Assumptions
Epidemiology ---- ----Effectiveness ---- ----Economic ---- ----Preferences ----- -----
Optimistic Best Pessimistic-------------- ------ ----------------
Calculations Results

10
Role of Predictive Models
Inpatient Admission Rate by Percentile Rank of Risk Score
0
100
200
300
400
500
600
700
0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 95 100
Risk Percentile
Ad
mit
s P
er T
ho
usa
nd
Per
Yea
r
Diabetes
Highest Risk= Best Candidate
Lowest Risk= Worst Candidate
Diabetes
Threshold
Y NWhich Threshold ValueIs Optimal?-- Depends on Intervention-- Depends on Objectives

11
Diabetes Disease Management
(1,000,000)
-
1,000,000
2,000,000
3,000,000
4,000,000
5,000,000
0% 5% 10%
15%
20%
25%
30%
35%
40%
45%
50%
55%
60%
65%
70%
75%
80%
85%
90%
95%
100%
Finding Target Penetration that Yields Max Net Savings
Gross Savings
Cost
Net Savings
Dollars
Target Penetration Rate (as % of Diabetes population)
41%
Fixed Cost

12
Highest ROI Does Not Yield Maximum Net Savings
Diabetes Disease Management
(1,000,000)
-
1,000,000
2,000,000
3,000,000
4,000,000
5,000,0000% 5% 10%
15%
20%
25%
30%
35%
40%
45%
50%
55%
60%
65%
70%
75%
80%
85%
90%
95%
100%
-
0.50
1.00
1.50
2.00
2.50
Gross Savings
Cost
Net Savings
ROIDollars
41%18%
Fixed Cost
ROI*
Increasing the target penetration rate from 18% to 41% leads to a lower ROI, but the net savings
increases by 24%.
Target Penetration Rate (as % of Diabetes population)
13
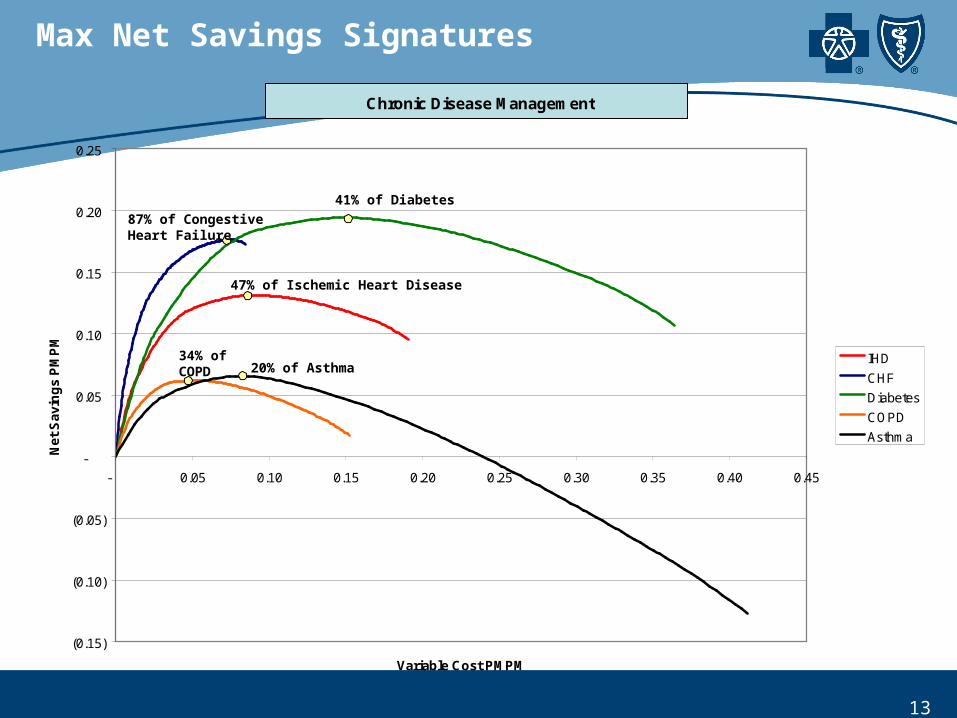
Chronic Disease Management
(0.15)
(0.10)
(0.05)
-
0.05
0.10
0.15
0.20
0.25
- 0.05 0.10 0.15 0.20 0.25 0.30 0.35 0.40 0.45
Variable Cost PMPM
Net
Sav
ing
s P
MP
M
IHD
CHF
Diabetes
COPD
Asthma
47% of Ischemic Heart Disease
87% of CongestiveHeart Failure
41% of Diabetes
34% ofCOPD 20% of Asthma
Max Net Savings Signatures

14
Preference-Sensitive Condition Management
(0.12)
(0.10)
(0.08)
(0.06)
(0.04)
(0.02)
-
0.02
0.04
0.06
0.08
- 0.05 0.10 0.15 0.20 0.25
Variable Cost PMPM
Net
Sav
ing
PM
PM Back Surg
Knee Repl Surg
Revasc Surg
BUC
Hip Repl Surg
BPH
7% of Back Surgery
43% of Knee Replacement Surgery
9% of Cardiac Revasc Surgery
5% of Surgery for Benign Uterine Conditions
6% of Hip Replacement Surgery
0% of Surg forBenign ProstaticHypertrophy
Max Net Savings Signatures

15
Dynamic Models
Disease ManagementAssumed Time Distribution of Savings for an Engaged Case
0%
5%
10%
15%
20%
25%
Month 1 Month 2 Month 3 Month 4 Month 5 Month 6 Month 7 Month 8 Month 9 Month 10
Cohort Sub-model:
Calendar Sub-model:

16
Dynamic Models
-$500,000
$0
$500,000
$1,000,000
$1,500,000
$2,000,000
$2,500,000
$3,000,000
$3,500,000
$4,000,000
Jan-
07
Feb
-07
Mar
-07
Apr
-07
May
-07
Jun-
07
Jul-0
7
Aug
-07
Sep
-07
Oct
-07
Nov
-07
Dec
-07
Jan-
08
Feb
-08
Mar
-08
Apr
-08
May
-08
Jun-
08
Jul-0
8
Aug
-08
Sep
-08
Oct
-08
Nov
-08
Dec
-08
Jan-
09
Feb
-09
Mar
-09
Apr
-09
May
-09
Jun-
09
Jul-0
9
Aug
-09
Sep
-09
Oct
-09
Nov
-09
Dec
-09
2007 Calculated$5.3M net savings
$9.9M gross savings
$4.6M cost
$35.5M gross savings
$21.8M net savings
$13.7M cost $14.0M cost
$26.7M net savings
$40.7M gross savings
2008 Projected 2009 Projected
Disease Management
RAMP-UPPHASE
STEADYSTATE
SATURATION/DECLINE?

17
Dynamic Models
-$200,000
$0
$200,000
$400,000
$600,000
$800,000
$1,000,000
$1,200,000
$1,400,000
$1,600,000
No
v-06
Dec
-06
Jan
-07
Feb
-07
Mar
-07
Ap
r-07
May
-07
Jun
-07
Jul-
07
Au
g-0
7
Sep
-07
Oct
-07
No
v-07
Dec
-07
Jan
-08
Feb
-08
Mar
-08
Ap
r-08
May
-08
Jun
-08
Jul-
08
Au
g-0
8
Sep
-08
Oct
-08
No
v-08
Dec
-08
Jan
-09
Feb
-09
Mar
-09
Ap
r-09
May
-09
Jun
-09
Jul-
09
Au
g-0
9
Sep
-09
Oct
-09
No
v-09
Dec
-09
2007 2008 2009
$16.9Mprojected
$8.7Mprojected
$8.7Mprojected
$7.1Mprojected
$4.1Mcalculated
Lower Intensity ($2.9 million program cost per year)
Higher Intensity ($5.4 million program cost per year)
Case Management Net SavingsCase Management

18
Analyzing Uncertainty
• When buying a bond, we intuitively understand that we need to know:– Price (cost, investment)– Yield (benefit, return)– Bond rating (uncertainty).
• Cost-Effectiveness & ROI consider only price and yield.• Evidence-Based Medicine (EBM) considers only uncertainty.• We need to consider all three.

19
Analyzing Uncertainty
• One-way Sensitivity Analysis– But there is uncertainty about many assumptions…
• Best & Worst Case Scenario Analysis– But the joint probability of “worst case” for every
assumption is exceedingly rare & irrelevant…
• Multi-way Sensitivity Analysis: Monte Carlo Simulation– Stochastic assumptions (shapes, not values)

20
Monte Carlo Simulation
Assumptions
Calculations
90% Interval of Uncertainty

21
Medical Home-based Coaching
• Traditional DM Industry Concept of Integration with Provider– Encourage providers to refer patients to health plan’s coaches– Send “gaps in care” reminders
• BCBSM’s deeper level of provider integration– 4 year goal: 25% of Blue Health Connection coaching done by
staff of primary care practices– Coordination and data exchange necessary to support customer
reporting of activity and outcomes

22
Patient Centered Medical Home
American Academy of Family PhysiciansAmerican Academy of PediatricsAmerican College of PhysiciansAmerican Osteopathic Association
• Care planning based on partnership of patient, patient’s family and personal physician
• Enhanced access • Whole person orientation• Focus of safety, quality, evidence-based
medicine• Integration and coordination of care,
facilitated by information technology• Physician practice accepts responsibility,
held accountable based on performance measures
• Payment structure redesign, including gain-sharing and performance-based components.

23
Physician Group Incentive Program
Initiatives to develop capabilities for collaborative improvement• Establishing staff dedicated to managing or coaching process improvement teams• Establishing analytics and reporting staff• *Performance reporting
Condition-specific initiatives• Diabetes management through Lean Thinking-Clinic Re-engineering CQI• CHF management through Lean Thinking-Clinic Re-engineering CQI
Service-specific initiatives• Increase the use of generic drugs• Radiology procedures utilization• Improve Oncology Practice Performance• Anticoagulation management
Core clinical process initiatives• *Evidence based care tracking/patient registry• *Patient-Provider agreement.• *Extended access• *Individual care management• *Test tracking and follow-up
Clinical information technology initiatives:• *Electronic prescribing
2
3
4
5
1
*Components of the Patient Centered Medical Home (PC-MH)

24
Patient Centered Medical Home
PCPPCP
PCP
PCP
PCPPCP
PCP
PCP
PCPPCP
PCP
PCP
PCP
PCP
PCPPCP
PCPPCP
PCPPCP
PCP
PCP
PCPPCP
PCP
PCP PCP
PCP
PCP PCPPCP
PCP
PCP
PCP
PCPPCP
PCP
PCP
PCP
PCP
PGIP Phys Org A
PGIP Phys Org B
PGIP Phys Org C“ControlGroup”
PC-MHNominee
PC-MHNominee
PC-MHNominee
PC-MHNominee
PC-MHNominee
PC-MHNominee

25
Patient Centered Medical Home
PCPPCP
PCP
PCP
PCPPCP
PCP
PCP
PCPPCP
PCP
PCP
PCP
PCP
PCPPCP
PCPPCP
PCPPCP
PCP
PCP
PCPPCP
PCP
PCP PCP
PCP
PCP PCPPCP
PCP
PCP
PCP
PCPPCP
PCP
PCP
PCP
PCP
PC-MH
PC-MH
PC-MHPGIP Phys Org A
PGIP Phys Org B
PGIP Phys Org C“ControlGroup”
PC-MHNominee
PC-MHNominee
PC-MHNominee

26
Wellness & Care Management Technology Architecture
Business Process Management (BPM) platform• process modeling & simulation• workflow automation
Clinical Programs Operational Data Store
BCBSM Business Intelligence Platform
Other BCBSM Systems (Membership, Claims, Provider Info, Customer Service, etc.)
Questionnaire Component• web• paperBCBSM
IntegrationFramework• internal• externalI
Wellness & Care Mgmt “Modules” (migrate to Portals)
Providers BCBSMStaff Members Customers
VendorPartners