bmj open · (vena saphena magna, vena saphena parva, and vena poplitea). the diagnosis is...
TRANSCRIPT
For peer review only
Structured wound management through a national quality
registry reduces healing time and antibiotic treatment
Journal: BMJ Open
Manuscript ID: bmjopen-2013-003091
Article Type: Research
Date Submitted by the Author: 22-Apr-2013
Complete List of Authors: Öien, Rut; Blekinge Wound Healing Center, Blekinge Centre of Competence Forssell, Henrik; Blekinge Centre of Competence,
<b>Primary Subject Heading</b>:
Medical management
Secondary Subject Heading: Diagnostics, General practice / Family practice, Medical management
Keywords: WOUND MANAGEMENT, GENERAL MEDICINE (see Internal Medicine), Quality in health care < HEALTH SERVICES ADMINISTRATION & MANAGEMENT
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on 27 January 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2013-003091 on 19 A
ugust 2013. Dow
nloaded from

For peer review only
1
Structured wound management through a national quality registry reduces
healing time and antibiotic treatment
Rut F Öien, 1,2 Henrik W Forssell 2
Rut F Öien, M.D., PhD, General Practitioner
Henrik W Forssell, M.D., PhD, Associate Professor
1 Blekinge Wound Healing Centre, Karlskrona, Sweden
2 Blekinge Centre of Competence, Karlskrona, Sweden
Correspondence to
Dr Rut F Öien
Blekinge Wound Healing Centre
Blekinge Centre of Competence,
S- 371 41 Karlskrona
Sweden
Page 1 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
2
ABSTRACT
Objectives: To investigate changes in ulcer healing time and antibiotic treatment in Sweden
following the introduction of a national quality registry in 2009.
Design: A statistical analysis of data from the Swedish Registry of Ulcer Treatment (RUT)
concerning healing time and antibiotic treatment for patients with hard-to-heal ulcers in
Sweden between 2009 and 2012.
Setting: RUT is a national web-based quality registry used to structure wound management
by registering patients with hard-to-heal leg, foot, and pressure ulcers. Registration includes
variables such as gender, age, diagnosis, healing time, antibiotic treatment, and ulcer duration
and size.
Population: Every patient with a hard-to-heal ulcer registered in RUT between 2009 and
2012 (n=1268).
Main outcome measures: The statistical analysis was performed using version 12.1 of the
Stata software package (StataCorp LP, College Station, Texas, USA). Healing time was
assessed with Kaplan-Meier analysis and adjustment was made for ulcer size. A log-rank test
was used for equality of survivor functions.
Results: Basic data from the adjusted registry in December 2012 (n=1268) showed a median
age of 80 years (mean age 77.5 years), ranging from 11 to 103 years. The median healing
time, adjusted for ulcer size, was 146 days (21 weeks) for all ulcers in 2009 and 63 days (9
weeks) for all ulcers in 2012 (p=0.001). Considering all years between 2009 and 2012,
antibiotic treatment for patients with hard-to-heal ulcers was reduced from 71% before
registration to 29% after registration to ulcer healing (p=0.001).
Conclusions: Healing time and antibiotic treatment both decreased significantly during the
three years after the introduction of RUT.
Results from RUT, a national quality registry
Key words: Hard-to-heal ulcers, ulcer assessment, diagnosis, ulcer care, ulcer healing,
antibiotic treatment, RUT (Registry of Ulcer Treatment)
Page 2 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
3
ARTICLE SUMMARY
Article focus
▪ The aim of the study was to statistically analyse the data from the Swedish Registry of Ulcer
Treatment (RUT) in order to detect any differences in healing time and antibiotic treatment
between 2009 and 2012.
Key messages
▪ Median healing time for all ulcers (adjusted for ulcer size) decreased significantly between
2009 and 2012.
▪ Median healing time for venous ulcers (adjusted for ulcer size) decreased significantly
between 2009 and 2012.
▪ The proportion of patients receiving antibiotic treatment before registration was significantly
higher than the proportion of patients receiving such treatment between registration and to
ulcer healing.
Strengths and limitations of this study
▪The data cover every patient registered in RUT during the years 2009 to 2012.
▪ RUT is used throughout Sweden and covers wound management in primary care,
community care, private care, and in-patient hospital care.
▪ RUT provides a reliable diagnosis, adequate strategies for ulcer care, and a structured
follow-up of ulcer healing.
▪ One limitation is that RUT is still in the process of being implemented, which means that in
some areas of Sweden every patient with a hard-to-heal ulcer is registered, while in other
areas only some patients are registered.
INTRODUCTION
Page 3 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
4
Wound management consumes time and money, and is a source of reduced quality of life for
the affected patients.1-3 A large proportion of patients with hard-to-heal ulcers are treated with
oral antibiotics (68–78%), 1,4-6 mostly because of problems with clinically assessing an ulcer
infection6,7 but also because of a lack of continuity of medical care.8
To address these difficulties, the Swedish Registry of Ulcer Treatment (RUT)9 was
introduced in May 2009. RUT (www.rikssar.se) is a national web-based quality register for
hard-to-heal ulcers developed to meet the demands of modern ulcer care in providing reliable
diagnosis, adequate strategies for ulcer care, and a structured follow-up of ulcer healing.
The aim of this study was to statistically analyse the data from RUT for the years 2009 and
2012 concerning healing time and antibiotic treatment for patients with hard-to-heal ulcers in
Sweden.
National registries
In recent decades, a system of national quality registries has been established in the Swedish
health and medical services, 10 covering different areas of medicine. There are currently 73
registries, which receive central funding from the Swedish Association of Local Authorities
and Regions (www.skl.se). Data from the registries are used for optimising medical care in
areas such as diabetes mellitus, dementia, and hard-to-heal ulcers.
Research in wound management Blekinge County is a Swedish county with 150,000
inhabitants and health care professionals with 25 years’ experience of quality improvement
and clinical research within the field of wound management.1,11 This tradition of research
resulted in the establishment of Blekinge Wound Healing Centre (BWHC) in 2003. BWHC is
a GP-led, primary care based specialist centre covering the treatment and follow-up of the
majority of ulcer patients in the whole county. It offers a structured team management of ulcer
care with emphasis on diagnosis, documentation, and treatment. The GP in charge of the
centre is the first author of this study (RFÖ).
The experience of our daily practice made it obvious that there is a need for a structured
programme for wound management; this was the reason behind the development of RUT, a
web-based quality registry for hard-to-heal ulcers. This approach has made RUT a useful tool
in daily clinical practice throughout Sweden since it became operational on 1st May 2009.
METHODOLOGY
Page 4 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
5
Study population and variables
Patients with a hard-to-heal leg, foot, or pressure ulcers are registered on two occasions. The
first registration, assessment of the ulcer diagnosis, is to guarantee optimal treatment. The
second registration is at follow-up; that is, at the point where the ulcer has healed or a
negative clinical event such as amputation or death has occurred. Every patient with a non-
healed ulcer remains in the registry until the ulcer is healed, no matter how long the healing
time.
At the first registration the following variables are recorded: social security number,
gender, age, date of diagnosis, profession or former profession, smoking habits, civil status,
number of children, mobility, exercise habits, and body mass index. The patient’s social
security number is linked and matched to the population statistics at the Council for Official
Statistics of Sweden.
Details are also taken regarding the nurse responsible for ulcer care; whether the ulcer is
recurrent, new, or traumatic; current or earlier concomitant diseases; current medication with
particular interest in analgesics and antibiotics; and ulcer-related pain. The patient history
focuses on the following variables: deep vein thrombosis (DVT), varicose veins, arterial or
venous surgery, history of recurrent leg ulcers, and ulcer localisation (foot, leg, or sacrum/hip;
and lateral or medial). Ulcer size is measured by digital planimeter (Visitrak®) and the
number of ulcers is noted.
The patient’s arterial circulation is assessed by palpating the arteria dorsalis pedis and
arteria tibialis posterior and measuring the ankle-brachial pressure index with a hand-held
Doppler. The Doppler is also used for measuring deep or superficial venous insufficiency
(vena saphena magna, vena saphena parva, and vena poplitea).
The diagnosis is determined from these variables together with the clinical examination.
The following ulcer diagnoses are used: venous ulcer, arterial ulcer, venous-arterial ulcer,
diabetic foot ulcer, pressure ulcer, traumatic ulcer, ulcer due to inflammatory vessel diseases
such as vasculitis, and other diagnosis (for example pyoderma gangrenosum). The strategy for
wound management includes dressings, care for the skin surrounding the ulcer, and treatment
for oedema. A photo gallery is linked to the registry for visualization of the healing process.
The second registration (at follow-up) includes date of healing, healing time, estimated
number of weekly dressing changes throughout healing, compression therapy, treatment with
antibiotics, pain relief, the most frequently used dressing material, and whether advice was
given on smoking cessation, exercise, and diet. Adverse events are also recorded at follow-up:
amputation, venous or arterial surgery, and death.
Page 5 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
6
Registration can be done at any time, and follow-up can be carried out when all the
mandatory variables are registered. Each unit has access only to data on its own patients; this
can be retrieved online at any time, and used to compare the unit’s quality of wound
management with that of the whole country.
Data analysis from RUT
The statistical analysis was performed using version 12.1 of the Stata software package
(StataCorp LP, College Station, Texas, USA). Continuous variables were expressed as mean
values (S.D.) and compared using two-sample Student’s t-tests. Group comparisons for
categorical variables were performed with Pearson’s chi square tests. Healing time was
assessed with Kaplan-Meier analysis and adjustment was made for ulcer size. A log-rank test
was used for equality of survivor functions. P < 0.05 was considered statistically significant.
RESULTS
Healing time
Basic data from the adjusted registry in December 2012 (n=1268) showed a median age of 80
years (mean age 77.5 years), ranging from 11 to 103 years.
The majority of the patients were women (60%). The median ulcer duration was 12 weeks
(mean 117 weeks), ranging from 1 to 2400 weeks, and the median ulcer size at inclusion in
RUT was 3 cm2 (mean 12 cm2), ranging from 0.05 cm2 to 600 cm2.
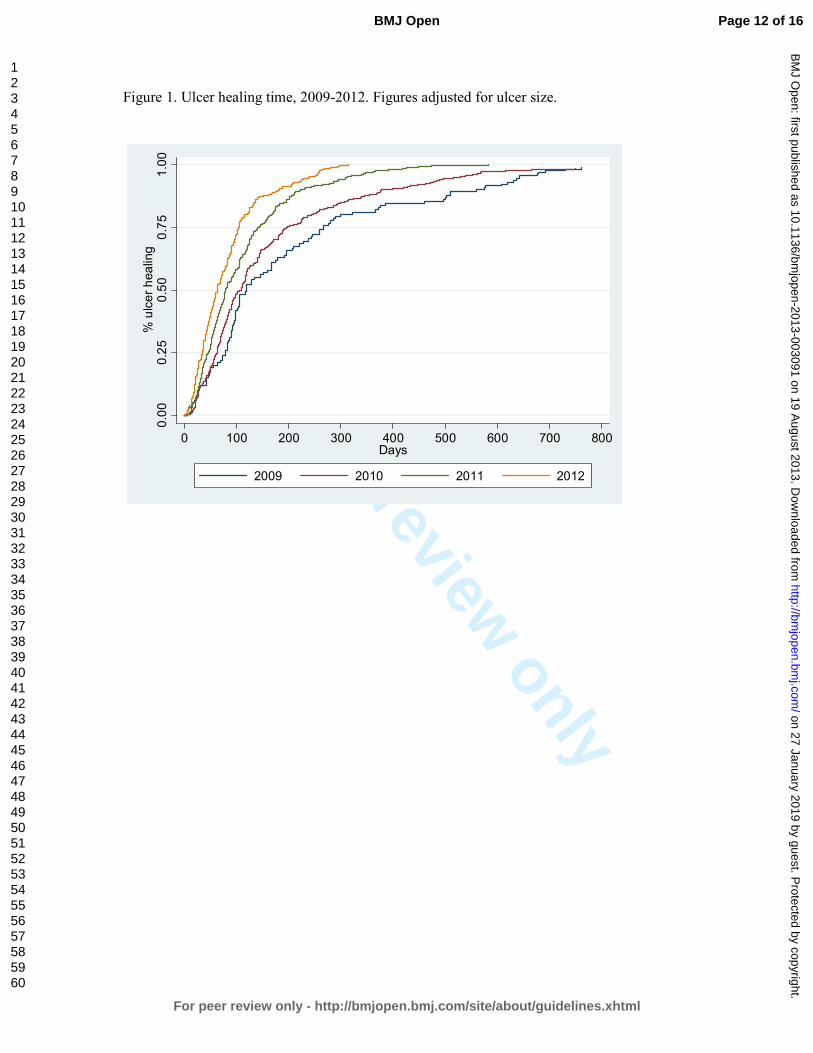
Figure 1 illustrates the median healing time, adjusted for ulcer size, from 2009 to 2012.
The median healing time was 146 days (21 weeks) for all ulcers in 2009 and 63 days (9
weeks) for all ulcers in 2012 (p=0.001).
Negative pressure wound therapy was introduced to the European market in 1997, and has
been used in Swedish primary health care since 2006. This technique was used in only 1.3%
of all cases during the study period.
Figure 2 illustrates the median healing time for venous ulcers, adjusted for ulcer size, from
2009 to 2012. The median healing time for these ulcers was 120 days (17 weeks) in 2009 and
69 days (10 weeks) in 2012 (p=0.001). Compression therapy was used in 87.3% of venous
ulcers in 2009 and 88.9% in 2012. In some areas of Sweden, every venous ulcer (100%) was
treated with compression therapy both in 2009 and 2012.
Antibiotic treatment
Page 6 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
7
Figure 3 illustrates antibiotic treatment from 2009 to 2012. In 2009, 76% of patients were
treated with antibiotics before registration, and 24% were treated after registration to ulcer
healing. In 2012, the corresponding figures were 73% before registration and 27% between
registration and healing. These differences were significant in both years (p=0.001).
Considering all years between 2009 and 2012, antibiotic treatment for patients with hard-to-
heal ulcers in the registry nationwide was reduced from 71% before registration to 29% after
registration to ulcer healing (p=0.001).
DISCUSSION
The principal finding in this study was the significantly reduced healing time for hard-to-heal
ulcers registered in RUT, the Swedish national quality registry; from 146 days (21 weeks) in
2009 to 63 days (9 weeks) in 2012. During this period, no new techniques and no innovative
new dressings were introduced for wound management on the Swedish market. Negative
pressure wound therapy was used in less than 2% of all cases, but has now become a more
widespread mode of treatment in clinical practice. There was some development of services,
such as the introduction of smaller wound healing centres based on the BWHC model.
Healing time is the one important endpoint in wound management.12 Earlier researchers
found a median healing time of 20-43 weeks when following patients through a period of 12
months.12 Some researchers noted a healing rate of 83% at 30 weeks,13 while others reported
that 62/90 (69%) of venous leg ulcers healed within 12 weeks.14 Moffatt et al.15 found that
70% of venous ulcers healed after 48 weeks of treatment; they also noted that much of the
evidence on healing rates is drawn from the results of randomized controlled trials. These
trials typically achieve 24-week healing rates in excess of 60%, but may not reflect the
complex issues faced in clinical practice.15
The significantly reduced healing time in our study seems to depend on the use of a
structured wound management, based on accurate diagnosis and thereby optimal treatment
and follow-up; all these factors are found in RUT.
Another important finding in the present study was the low rate (24-27%) of antibiotic
treatment administered to patients between registration and ulcer healing; that is, to patients
with a diagnosis and adequate treatment. This can be compared with earlier findings of 68–
78%1,5 for patients in primary care. Considering the years between 2009 and 2012, antibiotic
treatment for patients with hard-to-heal ulcers in the registry nationwide was reduced from
71% before registration to 29% between registration and ulcer healing (p=0.001).
Page 7 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
8
Antimicrobial therapy for local ulcer infection became more firmly established between
2009 and 2012, which could be one explanation for the reduced antibiotic treatment. This
issue is addressed in an ongoing research study within the frame of RUT.
A further explanation for the low rate of antibiotic treatment and reduced healing time
could be that RUT focuses on a stable doctor-patient relationship. Previous research has
shown the advantages of a structured organization in leg ulcer care.16,17 Petursson found that
lack of continuity of medical care was the main reason for general practitioners to prescribe
antibiotics in a “non-pharmacological” manner.8
The ulcer patient’s right to receive optimal treatment has been limited in recent decades,
due to lack of diagnosis and low continuity of ulcer care.1,18-20 Dressing changes over weeks,
months, and even years have been carried out, often without a proper diagnosis.1 It is well
known that understanding the aetiology of leg ulceration is a prerequisite for a systematic
clinical assessment as a base for appropriate wound management.13,14,21 RUT meets these
requirements.
Data must be collected in a uniform manner to capture the scale of the wound care, as
pointed out in previous studies.21 The conventional approach is to record details of all major
resources consumed (clinician time, dressings, antibiotics, analgesics, investigations, hospital
admissions, and surgical interventions) at each patient contact over the period from first
presentation to wound healing.21 RUT contains all these details.
The health care system requires information on the burden of care in order to inform
decisions on the needs of the population and the allocation of appropriate resources.15
RUT comprises a structured and practical methodology which can be used at any level in the
health care system.
The nationwide implementation of the RUT quality registry has not yet been fully achieved.
One area for future research is to investigate differences in the results of ulcer care between
areas in Sweden where RUT is used and areas where it is not used.
Another further research issue concerns the mapping of all pressure ulcers, such as ulcers
in younger patients with neurological diseases and in palliative care patients. RUT is an
appropriate basis for such a study, as it has a special section for pressure ulcers.
As of March 2013, the registry includes 1438 patients. The role of the registry manager
and the steering group is to show staff how data from the registry can be used to improve
ulcer care. We focus on documentation, treatment, education, research, and economic
analyses to guarantee improvement of health outcomes nationwide. Our ultimate aim is to
introduce RUT internationally.
Page 8 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
9
CONCLUSION
The findings from this study illustrate the immediate impact of RUT, concerning significantly
reduced healing time from 146 days (21 weeks) in 2009 to 63 days (9 weeks) in 2012.
Antibiotic treatment was reduced from 71% before registration to 29% between registration
and ulcer healing. They also demonstrate the potential for improved wound management,
when using a national quality registry for structured ulcer care.
Contributors
RFÖ led the research project and played the major role in the research design.
HWF contributed to the data analysis and assisted in the research design and interpretation of
the results.
Proper English provided language editing services.
Funding
This study was partly funded by the Council of Sciences in Blekinge County.
Competing interests None.
Ethics approval
The Lund Ethical Review Board has approved of this study concerning data from a quality
registry.
Provenance and peer review This study has not been externally peer reviewed.
Data sharing statement No additional data are available.
Acknowledgement This study was performed in the interests of the steering group for the
Swedish Registry of Ulcer Treatment (RUT).
REFERENCES
Page 9 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
10
1. Öien RF, Håkansson A, Ovhed I , Hansen BU . Wound management for 287 patients with
chronic leg ulcers demands 12 full-time nurses. Leg ulcer epidemiology and care in a well-
defined population in Southern Sweden . Scand J Prim Health Care 2000;18:220–5.
2. Lindholm C, Bjellerup M, Christensen OB, Zederfeldt B. Quality of life in chronic leg
ulcer patients: An assessment according to the Nottingham Health Profile . Acta Derm
Venereol 1993;73:440–3.
3. Anon. Evidence-based prescribing of advanced wound dressings for chronic wounds in
primary care. MeRec Bulletin 2010;1:1–7.
4. Wiström J, Lindholm C, Melhus A, et al . Infections and treatment in chronic leg ulcers:
The use of antibiotics is too excessive, restrictive prescription is recommended.
Lakartidningen.1999 ;6:96:42–6 [in Swedish].
5. André M, Eriksson M, Odenholt I. Treatment of patients with skin and soft tissue
infections: Results from the STRAMA survey of diagnoses and prescriptions among general
practitioners. Lakartidningen 2006;103:3165–7 [in Swedish].
6. Öien RF, Åkesson N. Bacterial cultures, rapid strep test, and antibiotic treatment in infected
hard-to-heal ulcers in primary care. Scand J Prim Health Care, 2012;30:254–258.
7. European Wound Management Association (EWMA) Position document: Management of
wound infection. London: MEP;2006.
8. Petursson P. G Ps’ reasons for “ non-pharmacological” prescribing of antibiotics: A
phenomenological study. Scand J Prim Health Care 2005;23:120-5.
9. Öien RF. R UT (Register of Ulcer Treatment) – a winning concept for both patients and the
health care sector. EWMA J 2009; 9:41–4.
10. Lundström M (ed.), Albrecht S, Serring I, Svensson K, Wendel E. Handbook for
establishing quality registries. EyeNet Sweden, Karlskrona, Sweden 2005.
ISBN 91-631- 8585-7.
11. Öien RF, Ragnarson Tennvall G. Accurate diagnosis and effective treatment of leg ulcer
reduce prevalence, care time and costs. J Wound Care 2006;15:259-62.
12. Morrell CJ, Walters SJ, Dixon S, et al. Cost effectiveness of community leg ulcer clinics:
randomised controlled trial. BMJ 1998 May 16;316(7143):1487-91.
13. Rybak Z, Franks PJ, Krasowski G, et al. Strategy for the treatment of chronic leg wounds:
a new model in Poland. Int Angiol 2012 Dec;31(6):550-6.
14. Hjerppe A, Saarinen JP, Venermo MA, et al. Prolonged healing of venous leg ulcers: the
role of venous reflux, ulcer characteristics and mobility. J Wound Care. 2010
Nov;19(11):474, 476, 478 passim.
Page 10 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
11
15. Moffatt CJ, Doherty DC, Smithdale R, Franks PJ. Clinical predictors of leg ulcer healing.
Br J Dermatol. 2010 Jan;162(1):51-8. doi: 10.1111/j.1365-2133.2009.09397.x. Epub 2009 Jul
7.
16. Moffatt CJ, Franks PJ, Oldroyd M, et al. Community clinics for leg ulcers and impact on
healing. BMJ 1992;305:1389–92.
17. Kjaer ML, Sorensen LT, Karlsmark T, et al. Evaluation of the quality of venous leg ulcer
care given in a multidisciplinary specialist centre. J Wound Care 2005 Apr;14(4):145-50
18. Törnvall E, Wilhelmsson S. Quality of nursing care from the perspective of patients with
leg ulcers. J Wound Care. 2010 Sep;19(9):388–95
19. Moffatt CJ, Doherty DC, Smithdale R, Franks PJ. Clinical predictors of leg ulcer healing.
Br J Dermatol. 2010 Jan;162(1):51-8. doi: 10.1111/j.1365-2133.2009.09397.x. Epub 2009 Jul
7.
20. Edwards H, Finlayson K, Courtney M et al. Health service pathways for patients with
chronic leg ulcers: identifying effective pathways for facilitation of evidence based wound
care. BMC Health Serv Res. 2013 Mar 8;13:86. doi: 10.1186/1472-6963-13-86.
21. Harding K, Posnett J, Vowden K. A new methodology for costing wound care.
Int Wound J. 2012 Dec 13. doi: 10.1111/iwj.12006.
Page 11 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
Figure 1. Ulcer healing time, 2009-2012. Figures adjusted for ulcer size.
0.00
0.25
0.50
0.75
1.00
% ulcer healing
0 100 200 300 400 500 600 700 800Days
2009 2010 2011 2012
Page 12 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
Figure 2.Venous ulcer healing time, 2009-2012. Figures adjusted for ulcer size.
0.00
0.25
0.50
0.75
1.00
% ulcer healing
0 100 200 300 400 500 600 700 800Days
2009 2010 2011 2012
Page 13 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
Figure 3. Antibiotic treatment before registration in RUT for the years 2009, 2010, 2011, and
2012, compared with antibiotic treatment between registration and ulcer healing for the same
years.
76
64
75 73
24
36
25 27
0
10
20
30
40
50
60
70
80
90
100
2009 2010 2011 2012
Before registration
After registration to ulcer healing
%
Page 14 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
STROBE Statement—Checklist of items that should be included in reports of cohort studies
Structured wound management through a national quality registry reduces healing time and
antibiotic treatment
Title and abstract
Introduction
Background/rationale
Objectives
Methods
Study design
Setting
Participants
Variables
Data sources/
measurement
Bias
Study size
Quantitative variables
Statistical methods
Results
Participants
Descriptive data
Outcome data
Main results
Other analyses
Discussion
Key results
Item
No
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
Recommendation
We have followed the recommendation
We have explained the scientific background in Introduction
We have stated the prespecified hypotheses
The key elements of study design are presented early in the
paper
The setting, locations, and relevant dates, including periods of
recruitment,
exposure, follow-up, and data collection are described
The eligibility criteria, and the sources and methods of selection
of participants. are described and methods of follow-up
All outcomes, exposures, predictors, potential confounders, and
effect modifiers are clearly defined.
Sources of data and details of methods of
assessment (measurement) for each variable of are given.
Since we have taken all patients in the registry, we considered it
not necessary to discuss sources of bias
We have described the results for every patient in the registry
during 2009 to 2012
No groupings were chosen
Statistics are thoroughly described for every moment
This section is written according to the check-list
Since we followed every patient to healing there are no missing
data for each variable of interest
The numbers of outcome events or summary measures over time
are reported
We have used the 95% confidence interval
We do not have any subgroups
key results with reference to study objectives have been
summarised
Page 15 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
Limitations
Interpretation
Generalisability
Other information
Funding
19
20
21
22
limitations of the study are discussed
An overall interpretation of results considering objectives,
limitations are being discussed. No similar studies have been
undertaken.
The generalisability (external validity) of the study results are
only mentioned,
This study was partly funded by the Council of Sciences in
Blekinge County.
Page 16 of 16
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
The Registry of Ulcer Treatment shows reduced healing time and antibiotic treatment – an improvement project in
the national quality registries in Sweden
Journal: BMJ Open
Manuscript ID: bmjopen-2013-003091.R1
Article Type: Research
Date Submitted by the Author: 14-Jun-2013
Complete List of Authors: Öien, Rut; Blekinge Wound Healing Center, Blekinge Centre of Competence Forssell, Henrik; Blekinge Centre of Competence,
<b>Primary Subject Heading</b>:
Medical management
Secondary Subject Heading: Diagnostics, General practice / Family practice, Medical management
Keywords: WOUND MANAGEMENT, GENERAL MEDICINE (see Internal Medicine), Quality in health care < HEALTH SERVICES ADMINISTRATION & MANAGEMENT
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on 27 January 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2013-003091 on 19 A
ugust 2013. Dow
nloaded from
For peer review only
The Registry of Ulcer Treatment shows reduced healing time and antibiotic
treatment – an improvement project in the national quality registries in
Sweden
Rut F Öien,1,2 Henrik W Forssell2
Rut F Öien, MD, PhD, General Practitioner, Registry Manager of RUT (Registry of Ulcer
Treatment)
Henrik W Forssell, MD, PhD, Associate Professor
1Blekinge Wound Healing Centre, Karlskrona, Sweden 2Blekinge Centre of Competence, Karlskrona, Sweden
Correspondence to:
Dr Rut F Öien
Blekinge Wound Healing Centre
Blekinge Centre of Competence
S-371 41 Karlskrona
Sweden
Phone: +46 706 687202
E-mail: [email protected]
Page 1 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
ABSTRACT
Objectives: To investigate changes in ulcer healing time and antibiotic treatment in Sweden
following the introduction of the Registry of Ulcer Treatment (RUT), a national quality
registry, in 2009.
Design: Statistical analysis was performed of RUT data concerning healing time and
antibiotic treatment for patients with hard-to-heal ulcers in Sweden between 2009 and 2012.
Setting: The RUT is a national web-based quality registry used to capture areas of
improvement in ulcer care and to structure wound management by registering patients with
hard-to-heal leg, foot and pressure ulcers. Registration includes variables such as gender, age,
diagnosis, healing time, antibiotic treatment and ulcer duration and size.
Population: Every patient with a hard-to-heal ulcer registered with the RUT between 2009
and 2012 (n=1,417) was included.
Main outcome measures: Statistical analyses were performed using Stata version 12.1.
Healing time was assessed with Kaplan-Meier analysis and adjustment was made for ulcer
size. A log-rank test was used for equality of survivor functions.
Results: According to the adjusted registry in December 2012, patients’ median age was 80
(mean 77.5, range 11–103) years. The median healing time for all ulcers, adjusted for ulcer
size, was 146 days (21 weeks) in 2009 and 63 days (9 weeks) in 2012 (p=0.001). Considering
all years between 2009 and 2012, antibiotic treatment for patients with hard-to-heal ulcers
was reduced from 71% before registration to 29% after registration to ulcer healing
(p=0.001).
Conclusions: Healing time and antibiotic treatment both decreased significantly during the 3
years after launch of the RUT.
Key words: hard-to-heal ulcers, ulcer assessment, diagnosis, ulcer care, ulcer healing,
antibiotics, RUT, pressure ulcer, topical antimicrobial treatment
Page 2 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
ARTICLE SUMMARY
Article focus
▪ The aim of this study was to analyse the data from the Swedish Registry of Ulcer Treatment
(RUT) to detect any differences in healing time and antibiotic treatment between 2009 and
2012.
Key messages
▪ Median healing time for all ulcers (adjusted for ulcer size) decreased significantly from 146
days in 2009 to 63 days in 2012.
▪ Median healing time for venous ulcers (adjusted for ulcer size) decreased significantly from
120 days in 2009 to 69 days in 2012.
▪ Antibiotic treatment for patients with hard-to-heal ulcers was reduced from 71% before
registration to 29% when using the RUT.
Strengths and limitations of this study
Strengths
▪ The data cover every patient registered with the RUT during 2009–2012.
▪ The RUT covers wound management in primary care, community care, private care and in-
patient hospital care throughout Sweden.
▪ The RUT provides a reliable diagnosis, adequate strategies for ulcer care, and a structured
follow-up of ulcer healing.
Limitations
▪ One limitation is that the RUT is still in the process of being implemented, which means that
in some areas of Sweden every patient with a hard-to-heal ulcer is registered, while
registration of patients in other areas is only partial.
Page 3 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
INTRODUCTION
Wound management not only consumes time and money, but ulcers and their treatment
reduce quality of life for affected patients.1–3
Patients with hard-to-heal ulcers have long been considered a neglected patient population.
Many are treated without diagnosis, and consequently receive suboptimal ulcer care. Overuse
of oral antibiotics in these patients (68–78%)1,4–6 is mostly due to absence of diagnosis or
inadequate clinical assessment of ulcer infections.6,7 The lack of continuity in ulcer care and
also the lack of team-working between health professionals in this field has further
contributed to antibiotic overuse.8 In Sweden, lack of national guidelines for medical ulcer
care has had a negative impact on wound management.
Structured wound management based on accurate diagnosis leads to effective treatment
and, consequently, decreased prevalence, care time and costs.9 For this reason, the Swedish
Registry of Ulcer Treatment (RUT)10 was started in May 2009. Its purpose is to assess
physician diagnoses of ulcers, give medical staff a structured check list for optimal treatment
and identify areas of improvement in wound management.
The focus of this study was to investigate whether ulcer healing time and antibiotic
treatment have been affected by the registry. We aimed to analyse data from the RUT from
the time the registry was introduced nationally (2009) to 2012.
National registries
In recent decades, a system of national quality registries has been established in the Swedish
health and medical services,11 covering different areas of medicine. There are currently 73
registries which receive central funding (www.skl.se).
The ambition of the Swedish national quality registries is to gather data on diagnoses and
symptoms, interventions and treatment outcomes in order to give a continuous, systematic
evaluation of medical practice.
The majority of the Swedish national quality registries have been developed by physicians
with special interest in a research field in order to bring about quality improvement to health
care for a specific medical problem.
Page 4 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
The Registry of Ulcer Treatment - RUT
Health care professionals in Blekinge have for the past 25 years focused on quality
improvement and clinical research within the field of wound management.1,9 This tradition of
research linked to clinical practice led to the establishment of the Blekinge Wound Healing
Centre (BWHC) in 2003. The BWHC is a general practitioner (GP)-led, primary care-based
specialist centre covering the treatment and follow-up of the majority of ulcer patients across
the county (150, 000 inhabitants). It offers a structured team management of ulcer care with
emphasis on diagnosis, documentation and treatment. The GP in charge of the centre is the
first author of this study (R.F.Ö.).
The experience of our daily practice combined with research results soon made it obvious
that there was a need for a structured programme for wound management to guarantee
optimal treatment. The RUT was started in Blekinge County by Rut F Öien, the registry
manager, who has developed and launched the registry.
The RUT was the first national registry in primary care. It is web-based and the
participating units use the registry as a check list for ulcer assessment and a base for quality
improvement in their units.
That data must be collected in a uniform manner to capture the scale of wound care has
been previously pointed out.12 The conventional approach is to record details of ulcer care
such as treatment strategies, dressings, antibiotics, analgesics, investigations, hospital
admissions and surgical interventions at each patient contact over the period from first
presentation to wound healing.12 These details are noted in the patient’s medical record for
decision support for the individual patient.
Registration in the RUT is usually done at the first patient contact, and follow-up can be
carried out when all the mandatory variables are registered. Each unit has access only to data
on its own patients; these can be retrieved online at any time, and used to compare the unit’s
quality of wound management with that across the country. By using accumulated data for the
whole country, areas of improvement can be highlighted.
To capture the situation of patients with pressure ulcers, the registry has during the study
period further developed the special pressure ulcer section. To cover community units where
these patients are mostly treated, we have established cooperation with another Swedish
national quality registry on pressure ulcer prevention. This could in the future give a more
accurate picture of pressure ulcer prevention linked to either pressure ulcer healing or
negative clinical events, such as death.
Page 5 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
Registering with the RUT has been mandatory in Blekinge County since 2012 and today
some of the larger national dermatological departments are likewise obliged to register with
the RUT.
METHODOLOGY
Study population and variables
During the study period we had frequent meetings with the participating units, at which nurses
and physicians evaluated the RUT. Having had access to the structure of the registry, they
commented on how the registry had made a difference in their approach to wound
management. Their new focus was on adequate diagnosis, continuity of care by nominating a
responsible ulcer nurse for every patient and follow-up to ulcer healing. The shorter time to
healing recorded was an acknowledgment of their effort to introduce improved wound
management.
Another area of improvement was the reduction in antibiotic treatment. Since the variable
antibiotic treatment before and after registration is mandatory, the participants’ attention was
drawn to antibiotic use and participants acknowledged the reduction in oral antibiotic
treatment for their patients as a success for their unit and an improvement of the patients’
quality of life.
During the study period 160 patients were registered in 2009, 348 patients in 2010, 400 in
2011 and 509 in 2012, making a total of 1,417 patients nationwide by 2012.
The RUT registers patients with hard-to-heal leg, foot or pressure ulcers on two occasions.
The first registration, assessment of the ulcer diagnosis, is to guarantee optimal treatment. The
second registration is at follow-up; that is, at the point where the ulcer has healed or a
negative clinical event such as amputation or death has occurred. Every patient with a non-
healed ulcer remains in the registry until follow-up is completed.
At the first registration the following variables are recorded: social security number,
gender, age, date of diagnosis, profession or former profession, smoking habits, civil status,
number of children, mobility, exercise habits, and body mass index. The patient’s social
security number is linked and matched to the population statistics at the Council for Official
Statistics of Sweden.
To guarantee continuity of care there is a mandatory variable containing the name of the
nurse responsible for ulcer care, facilitating follow-up of every patient to complete ulcer
healing. This nurse is often the person responsible for registering the patient with the RUT.
Page 6 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
Other details taken include whether the ulcer is new or recurrent; current or earlier
concomitant diseases; current medication, especially asking for analgesics and antibiotics; and
ulcer-related pain. The patient history focuses on the following variables: deep vein
thrombosis (DVT), varicose veins, arterial or venous surgery, history of recurrent leg ulcers,
and ulcer localization (foot, leg or sacrum/hip; and lateral or medial). Ulcer size is measured
by digital planimeter (Visitrak®, manufactured in the United Kingdom for
Smith & Nephew Medical Limited, Hull HU3 2BN) and the number of ulcers is noted.
The patient’s arterial circulation is assessed by palpating the arteria dorsalis pedis and
arteria tibialis posterior and measuring the ankle-brachial pressure index with a hand-held
Doppler, (manufactured by Histolab,Gothenburg, Sweden). The Doppler is also used for
measuring deep or superficial venous insufficiency (vena saphena magna, vena saphena
parva and vena poplitea).
The diagnosis is determined from these variables, in combination with the clinical
examination. The following ulcer diagnoses are used: venous ulcer, arterial ulcer, venous-
arterial ulcer, diabetic foot ulcer, pressure ulcer, traumatic ulcer, ulcer due to inflammatory
vessel diseases such as vasculitis, and other diagnoses (for example pyoderma gangrenosum).
The strategy for wound management includes dressings, care for the skin surrounding the
ulcer, and treatment for oedema. A photo gallery is linked to the registry for visualization of
the healing process.
The second registration (at follow-up) includes date of healing, healing time, estimated
number of weekly dressing changes throughout healing, compression therapy, treatment with
antibiotics, pain relief, the most frequently used dressing material, and whether advice was
given on smoking cessation, exercise and diet. Adverse events are also recorded: e.g.
amputation, venous or arterial surgery, and death.
Data analysis
The statistical analysis was performed using Stata version 12.1 (StataCorp LP, College
Station, TX, USA). Continuous variables were expressed as mean values (± standard
deviation (SD)) and compared using two-sample Student’s t-tests. Group comparisons for
categorical variables were performed using Pearson’s chi-square tests. Healing time was
assessed with Kaplan-Meier analysis and adjustment was made for ulcer size. A log-rank test
was used for equality of survivor functions. P<0.05 was considered statistically significant.
Page 7 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
Ethical approval
The Lund Ethical Review Board considered the study to be a valuable quality improvement
study, so no further ethical approval was required.
RESULTS
Healing time
Basic data from the adjusted registry in December 2012 showed a population (n=1,417) with
a median age of 80 years (mean age 77.5 years), ranging from 11 to 103 years.
The majority of the patients were women (60%). The median ulcer duration was 12 weeks
(mean 117 weeks), ranging from 1 week to 46 years, and the median ulcer size at inclusion in
the RUT was 3 cm2 (mean 12 cm2, range 0.05–600 cm2).
The participating units covered primary care (50%), community care (4%), hospital care
(22%), wound healing centres (22%) and private caregivers (2%). Patients from Blekinge
County constituted 39% of all patients.
Figure 1 illustrates the median healing time, adjusted for ulcer size, from 2009 to 2012.
The median healing time was 146 days (21 weeks) for all ulcers in 2009 and 63 days (9
weeks) for all ulcers in 2012 (p=0.001).
Negative pressure wound therapy was introduced in Europe in 1997, and has been used in
Swedish primary health care since 2006. During the study period, this technique was used in
only 1.3% of cases.
Figure 2 gives the median healing time for venous ulcers, adjusted for ulcer size, from
2009 to 2012. The median healing time for these ulcers was 120 days (17 weeks) in 2009 and
69 days (10 weeks) in 2012 (p=0.001). Compression therapy was used in 87.3% of venous
ulcers in 2009 and 88.9% in 2012. In some areas of Sweden, every venous ulcer (100%) was
treated with compression therapy both in 2009 and in 2012.
Antibiotic treatment
Figure 3 illustrates antibiotic treatment from 2009 to 2012. In 2009, 76% of patients were
treated with antibiotics before registration, compared with 24% after registration. In 2012, the
corresponding figures were 73% before and 27% after registration. These differences were
significant in both years (p=0.001).
Considering all years between 2009 and 2012, antibiotic treatment for patients with hard-
to-heal ulcers in the registry nationwide was reduced from 71% before registration to 29%
after registration (p=0.001).
Page 8 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
DISCUSSION
The principal finding in this study was the significantly reduced healing time for hard-to-heal
ulcers registered with the RUT, from 146 days (21 weeks) in 2009 to 63 days (9 weeks) in
2012. This reduction in healing time seems to be due to structured wound management, based
on accurate diagnosis, continuity of care by nominating a responsible ulcer nurse for every
patient and follow-up to healing, all of which factors were facilitated by the RUT.
Although topical antimicrobial therapy for local ulcer infection, such as iodine, silver,
honey and polyhexamethylene biguanide (PHMB), has become more firmly established, no
further innovative dressings or devices were introduced for wound management on the
Swedish market during the study period. Negative pressure wound therapy was used in less
than 1.5% of all cases during the study, but is now more widespread in clinical practice. There
was some development of services, such as the introduction of smaller wound healing centres
based on the BWHC model.
Healing time is the one important endpoint in wound management.13 Earlier researchers
found a median healing time of 20–43 weeks when following patients through a period of 12
months.13 Some researchers have noted a healing rate of 83% at 30 weeks,14 while others have
reported that 62/90 (69%) of venous leg ulcers healed within 12 weeks.15 Moffatt et al.16
found that 70% of venous ulcers healed after 48 weeks of treatment; they also noted that
much of the evidence on healing rates is drawn from the results of randomized controlled
trials. These trials typically achieve 24-week healing rates in excess of 60%, but may not
reflect the complex issues faced in clinical practice.16
Another important finding in the present study was the low proportion of patients (24-
27%) given antibiotics between registration and ulcer healing; that is, in patients with a
diagnosis and adequate treatment. This can be compared with earlier findings of 68–78%1,5
for patients in primary care. Between 2009 and 2012, antibiotic treatment for patients with
hard-to-heal ulcers in the registry nationwide was reduced from 71% before registration to
29% between registration and ulcer healing (p=0.001).
There is still a high rate of oral antibiotic treatment for patients outside the registry,
which may be explained by the fact that these patients do not receive continuity of care or
treatment by a specialized team, where topical antimicrobial treatment is the golden standard
when treating local ulcer infection.
The use of topical antimicrobial dressings could be one explanation for the reduction in
antibiotic treatment. This issue is being addressed in an on going research study within the
frame of the RUT.
Page 9 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
A further explanation for the recent low rate of antibiotic treatment and reduced healing
time could be that the RUT focuses on stable doctor-patient relationships. Previous research
has shown the advantages of a structured organization for leg ulcer care.17,18 Petursson argues
that lack of continuity in medical care is the main reason why GPs prescribe antibiotics in a
“non-pharmacological” manner.8
The ulcer patient’s right to receive optimal treatment has been limited in recent decades,
owing to lack of diagnosis and low continuity in ulcer care.1,19–21 Dressing changes over
weeks, months and even years have been carried out, often without a proper diagnosis.1 It is
well known that understanding the aetiology of leg ulceration is a prerequisite for a systematic
clinical assessment as a base for appropriate wound management.12,14,15 The RUT meets these
requirements.
A large proportion of the patient population (39%) in the registry was concentrated in
Blekinge County. This could be considered a bias as the registry was developed in Blekinge
County, from where it has spread to the whole country. That the majority of patients were
treated in primary care reflects the true situation in Sweden.
The health care system requires information on the burden of care in order to inform
decisions on the needs of the population and the allocation of resources.16 The RUT comprises
a structured and practical methodology which can be used at any level in the health care
system.
Nationwide implementation of the RUT has not yet been fully achieved. One area for
future research is to investigate differences in the results of ulcer care between areas in
Sweden where the RUT is being used and areas where it is not used.
Another further research issue concerns the mapping of all pressure ulcers, such as ulcers
in younger patients with neurological diseases and in palliative care patients. The RUT is an
appropriate basis for such a study, as it has a special section for pressure ulcers.
Since March 2013, the registry has included 1,438 patients. The role of the registry
manager and the steering group is to show staff how data from the registry can be used to
improve ulcer care. We focus on documentation, treatment, education, research, and
economic analyses to guarantee improvement of health outcomes nationwide. Our ultimate
aim is twofold: to serve as basis for national guidelines and for the registry to be implemented
internationally.
Page 10 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
CONCLUSION
The findings from this study illustrate the immediate impact of the RUT as an improvement
project within wound management, resulting in significantly reduced healing time from 146
days (21 weeks) in 2009 to 63 days (9 weeks) in 2012. Antibiotic treatment was reduced from
71% before registration to 29% between registration and ulcer healing. The results also
demonstrate the potential for improved wound management when using a national quality
registry for structured ulcer care.
Contributors
R.F.Ö. led the research project and played the main role in the research design.
H.W.F. contributed to the data analysis and assisted in the research design and interpretation
of results.
Funding
This study was partly funded by the Council of Sciences in Blekinge County, Sweden.
Competing interests
None.
Ethics approval
The Lund Ethical Review Board considered the study to be a valuable quality improvement
study, so no further ethical approval was required
Provenance and peer review
This study has not been externally peer-reviewed.
Data-sharing statement
No additional data are available.
Acknowledgement
This study was performed in the interests of the steering group for the Swedish Registry of
Ulcer Treatment (RUT).
REFERENCES
1. Öien RF, Håkansson A, Ovhed I , Hansen BU. Wound management for 287 patients with
chronic leg ulcers demands 12 full-time nurses. Leg ulcer epidemiology and care in a well-
defined population in Southern Sweden . Scand J Prim Health Care 2000;18:220–5.
Page 11 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
2. Lindholm C, Bjellerup M, Christensen OB, Zederfeldt B. Quality of life in chronic leg
ulcer patients: An assessment according to the Nottingham Health Profile . Acta Derm
Venereol 1993;73:440–3.
3. Anon. Evidence-based prescribing of advanced wound dressings for chronic wounds in
primary care. MeRec Bulletin 2010;1:1–7.
4. Wiström J, Lindholm C, Melhus A, et al. Infections and treatment in chronic leg ulcers:
The use of antibiotics is too excessive, restrictive prescription is recommended.
Lakartidningen.1999 ;6:96:42–6 [in Swedish].
5. André M, Eriksson M, Odenholt I. Treatment of patients with skin and soft tissue
infections: Results from the STRAMA survey of diagnoses and prescriptions among general
practitioners. Lakartidningen 2006;103:3165–7 [in Swedish].
6. Öien RF, Åkesson N. Bacterial cultures, rapid strep test, and antibiotic treatment in infected
hard-to-heal ulcers in primary care. Scand J Prim Health Care, 2012;30:254–258.
7. European Wound Management Association (EWMA) Position document: Management of
wound infection. London: MEP;2006.
8. Petursson P. G Ps’ reasons for “non-pharmacological” prescribing of antibiotics: A
phenomenological study. Scand J Prim Health Care 2005;23:120-5.
9. Öien RF, Ragnarson Tennvall G. Accurate diagnosis and effective treatment of leg ulcer
reduce prevalence, care time and costs. J Wound Care 2006;15:259-62.
10. Öien RF. R UT (Register of Ulcer Treatment) – a winning concept for both patients and
the health care sector. EWMA J 2009; 9:41–4.
11. Lundström M (ed.), Albrecht S, Serring I, Svensson K, Wendel E. Handbook for
establishing quality registries. EyeNet Sweden, Karlskrona, Sweden 2005.
ISBN 91-631- 8585-7.
12. Harding K, Posnett J, Vowden K. A new methodology for costing wound care.
Int Wound J. 2012 Dec 13. doi: 10.1111/iwj.12006
13. Morrell CJ, Walters SJ, Dixon S, et al. Cost effectiveness of community leg ulcer clinics:
randomised controlled trial. BMJ 1998 May 16;316(7143):1487-91.
14. Rybak Z, Franks PJ, Krasowski G, et al. Strategy for the treatment of chronic leg wounds:
a new model in Poland. Int Angiol 2012 Dec;31(6):550-6.
15. Hjerppe A, Saarinen JP, Venermo MA, et al. Prolonged healing of venous leg ulcers: the
role of venous reflux, ulcer characteristics and mobility. J Wound Care. 2010
Nov;19(11):474, 476, 478 passim.
16. Moffatt CJ, Doherty DC, Smithdale R, Franks PJ. Clinical predictors of leg ulcer healing.
Page 12 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
Br J Dermatol. 2010 Jan;162(1):51-8. doi: 10.1111/j.1365-2133.2009.09397.x. Epub 2009 Jul
7.
17. Moffatt CJ, Franks PJ, Oldroyd M, et al. Community clinics for leg ulcers and impact on
healing. BMJ 1992;305:1389–92.
18. Kjaer ML, Sorensen LT, Karlsmark T, et al. Evaluation of the quality of venous leg ulcer
care given in a multidisciplinary specialist centre. J Wound Care 2005 Apr;14(4):145-50
19. Törnvall E, Wilhelmsson S. Quality of nursing care from the perspective of patients with
leg ulcers. J Wound Care. 2010 Sep;19(9):388–95
20. Moffatt CJ, Doherty DC, Smithdale R, Franks PJ. Clinical predictors of leg ulcer healing.
Br J Dermatol. 2010 Jan;162(1):51-8. doi: 10.1111/j.1365-2133.2009.09397.x. Epub 2009 Jul
7.
21. Edwards H, Finlayson K, Courtney M et al. Health service pathways for patients with
chronic leg ulcers: identifying effective pathways for facilitation of evidence based wound
care. BMC Health Serv Res. 2013 Mar 8;13:86. doi: 10.1186/1472-6963-13-86.
Page 13 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
The Registry of Ulcer Treatment shows reduced healing time and antibiotic
treatment – an improvement project in the national quality registries in
Sweden
Rut F Öien,1,2 Henrik W Forssell2
Rut F Öien, MD, PhD, General Practitioner, Registry Manager of RUT (Registry of Ulcer
Treatment)
Henrik W Forssell, MD, PhD, Associate Professor
1Blekinge Wound Healing Centre, Karlskrona, Sweden 2Blekinge Centre of Competence, Karlskrona, Sweden
Correspondence to:
Dr Rut F Öien
Blekinge Wound Healing Centre
Blekinge Centre of Competence
S-371 41 Karlskrona
Sweden
Phone: +46 706 687202
E-mail: [email protected]
Page 14 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
ABSTRACT
Objectives: To investigate changes in ulcer healing time and antibiotic treatment in Sweden
following the introduction of the Registry of Ulcer Treatment (RUT), a national quality
registry, in 2009.
Design: Statistical analysis was performed of RUT data concerning healing time and
antibiotic treatment for patients with hard-to-heal ulcers in Sweden between 2009 and 2012.
Setting: The RUT is a national web-based quality registry used to capture areas of
improvement in ulcer care and to structure wound management by registering patients with
hard-to-heal leg, foot and pressure ulcers. Registration includes variables such as gender, age,
diagnosis, healing time, antibiotic treatment and ulcer duration and size.
Population: Every patient with a hard-to-heal ulcer registered with the RUT between 2009
and 2012 (n=1,417) was included.
Main outcome measures: Statistical analyses were performed using Stata version 12.1.
Healing time was assessed with Kaplan-Meier analysis and adjustment was made for ulcer
size. A log-rank test was used for equality of survivor functions.
Results: According to the adjusted registry in December 2012, patients’ median age was 80
(mean 77.5, range 11–103) years. The median healing time for all ulcers, adjusted for ulcer
size, was 146 days (21 weeks) in 2009 and 63 days (9 weeks) in 2012 (p=0.001). Considering
all years between 2009 and 2012, antibiotic treatment for patients with hard-to-heal ulcers
was reduced from 71% before registration to 29% after registration to ulcer healing
(p=0.001).
Conclusions: Healing time and antibiotic treatment both decreased significantly during the 3
years after launch of the RUT.
Key words: hard-to-heal ulcers, ulcer assessment, diagnosis, ulcer care, ulcer healing,
antibiotics, RUT, pressure ulcer, topical antimicrobial treatment
Page 15 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
ARTICLE SUMMARY
Article focus
▪ The aim of this study was to analyse the data from the Swedish Registry of Ulcer Treatment
(RUT) to detect any differences in healing time and antibiotic treatment between 2009 and
2012.
Key messages
▪ Median healing time for all ulcers (adjusted for ulcer size) decreased significantly from 146
days in 2009 to 63 days in 2012.
▪ Median healing time for venous ulcers (adjusted for ulcer size) decreased significantly from
120 days in 2009 to 69 days in 2012.
▪ Antibiotic treatment for patients with hard-to-heal ulcers was reduced from 71% before
registration to 29% when using the RUT.
Strengths and limitations of this study
Strengths
▪ The data cover every patient registered with the RUT during 2009–2012.
▪ The RUT covers wound management in primary care, community care, private care and in-
patient hospital care throughout Sweden.
▪ The RUT provides a reliable diagnosis, adequate strategies for ulcer care, and a structured
follow-up of ulcer healing.
Limitations
▪ One limitation is that the RUT is still in the process of being implemented, which means that
in some areas of Sweden every patient with a hard-to-heal ulcer is registered, while
registration of patients in other areas is only partial.
Page 16 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
INTRODUCTION
Wound management not only consumes time and money, but ulcers and their treatment
reduce quality of life for affected patients.1–3
Patients with hard-to-heal ulcers have long been considered a neglected patient population.
Many are treated without diagnosis, and consequently receive suboptimal ulcer care. Overuse
of oral antibiotics in these patients (68–78%)1,4–6 is mostly due to absence of diagnosis or
inadequate clinical assessment of ulcer infections.6,7 The lack of continuity in ulcer care and
also the lack of team-working between health professionals in this field has further
contributed to antibiotic overuse.8 In Sweden, lack of national guidelines for medical ulcer
care has had a negative impact on wound management.
Structured wound management based on accurate diagnosis leads to effective treatment
and, consequently, decreased prevalence, care time and costs.9 For this reason, the Swedish
Registry of Ulcer Treatment (RUT)10 was started in May 2009. Its purpose is to assess
physician diagnoses of ulcers, give medical staff a structured check list for optimal treatment
and identify areas of improvement in wound management.
The focus of this study was to investigate whether ulcer healing time and antibiotic
treatment have been affected by the registry. We aimed to analyse data from the RUT from
the time the registry was introduced nationally (2009) to 2012.
National registries
In recent decades, a system of national quality registries has been established in the Swedish
health and medical services,11 covering different areas of medicine. There are currently 73
registries which receive central funding (www.skl.se).
The ambition of the Swedish national quality registries is to gather data on diagnoses and
symptoms, interventions and treatment outcomes in order to give a continuous, systematic
evaluation of medical practice.
The majority of the Swedish national quality registries have been developed by physicians
with special interest in a research field in order to bring about quality improvement to health
care for a specific medical problem.
Page 17 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
The Registry of Ulcer Treatment - RUT
Health care professionals in Blekinge have for the past 25 years focused on quality
improvement and clinical research within the field of wound management.1,9 This tradition of
research linked to clinical practice led to the establishment of the Blekinge Wound Healing
Centre (BWHC) in 2003. The BWHC is a general practitioner (GP)-led, primary care-based
specialist centre covering the treatment and follow-up of the majority of ulcer patients across
the county (150, 000 inhabitants). It offers a structured team management of ulcer care with
emphasis on diagnosis, documentation and treatment. The GP in charge of the centre is the
first author of this study (R.F.Ö.).
The experience of our daily practice combined with research results soon made it obvious
that there was a need for a structured programme for wound management to guarantee
optimal treatment. The RUT was started in Blekinge County by Rut F Öien, the registry
manager, who has developed and launched the registry.
The RUT was the first national registry in primary care. It is web-based and the
participating units use the registry as a check list for ulcer assessment and a base for quality
improvement in their units.
That data must be collected in a uniform manner to capture the scale of wound care has
been previously pointed out.12 The conventional approach is to record details of ulcer care
such as treatment strategies, dressings, antibiotics, analgesics, investigations, hospital
admissions and surgical interventions at each patient contact over the period from first
presentation to wound healing.12 These details are noted in the patient’s medical record for
decision support for the individual patient.
Registration in the RUT is usually done at the first patient contact, and follow-up can be
carried out when all the mandatory variables are registered. Each unit has access only to data
on its own patients; these can be retrieved online at any time, and used to compare the unit’s
quality of wound management with that across the country. By using accumulated data for the
whole country, areas of improvement can be highlighted.
To capture the situation of patients with pressure ulcers, the registry has during the study
period further developed the special pressure ulcer section. To cover community units where
these patients are mostly treated, we have established cooperation with another Swedish
national quality registry on pressure ulcer prevention. This could in the future give a more
accurate picture of pressure ulcer prevention linked to either pressure ulcer healing or
negative clinical events, such as death.
Page 18 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
Registering with the RUT has been mandatory in Blekinge County since 2012 and today
some of the larger national dermatological departments are likewise obliged to register with
the RUT.
METHODOLOGY
Study population and variables
During the study period we had frequent meetings with the participating units, at which nurses
and physicians evaluated the RUT. Having had access to the structure of the registry, they
commented on how the registry had made a difference in their approach to wound
management. Their new focus was on adequate diagnosis, continuity of care by nominating a
responsible ulcer nurse for every patient and follow-up to ulcer healing. The shorter time to
healing recorded was an acknowledgment of their effort to introduce improved wound
management.
Another area of improvement was the reduction in antibiotic treatment. Since the variable
antibiotic treatment before and after registration is mandatory, the participants’ attention was
drawn to antibiotic use and participants acknowledged the reduction in oral antibiotic
treatment for their patients as a success for their unit and an improvement of the patients’
quality of life.
During the study period 160 patients were registered in 2009, 348 patients in 2010, 400 in
2011 and 509 in 2012, making a total of 1,417 patients nationwide by 2012.
The RUT registers patients with hard-to-heal leg, foot or pressure ulcers on two occasions.
The first registration, assessment of the ulcer diagnosis, is to guarantee optimal treatment. The
second registration is at follow-up; that is, at the point where the ulcer has healed or a
negative clinical event such as amputation or death has occurred. Every patient with a non-
healed ulcer remains in the registry until follow-up is completed.
At the first registration the following variables are recorded: social security number,
gender, age, date of diagnosis, profession or former profession, smoking habits, civil status,
number of children, mobility, exercise habits, and body mass index. The patient’s social
security number is linked and matched to the population statistics at the Council for Official
Statistics of Sweden.
To guarantee continuity of care there is a mandatory variable containing the name of the
nurse responsible for ulcer care, facilitating follow-up of every patient to complete ulcer
healing. This nurse is often the person responsible for registering the patient with the RUT.
Page 19 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
Other details taken include whether the ulcer is new or recurrent; current or earlier
concomitant diseases; current medication, especially asking for analgesics and antibiotics; and
ulcer-related pain. The patient history focuses on the following variables: deep vein
thrombosis (DVT), varicose veins, arterial or venous surgery, history of recurrent leg ulcers,
and ulcer localization (foot, leg or sacrum/hip; and lateral or medial). Ulcer size is measured
by digital planimeter (Visitrak®, manufactured in the United Kingdom for
Smith & Nephew Medical Limited, Hull HU3 2BN) and the number of ulcers is noted.
The patient’s arterial circulation is assessed by palpating the arteria dorsalis pedis and
arteria tibialis posterior and measuring the ankle-brachial pressure index with a hand-held
Doppler, (manufactured by Histolab,Gothenburg, Sweden). The Doppler is also used for
measuring deep or superficial venous insufficiency (vena saphena magna, vena saphena
parva and vena poplitea).
The diagnosis is determined from these variables, in combination with the clinical
examination. The following ulcer diagnoses are used: venous ulcer, arterial ulcer, venous-
arterial ulcer, diabetic foot ulcer, pressure ulcer, traumatic ulcer, ulcer due to inflammatory
vessel diseases such as vasculitis, and other diagnoses (for example pyoderma gangrenosum).
The strategy for wound management includes dressings, care for the skin surrounding the
ulcer, and treatment for oedema. A photo gallery is linked to the registry for visualization of
the healing process.
The second registration (at follow-up) includes date of healing, healing time, estimated
number of weekly dressing changes throughout healing, compression therapy, treatment with
antibiotics, pain relief, the most frequently used dressing material, and whether advice was
given on smoking cessation, exercise and diet. Adverse events are also recorded: e.g.
amputation, venous or arterial surgery, and death.
Data analysis
The statistical analysis was performed using Stata version 12.1 (StataCorp LP, College
Station, TX, USA). Continuous variables were expressed as mean values (± standard
deviation (SD)) and compared using two-sample Student’s t-tests. Group comparisons for
categorical variables were performed using Pearson’s chi-square tests. Healing time was
assessed with Kaplan-Meier analysis and adjustment was made for ulcer size. A log-rank test
was used for equality of survivor functions. P<0.05 was considered statistically significant.
Page 20 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
Ethical approval
The Lund Ethical Review Board considered the study to be a valuable quality improvement
study, so no further ethical approval was required.
RESULTS
Healing time
Basic data from the adjusted registry in December 2012 showed a population (n=1,417) with
a median age of 80 years (mean age 77.5 years), ranging from 11 to 103 years.
The majority of the patients were women (60%). The median ulcer duration was 12 weeks
(mean 117 weeks), ranging from 1 week to 46 years, and the median ulcer size at inclusion in
the RUT was 3 cm2 (mean 12 cm2, range 0.05–600 cm2).
The participating units covered primary care (50%), community care (4%), hospital care
(22%), wound healing centres (22%) and private caregivers (2%). Patients from Blekinge
County constituted 39% of all patients.
Figure 1 illustrates the median healing time, adjusted for ulcer size, from 2009 to 2012.
The median healing time was 146 days (21 weeks) for all ulcers in 2009 and 63 days (9
weeks) for all ulcers in 2012 (p=0.001).
Negative pressure wound therapy was introduced in Europe in 1997, and has been used in
Swedish primary health care since 2006. During the study period, this technique was used in
only 1.3% of cases.
Figure 2 gives the median healing time for venous ulcers, adjusted for ulcer size, from
2009 to 2012. The median healing time for these ulcers was 120 days (17 weeks) in 2009 and
69 days (10 weeks) in 2012 (p=0.001). Compression therapy was used in 87.3% of venous
ulcers in 2009 and 88.9% in 2012. In some areas of Sweden, every venous ulcer (100%) was
treated with compression therapy both in 2009 and in 2012.
Antibiotic treatment
Figure 3 illustrates antibiotic treatment from 2009 to 2012. In 2009, 76% of patients were
treated with antibiotics before registration, compared with 24% after registration. In 2012, the
corresponding figures were 73% before and 27% after registration. These differences were
significant in both years (p=0.001).
Considering all years between 2009 and 2012, antibiotic treatment for patients with hard-
to-heal ulcers in the registry nationwide was reduced from 71% before registration to 29%
after registration (p=0.001).
Page 21 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
DISCUSSION
The principal finding in this study was the significantly reduced healing time for hard-to-heal
ulcers registered with the RUT, from 146 days (21 weeks) in 2009 to 63 days (9 weeks) in
2012. This reduction in healing time seems to be due to structured wound management, based
on accurate diagnosis, continuity of care by nominating a responsible ulcer nurse for every
patient and follow-up to healing, all of which factors were facilitated by the RUT.
Although topical antimicrobial therapy for local ulcer infection, such as iodine, silver,
honey and polyhexamethylene biguanide (PHMB), has become more firmly established, no
further innovative dressings or devices were introduced for wound management on the
Swedish market during the study period. Negative pressure wound therapy was used in less
than 1.5% of all cases during the study, but is now more widespread in clinical practice. There
was some development of services, such as the introduction of smaller wound healing centres
based on the BWHC model.
Healing time is the one important endpoint in wound management.13 Earlier researchers
found a median healing time of 20–43 weeks when following patients through a period of 12
months.13 Some researchers have noted a healing rate of 83% at 30 weeks,14 while others have
reported that 62/90 (69%) of venous leg ulcers healed within 12 weeks.15 Moffatt et al.16
found that 70% of venous ulcers healed after 48 weeks of treatment; they also noted that
much of the evidence on healing rates is drawn from the results of randomized controlled
trials. These trials typically achieve 24-week healing rates in excess of 60%, but may not
reflect the complex issues faced in clinical practice.16
Another important finding in the present study was the low proportion of patients (24-
27%) given antibiotics between registration and ulcer healing; that is, in patients with a
diagnosis and adequate treatment. This can be compared with earlier findings of 68–78%1,5
for patients in primary care. Between 2009 and 2012, antibiotic treatment for patients with
hard-to-heal ulcers in the registry nationwide was reduced from 71% before registration to
29% between registration and ulcer healing (p=0.001).
There is still a high rate of oral antibiotic treatment for patients outside the registry,
which may be explained by the fact that these patients do not receive continuity of care or
treatment by a specialized team, where topical antimicrobial treatment is the golden standard
when treating local ulcer infection.
The use of topical antimicrobial dressings could be one explanation for the reduction in
antibiotic treatment. This issue is being addressed in an on going research study within the
frame of the RUT.
Page 22 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
A further explanation for the recent low rate of antibiotic treatment and reduced healing
time could be that the RUT focuses on stable doctor-patient relationships. Previous research
has shown the advantages of a structured organization for leg ulcer care.17,18 Petursson argues
that lack of continuity in medical care is the main reason why GPs prescribe antibiotics in a
“non-pharmacological” manner.8
The ulcer patient’s right to receive optimal treatment has been limited in recent decades,
owing to lack of diagnosis and low continuity in ulcer care.1,19–21 Dressing changes over
weeks, months and even years have been carried out, often without a proper diagnosis.1 It is
well known that understanding the aetiology of leg ulceration is a prerequisite for a systematic
clinical assessment as a base for appropriate wound management.12,14,15 The RUT meets these
requirements.
A large proportion of the patient population (39%) in the registry was concentrated in
Blekinge County. This could be considered a bias as the registry was developed in Blekinge
County, from where it has spread to the whole country. That the majority of patients were
treated in primary care reflects the true situation in Sweden.
The health care system requires information on the burden of care in order to inform
decisions on the needs of the population and the allocation of resources.16 The RUT comprises
a structured and practical methodology which can be used at any level in the health care
system.
Nationwide implementation of the RUT has not yet been fully achieved. One area for
future research is to investigate differences in the results of ulcer care between areas in
Sweden where the RUT is being used and areas where it is not used.
Another further research issue concerns the mapping of all pressure ulcers, such as ulcers
in younger patients with neurological diseases and in palliative care patients. The RUT is an
appropriate basis for such a study, as it has a special section for pressure ulcers.
Since March 2013, the registry has included 1,438 patients. The role of the registry
manager and the steering group is to show staff how data from the registry can be used to
improve ulcer care. We focus on documentation, treatment, education, research, and
economic analyses to guarantee improvement of health outcomes nationwide. Our ultimate
aim is twofold: to serve as basis for national guidelines and for the registry to be implemented
internationally.
Page 23 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
CONCLUSION
The findings from this study illustrate the immediate impact of the RUT as an improvement
project within wound management, resulting in significantly reduced healing time from 146
days (21 weeks) in 2009 to 63 days (9 weeks) in 2012. Antibiotic treatment was reduced from
71% before registration to 29% between registration and ulcer healing. The results also
demonstrate the potential for improved wound management when using a national quality
registry for structured ulcer care.
Contributors
R.F.Ö. led the research project and played the main role in the research design.
H.W.F. contributed to the data analysis and assisted in the research design and interpretation
of results.
Funding
This study was partly funded by the Council of Sciences in Blekinge County, Sweden.
Competing interests
None.
Ethics approval
The Lund Ethical Review Board considered the study to be a valuable quality improvement
study, so no further ethical approval was required
Provenance and peer review
This study has not been externally peer-reviewed.
Data-sharing statement
No additional data are available.
Acknowledgement
This study was performed in the interests of the steering group for the Swedish Registry of
Ulcer Treatment (RUT).
REFERENCES
1. Öien RF, Håkansson A, Ovhed I , Hansen BU. Wound management for 287 patients with
chronic leg ulcers demands 12 full-time nurses. Leg ulcer epidemiology and care in a well-
defined population in Southern Sweden . Scand J Prim Health Care 2000;18:220–5.
Page 24 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
2. Lindholm C, Bjellerup M, Christensen OB, Zederfeldt B. Quality of life in chronic leg
ulcer patients: An assessment according to the Nottingham Health Profile . Acta Derm
Venereol 1993;73:440–3.
3. Anon. Evidence-based prescribing of advanced wound dressings for chronic wounds in
primary care. MeRec Bulletin 2010;1:1–7.
4. Wiström J, Lindholm C, Melhus A, et al. Infections and treatment in chronic leg ulcers:
The use of antibiotics is too excessive, restrictive prescription is recommended.
Lakartidningen.1999 ;6:96:42–6 [in Swedish].
5. André M, Eriksson M, Odenholt I. Treatment of patients with skin and soft tissue
infections: Results from the STRAMA survey of diagnoses and prescriptions among general
practitioners. Lakartidningen 2006;103:3165–7 [in Swedish].
6. Öien RF, Åkesson N. Bacterial cultures, rapid strep test, and antibiotic treatment in infected
hard-to-heal ulcers in primary care. Scand J Prim Health Care, 2012;30:254–258.
7. European Wound Management Association (EWMA) Position document: Management of
wound infection. London: MEP;2006.
8. Petursson P. G Ps’ reasons for “non-pharmacological” prescribing of antibiotics: A
phenomenological study. Scand J Prim Health Care 2005;23:120-5.
9. Öien RF, Ragnarson Tennvall G. Accurate diagnosis and effective treatment of leg ulcer
reduce prevalence, care time and costs. J Wound Care 2006;15:259-62.
10. Öien RF. R UT (Register of Ulcer Treatment) – a winning concept for both patients and
the health care sector. EWMA J 2009; 9:41–4.
11. Lundström M (ed.), Albrecht S, Serring I, Svensson K, Wendel E. Handbook for
establishing quality registries. EyeNet Sweden, Karlskrona, Sweden 2005.
ISBN 91-631- 8585-7.
12. Harding K, Posnett J, Vowden K. A new methodology for costing wound care.
Int Wound J. 2012 Dec 13. doi: 10.1111/iwj.12006
13. Morrell CJ, Walters SJ, Dixon S, et al. Cost effectiveness of community leg ulcer clinics:
randomised controlled trial. BMJ 1998 May 16;316(7143):1487-91.
14. Rybak Z, Franks PJ, Krasowski G, et al. Strategy for the treatment of chronic leg wounds:
a new model in Poland. Int Angiol 2012 Dec;31(6):550-6.
15. Hjerppe A, Saarinen JP, Venermo MA, et al. Prolonged healing of venous leg ulcers: the
role of venous reflux, ulcer characteristics and mobility. J Wound Care. 2010
Nov;19(11):474, 476, 478 passim.
16. Moffatt CJ, Doherty DC, Smithdale R, Franks PJ. Clinical predictors of leg ulcer healing.
Page 25 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
Br J Dermatol. 2010 Jan;162(1):51-8. doi: 10.1111/j.1365-2133.2009.09397.x. Epub 2009 Jul
7.
17. Moffatt CJ, Franks PJ, Oldroyd M, et al. Community clinics for leg ulcers and impact on
healing. BMJ 1992;305:1389–92.
18. Kjaer ML, Sorensen LT, Karlsmark T, et al. Evaluation of the quality of venous leg ulcer
care given in a multidisciplinary specialist centre. J Wound Care 2005 Apr;14(4):145-50
19. Törnvall E, Wilhelmsson S. Quality of nursing care from the perspective of patients with
leg ulcers. J Wound Care. 2010 Sep;19(9):388–95
20. Moffatt CJ, Doherty DC, Smithdale R, Franks PJ. Clinical predictors of leg ulcer healing.
Br J Dermatol. 2010 Jan;162(1):51-8. doi: 10.1111/j.1365-2133.2009.09397.x. Epub 2009 Jul
7.
21. Edwards H, Finlayson K, Courtney M et al. Health service pathways for patients with
chronic leg ulcers: identifying effective pathways for facilitation of evidence based wound
care. BMC Health Serv Res. 2013 Mar 8;13:86. doi: 10.1186/1472-6963-13-86.
Page 26 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
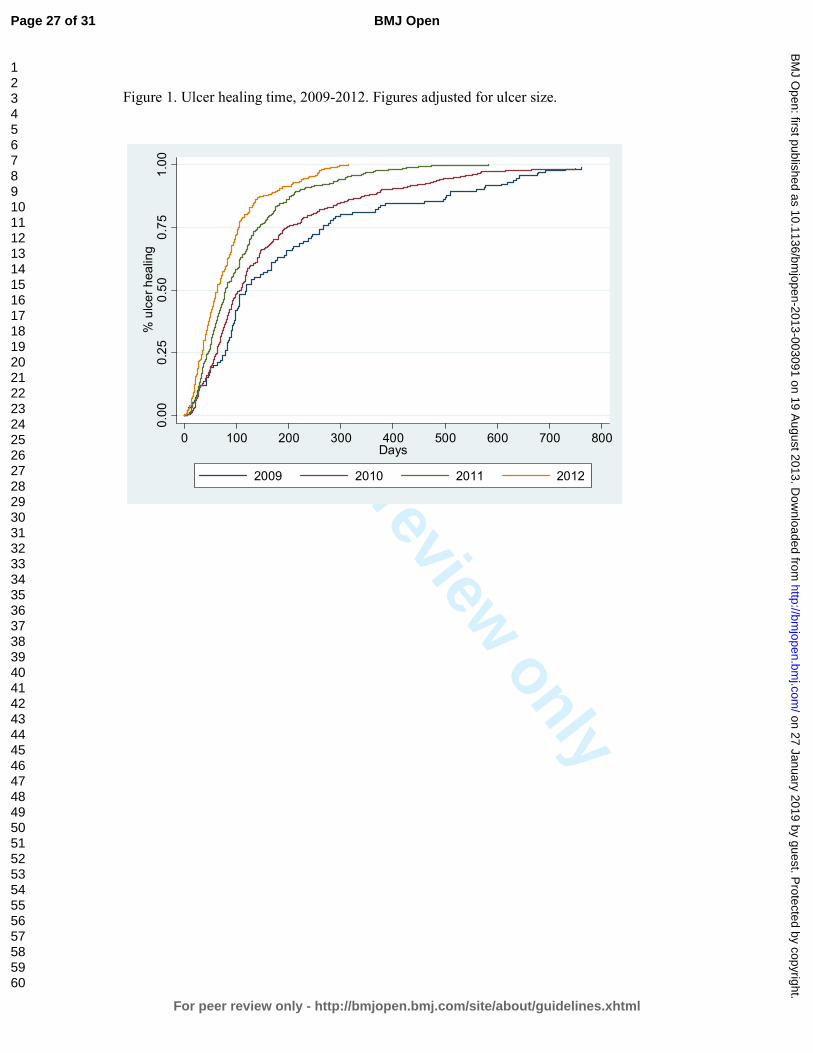
For peer review only
Figure 1. Ulcer healing time, 2009-2012. Figures adjusted for ulcer size.
0.00
0.25
0.50
0.75
1.00
% ulcer healing
0 100 200 300 400 500 600 700 800Days
2009 2010 2011 2012
Page 27 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
Figure 3. Antibiotic treatment before registration in RUT for the years 2009, 2010, 2011, and
2012, compared with antibiotic treatment between registration and ulcer healing for the same
years.
76
64
75 73
24
36
25 27
0
10
20
30
40
50
60
70
80
90
100
2009 2010 2011 2012
Before registration
After registration to ulcer healing
%
Page 28 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
Figure 2.Venous ulcer healing time, 2009-2012. Figures adjusted for ulcer size.
0.00
0.25
0.50
0.75
1.00
% ulcer healing
0 100 200 300 400 500 600 700 800Days
2009 2010 2011 2012
Page 29 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
STROBE Statement—Checklist of items that should be included in reports of cohort studies
Structured wound management through a national quality registry reduces healing time and
antibiotic treatment
Title and abstract
Introduction
Background/rationale
Objectives
Methods
Study design
Setting
Participants
Variables
Data sources/
measurement
Bias
Study size
Quantitative variables
Statistical methods
Results
Participants
Descriptive data
Outcome data
Main results
Other analyses
Discussion
Key results
Item
No
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
Recommendation
We have followed the recommendation
We have explained the scientific background in Introduction
We have stated the prespecified hypotheses
The key elements of study design are presented early in the
paper
The setting, locations, and relevant dates, including periods of
recruitment,
exposure, follow-up, and data collection are described
The eligibility criteria, and the sources and methods of selection
of participants. are described and methods of follow-up
All outcomes, exposures, predictors, potential confounders, and
effect modifiers are clearly defined.
Sources of data and details of methods of
assessment (measurement) for each variable of are given.
Since we have taken all patients in the registry, we considered it
not necessary to discuss sources of bias
We have described the results for every patient in the registry
during 2009 to 2012
No groupings were chosen
Statistics are thoroughly described for every moment
This section is written according to the check-list
Since we followed every patient to healing there are no missing
data for each variable of interest
The numbers of outcome events or summary measures over time
are reported
We have used the 95% confidence interval
We do not have any subgroups
key results with reference to study objectives have been
summarised
Page 30 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
Limitations
Interpretation
Generalisability
Other information
Funding
19
20
21
22
limitations of the study are discussed
An overall interpretation of results considering objectives,
limitations are being discussed. No similar studies have been
undertaken.
The generalisability (external validity) of the study results are
only mentioned,
This study was partly funded by the Council of Sciences in
Blekinge County.
Page 31 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
Ulcer healing time and antibiotic treatment before and after the introduction of the Registry of Ulcer Treatment – an
improvement project in a national quality registry in Sweden
Journal: BMJ Open
Manuscript ID: bmjopen-2013-003091.R2
Article Type: Research
Date Submitted by the Author: 20-Jul-2013
Complete List of Authors: Öien, Rut; Blekinge Wound Healing Center, Blekinge Centre of Competence Forssell, Henrik; Blekinge Centre of Competence,
<b>Primary Subject Heading</b>:
Medical management
Secondary Subject Heading: Diagnostics, General practice / Family practice, Medical management
Keywords: WOUND MANAGEMENT, GENERAL MEDICINE (see Internal Medicine), Quality in health care < HEALTH SERVICES ADMINISTRATION & MANAGEMENT
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on 27 January 2019 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2013-003091 on 19 A
ugust 2013. Dow
nloaded from
For peer review only
Ulcer healing time and antibiotic treatment before and after the
introduction of the Registry of Ulcer Treatment – an improvement project
in a national quality registry in Sweden
Rut F Öien,1,2 Henrik W Forssell2
Rut F Öien, MD, PhD, General Practitioner, Registry Manager of RUT (Registry of Ulcer
Treatment)
Henrik W Forssell, MD, PhD, Associate Professor
1Blekinge Wound Healing Centre, Karlskrona, Sweden 2Blekinge Centre of Competence, Karlskrona, Sweden
Correspondence to:
Dr Rut F Öien
Blekinge Wound Healing Centre
Blekinge Centre of Competence
S-371 41 Karlskrona
Sweden
Phone: +46 706 687202
E-mail: [email protected]
Page 1 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
ABSTRACT
Objectives: To investigate changes in ulcer healing time and antibiotic treatment in Sweden
following the introduction of the Registry of Ulcer Treatment (RUT), a national quality
registry, in 2009.
Design: A statistical analysis of RUT data concerning healing time and antibiotic treatment
for patients with hard-to-heal ulcers in Sweden between 2009 and 2012.
Setting: The RUT is a national web-based quality registry used to capture areas of
improvement in ulcer care and to structure wound management by registering patients with
hard-to-heal leg, foot and pressure ulcers. Registration includes variables such as gender, age,
diagnosis, healing time, antibiotic treatment and ulcer duration and size.
Population: Every patient with a hard-to-heal ulcer registered with the RUT between 2009
and 2012 (n=1,417) was included.
Main outcome measures: Statistical analyses were performed using Stata version 12.1.
Healing time was assessed with Kaplan-Meier analysis and adjustment was made for ulcer
size. A log-rank test was used for equality of survivor functions.
Results: According to the adjusted registry in December 2012, patients’ median age was 80
(mean 77.5, range 11–103) years. The median healing time for all ulcers, adjusted for ulcer
size, was 146 days (21 weeks) in 2009 and 63 days (9 weeks) in 2012 (p=0.001). Considering
all years between 2009 and 2012, antibiotic treatment for patients with hard-to-heal ulcers
was reduced from 71% before registration to 29% after registration to ulcer healing
(p=0.001).
Conclusions: Healing time and antibiotic treatment both decreased significantly during the 3
years after launch of the RUT.
Key words: hard-to-heal ulcers, ulcer assessment, diagnosis, ulcer care, ulcer healing,
antibiotics, RUT, pressure ulcer, topical antimicrobial treatment
Page 2 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
ARTICLE SUMMARY
Article focus
▪ The aim of this study was to analyse the data from the Swedish Registry of Ulcer Treatment
(RUT) to detect any differences in healing time and antibiotic treatment between 2009 and
2012.
Key messages
▪ Median healing time for all ulcers (adjusted for ulcer size) decreased significantly from 146
days in 2009 to 63 days in 2012.
▪ Median healing time for venous ulcers (adjusted for ulcer size) decreased significantly from
120 days in 2009 to 69 days in 2012.
▪ Antibiotic treatment for patients with hard-to-heal ulcers was reduced from 71% before
registration to 29% when using the RUT.
Strengths and limitations of this study
Strengths
▪ The data cover every patient registered with the RUT during 2009–2012.
▪ The RUT covers wound management in primary care, community care, private care and in-
patient hospital care throughout Sweden.
▪ The RUT provides a reliable diagnosis, adequate strategies for ulcer care, and a structured
follow-up of ulcer healing.
Limitations
▪ One limitation is that the RUT is still in the process of being implemented, which means that
in some areas of Sweden every patient with a hard-to-heal ulcer is registered, while
registration of patients in other areas is only partial.
Page 3 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
INTRODUCTION
Wound management not only consumes time and money, but ulcers and their treatment
reduce quality of life for affected patients.1–3
Patients with hard-to-heal ulcers have long been considered a neglected patient population.
Many are treated without diagnosis, and consequently receive suboptimal ulcer care. Overuse
of oral antibiotics in these patients (68–78%)1,4–6 is mostly due to absence of diagnosis or
inadequate clinical assessment of ulcer infections.6,7 The lack of continuity in ulcer care and
also the lack of team-working between health professionals in this field has further
contributed to antibiotic overuse.8 In Sweden, the absence of national guidelines for medical
ulcer care has had a negative impact on wound management.
Structured wound management based on accurate diagnosis leads to effective treatment,
and consequently to decreased prevalence, care time and costs.9 For this reason, the Swedish
Registry of Ulcer Treatment (RUT)10 was started in May 2009. Its purpose is to assess
physician diagnoses of ulcers, give medical staff a structured check list for optimal treatment
and identify areas of improvement in wound management.
The focus of this study was to investigate whether ulcer healing time and antibiotic
treatment have been affected by the registry. We aimed to analyse data from the RUT from
the time the registry was introduced nationally (2009) to 2012.
National registries
In recent decades, a system of national quality registries has been established in the Swedish
health and medical services,11 covering different areas of medicine. There are currently 73
registries which receive central funding (www.skl.se).
The ambition of the Swedish national quality registries is to gather data on diagnoses,
symptoms, interventions and treatment outcomes in order to give a continuous systematic
evaluation of medical practice.
The majority of the Swedish national quality registries have been developed by physicians
with special interest in a research field, in order to bring about quality improvement to health
care for a specific medical problem.
Page 4 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
The Registry of Ulcer Treatment - RUT
For the past 25 years, health care professionals in Blekinge have focused on quality
improvement and clinical research within the field of wound management.1,9 This tradition of
research linked to clinical practice led to the establishment of the Blekinge Wound Healing
Centre in 2003. This is a general practitioner (GP)-led, primary care-based specialist centre
covering the treatment and follow-up of the majority of ulcer patients across the county
(150,000 inhabitants). It offers a structured team management of ulcer care with emphasis on
diagnosis, documentation and treatment. The GP in charge of the centre is the first author of
this study (R.F.Ö.).
The experience of our daily practice combined with research results soon made it obvious
that there was a need for a structured programme for wound management to guarantee
optimal treatment. The RUT was started in Blekinge County by Rut F Öien, the registry
manager, who then developed the registry further and launched it nationwide.
The RUT was the first national registry in primary care. It is web-based, and the
participating units use the registry as a check list for ulcer assessment and a base for quality
improvement in their units.
The data must be collected in a uniform manner to capture the scale of wound care, as has
been previously pointed out.12 The conventional approach is to record details of ulcer care
such as treatment strategies, dressings, antibiotics, analgesics, investigations, hospital
admissions and surgical interventions at each patient contact over the period from first
presentation to wound healing.12 These details are noted in the patient’s medical record to
support decisions regarding the care for that individual patient.
Registration in the RUT usually takes place at the first patient contact, and follow-up can
be carried out when all the mandatory variables are registered. Each unit has access only to
data on its own patients; these can be retrieved online at any time, and used to compare the
unit’s quality of wound management with that across the country. By using accumulated data
for the whole country, areas of improvement can be highlighted.
To capture the situation of patients with pressure ulcers, during the study period the
pressure ulcer section of the registry was further developed. To improve our coverage of
community units (where these patients are mostly treated), we have established cooperation
with another Swedish national quality registry on pressure ulcer prevention.
This could in the future give a more accurate picture of pressure ulcer prevention linked to
either pressure ulcer healing or negative clinical events, such as death.
Page 5 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
Registering with the RUT has been mandatory in Blekinge County since 2012, and today
some of the larger national dermatological departments are likewise obliged to register with
the RUT.
METHODOLOGY
Study population and variables
During the study period we had frequent meetings with the participating units, at which nurses
and physicians provided feedback on the RUT. Having had access to the structure of the
registry, they commented on how the registry had made a difference in their approach to
wound management. Their new focus was on adequate diagnosis, continuity of care by
nominating a responsible ulcer nurse for every patient, and follow-up to ulcer healing. They
saw the documented shorter time to healing as an acknowledgment of their efforts to
introduce improved wound management.
Another area of improvement was the reduction in antibiotic treatment. Since the variable
for antibiotic treatment before and after registration is mandatory, the participants’ attention
was drawn to antibiotic use. They acknowledged the reduction in oral antibiotic treatment for
their patients as a success for their unit and an improvement of the patients’ quality of life.
During the study period, 160 patients were registered in 2009, 348 patients in 2010, 400 in
2011 and 509 in 2012, making a total of 1,417 patients nationwide by 2012.
The RUT registers patients with hard-to-heal leg, foot or pressure ulcers on two occasions.
The first registration, assessment of the ulcer diagnosis, is to guarantee optimal treatment. The
second registration is at follow-up; that is, at the point where the ulcer has healed or a
negative clinical event such as amputation or death has occurred. Every patient with a non-
healed ulcer remains in the registry until follow-up is completed.
At the first registration the following variables are recorded: social security number,
gender, age, date of diagnosis, profession or former profession, smoking habits, civil status,
number of children, mobility, exercise habits, and body mass index. The patient’s social
security number is linked and matched to the population statistics at the Council for Official
Statistics of Sweden.
To guarantee continuity of care there is a mandatory variable containing the name of the
nurse responsible for ulcer care, facilitating follow-up of every patient to complete ulcer
healing. This nurse is often the person responsible for registering the patient with the RUT.
Other details taken include whether the ulcer is new or recurrent; current or earlier
concomitant diseases; current medication, particularly analgesics and antibiotics; and ulcer-
Page 6 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
related pain. The patient history focuses on the following variables: deep vein thrombosis,
varicose veins, arterial or venous surgery, history of recurrent leg ulcers, and ulcer
localization (foot, leg or sacrum/hip; and lateral or medial). Ulcer size is measured by digital
planimeter (Visitrak®, manufactured in the United Kingdom for
Smith & Nephew Medical Limited, Hull HU3 2BN) and the number of ulcers is noted.
The patient’s arterial circulation is assessed by palpating the arteria dorsalis pedis and
arteria tibialis posterior and measuring the ankle-brachial pressure index with a hand-held
Doppler (manufactured by Histolab, Gothenburg, Sweden). The Doppler is also used for
measuring deep or superficial venous insufficiency (vena saphena magna, vena saphena
parva and vena poplitea).
The diagnosis is determined from these variables, in combination with the clinical
examination. The following ulcer diagnoses are used: venous ulcer, arterial ulcer, venous-
arterial ulcer, diabetic foot ulcer, pressure ulcer, traumatic ulcer, ulcer due to inflammatory
vessel diseases such as vasculitis, and other diagnoses (for example pyoderma gangrenosum).
The strategy for wound management includes dressings, care for the skin surrounding the
ulcer, and treatment for oedema. A photo gallery is linked to the registry for visualization of
the healing process.
The second registration (at follow-up) includes date of healing, healing time, estimated
number of weekly dressing changes throughout healing, compression therapy, treatment with
antibiotics, pain relief, the most frequently used dressing material, and whether advice was
given on smoking cessation, exercise and diet. Adverse events are also recorded, such as
amputation, venous or arterial surgery, and death.
Data analysis
The statistical analysis was performed using Stata version 12.1 (StataCorp LP, College
Station, TX, USA). Continuous variables were expressed as mean values (± standard
deviation (SD)) and compared using two-sample Student’s t-tests. Group comparisons for
categorical variables were performed using Pearson’s chi-square tests. Healing time was
assessed with Kaplan-Meier analysis and adjustment was made for ulcer size. A log-rank test
was used for equality of survivor functions. P<0.05 was considered statistically significant.
Page 7 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
Ethical approval
The Lund Ethical Review Board considered the study to be a valuable quality improvement
study, so no further ethical approval was required.
RESULTS
Healing time
Basic data from the adjusted registry in December 2012 showed a population (n=1,417) with
a median age of 80 years (mean age 77.5 years), ranging from 11 to 103 years.
The majority of the patients were women (60%). The median ulcer duration was 12 weeks
(mean 117 weeks), ranging from 1 week to 46 years, and the median ulcer size at inclusion in
the RUT was 3 cm2 (mean 12 cm2, range 0.05–600 cm2).
The participating units covered primary care (50%), community care (4%), hospital care
(22%), wound healing centres (22%) and private caregivers (2%). Patients from Blekinge
County constituted 39% of all patients.
Figure 1 illustrates the median healing time, adjusted for ulcer size, from 2009 to 2012.
The median healing time was 146 days (21 weeks) for all ulcers in 2009 and 63 days (9
weeks) for all ulcers in 2012 (p=0.001).
Negative pressure wound therapy was introduced in Europe in 1997, and has been used in
Swedish primary health care since 2006. During the study period, this technique was used in
only 1.3% of cases.
Figure 2 gives the median healing time for venous ulcers, adjusted for ulcer size, from
2009 to 2012. The median healing time for these ulcers was 120 days (17 weeks) in 2009 and
69 days (10 weeks) in 2012 (p=0.001). Compression therapy was used in 87.3% of venous
ulcers in 2009 and 88.9% in 2012. In some areas of Sweden, every venous ulcer (100%) was
treated with compression therapy both in 2009 and in 2012.
Antibiotic treatment
Figure 3 illustrates antibiotic treatment from 2009 to 2012. In 2009, 76% of patients were
treated with antibiotics before registration, compared with 24% after registration. In 2012, the
corresponding figures were 73% before and 27% after registration. These differences were
significant in both years (p=0.001).
Considering all years between 2009 and 2012, antibiotic treatment for patients with hard-
to-heal ulcers in the registry nationwide was reduced from 71% before registration to 29%
after registration (p=0.001).
Page 8 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
DISCUSSION
The principal finding in this study was the significantly reduced healing time for hard-to-heal
ulcers registered with the RUT, from 146 days (21 weeks) in 2009 to 63 days (9 weeks) in
2012. This reduction in healing time seems to be due to structured wound management, based
on accurate diagnosis, continuity of care by nominating a responsible ulcer nurse for every
patient and follow-up to healing, all of which factors were facilitated by the RUT.
Although topical antimicrobial therapy for local ulcer infection, such as iodine, silver,
honey and polyhexamethylene biguanide (PHMB), has become more firmly established, no
further innovative dressings or devices were introduced for wound management on the
Swedish market during the study period. Negative pressure wound therapy was used in less
than 1.5% of all cases during the study, but is now more widespread in clinical practice. There
was some development of services, such as the introduction of smaller wound healing centres
based on the model of the Blekinge Wound Healing Centre.
Healing time is the one important endpoint in wound management.13 Earlier researchers
found a median healing time of 20–43 weeks when following patients over a period of 12
months.13 Some researchers have noted a healing rate of 83% at 30 weeks,14 while others have
reported that 62/90 (69%) of venous leg ulcers healed within 12 weeks.15 Moffatt et al.16
found that 70% of venous ulcers healed after 48 weeks of treatment; they also noted that
much of the evidence on healing rates is drawn from the results of randomized controlled
trials. These trials typically achieve 24-week healing rates in excess of 60%, but may not
reflect the complex issues faced in clinical practice.16
Another important finding in the present study was the low proportion of patients (24-
27%) given antibiotics between registration and ulcer healing; that is, in patients with a
diagnosis and adequate treatment. This can be compared with earlier findings of 68–78%1,5
for patients in primary care. Between 2009 and 2012, antibiotic treatment for patients with
hard-to-heal ulcers in the registry nationwide was reduced from 71% before registration to
29% between registration and ulcer healing (p=0.001).
There is still a high rate of oral antibiotic treatment for patients outside the registry,
which may be explained by the fact that these patients do not receive continuity of care or
treatment by a specialized team, where topical antimicrobial treatment is the gold standard for
treating local ulcer infection.
The use of topical antimicrobial dressings could be one explanation for the reduction in
antibiotic treatment. This issue is being addressed in an ongoing research study within the
frame of the RUT.
Page 9 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
A further explanation for the recent low rate of antibiotic treatment and reduced healing
time could be that the RUT focuses on stable doctor-patient relationships. Previous research
has shown the advantages of a structured organization for leg ulcer care.17,18 Petursson argues
that lack of continuity in medical care is the main reason why GPs prescribe antibiotics in a
“non-pharmacological” manner.8
The ulcer patient’s right to receive optimal treatment has been limited in recent decades,
owing to lack of diagnosis and low continuity in ulcer care.1,19–21 Dressing changes over
weeks, months and even years have been carried out, often without a proper diagnosis.1 It is
well known that understanding the aetiology of leg ulceration is a prerequisite for a systematic
clinical assessment as a base for appropriate wound management.12,14,15 The RUT meets these
requirements.
A large proportion of the patient population (39%) in the registry was concentrated in
Blekinge County. This could be considered a bias, as the registry was developed in Blekinge
County before being expanded to the whole country. That the majority of patients were
treated in primary care reflects the true situation in Sweden.
The health care system requires information on the burden of care in order to inform
decisions on the needs of the population and the allocation of resources.16 The RUT comprises
a structured and practical methodology which can be used at any level in the health care
system.
Nationwide implementation of the RUT has not yet been fully achieved. One area for
future research is to investigate differences in the results of ulcer care between areas in
Sweden where the RUT is used and areas where it is not used.
Another further research issue concerns the mapping of all pressure ulcers, such as ulcers
in younger patients with neurological diseases and in palliative care patients. The RUT is an
appropriate basis for such a study, as it has a special section for pressure ulcers.
Since March 2013, the registry has included 1,438 patients. The role of the registry
manager and the steering group is to show staff how data from the registry can be used to
improve ulcer care. We focus on documentation, treatment, education, research, and
economic analyses to guarantee improvement of health outcomes nationwide. Our ultimate
aim is twofold: to serve as a basis for national guidelines, and for the registry to be
implemented internationally.
Page 10 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
CONCLUSION
The findings from this study illustrate the immediate impact of the RUT as an improvement
project within wound management, resulting in significantly reduced healing time from 146
days (21 weeks) in 2009 to 63 days (9 weeks) in 2012. Antibiotic treatment was reduced from
71% before registration to 29% between registration and ulcer healing. The results also
demonstrate the potential for improved wound management when using a national quality
registry for structured ulcer care.
Contributors
R.F.Ö. led the research project and played the main role in the research design.
H.W.F. contributed to the data analysis and assisted in the research design and interpretation
of results.
Funding
This study was partly funded by the Council of Sciences in Blekinge County, Sweden.
Competing interests
None.
Ethics approval
The Lund Ethical Review Board considered the study to be a valuable quality improvement
study, so no further ethical approval was required
Provenance and peer review
This study has not been externally peer-reviewed.
Data-sharing statement
No additional data are available.
Acknowledgements
This study was performed in the interests of the steering group for the Swedish Registry of
Ulcer Treatment (RUT).
REFERENCES
1. Öien RF, Håkansson A, Ovhed I , Hansen BU. Wound management for 287 patients with
chronic leg ulcers demands 12 full-time nurses. Leg ulcer epidemiology and care in a well-
defined population in Southern Sweden . Scand J Prim Health Care 2000;18:220–5.
Page 11 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
2. Lindholm C, Bjellerup M, Christensen OB, Zederfeldt B. Quality of life in chronic leg
ulcer patients: An assessment according to the Nottingham Health Profile . Acta Derm
Venereol 1993;73:440–3.
3. Anon. Evidence-based prescribing of advanced wound dressings for chronic wounds in
primary care. MeRec Bulletin 2010;1:1–7.
4. Wiström J, Lindholm C, Melhus A, et al. Infections and treatment in chronic leg ulcers:
The use of antibiotics is too excessive, restrictive prescription is recommended.
Lakartidningen.1999 ;6:96:42–6 [in Swedish].
5. André M, Eriksson M, Odenholt I. Treatment of patients with skin and soft tissue
infections: Results from the STRAMA survey of diagnoses and prescriptions among general
practitioners. Lakartidningen 2006;103:3165–7 [in Swedish].
6. Öien RF, Åkesson N. Bacterial cultures, rapid strep test, and antibiotic treatment in infected
hard-to-heal ulcers in primary care. Scand J Prim Health Care, 2012;30:254–258.
7. European Wound Management Association (EWMA) Position document: Management of
wound infection. London: MEP;2006.
8. Petursson P. G Ps’ reasons for “non-pharmacological” prescribing of antibiotics: A
phenomenological study. Scand J Prim Health Care 2005;23:120-5.
9. Öien RF, Ragnarson Tennvall G. Accurate diagnosis and effective treatment of leg ulcer
reduce prevalence, care time and costs. J Wound Care 2006;15:259-62.
10. Öien RF. R UT (Register of Ulcer Treatment) – a winning concept for both patients and
the health care sector. EWMA J 2009; 9:41–4.
11. Lundström M (ed.), Albrecht S, Serring I, Svensson K, Wendel E. Handbook for
establishing quality registries. EyeNet Sweden, Karlskrona, Sweden 2005.
ISBN 91-631- 8585-7.
12. Harding K, Posnett J, Vowden K. A new methodology for costing wound care.
Int Wound J. 2012 Dec 13. doi: 10.1111/iwj.12006
13. Morrell CJ, Walters SJ, Dixon S, et al. Cost effectiveness of community leg ulcer clinics:
randomised controlled trial. BMJ 1998 May 16;316(7143):1487-91.
14. Rybak Z, Franks PJ, Krasowski G, et al. Strategy for the treatment of chronic leg wounds:
a new model in Poland. Int Angiol 2012 Dec;31(6):550-6.
15. Hjerppe A, Saarinen JP, Venermo MA, et al. Prolonged healing of venous leg ulcers: the
role of venous reflux, ulcer characteristics and mobility. J Wound Care. 2010
Nov;19(11):474, 476, 478 passim.
16. Moffatt CJ, Doherty DC, Smithdale R, Franks PJ. Clinical predictors of leg ulcer healing.
Page 12 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
Br J Dermatol. 2010 Jan;162(1):51-8. doi: 10.1111/j.1365-2133.2009.09397.x. Epub 2009 Jul
7.
17. Moffatt CJ, Franks PJ, Oldroyd M, et al. Community clinics for leg ulcers and impact on
healing. BMJ 1992;305:1389–92.
18. Kjaer ML, Sorensen LT, Karlsmark T, et al. Evaluation of the quality of venous leg ulcer
care given in a multidisciplinary specialist centre. J Wound Care 2005 Apr;14(4):145-50
19. Törnvall E, Wilhelmsson S. Quality of nursing care from the perspective of patients with
leg ulcers. J Wound Care. 2010 Sep;19(9):388–95
20. Moffatt CJ, Doherty DC, Smithdale R, Franks PJ. Clinical predictors of leg ulcer healing.
Br J Dermatol. 2010 Jan;162(1):51-8. doi: 10.1111/j.1365-2133.2009.09397.x. Epub 2009 Jul
7.
21. Edwards H, Finlayson K, Courtney M et al. Health service pathways for patients with
chronic leg ulcers: identifying effective pathways for facilitation of evidence based wound
care. BMC Health Serv Res. 2013 Mar 8;13:86. doi: 10.1186/1472-6963-13-86.
Page 13 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
Ulcer healing time and antibiotic treatment before and after the
introduction of the Registry of Ulcer Treatment – an improvement project
in a national quality registry in Sweden
Rut F Öien,1,2 Henrik W Forssell2
Rut F Öien, MD, PhD, General Practitioner, Registry Manager of RUT (Registry of Ulcer
Treatment)
Henrik W Forssell, MD, PhD, Associate Professor
1Blekinge Wound Healing Centre, Karlskrona, Sweden 2Blekinge Centre of Competence, Karlskrona, Sweden
Correspondence to:
Dr Rut F Öien
Blekinge Wound Healing Centre
Blekinge Centre of Competence
S-371 41 Karlskrona
Sweden
Phone: +46 706 687202
E-mail: [email protected]
Page 14 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
ABSTRACT
Objectives: To investigate changes in ulcer healing time and antibiotic treatment in Sweden
following the introduction of the Registry of Ulcer Treatment (RUT), a national quality
registry, in 2009.
Design: A statistical analysis of RUT data concerning healing time and antibiotic treatment
for patients with hard-to-heal ulcers in Sweden between 2009 and 2012.
Setting: The RUT is a national web-based quality registry used to capture areas of
improvement in ulcer care and to structure wound management by registering patients with
hard-to-heal leg, foot and pressure ulcers. Registration includes variables such as gender, age,
diagnosis, healing time, antibiotic treatment and ulcer duration and size.
Population: Every patient with a hard-to-heal ulcer registered with the RUT between 2009
and 2012 (n=1,417) was included.
Main outcome measures: Statistical analyses were performed using Stata version 12.1.
Healing time was assessed with Kaplan-Meier analysis and adjustment was made for ulcer
size. A log-rank test was used for equality of survivor functions.
Results: According to the adjusted registry in December 2012, patients’ median age was 80
(mean 77.5, range 11–103) years. The median healing time for all ulcers, adjusted for ulcer
size, was 146 days (21 weeks) in 2009 and 63 days (9 weeks) in 2012 (p=0.001). Considering
all years between 2009 and 2012, antibiotic treatment for patients with hard-to-heal ulcers
was reduced from 71% before registration to 29% after registration to ulcer healing
(p=0.001).
Conclusions: Healing time and antibiotic treatment both decreased significantly during the 3
years after launch of the RUT.
Key words: hard-to-heal ulcers, ulcer assessment, diagnosis, ulcer care, ulcer healing,
antibiotics, RUT, pressure ulcer, topical antimicrobial treatment
Page 15 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
ARTICLE SUMMARY
Article focus
▪ The aim of this study was to analyse the data from the Swedish Registry of Ulcer Treatment
(RUT) to detect any differences in healing time and antibiotic treatment between 2009 and
2012.
Key messages
▪ Median healing time for all ulcers (adjusted for ulcer size) decreased significantly from 146
days in 2009 to 63 days in 2012.
▪ Median healing time for venous ulcers (adjusted for ulcer size) decreased significantly from
120 days in 2009 to 69 days in 2012.
▪ Antibiotic treatment for patients with hard-to-heal ulcers was reduced from 71% before
registration to 29% when using the RUT.
Strengths and limitations of this study
Strengths
▪ The data cover every patient registered with the RUT during 2009–2012.
▪ The RUT covers wound management in primary care, community care, private care and in-
patient hospital care throughout Sweden.
▪ The RUT provides a reliable diagnosis, adequate strategies for ulcer care, and a structured
follow-up of ulcer healing.
Limitations
▪ One limitation is that the RUT is still in the process of being implemented, which means that
in some areas of Sweden every patient with a hard-to-heal ulcer is registered, while
registration of patients in other areas is only partial.
Page 16 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
INTRODUCTION
Wound management not only consumes time and money, but ulcers and their treatment
reduce quality of life for affected patients.1–3
Patients with hard-to-heal ulcers have long been considered a neglected patient population.
Many are treated without diagnosis, and consequently receive suboptimal ulcer care. Overuse
of oral antibiotics in these patients (68–78%)1,4–6 is mostly due to absence of diagnosis or
inadequate clinical assessment of ulcer infections.6,7 The lack of continuity in ulcer care and
also the lack of team-working between health professionals in this field has further
contributed to antibiotic overuse.8 In Sweden, the absence of national guidelines for medical
ulcer care has had a negative impact on wound management.
Structured wound management based on accurate diagnosis leads to effective treatment,
and consequently to decreased prevalence, care time and costs.9 For this reason, the Swedish
Registry of Ulcer Treatment (RUT)10 was started in May 2009. Its purpose is to assess
physician diagnoses of ulcers, give medical staff a structured check list for optimal treatment
and identify areas of improvement in wound management.
The focus of this study was to investigate whether ulcer healing time and antibiotic
treatment have been affected by the registry. We aimed to analyse data from the RUT from
the time the registry was introduced nationally (2009) to 2012.
National registries
In recent decades, a system of national quality registries has been established in the Swedish
health and medical services,11 covering different areas of medicine. There are currently 73
registries which receive central funding (www.skl.se).
The ambition of the Swedish national quality registries is to gather data on diagnoses,
symptoms, interventions and treatment outcomes in order to give a continuous systematic
evaluation of medical practice.
The majority of the Swedish national quality registries have been developed by physicians
with special interest in a research field, in order to bring about quality improvement to health
care for a specific medical problem.
Page 17 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
The Registry of Ulcer Treatment - RUT
For the past 25 years, health care professionals in Blekinge have focused on quality
improvement and clinical research within the field of wound management.1,9 This tradition of
research linked to clinical practice led to the establishment of the Blekinge Wound Healing
Centre in 2003. This is a general practitioner (GP)-led, primary care-based specialist centre
covering the treatment and follow-up of the majority of ulcer patients across the county (150,
000 inhabitants). It offers a structured team management of ulcer care with emphasis on
diagnosis, documentation and treatment. The GP in charge of the centre is the first author of
this study (R.F.Ö.).
The experience of our daily practice combined with research results soon made it obvious
that there was a need for a structured programme for wound management to guarantee
optimal treatment. The RUT was started in Blekinge County by Rut F Öien, the registry
manager, who then developed the registry further and launched it nationwide.
The RUT was the first national registry in primary care. It is web-based, and the
participating units use the registry as a check list for ulcer assessment and a base for quality
improvement in their units.
The data must be collected in a uniform manner to capture the scale of wound care, as has
been previously pointed out.12 The conventional approach is to record details of ulcer care
such as treatment strategies, dressings, antibiotics, analgesics, investigations, hospital
admissions and surgical interventions at each patient contact over the period from first
presentation to wound healing.12 These details are noted in the patient’s medical record to
support decisions regarding the care for that individual patient.
Registration in the RUT usually takes place at the first patient contact, and follow-up can
be carried out when all the mandatory variables are registered. Each unit has access only to
data on its own patients; these can be retrieved online at any time, and used to compare the
unit’s quality of wound management with that across the country. By using accumulated data
for the whole country, areas of improvement can be highlighted.
To capture the situation of patients with pressure ulcers, during the study period the
pressure ulcer section of the registry was further developed. To improve our coverage of
community units (where these patients are mostly treated), we have established cooperation
with another Swedish national quality registry on pressure ulcer prevention.
This could in the future give a more accurate picture of pressure ulcer prevention linked to
either pressure ulcer healing or negative clinical events, such as death.
Page 18 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
Registering with the RUT has been mandatory in Blekinge County since 2012, and today
some of the larger national dermatological departments are likewise obliged to register with
the RUT.
METHODOLOGY
Study population and variables
During the study period we had frequent meetings with the participating units, at which nurses
and physicians provided feedback on the RUT. Having had access to the structure of the
registry, they commented on how the registry had made a difference in their approach to
wound management. Their new focus was on adequate diagnosis, continuity of care by
nominating a responsible ulcer nurse for every patient, and follow-up to ulcer healing. They
saw the documented shorter time to healing as an acknowledgment of their efforts to
introduce improved wound management.
Another area of improvement was the reduction in antibiotic treatment. Since the variable
for antibiotic treatment before and after registration is mandatory, the participants’ attention
was drawn to antibiotic use. They acknowledged the reduction in oral antibiotic treatment for
their patients as a success for their unit and an improvement of the patients’ quality of life.
During the study period, 160 patients were registered in 2009, 348 patients in 2010, 400 in
2011 and 509 in 2012, making a total of 1,417 patients nationwide by 2012.
The RUT registers patients with hard-to-heal leg, foot or pressure ulcers on two occasions.
The first registration, assessment of the ulcer diagnosis, is to guarantee optimal treatment. The
second registration is at follow-up; that is, at the point where the ulcer has healed or a
negative clinical event such as amputation or death has occurred. Every patient with a non-
healed ulcer remains in the registry until follow-up is completed.
At the first registration the following variables are recorded: social security number,
gender, age, date of diagnosis, profession or former profession, smoking habits, civil status,
number of children, mobility, exercise habits, and body mass index. The patient’s social
security number is linked and matched to the population statistics at the Council for Official
Statistics of Sweden.
To guarantee continuity of care there is a mandatory variable containing the name of the
nurse responsible for ulcer care, facilitating follow-up of every patient to complete ulcer
healing. This nurse is often the person responsible for registering the patient with the RUT.
Other details taken include whether the ulcer is new or recurrent; current or earlier
concomitant diseases; current medication, particularly analgesics and antibiotics; and ulcer-
Page 19 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
related pain. The patient history focuses on the following variables: deep vein thrombosis,
varicose veins, arterial or venous surgery, history of recurrent leg ulcers, and ulcer
localization (foot, leg or sacrum/hip; and lateral or medial). Ulcer size is measured by digital
planimeter (Visitrak®, manufactured in the United Kingdom for
Smith & Nephew Medical Limited, Hull HU3 2BN) and the number of ulcers is noted.
The patient’s arterial circulation is assessed by palpating the arteria dorsalis pedis and
arteria tibialis posterior and measuring the ankle-brachial pressure index with a hand-held
Doppler (manufactured by Histolab, Gothenburg, Sweden). The Doppler is also used for
measuring deep or superficial venous insufficiency (vena saphena magna, vena saphena
parva and vena poplitea).
The diagnosis is determined from these variables, in combination with the clinical
examination. The following ulcer diagnoses are used: venous ulcer, arterial ulcer, venous-
arterial ulcer, diabetic foot ulcer, pressure ulcer, traumatic ulcer, ulcer due to inflammatory
vessel diseases such as vasculitis, and other diagnoses (for example pyoderma gangrenosum).
The strategy for wound management includes dressings, care for the skin surrounding the
ulcer, and treatment for oedema. A photo gallery is linked to the registry for visualization of
the healing process.
The second registration (at follow-up) includes date of healing, healing time, estimated
number of weekly dressing changes throughout healing, compression therapy, treatment with
antibiotics, pain relief, the most frequently used dressing material, and whether advice was
given on smoking cessation, exercise and diet. Adverse events are also recorded, such as
amputation, venous or arterial surgery, and death.
Data analysis
The statistical analysis was performed using Stata version 12.1 (StataCorp LP, College
Station, TX, USA). Continuous variables were expressed as mean values (± standard
deviation (SD)) and compared using two-sample Student’s t-tests. Group comparisons for
categorical variables were performed using Pearson’s chi-square tests. Healing time was
assessed with Kaplan-Meier analysis and adjustment was made for ulcer size. A log-rank test
was used for equality of survivor functions. P<0.05 was considered statistically significant.
Page 20 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
Ethical approval
The Lund Ethical Review Board considered the study to be a valuable quality improvement
study, so no further ethical approval was required.
RESULTS
Healing time
Basic data from the adjusted registry in December 2012 showed a population (n=1,417) with
a median age of 80 years (mean age 77.5 years), ranging from 11 to 103 years.
The majority of the patients were women (60%). The median ulcer duration was 12 weeks
(mean 117 weeks), ranging from 1 week to 46 years, and the median ulcer size at inclusion in
the RUT was 3 cm2 (mean 12 cm2, range 0.05–600 cm2).
The participating units covered primary care (50%), community care (4%), hospital care
(22%), wound healing centres (22%) and private caregivers (2%). Patients from Blekinge
County constituted 39% of all patients.
Figure 1 illustrates the median healing time, adjusted for ulcer size, from 2009 to 2012.
The median healing time was 146 days (21 weeks) for all ulcers in 2009 and 63 days (9
weeks) for all ulcers in 2012 (p=0.001).
Negative pressure wound therapy was introduced in Europe in 1997, and has been used in
Swedish primary health care since 2006. During the study period, this technique was used in
only 1.3% of cases.
Figure 2 gives the median healing time for venous ulcers, adjusted for ulcer size, from
2009 to 2012. The median healing time for these ulcers was 120 days (17 weeks) in 2009 and
69 days (10 weeks) in 2012 (p=0.001). Compression therapy was used in 87.3% of venous
ulcers in 2009 and 88.9% in 2012. In some areas of Sweden, every venous ulcer (100%) was
treated with compression therapy both in 2009 and in 2012.
Antibiotic treatment
Figure 3 illustrates antibiotic treatment from 2009 to 2012. In 2009, 76% of patients were
treated with antibiotics before registration, compared with 24% after registration. In 2012, the
corresponding figures were 73% before and 27% after registration. These differences were
significant in both years (p=0.001).
Considering all years between 2009 and 2012, antibiotic treatment for patients with hard-
to-heal ulcers in the registry nationwide was reduced from 71% before registration to 29%
after registration (p=0.001).
Page 21 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
DISCUSSION
The principal finding in this study was the significantly reduced healing time for hard-to-heal
ulcers registered with the RUT, from 146 days (21 weeks) in 2009 to 63 days (9 weeks) in
2012. This reduction in healing time seems to be due to structured wound management, based
on accurate diagnosis, continuity of care by nominating a responsible ulcer nurse for every
patient and follow-up to healing, all of which factors were facilitated by the RUT.
Although topical antimicrobial therapy for local ulcer infection, such as iodine, silver,
honey and polyhexamethylene biguanide (PHMB), has become more firmly established, no
further innovative dressings or devices were introduced for wound management on the
Swedish market during the study period. Negative pressure wound therapy was used in less
than 1.5% of all cases during the study, but is now more widespread in clinical practice. There
was some development of services, such as the introduction of smaller wound healing centres
based on the model of the Blekinge Wound Healing Centre.
Healing time is the one important endpoint in wound management.13 Earlier researchers
found a median healing time of 20–43 weeks when following patients over a period of 12
months.13 Some researchers have noted a healing rate of 83% at 30 weeks,14 while others have
reported that 62/90 (69%) of venous leg ulcers healed within 12 weeks.15 Moffatt et al.16
found that 70% of venous ulcers healed after 48 weeks of treatment; they also noted that
much of the evidence on healing rates is drawn from the results of randomized controlled
trials. These trials typically achieve 24-week healing rates in excess of 60%, but may not
reflect the complex issues faced in clinical practice.16
Another important finding in the present study was the low proportion of patients (24-
27%) given antibiotics between registration and ulcer healing; that is, in patients with a
diagnosis and adequate treatment. This can be compared with earlier findings of 68–78%1,5
for patients in primary care. Between 2009 and 2012, antibiotic treatment for patients with
hard-to-heal ulcers in the registry nationwide was reduced from 71% before registration to
29% between registration and ulcer healing (p=0.001).
There is still a high rate of oral antibiotic treatment for patients outside the registry,
which may be explained by the fact that these patients do not receive continuity of care or
treatment by a specialized team, where topical antimicrobial treatment is the gold standard for
treating local ulcer infection.
The use of topical antimicrobial dressings could be one explanation for the reduction in
antibiotic treatment. This issue is being addressed in an ongoing research study within the
frame of the RUT.
Page 22 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
A further explanation for the recent low rate of antibiotic treatment and reduced healing
time could be that the RUT focuses on stable doctor-patient relationships. Previous research
has shown the advantages of a structured organization for leg ulcer care.17,18 Petursson argues
that lack of continuity in medical care is the main reason why GPs prescribe antibiotics in a
“non-pharmacological” manner.8
The ulcer patient’s right to receive optimal treatment has been limited in recent decades,
owing to lack of diagnosis and low continuity in ulcer care.1,19–21 Dressing changes over
weeks, months and even years have been carried out, often without a proper diagnosis.1 It is
well known that understanding the aetiology of leg ulceration is a prerequisite for a systematic
clinical assessment as a base for appropriate wound management.12,14,15 The RUT meets these
requirements.
A large proportion of the patient population (39%) in the registry was concentrated in
Blekinge County. This could be considered a bias, as the registry was developed in Blekinge
County before being expanded to the whole country. That the majority of patients were
treated in primary care reflects the true situation in Sweden.
The health care system requires information on the burden of care in order to inform
decisions on the needs of the population and the allocation of resources.16 The RUT comprises
a structured and practical methodology which can be used at any level in the health care
system.
Nationwide implementation of the RUT has not yet been fully achieved. One area for
future research is to investigate differences in the results of ulcer care between areas in
Sweden where the RUT is used and areas where it is not used.
Another further research issue concerns the mapping of all pressure ulcers, such as ulcers
in younger patients with neurological diseases and in palliative care patients. The RUT is an
appropriate basis for such a study, as it has a special section for pressure ulcers.
Since March 2013, the registry has included 1,438 patients. The role of the registry
manager and the steering group is to show staff how data from the registry can be used to
improve ulcer care. We focus on documentation, treatment, education, research, and
economic analyses to guarantee improvement of health outcomes nationwide. Our ultimate
aim is twofold: to serve as a basis for national guidelines, and for the registry to be
implemented internationally.
Page 23 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
CONCLUSION
The findings from this study illustrate the immediate impact of the RUT as an improvement
project within wound management, resulting in significantly reduced healing time from 146
days (21 weeks) in 2009 to 63 days (9 weeks) in 2012. Antibiotic treatment was reduced from
71% before registration to 29% between registration and ulcer healing. The results also
demonstrate the potential for improved wound management when using a national quality
registry for structured ulcer care.
Contributors
R.F.Ö. led the research project and played the main role in the research design.
H.W.F. contributed to the data analysis and assisted in the research design and interpretation
of results.
Funding
This study was partly funded by the Council of Sciences in Blekinge County, Sweden.
Competing interests
None.
Ethics approval
The Lund Ethical Review Board considered the study to be a valuable quality improvement
study, so no further ethical approval was required
Provenance and peer review
This study has not been externally peer-reviewed.
Data-sharing statement
No additional data are available.
Acknowledgements
This study was performed in the interests of the steering group for the Swedish Registry of
Ulcer Treatment (RUT).
REFERENCES
1. Öien RF, Håkansson A, Ovhed I , Hansen BU. Wound management for 287 patients with
chronic leg ulcers demands 12 full-time nurses. Leg ulcer epidemiology and care in a well-
defined population in Southern Sweden . Scand J Prim Health Care 2000;18:220–5.
Page 24 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
2. Lindholm C, Bjellerup M, Christensen OB, Zederfeldt B. Quality of life in chronic leg
ulcer patients: An assessment according to the Nottingham Health Profile . Acta Derm
Venereol 1993;73:440–3.
3. Anon. Evidence-based prescribing of advanced wound dressings for chronic wounds in
primary care. MeRec Bulletin 2010;1:1–7.
4. Wiström J, Lindholm C, Melhus A, et al. Infections and treatment in chronic leg ulcers:
The use of antibiotics is too excessive, restrictive prescription is recommended.
Lakartidningen.1999 ;6:96:42–6 [in Swedish].
5. André M, Eriksson M, Odenholt I. Treatment of patients with skin and soft tissue
infections: Results from the STRAMA survey of diagnoses and prescriptions among general
practitioners. Lakartidningen 2006;103:3165–7 [in Swedish].
6. Öien RF, Åkesson N. Bacterial cultures, rapid strep test, and antibiotic treatment in infected
hard-to-heal ulcers in primary care. Scand J Prim Health Care, 2012;30:254–258.
7. European Wound Management Association (EWMA) Position document: Management of
wound infection. London: MEP;2006.
8. Petursson P. G Ps’ reasons for “non-pharmacological” prescribing of antibiotics: A
phenomenological study. Scand J Prim Health Care 2005;23:120-5.
9. Öien RF, Ragnarson Tennvall G. Accurate diagnosis and effective treatment of leg ulcer
reduce prevalence, care time and costs. J Wound Care 2006;15:259-62.
10. Öien RF. R UT (Register of Ulcer Treatment) – a winning concept for both patients and
the health care sector. EWMA J 2009; 9:41–4.
11. Lundström M (ed.), Albrecht S, Serring I, Svensson K, Wendel E. Handbook for
establishing quality registries. EyeNet Sweden, Karlskrona, Sweden 2005.
ISBN 91-631- 8585-7.
12. Harding K, Posnett J, Vowden K. A new methodology for costing wound care.
Int Wound J. 2012 Dec 13. doi: 10.1111/iwj.12006
13. Morrell CJ, Walters SJ, Dixon S, et al. Cost effectiveness of community leg ulcer clinics:
randomised controlled trial. BMJ 1998 May 16;316(7143):1487-91.
14. Rybak Z, Franks PJ, Krasowski G, et al. Strategy for the treatment of chronic leg wounds:
a new model in Poland. Int Angiol 2012 Dec;31(6):550-6.
15. Hjerppe A, Saarinen JP, Venermo MA, et al. Prolonged healing of venous leg ulcers: the
role of venous reflux, ulcer characteristics and mobility. J Wound Care. 2010
Nov;19(11):474, 476, 478 passim.
16. Moffatt CJ, Doherty DC, Smithdale R, Franks PJ. Clinical predictors of leg ulcer healing.
Page 25 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
Br J Dermatol. 2010 Jan;162(1):51-8. doi: 10.1111/j.1365-2133.2009.09397.x. Epub 2009 Jul
7.
17. Moffatt CJ, Franks PJ, Oldroyd M, et al. Community clinics for leg ulcers and impact on
healing. BMJ 1992;305:1389–92.
18. Kjaer ML, Sorensen LT, Karlsmark T, et al. Evaluation of the quality of venous leg ulcer
care given in a multidisciplinary specialist centre. J Wound Care 2005 Apr;14(4):145-50
19. Törnvall E, Wilhelmsson S. Quality of nursing care from the perspective of patients with
leg ulcers. J Wound Care. 2010 Sep;19(9):388–95
20. Moffatt CJ, Doherty DC, Smithdale R, Franks PJ. Clinical predictors of leg ulcer healing.
Br J Dermatol. 2010 Jan;162(1):51-8. doi: 10.1111/j.1365-2133.2009.09397.x. Epub 2009 Jul
7.
21. Edwards H, Finlayson K, Courtney M et al. Health service pathways for patients with
chronic leg ulcers: identifying effective pathways for facilitation of evidence based wound
care. BMC Health Serv Res. 2013 Mar 8;13:86. doi: 10.1186/1472-6963-13-86.
Page 26 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
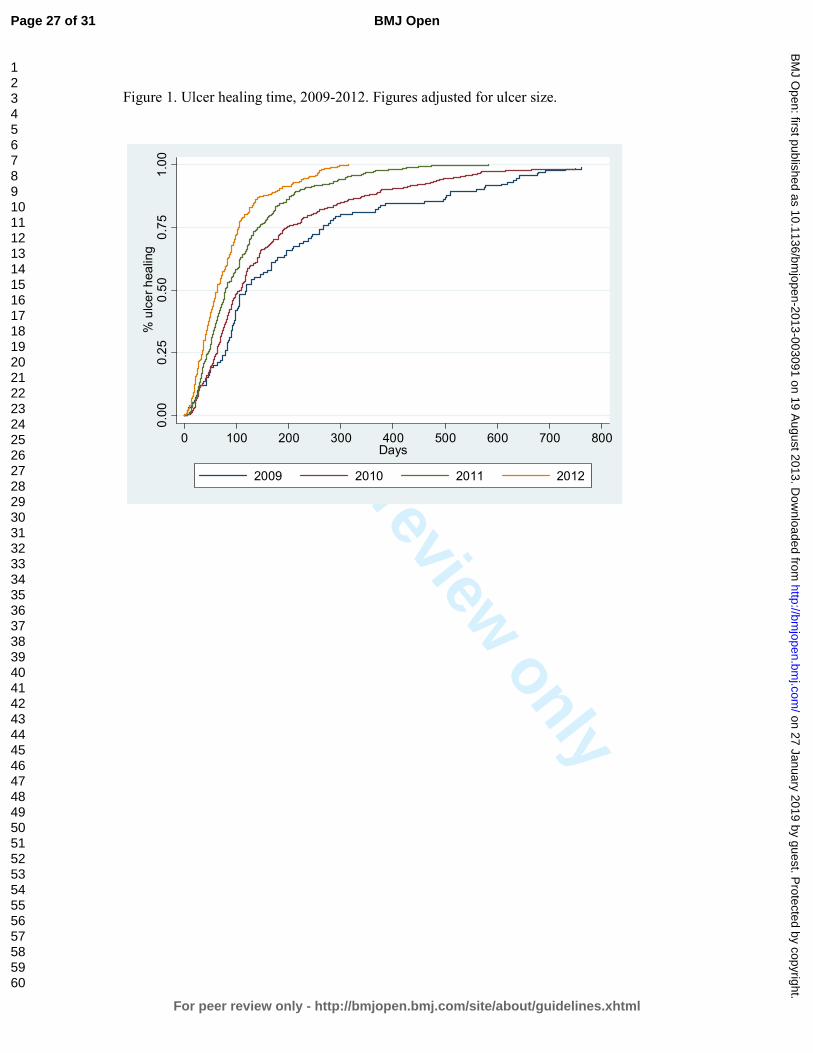
For peer review only
Figure 1. Ulcer healing time, 2009-2012. Figures adjusted for ulcer size.
0.00
0.25
0.50
0.75
1.00
% ulcer healing
0 100 200 300 400 500 600 700 800Days
2009 2010 2011 2012
Page 27 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from

For peer review only
Figure 2.Venous ulcer healing time, 2009-2012. Figures adjusted for ulcer size.
0.00
0.25
0.50
0.75
1.00
% ulcer healing
0 100 200 300 400 500 600 700 800Days
2009 2010 2011 2012
Page 28 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
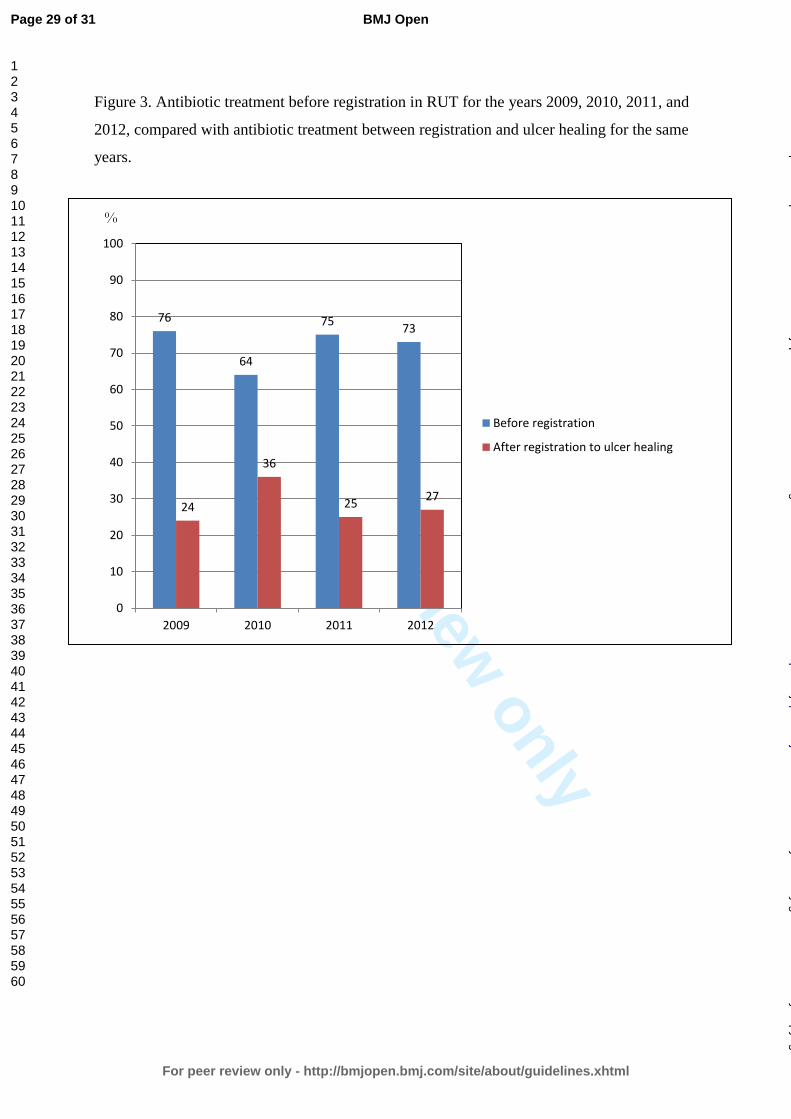
For peer review only
Figure 3. Antibiotic treatment before registration in RUT for the years 2009, 2010, 2011, and
2012, compared with antibiotic treatment between registration and ulcer healing for the same
years.
76
64
75 73
24
36
25 27
0
10
20
30
40
50
60
70
80
90
100
2009 2010 2011 2012
Before registration
After registration to ulcer healing
%
Page 29 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
STROBE Statement—Checklist of items that should be included in reports of cohort studies
Structured wound management through a national quality registry reduces healing time and
antibiotic treatment
Title and abstract
Introduction
Background/rationale
Objectives
Methods
Study design
Setting
Participants
Variables
Data sources/
measurement
Bias
Study size
Quantitative variables
Statistical methods
Results
Participants
Descriptive data
Outcome data
Main results
Other analyses
Discussion
Key results
Item
No
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
Recommendation
We have followed the recommendation
We have explained the scientific background in Introduction
We have stated the prespecified hypotheses
The key elements of study design are presented early in the
paper
The setting, locations, and relevant dates, including periods of
recruitment,
exposure, follow-up, and data collection are described
The eligibility criteria, and the sources and methods of selection
of participants. are described and methods of follow-up
All outcomes, exposures, predictors, potential confounders, and
effect modifiers are clearly defined.
Sources of data and details of methods of
assessment (measurement) for each variable of are given.
Since we have taken all patients in the registry, we considered it
not necessary to discuss sources of bias
We have described the results for every patient in the registry
during 2009 to 2012
No groupings were chosen
Statistics are thoroughly described for every moment
This section is written according to the check-list
Since we followed every patient to healing there are no missing
data for each variable of interest
The numbers of outcome events or summary measures over time
are reported
We have used the 95% confidence interval
We do not have any subgroups
key results with reference to study objectives have been
summarised
Page 30 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from
For peer review only
Limitations
Interpretation
Generalisability
Other information
Funding
19
20
21
22
limitations of the study are discussed
An overall interpretation of results considering objectives,
limitations are being discussed. No similar studies have been
undertaken.
The generalisability (external validity) of the study results are
only mentioned,
This study was partly funded by the Council of Sciences in
Blekinge County.
Page 31 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 27 January 2019 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2013-003091 on 19 August 2013. D
ownloaded from