bonemineral content determined …jnm.snmjournals.org/content/16/10/891.full.pdf,i‚ t'_...
TRANSCRIPT

Quantitation of bone mineral by photon absorptiometry is a simple and accurate method/or determining changes in bone volume andmineral content in serial studies. An extensionof the scintillation camera method for studyingsuch changes in the calcaneous is described.This technique is applicable to large areas ofbone, thereby minimizing the effect of reposihoning errors. Using a 40-mCi 2@Am sheetsource, a 2.1% reproducibility in bone phan.
toms and a 2.4% reproducibility in normal pa
tients was achieved. Several case studies arepresented to illustrate sensitivity and clinical up
plication of the method. Although bone mineraldeterminations are now performed in a limitednumber of health care facilities, the scintillationcamera method described in this report coul4increase the availability of these determinationssignificantly.
In 1962 Cameron, et al, described a scanningtechnique for determinating bone mineral contentin which a collimated monoenergetic photon beamcoupled to a scintillation detector moved across theselected bone in a linear fashion (1 ,2 ) . The bonemineral content was related to the intensity of radiation transmitted through bone and overlying softtissue compared with that transmitted through softtissue alone. This technique eliminated problems associated with the poorly defined beam energy and
nonuniform film response inherent in roentgenographic film methods for determining bone mineralcontent, and it avoided intersystem calibration sincephoton energy was constant (3) . Because of theirregularboneshapeand thicknessand the unevendistribution of mineral content, however, values obtamed from a single linear scan may not be representative of the entire bone and may in fact varysignificantly depending on the site of the scan path.To overcome these potential problems, we have ex
tended our previously reported method of photon
transmission scanning with the scintillation camera (4) ; we now use a dedicated minicomputer to
produce functional images representing mineral con
tent. A large area of interest in the selected boneis defined for computations, thereby obtaining amore representative sampling of total bone mineralcontent and minimizing errors due to imprecise repositioning of the bone in sequential patient studies.Because of the intrinsic flexibility of the technique,mineral content may be determined for irregularlyshaped bones and for various regions of interest.
METHODS
A simplified two-component model can be usedto explain the theoretical basis of the technique. Onecompartment consists of bone compressed to a thickness of Xb after all soft components have been extracted whereas the other compartment, of thicknessxs,is composedof water-equivalentsofttissuesurrounding the bone, and extracted from its intramedullary spaces (Fig. 1) . The intensity of incidentphotons (Ia) transmitted through the bone, water,and water-equivalent tissue (I) and through anequivalent thickness of water alone (I@*) can beexpressed as follows:
I = L,e_1@. —
10*= I,,e_i@.(x.+ Xb)
The iz5 iS the linear attenuation coefficient ofwater for the 241Am photons and is a constant.The linear attenuation coefficient of bone mineral,/@b, depends on its chemical composition. The re
maining parameter, Xb,is a variable that depends onboth the anatomic thickness of the bone and the
Received Oct. 7, 1974; revision accepted April 29, 1975.For reprints contact: J. A. Burdine, Nuclear Medicine
Section, Dept. of Radiology, Baylor College of Medicine,Houston,Tex.77025.
Volume 16, Number 10 891
BONE MINERAL CONTENT
DETERMINED BY FUNCTIONAL IMAGING
E.GordonDePuey,Wayne1.Thompson,VeerasamyAlagarsamy,andJohnA. Burdine
Baylor College of Medicine and St. Luke's Episcopal-Texas Children's Hospitals, Houston, Texas
by on July 3, 2018. For personal use only. jnm.snmjournals.org Downloaded from

, I―
t'_
DE PUEY, THOMPSON, ALAGARSAMY, AND BURDINE
by 14-cm sheet containing 40 mCi of 241@, whichemits 60-keV gammas. The patient's heel is fittedsnugly into a Plexiglas trough filled with water andplaced between the source and the low-energy, highresolution collimator of the scintillation camera
(Fig. 2) . To prevent rotation and movement, several troughs were constructed to fit heels of variouswidths.
Photon transmission through the immersed heel(I) and then through the trough filled with wateralone (1*) is monitored in a 64 X 64 matrix witheach cell measuring 4.3 X 4.3 mm at the cameraface. An information density of 26,000 counts/cm2over the regionof the calcaneusis requiredon boththe bone and no-bone data matrices in order to maintam the statistical deviation in a single BMI calcu
lation at a value less than 2% ( 1 s.d.) . Our system
currently requires a 10-mm data-collection periodfor each image, resulting in an absorbed radiationdose of 20 mrems to the patient's heel. Using adedicated minicomputer, the natural logarithm ofthe ratio I@@/Iis then computed for each cell and theresults are displayed in a maximum of seven levelson a cathode-ray tube (CRT) as a functional imageofBMI (Fig. 3A).
Scattered radiation and poor resolution (@/8in.)at 60 keV create an apparent zone of decreased BMIoutside the actual bounds of the calcaneus. To eliminate this zone and to correct for variation in imagesize due to long-term instrument drift, a steel platewith holes drilled at fixed points is imaged with eachstudy to determine a detector-to-CRT minificationfactor. The size of the functional image is adjustedby an edge-cutting technique so that the width ofthe image is equal to the minification factor timesthe width of the calcaneus at its narrowest point asdetermined by a lateral roentgenogram of the heel(Fig. 3B) . For each patient the distal 5 cm along
the axis of the calcaneus on the roentgenogram ismultiplied by the minification factor and markedwith the light pen on the functional image. Becausethis area is represented by at least 80 computer cells,small measurement errors have relatively little effecton the BMI averaged over the entire area.
RESULTS
To evaluate this method, a BMI was determinedfor each of 12 cylindrical bone phantoms composedof a uniform mixture of calcium carbonateandtissue-equivalent plastic. The BMI values obtainedwere representative of the range of values encountered in patients and normal control subjects. Thecorrelation coefficient of BMI to actual phantomcalcium content was 0.99 with a significance, p <0.001 (Fig. 4).
COMPRESSED
BONE
WATER ANDSOFT TISSUE
@_____Xb@ Xi -3ID—,
— —I— _ _ _ _
FIG. 1. SimplifiedmodelforBMIdetermination.x. representscombined thicknessof water and soft tissue surrounding bone, andXb i5 thickness of remaining material after all intramedullary com
ponents have been removed. l@ is intensity of incident photonbeam; I iS intensity transmittedthrough bone, soft tissueand water combined; and l@ is intensity through soft tissue and wateralone.
actual bone density. The bone mineral per square
centimeter of projected surface is proportional to thenatural logarithm of the ratio@ which we defineas the bone mineral index (BMI).
BMI=ln'j—= (,@b—i@)Xb.
The calcaneus is used routinely for the bone mmera! measurement (5,6) . The photon source is a 10-
J
C£0 ----.4
FIG.2. Tomeasurebonedensity,heelis fittedsnuglyintonarrow water-filled trough and placed between high-resolutioncollimator (left) and 40-mCi @Amsource (right).
892 JOURNAL OF NUCLEARMEDICINE
•1 r- :c;@
by on July 3, 2018. For personal use only. jnm.snmjournals.org Downloaded from

DIAGNOSTIC NUCLEAR MEDICINE
Sixteen repeated determinations over a 1-weekperiod using a representative phantom yielded anaverage coefficient of variation of 2. 1% with a maximum variation of 2.8% . Six BMI determinations atmonthly intervals on each of four healthy subjectsyielded an average coefficient of variation of 2.4%with a maximum variation of 2.9%.
CASE REPORTS
The following cases illustrate the clinical application of this technique.
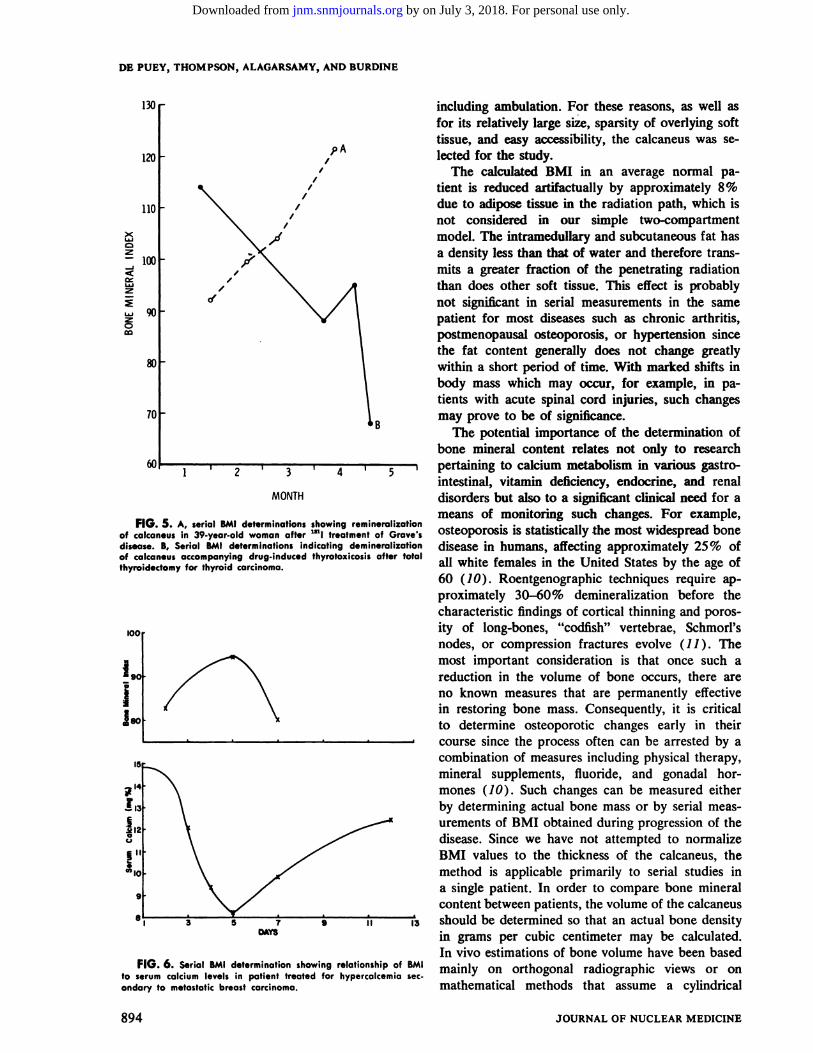
Case 1. A 39-year-old woman had an 8-month history of weight loss, heat intolerance, and palpitations. A diagnosis of diffuse toxic goiter (Grave'sdisease) was made based on physical examinationand laboratory testing. Following 131! therapy, sheimproved clinically with return to an ideal bodyweight. Serial BMI determinations for a 3-monthperiod revealed progressive bone remineralization(Fig. 5).
Case 2. A 25-year-old woman underwent a totalthyroidectomy and 131! ablation for thyroid carcinoma 3 months prior to the initiation of our study.At that time she was placed on a balanced combination of thyroxine and triiodothyronine, equivalentto 3 grains of thyroid daily. At the time of her firstbone mineral determination, she was clinically euthyroid. Over the subsequent 4 months, however, shedeveloped progressive weight loss, tremor, and palpitations. Clinical re-evaluation at that time indicatedthat she had become thyrotoxic, necessitating a reduction in the dose of thyroid replacement. Serialbone mineral determinations revealed progressivedemineralization parallel with the development ofher hyperthyroid state (Fig. 5).
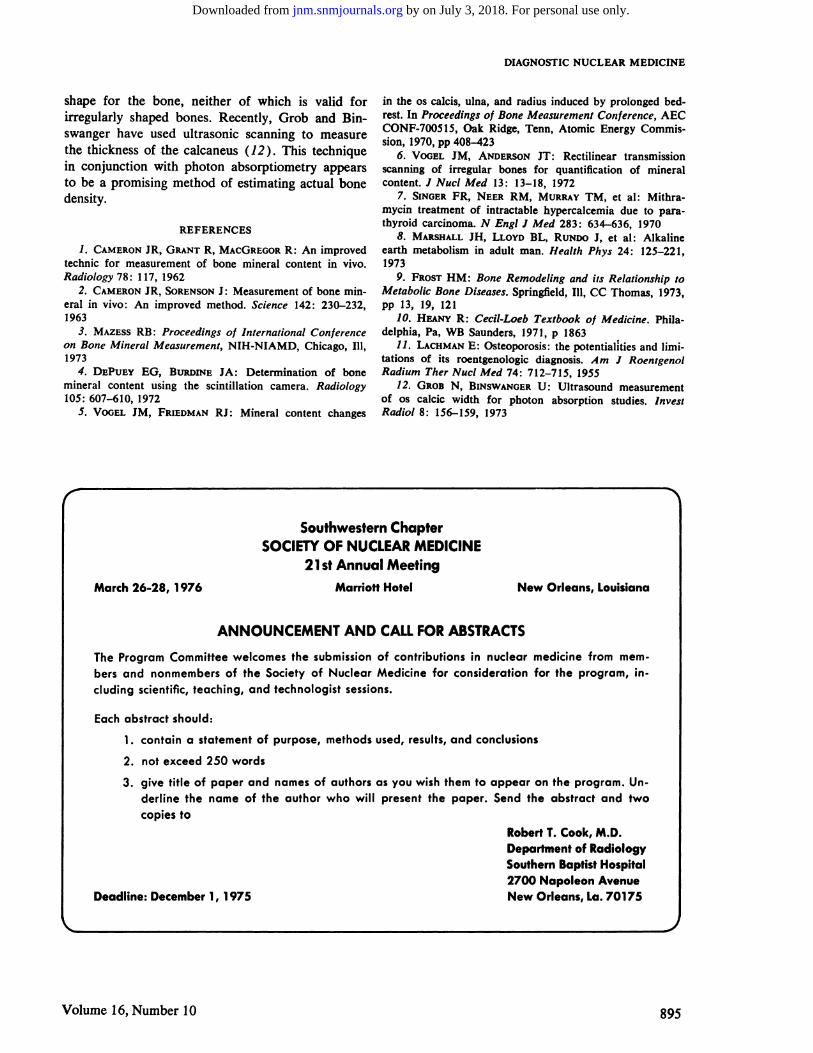
Case 3. A 59-year-old woman with documentedmetastatic breast carcinoma had constipation, ab
dominal pain, and progressive disorientation. Admission laboratory data revealed a serum calcium of14.8% and phosphorous of 4.5 mg% . After receiving 2 mg mithramycin intravenously, the serum cal
cium fell to 8.2 mg% with a subsequent rapid returnto hypercalcemiclevels.Singer,et al postulatethatmithramycin may act in part to inhibit bone resorption (7). A rise in BMI was demonstrated corresponding to the transient decrease in serum calciumlevel (Fig. 6).
DISCUSSION
Because of the large trabecular surface exposedto remodeling activity, cancellous bone is three tofour times more susceptible to changes in mineralization than cortical bone (8,9). Mineralization ofthe calcaneus is affected not only by normal metabolic processes and disease but also by stress-bearing,
—I
FIG.3. (A)Lateralroentgenogramof heel.(B)Correspondingfunctional image of calcaneus obtained from computer display.
S
S
S
5/5,
5/
VS
S
S
,@
l3t
I.
1m4
a
I B 9 tO N 12 13 14ColciwnContint
FIG.4. CorrelationofmeasuredBMIwithpercentcalciumcontent (by weight) in phantoms.
Volume 16, Number 10 893
by on July 3, 2018. For personal use only. jnm.snmjournals.org Downloaded from
II
DE PUEY, THOMPSON,ALAGARSAMY,ANDBURDINE
DAYS
z
z
z0
130@ including ambulation. For these reasons, as well asfor its relatively large size, sparsity of overlying softtissue, and easy accessibility, the calcaneus was se
120@ IP A lected for the study.I The calculated BMI in an average normal pa
,I tient is reduced artifactually by approximately 8%
110@ I due to adipose tissue in the radiation path, which isnot considered in our simple two-compartmentmodeL The intramedullary and subcutaneous fat has
100@ a density less than that of water and therefore transmits a greater fraction of the penetrating radiationthan does other soft tissue. This effect is probably
@ not significant in serial measurements in the same90 patient for most diseases such as chronic arthritis,
postmenopausal osteoporosis, or hypertension sincethe fat content generally does not change greatly
80@ within a short period of time. With marked shifts inbody mass which may occur, for example, in patients with acute spinal cord injuries, such changes
70@ may prove to be of significance.The potential importance of the determination of
bone mineral content relates not only to research6C@ , 2 ‘ 3 ‘ 4 1@ 1 pertaining to calcium metabolism in various gastro
intestinal, vitamin deficiency, endocrine, and renalMONTH disorders but also to a significant clinical need for a
means of monitoring such changes. For example,FIG.5. A,serialBMIdeterminationsshowingremineralization . . . .
of calcaneus in 39-year-old woman after @ltreatment of Grave's osteoporOSiS is statistically the most widespread bonedisease. B, Serial BMI determinations indicating demineralization disease in humans, affecting approximately 25% ofof calcaneus accompanying drug-induced thyrotoxicosisafter total . .thyroidectomyfor thyroid carcinoma. a―white females in the United States by the age of
60 (10) . Roentgenographic techniques require approximately 30—60% demineralization before thecharacteristic findings of cortical thinning and poros
100 ity of long-bones, “codfish― vertebrae, Schmorl's
nodes, or compression fractures evolve (1 1 ) . Themost important consideration is that once such a
@ 90 reduction in the volume of bone occurs, there are
.; no known measures that are permanently effectivein restoring bone mass. Consequently, it is critical
Ipo to determine osteoporotic changes early in their. & . . - . course since the process often can be arrested by a
combination of measures including physical therapy,mineral supplements, fluoride, and gonadal hormones (10) . Such changes can be measured eitherby determining actual bone mass or by serial messurements of BMI obtained during progression of thedisease. Since we have not attempted to normalizeBMI values to the thickness of the calcaneus, themethod is applicableprimarily to serial studiesina single patient. In order to compare bone mineralcontent betweenpatients, the volume of the calcaneusshould be determined so that an actual bone densityin grams per cubic centimeter may be calculated.In vivo estimations of bone volume have been based
FIG.6. SerialBMIdeterminationshowingrelationship?@BMI mainly on orthogonal radiographicviews or onto serum calcium levels in patient treated for hypercalcemia secondary to metastatic breast carcinoma. mathematical methods that assume a cylmdncal
894 JOURNAL OF NUCLEARMEDICINE
by on July 3, 2018. For personal use only. jnm.snmjournals.org Downloaded from
DIAGNOSTIC NUCLEAR MEDICINE
shape for the bone, neither of which is valid forirregularly shaped bones. Recently, Grob and Binswanger have used ultrasonic scanning to measurethe thickness of the calcaneus (12) . This techniquein conjunction with photon absorptiometry appearsto be a promising method of estimating actual bonedensity.
REFERENCES
1. CAMERONJR, GRANTR, MACGREGORR: An improvedtechnic for measurement of bone mineral content in vivo.Radiology78:117,1962
2. CAMERONJR, SORENSONJ: Measurementof bone mmeral in vivo: An improved method. Science 142: 230—232,1963
3. MAZESSRB: Proceedingsof International Conferenceon Bone Mineral Measurement, NIH-NIAMD, Chicago, Ill,1973
4. DEPUEYEG, BURDINEJA: Determinationof bonemineral content using the scintillation camera. Radiology105:607—610,1972
5. VOGEL JM, FRIEDMANRJ: Mineral content changes
in the os calcis, ulna, and radius induced by prolonged bedrest. In Proceedingsof BoneMeasurementConference,AECCONF-700515, Oak Ridge, Tenn, Atomic Energy Commission, 1970, pp 408—423
6. VOGELJM, ANDERSONIT: Rectilinear transmissionscanning of irregular bones for quantification of mineralContent. I Nuci Med 13: 13—18,1972
7. SINGERFR, NEERRM, MURRAYTM, et al: Mithramycin treatment of intractable hypercalcemia due to pamthyroid carcinoma. N Engl I Med 283 : 634—636,1970
8. MARSHALLJH, LLOYD BL, RUNDOJ, et al: Alkalineearth metabolism in adult man. Health Phys 24: 125—221,1973
9. FROSTHM : Bone Remodeling and its Relationship toMetabolic Bone Diseases. Springfield, Ill, CC Thomas, 1973,pp 13,19,121
10. Hp.@Ny R: Cecil-Loeb Textbook of Medicine. Philadelphia, Pa, WB Saunders, 1971, p 1863
11. LACHMANE: Osteoporosis: the potentialities and limitations of its roentgenologic diagnosis. Am I RoentgenolRadium TherNuclMed 74:712—715,1955
12. GROB N, BINSWANGERU: Ultrasound measurementof os calcic width for photon absorption studies. InvestRadio! 8: 156—159,1973
Volume 16, Number 10 895
Southwestern ChapterSOCIETYOF NUCLEARMEDICINE
21st Annual Meeting
March 26-28, 1976 Marriott Hotel New Orleans, Louisiana
ANNOUNCEMENT AND CALL FOR ABSTRACTS
The ProgramCommitteewelcomesthe submissionof contributions in nuclear medicine from members and nonmembers of the Society of Nuclear Medicine for consideration for the program, in
cluding scientific, teaching, and technologist sessions.
Each abstract should:
1. contain a statement of purpose, methods used, results, and conclusions
2. not exceed250 words
3. give title of paper and namesof authorsas you wish themto appear on the program. Underline the name of the author who will present the paper. Send the abstract and twocopiesto
RobertT. Cook, M.D.Department of RadiologySouthernBaptistHospital2700 Napoleon Avenue
Deadline: December1, 1975 New Orleans, La. 70175
by on July 3, 2018. For personal use only. jnm.snmjournals.org Downloaded from
1975;16:891-895.J Nucl Med. E. Gordon DePuey, Wayne L. Thompson, Veerasamy Alagarsamy and John A. Burdine Bone Mineral Content Determined by Functional Imaging
http://jnm.snmjournals.org/content/16/10/891This article and updated information are available at:
http://jnm.snmjournals.org/site/subscriptions/online.xhtml
Information about subscriptions to JNM can be found at:
http://jnm.snmjournals.org/site/misc/permission.xhtmlInformation about reproducing figures, tables, or other portions of this article can be found online at:
(Print ISSN: 0161-5505, Online ISSN: 2159-662X)1850 Samuel Morse Drive, Reston, VA 20190.SNMMI | Society of Nuclear Medicine and Molecular Imaging
is published monthly.The Journal of Nuclear Medicine
© Copyright 1975 SNMMI; all rights reserved.
by on July 3, 2018. For personal use only. jnm.snmjournals.org Downloaded from