bphc enrichment series for grantees: improving cervical cancer screening in health centers through...
TRANSCRIPT

BPHC Enrichment Series for Grantees:
Improving Cervical Cancer Screening in Health Centers through PCMH
Thursday, January 24, 20132:00-3:30pm ET

2
Cervical Cancer Screening & PCMHLearning Objectives
• Understand the epidemiological basis of cervical cancer and cervical cancer screening
• Identify barriers to improving cervical cancer screening rates
• Analyze how to overcome screening barriers using PCMH
• Describe successful grantee screening programs
• Identify additional TA and resources on PCMH and cervical cancer screening
Widening Perspectives to Improve Outcomes

3
Agenda in BriefWelcome
Seiji Hayashi, HRSA
Profile of Cervical Cancer & Cervical Cancer Screening
Jacqueline W. Miller, CDC
Challenges to Improving Cervical Cancer Screening Rates
Nina Brown, HRSA
Using PCMH to Improve Cervical Cancer Screening Rates
Preeta Chidambaran, HRSA
Successful Health Center Cervical Cancer Screening Programs
Rise Phillips, T.H.E. Clinic, Inc.
Chad Hess, Pueblo Community Health Center

Cervical Cancer Overview
CAPT Jacqueline Miller, MD, FACSUS Public Health Service
Medical Director, National Breast and Cervical Cancer Early Detection ProgramProgram Services Branch
National Center for Chronic Disease Prevention and Health Promotion
Division of Cancer Prevention and Control

Cervical Cancer Burden
In 2009,12,357 new cervical cancer cases (7.9/100,000)*3,909 cervical cancer deaths (2.3/100,000)*Over $2 billion per year is spent in the United States on the treatment of cervical cancerNumber of new cases and deaths decreasing
U.S. Cancer Statistics Working Group. United States Cancer Statistics: 1999–2008 Incidence and Mortality Web-based Report. Atlanta: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention and National Cancer Institute; 2012. Available at: www.cdc.gov/uscs.

Trend in Cervical Cancer Incidence and Mortality Rates*, 1975-2006
*Incidence source: Surveillance Epidemiology, and End Results Program ( 9 areas) Mortality source: US Mortality Files, National Center for Health Statistics, CDC Rates are per 100,000 and are age-adjusted to the 2000 US Std Population (19 age groups - Census P25-1130).
'76 '78 '80 '82 '84 '86 '88 '90 '92 '94 '96 '98 '00 '02 '04 '060
2
4
6
8
10
12
14
16
Year
Incidence
Death

Cervical Cancer Incidence Rate by Race, 2009
Source: U.S. Cancer Statistics Available at: http://www.cdc.gov/uscs.

Cervical Cancer Incidence Rate by State, 2009
Source: U.S. Cancer Statistics Available at: http://www.cdc.gov/uscs.

Cervical Cancer Mortality Rate by State, 2009
Source: US Cancer Statistics Available at http://www.cdc.gov/uscs

Cervical Cancer Screening
Two goals Prevention Early detection
Precancerous lesions can be treated before developing into invasive disease.
Main reason for decline in cervical cancer incidence and mortality.

Cervical Cancer Survival by StageStage 5-year survival rate
0 93%
IA 93%
IB 80%
IIA 63%
IIB 58%
IIIA 35%
IIIB 32%
IVA 16%
IVB 15%
Source: National Cancer Database

USPSTF Screening Guidelines
Recommends screening in women ages 21 to 65 years with cytology (Pap smear) every 3 years or, for women ages 30 to 65 years who want to lengthen the screening interval, screening with a combination of cytology and human papillomavirus (HPV) testing every 5 years. Grade: A Recommendation.

USPSTF Screening Guidelines
Recommends against screening in women younger than age 21 years. Grade: D Recommendation
Recommends against screening in women older than age 65 years who have had adequate prior screening and are not at high risk . Grade: D Recommendation

USPSTF Screening Guidelines Recommends against screening in women
who have had a hysterectomy with removal of the cervix and who do not have a history of a high-grade precancerous lesion or cervical cancer. Grade: D Recommendation
Recommends against screening with HPV testing alone or in combination with cytology in women younger than age 30 years. Grade: D Recommendation

Screening Guidelines
Consistent recommendations from USPSTF, ACS, and ACOG
Only for average risk women

U.S. Cervical Cancer Screening Rates, 2010
Data source: Behavioral Risk Factor Surveillance System

Cervical Cancer Screening Trend
Data source: National Health Interview SurveyHealthy People 2020 goal is 93%.
HP2020 goal

Cervical Cancer Screening by Demographics, 2010
Characteristics % 95% CI
Race
White 83.4 82.3-84.5
Black 85.0 82.8-87.0
American Indian/Alaska Native 78.7 65.9-87.5
Asian 75.4 71.1-79.3
Ethnicity
Non-Hispanic 83.8 82.6-84.9
Hispanic 78.7 76.3-80.8
US residence
Born 85.0 83.9-86.0
<10 years 67.1 62.3-71.5
10 years or more 77.8 74.6-80.7
CDC. Cancer Screening. MMWR 2012;61:41-45. Data source: National Health Interview Survey

Cervical Cancer Screening by Demographics, 2010
Characteristics % 95% CI
Education
Less than high school 69.4 66.1-72.5
High school graduate 77.7 75.4-79.9
Some college 85.3 83.6-86.8
College graduate 89.0 87.5-90.3
Usual source of care
No 64.9 617-67.9
Yes 86.4 85.4-87.4
Health Insurance
Private 88.7 87.7-89.7
Public 81.9 79.1-84.4
None 63.8 61.1-66.4
CDC. Cancer Screening. MMWR 2012;61:41-45. Data source: National Health Interview Survey

Human Papilloma Virus (HPV)
• Majority of cervical cancer associated with HPV
• High-risk HPV DNA testing added to screening regimen
• No role for low-risk HPV DNA testing• HPV vaccine may decrease disease burden
further, but results too early• Continue screening despite vaccination status• Hopefully begin to monitor national testing
rates

Benefits of Screening
• Usually no early signs• May have vaginal bleeding/discharge,
pelvic pain, or painful intercourse• Cervical cancer is easily detectable and
highly treatable• Prognosis depends of stage of tumor and
patient’s overall health• Screening to look for abnormal cells early
leads to better prognosis

Improving Cervical Cancer Screening
in Health Centers through PCMH
Thursday, January 24, 20132:00-3:30pm ET
BPHC Grantee TA call

23
Case Study – Undiagnosed Vaginal Bleeding
The patient is a 34-year-old gravida 3, para 3 woman with a 2-year history of increasingly profuse vaginal bleeding. Over the past two years, the patient had been placed on oral contraceptives, but these had not stanched the bleeding. The patient reported having a Pap smear approximately 18 months earlier, read as "unsatisfactory, obscured by blood." However, she had not had a follow-up study.
Source: http://www.webmm.ahrq.gov/

24
Case Study – Undiagnosed Vaginal Bleeding
A gynecologist had seen her about 6 months earlier, and told her she needed a hysteroscopy and a dilation and curettage (D&C). However, he explained that he did not accept Medicaid, which was her source of health insurance. Her follow-up remained sporadic, and her bleeding continued—profuse enough that she required hospitalization for transfusions twice in the preceding 2 months.
Source: http://www.webmm.ahrq.gov/

25
Case Study – Undiagnosed Vaginal Bleeding
Her bleeding increased again, and she presented to the emergency department (ED). Physical exam revealed that the patient had an extremely friable exophytic cervical lesion, which was biopsied and confirmed to be invasive cervical cancer. Upon evaluation by a gynecologic-oncologist, she was found to be Stage IIB cancer. After undergoing radiation therapy and chemotherapy, she still has persistent disease. Her prognosis is currently guarded. Her oncologist believes that her delayed diagnosis profoundly affected her prognosis.
Source: http://www.webmm.ahrq.gov/

26
Cervical Cancer Related Malpractice Concerns/Issues in Health Centers
• Over the past 10 years, the majority (58%) of incidents involving cervical cancer have involved the following:• a failure to diagnose • or delay in diagnosis
• Significant payout per closed event
Source: FTCA Claims Data

27
Cervical Cancer Screening Trends and Goals in Health Centers

28
Patient Survey (2009)
Cancer Screening All Groups
NH Whites
NH Blacks
Hispanic/Latino
Women 21 to 70 years Had Pap Test in past 3 years
85.3 79.6 87.6 87.9
National Health Interview Survey (2010)
Women 24-64 years Had Pap Test in past 3 years
83.5 82.7 85.7 84.9
Cancer Screening Outcomes among Health Cancer Screening Outcomes among Health Center PatientsCenter Patients
Source: 2009 Patient Survey and 2010 NHIS

29
BPHC’s Efforts to Support Cervical Cancer Screening
• 811 health centers funded
• $44 million dollars: $55,000 per health center
• Focus on PCMH transformation as a tool to improve clinical quality
• Cervical Cancer Screening Improvement

30
Cervical Cancer Clinical Measure
• Current Measure
• Numerator: Number of female patients 24-64 years of age receiving one or more Pap tests during the measurement year or during the two years prior to the measurement year, among those women included in the denominator
• Denominator (Universe): Number of female patients 24-64 years of age as of December 31 of the measurement year who were seen for a medical encounter at least once during the measurement year and were first seen by the grantee before their 65th birthday
30

31
Cervical Cancer Clinical Measure• Cervical Cancer Clinical Measure• Modified for 2013
• Whereas the current measure counts as compliant women age 24 to 64 years with 3 year intervals between screenings, the revision allows 5 year intervals for women age 30 to 64 years with a Pap test accompanied by an HPV test. This change aligns with the 2012 recommendation of the U.S Preventive Services Task Force.

32
Qualitative Study of PCMH Supplemental 2012
Key Barriers to PCMH Transformation to Improve Cervical Cancer Screening
32

33
Patient Level Barriers• Access to care
• Patient Demographics (SES factors) • Geographic Issues• Patient Engagement• Cultural Competency *
• Workflow Issues • Type of providers• Care coordination between multiple providers
• Financial Barriers
33

34
Provider Level Barriers
• Workflow Issues• Disconnect between QI staff and clinicians• Significant gaps between patients identified by registry
and scheduling appointments
• Training and Technical Assistance• Turnover of staff or high growth rate in staff• Software training• Best Practice Guidelines including recent changes to
screening recommendations
34

35
System Level Barriers
• Clinical Process and workflow issues• EHR
• Decision Support systems • Technical and data integrity issues
• Resources for outreach and education programs
35
36
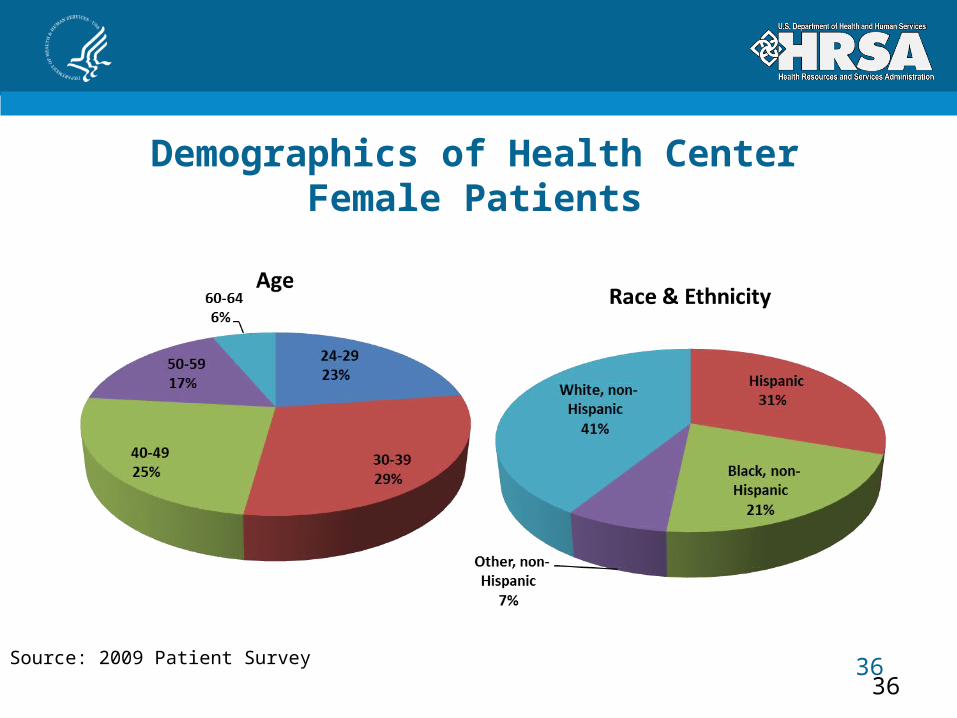
Demographics of Health Center Female Patients
Source: 2009 Patient Survey
36

37
Barriers Related to Cultural Competency
• Need for interpretive services
• Need for special outreach programs
• Need for multilingual patient education materials
37

38
Qualitative Study of PCMH Supplemental 2012
Solutions to PCMH Transformation to Improve Cervical Cancer Screening
38

39
Solutions Targeting Patients• Workflow
• Appropriate matching of patients to providers for first visit• EHR: Patient registries, automatic prompts, Follow up
Reminders, Patient Portal• Patient Education Materials
39
Source: FY2012 PCMH Supplemental Application Qualitative Review

40
Solutions Targeting Patients
• Outreach• Follow up on referrals, Batch mailings, Appointment
Reminders• Advertisement Media, Women’s health fair
• Finance• Discounted fee for screening (PAP tests, lab fees)• Incentive gift cards, One time cash rewards• Use funds for out of state patients who don’t qualify
for in state programs

41
Patient Level Solutions Corresponding NCQA PCMH Domain
Workflow
EHR: Patient Registries PCMH 3: Plan & Manage Care•Element 3b: Identify High Risk Patients
Patient Portals PCMH 1: Enhance Access & Continuity•Element 1c: Electronic Access
Automatic Prompts PCMH 2: Identify & Manage Patient Populations•Element 2d: Use Data for Population Management
Patient Education Materials PCMH 4: Provide Self-Care Support & Community Resources
Outreach
Follow up on referrals PCMH 5: Track & Coordinate Care•Element 5b: Referral tracking & follow-up
Solutions Targeting Patients
Source: FY2012 PCMH Supplemental Application Qualitative Review

42
Solutions Targeting Providers
• Workflow• Pre visit planning• Standing orders• Peer review, quarterly data reports
• Access to care• Increase clinic hours, walk ins, bundling approach• Hiring dedicated staff for care coordination, referral follow up • Additional staff resources
• Training• Evidence based guidelines, PCMH, Software, Lab protocols
• Outreach Efforts
42
Source: FY2012 PCMH Supplemental Application Qualitative Review

43
Provider Level Solutions Corresponding NCQA PCMH Domain
Workflow
Pre-Visit Planning PCMH 3: Plan & Manage Care•Element 3b: Identify High Risk Patients
Quarterly Data Reports PCMH 2: Identify & Manage Patient Populations•Element 2d: Use Data for Population Management
Access to Care
Increase Clinic Hours, Walk-Ins PCMH 1: Enhance Access & Continuity•Element 1b: After Hours Access•Element 1a: Access During Office Hours
Hiring Dedicated Staff for Care Coordination
PCMH 1: Enhance Access & Continuity•Element 1g: Practice TeamPCMH 3: Plan & Manage Care•Element 3c: Care Management
Solutions Targeting Providers
Source: FY2012 PCMH Supplemental Application Qualitative Review

44
System Based Solutions• Organizational Policy and Procedures
• Identifying cervical cancer screening measure as a Health Center goal
• Leadership commitment to internal policy changes
• Quality Improvement QI• Identifying quality gaps• Pursuing PCMH/ Accreditation • Participating in BPHC quality initiatives
• HIT• EHR system (registries, educational resources, decision support
system)
• Training 44
Source: FY2012 PCMH Supplemental Application Qualitative Review

45
Systems Based Solutions Corresponding NCQA PCMH Domain
Organizational Policy and Procedures
Cervical Cancer Screening as a Health Center Goal
PCMH 6: Measure & Improve Performance•Element 6c: Implement Continuous Quality Improvement
Quality Improvement
Identify Quality Gaps PCMH 6: Measure & Improve Performance•Element 6c: Implement Continuous Quality Improvement•Element 6d: Demonstrate Continuous Quality Improvement
Health Information Technology (HIT)
EHR System (registries, educational resources, decision support system)
PCMH 6: Measure & Improve Performance•Element 6g: Use Certified EHR Technology
Systems Based Solutions
Source: FY2012 PCMH Supplemental Application Qualitative Review

46
Solutions Related to Cultural Competency*
• Multi lingual patient education materials
• Interpretive services for appointments and front desk
• Multi lingual patient education classes
• Culturally competent events ex: Hmong Tea Ceremony
• Training staff on cultural competency
* Corresponding NCQA PCMH Domain
PCMH 1: Enhance Access and Continuity- Element 1f: Culturally and Linguistically Appropriate Services
PCMH 2: Identify and Manage patient Populations - Element 2a: Patient Information
46
Source: FY2012 PCMH Supplemental Application Qualitative Review
47
Case Study – Undiagnosed Vaginal Bleeding
The patient is a 34-year-old (Automatic prompt for preventive
care service- PAP) gravida 3, para 3 woman with a 2-year history of increasingly profuse vaginal bleeding. Over the past two years, the patient had been placed on oral contraceptives, but these had not stanched the bleeding. The patient reported having a Pap smear approximately 18 months earlier, read as "unsatisfactory, obscured by blood." However, she had not had a follow-up study.(Protocol for appropriate follow up on lab result)
47
Source: http://www.webmm.ahrq.gov/

48
Case Study – Undiagnosed Vaginal Bleeding
A gynecologist had seen her about 6 months earlier,(Missed opportunity to repeat PAP, better care coordination and
documentation between providers) and told her she needed a hysteroscopy and a dilation and curettage (D&C).
However, he explained that he did not accept Medicaid, which was her source of health insurance. Her follow-up remained sporadic, (Adequate follow up on referral) and her bleeding continued—profuse enough that she required hospitalization for transfusions twice in the preceding 2 months. (Consolidated records from multiple providers)
48
Source: http://www.webmm.ahrq.gov/

49
Case Study – Undiagnosed Vaginal Bleeding
Her bleeding increased again, and she presented to the emergency department (ED). Physical exam revealed that the patient had an extremely friable exophytic cervical lesion, which was biopsied and confirmed to be invasive cervical cancer.
Upon evaluation by a gynecologic-oncologist, she was found to be Stage IIB cancer. After undergoing radiation therapy and chemotherapy, she still has persistent disease.
Her prognosis is currently guarded. Her oncologist believes that her delayed diagnosis profoundly affected her prognosis.
49
Source: http://www.webmm.ahrq.gov/

50
FY12 Supplemental Important Dates and Reminders
• Survey Submission for at least 1 site or Site Visit Scheduling• June 1, 2013
• Interim Report Due: Including proof of submission or schedules site visit• June 3, 2013
• Achieve PCMH Recognition• September 30, 2013
• Final Reports Due: Including Proof of PCMH Recognition• November 1, 2013
50

CHCs and CDC Working Together to Improve Outcomes
CAPT Jacqueline Miller, MD, FACSUS Public Health Service
Medical Director, National Breast and Cervical Cancer Early Detection Program
Program Services Branch
National Center for Chronic Disease Prevention and Health Promotion
Division of Cancer Prevention and Control

CHC’s and CDC’s National Breast and Cervical Cancer Early Detection
Program
• NBCCEDP target population are never screened and rarely screened women
• 60% of invasive cervical cancer occurs in this population
• Contract with many CHC’s across the U.S. to provide clinical services

CHC’s and CDC’s National Breast and Cervical Cancer Early Detection
Program
• NBCCEDP eligible population– Low income (< 250% FPL)– Women aged 21 to 64 years– Uninsured or underinsured

CHC’s and CDC’s National Breast and Cervical Cancer Early Detection
Program
• Outreach• In-reach• Public education• Patient navigation• Case management

CHC’s and CDC’s National Breast and Cervical Cancer Early Detection
Program
• Quality assessment and quality improvement
• Using data to monitor quality indicators• Completeness of care
– 90% of abnormal screens must get final diagnosis
• Timeliness of care– 90 days for final diagnosis– 60 days to begin treatment

For more information please contact Centers for Disease Control and Prevention
1600 Clifton Road NE, Atlanta, GA 30333
Telephone: 1-800-CDC-INFO (232-4636)/TTY: 1-888-232-6348
E-mail: [email protected] Web: http://www.cdc.gov
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
National Center for Chronic Disease Prevention and Health Promotion
Division of Cancer Prevention and Control
Thank [email protected]

Cervical Cancer Screening for Success: T.H.E. (To Help
Everyone) Clinic
Risë K. Phillips, MPH, MBAPresident and CEOT.H.E. Clinic, Inc.

58
T.H.E. Clinic

59
Relevant Facts concerning T.H.E and its Patient Population
• T.H.E. (To Help Everyone) Clinic was founded in 1974 as a women’s clinic
• Expanded to serve families within a decade• Serves over 12,500 patients with over
36,000 visits in six sites throughout South and Southwest Los Angeles
• Staff speak over 12 languages

60
T.H.E. Patient Demographics

61
T.H.E. Patient Demographics

62
Target Patient Demographics (continued)
• Female population ages 21 to 64 composed of N=5,752 representing 47.5% of total clinic population

63
T.H.E. Clinic Female Population Ages 21 to 64 as of Dec. 31, 2011
Age Interval Number Percent
21-24 592 10.3
25-29 771 13.4
30-34 616 10.7
35-39 564 9.8
40-44 655 11.4
45-49 739 12.8
50-54 779 13.5
55-59 590 10.3
60-64 446 7.8
64
T.H.E. Clinic Cervical Cancer Risk Factors
• High rates of sexually transmitted infection (STIs including HPV and HIV)
• Lack of regular Pap tests
• Weakened immune systems
• Age over 40 – represent 55.8% of total female patient population

65
T.H.E. Clinic Cervical Cancer Risk Factors (continued)
• Sexual history – many partners or partner with many partners
• High percentage of cigarette smokers
• High percentage using birth control pills for 5 or more years

66
Cervical Cancer Screening Challenges
• Women without a regular primary care provider and medical home less likely to have reported a recent Pap test
• Transient populations
-- Homeless, Hard-to-reach
• Patients not knowing or understanding their risk for cervical cancer
67
Screening Challenges (continued)
• Cultural and language barriers to cervical cancer screening
-- Mistrust of medical care providers
-- Lack of culturally sensitive screening & treatment environments
-- Modesty, fatalism, cultural prohibitions against examinations by male providers

68
Overcoming Cervical Cancer Screening Challenges
• Developed a patient-centered Women’s Health practice with a cervical cancer screening initiative
-- Identify all eligible female patients between ages 21 to 64
-- Assess pap test records via electronic medical records (EMR)

69
Overcoming Cervical Cancer Screening Challenges (cont.)
• Formed Women’s Health Teams with Health Coaches to reinforce positive sexual health and behavioral goals by patients
-- Assess and create screening plan for all target female patients

70
Overcoming Cervical Cancer Screening Challenges (cont.)
• Women’s Health Team
-- Report measures and outcomes regularly during medical quality improvement meetings
-- Discuss ways to enhance the patient experience and how to communicate difficult test results

71
Overcoming Cervical Cancer Screening Challenges (cont.)
• Performance measures generated through EMR and patient tracking systems
-- Team benefits by being able to adjust strategies to impact and enhance the patient experience at all sites

72
Overcoming Cervical Cancer Screening Challenges (cont.)
• Non-clinical activities to support patient-centered outreach
-- Patients receive “Happy Birthday” telephone calls with a reminder to come to the clinic for their annual exam
-- Social media & other community outreach
-- Patient satisfaction surveys

73
How Quality Incentives from BPHC May Have Been Used to Help Achieve Results
• Behavioral change prevention strategies discussed with patients
-- Avoidance of STIs (including HPV) by modifying sexual behavior
-- Avoidance of cigarette smoking
-- Better family planning

74
How Quality Incentives from BPHC May Have Been Used to Help Achieve Results
(continued)
• Risks and benefits of cervical cancer screening discussed with each individual patient-- individual risk
-- fear of diagnosis
-- harm from screenings/treatments
-- cultural influences
-- values
-- perceived barriers to screening

75
Results/Data of Screenings
• 85.7% or higher of eligible patients ages 21 to 64 received a Pap Test
-- 2% had abnormal cervical findings• 2012/2013 goals set for 90% or higher
screening goals• Enhanced communication between patient and
Women’s Health Team leads to better patient experience

76
Lessons Learned
• Know your patient population and tailor patient-centered screening strategies
• Develop Team approach with Health Coaches to reinforce patient behaviors
• Analyze patient outcome data regularly and change strategies to enhance quality, patient experience & satisfaction

77
Successful Private/Public Partnerships Helping Cervical
Cancer Screening Program
• Partnership with LA County Health Services for referrals/specialty care
• Shared clinical best practices within the Community Clinic Association of LA County

78
Contact Information
Ms. Risë K. Phillips, MPH, MBA
President and CEO
(213)730-1920 ext. 3053
www.theclinicinc.org

Cervical Cancer Screening
Chad Hess PA-C, RN, MBADirector of Nursing Services

80

81
About Pueblo Community Health Center
Since 1983, Pueblo Community Health Center’s mission has been to provide primary health care to those in need.
•PCHC served 23,104 individual patients with 106,927 medical, dental and mental health visits in 2011
•PCHC has grown by 45% since 2003

82
About Pueblo Community Health Center (cont’d)
• Uninsured = 33%; Medicaid = 43%; Public/Private Insurance = 9%; and Medicare = 15%
• Nearly 40% of Pueblo County is Latino/a• Over 60% of PCHC’s patients represent ethnic
minority populations

83
Cervical Cancer Screening Outreach

84
Cervical Cancer Screening Outreach-In-Reach and Challenges-2000
• Send Patient Reminder Card• Provider\MA to identify patients (tickler system) • Free Pregnancy Tests• Provision of OB & GYN Services • No Electronic Data base

85
Patient Focus Group(Barrier’s)
• Provider-Gender Preference• Appointment Availability • Patient’s not assigned to a PCP• Evening Clinics (reserved for Acute Care Only)• Patient Perceived Need of Service• Patient Concern of Cost For Screening • Lack of Specialty Care if abnormality is found

86
Cervical Cancer Screening Outreach
• Outreach- modeled from Well Women’s Connection program (WWC)
• Designed a Cancer Screening Clinic• Provide Patient Reminders• Provide Preventative Health Education• Schedule Appointments• Monitor Compliance• Coordinates Patient Care• Patient Advocate

87
Cervical Cancer Screening Outreach
• Bilingual Case Managers • Cultural Sensitivity Competence• Patient’s Word of Mouth • Radio PSA’s –Women Cancer Screening
Clinics• Community Health Fair Participation• Organization’s Web Page (Women’s Cancer
Screening)• Close Collaboration with Community Partners
88
Cervical Cancer Screening In-reach by Medical & Nursing Staff
• Patient emphasis on Preventative Health • Health Care Maintenance Flow Sheet• Provide Updates for Nursing Staff • PCP-Continuity of Medical Care• Acute Care Visit Opportunities• Nurse Visit Opportunities

89
Cervical Cancer Screening Rates
• 31% of women age 40-64 are screened annually
• 29% of women age 21-39 are screened annually
• 13% abnormal findings

90
Where Screening Takes Place
• 40% -Women’s Cancer Screening Clinic
• 55%-Primary Care Provider
• 5%-Evening Clinic Option
* Patient Preference

91
Cervical Cancer Screening Challenges
• Identify Patients who are currently not following ACOG Screening Guidelines
• Medical and Nursing Staff-ACOG Guidelines
• Patient’s ability to pay for Screening if not eligible for WWC
• Patient compliance with scheduled appointments
92
Cervical Cancer Screening Challenges
• Patient Perspective on Preventative Health
• HPV vaccine-uninsured
• Myths and taboo of why Cervical Cancer Screening is necessary
• Database inefficiencies in support of case management

93
How Cervical Cancer Screening Challenges Were Overcome
• Patient education of current ACOG screening recommendations
• Provide Medical and Nursing Staff updates of ACOG screening recommendations
• Quality Improvement Activities
• Medical Peer Review

94
How Quality Incentives from BPHC May Have Been Used to Help Achieve Results
• Develop Cervical Cancer Screening database
• Plan to duplicate within E HR
• Generate Patient Compliance Reports
• Provider\Nurse-Patient Chart Flag
• Cost of Service Information
• HPV Vaccine Subsidy Program

95
Cervical Cancer Screening Rates
• 87% of Women between 21-39 are screened every 3 yrs if previous Pap Smear\HPV has been nl\neg.
• 91% of Women between 40-64 are screened every 3 yrs if previous Pap Smear\HPV has been nl\neg.
* 2020 Healthy People Goal is 93% for Women 21-65 yrs

96
Lessons Learned
• Understand Patient Needs
• Centralize case management (Patient ID, Scheduling, Tracking)
• Design Cervical Cancer Screening Clinics within a Family Practice Model
• Provide Female Medical Provider
• Provide training to nursing and medical staff

97
Lessons Learned
• Remove cultural and language barriers
• Standing Medical Director orders
• Monitor “Missed Opportunities”
• Gynecologist onsite
• Develop Electronic Database
• Measure and Report Outcomes

98
Successful Private/Public Partnerships Helping Cervical Cancer Screening Program
• Well Women’s Connection Contract• Colorado Community Health Network (CCHN) • CCHN-WWC Advisory Committee Member• Colorado Dept of Public Health & Environment
(CDPHE) WWC Quality Indicators • CDPHE Monthly Health Improvement Team Calls

99
Contact InformationBernadette Lujan MA (WWC CM)
Linda Thurman-Sanchez BSN, RN
(Clinical Programs Nursing Manager)
www.PuebloCHC.org