brain tumers d8
DESCRIPTION
BRAIN TUMORSTRANSCRIPT
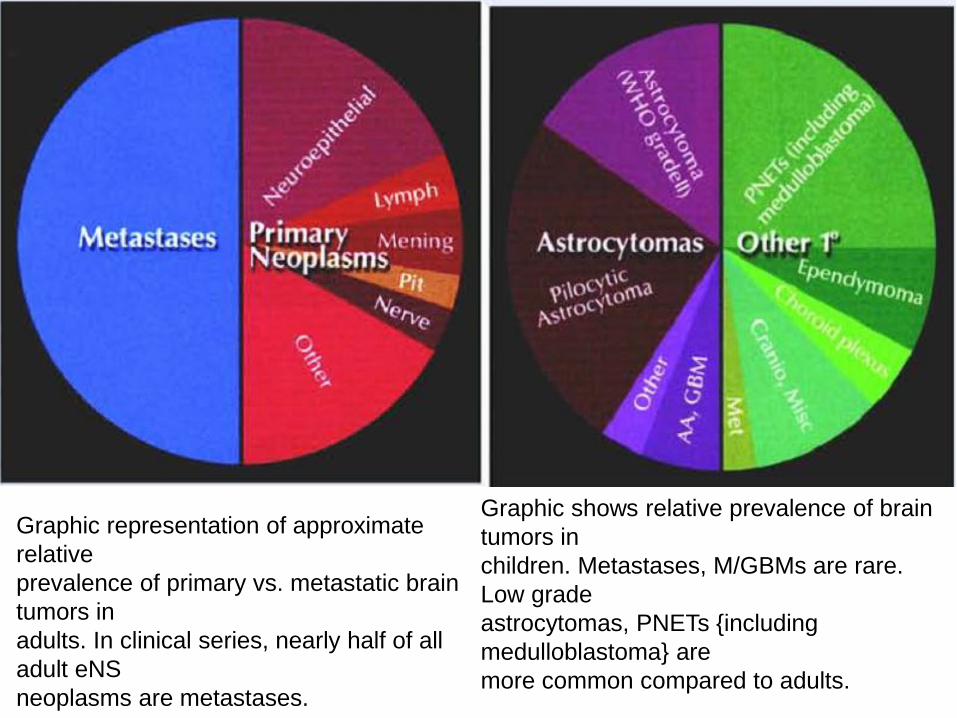
Graphic representation of approximate
relative
prevalence of primary vs. metastatic brain
tumors in
adults. In clinical series, nearly half of all
adult eNS
neoplasms are metastases.
Graphic shows relative prevalence of brain
tumors in
children. Metastases, M/GBMs are rare.
Low grade
astrocytomas, PNETs {including
medulloblastoma} are
more common compared to adults.
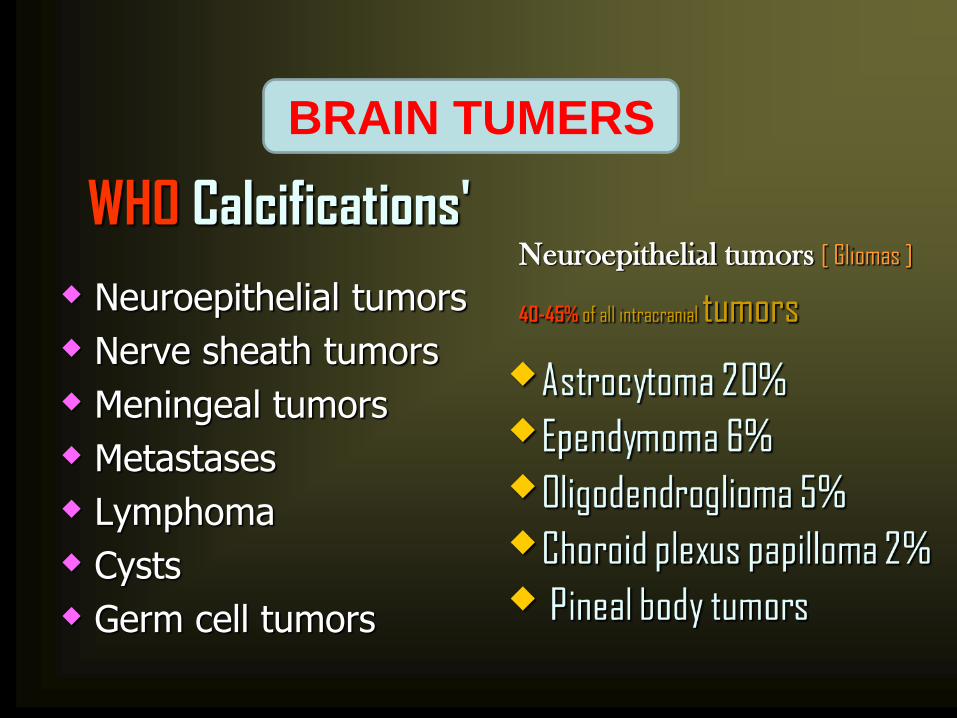
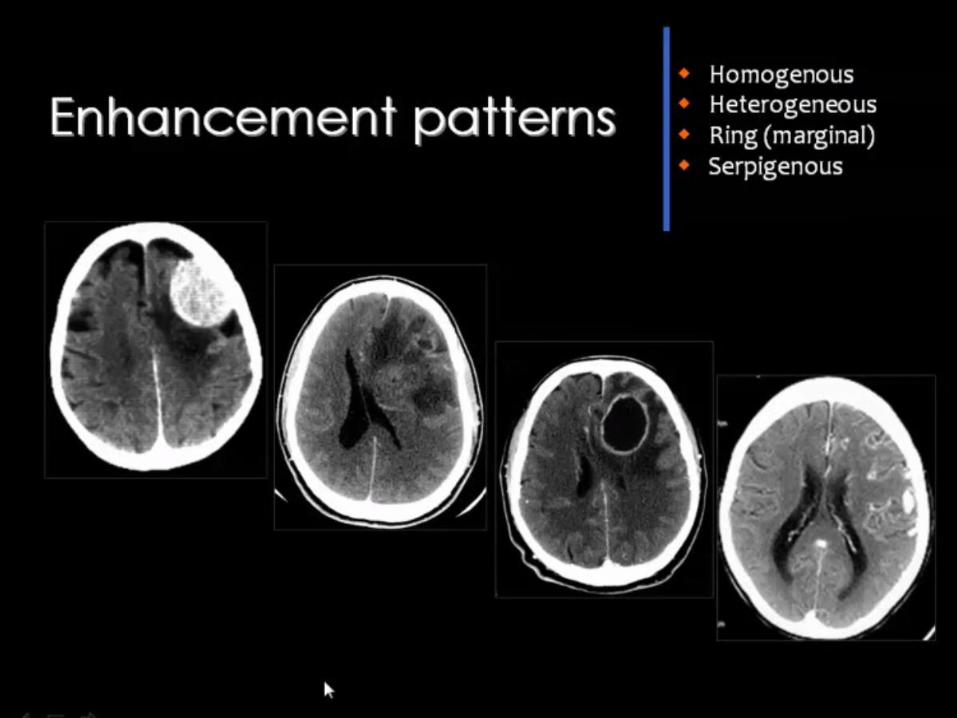
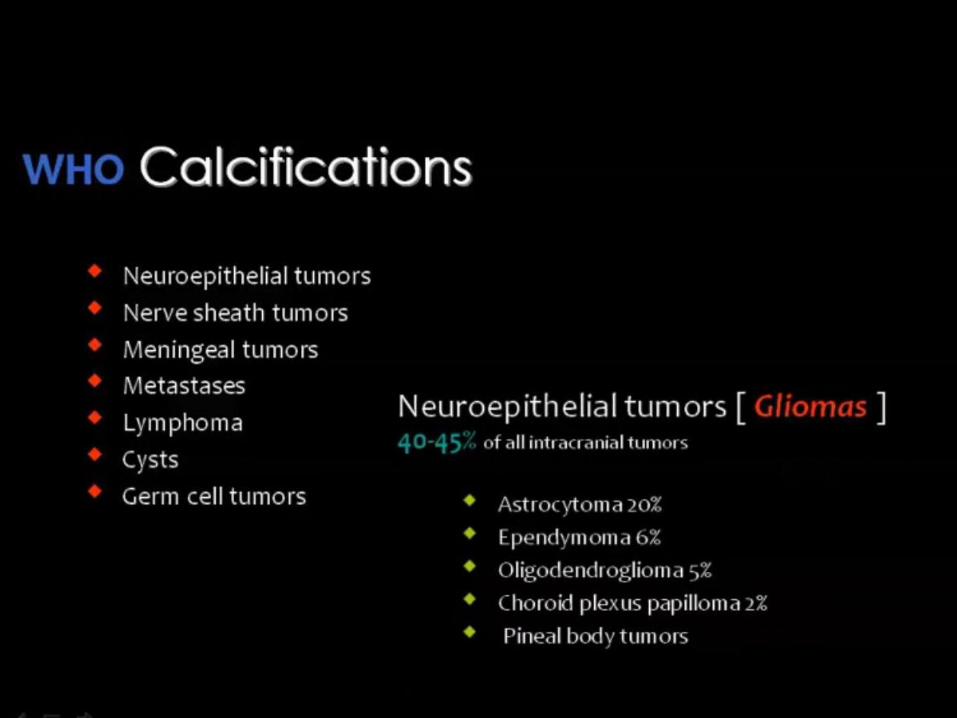
WHO Calcifications'
Neuroepithelial tumors
Nerve sheath tumors
Meningeal tumors
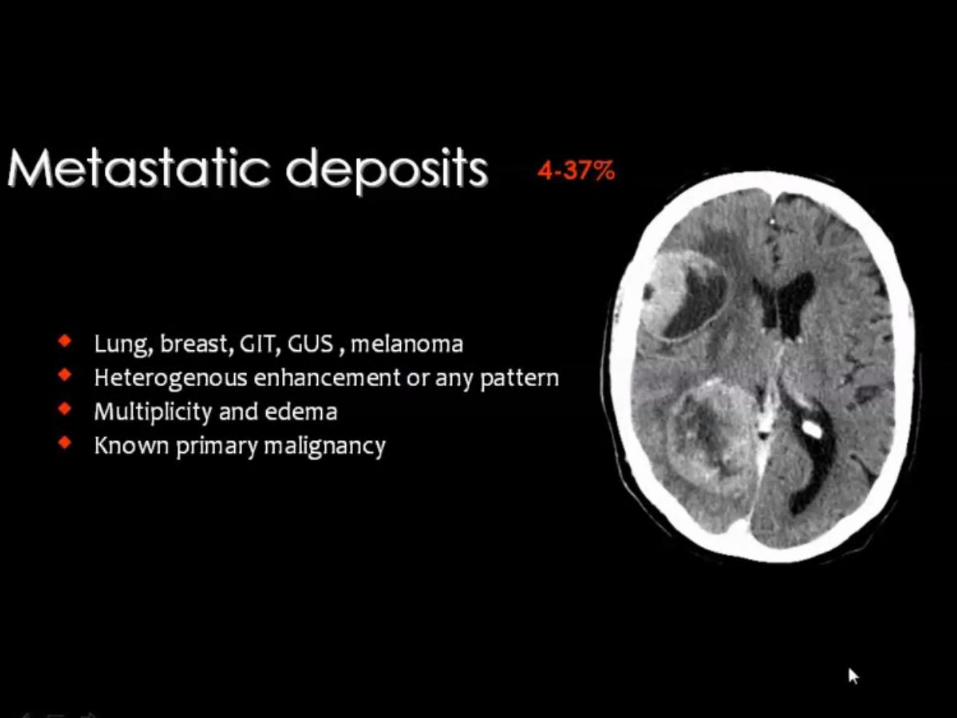
Metastases
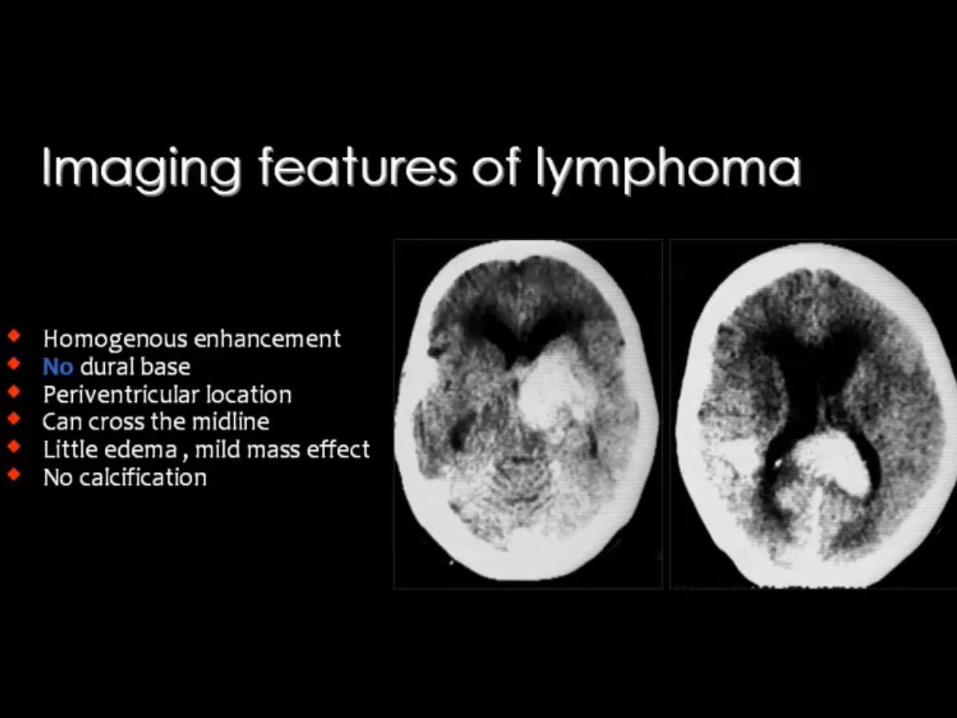
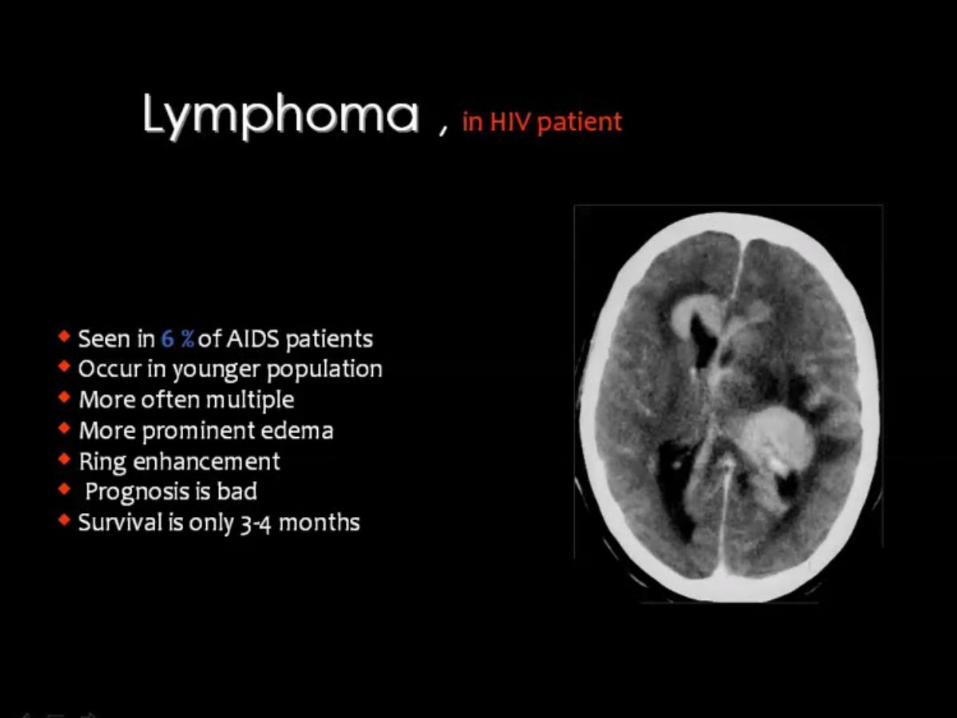
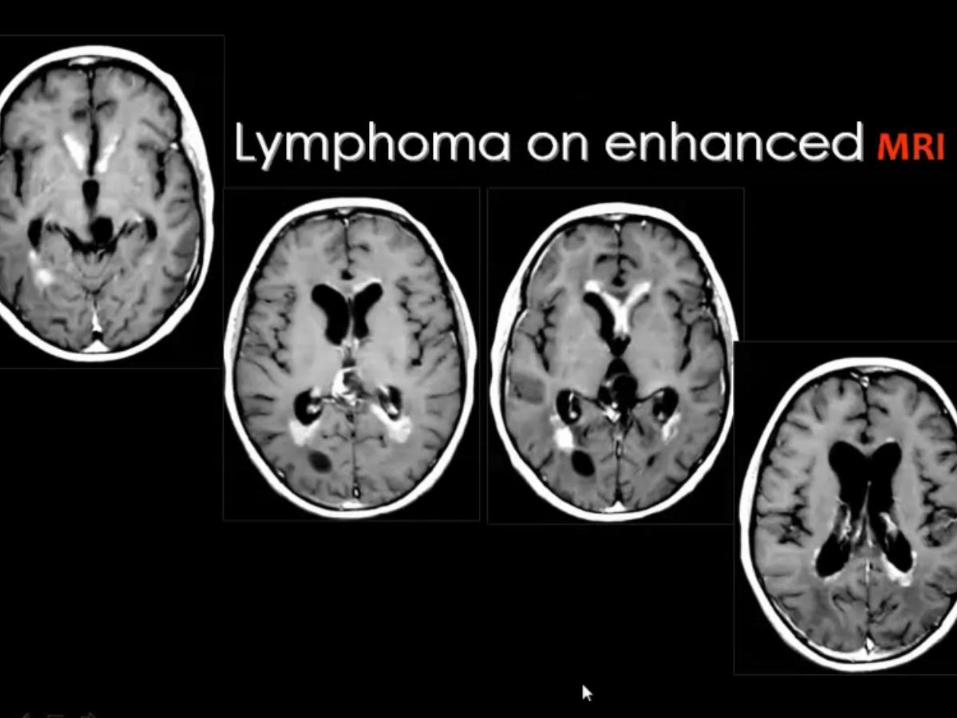
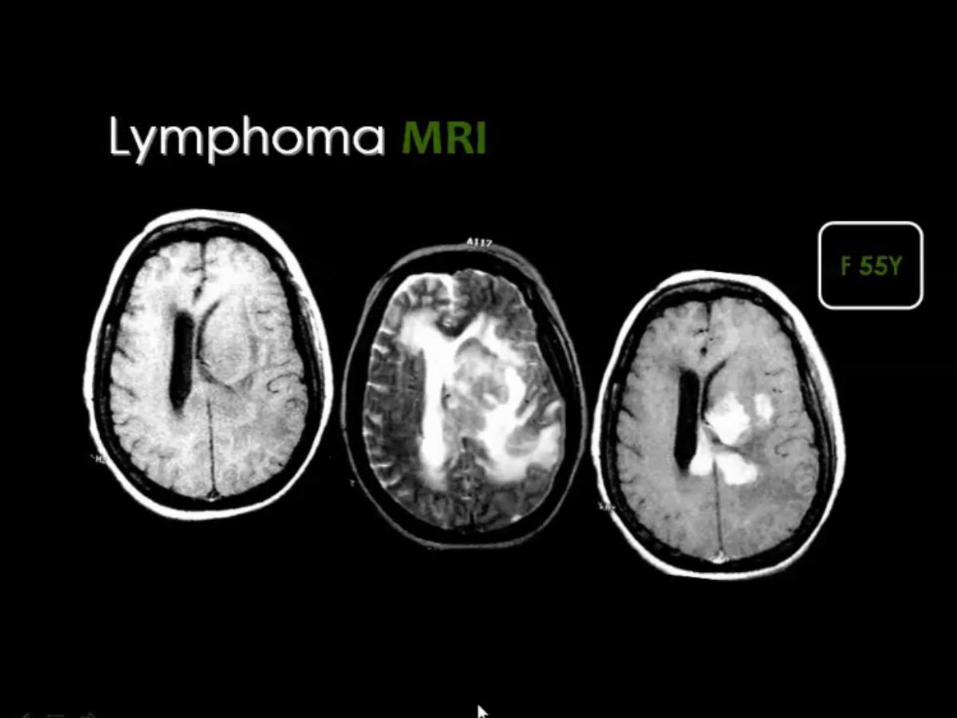
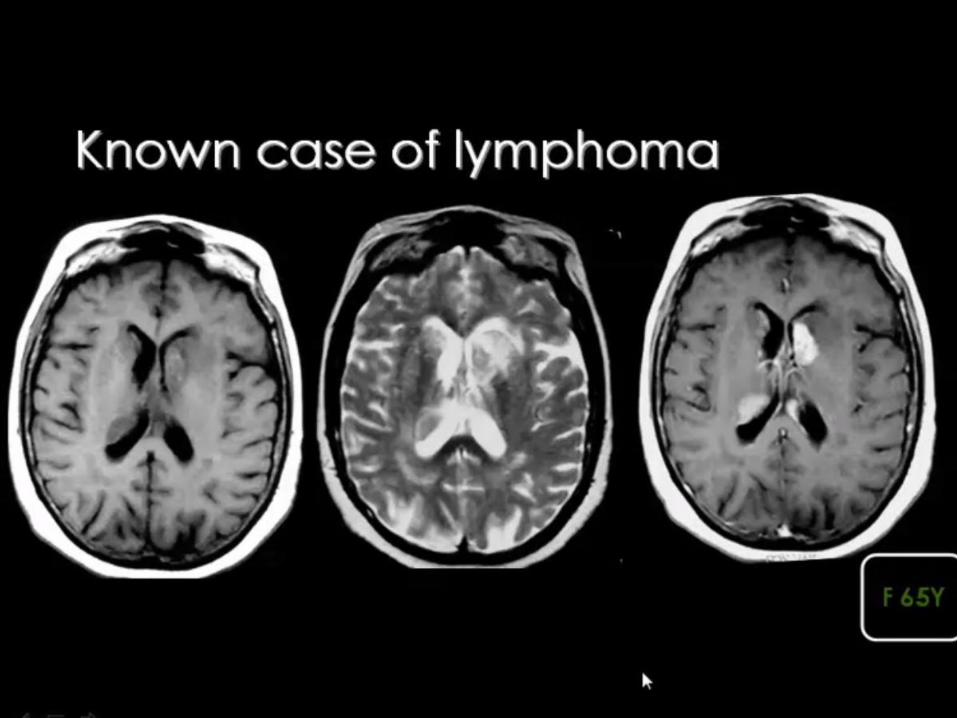
Lymphoma
Cysts
Germ cell tumors
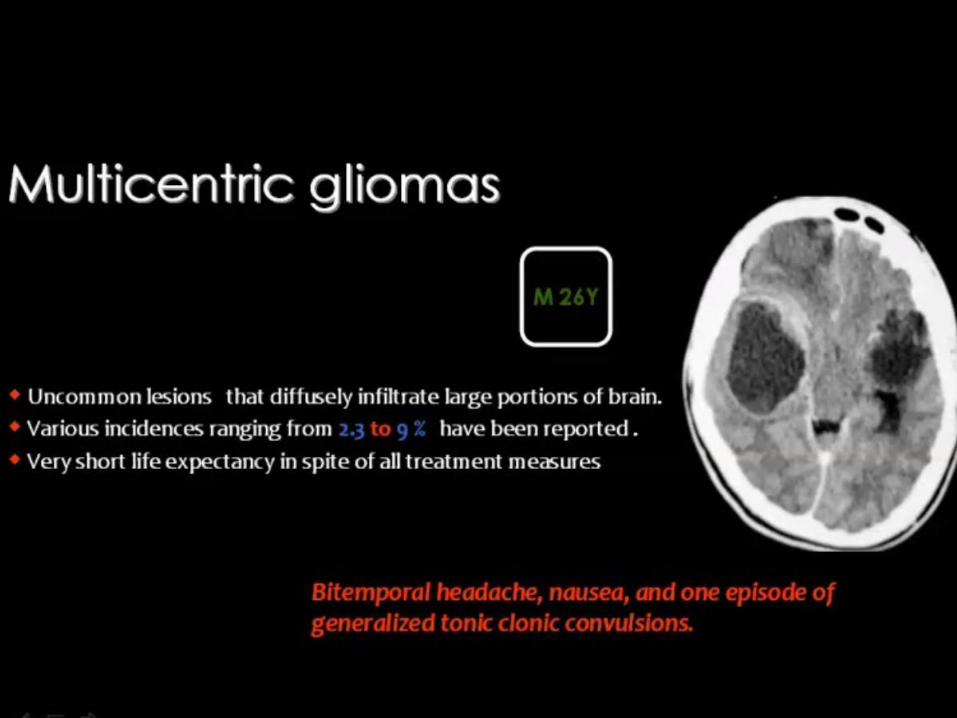
Neuroepithelial tumors [ Gliomas ]
40-45% of all intracranial tumors
BRAIN TUMERS
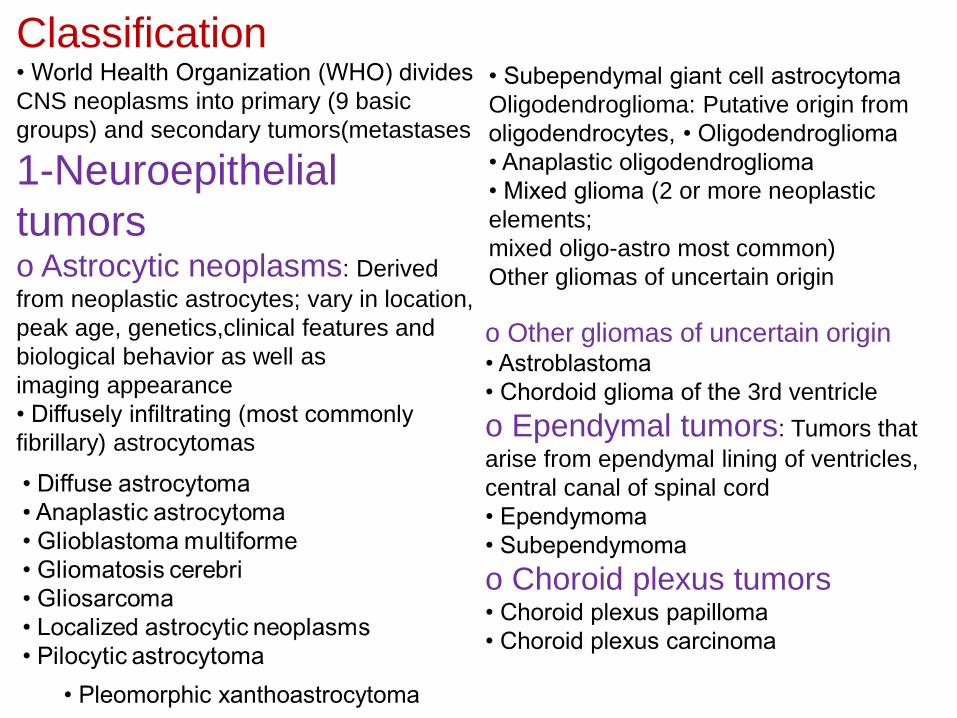
Classification • World Health Organization (WHO) divides
CNS neoplasms into primary (9 basic
groups) and secondary tumors(metastases
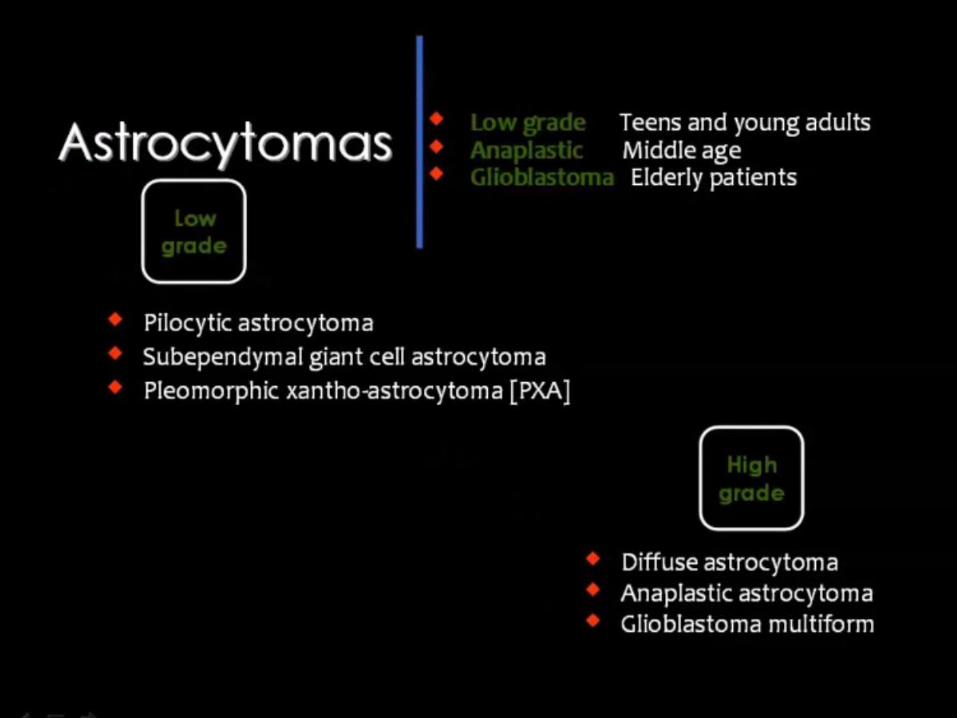
1-Neuroepithelial
tumors o Astrocytic neoplasms: Derived
from neoplastic astrocytes; vary in location,
peak age, genetics,clinical features and
biological behavior as well as
imaging appearance
• Diffusely infiltrating (most commonly
fibrillary) astrocytomas
• Subependymal giant cell astrocytoma
Oligodendroglioma: Putative origin from
oligodendrocytes, • Oligodendroglioma
• Anaplastic oligodendroglioma
• Mixed glioma (2 or more neoplastic
elements;
mixed oligo-astro most common)
Other gliomas of uncertain origin
o Other gliomas of uncertain origin • Astroblastoma
• Chordoid glioma of the 3rd ventricle
o Ependymal tumors: Tumors that
arise from ependymal lining of ventricles,
central canal of spinal cord
• Ependymoma
• Subependymoma
o Choroid plexus tumors • Choroid plexus papilloma
• Choroid plexus carcinoma
• Pleomorphic xanthoastrocytoma
2- Neuronal, mixed glial-neuronal and neurocytic tum (neoplasms with variable neuronal and/or glial differentiation)
o Ganglioglioma and gangliocytoma (in cerebellum Lhermitte-Duclos disease
o Desmoplastic infantile ganglioglioma/astrocytom
o Dysembryoplastic neuroepithelial tumor (DNET
o Hypothalamic hamartoma
o Central neurocytoma and parenchymal(extraventricular) neurocytic tumors
• Pineal parenchymal tumors: Derived from pineocyt
(pineal parenchymal cells) or embryonic prercursor with wide spectrum of differentiation
o Pineoblastoma o Pineocytoma
3-Embryonal tumors: Round-cell tumors with variable spectrum of
differentiation; some neuropathologists classify all these as primitive neuroectodermal
tumors(PNETs)
o Medulloepithelioma
o Ependymoblastoma
o Medulloblastoma (posterior fossa primitive neuroepithelial tumor or PNET-MB)
o Primitive neuroepithelial tumor (supratentorial small round cell embryonal tumor
o Atypical teratoid/rhabdoid tumor (AT/RT)
4- Peripheral neuroblastic tumors: Tumors with wide
range of neuronal differentiation, may involve/invade CNS
o Neuroblastoma (when involves CNS, is usually metastatic from extracranial site)
5- Tumors of cranial and spinal or peripheral nerves: Tumors with wide range of
histopathological features;
multiple tumors in skull/brain are associated with inherited familial tumor syndromes (Le.neurofibromatosis)
o Neurofibroma
o Schwannoma
o Malignant peripheral nerve sheath tumor (MPNST)
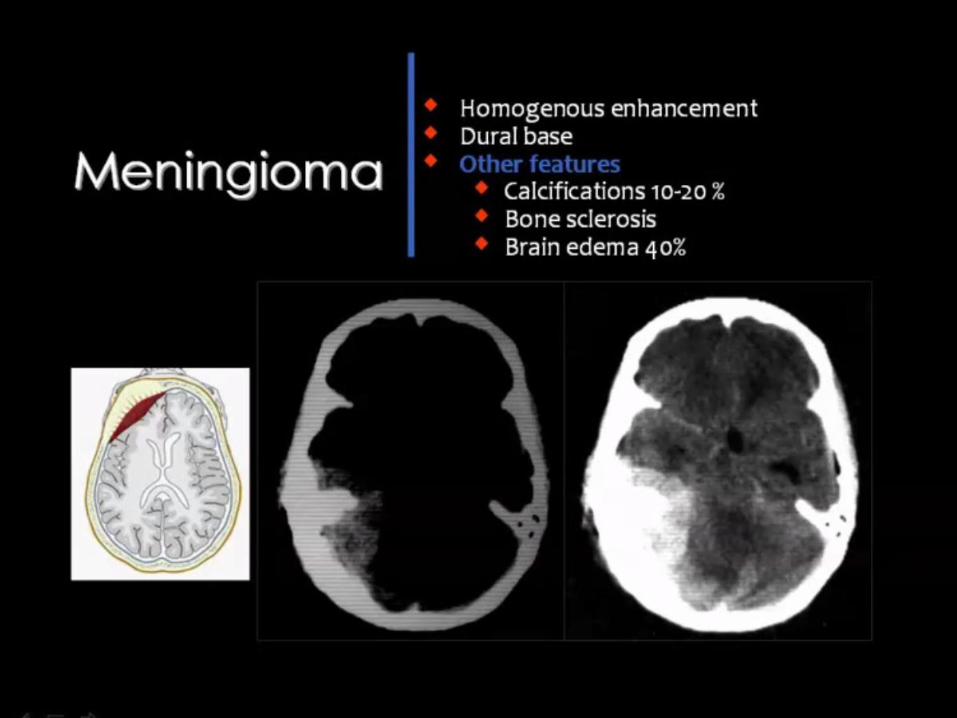
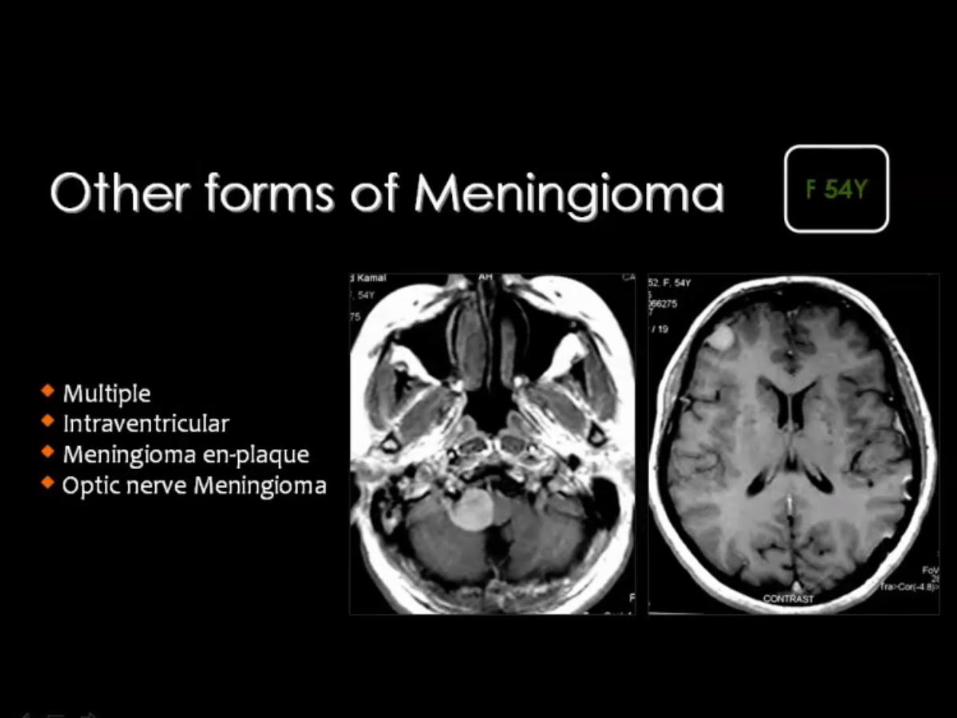
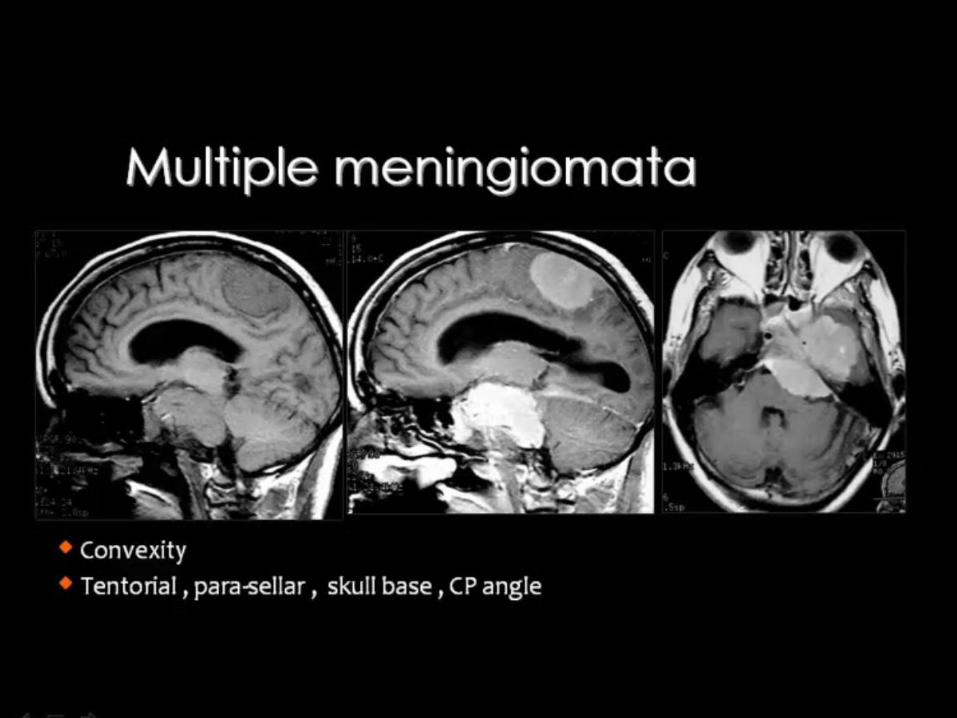
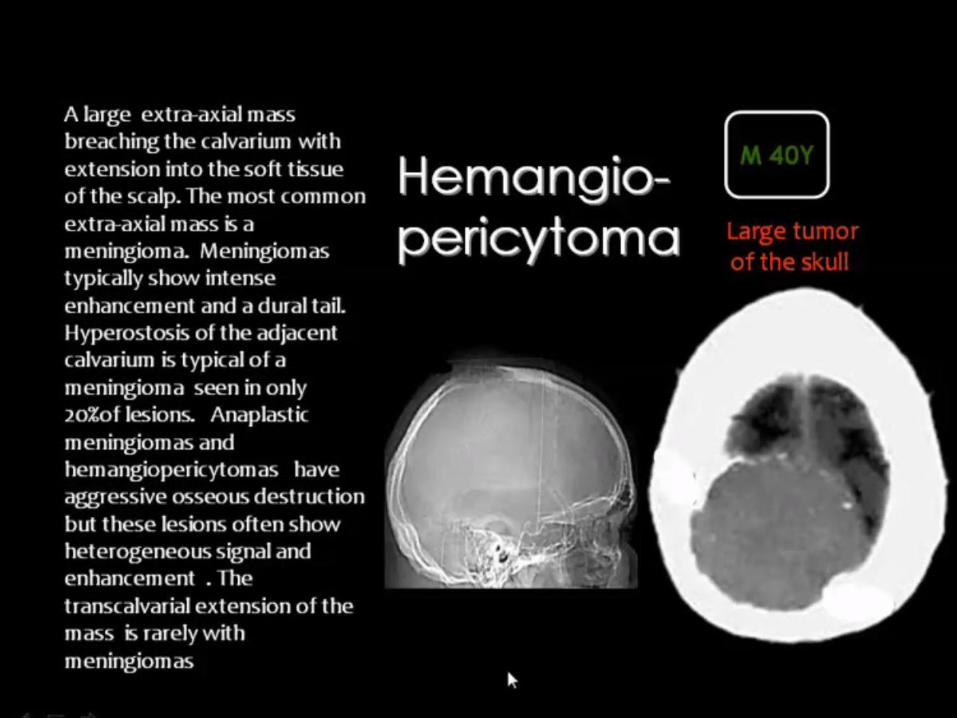
6- Meningeal tumors o Meningothelial cell tumors (e.g., meningioma)
o Mesenchymal, nonmeningothelial cell tumors (e.g.,chondrosarcoma)
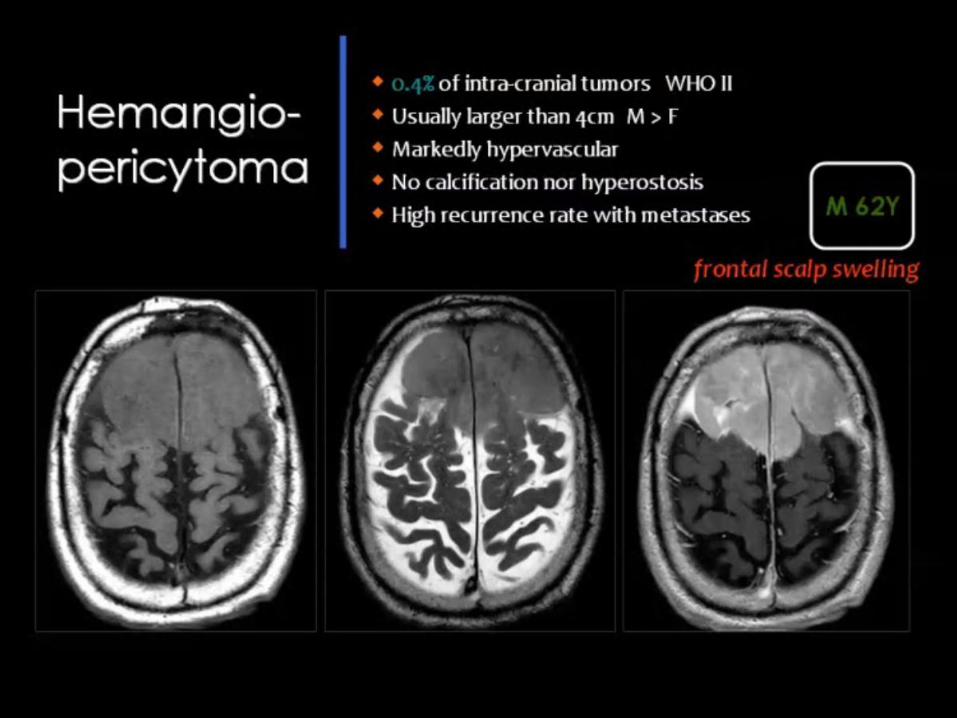
o Tumors of uncertain histogenesis (e.g.,hemangioblastoma)
•
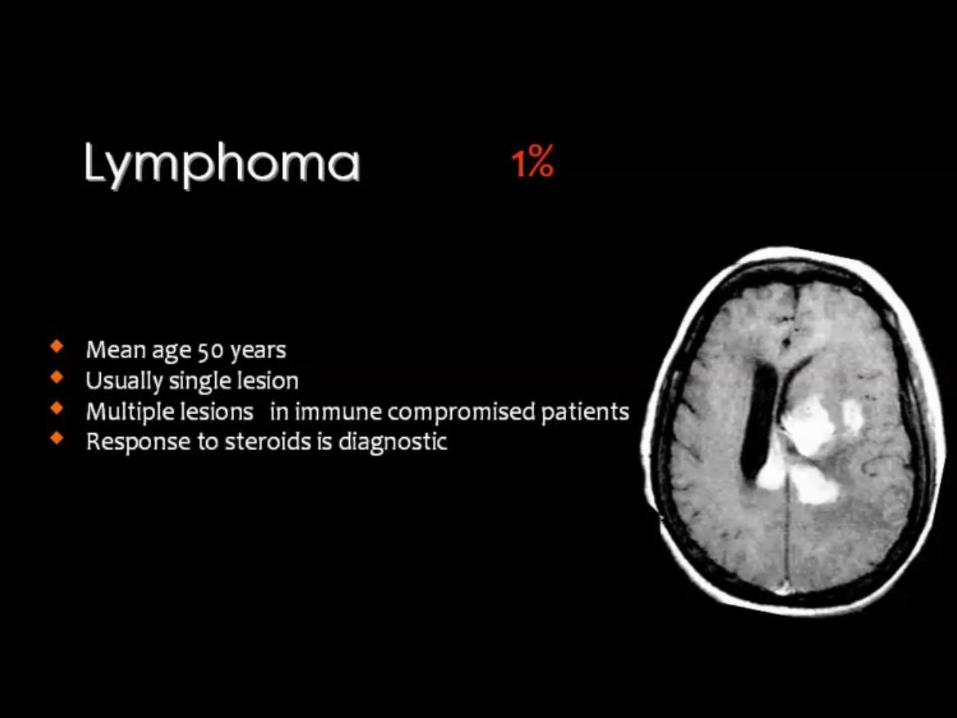
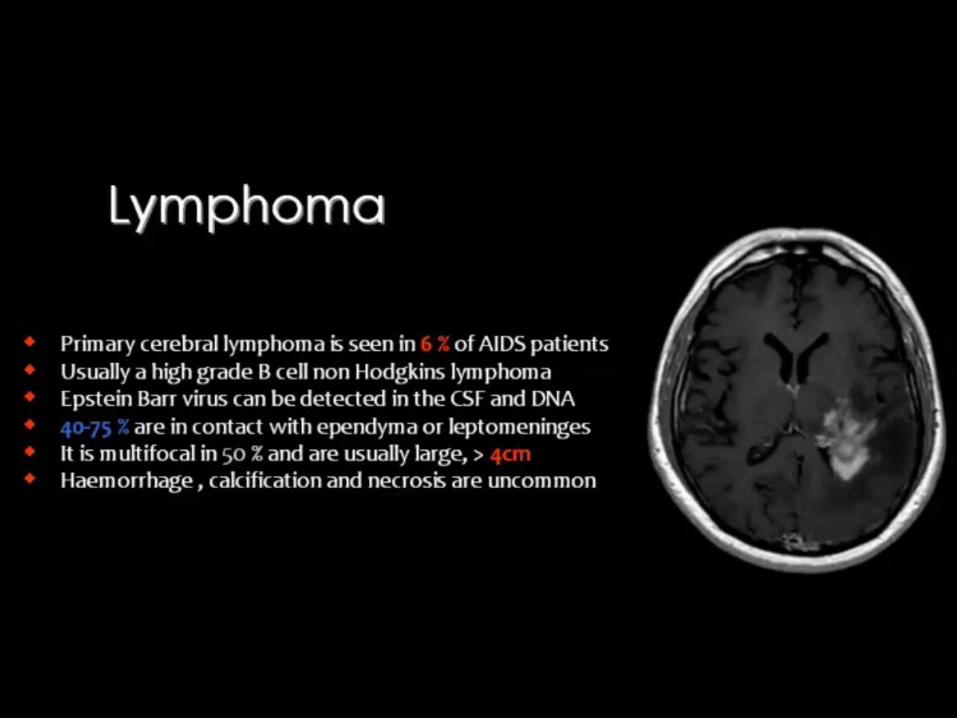
7- Lymphoma and tumors of hemopoietic system: May be primary or
secondary, variably involve skull,meninges, and/or brain
o Lymphoma o Plasmacytoma o Leukemia (granulocytic sarcoma)
8- Germ cell tumors: Broad histopathological spectrum of extragonadal germ cell neoplasms with
variable
biological behavior
o Germinoma o Teratoma o Embryonal carcinoma
o Others (e.g., yolk sac tumor, choriocarcinoma,
mixed germ cell tumors)
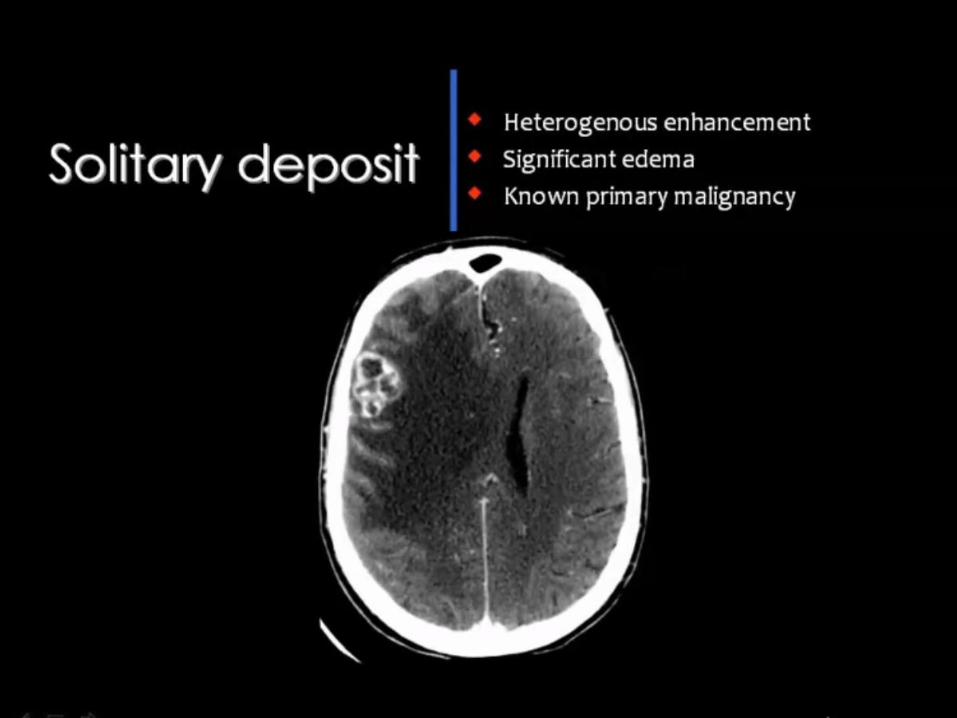
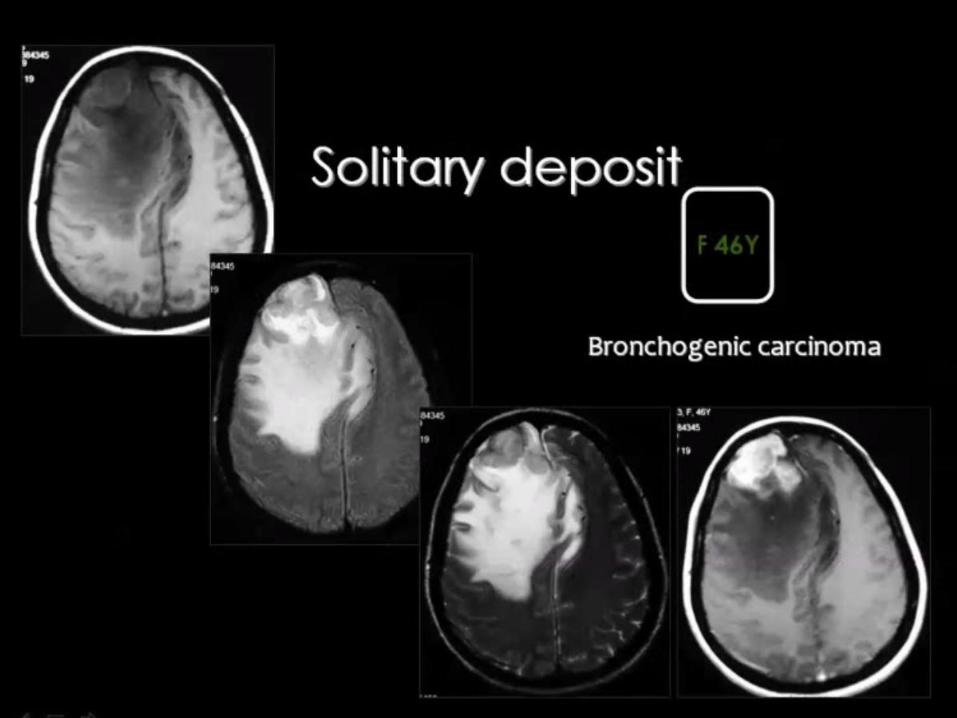
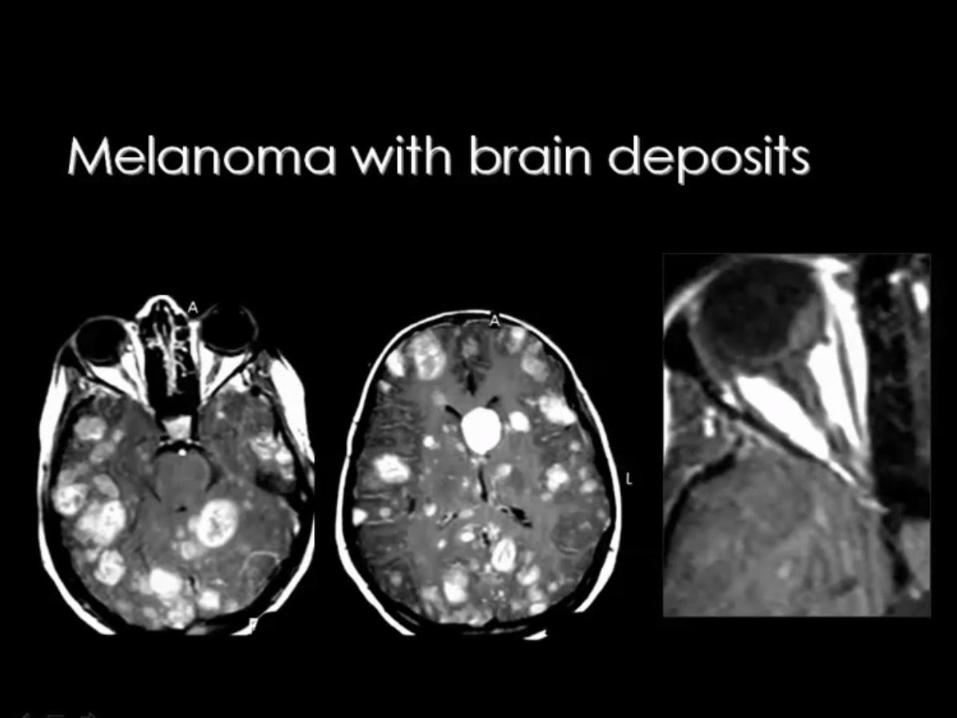
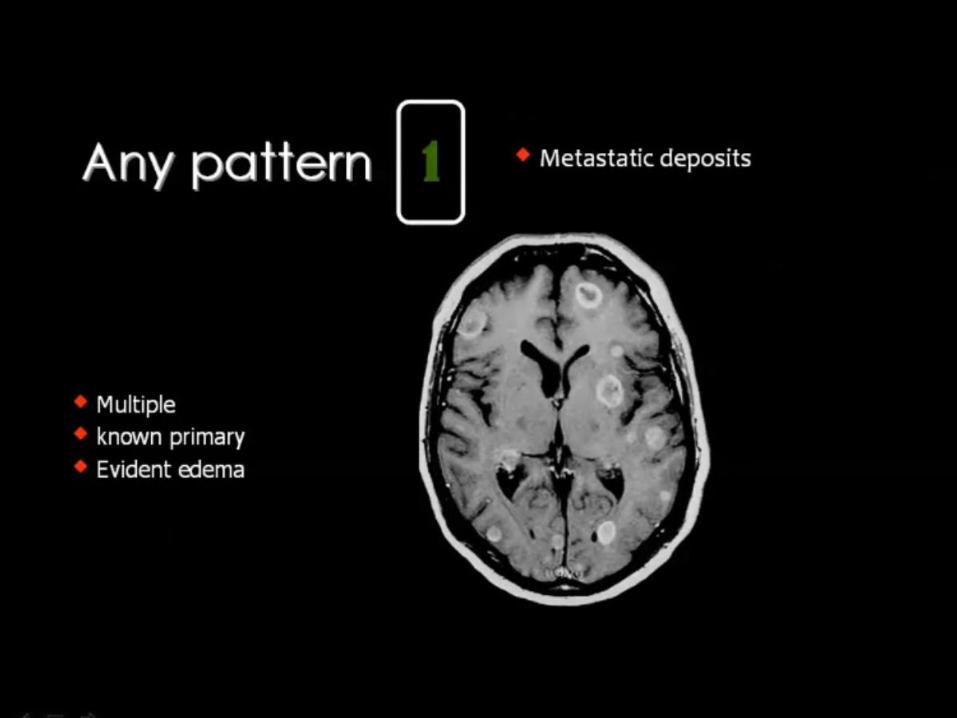
9-Metastatic tumors and remote effects of cancer on the CNS o Metastases (brain parenchyma, other sites such as
meninges and pituitary gland)
o Paraneoplastic syndromes
Tumors in children < 2 yrs
• Astrocytoma
• Choroid plexus papilloma
• Teratoma
• Embryonal tumors
Cortically-based tumors
• DNET
• Ganglioglioma
• Oligodendroglioma
• PXA
Intraventricular tumors
• Ependymoma, subependymoma
• Central neurocytoma
• Choroid plexus papilloma/carcinoma
Pineal region tumors
• Pineal parenchymal tumors
(pineocytoma/blastoma
• Germ cell tumors (germinoma,teratoma,etc)
• "Other" tumors/masses in
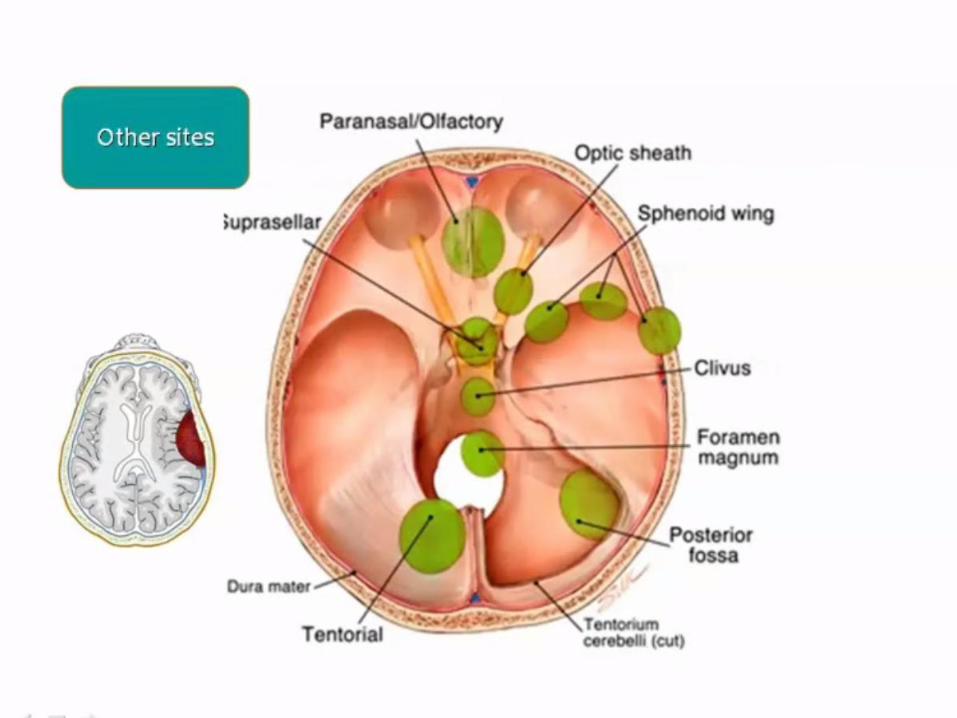
o Meningioma (tentorial apex)
o Astrocytoma (rare in pineal gland;
more common in tectum, thalamus)
o Nonneoplastic pineal cyst
Dural-based tumors and mimics
• Meningioma
• Metastasis
• Inflammatory pseudotumor
• Infection (e.g., tuberculosis)
• Extramedullary hematopoiesis
Local intracranial extension from
extracranial
neoplasms
• Chordoma
• Paraganglioma
• Carcinomas (e.g., nasopharyngeal
squamous cell),
sarcomas (rhabdomyosarcoma)
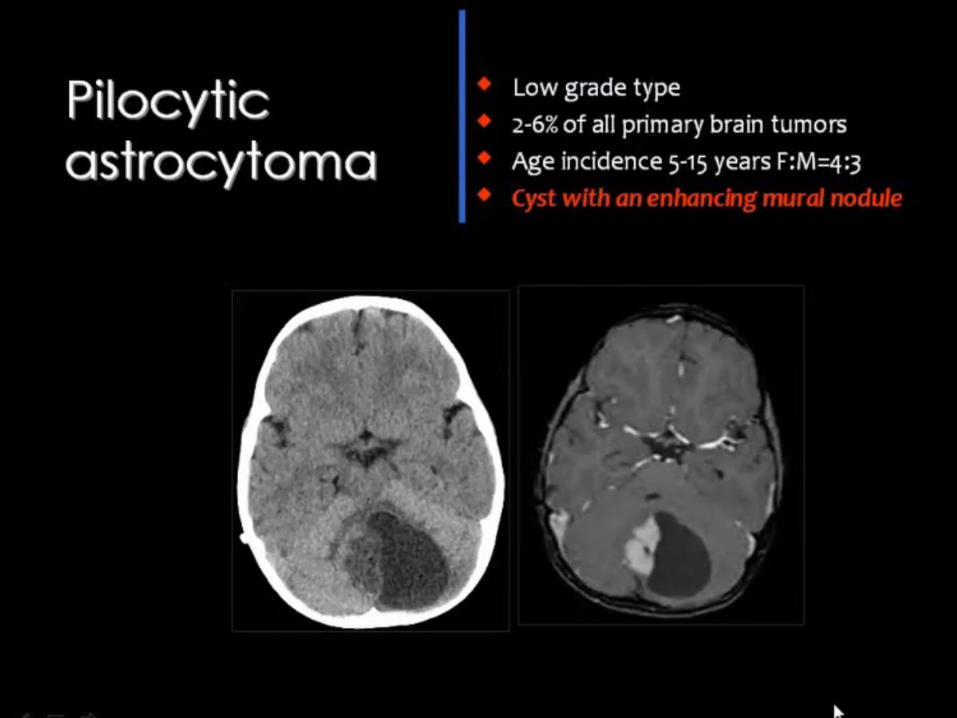
Neoplasms that often have cyst + nodule
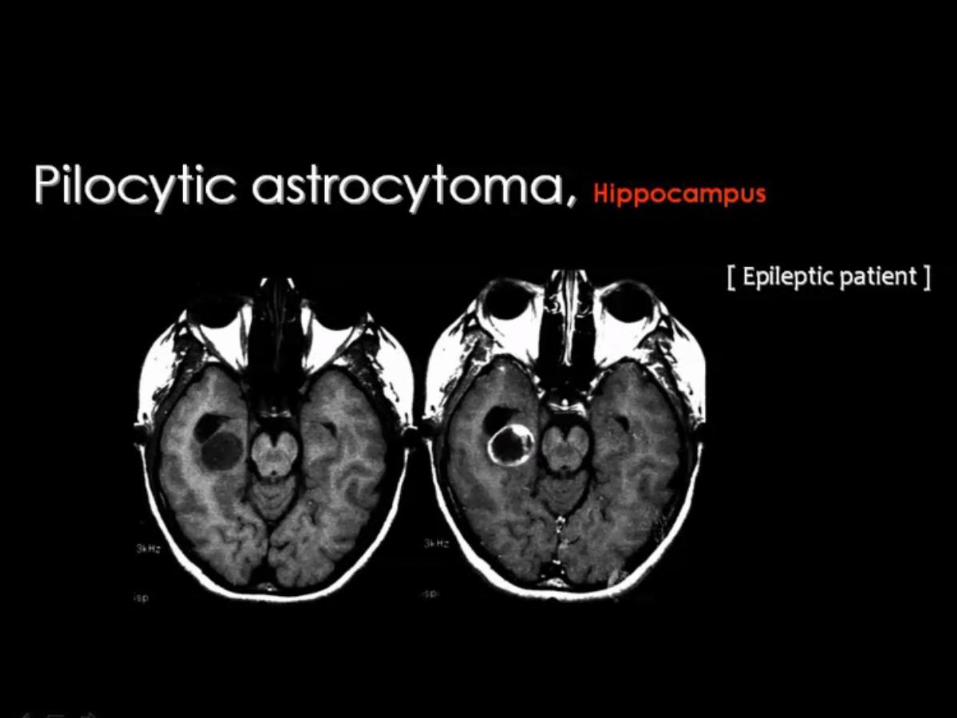
• Pilocytic astrocytoma
• Craniopharyngioma
• Ganglioglioma
• Hemangioblastoma


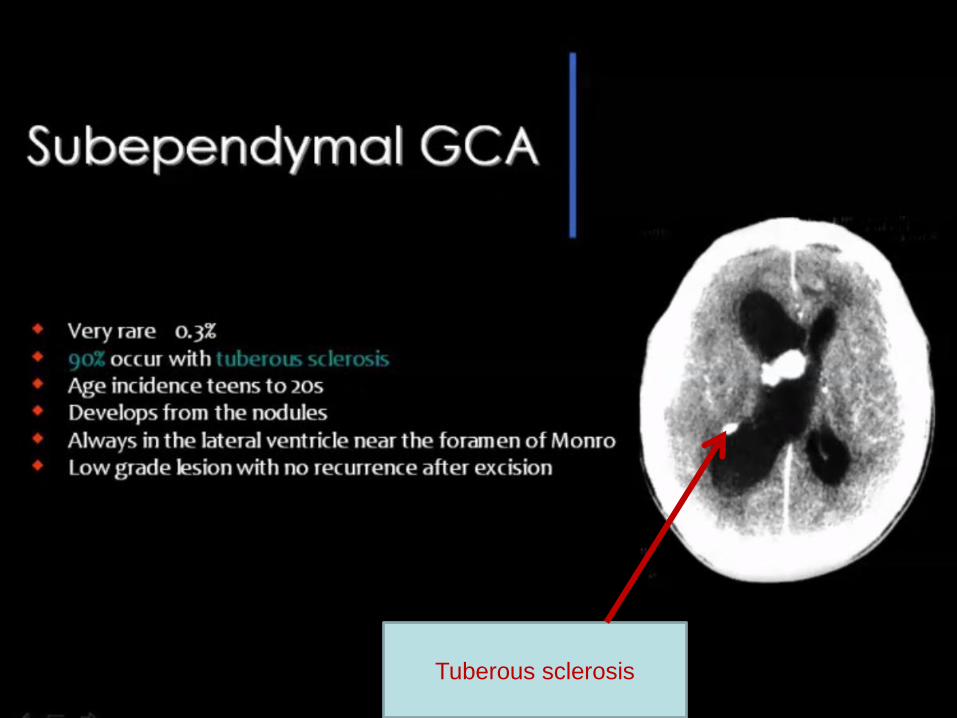
Tuberous sclerosis
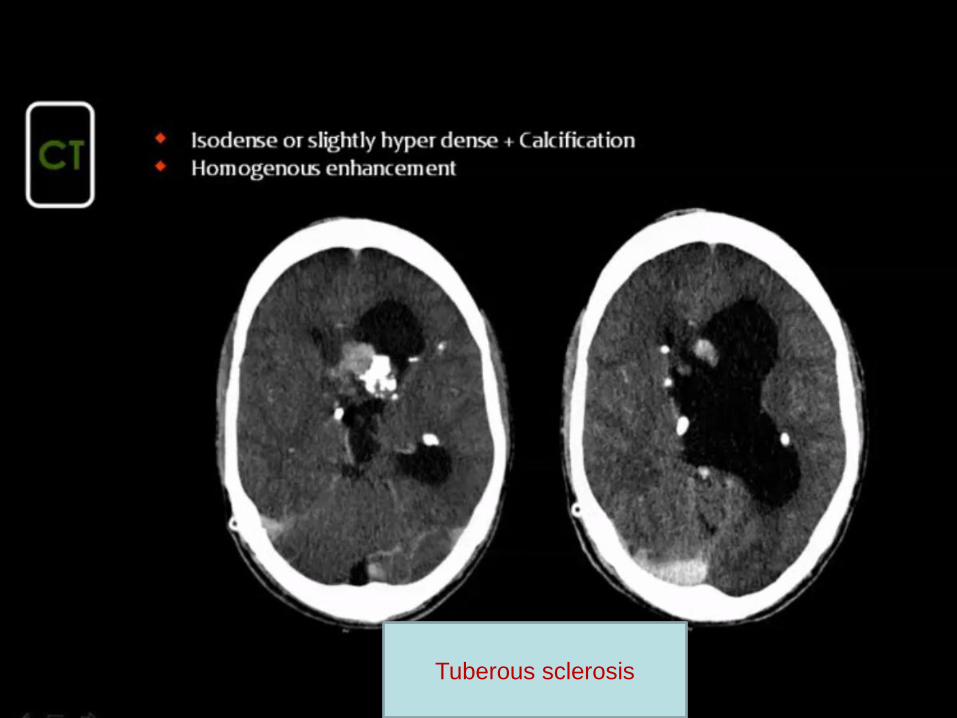
Tuberous sclerosis
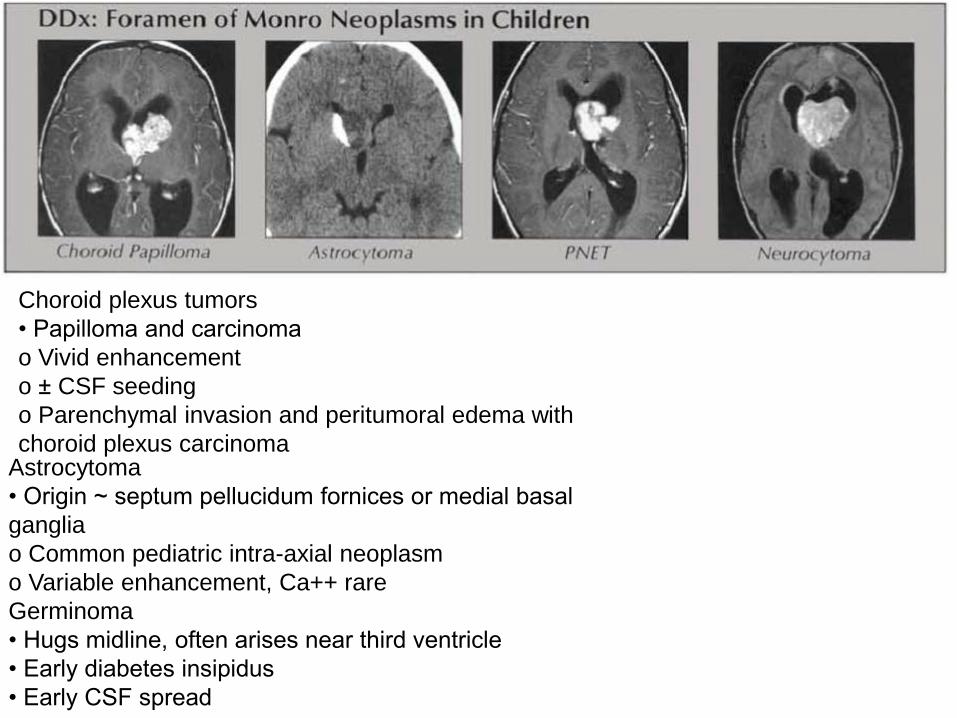
Choroid plexus tumors
• Papilloma and carcinoma
o Vivid enhancement
o ± CSF seeding
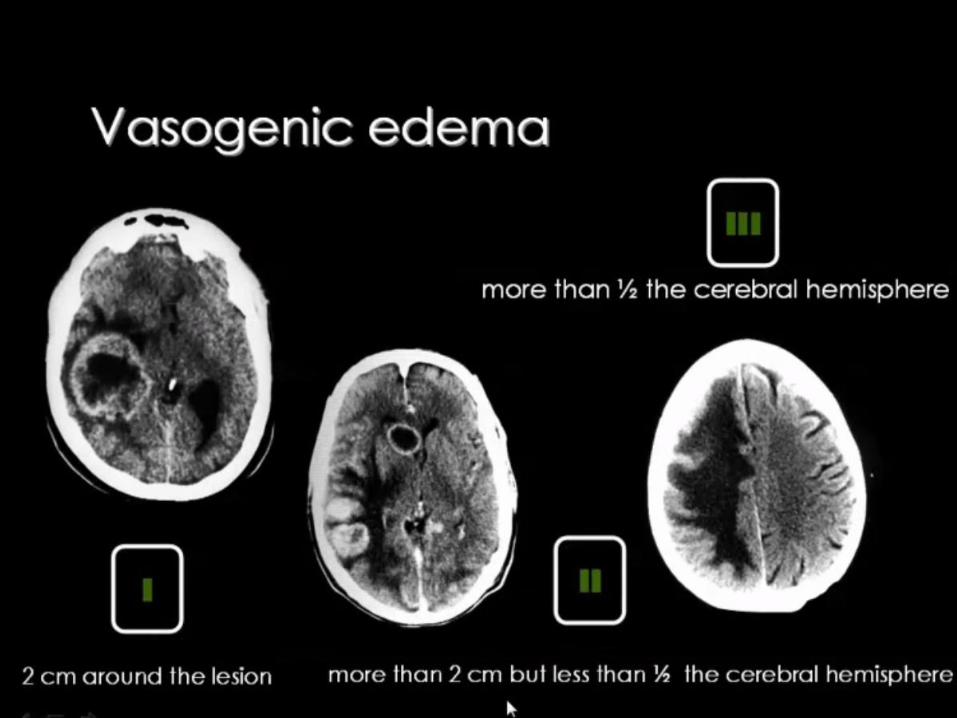
o Parenchymal invasion and peritumoral edema with
choroid plexus carcinoma Astrocytoma
• Origin ~ septum pellucidum fornices or medial basal
ganglia
o Common pediatric intra-axial neoplasm
o Variable enhancement, Ca++ rare
Germinoma
• Hugs midline, often arises near third ventricle
• Early diabetes insipidus
• Early CSF spread
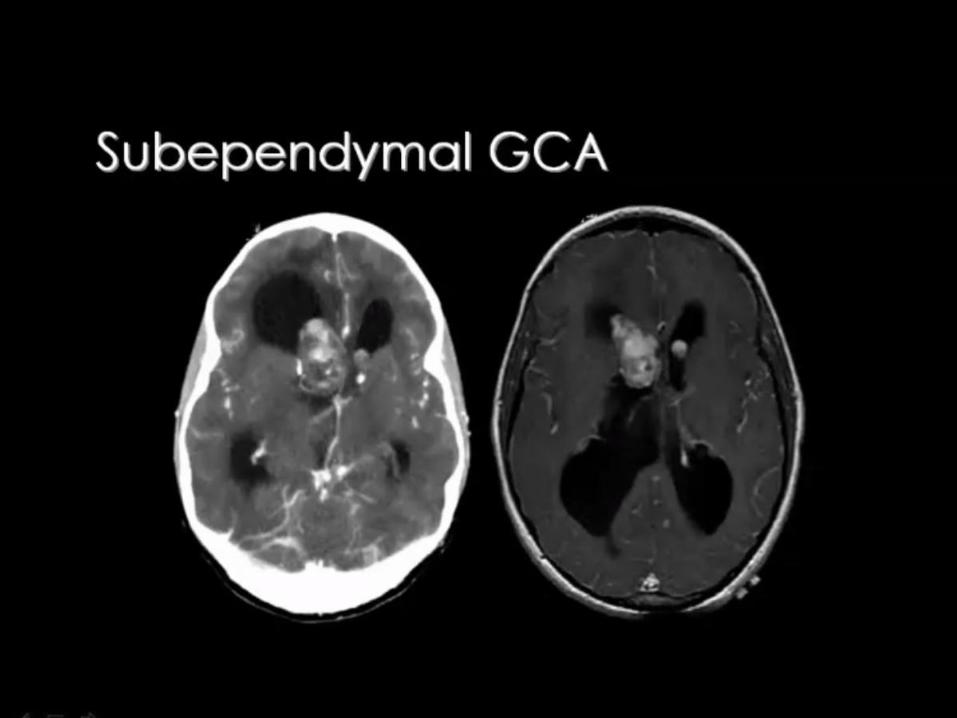
Subependymoma
• Inferior fourth and frontal horn most common
locations
• Nonenhancing mass
• Tumor of middle age and elderly
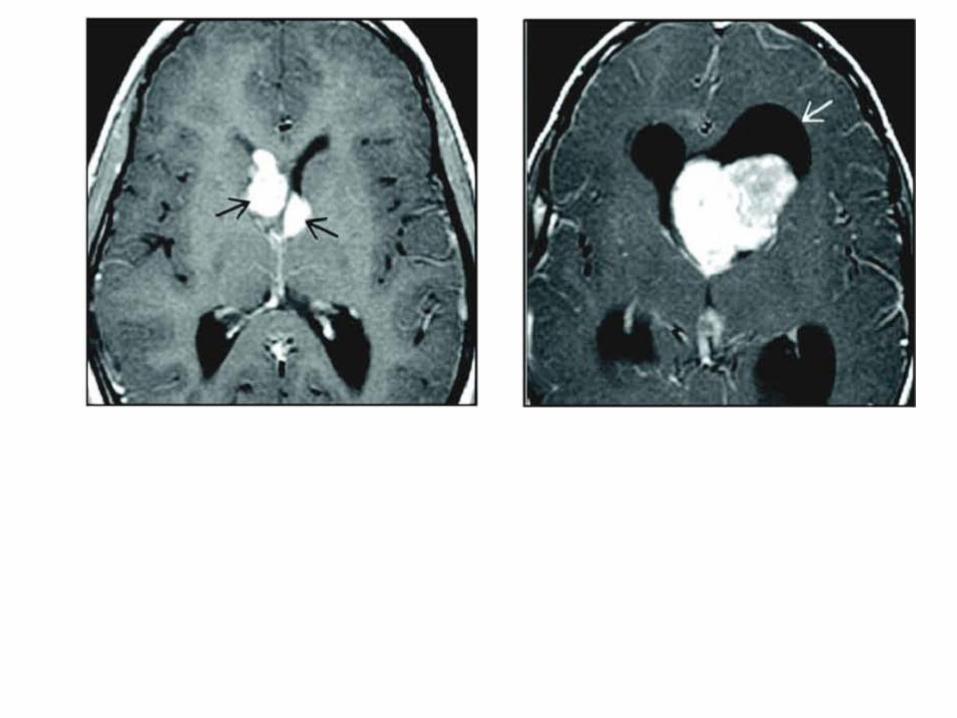
Central neurocytoma
• Well defined, variably vascularized lobulated mass
• Origin near foramen of Monro or septum pellucidum
• Necrosis and cyst formation are common
• Seen in young adults
Supratentorial PNET
• May exophytically extend into ventricle
• Lack of peritumoral edema
• Highly cellular tumor, isointense ~ slightly
hyperintense on T2WI
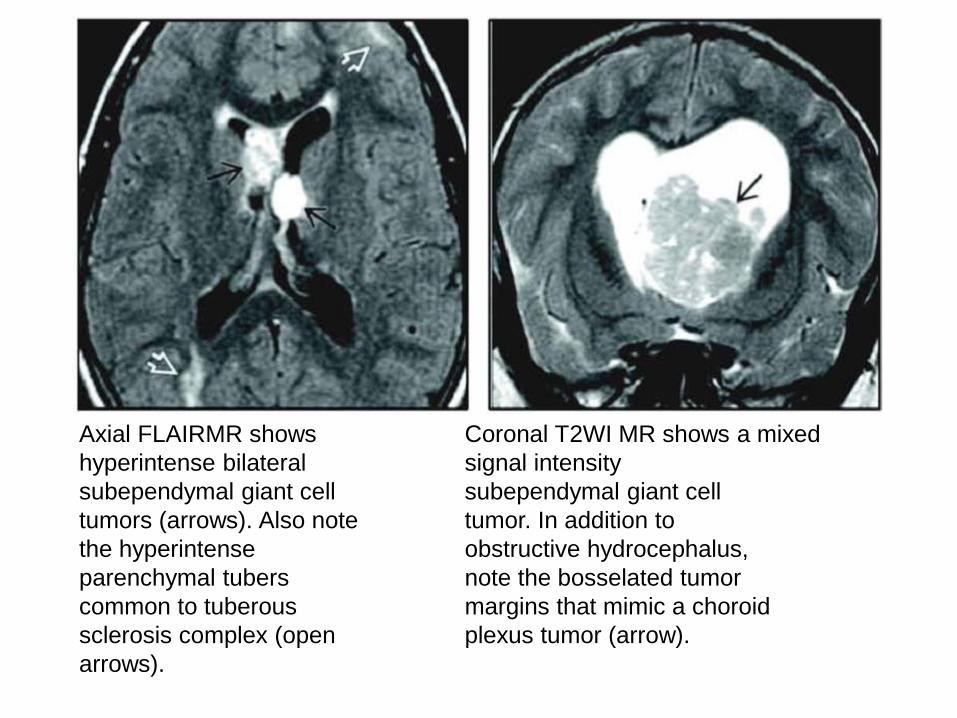
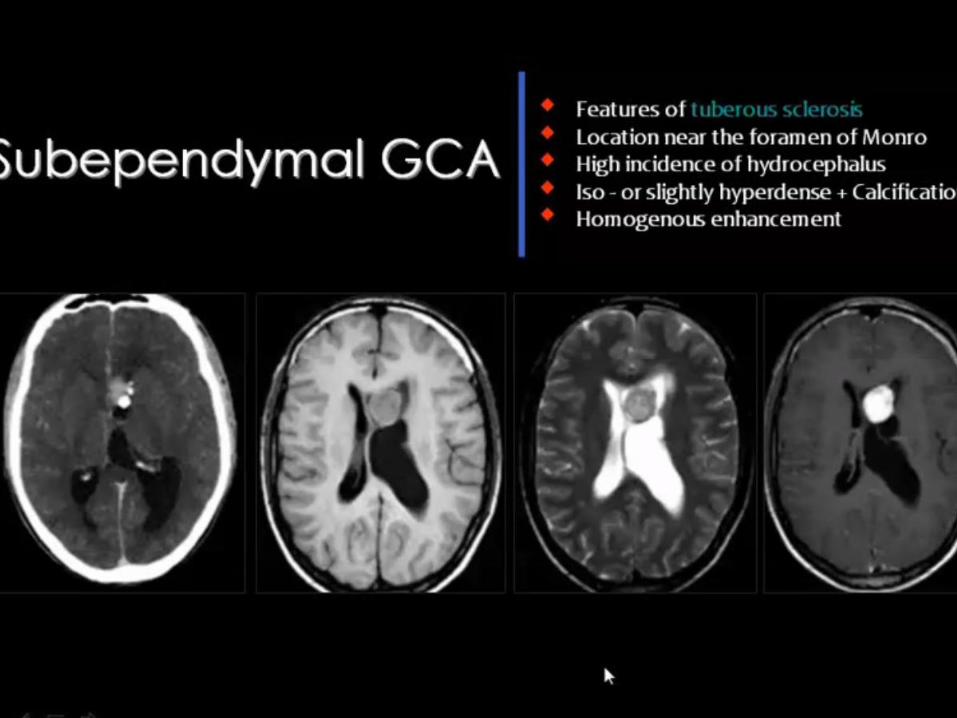
Axial FLAIRMR shows
hyperintense bilateral
subependymal giant cell
tumors (arrows). Also note
the hyperintense
parenchymal tubers
common to tuberous
sclerosis complex (open
arrows).
Coronal T2WI MR shows a mixed
signal intensity
subependymal giant cell
tumor. In addition to
obstructive hydrocephalus,
note the bosselated tumor
margins that mimic a choroid
plexus tumor (arrow).
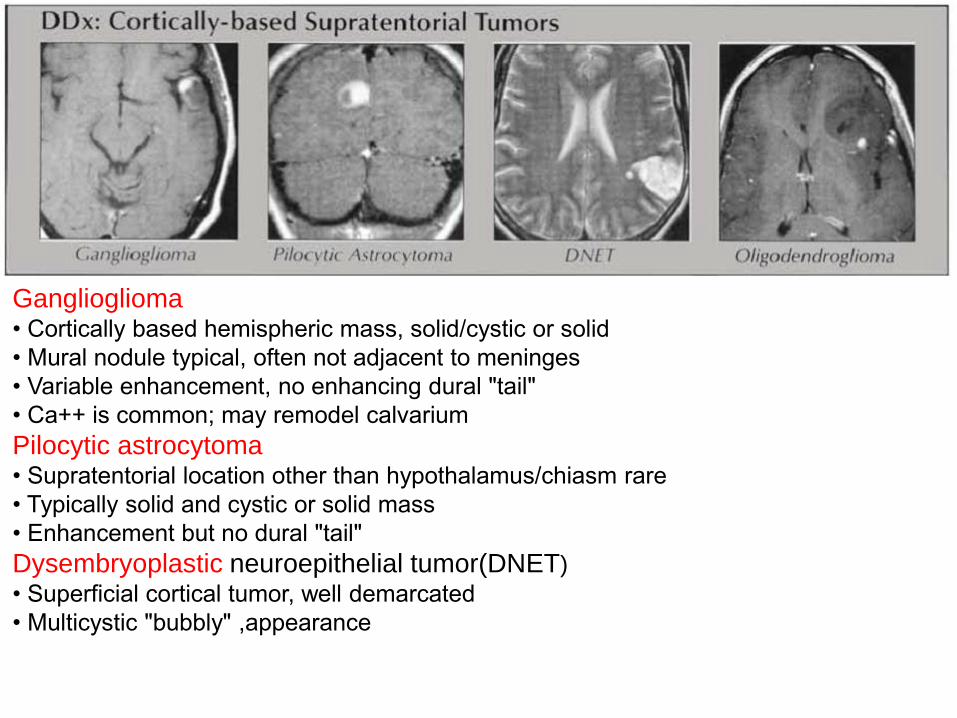
Ganglioglioma • Cortically based hemispheric mass, solid/cystic or solid
• Mural nodule typical, often not adjacent to meninges
• Variable enhancement, no enhancing dural "tail"
• Ca++ is common; may remodel calvarium
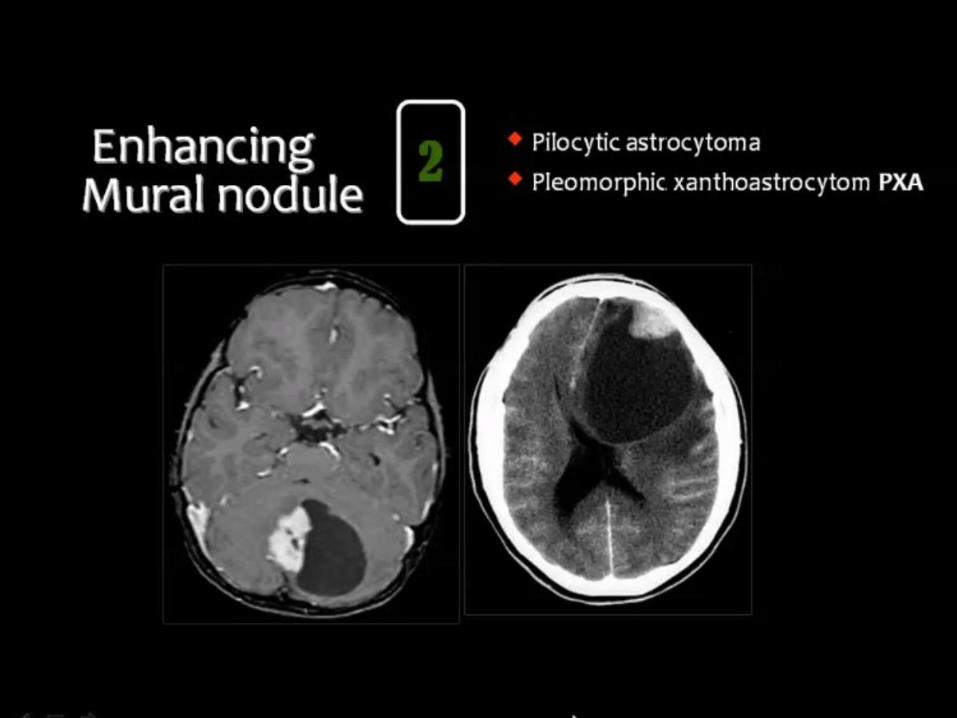
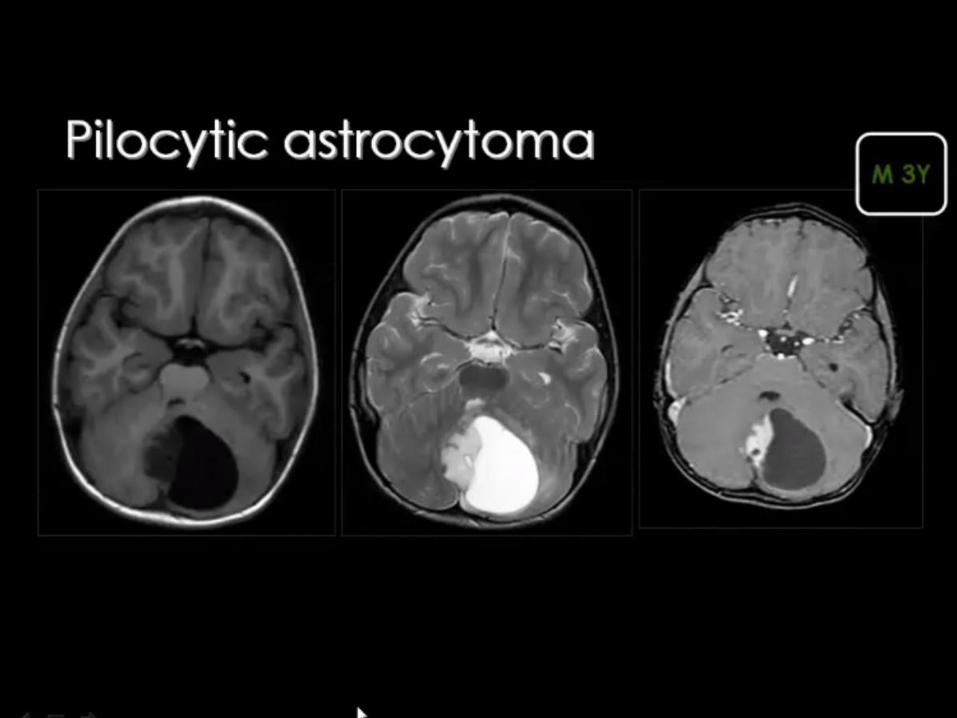
Pilocytic astrocytoma • Supratentorial location other than hypothalamus/chiasm rare
• Typically solid and cystic or solid mass
• Enhancement but no dural "tail"
Dysembryoplastic neuroepithelial tumor(DNET)
• Superficial cortical tumor, well demarcated
• Multicystic "bubbly" ,appearance
• T2 hyperintense mass with rare, mild enhancement
• May remodel calvarium
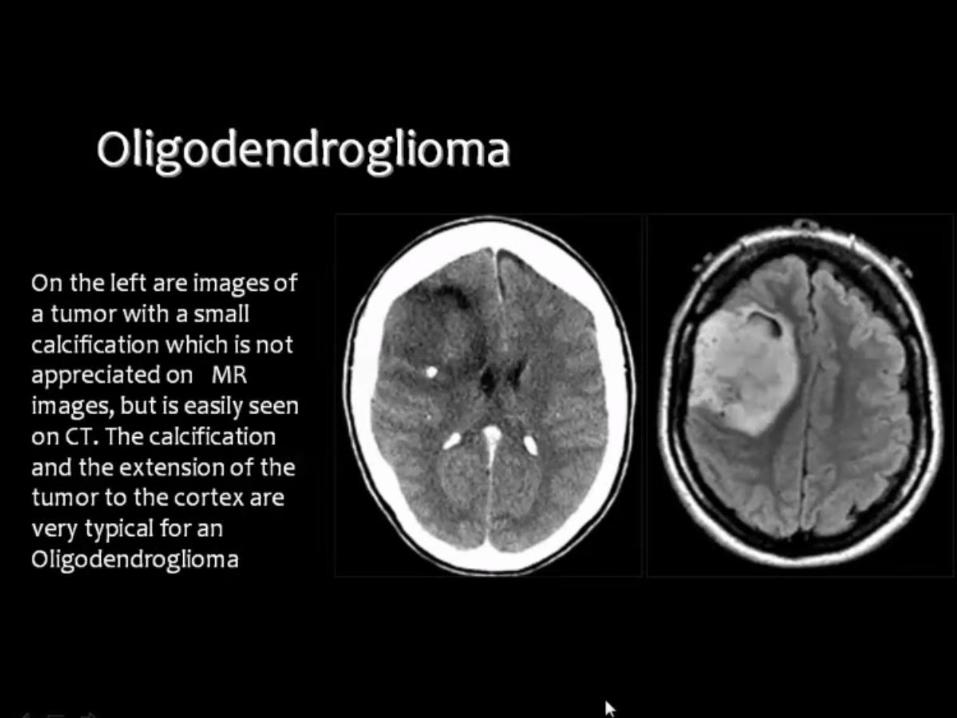
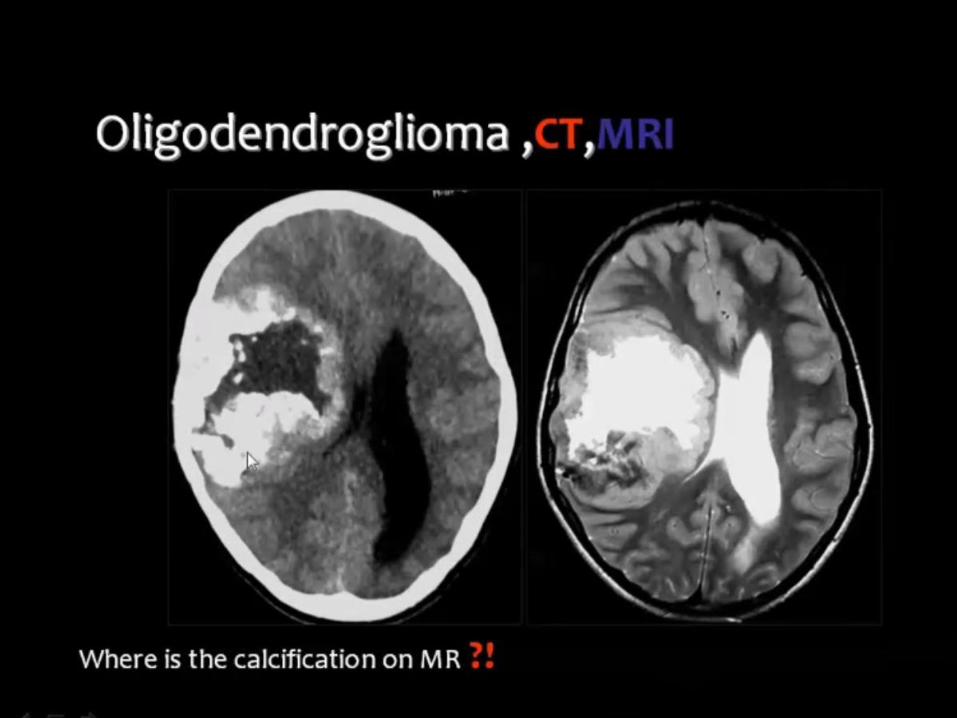
Oligodendroglioma • Heterogeneous, Ca++ mass
• Typically larger and more diffuse than PXA
• May remodel/erode calvarium
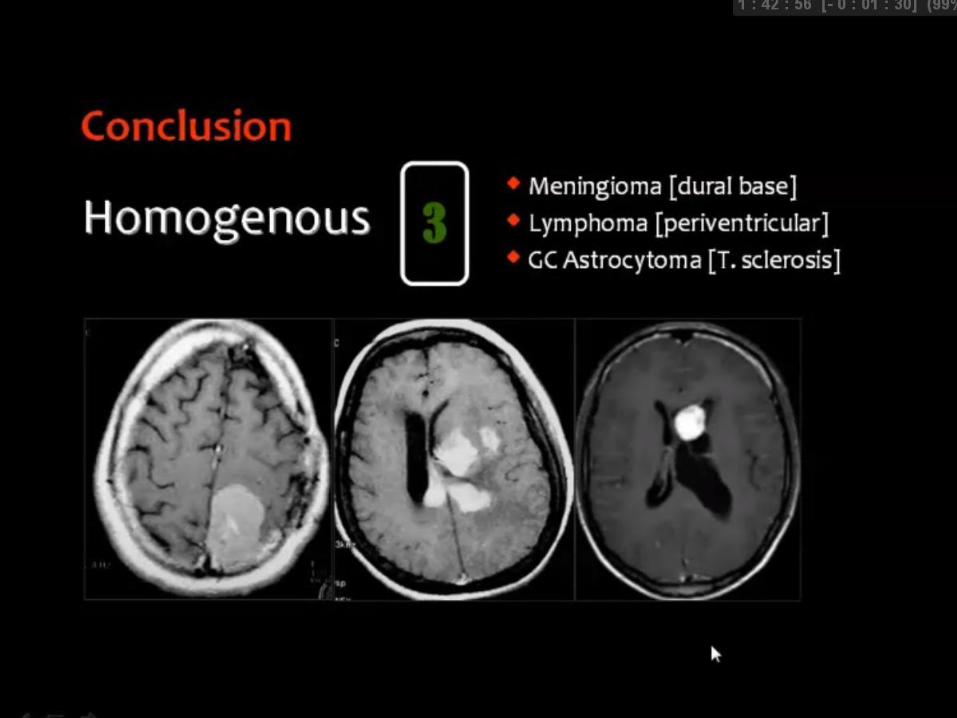
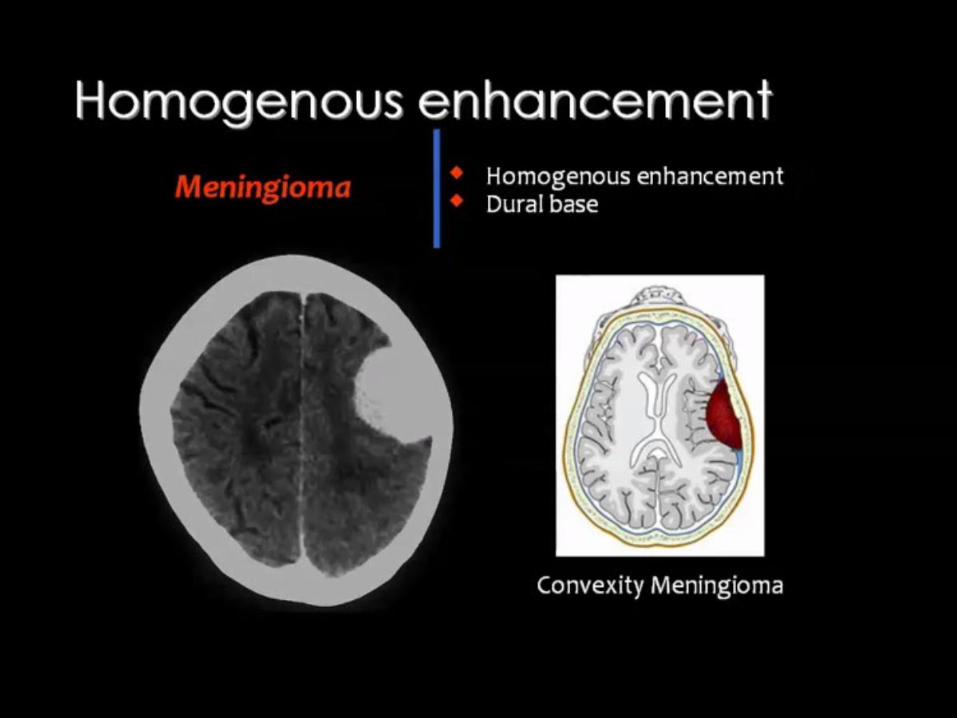
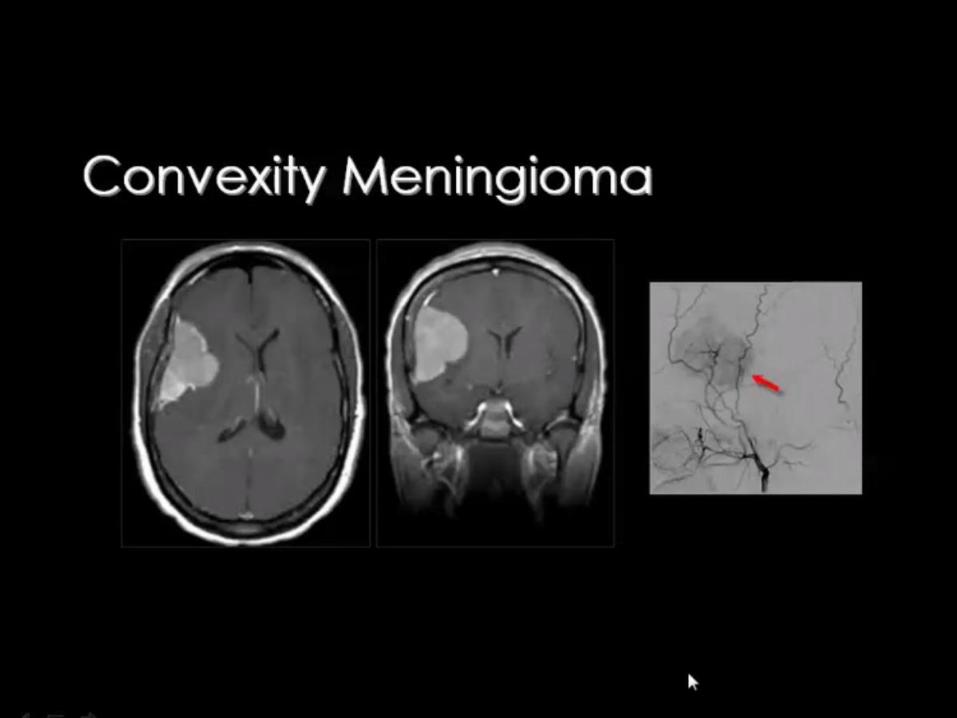
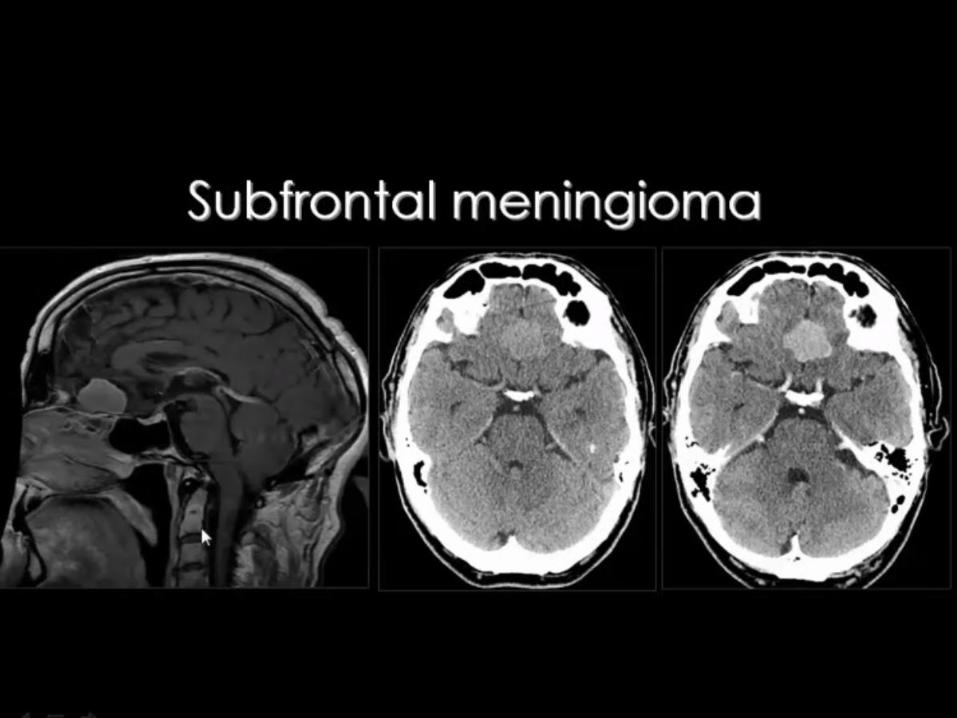
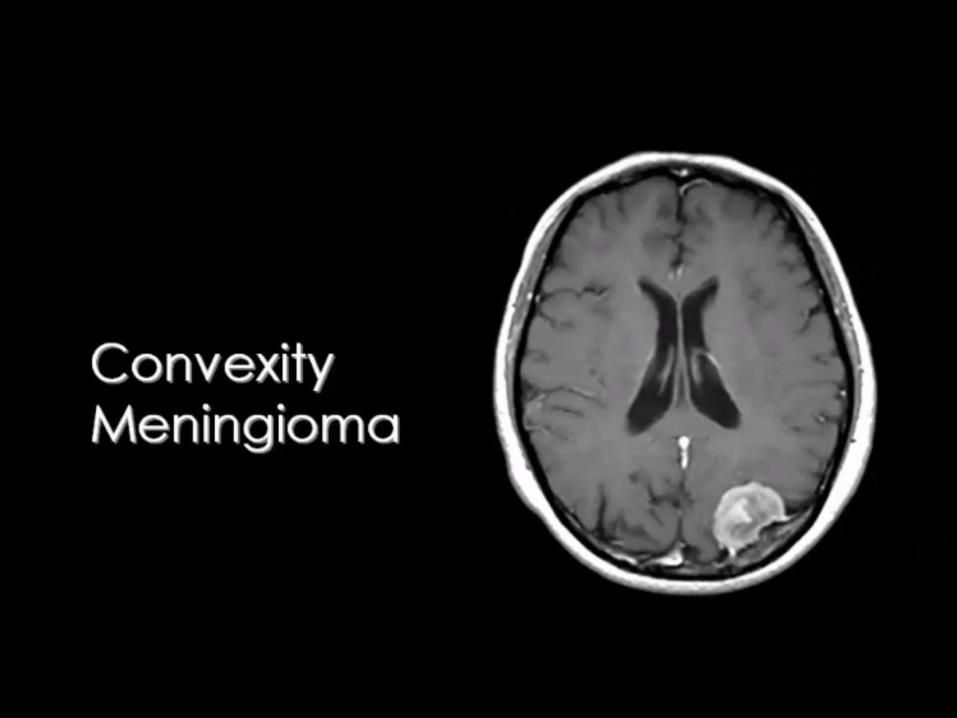
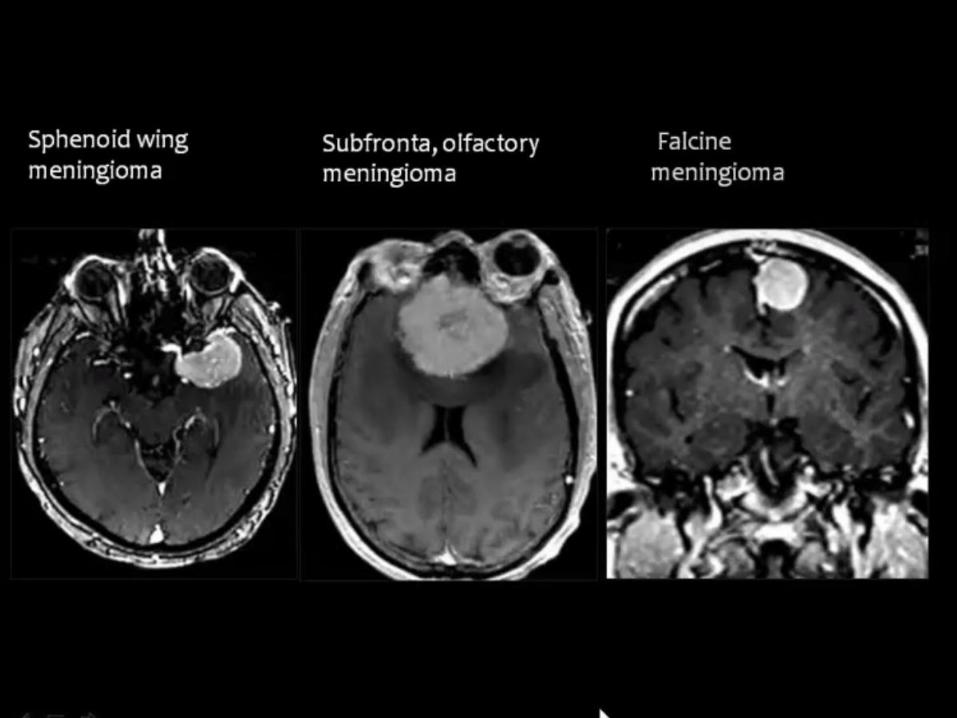
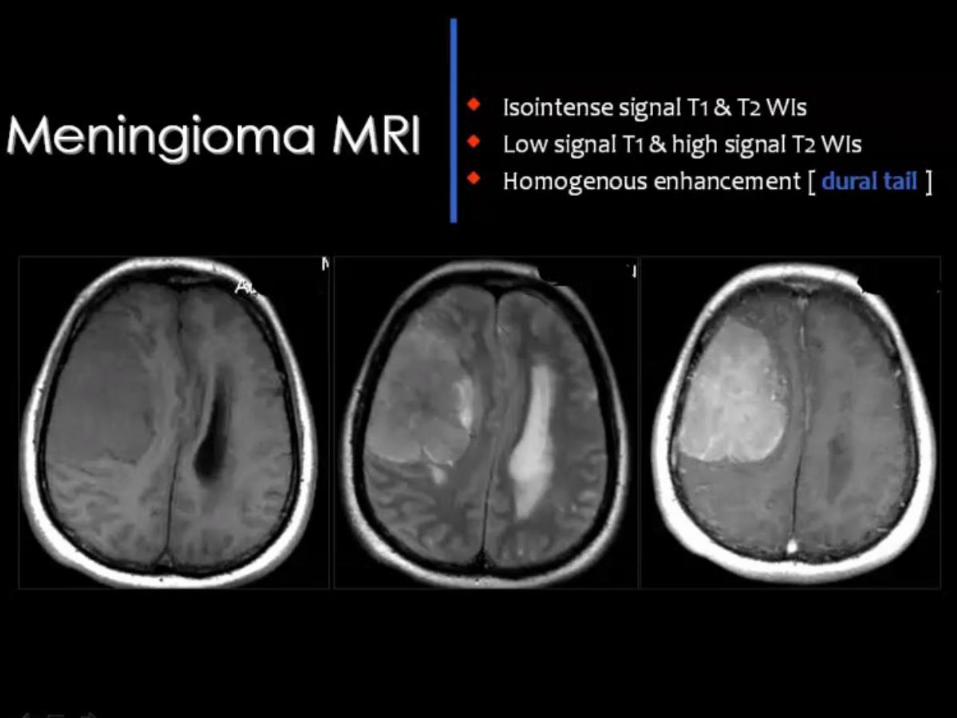
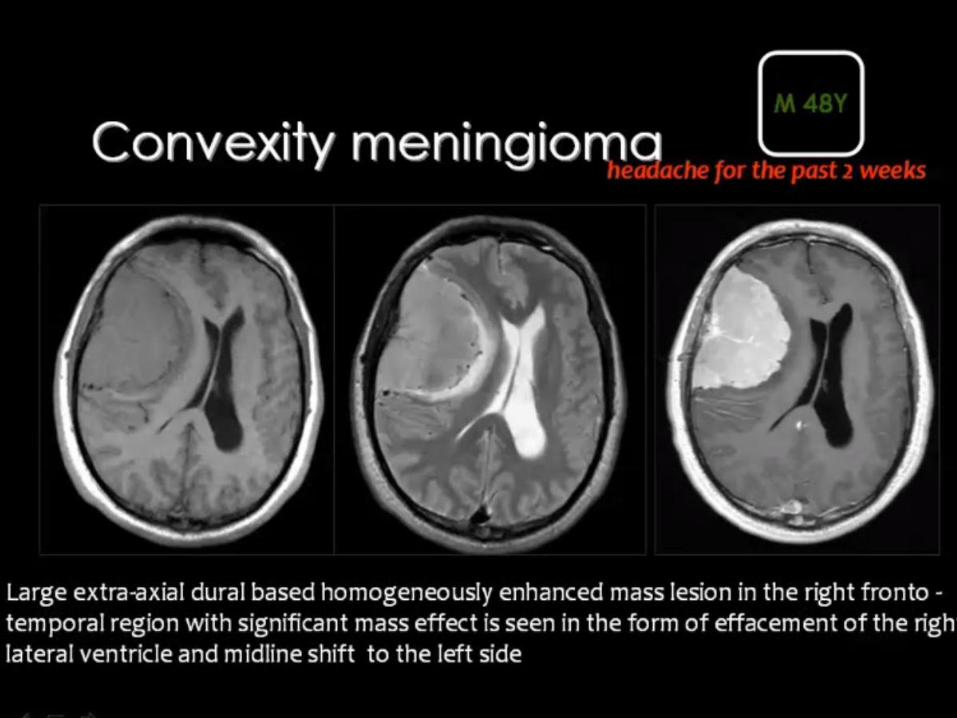
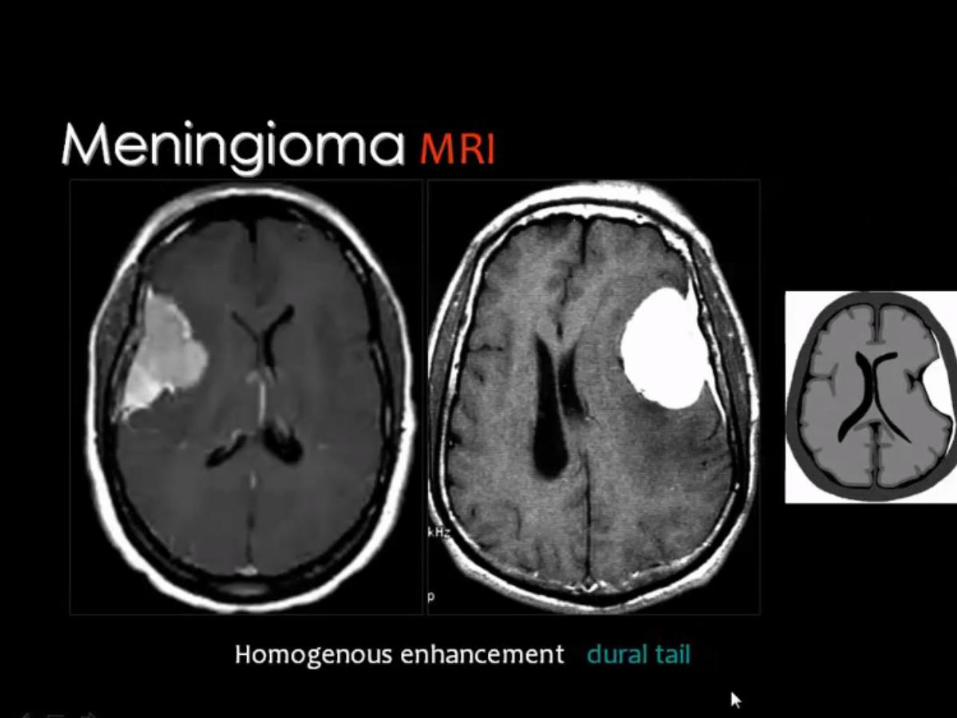
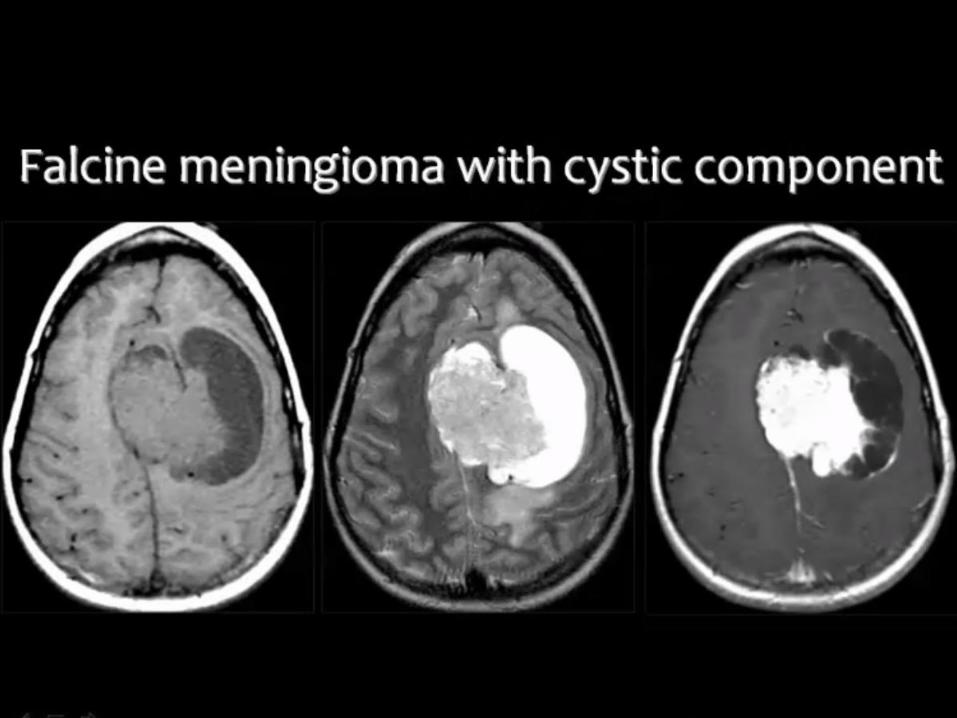
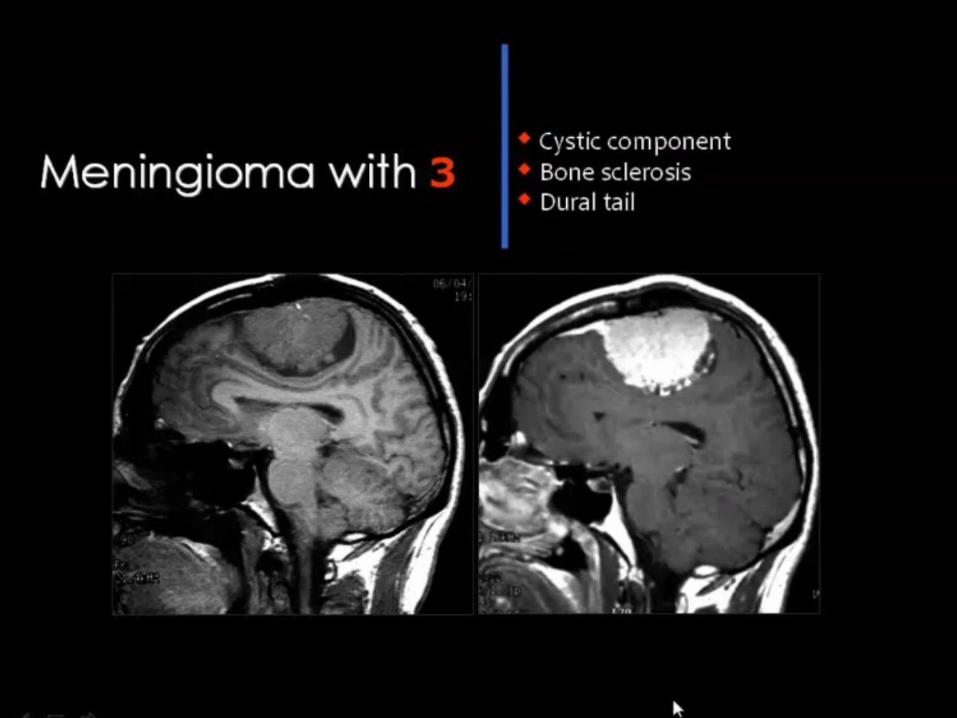
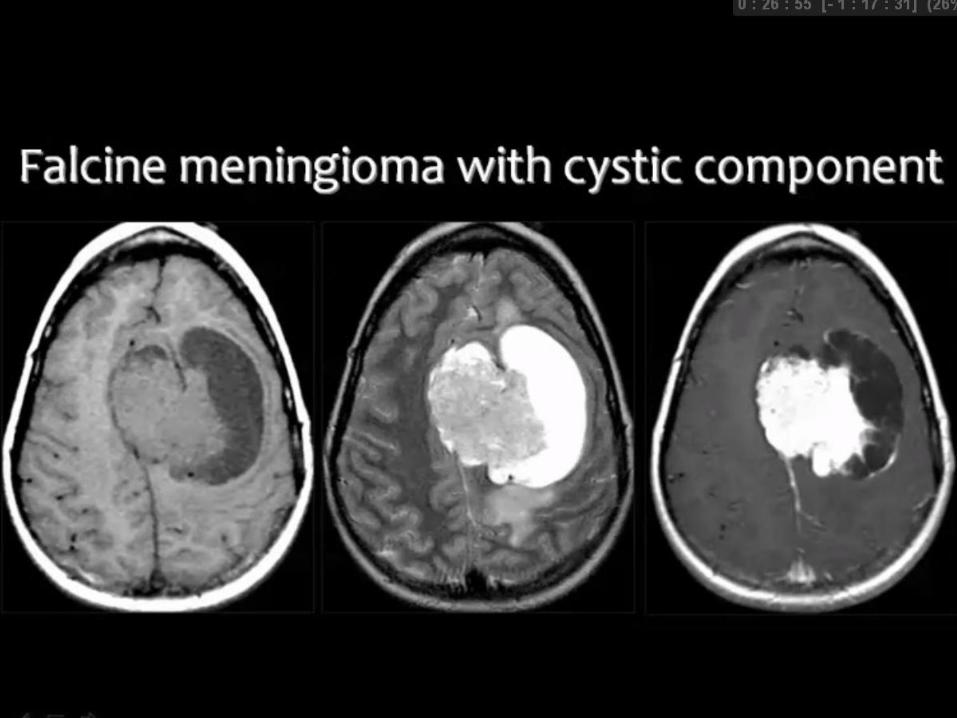
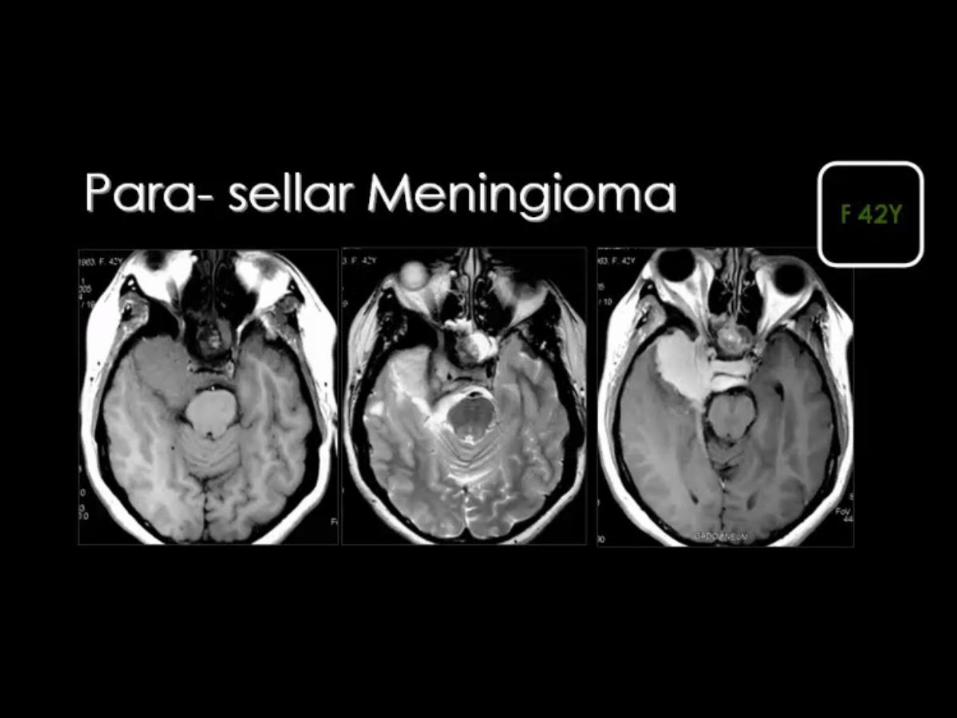
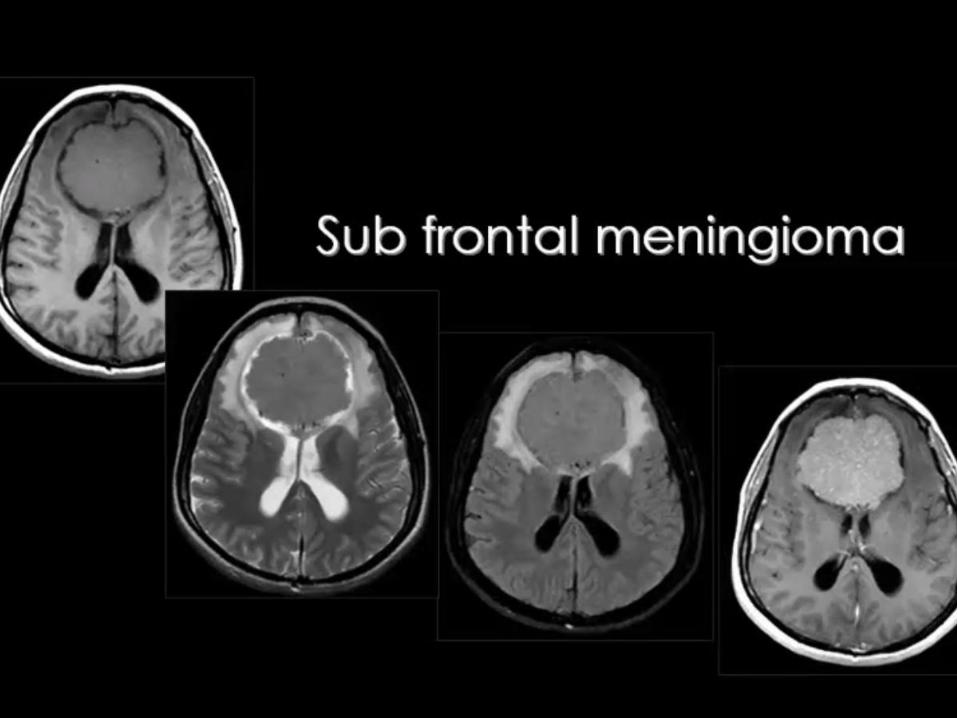
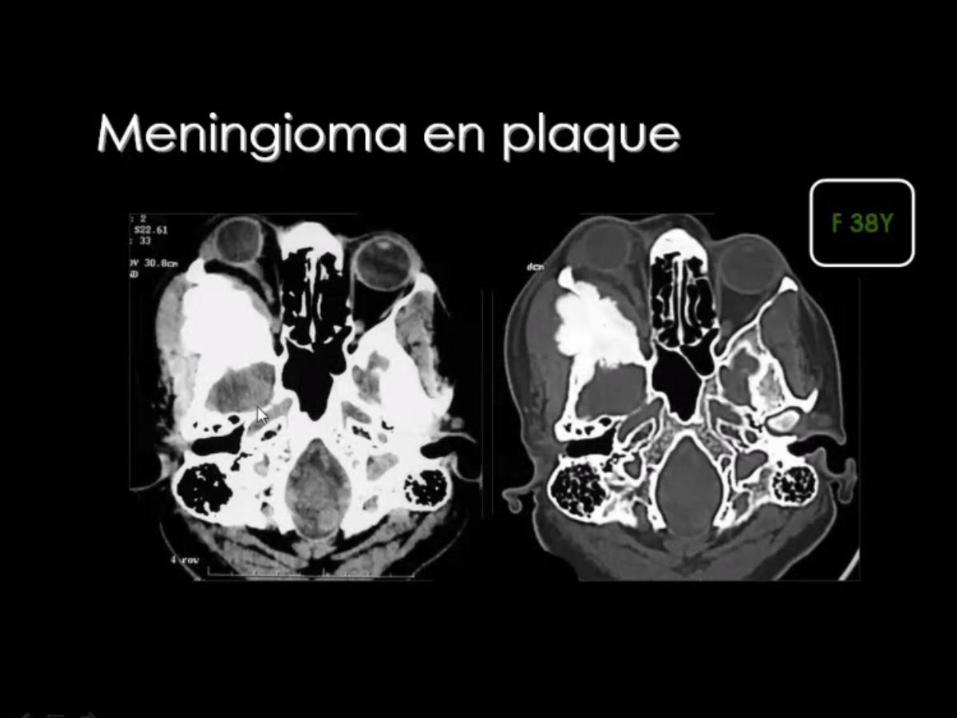
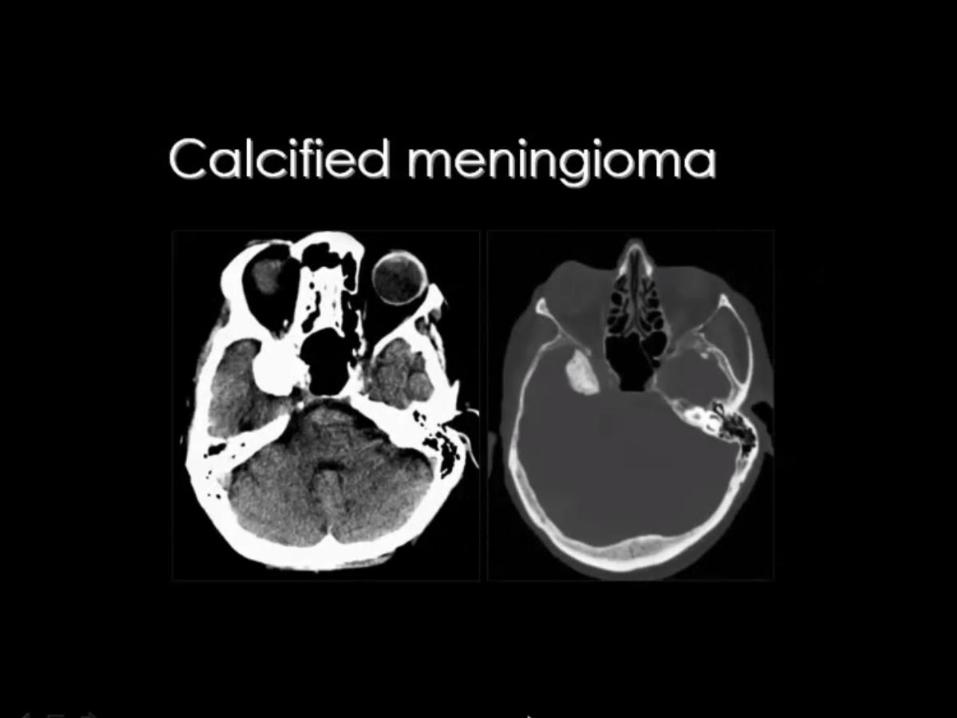
Meningioma • Diffusely enhancing dural-based mass with dural "tail"
• Usually older patients
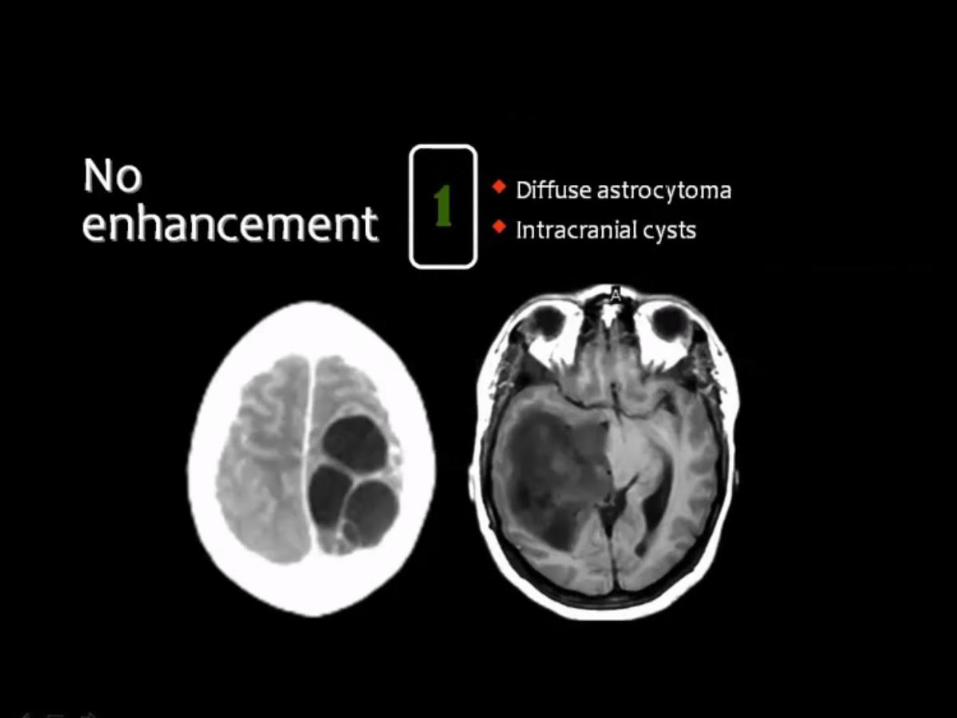
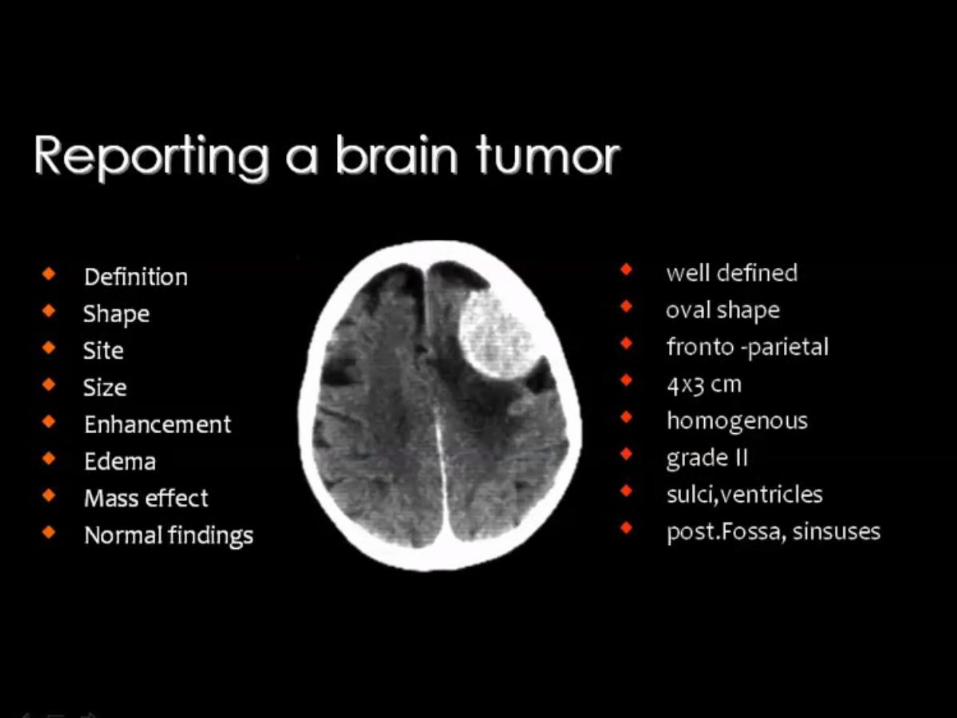
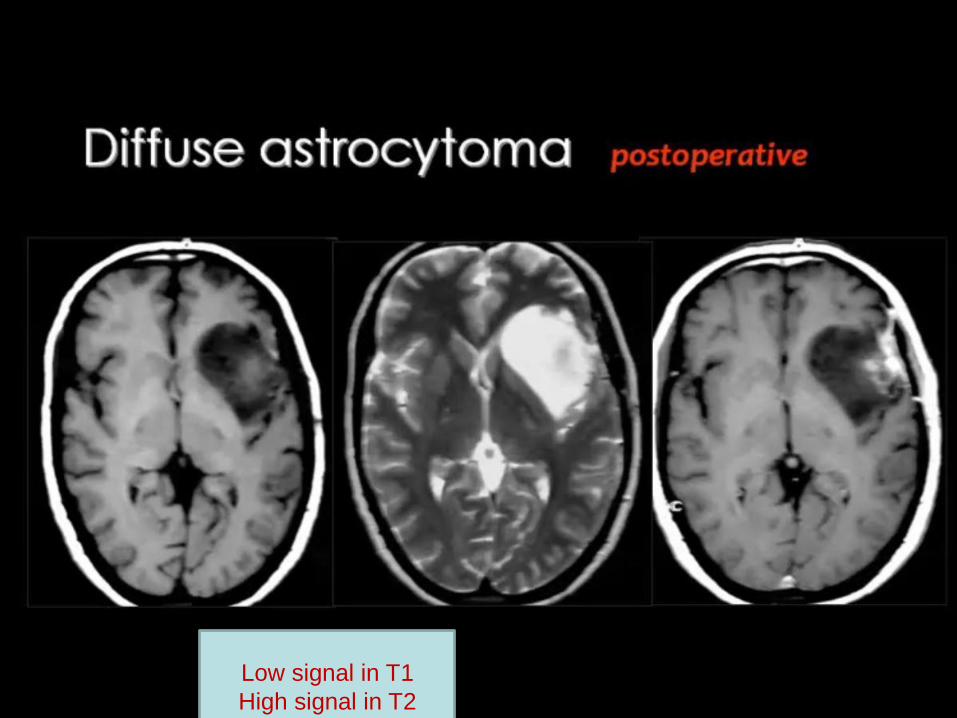
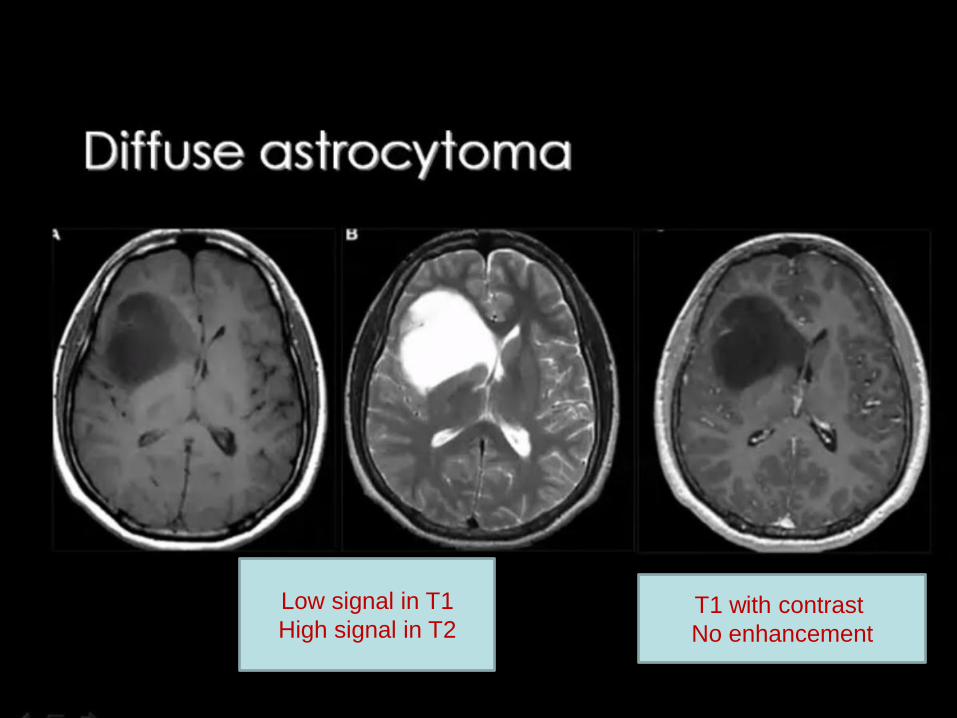
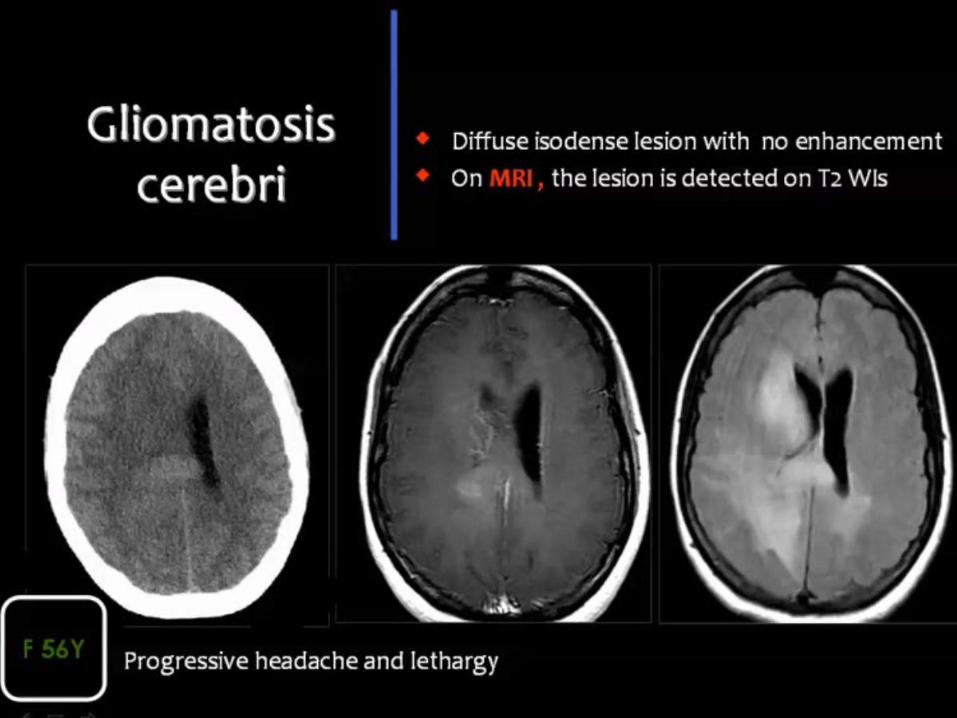
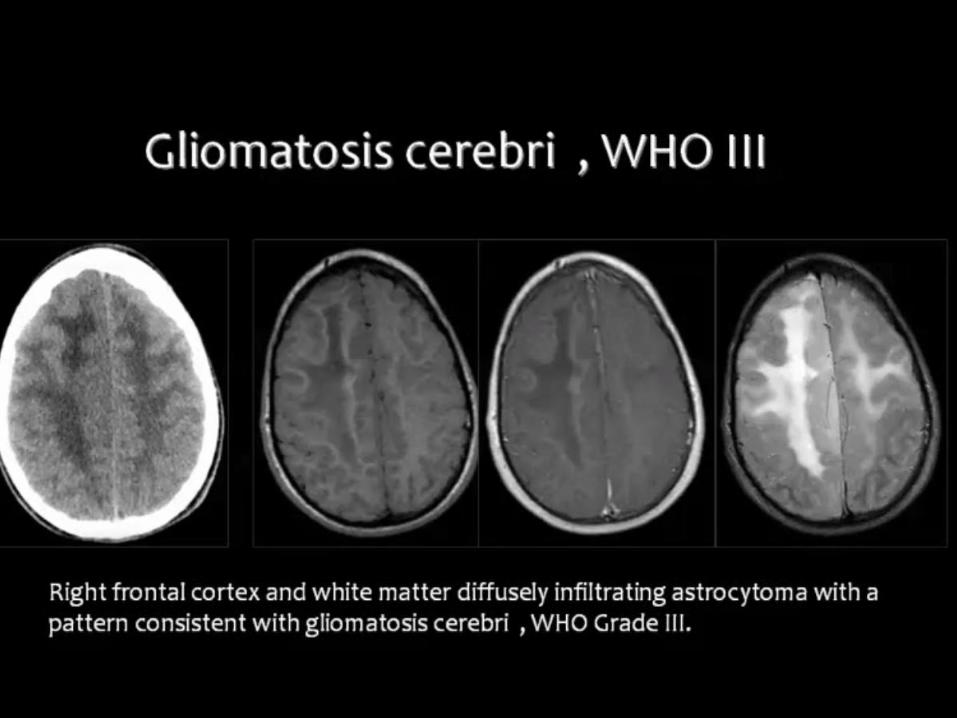
Low grade astrocytoma (Grade II) • Demarcated but infiltrative white matter mass
• No enhancement
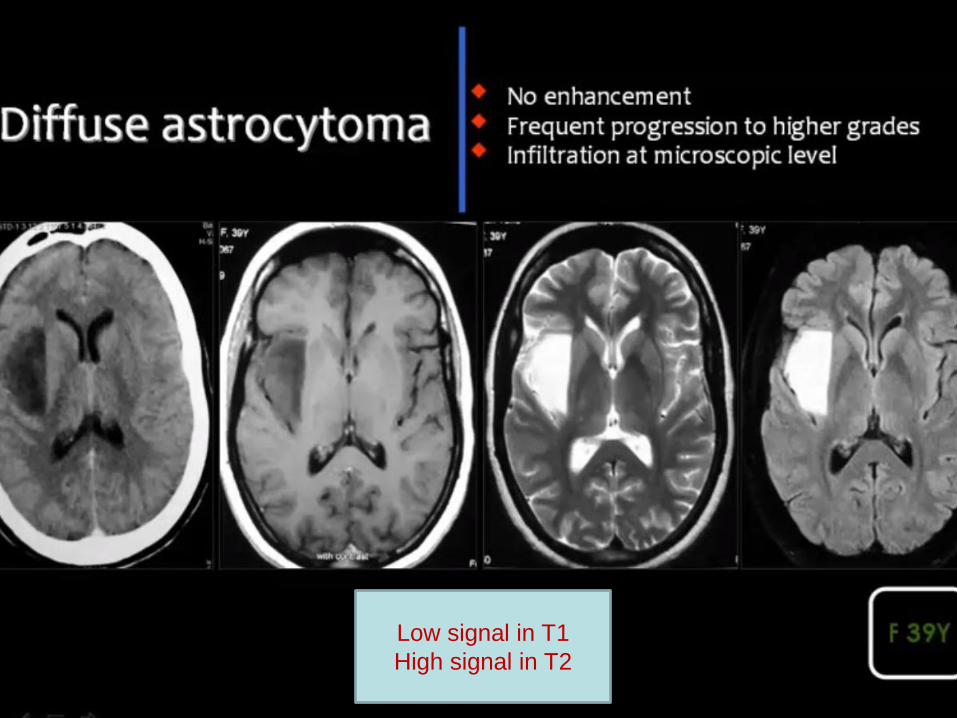
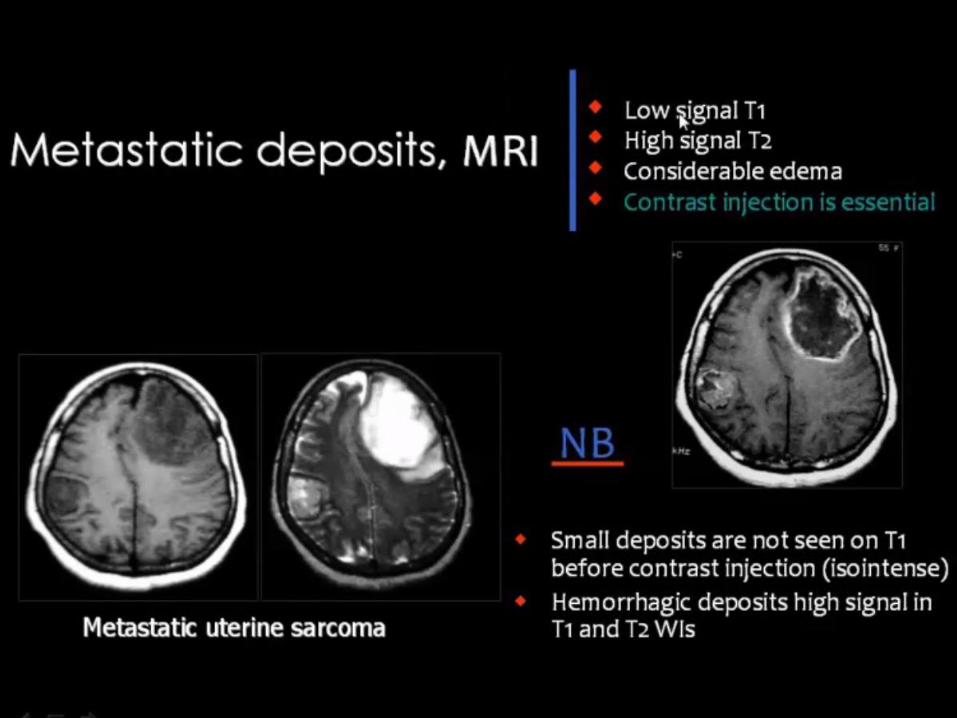
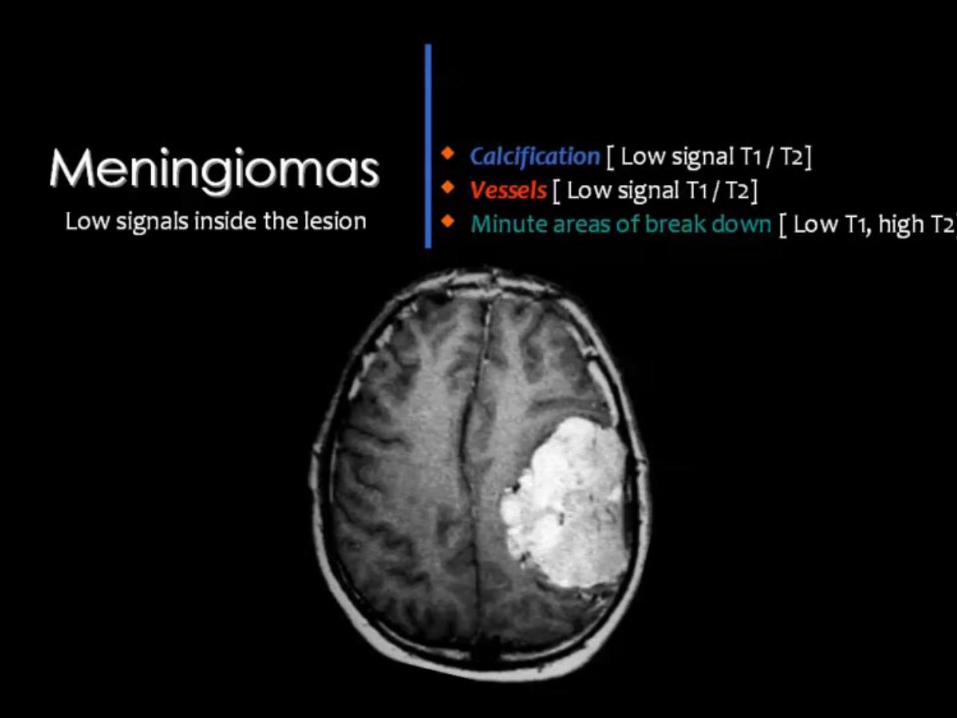
Low signal in T1
High signal in T2
Low signal in T1
High signal in T2
Low signal in T1
High signal in T2 T1 with contrast
No enhancement
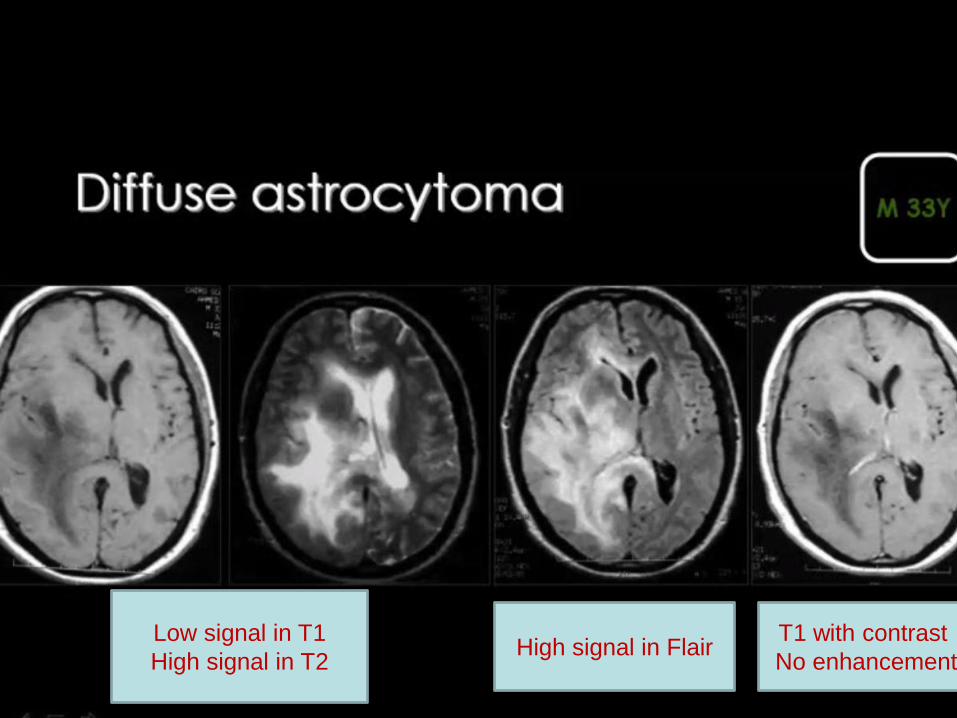
Low signal in T1
High signal in T2
T1 with contrast
No enhancement High signal in Flair
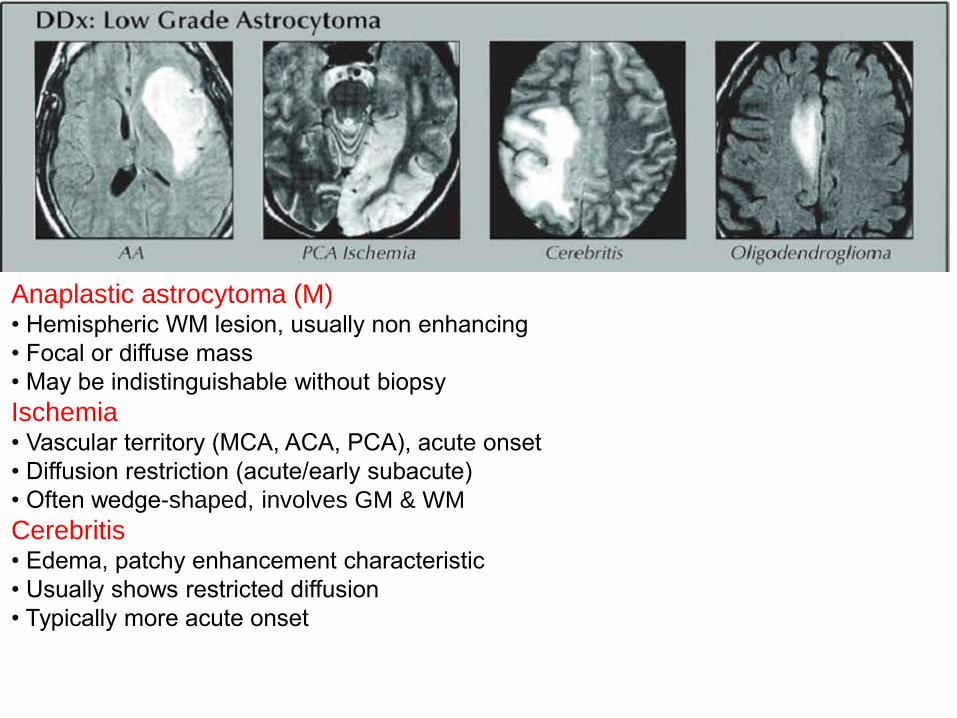
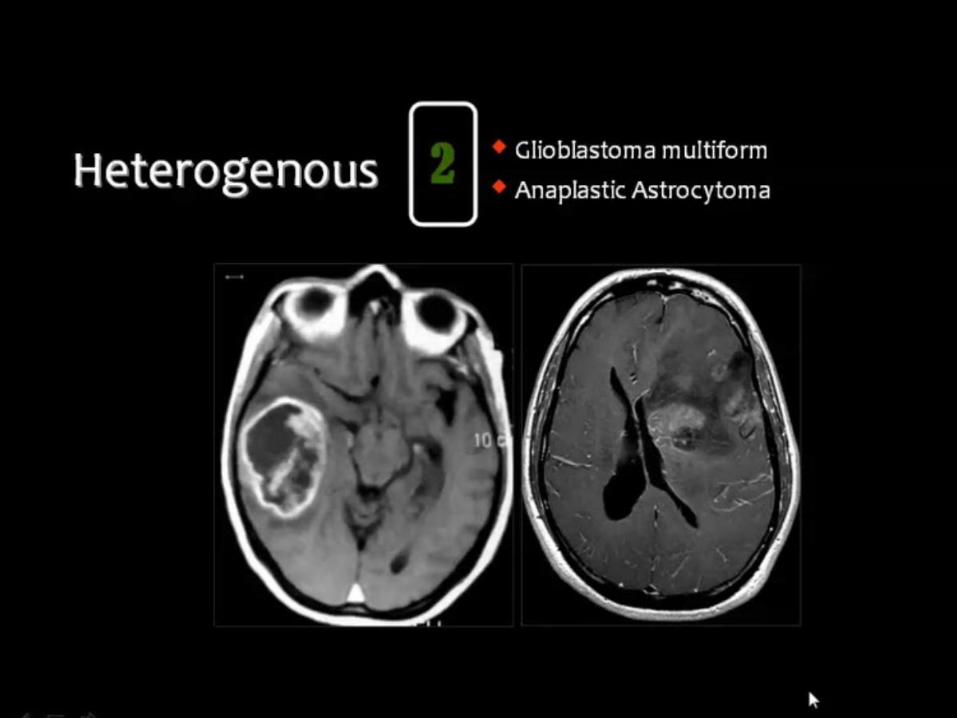
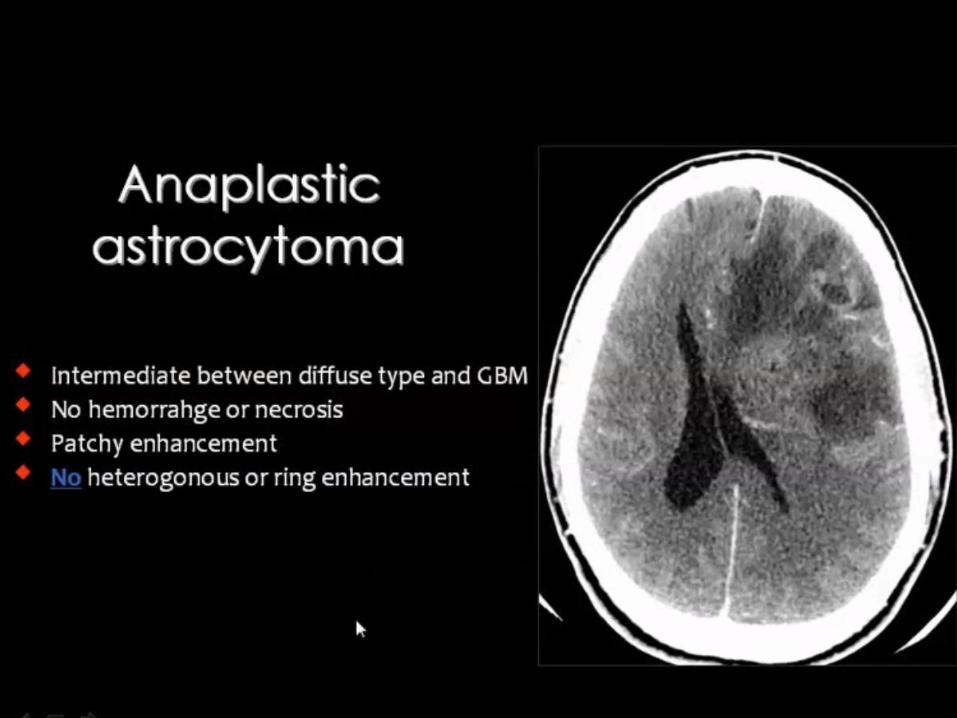
Anaplastic astrocytoma (M) • Hemispheric WM lesion, usually non enhancing
• Focal or diffuse mass
• May be indistinguishable without biopsy
Ischemia • Vascular territory (MCA, ACA, PCA), acute onset
• Diffusion restriction (acute/early subacute)
• Often wedge-shaped, involves GM & WM
Cerebritis • Edema, patchy enhancement characteristic
• Usually shows restricted diffusion
• Typically more acute onset
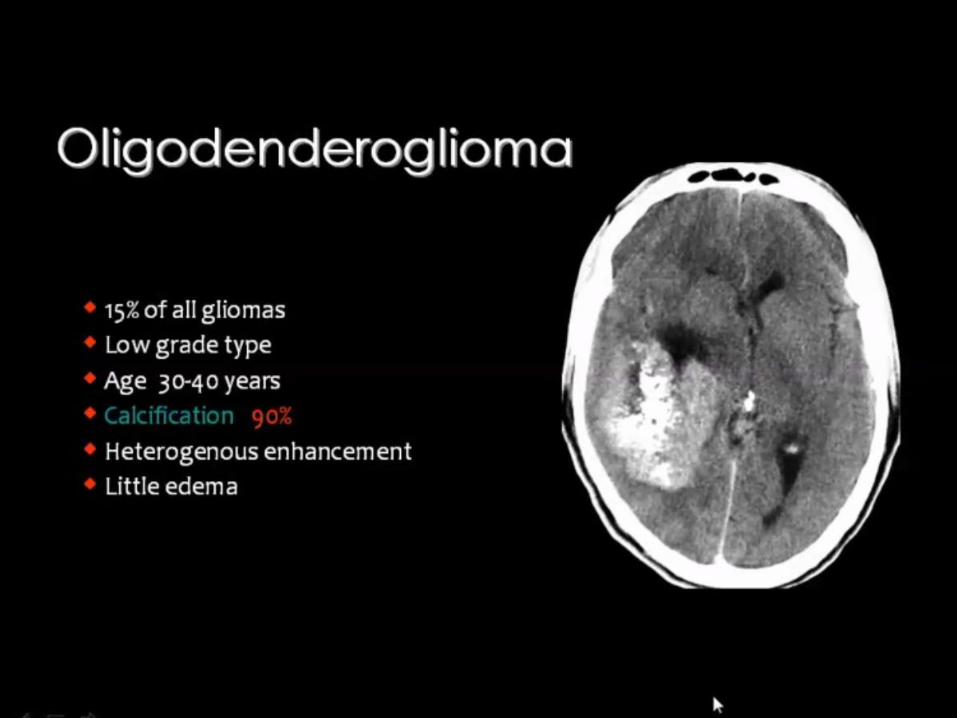
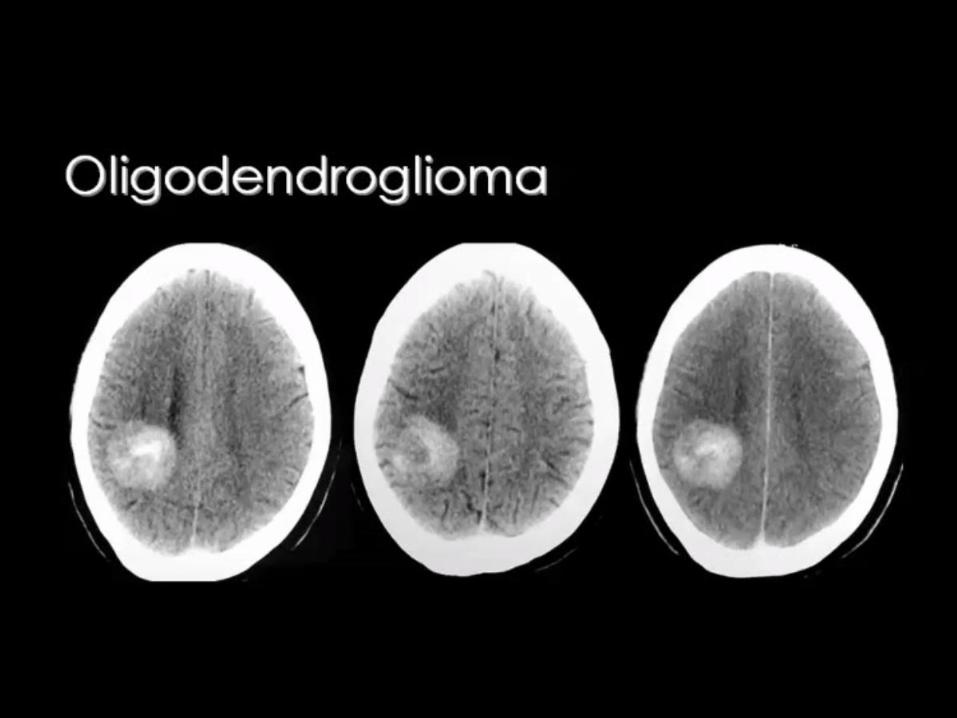
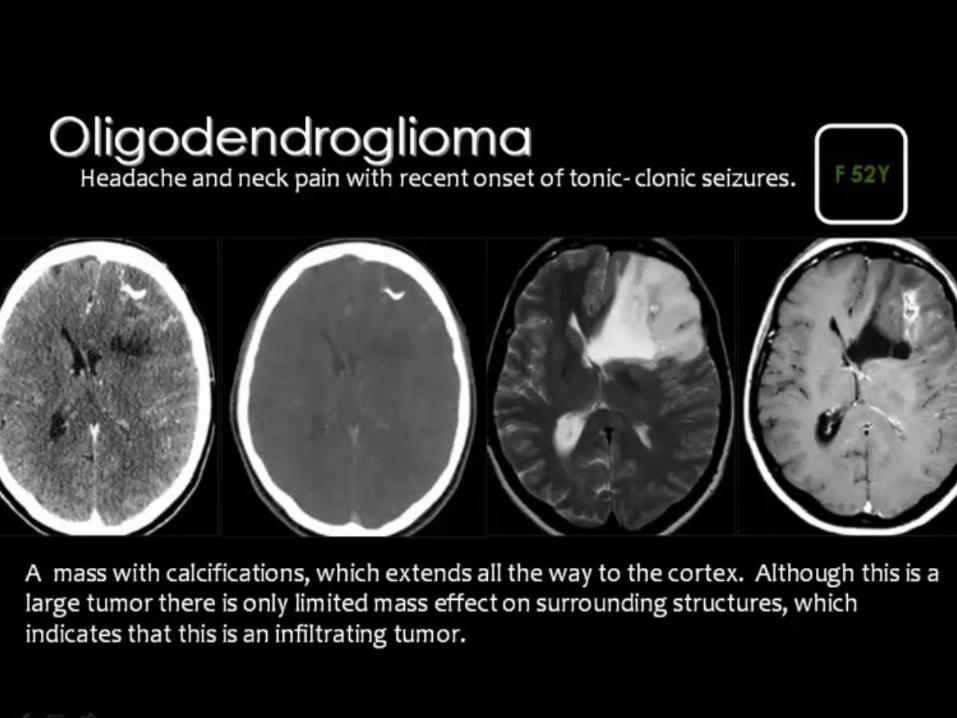
Oligodendroglioma
• Cortically-based mass with variable
enhancement
• Ca++ common
• May be indistinguishable
Herpes encephalitis
• Confined to limbic system, temporal lobes
• Hemorrhage and enhancement common
• Acute onset
Herpes encephalitis
• Confined to limbic system, temporal lobes
• Hemorrhage and enhancement common
• Acute onset
Status epilepticus
• Active seizures may cause signal
abnormalities and
enhancement
• Clinical history of seizures
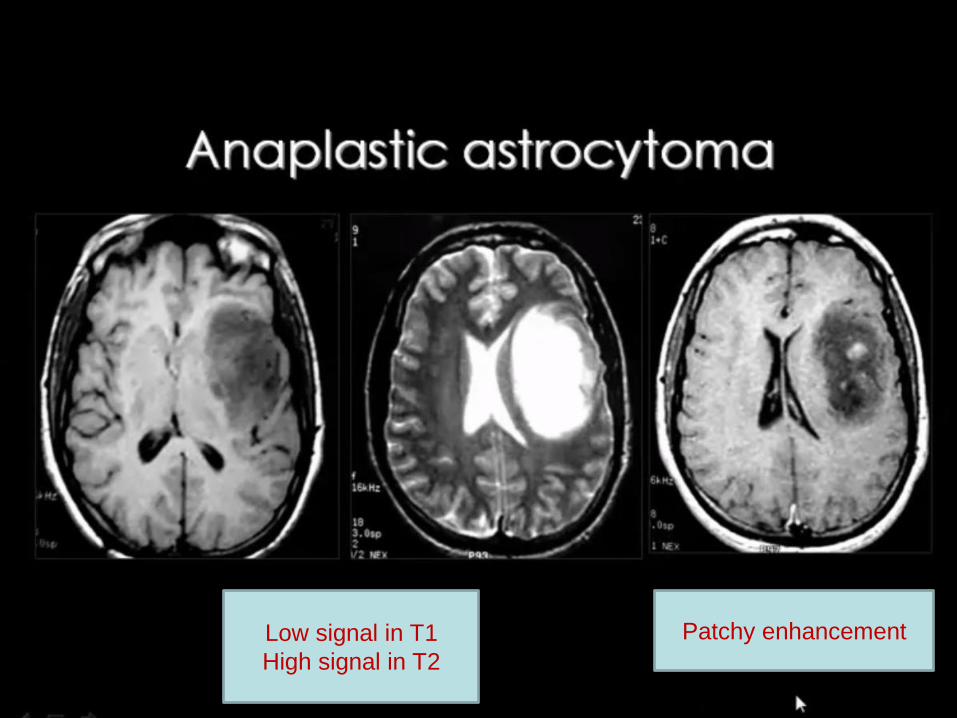
Low signal in T1
High signal in T2
Patchy enhancement
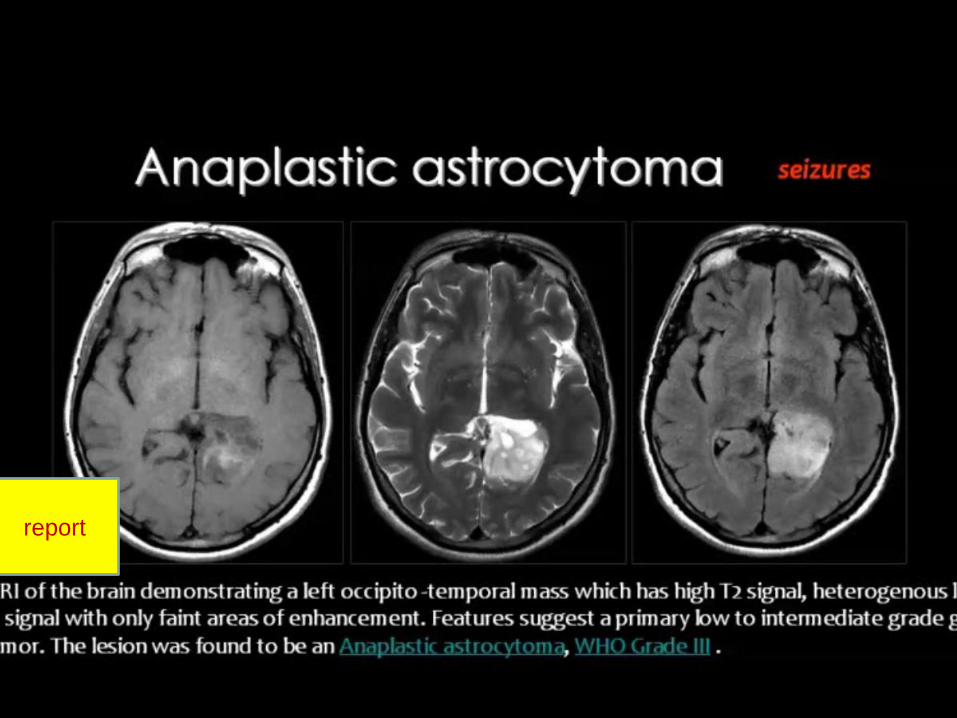
report

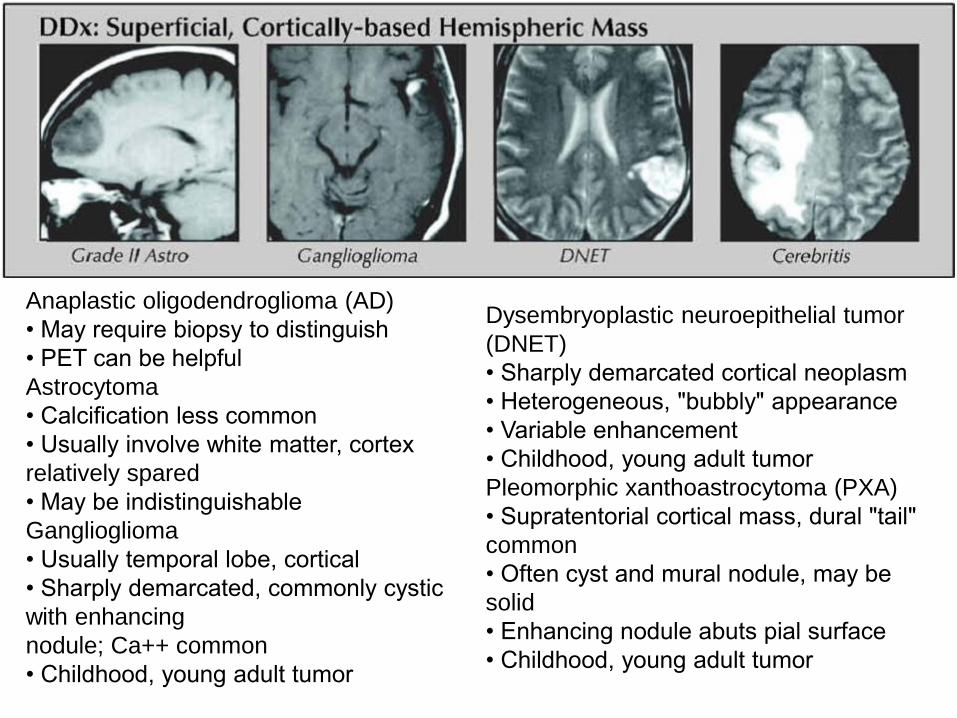
Anaplastic oligodendroglioma (AD)
• May require biopsy to distinguish
• PET can be helpful
Astrocytoma
• Calcification less common
• Usually involve white matter, cortex
relatively spared
• May be indistinguishable
Ganglioglioma
• Usually temporal lobe, cortical
• Sharply demarcated, commonly cystic
with enhancing
nodule; Ca++ common
• Childhood, young adult tumor
Dysembryoplastic neuroepithelial tumor
(DNET)
• Sharply demarcated cortical neoplasm
• Heterogeneous, "bubbly" appearance
• Variable enhancement
• Childhood, young adult tumor
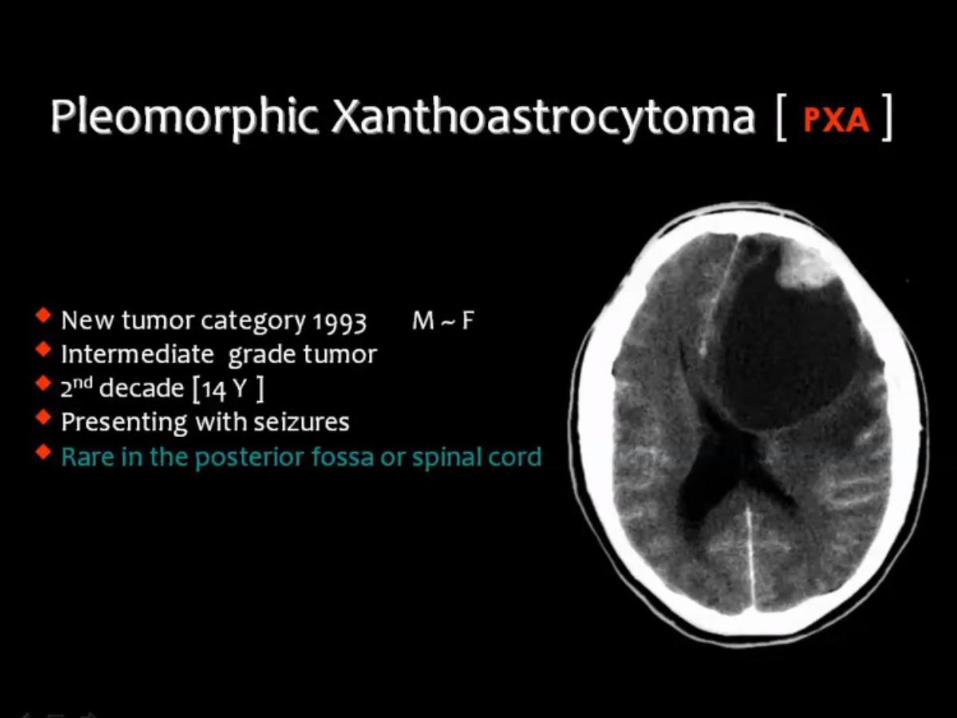
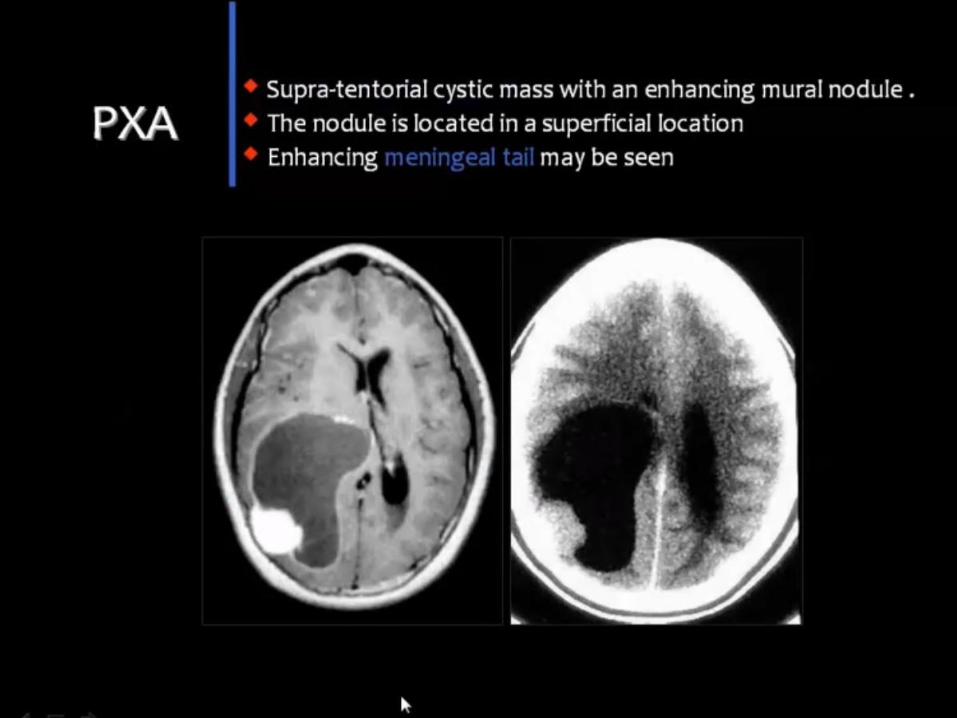
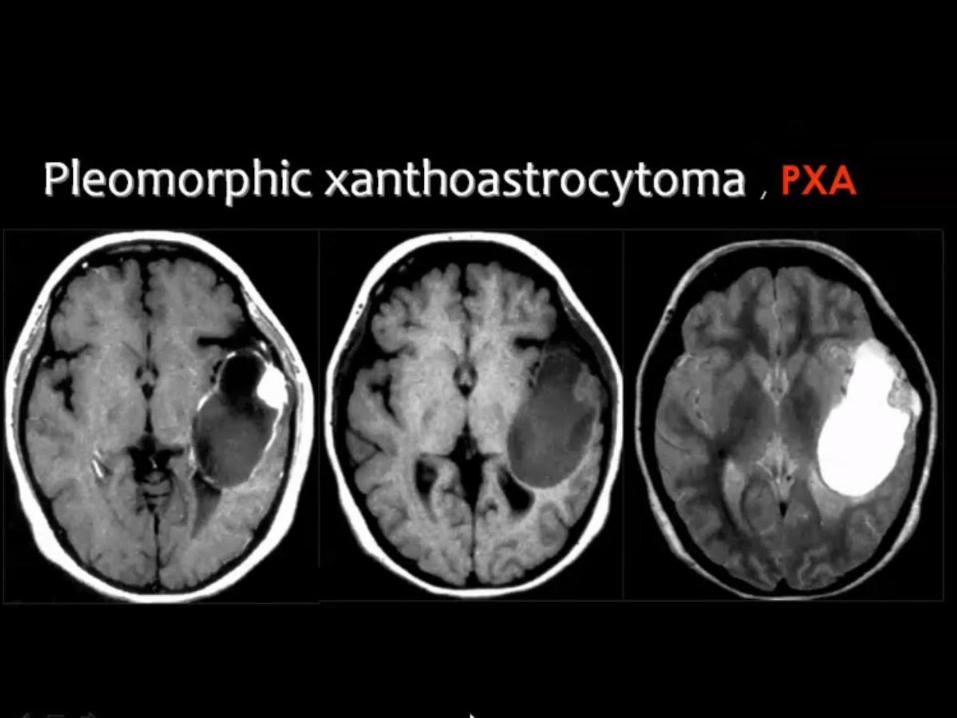
Pleomorphic xanthoastrocytoma (PXA)
• Supratentorial cortical mass, dural "tail"
common
• Often cyst and mural nodule, may be
solid
• Enhancing nodule abuts pial surface
• Childhood, young adult tumor
Cerebritis
• T2 hyperintensity and patchy enhancement
• Diffusion restriction typical
Ischemia
• Typical vascular distribution (MCA, ACA, PCA)
• Diffusion restriction if acute/subacute
• Involves GM and WM, often wedge-shaped
• Cortical, gyriform enhancement if subacute
Arteriovenous malformation (AVM)
• Typically multiple enlarged flow voids
• Often calcified
• If thrombosed, may be indistinguishable
Herpes encephalitis
• Confined to limbic system, temporal lobes
• Blood products and enhancement common
• Acute onset is typical