brainstem pathways, reflexes - iresys medical portaliresys.com/browsable/histology/eagyt.pdf ·...
TRANSCRIPT

Brainstem pathways, reflexes


• Ascending tracts• 1. going through brainstem
– spinothalamic tract– ant., post., rostral spinocerebellar
• 2. ending in brainstem– Fasciculus gracilis, cuneatus– spinoreticular tract
• 3. beginning in brainstem– medial lemniscus– trigeminal and dorsal trigeminal lemniscus – lateral lemniscus– to cerebellum: olivocerebellar, cuneocerebellar,
pontocerebellar– nigrostriatal tract– Monoaminergic tracts

sensory systemsoverview
somatosensory viscerosensory
protopathic
(organs)
epicritic
proprioceptive
spinothalamic tract+ trigeminal lemniscus
ant. post spinocerebellar
dorsal column/medial lemniscus+ dorsal trigeminal lemniscus
(dorsal column/medial lemniscus)
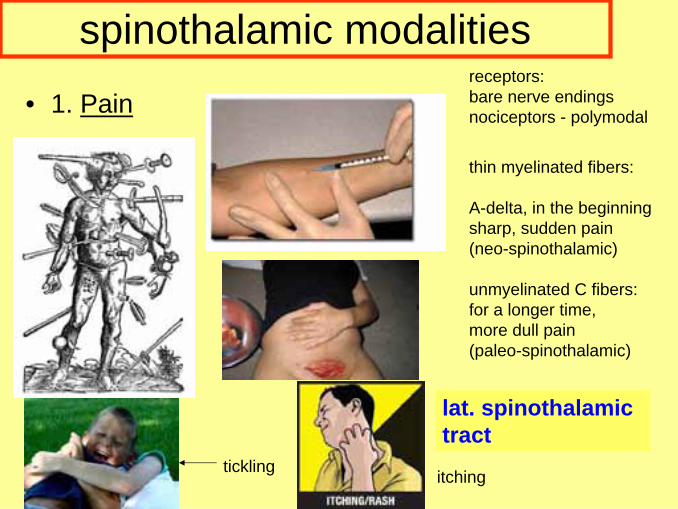
• 1. Pain
lat. spinothalamictract
receptors:bare nerve endingsnociceptors - polymodal
thin myelinated fibers:
A-delta, in the beginningsharp, sudden pain(neo-spinothalamic)
unmyelinated C fibers:for a longer time,more dull pain(paleo-spinothalamic)
tickling itching
spinothalamic modalities

• 2. Temperature
lat. spinothalamic tract
warm receptors:
free nerve endings
C fibers
(active: 35-45 oC)cold receptors: bare (free) nerve endingsA delta fibers, aktiv: <35 oC, >45 oC (!)(Paradox: goosebumps in hot water!)
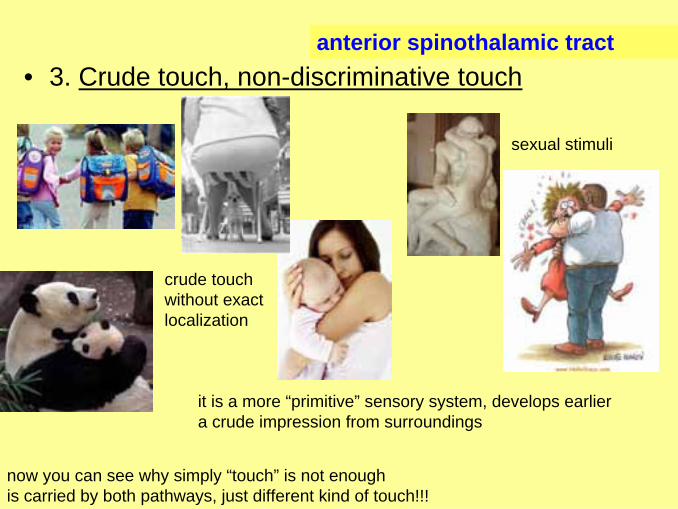
• 3. Crude touch, non-discriminative touch
crude touchwithout exactlocalization
sexual stimuli
anterior spinothalamic tract
now you can see why simply “touch” is not enoughis carried by both pathways, just different kind of touch!!!
it is a more “primitive” sensory system, develops earliera crude impression from surroundings

• 4. viscerosensory fibers run in spinothalamicsystem – poor localization!!!

epicritic sensibility/dorsal column medial lemniscus modalities
fine touch-discriminative touch(2-point discrimination) pressure,vibration
EXACT localization
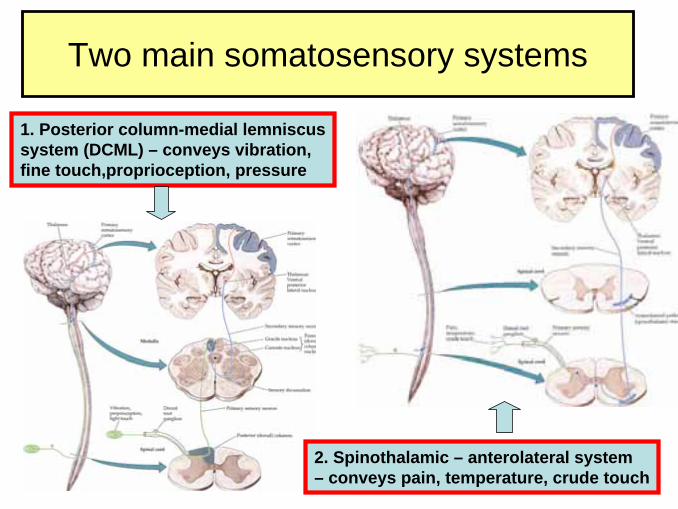
Two main somatosensory systems
1. Posterior column-medial lemniscussystem (DCML) – conveys vibration, fine touch,proprioception, pressure
2. Spinothalamic – anterolateral system– conveys pain, temperature, crude touch

the two sensory systems converge, and reach thalamus together - end in VPL
spinal cord
Medulla
Medulla
pons
Mesenc

proprioception
muscle spindle, Golgi tendon organ, (Pacini corpuscles)remember: proprioceptive information:• proprioceptive reflex • spinocerebellar system ant. and post • dorsal column- medial lemniscus system – for LOCALIZATION
and CONSCIOUS BODY POSITION

cerebellar tracts• 3 main inputs to cerebellumall starting or going through brainstem
1. vestibular: vestibulocerebellar tract2. spinal cord: spinocerebellar tracts3. cortex – pons- pontocerebellar tracts
(others:olivocerebellar, reticulocerebellar etc)
brainstem- cerebellum – 3 Pedunculi

face/head area somatosensoryinformation– n. V.
nucl. spinaltract of
n V
princ. nucl..of n V
mesnucl
of n V.
temp, pain, crude touch
vibration, fine touch
proprioceptive
trigeminallemniscus
dorsalistrigeminallemniscus
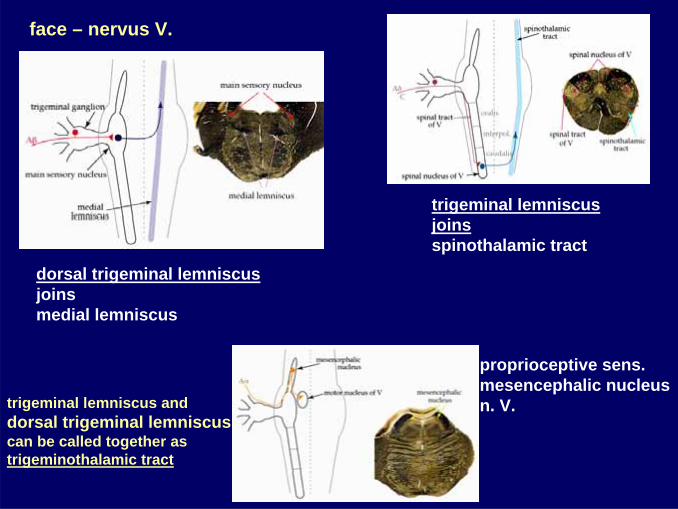
face – nervus V.
trigeminal lemniscus joinsspinothalamic tract
proprioceptive sens.mesencephalic nucleusn. V. trigeminal lemniscus and
dorsal trigeminal lemniscuscan be called together astrigeminothalamic tract
dorsal trigeminal lemniscusjoins medial lemniscus

Examination
pain (pinprick test)–spinothal.
2-point discriminationfine touch - DCML
VibrationDCML
graphesthesiaDCML
temperaturespinothal.
http://www.prohealthsys.com/physical/sensory.php
cottontip-light touchnot specific for eitherpathway!!!
position senseDCML

Spinocerebellar contra dorsal column ataxia
spinocerebellar:
always ataxia
dorsal column:
increased ataxiain darknessor closing the eyes
visual inputcan compensate
Romberg test positive

blind and deaf– what remains?Helen Keller- a true storyonly somatosensory info
today: pregnancyviral infections –eg. CMV, rubella
At the age of 18 months, encephalitis??, is left blind and deafthe family found a teacher when she was 6, she taught her with drawingon her hand!! , Helen did her doctoral thesis (!!) in comparative literature


descending tracts
somatomotorvisceromotor
from motor centers from autonomic centers
Hypothalamus
hypothalamospinal tract
spinal cord lateral horn
-pyramidal tract
-other motor tracts-1. rubrospinal-2. tectospinal-3. vestibulospinal-4. reticulospinal-5. olivospinal
brainstem

• descending tracts• 1. going through brainstem
– corticospinalis (pyramidal tract) – hypothalamospinal
• 2. ending in brainstem– corticonuclear tract (pyramidal tract)– corticopontine– corticorubral
• 3. ending in brainstem– tectospinal– vestibulospinal– rubrospinal– reticulospinal– monoaminergic tracts (eg. raphespinal)
medial longitudinal fascicle / begins and ends in brainstem, both ascending and descending

PyramisDecussatio pyramidorum
Medulla Oblongata:
Capsulainterna
spinal cord: Neuron 2. interneuron (10% direct motoneuron)Neuron 3. Motoneuron – ant. horn
motor cortex(Br 4,6, 3,1,2):
Neuron 1
Mesencephalon:Pedunculuscerebri
Neuron 2. brainstemmtor brainstem nucleiV → masticationVII → facial expressionIX, X → pharynx, larynxXII → tongue
corticonuclear(corticobulbar,
corticomesencephal.
Tr. corticospinalis- cruciatus (oldalköteg)- directus (elülső köteg)
1. pyramidal tract

MesencephalonCrus cerebriMitte
Pons:Basis
Medulla:Pyramis
Medulla:Decussatio
Tr. cortico-spinalislat/cruciatus
Tr. corticospinalis ant/directus
spinal cord
corticospinal tract – gors through brainstem
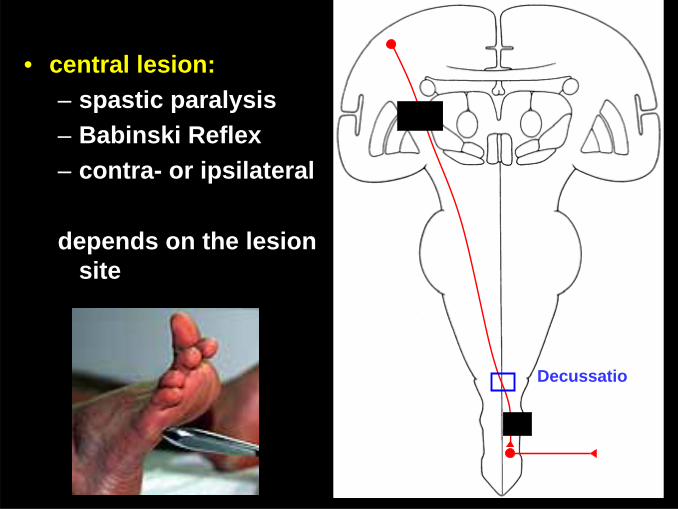
• central lesion:– spastic paralysis– Babinski Reflex– contra- or ipsilateral
depends on the lesion site
Decussatio

facial n. trigeminal n.corticonuclear (corticomesencephalic, corticobulbar)
partially bilateral innervation!!
n. X n. XII

clinical
• central lesion:= supranuclear• peripheral= in nucleus or after

facial nerve palsy
central
peripheral

facial nerve palsy
central – contralateral, BUT
forehead, m. orbicularis oculi functionsperipheraltotal ipsilateral palsy
eg. internal capsule lesion eg. inflammation in facial canal, acustic neurinoma.
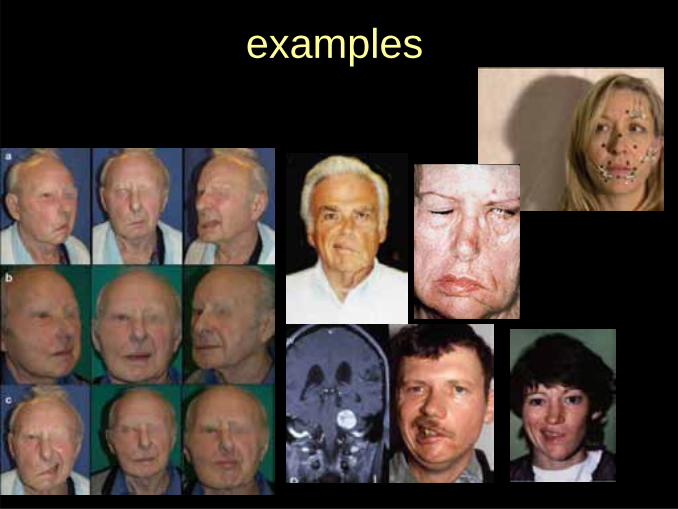
examples

other cranial nerve palsy: IX, X, XII

„Extrapyramidal” tract
proximál muscles
mimic
tone
automatic movements (driving)

1. rubrospinal – nucleus ruberstimulates flexorsinhibits extensorswith the pyramidal tract responsible for FiNEmovements
bigger role in an alreadylearnt movement

2. tectospinal tract Retina
Colliculus superior
spinal cord
Tractustectospinalis
Tr. opticus
HAMM...
head movesto visual stimuli

•lateral vestibulospinal tract:from nucleus vestibularis lateralis –all through spinal cordstimulates extensorpostural stabilization
3. vestibulospinas
•medial vestibulospinal tract:
nucleus vestibularis medialis, only cervical and upper thoracal spinal cordcoordinates head movements

4. reticulospinal –Formatio reticularis (Pons, Medulla)
medialis : pons
tone, reflexes
bilateral
lateralis: medulla

brainstem reflexes
1. monosynaptic, proprioceptive reflex:
nucleusmesencephalicusn. trigemini (V)
PonsNucleusmotorius
n. trigemini (V)
Receptor:masseterspindle
afferent(N. V/3)
efferentsN. V/3
masseter reflex
2. polysynapticreflexes
-autonomic reflexes:see reticular formationrespir, cardiac, vomiting etc

Facial reflexesCornea Reflexafferent: N. V/1
strong light:Afferent: optic nerve-Colliculus superior-n. facialis nucleus
both casesefferents: facial nerve– reflectoryclosing of eyes(M. orbicularis oculi – Pars palpebralis, Pars orbitalis)
strong light

Medialis Medulla syndrome
Nucl. XII: ipsilateralis tongue deviation (m. genioglossus)pyramidal tract: paralysis (before crossing - contralateral)medial lemniscus – after decussation – contralateral epikritic sensibility loss

Wallenberg syndrome: lateral part of medulla, posterior inferior cerebellar artery
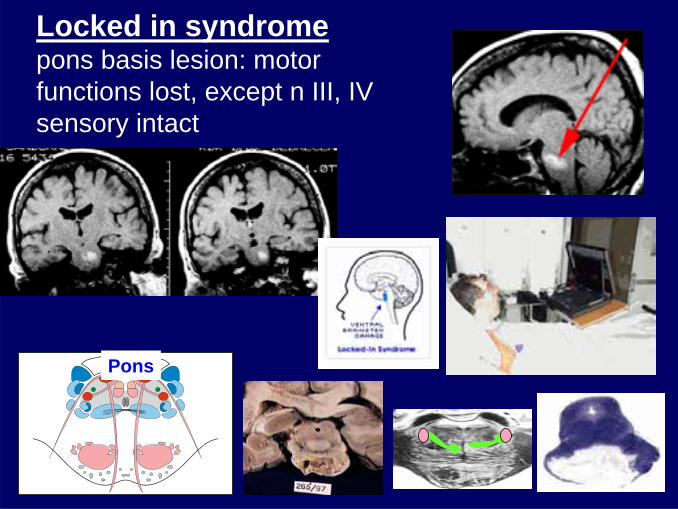
Locked in syndromepons basis lesion: motor functions lost, except n III, IV sensory intact
Pons

ALS: amiotrophic lateralsclerosis- degeneration of motoneurons in spinal cord AND brainstem

Tractography – shows tracts
END