breast cancer at the abc toowong queensland - final...
TRANSCRIPT

Breast Cancer at the ABC Toowong Queensland - Final Report Page 1 of 75
Breast Cancer at the ABC Toowong Queensland
Final Report of the Independent Review and Scientific Investigation Panel
Panel members Bruce Armstrong (Chair) Sydney Cancer Centre, Royal Prince Alfred Hospital and School of Public Health, The University of Sydney Joanne Aitken Viertel Centre for Research in Cancer Control, The Cancer Council Queensland Malcolm Sim Monash Centre for Occupational and Environmental Health, Department of Epidemiology & Preventive Medicine, Monash University Norman Swan, Producer and Presenter of the ABC’s Health Report, Australian Broadcasting Corporation
2nd June 2007

Breast Cancer at the ABC Toowong Queensland - Final Report Page 2 of 75
Table of Contents Summary ........................................................................................................................3
Background ....................................................................................................................6
Investigations .................................................................................................................8
Findings........................................................................................................................10
Epidemiology of breast cancer at the ABC Toowong .............................................10
Observed number of breast cancers .....................................................................10
Expected number of breast cancers......................................................................10
Workplace and other exposure history of women who had breast cancer or other breast tumours or lumps...........................................................................................13
Women with breast cancer...................................................................................13
Women with other breast tumours or lumps........................................................17
Survey of the site for possible sources of carcinogenic exposure ...........................18
Measurement of exposure to electromagnetic fields and ionising radiation............20
Radiofrequency electromagnetic fields (RF) .......................................................20
Extremely low frequency electromagnetic fields (ELF)......................................21
Ionising radiation .................................................................................................23
Review of published literature on risk factors for breast cancer .............................25
Feedback from the community following release of the Panel’s third interim report and subsequent news media coverage......................................................................30
Additional cases of breast cancer.........................................................................30
Possible causes.....................................................................................................30
Interpretation................................................................................................................35
Conclusions..................................................................................................................40
Acknowledgements......................................................................................................41
Appendices...................................................................................................................42
Appendix 1: Questionnaire ..................................................................................43
Appendix 2: Hazards assessment.........................................................................61
Appendix 3: Report on water testing ...................................................................69
Appendix 4: Report on ELF measurements.........................................................71
Appendix 5: Report on ionising radiation measurements....................................72

Breast Cancer at the ABC Toowong Queensland - Final Report Page 3 of 75
Summary After two attempted, earlier investigations, the Australian Broadcasting Corporation (ABC) appointed, in July 2006, the Independent Review and Scientific Investigation Panel to investigate an apparent cluster of breast cancers in women employed at its Toowong studios in Brisbane, Australia. The Panel reviewed relevant scientific literature, investigated the epidemiology of breast cancer in the Toowong female workforce, interviewed affected women about their work and workplace and known risk factors for breast cancer, and investigated the site for possible contamination with or high levels of exposure to known or suspected environmental risk factors for breast cancer.
Thirteen women who had worked at the ABC Toowong were found to have been diagnosed with breast cancer between 1st January 1994 and 30th June 2006. An additional woman was probably diagnosed with breast cancer while working there in this period, but the details were not confirmed. Ten women were diagnosed with invasive breast cancer while still employed at Toowong; the expected number, based on breast cancer rates in all Queensland women, was 1.6 (standardised incidence ratio (SIR) 6.25, 95% confidence interval (CI) 3.0-11.5, P=0.000001). This suggests that the likelihood of this event occurring by chance is about one in a million. This, however, may oversimplify the situation and, when further analyses are performed, adjustment of the P-value for implied multiple comparisons increased its estimated value to 0.04. That potentially increases the likelihood of the cluster occurring by chance to one in 25. Counterbalancing that is our finding that the longer the time of ABC employment, the greater the risk. We found a significant trend of 12% a year (95% CI 2-23%; P=0.022) towards increasing breast cancer risk with increasing duration of employment with the ABC. Half the women had breast cancer diagnosed at less than 40 years of age, which corresponded to an SIR for breast cancer at this age of 18.23 (95% CI 5.9-42.5).
The affected women had, on average, begun work at Toowong earlier and worked there longer than had other female employees in the study period. They also appeared to have been more likely to work in the newsroom. Relative to Australian women in general, they had higher educational levels, were somewhat more likely to drink alcohol, to have used oral contraceptives and to perform shift work, but less likely to smoke and more likely to exercise regularly. They were similar to other Australian women with respect to age at menarche, childbearing and breast feeding. Only one was menopausal, none had taken hormone replacement therapy and none had a family history of breast cancer.
Apart from ionising radiation, which is a well established cause of breast cancer, our literature review found very limited evidence that any other workplace exposures might cause breast cancer. We considered it prudent, however, to investigate the Toowong site and workplace for environmental exposures that are known or suspected to cause any cancer and might plausibly be present there.
No historical or other evidence was found of unusual contamination with or exposure to known or suspected carcinogens on the site. Asbestos had been used in construction and insulation of site buildings and had been removed on a number of occasions, including as recently as 1998. Measurements of asbestos in air in the mid 1980s and in 1998 at the time of asbestos removal, however, showed asbestos concentrations of

Breast Cancer at the ABC Toowong Queensland - Final Report Page 4 of 75
<0.01 fibres/ml except on one occasion (0.01 fibres/ml). Although broadband measurements of radiofrequency electromagnetic fields on site showed higher than usual levels in a few locations, these were only in close proximity to identifiable sources to which only infrequent or brief exposure would have been likely. Measurements of extremely low frequency electromagnetic fields were similarly unremarkable. Although there was an unusually high level in an equipment room, levels measured at all other locations and individually monitored for several staff members for a few hours were similar to those observed in a small survey of Australian residences and in people without specific occupational exposure in an overseas survey. Levels of possibly carcinogenic elements in the Toowong water supply met Australian standards and measured ionising radiation was at background levels, except for radon levels in the air of the TV building. These mildly elevated levels, however, were measured, unavoidably, after staff had vacated the TV building when the building was closed and the air conditioning turned off. Under these conditions falsely high readings could be produced.
These measurements of environmental exposure were inevitably limited to the present; whereas the environment of the 1980s and 1990s, or even earlier, is that most likely to have contributed to breast cancers occurring between 1994 and 2006. Nothing in our inquiries, however, produced evidence to suggest, with the probable exception of environmental tobacco smoke, that there was important past exposure to carcinogens at Toowong that would not have been present in 2006.
The Panel concluded that:
• There was a real increase in the risk of breast cancer in women working at the ABC Toowong site that was related to length of employment and may have been contributed to by some aspect of work or the working environment at Toowong.
• It was highly unlikely that this increase was caused by exposure during work on the Toowong site to radiofrequency electromagnetic fields, extremely low frequency electromagnetic fields, ionising radiation or chemicals known or suspected to cause breast cancer.
• There was also little or no evidence to suggest that the increase in risk could be explained by an underlying high risk of breast cancer in women employed at Toowong due to their sharing of known genetic or lifestyle risk factors for breast cancer.
• While we have not been able to find a cause for the increase in risk of breast cancer at the ABC Toowong, we believe that we have considered and excluded all plausible environmental explanations for such an increase. We do not recommend, therefore, that any further environmental investigations are done on the site.
• If there is a currently unknown or undetected aspect of work or the working environment at the ABC Toowong that could have contributed to the observed increase in risk of breast cancer, it might also be present in similar ABC studio complexes elsewhere in Australia. We recommend, therefore, the conduct of similar investigations into the frequency of breast cancer among women who have worked on those sites at some time since 1994, as we have done at Toowong.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 5 of 75
Absence of an increase in risk of breast cancer in women working at these other sites would provide reassurance to them and the ABC that this is not a systemic problem. It would also help to reassure women who worked at the ABC Toowong that whatever has caused their increased risk of breast cancer is unlikely to be present in their new workplaces. Presence of an increase would justify more extensive investigations as to possible causes.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 6 of 75
Background Female staff members employed by the ABC (Australian Broadcasting Corporation) at its premises in Toowong, Queensland, reported what appeared to be an unexpectedly large number of cases of breast cancer covering a period from 1994 to mid 2006. Particular concern was expressed at the number of cases among women in the TV newsroom and at the relative youth of those affected. Action to investigate the issue began in February 2005 and included:
Engagement of a senior occupational health physician from Health Services Australia (Health for Industry) to advise on the issue Dr Keith Adam was engaged to complete an exposure history for cases of breast cancer; confirm cases through accurate clinical diagnosis; educate staff about the occurrence of the disease; review the results of radiofrequency electromagnetic energy testing; and provide the ABC with an evaluation report. It is understood that Dr Adam gave a lecture to the staff and developed and circulated a questionnaire to employees reported to have had breast cancer. Some questionnaire recipients were concerned that the questionnaire did not address possible hazards in the workplace adequately. As a result few questionnaires were completed, staff members withdrew their cooperation with the investigation and Dr Adam did not prepare an evaluation report.
Conduct of a radiofrequency electromagnetic radiation (EMR) survey of the ABC Toowong In connection with Dr Adam’s investigation, EMC Technologies was contracted to survey broadband RF electromagnetic radiation (electric fields 100 kHz to 45 GHz and magnetic fields 100 kHz to 30 MHz) on the ABC Toowong site. The survey was done on 4th to 6th April and results were reported to the staff on 6th May 2005. All the tests were reported as complying with ARPANSA (Australian Radiation and Nuclear Safety Agency) reference levels. Measurable levels were reported in proximity to security card readers and areas inside and near outside-broadcasting vans.
Investigation of the occurrence of breast cancer in women on the Toowong site by Queensland Health Concerned ABC staff members asked Queensland Health in May 2005 to determine whether there were more breast cancer cases in the female workforce than would be expected and to consider whether the working environment might be responsible. Reported in December 2005, Queensland Health’s investigation concluded that there was a likelihood of a statistical excess of cases (based on eight cases it had identified) but that a valid statistical conclusion about the expected number of cases in the workplace in the period in question could not be drawn and, thus, that the size of any excess could not be quantified. It concluded, in addition, that an environmental appraisal did not indicate any plausible explanation for an increase in the number of breast cancers at the ABC Toowong and, therefore, that workplace related factors were an unlikely explanation for it.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 7 of 75
Appointment of the Independent Review and Scientific Investigation Panel Staff concern about the breast cancer cases at the Toowong site increased in July 2006 with the report of another staff member diagnosed with breast cancer. In response to this news, the ABC’s Managing Director, Mr Mark Scott, invited cancer and environmental epidemiologist, Professor Bruce Armstrong, Director of Research at the Sydney Cancer Centre, to constitute and lead an independent Investigative Panel. Dr Norman Swan, Producer and Presenter of the ABC’s Health Report, Professor Malcolm Sim, Director of the Monash Centre for Occupational and Environmental Health at Monash University, and Associate Professor Joanne Aitken, Director of Cancer Registries and Consultant Epidemiologist at the Viertel Centre for Research in Cancer Control at The Cancer Council Queensland, were the other members. The Panels terms of reference were to: 1. Review the scientific work undertaken to date on the reported breast cancer cluster
at Toowong including efforts made in 2005 to identify any cause; 2. Consider submissions and briefings from the staff-elected Staff Reference Group
(SRG) and communicate with the SRG on the Panel’s work and plans; 3. Advise the ABC on further investigations that should be made to identify any
cause for breast cancer clustering at Toowong; 4. Oversee the conduct of any such further investigations; and 5. Advise the ABC on any actions that should be taken in the light of the Panel’s
review of existing information and the results of any further investigations done.
The Panel was independent in the sense that it: • Would seek to apply sound scientific principles to its review and investigations
and to apply only those principles when formulating its advice; • Was freely able to speak with both management and staff about its investigations
and their outcomes and to seek information from and through both; • Would provide its progress and draft final reports to management and staff
(through the SRG) at the same time; and • Would take account of issues that both management and staff raise from the draft
final report in preparing its final report.
Panel members contracted independently with the ABC to provide their services at an agreed hourly rate of remuneration.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 8 of 75
Investigations The Panel, in consultation with the SRG and ABC management, took the following steps in its investigation.
Conduct of a study of the epidemiology of breast cancer on the ABC’s Toowong site The Panel sought to ascertain all cases of breast cancer diagnosed in women during their employment by the ABC at Toowong between 1st January 1994 and 30th June 2006 (the study period), a period that encompassed all the cases that had led to concern about the possibility of a breast cancer cluster at Toowong. It did so by seeking the assistance of Toowong staff members, through the SRG, in identifying the cases known to them. Expected numbers of breast cancers diagnosed during the above period were then estimated using ABC staff employment records covering the period and incidence rates of breast cancer in Queensland provided by the Queensland Cancer Registry. Dr Peter Baade, senior biostatistician at the Viertel Centre for Research in Cancer Control, estimated the expected numbers of breast cancers under Associate Professor Aitken’s oversight.
Workplace and other exposure history of women who had breast cancer or other breast tumour or lumps Women who were identified as having breast cancer diagnosed in the study period were asked for access to their pathology records to allow confirmation of the diagnosis and to give an interview. Professor Malcolm Sim, a Panel member, conducted the interviews, which covered, among other things, date of birth; date of diagnosis of breast cancer and circumstances leading to diagnosis; the women’s work, work patterns (including shift work) and workplace location histories during their employment with the ABC; and their family history of breast cancer and exposure, through lifestyle or other means, to other known risk factors for breast cancer. A copy of the interview questionnaire is at Appendix 1.
Women who had been identified as having breast lumps and tumours that were not cancer treated during the study period were also asked to give access to their medical records to allow confirmation of the diagnosis and to complete an abbreviated, self-administered version of the interview questionnaire. This questionnaire focused on diagnosis of the other breast lumps or tumours, including use of mammography, and the women’s work, work patterns (including shift work) and workplace location histories during their employment with the ABC.
Protocols for the epidemiological study and these investigations that directly involved women who were or had been ABC employees at Toowong were submitted to and approved by the Human Research Ethics Committee at The University of Sydney.
Survey of the Toowong site for possible sources of carcinogenic exposure An expert occupational hygienist, Dr Geza Benke of the Monash Centre for Occupational and Environmental Health, was engaged to visit the Toowong site, survey it and to obtain information about possible sources of exposure to carcinogenic agents, such as organochlorine pesticides, PCBs, heavy metals such as cadmium or lead, and organic solvents. Information about the history of the site with respect to

Breast Cancer at the ABC Toowong Queensland - Final Report Page 9 of 75
possible chemical or electromagnetic field exposure and any remediation actions previously taken were also obtained. Dr Benke also recommended that water be collected for testing for possible carcinogenic contaminants and this was done.
Measurement of levels of exposure to radiofrequency (RF) and extremely low frequency (ELF) electromagnetic fields and ionising radiation in the Toowong workplace Dr Benke also advised the Panel on measurement of exposure to RF, ELF and ionising radiation. It was decided to accept the EMC Technologies report on RF fields on the site as sufficient for the Panel’s purposes. The Australian Radiation Protection and Nuclear Safety Agency undertook surveys of ELF exposure and ionising radiation exposure in the Toowong workplace in accordance with specifications provided by the occupational hygienist.
Review of published literature on risk factors for breast cancer The Panel commissioned an environmental epidemiologist, Ms Lesley Walker, to review published literature on risk factors for breast cancer, focusing particularly on those that might be influenced by work or the working environment. This review guided directions taken by the Panel in the investigations outlined above. It was added to and updated by the Panel and is presented below in summary form.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 10 of 75
Findings
Epidemiology of breast cancer at the ABC Toowong Observed number of breast cancers A total of thirteen women were initially identified by ABC staff members as having been diagnosed with breast cancer during the study period. All agreed to be contacted by the Panel and all gave access to information on the pathology of their breast cancers. Pathology information was obtained for all 13 women.
The Panel received details, quite late in its investigations, of a fourteenth woman who was probably diagnosed with breast cancer between 1995 and 1997 while working at Toowong. We were advised that she had since died and we decided not to seek confirmation of her diagnosis or of her work with the ABC. She will not be referred to further in this report.
All 13 breast cancers about which we were initially advised had been diagnosed during the study period. Their diagnosis years were: 1994 one woman, 1998 four women, 2001 one woman, 2002 one woman, 2003 one woman, 2004 two women, 2005 two women and 2006 one woman. Two of the women were not employed at Toowong at the time their breast cancers were diagnosed in 1998 and 2003.
Invasive breast cancer was reported in 11 of the 13 women. One of the other two had a mucoid carcinoma, which while not specified as invasive is always invasive, so the Panel treated it as such for the purposes of this investigation. One had “duct carcinoma in situ of the breast” (DCIS) diagnosed in 2004, a lesion whose cells look like breast cancer but have not invaded adjacent normal tissue.
After excluding the two women who were not employed at Toowong when their breast cancers were diagnosed and the woman who did not have an invasive breast cancer, there were 10 women who had invasive breast cancer diagnosed while they were employed at the ABC Toowong during the study period. These are the women who were in the primary scope of this epidemiological investigation.
Expected number of breast cancers To be able to calculate the expected number of breast cancers (to compare with the observed number), the panel needed to know: • how many women were employed at the ABC Toowong during the study period
and what their ages were during that period; and • what the rate of breast cancer was in the general population of women in
Queensland during that period.
Women employed at the ABC Toowong in the study period The ABC provided information to the Panel on its female workforce for the period 1st January 1994 to 30th June 2006 from the ABC Toowong employment records.
Altogether, 550 women had been employed at Toowong at any time in the study period. The characteristics of these women are summarised in Box 1.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 11 of 75
Box 1. Characteristics of women employed by the ABC at Toowong between 1st January 1994 and 30th June 2006 • The women worked at Toowong for an average of 3.3 years in the period. Forty
had worked there for the whole study period (12.5 years); 16 had worked there for less than a month (30 days).
• Two payroll systems were in operation during the study period. More than half the women (59%, 324 women) had worked at Toowong between 1st January 1994 and 27th August 2001 (the part of the study period covered by the first system) and more than two-thirds (67%, 370 women) had worked there during the rest of the period (covered by the second system). About a quarter had worked there in both periods (26%, 144 women).
• In the first period, 30% of women staff members were recorded as working in the newsroom. This was 41% in the second period.
• Most women were aged in their 20s (47%) or 30s (28%) when they entered the study period; 3% were aged 18-19, 15% were in their 40s, and the remainder (7%) were aged 50 years or older.
Estimation of how many of these 550 women would be expected to develop breast cancer under normal circumstances was based on the numbers of years the women were in each age group while they were employed at the ABC during the study period. These numbers are referred to as “woman years”; each represents one woman in a particular age group working for one year at the ABC. They are shown in Table 1 below (the youngest woman employee during the period was 15 years of age and the oldest 73). Casual, part-time and full-time employees were treated the same when calculating woman years. The total number of woman years in the whole study period of 12.5 years was 1,810.
Table 1. Age distribution of woman years of employment with the ABC at Toowong in the period 1st January 1994 to 30th June 2006
Age group Woman years
Age group Woman years
Age group Woman years
15-19 years 14.8 35-39 years 283.4 55-59 years 86.4 20-24 years 217.2 40-44 years 215.2 60-64 years 53.2 25-29 years 293.4 45-49 years 162.5 65-69 years 3.3 30-34 years 337.1 50-54 years 141.1 70-74 years 2.0
Breast cancer rates in women in general in Queensland Data on invasive breast cancer incidence among women in Queensland were obtained from the Queensland Cancer Registry for the period 1994 to 2003 (2003 was the latest year for which data were available) in 5-year age groups from 0-4 to 85+ years of age. The numbers and ages of the women in the population in whom these cancers occurred were obtained from the Australian Bureau of Statistics (estimated resident population) for the same period. Age-specific incidence rates were calculated by dividing the total number of breast cancer cases in each age group (between 1994 and 2003) by the total population in that age group (summed over 1994 to 2003). These age specific incidence rates were used as the expected incidence rates.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 12 of 75
The expected number of breast cancers To obtain the expected number of invasive breast cancers diagnosed in women employed at the ABC Toowong in the study period, the Queensland invasive breast cancer incidence rates in each age group were multiplied by the number of woman years worked at the ABC Toowong in the study period in each age group (Table 1). The expected numbers of breast cancer cases in each 5-year age group were then added together to get the total expected number. This number was 1.60.
Comparison of risk of breast cancer in ABC Toowong women with that in women in general in Queensland This comparison was made by dividing the observed number of women with breast cancer diagnosed while employed at the ABC Toowong in the study period by the expected number to obtain a standardised incidence ratio (SIR). The SIR is a measure of how much higher the incidence (risk) of breast cancer was in the ABC women than in Queensland women in general. It is “standardised” in the sense that the same age distribution of women is used for obtaining the observed number and the expected number.
The SIR was 6.25 and had a 95% confidence interval (CI) of 3.0 to 11.5. The confidence interval means simply that because of statistical variability the true value of the SIR could be as low as 3.0 and as high as 11.5; however, the best estimate of the SIR is 6.25. The amount of statistical variability depends on the number of observed cases and is higher the smaller the number of cases.
The P value, or probability of occurrence by chance, of an SIR for breast cancer of 6.25, estimated on the premise of a single, planned comparison of one observed value with one expected value, was 0.000001; that is, “one in a million”.
A number of other calculations were done to examine the sensitivity of the SIR to different factors. The results of these calculations are summarised in Table 2. The SIR was a little less (6.02) if breast cancer risk in ABC Toowong women was compared with that in Brisbane women. In addition, the occurrence of only one case of in situ breast cancer (SIR 5.38) is compatible with the estimated 6-fold increase in risk of invasive breast cancer; for this calculation statewide estimates of invasive breast cancer incidence rates were used. There was substantial concentration of the increased risk in younger women, being greatest in those 15-39 years of age.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 13 of 75
Table 2. Estimates of increased risk of breast cancer in ABC Toowong women
Comparisons made Observed number
Expected number
SIR 95% CI
Invasive breast cancer at ABC compared with all Qld women
10 1.60 6.25 3.0-11.5
Invasive breast cancer at ABC compared with Brisbane women
10 1.66 6.02 2.9-11.1
In situ breast cancer at ABC compared with all Qld women
1 0.19 5.38 0.1-29.5
Invasive breast cancer at ABC compared with all Qld women in specific age groups
15-39 years 5 0.27 18.23 5.9-42.5 40-49 years 4 0.55 7.23 2.0-18.5 50 years + 1 0.77 1.30 0.0-7.2
Effect of duration of employment The effect of duration of employment with the ABC on risk of breast cancer was also estimated. A Cox proportional hazards regression model was used with age (in single years) as the time axis and past work duration (including time worked before 1994) as a time-dependent covariate, updated over follow-up time. Time worked with the ABC before 1st January 1994 may not have been at the ABC Toowong studios.
This model indicated a trend towards increasing risk of invasive breast cancer with increasing duration of past work at the ABC. Adjusting for the women’s age, the risk of invasive breast cancer increased significantly by about 12% for a one year increase in the duration of past work at the ABC (hazard ratio: 1.12; 95% CI: 1.02-1.23; P=0.022); this is a statistically significant trend.
Workplace and other exposure history of women who had breast cancer or other breast tumours or lumps Women with breast cancer In addition to the one woman who had in situ not invasive breast cancer, it was established at interview that two other women fell outside the predefined, primary scope of the epidemiological investigation; that is, women diagnosed with invasive breast cancer while they were employed at the ABC Toowong in the period 1st January 1994 to 30th June 2006. One of these women was diagnosed with breast cancer several decades after leaving her employment with the ABC and the other, while a regular radio interviewee at the ABC, had never been an ABC employee.
Information about these women of direct importance to the epidemiological investigation is summarised separately for the 10 women who were in the primary scope of the investigation and the 3 who were not.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 14 of 75
Workplace and disease factors Age and employment history Women in scope Five of the 10 women were <40 years of age when diagnosed with breast cancer, 4 were 40-49 years of age and one was 50+ years of age. They had worked at the ABC Toowong for 6 to 18 years, median 11 years, and had begun working there between 1983 and 2001, median year 1990.
Seven of the 10 women reported working in the newsroom. The other three either didn’t work there at all or made only occasional visits as part of their work. Of the seven women who worked in the newsroom, five spent at least part of their working time at one of the six workstations at the TV production desk on the lower floor of the TV building. The other two women who worked in the newsroom worked at other workstations in the vicinity of the TV production desk.
As noted in Box 1 above, 30% to 41% of all women who worked at the ABC Toowong in the study period were recorded in personnel records as having worked in the newsroom.
Three of the 10 women worked shift work most of the time, six some of the time and one none of the time.
In November 2003 in Australia, 12% of women who worked full time and 14% who worked part time had done shift work in the preceding 4 weeks1.
Women out of scope These women were 50-60 years of age at diagnosis of breast cancer. As noted above, one had never been an ABC employee, one worked there less than two years and one more than 20 years. They had first worked at Toowong between 1965 and 1992.
One of the three women reported working at the TV production desk in the newsroom. Neither of the other two worked in the newsroom.
Two of the three women worked shift work.
Breast cancer screening Women in scope Screening for breast cancer can both bring the diagnosis of breast cancer forward by a number of years and lead to diagnosis of some, perhaps slowly developing, breast cancers that would not otherwise come to clinical attention in a woman’s lifetime. Thus higher levels of screening can increase breast cancer incidence.
One of the 10 woman said that her diagnosis of breast cancer had been made after requesting a screening mammogram because of the apparent cluster of breast cancers at ABC Toowong. Three of the 10 said that their breast cancers had been diagnosed following attendance for a routine screening mammogram.
If the woman who requested a mammogram because of the apparent cluster is removed from the observed number of women with breast cancer, the SIR falls to
1 Australian Bureau of Statistics. Working arrangements, Australia, November 2003. Catalogue number 6342.0
Breast Cancer at the ABC Toowong Queensland - Final Report Page 15 of 75
5.63 and its lower confidence bound to 2.6. If all four of these women are removed, the SIR is 3.75 (95% CI 1.4-8.2). Such an extreme correction, however, is not justified. About 35% of breast cancers in women 50-69 years of age in Australia, the target population for breast screening, are first detected by screening. While the ABC women whose breast cancers were detected by routine screening were aged 41, 43 and 50 years, there is a high level of screening outside the organised program. Thus 3 breast cancers detected by screening out of a total of 10 is about the number expected in the population.
Women out of scope The one in situ breast cancer was found through routine screening; such cancers almost invariably are. Of the two women with breast cancer diagnosed when they were not employed at the ABC, one had the cancer found at routine screening and one didn’t. None was prompted by knowledge of the apparent cluster.
The breast cancers Women in scope Two of the 9 cancers with known pathology were reported to have very small invasive components – 1mm and 3.3mm, the diagnosis of one having been prompted by knowledge of the cluster. The remaining 7 cancers ranged in diameter from 13mm to 100mm, median 15mm.
Women out of scope Two of these 3 women had their cancers diagnosed through attendance for routine screening mammography. Both invasive cancers were small.
The Panel also asked women about exposure to known or suspected risk factors for breast cancer. Information obtained at interview is given here only for the 10 women who were in the primary scope of the epidemiological investigation. In addition, where possible, we have given comparative data for women of a similar age in the Australian population in the same time period.
Other risk factors The Panel asked women about known or suspected risk factors for breast cancer; they are outlined below. Information obtained at interview is given here only for the 10 women who were in the primary scope of the epidemiological investigation. In addition, where possible, we have given comparative data for women of a similar age in the Australian population in the same time period.
Educational level Three of the 10 women had been educated to year 10, 1 to year 12, 1 had a post-school diploma and five had university degrees. Comparative figures for all Queensland women in May 2006 were 30% educated to year 10, 28% to year 11 or 12, 21% with a post-school certificate or diploma and 21% with university degrees2. Thus in the women with breast cancer there were similar proportions with education to year 10, a lower proportion with education to years 11 or 12 and a higher proportion with post-school education, particularly university degrees. 2 Australian Bureau of Statistics. Education and work Australian 2006. Catalogue number 6227.0.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 16 of 75
Family history of breast cancer None of the 10 women reported any family history of breast cancer.
Body height and weight The ten women reported heights of 151cm to 176cm, weights of 55kg to 98kg and body mass indexes of 20.1 to 37.7 kg/m2. On the basis of the body mass index five of the women could be considered to be overweight.
In 2001, 44% of Australian women 25-64 years of age were overweight3.
Smoking Five of the ten women had ever smoked and none were current smokers.
In 2004, 50.3% of Australian women 30-59 years of age reported having ever smoked4 and 19.1% were current smokers.
Alcohol drinking Eight of the ten women reported having at least one drink of alcohol a week, 3 averaged one or more drinks a day, none more than two drinks a day.
In 2004, 45% of Australian women 30-59 years of age reported drinking alcohol at least once a week and 6% reported drinking every day1.
Exercise Eight of the 10 women engaged in exercise at least 2-3 times a week; five engaged in strenuous exercise at least 2-3 times a week.
In 1999, 82.4% of Australian women 30-59 years of age did some physical activity each week and 51.8% did sufficient to gain some health benefit5.
Menarche The average age at menarche (onset of periods) of the ten women was 13.0 years.
This is the same as that reported for Australian women surveyed between 1979 and 19866.
Menopause Only one woman would have been likely to be menopausal. None had taken menopausal hormone replacement therapy.
Oral contraceptive use All 10 women had used oral contraceptives for periods varying from 2 to 18 years, average 9.4 years.
3 Australian Institute of Health and Welfare. Differentials in overweight and obesity among adults, 1989-90 to 2001. AIHW Bulletin No. 11. Canberra: AIHW 2003 4 Australian Institute of Health and Welfare. 2004 National Drug Strategy Household Survey: First Results. Drug Statistics Series No. 13. Canberra: AIHW 2005 5 www.aihw.gov.au/publications/health/papaa/papaa-c02.pdf 6 Morabia A, Costanza MC. International variability in ages at menarche, first livebirth, and menopause. World Health Organization Collaborative Study of Neoplasia and Steroid Contraceptives. American Journal of Epidemiology 1998; 148: 1195-205

Breast Cancer at the ABC Toowong Queensland - Final Report Page 17 of 75
In Australia in 2001, 79% of women 30-49 years of age had ever used oral contraceptives7.
Childbearing Three of the women had not borne a child. The seven women who had borne a child, had their first child between 25 and 34 years of age, median age 28 and average age 29.4 years of age. One had 1 child, four had 2 children, and two had 3 or 4 children. The average number of babies per women was 1.6.
Given birth rates in 1999 it was estimated that 26% of women in Australia would remain childless. In Australia in 1996, the mean age at first nuptial birth was 28.7 years. Since the late 1990s, the number of babies per woman in Australia has been 1.8 or below8.
Breastfeeding Each woman who had borne a child had breastfed for an average of 2.3 to 12 months per child (median 7 months).
In 1996 and 2001, the median duration of breastfeeding by women in Australia was about 6 months with about 12% of children not being breastfed at all9.
Women with other breast tumours or lumps The Panel was advised of 12 women who had had other breast tumours or lumps diagnosed in the study period. A letter requesting access to information about the pathology of the tumour or lump and completion of an enclosed, self-administered questionnaire was sent to all 12 women. Nine women responded and provided some or all of the information requested.
Nature of the breast lumps or tumours Five women had only one breast lump or tumour episode; four had two. Four women provided copies of relevant medical records; one provided a core biopsy report, one included a report on cytology of cyst fluid, the others had only mammography or ultrasound reports. All had consented to our access to their records but we decided not to seek it when not provided. Of the five women who did not provide copies of medical records, three had had biopsies, one had a cyst aspirated and one had ultrasound only for the diagnosis of her lesion.
The diagnoses stated by the women or reported in medical records (including multiple lesions) were: galactocoele, fibrocystic change, fibrous tissue, cyst (2), sclerosing adenosis, “fibroid” (2), lactational tumour, cystosarcoma phylloides (considered benign), necrotic tissue, no specific diagnosis (2). None of the information the women gave about the diagnosis of their breast lesion suggested that a diagnosis of breast cancer had been made.
7 Yusuf F, Siedlecky S. Patterns of contraceptive use in Australia: Analysis of the 2001 National Health Survey. Journal of Biosocial Science 2006 Nov 23 [Epub ahead of print] 8 Australian Bureau of Statistics. Australian Social Trends, 1998, 2001, 2002. Catalogue number 4102.0 9 Australian Bureau of Statistics. Breastfeeding in Australia, 2001. Catalogue number 4810.0.55.001.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 18 of 75
Age and employment history Six of the 9 women were <40 years of age when last investigated for a breast lump or tumour and 3 were 40-49 years of age. They had worked at the ABC Toowong site for 3 to 17 years, median 6 years, and had begun working there between 1986 and 2001, median year 1996.
Compared to the women with invasive breast cancer diagnosed while they were employed at Toowong, the women with other breast lumps or tumours were somewhat younger, had begun work at Toowong more recently, and had worked there for shorter periods of time.
Seven of the 9 women reported working in the newsroom. They had worked there for from 5 to 18 years.
Eight of the 9 women had worked shift work.
Thus, in respect of both working in the newsroom and shift work, the women with other breast tumours or lumps were similar to the women with breast cancer.
Mammography detection of the breast lump or tumour Only one of the 9 women had her breast lump or tumour detected through screening mammography. Her attendance for screening was prompted by her knowledge of and concern about the apparent cluster of breast cancers at the ABC Toowong.
Survey of the site for possible sources of carcinogenic exposure An expert occupational hygienist was asked to visit the Toowong site to: • Ascertain the history of possible exposure to carcinogenic chemicals on the site –
eg, chemical waste, pesticides (eg termite control), solvents, PCBs, heavy metals, formaldehyde (as from building material or furnishings), flooding; and
• Do so by viewing relevant site records relating to sources of non-ionizing radiation and chemical exposures and interviewing current or past members of staff who may be in a position to recall any relevant exposure sources or episodes.
The hygienist’s report is at Appendix 2. In summary, he made the following observations.
Asbestos Materials containing asbestos (mainly asbestos cement sheeting, asbestos vinyl tiles and millboard) had been used in the construction of the TV building. These materials were removed over two periods, in the late 1980s and in about 2000, by an approved asbestos removalist working in accordance with Queensland occupational health and safety regulations. The hygienist judged that staff members would have been unlikely to have been exposed to asbestos during these removal processes.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 19 of 75
Environmental tobacco smoke (ETS) Smoking was banned inside ABC Toowong buildings in March 1989. ETS exposure would have occurred before that time. The hygienist had no basis on which to judge whether that exposure was greater than was experienced generally by the Queensland female population at the time.
Pesticides The Toowong site was residential before the construction of the ABC buildings in the 1960s. Heavy use of pesticides on the site during that early period is therefore unlikely. Organochlorines would be the main pesticides of concern because of their suspected cancer causing properties. Use of these chemicals inside buildings in Queensland ended in the early 1980s. Limited use, however, continued around the exterior of buildings and under slabs until about 1995. Arrest-a-Pest has been the pest control contractor for the ABC Toowong since at least the early 1980s. The hygienist spoke to Mr Chris Hill, who had been employed by Arrest-a-Pest since 1989; Mr Hill said that no significant quantities of organochlorines had been used by Arrest-a-Pest on the Toowong site.
Water The ABC Toowong is supplied by Brisbane Water. Contamination of the ABC’s water supply by heavy metals would be possible if there had been contamination of the piping from some outside source or there was significant corrosion of old piping. In consequence of this, the hygienist recommended that the drinking water supply be tested in accordance with the NHMRC Australian Drinking Water Guidelines 2004 to see if heavy metal contamination is present.
Water samples were collected from ten different drinking water outlets on the Toowong site on 15th December 2006 and sent to Brisbane Water’s Scientific Analytical Services for testing for arsenic, cadmium, chromium, lead, mercury, barium and nickel, some of which are known human carcinogens. All samples contained these elements at levels below the Guideline Values recommended under the Australian Drinking Water Guidelines, which are established by the National Health and Medical Research Council (http://www.nhmrc.gov.au/publications/synopses/eh19syn.htm). Further details of the measured levels are available in the Brisbane Water report at Appendix 3.
Other possible chemical contamination issues Tanks removed from the car-park area in 2000 Two petrol tanks that had been unused since 1996 were removed from the Toowong car-park in 2000. This time period would have permitted evaporation of any volatile hydrocarbons trapped in the tanks or soil. Soil measurements taken at the time of the removal showed no contamination.
Cleaning the air-conditioning system Contact was made with Mr Bruce Clayton of Haden, the air-conditioning contractors for the Toowong site. He said that the condensate trays were cleaned infrequently with a common, soap-based detergent to remove slime. The ductwork is vacuumed on an infrequent basis. The filters are not cleaned but replaced about once a year. The heat exchangers are cleaned infrequently with a chemical named Coil and Filter

Breast Cancer at the ABC Toowong Queensland - Final Report Page 20 of 75
cleaner AK manufactured by Sterile-Care Pty Ltd. The Material Safety Data Sheet (MSDS) for this product indicates that the active ingredient is a quaternary ammonium compound and it also contains alkaline salts. Neither of these is considered or suspected to be a carcinogen.
Ceiling tiles The ceiling tiles in the ground floor of the TV building were installed in 2000. These are Armstrong RH90 tiles manufactured in the USA. The MSDSs currently on the Armstrong website (http://www.armstrong.com/commceilingsna/msds_search.jsp) show that the commercial ceiling tiles all contain mineral wool fibre and fibrous glass, and some contain hydrous aluminium silicate. Each of these is (hydrous aluminium silicate) or may be carcinogenic if inhaled. There is no evidence, however, that they cause breast cancer. Prior to installation of these tiles in 2000, there were vinyl-coated Gyprock ceiling tiles in the building. They are unlikely to have produced any off-gassing of volatile organic compounds such as formaldehyde, n-hexane, n-pentane, xylenes, toluene or 2-methyl butane.
Measurement of exposure to electromagnetic fields and ionising radiation Radiofrequency electromagnetic fields (RF) The occupational hygienist (see Appendix 2) considered RF exposure during his visit to the ABC Toowong. Briefly, these were his findings.
• The site has numerous RF communications devices located within its perimeter. A history of the equipment on site prior to 1980 was not available. However, it appears that most of the equipment was added in the past twenty years due to advances in technology, with little replacement of older receivers and transmitters. It can be assumed that the current RF exposure levels are probably higher than at any other time during the operation of the site, due to the incremental addition of RF sources.
• The THL RF Hazard control document10 indicates that the most prominent RF source is the 7 meter satellite dish on the TV Building rooftop, operating at 14 Ghz. The three VHF Comms 3-metre antennae have high maximum power and operate between 168 and 172 MHz. Overall the RF sources on site cover a wide range of frequencies and power outputs. In these circumstances it is advisable to check the broadband exposures in the offices below.
• The EMC RF survey11 showed that broadband (100kHz to 45 GHz) RF levels in all the office work areas in the TV building were below the detection limit of the survey meter (<2 V/m). This is not surprising in view of the RF sources currently in place and the known high directionality of these sources. Additionally, since the broadband measurements do not indicate any excess exposure to RF it is most unlikely any future narrow band measurements will find excessive exposure levels in the office areas.
10THL Australia. RF Hazard Control Document Toowong Studio Brisbane Australian Broadcasting Commission. Date of Survey 16th February 2004. 11EMC Technologies Pty Ltd. Electromagnetic radiation survey conducted for Australian Broadcasting Corporation at 600 Coronation Drive, Toowong, Qld Australia. Report number B050401, issue date 2nd May 2005.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 21 of 75
• The EMC RF survey found measurable levels of RF in areas near to and inside outside-broadcasting vans [electric (E) fields up to 7V/m] and in proximity to security card readers [magnetic (H) fields up to 1.93A/m and electric fields up to 121.3V/m (next highest 37.4 V/m)]. Staff members were concerned that if their hands were full carrying books, bags or equipment, they would bring their chest into close proximity to the card reader and, perhaps, be exposed to intermittent high levels of RF radiation. The EMC report indicated that at 5 centimetres from the card reader the levels were only about a quarter of the ARPANSA reference levels. In addition, given the brief exposure periods over the course of a work-shift i.e. perhaps 1 to 2 minutes at most per day; the time-weighted average exposure should be extremely low.
The Panel noted that the highest strength electric field (121.3V/m) was at chest height in proximity to the external, security gate card reader and exceeded the ARPANSA time averaged and instantaneous reference levels for general public exposure. Exposure to this card reader, as compared with exposure to those at doors leading to the TV building and newsroom, however, would generally be infrequent and distant.
The EMC report also drew attention to the transmission antenna for the TV studio floor manager’s radio system, which is described in the THL document as 300mm in length and located on the “underside of the ceiling of the TV studio building, above the stage door”. EHC confirmed the THL report that RF levels may exceed ARPANSA limits at distance of less than 5cm from the antenna. Neither report states the RF levels actually measured. The THL report indicates that the area of hazard extended circumferentially around the antenna but not above or below it. It appears unlikely to have been a source of significant exposure to anyone engaged in normal use of the studio.
In the light of these considerations and advice of ARPANSA experts that further measurements would be unlikely to uncover any further evidence of high levels of exposure, the Panel decided not to request further monitoring of RF on the ABC Toowong site.
Extremely low frequency electromagnetic fields (ELF) ELF are produced by the flow of electrical current in power transmission and distribution cable and during the use of electrical equipment and appliances. ELF measurements were made at the ABC Toowong by ARPANSA on 18th December 2006. A full report on these measurements is at Appendix 4.
The ARPANSA report is based on two series of measurements:
• those made by the ARPANSA officer during a 2-hour (11:17am to 1:10pm) walk through the ground and first floors of the TV building while measuring and recording broad band magnetic field strengths (40-800 Hz) every 1.5 seconds; and
• those made using similar instruments worn by three staff members, one each from the ground and first floors of the TV building and from the radio building, over 4 hours (11am to 3pm) on the 18th December.
All measurements were made with ABC and other equipment operating under normal conditions.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 22 of 75
Graphical displays are provided from all four monitors used can be found in Appendix 4. From these is can be seen that:
• During the walk-through, the magnetic fields generally measured under 2 milliGauss (mG), but there were occasional spikes to between 5 and 10mG and rare spikes above 15mG. Average levels in different work areas were all below 2mG with the exception of the kitchen on the first floor of the TV building (2.5mG), the news control room on the ground floor (3.5mG) and the ground floor equipment room (21.1mG). The level in the general office area, in which most newsroom staff members worked, was 1.2mG. The average measurement was 0.87mG.
• All staff member measurements on the ground floor of the TV building were less than 2mG and most were less than 1mG. The average was 0.34mG.
• Most staff member measurements on the first floor of the TV building were less than 2mG but there were several spikes, two in close proximity, reaching just under 9mG. The average was 0.56mG.
• In the radio building, the baseline magnetic field was about 2mG with periods of increase to about 4mG and occasional peaks to 6-8mG and to between 15 and 20mG. The average was 2.03mG.
In considering the implications of these measurements, a key consideration is: How do they compare with levels that people commonly experience during the course of their daily lives? We have found two relevant sources of measurements.
The first and most directly relevant is a report on measurements from an ARPANSA pilot study of 26 residences in Melbourne made using equipment similar to that used for the Toowong measurements12. Table 3 below summarises the measurements obtained. The mean levels measured were on average higher than those measured at Toowong (0.97 to 3.34 compared with 0.34 to 2.03), although the peaks were not as great as some observed at Toowong – maximum 11.6mG near the front gate of a house compared with 21mG in the equipment room in the TV building at Toowong. Levels much higher than the peak measurement at Toowong, however, were observed within 30 cm of several commonly used household appliances: for example, microwave oven mean 97.1mG, hair dryer mean 25.3mG, television peak 25.4mG.
12 Karipidis K and Martin LJ. Pilot study of residential power frequency magnetic fields in Melbourne (2005). ARPANSA Technical Report 142, October 2005.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 23 of 75
Table 3. Descriptive statistics for ELF spot measurements under low power conditions at selected locations in 26 homes in Melbourne in June to August 2004.
The second set of measurements was reported by Kim and Cho (2001)13. The measurements were made in the Seoul area in Korea from 1996 to 1999 using the same equipment as ARPANSA. The investigators undertook personal monitoring of magnetic field exposures of 102 people in two groups: a group with probable occupational exposure to ELF and a group without probable occupational exposure to ELF. Table 4 below is extracted from their report and summarises the findings. The results in it are reported in microTesla (μT) units: 1μT = 10mG.
Table 4 shows that people without probable occupational exposure to ELF had average workplace levels of exposure that were similar to the home levels, 0.9mG compared with 0.7mG. In comparison, those with workplace exposure had much higher levels of workplace exposure 3.5 to 12.1mG than home exposure 0.8 to 1.8mG. The average levels measured at Toowong, with the exception of that measured when monitoring a staff member who worked in the radio building, were similar to those in the Koreans without probable occupational exposure. That measured on the staff member from the radio building was appreciably less than that measured on any of the Korean groups with probable occupational exposure.
Table 4. Personal exposure to ELF (in μT) in groups with and without presumed occupational exposure to ELF in Seoul, Korea, in 1996 to 1999
Ionising radiation Ionising radiation is better known as nuclear radiation, or just radiation. It is present naturally in cosmic rays from outer space (mainly the sun), some of which reach the 13 Kim YS and Cho YS. Exposure of workers to extremely low frequency magnetic fields and electric appliances. Journal of Occupational Health 2001; 43: 141-9.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 24 of 75
surface of the earth, and occurs naturally in the earth’s crust through the process of radioactive decay of radioactive elements. There is a natural and unavoidable background level of ionising radiation, which varies from place to place depending on the make up of the earth’s crust. There is also exposure to ionising radiation from its use in medicine (radiology, nuclear medicine and radiotherapy). ARPANSA has estimated that the average person absorbs about 2.3 mSv (milliSieverts) of ionising radiation each year: 0.8mSv comes from medical sources, 0.8 from external sources other than cosmic rays, 0.4 from internal sources (radioactive elements that are part of the structure of the body), and 0.3 from cosmic rays. The 0.8mSv from external sources includes 0.2 from radon, a radioactive gas in the atmosphere that originates from the Earth’s crust)14.
Ionising radiation measurements were also made, or initiated, at the ABC Toowong by ARPANSA on 18th December 2006. A full report on these measurements is at Appendix 5. The measurements methods were as follows:
• Surface contamination and dose rates were measured on the ground floor and first floor of the TV Building. The measurements included all staff workstations, studios, control rooms, staff amenities areas, reception, equipment rooms and corridors. These measurements were compared with background measurements taken outside the building.
• Thermoluminescent dosimeter (TLD) personal monitors were issued to five staff members from each floor of the TV Building for a two month wearing period. Following the decision to relocate staff from the Building it was requested that the personal monitors be left at the staff members’ workstations for the remainder of the exposure period. A control personal monitor, used for background subtraction, was held in another building at the Toowong site that was not associated with the breast cancer cluster.
• Air-conditioner inlet filters were monitored for a build-up of radioactivity from airborne contamination that may have accumulated over time.
• Average concentrations of radon in air were measured over a two-month exposure period by use of the ARPANSA Personal Radiation Monitoring Service radon area monitors. Three of the monitors were placed on the ground floor and two were placed on the first floor of the TV Building for a two month exposure period.
• A TLD disk included in each radon monitor measured natural background gamma radiation during the monitoring period.
The following measurement results were obtained:
• Radiation dose rates were within the range of 0.05μSv (microSieverts) per hour to 0.12μSv per hour. They equate to about 0.4 to 1.1mSv per year, which are comparable with normal, external background radiation levels found in Australia (see above).
• Radioactive accumulation was not found on the air conditioning inlet filters.
• Some of the TLD personal monitors were lost. The one remaining ground floor monitor and one of the first floor monitors showed no increase in dose above that
14 ARPANSA. What’s background radiation? http://www.arpansa.gov.au/baseline.htm accessed 24th May, 2007.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 25 of 75
of the background in the building where the control monitor was kept. The other three first floor monitors showed beta radiation doses of 180μSv, 280μSv and 140μSv for the two month exposure period but no increase in gamma radiation doses. That the building was vacated shortly after these monitors were initiated and the air conditioning turned off may have contributed to these small increases (equal to about half the total background level), because of build up of radon gas concentrations in the enclosed airspace.
• Two of the three radon monitors from the ground floor were lost. The remaining monitor from the ground floor and the two from the first floor showed average radon concentrations of 36.7, 20.6 and 20.6Bq/m3 (Becquerel per cubic meter) respectively. These levels are higher than levels measured in Australian homes in the 1980s, which varied between a median level of 6Bq/m3 in Queensland (highest levels up to about 25Bq/m3) and 14Bq/m3 in the ACT (highest levels up to more than 50Bq/m3)15. They do not, however, approach levels in the United States at which action to reduce home levels is currently recommended; that is, 74-148Bq/m3 (2-4 picoCuries per litre)16. It is also possible that the levels measured were atypically high because the building had been vacated and the air conditioning turned off. (Curies and Becquerels measure the same thing – actual amounts of radioactivity in something – in this case, air in a room. Exposure on average to 20Bq/m3 of radon has been estimated to give a radiation dose of about 1mSv per year).
• The respective annual average background gamma radiation doses estimated from the TLD disks in the radon monitors were 1,020, 1,320 and 1,020μGy (microGrays) for the two months exposure as compared with typical annual gamma background levels of approximately 1,000μGy. (Grays and Sieverts are closely related measures of ionising radiation. Grays measure the amount of radiation absorbed by an exposed human or animal body while Sieverts take account of, in addition to the absorbed dose, the different effects of, and different responses of different body tissues to, different types of ionising radiation.)
Review of published literature on risk factors for breast cancer The 2006 third revision of a major text on cancer epidemiology and prevention gives a broad overview. Table 5 below summarises the familial, environmental and lifestyle risk factors identified in its authoritative chapter on breast cancer. In addition to these, it identified some previously suspected risk factors that, it stated, are now thought not to cause breast cancer: • Exposure to organochlorine pesticides; • Active smoking and passive smoking; • Use of underarm deodorants and • Breast implants.
15 Langroo MK, Wise KN, Duggleby JC, Kotler LH. A nation-wide survey of radon and gamma radiation levels in Australian homes. Australian Radiation Laboratory [now ARPANSA], 1990. 16 US Environmental Protection Agency. Radon. http://www.epa.gov/radiation/radionuclides/radon.htm#recommendations, accessed 24th May 2007.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 26 of 75
Table 5. Familial, environmental and lifestyle factors associated with risk of breast cancer Summarised from Colditz G, Baer HJ and Tamimi RM, Breast Cancer, in Shottenfeld D and Fraumeni JF, Cancer Epidemiology and Prevention Third Edition, New York, Oxford University Press 2006: 995-1012
Risk factor Comment
Family history of breast cancer Risk increases with increasing number of relatives with a history of breast cancer
Socioeconomic status (SES) Risk higher in women of higher SES Age at menarche Risk is higher in women with an earlier menarche Age at first full-term pregnancy Risk is higher in women with a later first full-term
pregnancy Number of births Risk is higher in women who give birth fewer
times Breastfeeding Risk is higher the shorter the time a woman breast
feeds her babies Oral contraceptive pill use Risk is increased by a small amount while taking
the pill Age at menopause (natural or artificial)
The later the age, the higher the risk
Hormone replacement therapy Risk is increased while using HRT Body height Risk is greater in taller women Body weight or obesity Risk of post-menopausal breast cancer is increased
in overweight and obese women Alcohol intake Risk increases as alcohol intake increases Physical activity Risk is higher in those have less physical activity Ionising (nuclear) radiation Risk increases with increasing exposure
A separate chapter on occupation and cancer listed workplace exposures that are considered to definitely or probably cause cancer. None of these exposures were known to cause breast cancer specifically.
Other environmental factors for which there is some evidence of an association with breast cancer or about which concern has been expressed include: Bisphenol-A, a chemical used to make polycarbonate plastic; polyvinyl chloride, which is commonly used in plastics; dieldrin and related pesticides (eg, DDT and chlordane/heptachlor); PCBs (polychlorinated biphenyls), used in the manufacture of electrical equipment; polycyclic aromatic hydrocarbons, compounds found in soot and fumes from combustion of diesel and other fuels and from grilling meat; dioxin, ethylene oxide, and electromagnetic fields (RF and ELF)17, 18.
17 Breast Cancer Fund and Breast Cancer Action. State of the evidence: What is the connection between the environment and breast cancer? Fourth Edition 2006. http://www.bcaction.org/PDF/StateofEvidence.pdf accessed 31st May 2007. 18 Brody JG, Moysich KB, Humblet O, Attfield KR, Beehler GP, Rudel RA. Environmental pollutants and breast cancer. Cancer 2007. Published online 14th May 2007.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 27 of 75
Occupational and environmental chemical exposure A recent comprehensive review of occupational and environmental chemical exposure and breast cancer observed19: • Increased incidence rates of breast cancer have been observed repeatedly in
women in white collar jobs. They are related to both socioeconomic status and late childbearing.
• Occupational studies provide fairly consistent evidence that increased risk independent of socioeconomic status is associated with a few specific exposures: Benzene, organic solvents and PAHs (polycyclic aromatic hydrocarbons, generally produced as a result of combustion). Chemicals with the most consistent human evidence have also been identified as animal mammary carcinogens.
A further, very recent and comprehensive review by the same authors reached the following conclusions with respect to some of the potentially important chemicals listed above28. • existing research strategies provide conflicting and mostly negative evidence with
respect to DDT, DDE and dieldrin. Lack of evidence for an association between organochlorine pesticides and breast cancer may be due to a true lack of association or to shared methodological weakness across a large number of studies;
• In studies of general populations, the evidence for an association between total PCBs and breast cancer risk was inconsistent, regardless of the exposure measure; as were studies of individual congeners. There is, however, evidence that suggests that PCBs increase breast cancer risk in women with certain genetic variants;
• The evidence regarding dioxin and breast cancer is thus far inconclusive; • A few strong studies and numerous records-based occupational assessments
provide evidence of an association between breast cancer and organic solvents.
With respect to other chemicals of possible concern, our review of published literature found the following: • No direct evidence that the xeno-oestrogen bisphenol-A causes cancer of the
breast20; • Vinyl chloride monomer is a potent carcinogen. Polyvinyl chloride has not been
shown to increase risk of breast cancer, though very limited studies have been done.
• There is some evidence, although somewhat inconsistent, that ethylene oxide increases risk of breast cancer in women21,22
19 Brody JG and Rudel RA. Environmental pollutants and breast cancer. Environmental Health Perspectives 2003; 111: 1007-19. 20 Haighton LA, Hlywka JJ, Doull J, Kroes R, Lynch BS, Munro IC. An evaluation of the possible carcinogenicity of bisphenol A to humans. Regul Toxicol Pharmacol. 2002; 35: 238-54. 21 Steenland K, Whelan E, Deddens J, Stayner L, Ward E. Ethylene oxide and breast cancer incidence in a cohort study of 7576 women (United States). Cancer Causes Control. 2003; 14: 531-9. 22 Coggon D, Harris EC, Poole J, Palmer KT. Mortality of workers exposed to ethylene oxide: extended follow up of a British cohort. Occup Environ Med. 2004; 61 :358-62.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 28 of 75
Extremely low frequency electromagnetic fields (ELF) ELF are the alternating electrical and magnetic fields (50-60 Hz) produced in proximity to electrical power transmission and distribution cables and electrical devices that have a high current flow. The most recent, comprehensive review of the association of ELF with risk of breast cancer concluded: “The weight of the evidence available today suggests that power frequency magnetic field exposure most likely is not a risk factor for breast cancer development.”23 More recently published results from a large case-control study of breast cancer in women show a very weakly rising trend in risk with increasing ELF exposure: relative risk 1.16 (95% CI 0.90–1.50) and P value for trend 0.04. The authors concluded “Our findings, taken together with previous occupational studies, suggest that EMF exposure at the workplace may be associated with a slight elevation in breast cancer risk”, a conclusion that is not much different from that of the earlier review24.
Radiofrequency electromagnetic fields (RF) Radiofrequency fields cover the whole electromagnetic spectrum from 100 kHz to 300 GHz and include all frequencies used in radio, TV and microwave transmission. A comprehensive review published in 1999 reported on two studies of breast cancer, one in Norwegian female radio and telegraph operators and one of 227 men with breast cancer and 300 control subjects. The relative risk of breast cancer in the female radio and telegraph operators was 1.5 (95% confidence interval CI 1.1-2.0) and the relative risk of male breast cancer was 2.9 (95% CI 0.8-10.0) in radio and communications workers. Overall, the author concluded: “The epidemiologic evidence falls short of the strength and consistency of evidence that is required to come to a reasonable conclusion that RF emissions are a likely cause of one or more types of human cancer.”25 A later review mentioned some additional smaller studies, which had not found an association between RF and breast cancer, and reached a similar conclusion to the earlier study: “The available data are insufficient to reach any conclusion on whether RF exposure is related to breast cancer risk.”26
Shift work There is a growing literature on the possible role of shift work on risk of breast cancer, through the suppressive effect that “light at night” has on the release of the hormone melatonin from the pineal gland. This work has recently been reviewed in three companion papers.27 These reviews conclude that there is an increased risk of
23 Feychting M and Forssén U. Electromagnetic fields and female breast cancer. Cancer Causes and Control 2006; 17:553-8. 24 McElroy JA, Egan KM, Titus-Ernstoff L, Anderson HA, Trentham-Dietz A, Hampton JM, Newcomb PA. Occupational exposure to electromagnetic field and breast cancer risk in a large, population-based, case-control study in the United States. J Occup Environ Med. 2007; 49: 266-74. 25 Elwood JM. A critical review of epidemiologic studies of radiofrequency exposure and human cancers. Environmental Health Perspectives 1999; 107 (Suppl 1): 155-68. 26 Ahlbom A, Green A, Kheifets L, Savitz D, Swerdlow A; ICNIRP (International Commission for Non-Ionizing Radiation Protection) Standing Committee on Epidemiology. Epidemiology of health effects of radiofrequency exposure. Environ Health Perspect. 2004; 112: 1741-54. 27 Stevens RG. Artificial lighting in the industrialized world: circadian disruption and breast cancer. Cancer Causes and Control 2006; 17: 501-7. Hansen J. Risk of breast cancer after night- and shift-work: current evidence and ongoing studies in Denmark. Cancer Causes and Control 2006; 17: 531-7. Davis S and Mirick DK. Circadian disruption, shift work and the risk of cancer: a summary of the evidence and studies from Seattle. Cancer Causes and Control 2006: 17: 539-45.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 29 of 75
breast cancer associated with indicators of light-at-night and night shift work. These conclusions are based on studies of breast cancer risk associated with occupations that commonly entail night-shift working and studies in the general population of the relationship of self-reported working hours to breast cancer. While statistically significant results have been obtained, the relative risks observed have generally ranged between 1.5 and 2.0. There was some evidence of dose-response relationships; that is, risk increasing with frequency and duration of shift working.
Psychological factors Stress and an individual’s response to it are popularly believed to be important factors in causing cancer. A recent critical review of psychological factors and cancer development concluded that: “…there is not any psychological factor for which an influence on cancer development has been convincingly demonstrated in a series of studies.”28 In an earlier review focusing specifically on breast cancer, and commissioned by Australia’s National Breast Cancer Centre, the authors concluded: “In general, the evidence for a relationship between psychosocial factors and breast cancer is weak. The strongest predictors are emotional repression (especially of anger) and severely threatening life events that would include the loss of a significant other. Although the available evidence does not support a major role for psychosocial factors in breast cancer development, few studies have been of sufficient quality to state definitively that such a role does not exist”29.
Smoking Whether or not risk of breast cancer is affected by active or passive smoking has become, in recent years, an increasingly live and controversial issue. A meta analysis of published results from 19 studies showed small, but statistically significant increases in risk of breast cancer with any passive smoking – relative risk 1.27 (95% CI 1.11-1.45) and any active smoking – relative risk 1.46 (95% CI 1.15-1.85)30. The comparative similarity of these two relative risks, given the very large difference in relative risks of lung cancer between active and passive smokers, has contributed to the scepticism with which evidence that smoking causes breast cancer has been met. That the issue is complex, however, is suggested by very recent evidence from a large US cohort study that the risk of breast cancer associated with active smoking is confined to exposure before the first pregnancy and is greatest for exposure before menarche31. There are biological grounds for believing the sensitivity of breast tissue to tobacco smoke carcinogens is less after the first pregnancy.
28 Garssen B. Psychological factors and cancer development: Evidence after 30 years of research. Clinical Psychology Review 2004; 24: 315-338. 29 Butow PN, Hiller JE, Price MA, Thackway SV, Kricker A, Tennant CC. Epidemiological evidence for a relationship between life events, coping style, and personality factors in the development of breast cancer. Journal of Psychosomatic Research 2000; 49: 169-81. 30 Johnson KC. Accumulating evidence on passive and active smoking and breast cancer risk. Int J Cancer. 2005; 117: 619-28. 31 Ha M, Mabuchi K, Sigurdson AJ, Freedman DM, Linet MS, Doody MM, Hauptmann M. Smoking Cigarettes before First Childbirth and Risk of Breast Cancer. Am J Epidemiol. 2007. Published online Apr 9.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 30 of 75
Feedback from the community following release of the Panel’s third interim report and subsequent news media coverage Many members of the community wrote to the ABC or to Panel members, following release of the Panel’s third interim report and news media coverage of it, with information about additional breast cancer cases and ideas and suggestions about the cause of the increased risk of breast cancer and the way it might be investigated further. The Panel considered all the ideas and suggestions and sought expert advice when necessary. The following sections summarise some of this additional information and suggestions and the Panel’s response to them.
Additional cases of breast cancer Three people contacted the ABC and told them about former ABC employees who had suffered from breast cancer. All three were diagnosed seven or more years before the study period. These reports do not suggest that risk of breast cancer was increased at the ABC before the study period but also do not exclude this possibility.
Advice was also received regarding four women who had lived in the neighbourhood of the ABC Toowong studios and had been diagnosed with breast cancer. Three were diagnosed before the study period and one after it; none during the study period. These reports do not suggest that risk of breast cancer was increased in women residing in the neighbourhood of the ABC but also do not exclude this possibility.
Possible causes Electromagnetic energy Most suggestions related to exposure to electromagnetic energy covering the full spectrum from ionising radiation to ELF. A number have been covered in the sections above on RF, ELF and ionising radiation; others are dealt with here.
Some novel suggestions were made regarding exposure to RF. One writer knew of a government agency in Brisbane that had bounced microwave signals off nearby buildings when establishing communications links. We found it difficult to see how this might have affected RF exposure of ABC staff members at Toowong. Two writers suggested that bra underwires might focus RF on the breast. Given, however, the generally low levels of RF in the Toowong studios it is difficult to see how such an effect would produce a much higher rate of breast cancer there than in other women who are, presumably, as prone to wear bras with underwires. Another writer suggested that signals from mobile phone towers might have intersected in the vicinity of the newsroom and produced localised high exposure to electromagnetic energy through resonance. We could find no evidence to support such a possibility.
Two writers suggested, on the basis of published hypotheses32,33, that there may be increased concentration or deposition of carcinogenic air pollutants, both chemical and radioactive, in the vicinity of sources of high ELF (eg, power transmission lines) and that this might have happened on the Toowong site. Subsequent investigations,
32 Hopwood A 1992 Natural radiation focused by power lines: New evidence. Electronics World and Wireless World. November, 912–5. 33 Fews AP, Henshaw DL, Keitch PA, Close JJ, Wilding RJ. Increased exposure to pollutant aerosols under high voltage power lines. Int J Radiat Biol. 1999; 75: 1505-21.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 31 of 75
however, do not suggest that the hypothesised effects would have any material impact on exposure to carcinogens.34,35
One writer drew attention to exposure to ionising radiation from emergency lighting, smoke detectors, and luminous direction signage. Exposure from such sources, however, would be very low and not unique to the Toowong building, if these devices had ever been installed there. Another writer raised the possibility of exposure to x-rays from the electron beam in a faulty cathode ray tube (older style) computer monitor. Such an effect would be unlikely to produce a cluster of breast cancers.
Chemicals There were a number of suggestions about possible chemical causes of cancer; most of these related to possible exposure to pesticides, dioxin, PCBs from transformers, and trace metals. It was suggested that there had been a transformer in the electrical sub-station on site that had leaked PCBs or had even “blown up”. One writer raised the possibility of leakage of chemicals, possibly PCBs, from capacitors in old fluorescent lights. Some writers suggested that the soil on the site should be tested for one or more of these chemicals and one suggested that blood tests should be done for organochlorines, other pesticides and trace metals.
The Panel considers that its investigations had largely ruled out the possibility of organochlorine contamination of the site in the past 20 or so years. It was also unable to confirm the occurrence of any leakage or other major event involving a transformer. It judged that any significant contamination of the site from capacitors in fluorescent lights was unlikely.
None of the chemicals mentioned is volatile. Thus, even if contamination was present exposure by inhalation would be negligible unless there was an acute event, such as an explosion. In addition, exposure of ABC staff members to soil on the site would be negligible except for those involved in maintenance of the buildings and grounds. The Panel does not recommend testing of soil on the Toowong site for increased concentrations of organochlorine pesticides, PCBs, dioxin, or known or possibly carcinogenic heavy metals; nor does it recommend that women diagnosed with breast cancer or other staff members have blood tests for these chemicals.
The possibility of major contamination of the Toowong site with asbestos was raised. An anonymous writer advised that loose, fibrous blue asbestos had been found by Qld Health scientists in the roof cavity of the TV building in 1986. ABC records reviewed by the Panel do not make specific mention of such a finding. Major asbestos removal work was done in the TV Building in 1985 and 1986. Further removal work was done in 1998: it entailed removal of asbestos debris from several areas of the TV building, removal of asbestos millboard (a soft asbestos cardboard like material) from air conditioning heater banks in both the TV building and the Radio building and removal of asbestos flu pipe from the Radio building.
34 Vistnes AI, Strand T, Thommesen G. Focusing of cosmic radiation by power lines? J Radiol Prot. 1997; 17: 185-93. 35 Jeffers D. Modelling and analyses do not support the hypothesis that charging by power-line corona increases lung deposition of airborne particles. Radiat Prot Dosimetry. 2007; 123 257-61.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 32 of 75
Part of the removal of debris entailed removal and replacement of synthetic mineral fibre insulation from the ceiling of a TV studio, which was described as “heavily contaminated with blue asbestos” in one area. This suggests that there was a larger quantity of blue asbestos in this ceiling space before the 1985 and 1986 removals. A letter from the 1998 removal contractor stated that “Previously this ceiling has been sprayed in limpet asbestos…” Monitoring of asbestos concentrations in air before, during and after the removal in 1985 and 1986 showed fibre concentrations of <0.01 fibre/ml in all locations except one, taken immediately after removal, where it was 0.01 fibres/ml. In 1998, similar measurements were consistently <0.01 fibres/ml. The completion report prepared following the 1998 removal stated that asbestos contamination was possible in air supply ducting due to the deteriorated state of the asbestos millboard removed from the air conditioning heater banks. Some asbestos millboard debris was identified in dust samples collected.
There is some weak evidence that asbestos increases risk of breast cancer in women36.
One writer suggested that “outgassing” of formaldehyde from a wood/glue composite used in office furniture could have increased risk of breast cancer. Formaldehyde is a known cause of cancer in humans; there is sufficient evidence that it causes cancers of the nasopharynx and limited evidence that it causes cancers of the nasal passages and sinuses and leukaemia37. There is no direct evidence that it can increase risk of breast cancer, although two studies of women who work with formaldehyde were suggestive of an increased risk of breast cancer. In Australia, formaldehyde may be present in glues, fibreboard and particleboard, furniture, textiles and some insulation. It is commonly found in the air in homes and offices; higher levels have been found where construction materials included unsealed wood panel or plywood products. The amount of formaldehyde released from manufactured wood products, however, has fallen substantially over the past 20 years.
The Panel asked the ABC for information on the construction of walls and furniture in the newsroom. We were advised that the internal walls of the Newsroom at Toowong were lined with gyprock. The desks were generally made from laminated particleboard or laminated medium density fibreboard (MDF). The desk partitions were aluminium framed with a bottom half of fabric covered plywood or MDF. The doors had a painted plywood finish. Laminating substantially reduces formaldehyde emissions from particleboard and MDF. Emissions also fall quite quickly with time following manufacture.
A question was raised about gases coming from a pipe in the floor of the newsroom, near the news production area where a number of the women who had developed breast cancer had worked. The end of the pipe was visible and it was capped at floor level. It had been taped over by staff members to reduce the smell coming from it. The Panel asked the ABC for information about the pipe. The Building Services Coordinator advised that it had been the drain from a kitchen sink before that area was rebuilt. It leads by way of the site's waste water drainage system 36 Weiderpass E, Pukkala E, Kauppinen T, Mutanen P, Paakkulainen H, Vasama-Neuvonen K, Boffetta P, Partanen T. Breast cancer and occupational exposures in women in Finland. Am J Ind Med. 1999; 36: 48-53. 37 International Agency for Research on Cancer. Formaldehyde, 2-Butoxyethanol and 1-tert-Butoxypropan-2-ol. IARC Monographs on Carcinogenic Risks to Humans Volume 88. Lyon, IARC 2006.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 33 of 75
to Brisbane's sewers. The smell, therefore, is probably sewer gases, particularly methane and hydrogen sulphide. These gases are not carcinogenic.
Infection Several writers suggested to us that the cluster of breast cancers might have been caused by woman to woman transmission of the human mammary tumour virus. Another gave his personal theory that breast cancer is caused by a nematode worm that can be transmitted from one person to another.
There is convincing evidence for a mouse mammary tumour virus (MMTV), which is transmissible from one mouse to another38. Ever since MMTV was discovered in the 1930s, scientists have searched for a human mammary tumour virus. There is now substantial evidence that DNA sequences similar to those of the MMTV can be found in human breast cancer, but they have also been found in the blood of healthy people39. At present, however, there is no evidence that an MMTV-like virus plays a role in causing breast cancer40. Other viruses, including human papilloma virus and Epstein-Barr virus, have also been found to be associated with breast cancer tissue. There is no evidence that breast cancer risk can be transmitted from one person to another, except genetically.
Other factors A community group (Endeavour Forum) sent the Panel information about induced abortion and breast cancer. We had not asked women about their history of spontaneous or induced abortion, both because of the intrusiveness of the question and the limited evidence that it might influence breast cancer risk. In the most substantial research on abortion and breast cancer published to date41, the investigators pooled data from 53 studies. Results of studies that used prospective information on abortion (ie, information that had been recorded before the diagnosis of breast cancer—including a total of 44 000 women with breast cancer) were considered separately from results of the studies that used retrospective information (recorded after the diagnosis of breast cancer—including 39 000 women with the disease). In the prospective studies, the overall risk of breast cancer after having had one or more pregnancies that ended as an induced abortion was 0.93 (95% CI 0.89-0.96) relative to having had no pregnancy ending in induced abortion. When the information on induced abortion was retrospectively recorded, the relative risk for breast cancer with induced abortion was 1.11 (95%CI 1.06-1.16). If the result on induced abortion for the studies with prospective records is combined with the result for those with retrospective records, the relative risk is 1.00. Retrospective recording is less reliable than prospective recording because it may be influenced by the experience of having been diagnosed by breast cancer. A recent analysis of the very large Nurses Health
38 Cardiff RD, Kenney N. Mouse mammary tumor biology: a short history. Adv Cancer Res. 2007; 98: 53-116. 39 Szabo S, Haislip AM, Garry RF. Of mice, cats, and men: is human breast cancer a zoonosis? Microsc Res Tech. 2005; 68: 197-208. 40 Lawson JS, Tran DD, Carpenter E, Ford CE, Rawlinson WD, Whitaker NJ, Delprado W. Presence of mouse mammary tumour-like virus gene sequences may be associated with morphology of specific human breast cancer. J Clin Pathol. 2006; 59: 1287-92. 41 Collaborative Group on Hormonal Factors in Breast Cancer. Breast cancer and abortion: collaborative reanalysis of data from 53 epidemiological studies, including 83 000 women with breast cancer from 16 countries. Lancet 2004; 363: 1007-16.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 34 of 75
Study II, in which history of induced abortion was prospectively recorded, obtained similar results: relative risk 0.89 (95% CI 0.78-1.01)42.
42 Michels KB, Xue F, Colditz GA, Willett WC. Induced and spontaneous abortion and incidence of breast cancer among young women: a prospective cohort study. Arch Intern Med. 2007; 167: 814-20.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 35 of 75
Interpretation Chance Our statistical findings suggest that the risk of breast cancer in women working at the ABC Toowong from 1st January 1994 to 30th June 2006 was some six times higher than that in the general population of women in Queensland. We estimated that there is a 1 in a million probability that the observed or a greater number of cases of breast cancer could have arisen there simply by chance.
The estimate of the probability that the increase is due to chance alone, however, requires some qualification. In interpreting it we must consider the existence of implicit multiple comparisons. “When a cluster is reported from one community, it implies that comparisons have taken place in many similar communities about which we do not hear because no clusters were found.”43 For the cases of breast cancer at the ABC Toowong, we can argue that these implicit multiple comparisons have been made in an estimated 40,000 groups of 150 women (the approximate average size of the Toowong female workforce over the study period) in the whole Australian female population 15-64 years of age. Using the method described by Armon et al17 to adjust the P value for these multiple comparisons, we can estimate a revised P value of 0.04 for the increase in risk of breast cancer in ABC Toowong women. This value, while still indicating statistical significance in conventional terms – because it is less than 0.05 – indicates that there is much less certainty about the proposition that the breast cancers did not cluster by chance than had otherwise appeared. That is, there is about a 1 in 25 probability that the cluster occurred by chance.
Error in the estimates of breast cancer incidence at Toowong There are three possible sources of error: ascertaining the number of cancers, counting the number of woman years in the employed women at Toowong, and calculating the expected number of breast cancer cases. The last has been carefully checked by Dr Baade and Associate Professor Aitken and been the subject of external review by Professor Michal Abrahamowicz, a Professor of Biostatistics at McGill University, Montreal, who was visiting Sydney at the time. We are confident there is no error there.
We thoroughly checked all the ascertained cases of breast cancer, confirmed that they were in the scope of the investigation and obtained histopathology reports. We also obtained information from 9 of 12 ABC Toowong women who were said to have had tumours or lumps in the breast that were not breast cancer, and found no suggestion that any of them might have had breast cancer. After extensive media coverage about the cluster and this investigation, we received advice from community members about three women diagnosed with breast cancer who had worked at the ABC. All, however, were diagnosed well before the study period. The only possible error is under-ascertainment of breast cancers; this would have produced a falsely low standardised incidence ratio not a falsely high one.
ABC staff records were used to estimate the woman years. While concern had been expressed at the possibility that some casual employees might have remained on the “books” for a period after they stopped working at Toowong, this would have inflated 43 Armon C, Daube JR, O’Brien PC, Kurland LT, Mulder DW. When is an apparent excess of neurologic cases epidemiologically significant? Neurology 1991; 41: 1713-18.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 36 of 75
the number of person years not diminished it, and led to an underestimate of the standardised incidence ratio.
Higher levels of breast cancer screening in ABC Toowong women The Panel thought initially that awareness of the number of breast cancer cases at Toowong would have prompted women to seek breast cancer screening when they might not otherwise do so. This could increase the number of cases diagnosed. Indeed one of the women diagnosed with breast cancer had sought screening as a result of her knowledge of the number of cases. If she is removed from the observed number of women with breast cancer, the standardised incidence ratio falls to 5.63 and its lower confidence limit to 2.6. This is still a substantial and significant increase in risk. Three of the other women had their breast cancer diagnosed when they attended routinely for a screening mammogram. Does this indicate a higher level of screening in this population than in the general population? Probably not; about 35% of breast cancers in women 50-69 years of age in Australia, the target population for breast screening, are first detected by screening. While those detected by screening were 50 years of age or younger, there is a continuing high level of screening outside the organised program, particularly in younger women. Thus three breast cancers detected by screening out of a total of 10 is about the number expected in the population.
Risk factors unrelated to work or the working environment at Toowong It is possible that women working at ABC Toowong are at an unusually high risk of breast cancer because of risk factors unrelated to work or the working environment there: perhaps because of personal and social factors that attract people to different work or workplaces, or simply by chance. Because of this possibility we documented risk factors in the women who had been diagnosed with breast cancer to give some indication of the distribution of risk factors in the underlying workplace population. On most counts, the women with breast cancer were similar in their risk factors to the general female Australian population of the same age. They were somewhat better educated, and possibly, therefore, of higher socioeconomic status, and perhaps drank more alcohol than average, but within national guidelines. They may also have been more inclined to use oral contraceptives than Australian women in general. On the other hand, they probably smoked less and exercised more than women in general, both of which might reduce their risk of breast cancer. None of these is a particularly strong risk factor for breast cancer and there is no possibility that the small differences we observed in any of them could explain a six-fold increase in risk of breast cancer in ABC Toowong women, or even a three-fold increase (the lower 95% confidence bound).
Risk factors related to work or the working environment at Toowong By a process of exclusion we arrive at some aspect of work or the working environment at Toowong as the likely explanation for the high incidence of breast cancer there during the study period. Its plausibility is enhanced by the evidence that risk increased significantly with increasing duration of employment with the ABC and, arguably, by the concentration of cases of breast cancer in women who had worked in the newsroom. It is also a matter of concern that the increase in risk of breast cancer, relative to that in the general Queensland population, was much greater in younger than older women. While it has been pointed out to us that this

Breast Cancer at the ABC Toowong Queensland - Final Report Page 37 of 75
concentration in younger women could indicate the presence of high genetic risk of breast cancer, there seems to us to be no likely mechanism, except chance, that could have produced a clustering of women with a high genetic risk of breast cancer at the ABC. None with breast cancer reported a family history of the disease, which is against the possibility of such clustering.
What are the risk factors that could be responsible? We have failed to pinpoint any strongly plausible risk factor. It appears highly unlikely, on the basis of lack of evidence of unusual levels of exposure or lack of evidence that particular exposures increase risk of breast cancer, that any of the following are responsible:
• Radiofrequency electromagnetic fields, • Extremely low frequency electromagnetic fields, • Ionising radiation, • Chemical contamination of the site or • Chemical contamination of the site’s water supply.
We have noted, though, the evidence relating shift work to risk of breast cancer and it does appear that there is an unusually high level of shift work in this population, at least among those who were diagnosed with breast cancer and those who had other breast tumours or lumps. While we offer this as a possible contributing factor, present evidence on it as a risk factor for breast cancer does not suggest that it would be strong enough to explain a six-fold, or even perhaps a three-fold increase in risk in an exposed population.
Should we be concerned that there is no obvious cause for the cluster of breast cancers that has been observed at the ABC Toowong? While many might say yes, to find an explanation for such a cluster when investigated is the exception not the rule.
Heath and Hasterlick reported an early formal epidemiological investigation of a cancer cluster44. Eight children were diagnosed with leukaemia in Niles, a suburb of Chicago, from 1957 to 1960. All lived in the same residential neighbourhood and seven attended, or had older siblings who attended, a single parochial school. The authors concluded: “Although the exact cause of these cases was not identified, their association with one particular school, the time pattern of their occurrence and the parallel occurrence of a “rheumatic like” illness suggest an etiologic relationship to infection.” They also stated: “In the light of the experience in Niles further search for case clusters, coupled with detailed study of cases of leukemia and other cancers as they occur within particular communities, represents a promising approach to understanding the etiology of these diseases”.
In part prompted by the above conclusion and in part in response to community concerns, the United States Centre for Disease Control investigated 108 cancer clusters, mostly involving leukaemia, over the years from 1961 to 1981. No clear cause was found for any cluster45. More relevantly, perhaps, a review of the results of 61 workplace cancer cluster investigations done by the US National Institute for
44 Heath CW, Hasterlik RJ. Leukaemia among children in a suburban community. Am J Med 1963; 34: 796-812. 45 Caldwell G. Twenty-two years of cancer cluster investigations at the Centers for Disease Control. Am J Epidemiol 1990; 132: S43-S47.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 38 of 75
Occupational Safety and Health between 1978 and 1984 has also been reported46. The authors concluded that “Most of the clusters … had no plausible occupational etiology”. Known or suspected human carcinogens were identified in 43% of the investigations but “In almost all cases, only the presence of the carcinogen was determined, with no demonstrable relationship between the extent of exposure and risk of disease among individuals comprising the cluster”.
Reflection In the light of our failure to find a cause for the breast cancer cluster at the ABC Toowong and the unfruitful history of cluster investigations, should we have embarked on this investigation at all? We might, perhaps, have advised the ABC that no investigation should be done.
Present best advice about the conduct of cancer cluster investigations suggests that epidemiological investigations should be done only when these conditions are met47:
1. The observed number of cases of a specific type of cancer significantly exceeds the number expected;
2. Either the type of cancer or the age at onset is highly unusual; 3. The population at risk can be defined; and 4. Prolonged exposures to known or suspected carcinogens at levels that exceed
environmental limits can be documented.
In retrospect, at least, conditions 1, 2 and 3 were met. Condition 4 was not; though, in prospect, scientific and community concerns about possible carcinogenic effects of electromagnetic fields, albeit not strongly evidence-based, that might have been significantly elevated at the ABC could be said to have met it.
It is also true to say that had some cancer clusters not been investigated or exposed to some wise, scientific consideration, we would know much less about the causes of cancer now than we do. That prolonged exposure to soot causes scrotal cancer, to aniline dye manufacture causes bladder cancer, to asbestos (and some other mineral fibres) causes mesothelioma and to vinyl chloride monomer causes angiosarcoma of the liver, to mention just some examples, would not have been discovered when they were, and might not yet have been discovered at all, had not an alert scientific mind first observed and then investigated a cancer cluster.
Regardless of how one views this investigation’s justification from a scientific point of view, it is important not to lose sight of the wider contribution that an investigation like this might sometimes make. Clusters are often associated with a high level of anxiety in the affected community and great pressure on those in authority to do something. The ABC Toowong cluster is no exception. It seems to us that ABC management had three broad options: to do nothing and “dig in”, at considerable industrial risk; to agree to demands to move its operations from the Toowong site; or to investigate. Faced with these alternatives, investigation is not an unreasonable option to take.
46 Schulte PA, Ehrenberg RL, Singal M. Investigation of occupational cancer clusters: theory and practice. Am J Public Health 1987; 77: 52-6. 47 Thun MJ, Sinks T. Understanding cancer clusters. CA Cancer J Clin 2004; 54: 273-80.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 39 of 75
In the event, while inconclusive with respect to the cause of the cluster, our investigation found sound statistical evidence that breast cancer was related to length of employment and thus may have been contributed to by some aspect of work or the working environment at Toowong. On this basis, ABC management chose to remove its operations from the Toowong site. This outcome appears to have substantially addressed the concerns of the affected workforce and to have largely eliminated pressure on management for further action directed specifically towards the cancer cluster.
Time will tell if it has also brought an end to clustering of breast cancer in the ABC female workforce formerly at Toowong.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 40 of 75
Conclusions The Panel concludes that
• There was a real increase in the risk of breast cancer in women working at the ABC Toowong site that was related to length of employment and may have been contributed to by some aspect of work or the working environment at Toowong.
• It was highly unlikely that this increase was caused by exposure during work on the Toowong site to radiofrequency electromagnetic fields, extremely low frequency electromagnetic fields, ionising radiation or chemicals known or suspected to cause breast cancer.
• There was also little or no evidence to suggest that the increase in risk could be explained by an underlying high risk of breast cancer in women employed at Toowong due to their sharing of known genetic or lifestyle risk factors for breast cancer.
• While we have not been able to find a cause for the increase in risk of breast cancer at the ABC Toowong, we believe that we have considered and excluded all plausible environmental explanations for such an increase. We do not recommend, therefore, that any further environmental investigations are done on the site.
• If there is a currently unknown or undetected aspect of work or the working environment at the ABC Toowong that could have contributed to the observed increase in risk of breast cancer, it might also be present in similar ABC studio complexes elsewhere in Australia. We recommend, therefore, the conduct of similar investigations into the frequency of breast cancer among women who have worked on those sites at some time since 1994, as we have done at Toowong.
Absence of an increase in risk of breast cancer in women working at these other sites would provide reassurance to them and the ABC that this is not a systemic problem. It would also help to reassure women who worked at the ABC Toowong that whatever has caused their increased risk of breast cancer is unlikely to be present in their new workplaces. Presence of an increase would justify more extensive investigations as to possible causes.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 41 of 75
Acknowledgements We gratefully acknowledge the contributions that many other people made to our investigations and to the completion of this report.
Most importantly, we thank the ABC staff at Toowong for supporting the Panel’s investigations and being understanding and patient while they were done. We especially thank present and former female staff members who had been diagnosed with breast cancer or other breast tumours or lumps and generously gave us the information we needed to do our task. Without their assistance and support, this investigation would have been impossible. Deb Beel was our day-to-day link with the staff at Toowong and made all our administrative arrangements; she has our special thanks. We are also very grateful for the contribution made by members of the Staff Reference Group: Ian Eckersley, Nadia Farhar and Kate Scanlan. Their advice in the formative stages of our investigation was invaluable, as was there ongoing support and the links that they provided to other ABC staff members and, particularly, the women who had been diagnosed with breast cancer. We also thank Neville Lesleighter, the Building Services Coordinator for ABC Queensland, who gave advice on and responded to many questions about the Toowong site.
We were greatly aided by the support and understanding of ABC senior management. The Managing Director, Mark Scott, gave us an open brief to investigate the occurrence and causes of breast cancer at Toowong and independence to work equally with and for staff and management. David Pendleton, the ABC’s Chief Operating Officer, made it very easy for us to engage all other assistance we needed to get the job done and thus contributed greatly to the timely conduct of our investigations.
Many other people contributed to the work of the investigation. Specifically we acknowledge and thank: • Lesley Walker for assisting in the development of the questionnaire used when
interviewing women diagnosed with breast cancer and preparing an initial draft of the literature review;
• Dr Peter Baade and Mr Danny Youlden from the Viertel Centre for Research in Cancer Control at The Cancer Council Queensland who compiled, analysed and prepared a report on data on the epidemiology of breast cancer at the ABC Toowong;
• Geza Benke for his assessment of possible carcinogenic hazards in the Toowong workplace, his advice on measurements that we should make and for his willing advice and guidance on the results and interpretation of the measurements;
• John Loy, CEO, Colin Roy and other staff members of ARPANSA, for their willingness to undertake measurements at Toowong with short notice and close to Christmas;
• Ken Karipidis and Lindsay Martin of ARPANSA, who measured ELF at Toowong and advised us on interpretation of the results;
• Owen Wilson of ARPANSA, who measured ionising radiation at Toowong and advised us on interpretation of the results; and
• Many members of the public who contacted us directly or through the ABC to give us their ideas and suggestions about the nature and causes of the breast cancer problem at Toowong. Their contributions have enriched our understanding.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 42 of 75
Appendices
Appendix 1 Questionnaire used when interviewing women who were diagnosed with breast cancer while working at the ABC Toowong between 1st January 1994 and 30th June 2006
Appendix 2 ABC Toowong: Hazards assessment and further monitoring requirements. Report of the occupational hygienist, Dr Geza Benke, following a visit to Toowong on 13th November 2006
Appendix 3 Brisbane Water’s Scientific and Analytical Services Report on water samples collected from the ABC Toowong water supply on 15th December 2006
Appendix 4 Assessment of Exposure to Power Frequency Magnetic Fields in the ABC TV Building at Toowong, Brisbane. Report of ARPANSA measurements and monitoring in December 2006
Appendix 5 Ionizing Radiation Survey of the ABC TV News Building – Toowong Queensland. Report of ARPANSA measurements and monitoring, December 2006 to February 2007

Breast Cancer at the ABC Toowong Queensland - Final Report Page 43 of 75
Appendix 1: Questionnaire Questionnaire used when interviewing women who were diagnosed with breast cancer while working at the ABC Toowong between 1st January 1994 and 30th June 2006

ABC EXPERT PANEL INTERVIEW
Breast Cancer at the ABC Toowong Queensland - Final Report Page 44 of 75
NAME OF INTERVIEWER ID NUMBER Day Month Year _____________________________________ DATE NAME OF INTERVIEWEE Day Month Year _____________________________________ DOB BEST CONTACT NUMBER __________________________________________________________________________ LOCATION OF INTERVIEW __________________________________________________________________________ __________________________________________________________________________ __________________________________________________________________________ The questions I’m going to ask you will be about aspects of your health, work and lifestyle that are known or thought to influence risk for breast cancer. To be able to fully investigate the concern about breast cancer we need both the work history and health and lifesyle information. Any questions? The way we have set the questions is in sections, we have started with your work, present lifestyle and leisure activities, we will then go through your whole menstrual history from the start of your periods up to now. Then we will go on to your breast health history and your family history. If at any point if there is anything you feel is relevant for us to know, please feel free to tell me.

ABC EXPERT PANEL INTERVIEW
Breast Cancer at the ABC Toowong Queensland - Final Report Page 45 of 75
SECTION A: WORK HISTORY AT THE ABC AND ELSEWHERE AND RESIDENTIAL HISTORY I WOULD LIKE TO ASK YOU SOME QUESTIONS ABOUT YOUR WORK AT THE ABC 1. WHEN DID YOU START WORKING AT THE ABC? Month Year 2. STARTING WITH YOUR FIRST JOB, I’M GOING TO ASK YOU A SERIES OF QUESTIONS ABOUT EACH OF YOUR JOBS AT THE ABC Job No.
Job title
Main duties
Hours per week
Shift work
Month and year started
Month and year finished
Main location (please mark on the site map)
Any special equipment or exposures you are concerned about
1
2
3
4
5
6

ABC EXPERT PANEL INTERVIEW
Breast Cancer at the ABC Toowong Queensland - Final Report Page 46 of 75
7
8
9
10
11
12
13
14
15

ABC EXPERT PANEL INTERVIEW
Breast Cancer at the ABC Toowong Queensland - Final Report Page 47 of 75
I WOULD LIKE TO ASK YOU SOME QUESTIONS ABOUT YOUR WORK OTHER THAN AT THE ABC 3. HAVE YOU WORKED WITH ANOTHER EMPLOYER? YES NO 4. IF YES, STARTING WITH YOUR FIRST JOB, I’M GOING TO ASK YOU A SERIES OF QUESTIONS ABOUT EACH OF THESE JOBS Job No.
Job title
Main duties
Hours per week
Shift work
Month and year started
Month and year finished
Location Any special equipment or exposures you are concerned about
1
2
3
4
5
6
7

ABC EXPERT PANEL INTERVIEW
Breast Cancer at the ABC Toowong Queensland - Final Report Page 48 of 75
8
9
10
5. IS THERE ANYTHING ELSE YOU WOULD LIKE TO TELL ME ABOUT YOUR WORK AT THE ABC OR ELSEWHERE?
I WOULD LIKE TO ASK YOU SOME QUESTIONS ABOUT PLACES YOU HAVE LIVED 6. STARTING WITH YOUR FIRST RESIDENCE, I’M GOING TO ASK YOU A SERIES OF QUESTIONS ABOUT EACH OF THESE PLACES

ABC EXPERT PANEL INTERVIEW
Breast Cancer at the ABC Toowong Queensland - Final Report Page 49 of 75
Residence
No. Name of town or suburb
Nature of this area, eg city/rural/industrial/farming
Month and year started living here
Month and year finished living here
Any parrticular exposures you were concerned about in this area
1
2
3
4
5
6
7
8
9
10
ABC EXPERT PANEL INTERVIEW
Breast Cancer at the ABC Toowong Queensland - Final Report Page 50 of 75
11
12
13
14
15
7. WHAT WAS YOUR FATHER’S MAIN OCCUPATION? _____________________________________________ 8. WHAT WAS YOUR MOTHER’S MAIN OCCUPATION? _____________________________________________

ABC EXPERT PANEL INTERVIEW
Breast Cancer at the ABC Toowong Queensland - Final Report Page 51 of 75
SECTION B I WOULD LIKE TO ASK YOU SOME GENERAL QUESTIONS ABOUT YOU AND YOUR LEISURE ACTIVITIES 1. How tall are you? Feet & Inches OR Cms
and
2. How much do you weigh? Stones & lbs OR Kgs
3. How often do you do any exercise? Give some examples like walking
Rarely/Never 2-3 times a week less than once a week 4-6 times a week Once a week Every day
4. How often do you do strenous exercise like running, aerobics? explain
Rarely/Never 2-3 times a week less than once a week 4-6 times a week Once a week Every day
5. On average, how many hours on a typical weekday would you spend doing sitting down activities like driving, reading, watching television or working at a desk or computer?
<1hr 5-6 hrs 1-2 hrs 7-8 hrs 3-4 hrs >8 hrs
6. On average, how many hours on a typical weekend would you spend doing sitting down activities like driving, reading, watching television or working at a desk or computer?
<1hr 5-6 hrs 1-2 hrs 7-8 hrs 3-4 hrs >8 hrs
NO YES 7. Have you ever been a smoker? If ‘NO’ go to Question 8
Years

ABC EXPERT PANEL INTERVIEW
Breast Cancer at the ABC Toowong Queensland - Final Report Page 52 of 75
7a How old were you when you first started smoking? Number 7b. How many cigarettes do you now or did you smoke each day, on average?
NO YES 7c. Are you an ex-smoker?
Years
7d. For how many years did you smoke? 8. On average each week how much wine, beer or spirits do you drink?
Number 8a. Wine – number of glasses (125ml) per week explain
Number 8b. Beer – number of glasses (250ml of 5%; 500ml of light beer) per week explain
Number 8c. Spirits – number of measures (30ml) per week 8d. What is your marital status? TICK BOX
Single 1 Married 2 Divorced 3 Separated 4 Widowed 5 Other [please specify]: 6
Is there anything else you would like to add?

ABC EXPERT PANEL INTERVIEW
Breast Cancer at the ABC Toowong Queensland - Final Report Page 53 of 75
SECTION B I’D NOW LIKE TO ASK YOU SOME QUESTIONS ABOUT WHEN YOU WERE YOUNGER
Years
9. What age were you when you finished school? 10. What is the highest level of qualification you have completed? TICK BOX
No formal qualification 1 School Certificate (or equivelent) 2 HSC (or equivalent) 3 Trade / apprenticeship 4 Certificate or Diploma 5 Degree or higher degree 6 Other [please specify]: 7
Years
11. How old were you when your periods started ?
NOTES

ABC EXPERT PANEL INTERVIEW
Breast Cancer at the ABC Toowong Queensland - Final Report Page 54 of 75
SECTION C I WOULD NOW LIKE TO ASK YOU SOME QUESTIONS ABOUT YOUR USE OF THE PILL
NO YES 12. Have you ever used the pill (oral contraceptive)?
if No, please go to Question13
Years 12a. Can you remember how old were you when you first went on the pill?
Years 12b. Do you remember how old were you when you last came off the pill?
Years
12c. can we work out how many years in total you did take the pill? (Add together the years and months when she actually took the pill. Do not count the years and months when she was not taking it. Write "0" if she used the pill for less than a year in total) I WOULD LIKE TO ASK YOU SOME QUESTIONS ABOUT PREGNANCIES
Number
13. How many pregnacies have you had excluding miscarriages ?
If None, please go to Question 14 13a. What was the date of birth for each child born, (including stillbirths)? List from eldest to youngest and if they were twins or triplets repeat the same date for each child. And for how many months did you breastfeed, if at all? Breastfeeding, if not breast fed put ‘0’ if breastfed for a month or less put ‘1’
DATE OF BIRTH (if livebirth) Day Month Year Stillbirth Livebirth Breastfed- Months Child 1 Child 2 Child 3 Child 4 Child 5 Child 6

ABC EXPERT PANEL INTERVIEW
Breast Cancer at the ABC Toowong Queensland - Final Report Page 55 of 75
NOW I WOULD LIKE TO ASK YOU SOME QUESTIONS ABOUT THE USE OF HORMONE REPLACEMENT THERAPY (HRT) NO YES 14. Have you ever had a hysterectomy?
Years 14a. If Yes how old were you? DON'T NO YES KNOW
15. Have you ever had both ovaries removed?
DON'T NO YES KNOW
16a. Have you gone through the menopause? NO YES Irregular
16b. Have your Periods now stopped?
If Yes Years
16c. How old were you when they stopped?
16d. For what reason did your periods stop TICK BOX A Hysterectomy and/or removal of overies Post Menopause Medication (pls describe) ________________________ Other (pls describe) _____________________________
NO YES
17. Have you ever used hormone replacement therapy (HRT)? If NO go to SECTION D Years
17a. How old were you when you first started using HRT? NO YES
18. Had your periods stopped before you started using HRT? ("Yes" if you had a hysterectomy before starting HRT)
Years
19. How many years in total you have used HRT? (Add together the years and months when you used HRT – do not count the years and months when you were not using HRT. Please write "0" if you used HRT for less than a year in total)
NO YES
20. Are you now using HRT?

ABC EXPERT PANEL INTERVIEW
Breast Cancer at the ABC Toowong Queensland - Final Report Page 56 of 75
If NO Years 20a., (Name) how old were you when you last used HRT? Is there anything else you would like to add?
NOTES

ABC EXPERT PANEL INTERVIEW
Breast Cancer at the ABC Toowong Queensland - Final Report Page 57 of 75
SECTION D Part 1. The next section is about your breast cancer diagnosis, if you find the questions upsetting or painful just let me know and we can stop for a while or we can come back to the questions later. I WOULD NOW LIKE TO ASK YOU SOME QUESTIONS ABOUT MAMMOGRAPHY, BREAST CANCER AND OTHER BREAST LUMPS 21. When was the breast cancer diagnosed? Month Year
Age 22. How old were you ? 23. How was the breast cancer found TICK BOX
Felt a lump in the breast 1 Some other symptom -if so what____________________________ 2 Mammogram 3
If BY Mammogram
23a. Was this mammogram: TICK BOX A regular screening mammogram (define) done at time it was due? 1 Prompted by publicity or concerns about the occurance of breast ca in women at the ABC 2 Prompted by a symptom or some other factor not related to the publicity at the ABC 3 If yes, what symptom or factor? ____________________________________ 24. How was the breast cancer treated? TICK BOX
Surgically removed - mastectomy 1 Surgically removed - lumpectomy 2 Radiotherapy 3 Chemotherapy 4 Other____________________________ 5
24a. If surgically treated, when was this? Month Year
25. Have you had any other kind of breast lump or tumour in the breast NO YES Including, a prior breast cancer?
If yes, for each instance
25a. When was it found? Month Year

ABC EXPERT PANEL INTERVIEW
Breast Cancer at the ABC Toowong Queensland - Final Report Page 58 of 75
25b. How was it first found? ____________________________________________ ________________________________________________________________ 25c. Was it biopsied or removed surgically? NO YES 25d. What were you told it was? ___________________________________________ ________________________________________________________________ Is there anything else you would like to add?
NOTES

ABC EXPERT PANEL INTERVIEW
Breast Cancer at the ABC Toowong Queensland - Final Report Page 59 of 75
SECTION D - Part 2: Other questions about mammography
26. Excluding any mammograms already mentioned: Had you had any other screening mammograms before diagnosis NO YES of your most recent breast cancer/breast lump
A screening mammogram is an x-ray of the breast used to detect breast changes in women who have no signs or symptoms (asymptomatic) of breast cancer. It usually involves two x-rays of each breast
If NO go to Section E
27. When was your first screening mammogram? Year Month
28. When was your last screening mammogram? Year Month
Number
29. How many screening mammograms in total have you had? Or
Months 29a. On average how often do have a screening mammogram?
Is there anything else you would like to add?
Notes:

ABC EXPERT PANEL INTERVIEW
Breast Cancer at the ABC Toowong Queensland - Final Report Page 60 of 75
SECTION E NOW I WOULD LIKE TO ASK YOU SOME QUESTIONS ABOUT YOUR FAMILY NO YES 30. Do you have any sisters
DON'T
31. Have either of your grandmothers, your mother, or (either/any of) NO YES KNOW your sister(s) ever been diagnosed with breast cancer?
If YES who TICK BOX Your Maternal grandmother Paternal Grandmother Mother Sister(s) (if yes how many) (Name) Age 32. How old was your ____________ when the breast cancer was first diagnosed? and Age 33. How old was your _____________ when the breast cancer was first diagnosed? Age 34. How old was your _____________ when the breast cancer was first diagnosed? Is there anything else you feel is relevant for us to know which hasn’t been covered in this interview?
I WOULD LIKE TO THANK YOU FOR YOUR ASSISTANCE IN COMPLETING THIS INTERVIEW

Breast Cancer at the ABC Toowong Queensland - Final Report Page 61 of 75
Appendix 2: Hazards assessment ABC Toowong: Hazards assessment and further monitoring requirements. Report of the occupational hygienist, Dr Geza Benke, following a visit to Toowong on 13th November 2006
ABC Toowong
Hazards assessment and further monitoring requirements
Geza Benke, PhD
Centre for Occupational and Environmental Health Department of Epidemiology and Preventive Medicine
Monash University Victoria
Brief
This report aims to document the history of the ABC Toowong site with respect to hazards possibly causative of breast cancer. The hazards investigated were in part identified through information from the work histories collected by Professor Malcolm Sim and also in part from a walk through survey undertaken by Dr Benke on Monday 13th November 2006. The information in this report should be used to direct further environmental monitoring where considered necessary and to comparatively assess risk from all possible environmental hazards on the site. 1. Site history: Overview Prior to the construction of the first ABC buildings on the site in 1959, the site spanned two residential premises, Middenbury House and Sydney House. The plans of 1/5/1959 clearly show that the TV building was constructed over a former driveway/car-park to the original residences. This history eliminates the possibility that the TV building was constructed on a former orchard (possible pesticide residues) or an industrial site (unknown radiation source or contaminated site). The TV building was constructed in five stages, with the initial stage in 1959, stage two in 1961, stage three about 1967, stage four in about 1985 and the latest refurbishment over the former car-park in 2000. The current TV building is constructed on a concrete slab and does not have any basement levels. Prior to 1985 the TV News group was broken across a number of locations i.e. under the lower ground and off site. Management of Radio was at Sherwood Road prior to 1985. In 1985 TV News was located in the First Floor of the TV Building. In 2000, following an extension of the ground floor, that involved the inclusion of the former river side car-park, the TV News group was relocated to the ground floor. The current occupiers of the first floor are the Digital group that went “On-line” about 2003, but

Breast Cancer at the ABC Toowong Queensland - Final Report Page 62 of 75
were formed in 1997. The Digital group formed as a small subunit in 1997 and were part of the Radio News group for the first 5 to 6 years of operation. Radio News has been located on the ground floor since 1985, and was joined by TV News after the 2000 refurbishment. 2. Physical Hazards 2.1 Ionizing radiations There is no documented history of the use of ionizing radiation on the site. Given the nature of the operation of the ABC at Toowong it is also unlikely any irradiating apparatus i.e. X-ray or industrial radiography machines, or radioisotopes, have been ever used/operated on the site. Radiation contamination could only be possible on-site if the original (or subsequent) construction material had been inadvertently contaminated (an extremely unlikely occurrence) prior to it arriving on-site. Radon gas exposure is unlikely, but possible. Radon gas and it’s progeny usually builds-up in cellars and well sealed buildings and a survey undertaken by ARPANSA about 20 years ago found that exposure inside Australian buildings and dwellings to radon is negligible. 2.2 Non-Ionizing radiations 2.2.1 Radiofrequency (RF) Since this has been a TV and radio broadcasting and receiving site for over 40 years it has numerous RF communications devices located within its perimeter. The current RF sources are described in both the THL Australia report of 16th February 2004 and the EMC Technologies report B050401, 2nd May 2005. A history of the equipment on site prior to 1980 was not forthcoming. However, it appears that most of the equipment on site was added in the past twenty years due to advances in technology, with little replacement of older receivers and transmitters. It can be assumed that the current RF exposure levels are probably higher than at any time during the operation of the site, due to the incremental addition of RF sources. The THL RF Hazard control document of 16th February 2004 indicates that the most prominent RF source on site is the 7 meter satellite dish on the TV Building rooftop, operating at 14 Ghz. The three VHF Comms, 3 metre antennae have high maximum power and operate between 168 and 172 MHz. Overall the RF sources on site cover a wide range of frequencies and power outputs. In these circumstances it is advisable to check the broadband exposures in the offices below. The EMC RF survey clearly indicated that broadband exposure levels were well below the ARPANSA reference levels, as outlined in the 2002 ARPANSA standard for exposure to RF radiation between frequencies of 3kHz and 300GHz. In all the office work areas in the TV building the levels were below the detection limit of the survey meter (<2 V/m). This is not surprising in view of the RF sources currently in place and the known high directionality of these sources. Additionally, since the broadband measurements do not indicate any excess exposure to RF it is most unlikely any future narrow band measurements will result in excessive exposure results in the office areas.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 63 of 75
The security card readers operate at only 125kHz , significantly lower than the other RF sources on site. The card readers can be categorized as low frequency (LF) sources compared to the other sources on site. The concern from staff was that if the hands were engaged in carrying books, bags or equipment, the employee would simply bring their chest in close proximity to the card reader and perhaps be exposed to intermittent high levels of RF radiation. The EMC report indicated that at 5 centimetre distance from the card reader the levels were only about a quarter the reference levels. In addition, given the brief exposure periods over the course of a work-shift i.e. perhaps 1 to 2 minutes at most per day, the time-weighted average exposure should be extremely low. 2.2.2 ELF-EMF The ELF-EMF (50/60 Hz) exposure has not been measured in the TV building. Given the high concentration of communications equipment in many of the workstations in this building, exposure is expected to be higher than in a normal office environment e.g. computers and Decart audio systems are located at many workstations, there are also large number of editing rooms with electronic equipment etc. The power requirement to the ABC Toowong site is clearly significant, given the site has its own substation. This indicates that there exists many potential power intensive sources and that power frequency currents, required for high ELF-EMF exposures are present. 3. Chemical Hazards 3.1 Asbestos The construction of the TV building involved the use of materials containing asbestos. These were primarily the use of AC sheeting, asbestos vinyl tiles and millboard. Significant removal was undertaken in the late 1980s with a few small batches removed about 2000 (at the time of refurbishment of the ground floor and renovation of the air-conditioning system). Asbestos in the heater banks and asbestos containing millboard were also involved in the latter removals. All removal was undertaken by an approved asbestos removalist and all documentation required under Queensland OHS regulations are kept on site. Generally, the removal of AC sheeting does not present a high risk for asbestos exposure, if the removal is undertaken by a competent removalist. It is also unlikely exposure to friable asbestos would be present in the office areas of the TV building at the times during removal given the requirement for containment in the Queensland regulations dating back to the mid-1980s. 3.2 Environmental Tobacco Smoke (ETS) Smoking was banned inside buildings at the Toowong ABC site in March 1989. It is now impossible to assess the extent of passive smoke exposure in the work areas of the TV building in the 1980s. Recall of persons that may have worked in this environment would be unreliable and could not be compared with other office environments. Population smoking rates were higher in the 1980s and so an estimate of exposure based on the current number of smokers in the employ of the ABC today would probably be an underestimate.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 64 of 75
3.3 Pesticides Since the site was a residential premise prior to construction of the ABC buildings it is unlikely any pesticide contamination was present at the site pre-1960. Arrest-a-Pest has been the pest control contractor since at least the early 1980s. The pesticides of most concern are the organochlorines (OCs) comprising chemicals such as DDT, Lindane and Chlordane. This group of insecticides has a relatively long residual time in the environment (5 years) and they are weak estrogens which may increase breast cancer risk by mimicking endogenous estradiol. The pesticides of less concern are the organophosphates, carbamates and synthetic pyrethrins, which have relatively short environmental residual times (days to a month at most) and do not accumulate in body tissue over prolonged time periods. The use of OCs was discontinued in Queensland about 1995. Between 1985 and 1995 OCs were used in very limited quantity for termite control around the exterior of buildings and under slabs prior to construction. The use of OCs inside buildings and homes was discontinued in Queensland in the early 1980s. Synthetic pyrethrins have been predominantly used for termite control in the past 10 years. Following contact with Mr Chris Hill of Arrest-a-Pest it was confirmed that no significant quantities of OCs were used at the ABC Toowong site (Mr Hill has been in the employ of Arrest-a-Pest since 1989). Mr Hill could not comment on the use of OCs at the site pre-1980s. 3.4 Water The water supply to the site is from the Brisbane community water supply and most unlikely to be contaminated. There has been no water testing undertaken from water taps at the site. Heavy metal contamination, such as arsenic, cadmium, chromium, lead, mercury or nickel is possible if the water piping has been contaminated by some outside source or there has been significant corrosion of old piping. Testing of the drinking water in accordance with the NHMRC Australian Drinking Water Guidelines 2004, could reveal if heavy metal contamination is present. Although we believe these measurements are unlikely to identify any heavy metal concentrations above the guideline standards, they should eliminate this as a potential source of toxic intake. It must also be emphasised that measurements undertaken in 2006 are unlikely to have much bearing upon the water quality of earlier years e.g. 1995 or 1985, since concentrations to some metals could change due to corrosion in the metal pipes etc. 3.5 Other chemicals, hydrocarbons and solvents Concerns were raised that there may have been exposure to other chemicals, hydrocarbons and solvents via: (i) Tanks removed from the car-park area in 2000
Two former petrol tanks were removed from the car-park in 2000. These tanks were disused since 1996 and remained in-situ for four years. This time period would have enabled any volatile hydrocarbons trapped in the tanks or soil to have successfully evaporated. There would only have been high-carbon hydrocarbons remaining at the time of removal, with little if any volatile hydrocarbons present. Soil measurements were taken at the time of the removal with the results showing no contamination found.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 65 of 75
(ii) Cleaning of the air-conditioning system Concerns had been raised about chemicals used for the cleaning of the air-conditioning system for the TV building. Contact was made with Mr Bruce Clayton of Haden, the air-conditioning contractors for the site. Mr Clayton confirmed that the condensate trays were cleaned with a common detergent to remove slime on an infrequent basis. This is a soap-based detergent and therefore not considered toxic. There is also routine maintenance undertaken on the ductwork that involves vacuuming also on an infrequent basis. The filters are not cleaned but replaced once the pressure drop exceeds 150 pascals, and this is normally required about once a year. The heat exchangers are cleaned of grime on an infrequent basis by a chemical named “Coil and Filter cleaner AK’ manufactured by Sterile-Care Pty Ltd. The Material Safety Data Sheet (MSDS) was obtained for this product and indicated that the active ingredient was a Quaternary ammonium compound and that it also contained alkaline salts at a concentration of 90 grams per litre. Neither of these compounds are considered carcinogens or suspected carcinogens in the literature. Ammonium compounds have been linked with respiratory disease such as occupational asthma, and alkaline salts are considered skin irritants.
(iii) Ceiling tiles
The ceiling tiles in the ground floor of the TV building were installed during the refurbishment undertaken in 2000. These are Armstrong RH90 tiles manufactured in the USA in December 1997 with batch no. S3570B, recorded on them. Access to the MSDS of this product can be obtained via the Armstrong website: www.armstrong.com/home/us/en/. Prior to the refurbishment in 2000, Gyprock with vinyl coating ceiling tiles were fitted throughout the building since the 1970s. These products are unlikely to have any off-gassing of volatile organic compounds (VOCs) such as n-hexane, n-pentane, xylenes, toluene or 2-mthyl butane. Formaldehyde off-gassing has been a hazard in commercial office buildings using older style ceiling tiles, but this is almost certainly not the case in the TV building.
4. Recommendations for further monitoring Recommendation 1: Given that ionizing radiation is the only known environmental exposure that increases breast cancer risk, it would be prudent to undertake radiation dose rates, contamination monitoring and radon gas concentration measurements in the TV building. This should confirm whether radiation levels are at normal background or whether there has possibly been some contamination present from an as yet unknown source. Recommendation 2: An ELF-EMF measurement survey should be undertaken on the ground and first floor of the TV building. This should involve dosimetry to workers in various workstations on both floors. Recommendation 3: Water testing be undertaken in accordance with the NHMRC Australian Drinking Water guidelines 2004.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 66 of 75
5. References Hansen J. Breast cancer risk among relatively young women employed in solvent–using Industries. Am J Ind Med 1999;36:43-47 McElroy J, Shafer M, Trentham-Dietz A et al. Cadmium exposure and breast cancer risk. J Natl Cancer Inst 2006;98:869-73 Tokunaga M, Land C, Tokuoka S et al. Incidence of female breast cancer among atomic bomb survivors 1950-1985. Radiat Res 1994;138:209-223 Weiderpass E, Pukkala E, Kauppinen T et al. Breast cancer and occupational exposures in women in Finland. Am J Ind Med 1999;36:48-53 Wells A. Breast cancer, cigarette smoking, and passive smoking. Am J Epidemiol 1991;133:208-210 APPENDIX 1. Specifications for measurements according to recommendations: Ionizing Radiation Surface contamination should be checked in the office areas of the ground floor and first floor of the TV Building with a Portable Contamination Meter fitted with an alpha/beta radiation probe. Dose rates are to be measured in the office areas with a calibrated dose-rate meter. Radon concentrations should be measured by use of a real-time radon monitor. In addition, dose-rate measurements should be measured at the air-conditioner filters to the building, as these are most likely to trap natural radioactivity from the air. Results are to be compared with the backgrounds in the Brisbane area. Power Frequency EMF For a survey of ELF-EMF exposure we suggest the use of EMDEX-II dosimeters to assess the time-weighted daily exposure of about four or five workers on the ground floor and a similar number on the first floor of the TV Building. It is important that personal measurements are ascertained as spot measurements alone will not be sufficient. A handful of measurements should also be undertaken with workers in the Woodhouse building and the Riverside Block (to act as controls). The results may then be compared with industry norms published in the Australian and international literature. Spot magnetic field measurements should also be undertaken in the TV Building, particularly in the vicinity of the workstations where the personal dosimetry is undertaken. These measurements should indicate the main sources of ELF exposure. Water Testing The water testing should be undertaken according to the National Health and Medical Research Council- Australian Drinking Water Guidelines 2004. We suggest that samples be taken on the ground floor and first floor of the TV Building. The samples should be analysed for concentrations of arsenic, cadmium, chromium, lead, mercury,

Breast Cancer at the ABC Toowong Queensland - Final Report Page 67 of 75
barium and nickel and compared with the health standards in Table 10.10 in section 10.8 of the Guidelines. We do not see any need to analyse the samples for organochlorine pesticides listed in Table 10.11 of the guidelines.
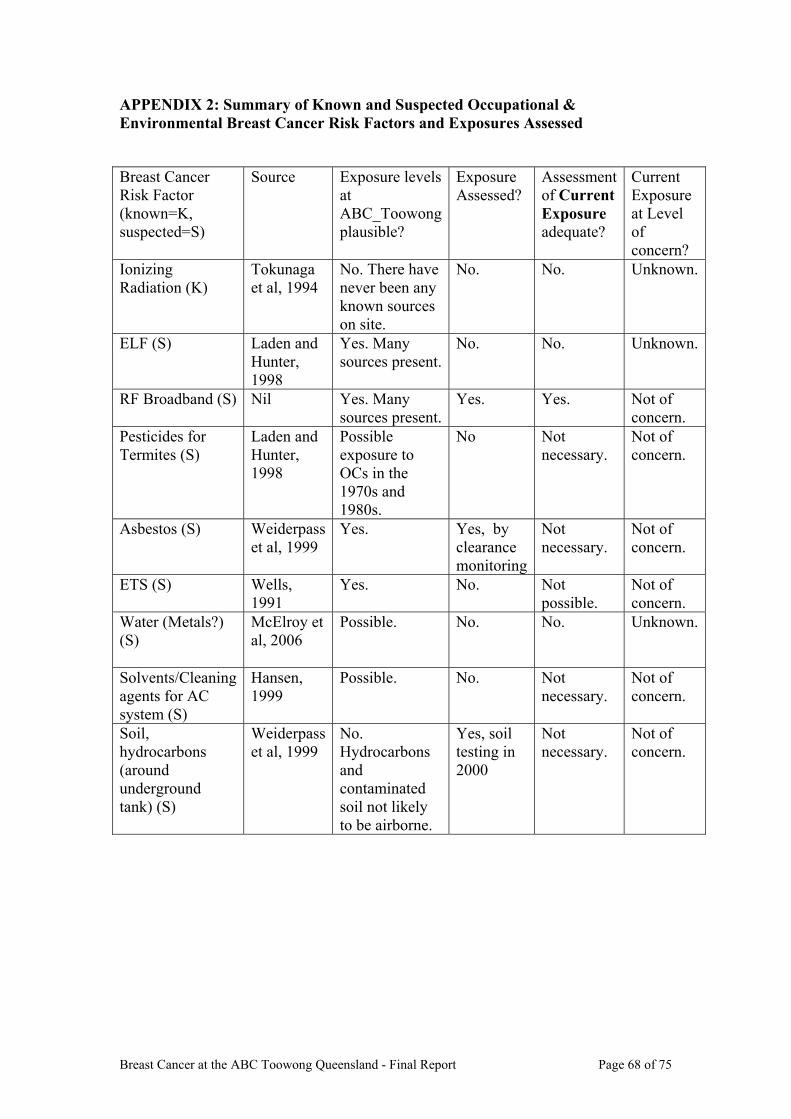
Breast Cancer at the ABC Toowong Queensland - Final Report Page 68 of 75
APPENDIX 2: Summary of Known and Suspected Occupational & Environmental Breast Cancer Risk Factors and Exposures Assessed
Breast Cancer Risk Factor (known=K, suspected=S)
Source Exposure levels at ABC_Toowong plausible?
Exposure Assessed?
Assessment of Current Exposure adequate?
Current Exposure at Level of concern?
Ionizing Radiation (K)
Tokunaga et al, 1994
No. There have never been any known sources on site.
No. No. Unknown.
ELF (S)
Laden and Hunter, 1998
Yes. Many sources present.
No. No. Unknown.
RF Broadband (S)
Nil Yes. Many sources present.
Yes. Yes. Not of concern.
Pesticides for Termites (S)
Laden and Hunter, 1998
Possible exposure to OCs in the 1970s and 1980s.
No Not necessary.
Not of concern.
Asbestos (S)
Weiderpass et al, 1999
Yes. Yes, by clearance monitoring
Not necessary.
Not of concern.
ETS (S)
Wells, 1991
Yes. No. Not possible.
Not of concern.
Water (Metals?) (S)
McElroy et al, 2006
Possible. No. No. Unknown.
Solvents/Cleaning agents for AC system (S)
Hansen, 1999
Possible. No. Not necessary.
Not of concern.
Soil, hydrocarbons (around underground tank) (S)
Weiderpass et al, 1999
No. Hydrocarbons and contaminated soil not likely to be airborne.
Yes, soil testing in 2000
Not necessary.
Not of concern.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 69 of 75
Appendix 3: Report on water testing Brisbane Water’s Scientific and Analytical Services Report on water samples collected from the ABC Toowong water supply on 15th December 2006

Breast Cancer at the ABC Toowong Queensland - Final Report Page 70 of 75

Breast Cancer at the ABC Toowong Queensland - Final Report Page 71 of 75
Appendix 4: Report on ELF measurements Assessment of Exposure to Power Frequency Magnetic Fields in the ABC TV Building at Toowong, Brisbane. Report of ARPANSA measurements and monitoring in December 2006 [Provided as a separate pdf file]

Breast Cancer at the ABC Toowong Queensland - Final Report Page 72 of 75
Appendix 5: Report on ionising radiation measurements Ionizing Radiation Survey of the ABC TV News Building – Toowong Queensland. Report of ARPANSA measurements and monitoring, December 2006 to February 2007 Ionizing Radiation Survey of the ABC TV News Building – Toowong
Queensland
Owen Wilson Radiation Safety Officer
ARPANSA March 2007
Introduction At the request of the ABC Breast Cancer Investigation Panel, ionizing radiation levels in the ABC TV News Building, 600 Coronation Drive Toowong, were monitored by ARPANSA officers on 18 December 2006. Significant exposure to ionizing radiation is a recognised risk factor for various cancers. No such exposures were known to have occurred in the TV News Building. The measurements were carried out to ensure that no unknown source of ionizing radiation existed that may have linked the TV News Building with the observed breast cancer cluster. Monitoring Equipment Surface contamination levels were monitored by use of an NE Technology LTD, Electra 1A rate meter (Serial No. 4045), connected to an NE Technology LTD, DP2R/4A dual phosphor scintillation probe (Serial No. 10744). This contamination monitor is sensitive to alpha and beta radiation. It also detects gamma radiation but with less sensitivity. Dose rates were measured by use of a Rados RDS-120 Universal Survey Meter (Serial No. 990079). This instrument is sensitive to gamma radiation over the energy and dose rate ranges needed to identify a source of potential risk. Personal doses were measured by use of TLD (thermoluminescent dosimeter) personal radiation monitors issued by the ARPANSA Personal Radiation Monitoring Service (PRMS). These monitors measure accumulated occupational dose over an extended exposure period. The results from these monitors are background subtracted. A control monitor is used to subtract natural background, leaving only personal radiation dose in excess of background. Radon concentrations in air were monitored by use of CR-39 track-etch radon area monitors, issued by PRMS. These monitors measure the average radon concentration over an extended exposure period. Each monitor also contains a TLD disk that is sensitive to beta and gamma radiation. The TLD is used to estimate environmental radiation dose for the exposure period. The results from these TLD are not background subtracted.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 73 of 75
Methods The measurement methods were consistent with the recommendations of the “ABC Toowong Hazards assessment and further monitoring requirements” report by Geza Benke, PhD from Monash University Victoria. The surface contamination and dose rate levels were measured on the ground floor and first floor of the TV News Building. The measurements included all staff workstations, studios, control rooms, staff amenities areas, reception, equipment rooms and corridors. These measurements were compared with background measurements taken outside the building. In addition to the recommended dose rate measurements, TLD personal monitors were issued to five staff members from each floor for a two month wearing period. The decision to relocate staff from the TV News Building occurred a few days after the monitors were issued. Our advice was that the personal monitors be placed at the workstation locations of the ten staff members for the remainder of the exposure period. The personal monitors measured the accumulated dose for the exposure period. The purpose of these measurements was to explore the possibility of any unknown source of exposure that might not have been present when the onsite survey was carried out. The control TLD used for background subtraction was held at the Toowong site but in another building not associated with the breast cancer cluster. The air-conditioner inlet filters were monitored for a buildup of radioactivity from airborne contamination that may have accumulated over time. Access to the filters was provided by the site engineers. These measurements were made by use of the contamination monitor. Average radon concentrations were measured over a two month exposure period by use of the PRMS radon area monitors. Five monitors were issued. Three of the monitors were placed on the ground floor and two were placed on the first floor. When occupied, the TV News Building was in twenty-four hour use. Significant variations in radon level can occur due to diurnal effects, ventilation air exchange rates and changes in atmospheric condition. The two month exposure period was expected to give a more meaningful result than a one off real time measurement taken at the time of the onsite inspection. The TLD disk in each radon monitor was used to assess the natural background levels in the TV News Building. The TLD disk was sandwiched between foam pads underneath the CR-39 plaque. The foam held the TLD disk in place and the configuration minimised the influence of radon daughter on the reported dose. Results The search for alpha, beta and gamma contamination was negative. The contamination monitor remained within its normal 2 to 6 c/s count rate range at all times. There was neither surface contamination nor radioactive objects found in the TV News Building. Radioactive accumulation was not found on the air conditioning inlet filters of the building. The dose rate measurements were comparable with normal background radiation levels found in Australia. Dose rates within the 0.05 uSv/h to 0.12 uSv/h range were found, most of which were at the lower end of this range.

Breast Cancer at the ABC Toowong Queensland - Final Report Page 74 of 75
The TLD personal monitors were not worn by individuals as intended but were left behind when the building was vacated and office furniture and equipment moved. Some of these badges were lost. The one remaining ground floor monitor and one of the first floor monitors showed no increase in dose above that of the background in the building where the control monitor was kept. However, the other three first floor monitors showed beta radiation doses of 180 uSv, 280 uSv and 140 uSv for the two month exposure period but no increase in gamma radiation doses. PRMS confirmed these results by remeasuring the redundant areas of the TLD monitors. Two of the three radon monitors from the ground floor were lost when the building was vacated. The remaining monitor from the ground floor and the two from the first floor were assessed by PRMS and the reported radon levels for the two month exposure period were 2.3, 1.3 and 1.3 kBq.day/m3. Using a simple formula provided by PRMS, the average radon concentrations were estimated to be 36.7, 20.6 and 20.6 Bq/m3 respectively. The highest value was from the monitor located on the ground floor. The respective total background gamma doses reported from the TLD disks in the radon monitors were 170, 220 and 170 uGy for the two months exposure. This can be compared to the average background radiation exposure in Australia of approximately 1500 uGy per year. Discussion The search for alpha, beta or gamma contamination by use of the hand held contamination monitor did not reveal any radioactivity levels above that normally found in the local natural environment. It was concluded from the measurements that radioactivity levels were within the normal range of natural background. A similar result was found for gamma dose rate when measured by use of the hand held dose rate monitor. The dose rates found in the building were all within the normal range of natural background. The doses reported from the TLD personal monitors on the first floor were interesting but inconclusive. The purpose of these TLD monitors was to allow for variations in exposure that might not have been observable at the time of inspection. While the monitors did not show an increase in gamma radiation dose compared to the control monitor located in another building there was a slight increase in beta radiation dose for the area of the badge sensitive to beta radiation. Unfortunately, the decision to vacate the building during the exposure period changed the measurement conditions. When the building was vacated the air conditioning system was turned off and the forced airflow ceased. In still air, radon levels can rise and the active decay products of radon, known as radon daughters, can build up and plate out onto surfaces, including the beta sensitive surfaces of the TLD monitors which are open to the air. As the control personal monitor was held in a different building, it didn’t have this problem. If the reported doses were due to radon daughter plate out, as suspected, the results would not be representative of the actual personal doses received by those in the TV News Building. When the air conditioning was turned off following evacuation of the TV News Building, if its natural ventilation was poor, one would expect higher than normal

Breast Cancer at the ABC Toowong Queensland - Final Report Page 75 of 75
radon levels. This means that the radon levels estimated from the radon monitors left for the two month period are probably an overestimate. The radon levels monitored were however not higher than radon levels in many buildings in Australia. It can be concluded that the radon levels were reasonable and that the natural ventilation of the TV News Building was sufficient to maintain acceptable radon levels without forced ventilation. During normal occupancy with the air conditioning operating the radon levels would have been even lower. The radon monitors also contain TLD disks to measure gamma radiation levels and these showed that the annual natural gamma background level on the ground floor was 1020 uGy and on the first floor were 1320 uGy and 1020 uGy. It can be seen from the results that the TV News Building compared favourably with the typical annual gamma background level of approximately 1000 uGy. This result is consistent with that obtained form the Personal Monitors. Conclusions The annual doses to individuals from natural background in Australia are commonly in the range 1000 to 2000 µSv per year. The risk of developing a fatal cancer from exposure to ionizing radiation is estimated by the International Commission on Radiological Protection to be less than one in 20,000 per 1000 µSv dose to the whole body. The highest reported doses for the two month exposure period were 280 µSv for beta radiation and 220 µSv for gamma radiation. It is quite likely that the exposure conditions that gave rise to the beta dose would not apply during times on normal occupancy when the air conditioning is operating. Assuming a 40 hour working week, it can be estimated that the annual dose to someone in the building would be approximately 400 uSv for 2000 hours exposure per year, which is similar to the dose rate from normal background radiation levels in Australia. The annual risk to an individual of developing a fatal cancer (for all types of cancers including breast cancer) from this dose would each be less than one in 50,000. At these low dose levels, breast cancer rates would be negligible and too low to be observable. It must be concluded that the dose rates found in the TV News Building at the time of inspection, were insufficient to be able to explain the observed breast cancer cluster. Acknowledgments: The author wishes to thank D Beel of the ABC Breast Cancer Investigation Panel, P Burns ERH Branch Director, M Cox of the ARPANSA Health Physics Section and N Morris, K Rafferty, T Wright and staff of the ARPANSA PRMS for their valuable assistance in this work.