breast cancer: its more then just pink ribbons … · – ideal for imaging implants, skin,...
TRANSCRIPT

Breast Cancer:
Its More Then Just Pink Ribbons
OAAPN Marla Sustin RN APRNOctober 20th,2017
Marla Sustin RN APRN-BCBreast Cancer Survivorship
Seidman Cancer Center

Objectives
• Review statistics the breast cancer survivorship from the past and compare survival rates for each stage.
• Discuss the newer chemotherapy, immunotherapy, and endocrine therapy regimens including side effects and how to manage them
• Consider the latest data on complete axillary dissection vssentinel node biopsy. Examine onco-plastic surgery and the benefits of a more natural reconstructed breast after mastectomy
• Understand the management of side effects of breast cancer treatment such as depression, anxiety, body image issues, vaginal atrophy and dryness, sexual dysfunction, bone pain, leg cramps, neuropathy.
2

Statistics
• In 2015 there are over 2.8 million women with a history of breast cancer in the U.S. This includes women currently being treated and women who have finished treatment.
• The 5-year survival rate for women diagnosed with cancer is 80%.
• The good news is that women are living longer with breast cancer. Due to better treatment options, breast cancer mortality rates declined by about 25% since 1990.
New York Times, September 10, 2015
Breastcancer.org accessed September 10, 2015
3

Latest Statistics in Breast Cancer Survival 2016
4
• 246,660 new cases of invasive breast cancer (This includes new
cases in survivors but not recurrence).
• 61,000 new cases of in situ breast cancer
– DCIS (non-invasive BC)
– LCIS (increases risk of BC)
• 40,450 breast cancer deaths
Cancer.gov, New health guide.org, Komen.org

Relative Statistics
5
Based on data from SEER 18 2005-2011. Gray figures represent those who have died from female breast cancer. Green figures represent those who have survived 5 years or more.


7
National Cancer Institute



Cancer Survivorship on the Rise!
10

Summary/SEER
Staging Category
Definition
(for all types of cancer)
5-Year Relative
Breast Cancer
Survival*
Localized
Stage 0 & I
The cancer cells have not spread beyond the
organ where they began to grow.
99%
Regionalized
Stage II-III
The cancer cells have spread beyond the
organ where they began (for example to
nearby lymph nodes), but this spread is
limited.
85%
Distant
Stage IV
The cancer cells have spread to other parts of
the body (metastasis).
26%
Dawood S, Broglio K, Valero V, et al. Circulating tumor cells in metastatic breast cancer: from prognostic
stratification to modification of the staging system? Cancer. 113(9):2422-30, 2008
Adapted from 2006-2012 SEER Data

Why do many more women survive?
12

Breast Imaging
13

Advantages
of Digital Mammography
Radiologist:
– Superior contrast resolution and dynamic range
– Post processing allows for enhancement of specific features (window, level, magnify, inversion)
– Ideal for imaging implants, skin, retroglandular fat
– Fewer callbacks
– Telemammography
Patient:
– Lower average dose of radiation
– Speed – no wait time for film to develop
– Wire localizations – compression time shortened limiting total procedure time and patient discomfort

What is Digital Mammography?
Mammogram acquired electronically
without using x-ray film
Digital detectors divided into individual
picture elements (pixels)
Xray photons pass through the breast and
strike each cell/detector
A shade of gray then assigned to each
cell in proportion to the number of
photons counted at that cell
Ultimately results in a gray scale image
displayed on computer monitors
Dietz, J., PP 2016

Southern Illinois Health Care

B

University Hospitals Case Medical Center 18
Digital Mammogram Tomosynthesis

Dense Breast Tissue vs Fat Replaced Breast Tissue

Southern Illinois Healthcare
Breast Density in the U.S.
10% of women have almost entirely fatty breasts.
40% of women have scattered areas of fibro glandular
density
50% of women have either heterogeneously dense or
extremely dense breast tissue

Breast Density Law in Ohio
• Ohio Resident Anne Gates lost her sister
Chris Nestor to breast cancer January 23,
2013.
• Her sister’s cancer was “invisible” on
mammogram
• Anne Gates lead the cause in Ohio to pass
a breast density law

Image courtesy of ITN January 2017

Breast Density Legislation
In Ohio Bill S.B. No. 54
• ”A physician interpreting a mammogram shall determine based on the breast imaging reporting and data system established by the American college of radiology whether the patient has dense breast tissue. If so, the physician shall include the following in the report or summary sent to the patient pursuant to 21 C.F.R. 15900.12:”

OHIO BREAST DENSITY LAW:
signed by governor Kasich 12-22-2014.
“Your mammogram demonstrates that you have dense breast tissue, which could hide abnormalities. Dense breast tissue, in and of itself, is a relatively common condition. Therefore, this information is not provided to cause undue concern; rather, it is to raise your awareness and promote discussion with your health care provider regarding the presence of dense breast tissue in addition to other risk factors."

Update on Chemotherapy
25

In the old days…..
26
NSABP
Protocol B-13 (Schema 1)
To determine whether tamoxifen is more effective
than no treatment
In 1987, added Protocol B-14 (Schema 2) to
evaluate the effectiveness of tamoxifen for 10
years; specifically, to determine whether an
additional 5 years of tamoxifen therapy is
effective in prolonging disease-free survival and
survival in patients with negative nodes and
estrogen-receptor-positive tumors. Patients who
complete the initially assigned 5 years of
tamoxifen therapy were re-randomized to 5
additional years of either tamoxifen or placebo.
NSABP.pitt.edu/B-14.asp

Early Breast Cancer Trialists’ Collaborative Group
(EBCTCG)
Relevance of breast cancer hormone receptors and other factors to the efficacy of
adjuvant tamoxifen: patient-level meta-analysis of randomised trials.
27
2011 Aug 27;378(9793):771-84. doi: 10.1016/S0140-6736(11)60993-8. Epub 2011 Jul 28

Paloma1 CT
28

Paloma3 CT
• PALOMA-3 is a randomized (2:1), multi-center, double-blind Phase
3 study that evaluates palbociclib in combination with fulvestrant
versus fulvestrant plus placebo in women with HR+, HER2-
metastatic breast cancer whose disease has progressed after prior
endocrine therapy.
• Primary endpoint: investigator-assessed progression-free survival†
• Secondary endpoints: objective response (OR),‡ clinical benefit
response (CBR),§ duration of response (DOR), overall survival
(OS), and safety and tolerability2
29

Administration/Side effects Ibrance
For post-menopausal women with metastatic ER/PR+ HER2 - BC
Dosing: 125mg PO on days 1-21 of 28-day cycle.
– CBCw/diff at baseline, Q 2 weeks x6 weeks, then prior to each
cycle.
– Contraindication: Hypersensitivity, ANC < 1000, Caution if
thrombosis risk
Common reactions: Neutropenia, leukopenia, anemia,
alopecia, fatigue, stomatitis, thrombocytopenia, URI, N/V/D,
peripheral neuropathy, asthenia, epistaxis, infection, PE
Severe reactions: anaphylaxis, nephrotoxicity,
myelosuppressoion, ototoxicity, peripheral neuropathy, severe
N/V, vision loss
30
Epocrates.com

CALGB 40603 (Alliance)
• One third of patients with triple-negative breast cancer (TNBC)
achieve pathologic complete response (pCR) with standard
neoadjuvant chemotherapy (NACT). CALGB 40603 (Alliance), a 2
× 2 factorial, open-label, randomized phase II trial, evaluated the
impact of adding carboplatin and/or bevacizumab.
31

Schema of randomized phase II CALGB (Cancer and Leukemia Group B) 40603 trial. ddAC,
dose-dense doxorubicin plus cyclophosphamide.
William M. Sikov et al. JCO 2015;33:13-21
©2015 by American Society of Clinical Oncology

(A) Pathologic complete response (pCR) breast (ypT0/is); (B) pCR breast/axilla (ypT0/is N0);
95% CIs shown in parentheses.
William M. Sikov et al. JCO 2015;33:13-21
©2015 by American Society of Clinical Oncology

Carboplatin administration/side effects• Dosing:
– Institutions protocol: Seidman - Carbo AUC 6 IVPB w/ filigrastim or peg-filgrastim.Creatanine at baseline, frequent CBC, CMP
HOLD: ANC >or = to 1500, PLTS > or = 100,000, grade III peripheral neuropathy.
• Contraindications:
Thrombocytopenia, anemia, leukopenia, nausea, vominting,
hypomagnesemia, hyponatremia, hypokalemia, hypocalcemia,
elevated alk phos, elevated LFTs, BUN/Cr elevation….
• Common reactions: Hypersensitivity to drug/class, mannitol,
cisplatin, platinum, compounds, myelosuppression, active bleeding,
renal impairtments…
• Serious reactions: anaphylaxis, nephrotoxicity, myelosuppression, ototoxicity, peripheral neuropathy, severe N/V, vision loss, severe hypokalemia, hponatremia, hypocalcemia
34

Adverse Events CALGB 40603
35
Sikov, W.M. J Clin Oncol 32. © 2014 by American Society of Clinical Oncology

Chemotherapy and Targeted Therapies
Neoadjuvant Chemotherapy
36

Clinical Rationale for neo-adjuvant Chemotherapy
• Regimens should be the same as those established
as safe and active in the adjuvant setting
• No survival advantage
• A variety of clinical, imaging, and pathologic
measurements are available to gauge tumor
response
• clear correlation between tumor response in the breast and lymph
nodes and both disease-free and overall survival. Pathologic
complete
• response and other pathologic measures may be useful as
surrogate end points in evaluating and understanding new
therapies.
• preoperative systemic therapy is effective and can improve breast
conservation rates as a result of tumor response to therapy
37

Imaging before and after
Neoadjuvant Chemoptherapy
38
PRE POST

Primary systemic
therapy
Conventional
therapy
(Mastectomy)
Local
therapy
(Lumpectomy)
Neoadjuvant Hormonal Therapy
(4 months)
Dietz, Jill MD

Survival after Neoadjuvant Chemotherapy
40
0%
20%
40%
60%
80%
100%
NSABP-18 Royal
Marsden
EORTC
10902
Neoadj OS
Postop OS
Neoadj DFS
Postop DFS
Outcome
neoadjuvant
group =
outcome of
adjuvant
group

Individualized Treatment
• Neoadjuvant Chemotherapy
• Immune Therapies
• Targeted Therapies (Her-2)
• Studies
41
CHRISTUS Stehlin Foundation for Cancer Research

Immunotherapy & Targeted Therapy
• https://www.youtube.com/watch?v=5AXApBbj1ps&sns=em
42

Immunotherapy
• There are several types of immunotherapy, including:
• Monoclonal antibodies
• Non-specific immunotherapies
• Oncolytic virus therapy
• T-cell therapy
• Cancer vaccines
43

Check Point Inhibitors
• Ipilimumab (Yervoy)
• Nivolumab (Opdivo)
• Pembrolizumab (Keytruda)
• Atezolizumab (Tecentriq)
• Avelumab (Bavencio)
• Durvalumab (Imfinzi)
44

Toxicities• Pneumonitis – 4% (any grade) *more in lung patients then solid
tumor
• Rash or dermatitis (up to 15%)
• Diarrhea or colitis (up to 20%)
• Endocrinopathies, especially hypothyroidism (10% or more)
• Between 1% and 5% of patients each experience grade 3/4
hepatitis and grade 3/4 nephritis.
Rare toxicities:
• neuromuscular toxicity (eg, peripheral neuropathy, Guillain-Barre
syndrome), ocular toxicity (uveitis), pancreatitis, myocardial fibrosis,
polymyositis, or autoimmune hematologic toxicity.
45

Toxicity Management
• Steroids!!!
• High doses and then tapering them over a month. Certainly, if the
toxicity is severe, grade 3 or grade 4, the patient needs to be
admitted for intravenous (IV) steroid use. Then the steroids can be
tapered, over at least a month.”
• Generally, for grade 3 or 4 toxicity, we will discontinue the
immunotherapy. There is no dose reduction. You discontinue the
drug and then you treat the toxicity”
• Once the symptoms are under control, patients who had grade 2
toxicity that has improved to grade 1 or entirely resolved and
patients who had grade 3 or 4 endocrine or dermatologic toxicity
can often restart immunotherapy
46

Pembrolizumab in Patients With Advanced Triple-Negative Breast
Cancer: Phase Ib KEYNOTE-012 Study
• •Multicenter, nonrandomized phase Ib trial of single-agent
pembrolizumab given intravenously at 10 mg/kg every 2 weeks to
patients with advanced PD-L1-positive (expression in stroma or ≥
1% of tumor cells by immunohistochemistry) TNBC, gastric cancer,
urothelial cancer, and head and neck cancer.
• •This report focuses on the TNBC cohort.
• •Among 111 patients with TNBC whose tumor samples were
screened for PD-L1 expression, 58.6% had PD-L1-positive tumors.
• •Thirty-two women (median age, 50.5 years; range, 29 to 72 years)
were enrolled and assessed for safety and antitumor activity.
Nanda R et al. KEYNOTE-012 Study. JCO 2016 34:2460-7
Joseph Baar MD 2/17
47

Baseline Characteristics
48

Kaplan-Meier Estimates of (A) Progression-free Survival and (B)
Overall Survival
49
Rita Nanda et al. JCO 2016;34:2460-2467©2016 by American Society of Clinical
Oncology
Median

Pembrolizumab (Keytruda)
Toxicities
Common Serious
Fatigue Immune-mediated rxn
Hyperglycemia Pneumonitis
Anemia Septic Shock
Hyponatremia Colitis
Hypoalbuminemia Hepatitis
Increased LFT’s Pancreatitis
Lymphopenia Diabetes Mellitus Type I
Nausea Diabetic Ketoacidosis
Rash Hypophysitis
Decreased appetite Hypothyroidism
50

Update 2016
• •As of the data cutoff date of April 26, 2016:
• –Median follow-up duration was 10.7 mo (range, 0.4-32.7)
• –Median OS was 10.2 mo (95% CI, 5.3-17.5)
• –2-mo OS rate was 41.1%
• •Median PFS was 1.9 mo (95% CI, 1.3-4.3) and 12-mo PFS rate was 15.0%.
• •Of the 5 responders (including 1 complete response [CR] and 4 partial responses
[PR]): 3 have had long-lasting benefit from pembrolizumab.
• –CR (1): discontinued study medication 11 mo after achieving CR and has remained
in CR for approximately 15 mo without receiving any additional anticancer
treatment.
• –PR (2) discontinued pembrolizumabafter completing 2 yr of treatment.
• •First pt has maintained response for 22.7 mo
• •Second pt had disease progression after 7.7 mo of response and restarted
pembrolizumab.
• •Median duration of response has not been reached (range, 15-58+ wk
51

Conclusion
• Preliminary evidence of clinical activity and a potentially acceptable
safety profile of pembrolizumab given every 2 weeks to patients
with heavily pretreated, advanced TNBC.
52
Diagram Freetobreath.org

Chemo-Immunotherapy?
Hypothesis
• 1.The immune system needs tumor antigen to generate a broad
anti-tumor T cell response
• 2.Chemotherapy helps the immune system by
• a)Killing tumor cells to provide a source of such antigen
• b)Suppressing the suppressors
• 3.Further amplifying anti-tumor immunity by interfering with
immunosuppressive pathways (PD-1/PD-L1) is a good thing
53

OT2-01-10: Pilot Study of Carboplatin, Nab-Paclitaxel and
Pembrolizumab for mTNBC (CASE 6115)
DAY 1 8 15 22 29 36 43 50 57
C X X X
N X X X X X X X X X
P X X X
54
C, Carboplatin, AUC 6 IV day 1 of 21-day
cycle
N, Nab-paclitaxel, 100mg/m2IV days 1, 8
and 15 of 21-day cycle
P, Pembrolizumab, 200 mg IV every 3 weeks

Aims
• Aim 1. Determine overall response rate (RR) in patients treated
with CNP
• •Aim 2. Determine progression-free survival (PFS) in patients
treated with CNP
• •Aim 3. Identify pathologic and genomic correlates of response to
CNP
55

Other Ongoing Metastatic Trials
OT2
• OT2-01-17. A Phase II randomized trial of pembrolizumabwith
carboplatinand gemcitabinefor treatment of patients with metastatic
triple-negative breast cancer (mTNBC). Obeid E, et al.
• OT2-01-03. Phase II trial of the addition of pembrolizumabto
letrozoleand palbociclibin patients with metastatic estrogen
receptor positive breast cancer who have stable disease on
letrozoleand palbociclib. Yuan Y, et al.
56

Targeted Therapy“is a cancer treatment that uses drugs.
It is different from traditional chemotherapy. The drugs known as targeted therapy help stop cancer from growing and spreading. They work by targeting specific genes or proteins”
Cancer.net
57

58

Herceptin/Perjeta
59

HERCEPTIN (trastuzumab)
• Patients with early breast cancer should be treated for 1 year or until
disease recurrence . 6mg/kg IV Q 3 weeks
• Serious Reactions Common Reactions
– Ventricular dysfunction (severe or fatal) Infusion Rx
– Cardiomyopathy Pain
– CHF Asthenia
– Thromboembolism Fever/Rigors
– Infusion reaction (severe or fatal) Nausea/Vomiting
– Dyspnea Diarrhea
Headache/Fatigue/Cough/Dyspnea
**Echocardiogram required prior to start, monitored routinely during treatment
Dose may differ at initiation of treatment, if tx is for metastatic disease, or if used
in combination with other drugs.**
60

Perjeta (pertuzamab)
• Perjeta (chemical name: pertuzumab) is approved by the U.S. Food
and Drug Administration (FDA) to be used in combination with
Herceptin (chemical name: trastuzumab), another targeted therapy
medicine, and Taxotere (chemical name: docetaxel), a type of
chemotherapy, to treat HER2-positive, metastatic breast cancer
that hasn’t been treated with either Herceptin or chemotherapy yet.
(Perjeta was called Omnitarg in earlier studies.)
• Perjeta also has accelerated FDA approval to be used in
combination with Herceptin and Taxotere before surgery to treat
HER2-positive, early-stage (the cancer must be larger than 2 cm or
cancer must be in the lymph nodes), inflammatory, or locally
advanced-stage breast cancer with a high risk of metastasizing or
becoming fatal. Breast cancer. org
61

Perjeta Side Effects
• Dose: 840MG IVx1 of 21 day cycle then 420mg Q3-6cycles
• Serious Side effects: Common Side Effects:
– Cardiac failure Diarrhea
– Cardiomyopathy Alopecia
– Left ventricular dysfxn Neutropenia
– CHF N&V
– Infusion rxn Fatigue
– Hypersensitivity rxn Rash
– Anaphylaxis Anorexia
– Anemia Mucositis
– Leukopenia/neutropenia Anemia
– Febrile neutropenia Headache, Fever,Stomatitis
62

Cleopatra Trial
63
Cleopatra Study
• The large phase II trial assessed the safety profile during which either
pertuzumab or placebo was added to docetaxel and trastuzumab for
first-line treatment of HER2-positive metastatic breast cancer.
• Toxicity profiles between the pertuzumab and placebo group were
similar for grade 1 and 2 adverse events including diarrhea (46.3 vs.
66.8%), alopecia (60.5 vs. 60.9%), neutropenia (49.6 vs. 52.8%),
nausea (41.6 vs. 42.3%), and fatigue (36.8 vs. 37.6%). For grade 3 or
higher adverse events, neutropenia was the most common (45.8 vs.
48.9%), followed by febrile neutropenia (7.6 vs. 13.8%), leukopenia
(14.6 vs. 12.3%), and diarrhea (5.0 vs. 7.9%).
• Deaths related to adverse effects of the treatment were 2.5% for the
control group and 2.0% for the pertuzumab groups, with infection cited
as the primary cause.29
64

Add pertuzamab to trastuzumab
• For HER2 + BC
– Originally FDA in June 2012 for use in combination with trastuzumab
and docetaxel for the treatment of patients with HER2-positive
metastatic breast cancer without prior treatment with anti-HER2 therapy
for metastatic disease.
– 2013, pertuzumab was expeditiously approved by the FDA for
neoadjuvant therapy in HER2-positive patients with locally advanced,
inflammatory, or early stage breast cancer. In this clinical scenario,
pertuzumab is administered with trastuzumab and docetaxel with data
indicating an improved pathologic complete response (pCR) when
compared to trastuzumab and docetaxel alone
65
Maley, J.J. & Macrae, E.R. (2014)Pertuzumab in Combination with Trastuzumab and Chemotherapy in the Treatment of HER2-Positive
Metastatic Breast Cancer: Safety, Efficacy, and Progression Free Survival. Breast Cancer (Auckl). 2014; 8: 81–88.

Cleopatra Study
66

Identification of Multigene panel
67
• Viable option to assess risk for
women at increased risk to
develop BC
2013 Supreme court decision –
NO to Myriad genetics patent
Covers over 100 genese, 21
specifically for breast cancer
Easton, D.F. et al. N Engl J Med 2015; 372:2243-2257. 2015

Hormonal Therapy
• Tamoxifen/Evista (tamoxifen 20mg daily) (Evista 60mg daily)
– Pre or Post-menopausal women
– Evista only in DCIS
– Bone and heart protective
Common Side effects Serous Side effects
Hot flashes Thromboembolism
N/V Stroke
Vaginal discharge Endometrial Cancer
Menstrual irregularities Endometrial Hyperplasia
Vaginal bleeding Endometriosis
Disease flare, transient Uterine Sarcoma
Lightheadedness Uterine Fibroids
Dizziness Ovarian Cysts
Peripheral edema Erythema multiforme
Fatigue Thrombocytopenia
Headache Leukopenia/neutropenia
68

Aromatase Inhbitors
• Arimidex (anastrozole) 1mg daily
• Aromasin (exemestane) 25mg daily
• Femara (letrozole) 2.5mg daily
– For post-menopausal women only (natural or artificial)
– Must monitor bone density
– Consider bone health prior to initiating treatment
Common S/E Serious SHot flashes FracturesAsthenia OsteoporosisPain Endometrial CAArthralgias ThromboembolismArthritis MIN/V Stroke
Headaches Angina
Depression HTN
Rash Cataracts
69

ER+ disease, 5 yrs v 0, and 10yrs v 5 Breast cancer death rate ratio (rr)
70

ER+ disease, 5 yrs v 0, and 10yrs v 5 Breast cancer death rate ratio (rr)
71

ER+ disease, 5 yrs v 0, and 10yrs v 5 Breast cancer death rate ratio (rr)
72

73

Conclusion: ATLAS TRIAL
• 10 vs. 5 years of tamoxifen improves DFS and OS in ER+ invasive breast cancer
• Increased side effects were modest
• Benefit vs. other switching strategies with aromatase inhibitors for postmenopausal women is unknown
74

75

MA17 Trial :Menopause Status at Primary Diagnosis
76
Silverman, Paula MD, May 2015
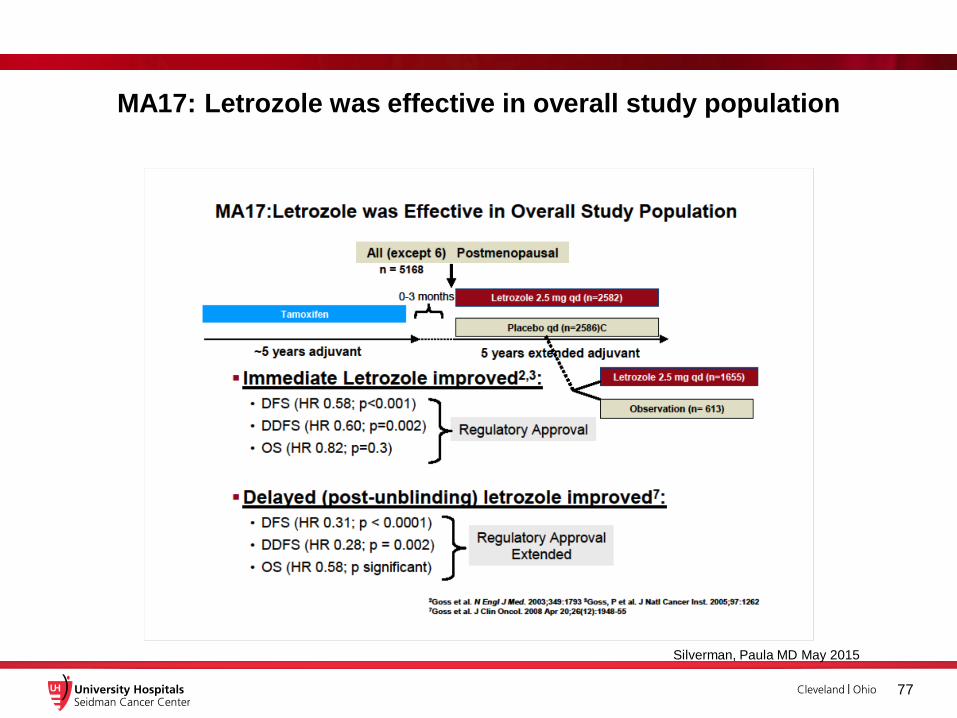
MA17: Letrozole was effective in overall study population
77
Silverman, Paula MD May 2015

Among untreated (placebo) women, pre-menoapausal had Greater
Disease Recurrence
78
Silverman,Paula, May 2015

Premenopausal women had a greater benefit from treatment
79

Intergroup Exemestane Study
Tamoxifen2-3 years Exemestane
2-3 years
Tamoxifen2-3 years
Post-menopausal women with ER +/unknown breast cancer
June 2009 dataset = 91 month F/U from randomization
Total 5 years endocrine therapy
Post Treatment Follow up
80
Randomize

Patient Characteristics
• 4724 postmenopausal women recruited between1998
and 2003
• 44% node positive, 33% received adjuvant
chemotherapy
• Mean age at randomization 64
• ER positive 86%,ER unknown 12%
– Excluded 3% ER negative
• N=4599; all analyses relate to the ER positive/unknown
population
81

International Exemestane Study Results
• Overall Survival
– Absolute difference at 8 years 2.5% favoring
exemestane
– HR 0.86 (95%CI: 0.75-0.99, p=0.04)
• Disease free survival
– Absolute difference at 8 years 4.4% favoring
exemestane
– HR 0.82 (95%CI: 0.73-0.92, p=0.0009)
82

IES results SABCS 2009
Hypothesis generating findings
• Distant recurrences not including bone were the same, but there were more recurrences including bone in the tamoxifen group (147 E vs192 T)
• Exemestane had a lower than expected non-breast second primary cancers
– GI, lung, other improved in addition to expected endometrial
– Total 106 E vs 159 T (could not exclude mets)
83

IES conclusions
• In patients treated with tamoxifen for 2-3 years, switching to exemestane as compared to continuing with tamoxifen out to 5 years results in
– Persistent improvement in breast cancer outcome at 9 years
– Modest but persistent improvement in overall survival
84
Silverman,Paula MD May 2015

85

Randomization
86

87

88

Randomization, Treatment, Follow-up
89
Silverman, Paula MD, May 2015

Conclusions: adjuvant endocrine treatment update
1. Late adjuvant letrozole improve DFS, DDFS and OS
2. Premenopausal women who become menopausal while on tamoxifen should be offered letrozole at completion of treatment or after up to 6 years of observation
3. From International Exemestane Study, patients treated with tamoxifen for 2-3 years, switching to exemestane as compared to continuing with tamoxifen out to 5 years results in improved overall survival and breast cancer outcomes
90

Conclusions: adjuvant endocrine treatment update
5. Ovarian suppression plus tamoxifen did not provide a
significant benefit to the overall study population.
However, in women who remained premenopausal
and received adjuvant chemotherapy, there was
improvement in outcomes
6. In premenopausal women where ovarian suppression is
recommend, exemestane combined with ovarian
suppression reduced recurrence
91

Surgery for Breast Cancer
• Whats new?
– New technology
– Margins
– Latest on Axillary Management
– Oncoplastic Surgery
92

MastectomyBreast
Conservation
Surgery for Breast Cancer

GENETICS
94

Oncoplastic Surgery
95

Trying to avoid this
96

Prevent vs Cause deformity
97

Oncoplastic Surgery
An extension of the multidisciplinary approach to the breast cancer patient
Genetics: If gene + consider contralateral prophylactic
Imaging: MRI if remodeling the whole breast. How far from the nipple? Extent of disease?
Med Onc: Would neoadjuvant chemo or hormonal therapy allow for BCT? Timing of therapy…consider delays with more extensive surgery
Rad Onc: PBI or intraop? Post mastectomy radiation needed? Timing of reconstruction needs to be determined.
Path: How to label and assess margins when rearranging the breast.
Plastics: Flaps, reconstruction of the partial mastectomy defect, contralateral symmetry
98

Batwing Procedure Post-op
99

Batwing procedure: One week post-op
100

Nipple Sparing mastectomy in patients with previous
reduction mammoplasty
101

Pre-operative assessment of skin
reduction and symmetry

De-epithelialize skin (before or after mastectomy)

Nipple Sparing Mastectomy
104
Make inferior incision
on superior border of
lower flap

Nipple Sparing Mastectomy Complete
105

Complete skin reduction closure
106

Two months post-op
107

108
Halestead Mastectomy
Nipple Sparing Mastectomy

Sentinel Node Biopsy vs. Complete Axillary Dissection
• Sentinel node biopsy is a surgical procedure used to determine if
cancer has spread beyond a primary tumor into your lymphatic
system. Sentinel node biopsy is used most commonly in
evaluating breast cancer and melanoma. The sentinel nodes are
the first few lymph nodes into which a tumor drains.
• An axillary lymph node dissection (ALND) is surgery to remove
lymph nodes from the armpit (underarm or axilla). The lymph
nodes in the armpit are called axillary lymph nodes. An ALND is
also called axillary dissection, axillary node dissection or
axillary lymphadenectomy.
109

Complete Axillary Dissection
110
Common post-surgery
effects:
Parasthesia – 53%
Lymphedema – 3.5%
Limited arm abductions –
24%
Pain – 27%
Emerson, et al. World Journal of Surgical
Oncology201412:67

Sentinel Node Biopsy
• A sentinel lymph node is the first lymph node to receive lymphatic drainage
from a tumor. It can be detected by injection of a blue dye or radioactive
colloid (Technetium 99m sulfur colloid (Tc99m) around the nipple, which
travels to and identifies the first draining (sentinel) node. Biopsy of a
sentinel lymph node can reveal whether there are lymphatic metastases,
thereby eliminating the need for extensive dissection of the regional lymph-
node basin.
111
Aboutcancer.com

112

The New Normal
113
What is it?
Sadness
Stress
Fear of recurrence
Will life every be the same?
Permanent scars
Emotional scares
Unable to go back to usual
activities
Fear of the unknown

114
Personal Quote
"I'm so exhausted from dealing with all
the emotional ups and downs with my
disease. I'm wondering how much of this
overtiredness is not physical at all. And if
I'll ever feel stronger. I barely sleep since
I've been home from my surgery. I'm tired,
but never tired enough to just sleep
soundly."
— Shawna

115
Exercise - may be the only cure for
fatigue! Do it together, encourage!!
America College of Sports Medicine –
150 minutes of exercise/week . Build
up slowly.
Yoga, tai chi
Walking
Join a class
Swim
Gift of personal trainer

Memory/Concentration
• Chemo brain” – not the entire picture!
Theories:
• Stress has been found to be a cause of memory loss
➢ Too much energy in one area such as coping with cancer
diagnosis can cause lack of energy in other areas
• Not much time from diagnosis to treatments to emotionally
prepare
• Physiological changes – release of stress hormone
cortisol. Excessive stress hormone levels can make it difficult
to think or retrieve long-term memories.
116
Stress, Coping and Cognitive Deficits in Women After Surgery for Breast Cancer.
Published online January 10, 2012, in the Journal for Clinical Psychology in Medical
Settings. First author: Stephanie Reid-Arndt, PhD, ABPP, University of Missouri,
Columbia, Mo. Assessed 9/22/15 from Breast Cancer.org

Emotional Change/Fear of Recurrence
• Damocles syndrome.” According to Greek legend, once Damocles realized that a
sword was dangling precariously over his head, he could no longer enjoy the
banquet spread in front of him. In the same way, the specter of cancer hangs over
some cancer survivors. They can become emotionally paralyzed and have a hard
time deciding to get married, change jobs, or make other major decisions.
• Fear of Recurrence – follow up visits, unexplained pain, sights sounds that are
reminders trigger the fear of recurrence leading to anxiety, emotions
• Post-traumatic stress - recognize triggers; office visits, other survivors
• Survivorship guilt – “Why me” “Why not me”
Recognize and understand these emotions!
• McDonald, Ann:The mental and emotional challenges of surviving breast
cancer . POSTED March 28, 2011. 5:03 PM Updated March 29,2011
9:27AM
117

Emotions: Pain, Anger, Loneliness
118
PainSkin sensitivity where you received
radiation
Painful scars from cancer surgery.
Pain in a missing limb or breast.
Pain in breast from surgery
Pain or numbness in the hands and
feet due to injured nerves
Vaginal pain/discomfort
How we can help:
Recognize the pain as real!!
Advocate for your partner
Pain medications Hypnosis, meditation, yoga
Anti-depressants Relaxation skills
Physical Therapy Acupuncture

Emotions: Pain, Anger, Loneliness
“Anger is nothing more than a cover for hurt, frustration or fear or all three”
- Phil McGraw
• “I was healthy; I did everything right. I exercised, ate right, went for my
mammograms every year and I still got cancer.” - my anonymous patient
• I am angry that I am alive and my friend is not
• I am angry that I have to live with pain
• I feel angry at the friends and family that abandoned me during treatment
• I am angry that I had to quite my job
• I get angry when people complain about minor things because I had to face my
mortality
• I feel grateful to be alive but I am still angry
!After Breast Cancer Treatment, Breast Cancer and Mental Health, depression and breast cancer. Denise4health.December
9, 2013
119

• “There is no greater agony than bearing an untold
story inside you.” - Maya Angelou
• Loneliness
– Loneliness in recognizing mortality
– Loneliness in symptom burden
– Changed sense of identity and connection with others
– Altered threshold for distress (coping)
120
Mary Rosedale, PhD, APRN-BC, NEA-BC: Survivor Loneliness of Women
Following Breast Cancer. Oncology Nursing Forum • Vol. 36 No2 March 2009 183

Lymphdedema
• Build up of lymph fluid under fatty tissues under skin
• Interruption of the lymph nodes and lymph vessels that carry fluid
from distant parts of the body back to the heart.
• Lymph system is part of the immune system, fights of harmful
substances; infection, cancer.
• Surgery can disrupt the lymphatic system causing swelling (breast
surgery, lymph node removal)
121
American Cancer Society:Signs and symptoms of lymphedema. Accessed
9/22/15

122
Natural remedies.org

Sexual Issues/Intimacy
• Chronic or acute illness can affect can disrupt intimate relationships
• Body image issues after surgery/treatment
• Loss of desire
• Chemotherapy, oophorectomy or hormonal therapy can cause
immediate menopause which can lead to physical difficulties with
intimacy
– Vaginal dryness
– Dyspareunia (painful intercourse)
123

Sexual issues and intimacy
• Educate patient and partner:
– Encourage partner to share feelings
– Decrease alcohol, caffeine, chocolate
– Foreplay
– Encourage to discuss treatments with provider:
• Natural lubricants Anti-depressants:
– Olive oil Effexor
– Coconut oil Paxil (Brisdelle)
• Vaginal moisturizers Celexa, Prozac
– Replens Neurontin
• Vaginal lubricants
– KY Jelly– Astroglide– goodcleanlove.com– yesyesyes.co
124

Work and Family Issues
• Family issues:
– Role changes
– Hard for family to come to terms with the cancer diagnosis
– Children or grandchildren may fear cancer means “will die”
– Increased responsibilities while managing emotions and trying to
be sensitive to the needs of the family member with cancer
– Communication from all family members is key
– Talk with someone who has had a relative diagnosed with cancer
– Seek out community resources
• The Gathering Place (Cleveland)
• Stewarts Caring Place (Akron
125

Weight and Eating Habits
• Weight gain is common during/after cancer treatment. If received
chemotherapy were 65% more likely to gain weight then women who
did not have chemotherapy.
• Average weight gain is 5-15 pounds
• Weight gain is enhanced if patient goes through menopause
• Reasons – change in metabolism, decreased activity
• Only way to increase metabolism is through exercise
Saquib N, Flatt SW, Natarajan L, et al. Weight gain and recovery of pre-cancer weight after breast cancer treatments: evidence from the women's healthy eating and living (WHEL) study. Breast Cancer Res Treat. 105(2):177-86, 2007. - See more at: http://ww5.komen.org/BreastCancer/Treatment_References.html#sthash.vrd5hNfv.dpuf
Stan D, Hershman D, Loprinzi CL. Chapter 51: Management of menopausal symptoms in breast cancer survivors, in Harris JR, Lippman ME, Morrow M, Osborne CK. Diseases of the Breast, 5th edition. Lippincott Williams and Wilkins, 2014.
126

Weight and Eating Habits
• How we can help - educate:
– One area where partners can have most impact!
– Do the shopping, prepare the meals
• Encourage:
– 3 meals a day
– Avoid snacks
– Use healthy fat (olive oil, coconut oil, nuts, natural nut
butters, avocados
– Limit refined carbs (white stuff – pasta, white rice,
cookies, cake, ice cream)
– Half the plate should be vegetables
– Avoid other activities while eating – turn off tv!Komen.org. assessed September 21, 2015
127

Bone Pain
• Joint pain (arthralgia) and muscle pain (myalgia) are common side effects
of aromatase inhibitors. The pain may be in the hands and wrists, feet and
ankles, knees, back or other parts of the body.
• Up to 36 percent of women in clinical trials of aromatase inhibitors have
reported joint pain and up to 15 percent have reported muscle pain. Other
studies have found even higher rates of these side effects.
• Joint and muscle pain can mimic carpal tunnel syndrome. And, in rare
cases, aromatase inhibitors can cause carpal tunnel syndrome.
• Although aromatase inhibitors can cause joint and muscle pain, they don’t
cause permanent joint or muscle damage.
128

Bone pain treatment/Leg Cramps
• NSAIDS Magnesium 500mg
• Acupuncture Banana
• Exercise hydrate
• Tumeric (1,500mg/day – though dose varies by type used)
• Cortisone injection
• Livestrong.com updated 10.3.2017
129

Neuropathy
Chemotherapy. Specific types of chemotherapy can injure peripheral
nerves, particularly high-dose chemotherapy. These include:
• Bortezomib (Velcade)
• Platinums, including cisplatin (Platinol), oxaliplatin (Eloxatin), and
carboplatin (Paraplatin)
• Taxanes, including docetaxel (Docefrez, Taxotere) and paclitaxel
(Taxol)
• Thalidomide (Synovir, Thalomid)
• Vinca alkaloids, including vincristine (Vincasar), vinorelbine
(Navelbine), and vinblastine (Velban)
130
Cancer.net

Neuropathy Treatment
• Pain relievers (OTC, though may need opioids; tramadol, oxycontin,
used only if other treatments have failed.
• Anti-seizure medications Lyrica (pregabelin), Neurontin (gabapentin)
• Topical treatments - Capsaicin cream (may have burning sensation at
first. Theory is the heat deadens the nerves
• Lidocaine patch
• Antidepressants – amitriptyline,nortryptiline, cymbalta, effexor
• Transcutaneous electrical nerve stimulation (TENS)
• Physical therapy
• GLA (gamma linolenic acid) ALA (Alpha Lipoic Acid), Vitamin B1 & B6
• Amino Acids - acetyl-L-carnitine
131
Mayoclinc.org

Favorite Quote
"The most beautiful people we have known are those who have known defeat, known suffering, known struggle, known loss, and have found their "The most beautiful people we have known are those who have known defeat, known suffering, known struggle, known loss,
ant"The most beautiful people we have known are those who have
known defeat, known suffering, known struggle, known loss, and
have found their way out of the depths. These persons have an
appreciation, a sensitivity, and an understanding of life that fills
them with compassion, gentleness, and a deep loving concern.
Beautiful people do not just happen."
- Elizabeth Kubler Ross
hem with compassion, gentleness, and a deep loving concern. Beautiful people dThe most beautiful people we have known are those
who have known defeat, known suffering, known struggle, known loss, and have found their way out of the depths. These persons have an appreciation, a sensitivity, and an understanding of life that fills them with compassion, gentleness, and a deep loving concern.
Beautiful people do not just happen."
132

Thank- you!!!!
Pink ribbon
The pink ribbon is an international symbol
of breast cancer awareness. Pink ribbons,
and the color pink in general, identify the
wearer or promoter with the breast cancer
brand and express moral support for
women with breast cancero not just happen."
- appreciation, a sensitivity, and an understanding of life that fills them with compassion, gentleness, and a
deep loving concern. Beautiful people do not just happen."
- Ross
133