breast cancer quality performance indicators
TRANSCRIPT

Information Services Division
An Official Statistics publication for Scotland
Breast Cancer Quality Performance Indicators
Patients diagnosed between January 2015 and December 2017
Publication date
9 April 2019

Information Services Division
2
This is an Official Statistics Publication
The Official Statistics (Scotland) Order 2008 authorises NHS National Services Scotland (the
legal name being the Common Services Agency for the Scottish Health Service) to produce
official statistics.
All official statistics should comply with the UK Statistics Authority’s Code of Practice which
promotes the production and dissemination of official statistics that inform decision making.
They can be formally assessed by the UK Statistics Authority’s regulatory arm for National
Statistics status.
Find out more about the Code of Practice at:
https://www.statisticsauthority.gov.uk/osr/code-of-practice/
Find out more about official statistics at:
https://www.statisticsauthority.gov.uk/national-statistician/producers-of-official-statistics/

Information Services Division
3
Contents
Introduction .............................................................................................................................. 4
Key Points ......................................................................................................................... 7
Results and Commentary ....................................................................................................... 10
Case Ascertainment ........................................................................................................ 10
Overall Performance Summary ....................................................................................... 11
Quality Performance Indicators ....................................................................................... 14
Clinical Trials .................................................................................................................. 40
List of Tables .......................................................................................................................... 43
Contact ................................................................................................................................... 44
Further Information ................................................................................................................ 44
Rate this publication ............................................................................................................... 44
Appendices ............................................................................................................................ 45
Appendix 1 – Background information ................................................................................ 45
Appendix 2 – Breast Cancer QPIs ...................................................................................... 45
Appendix 3 – Breast Cancer Clinical Trials ........................................................................ 48
Appendix 4 – Publication Metadata .................................................................................... 49
Appendix 5 – Early access details ...................................................................................... 51
Appendix 6 – ISD and Official Statistics ............................................................................. 52

Information Services Division
4
Introduction
The cancer strategy ‘Beating Cancer: Ambition and Action’ published in March 2016
builds on the commitment made in the Better Cancer Care plan to 'develop a work
programme which will define how we will take forward… quality indicators for cancer services'
by further supporting a culture of continuous quality improvement in cancer care across
NHSScotland. The new cancer strategy states a commitment to improving data collection to
advance the quality and delivery of care for cancer patients.
To achieve this, the Scottish Cancer Taskforce established the National Cancer Quality
Steering Group (NCQSG), which includes responsibility for:
▪ The development of small sets (approximately 10-15 indicators) of tumour specific national quality performance indicators (QPIs) as a proxy measure of quality care.
▪ Overseeing the implementation of the national governance framework that underpins the reporting of performance against these national QPIs.
The QPIs have been developed collaboratively with the three Regional Cancer Networks:
North Cancer Alliance (NCA), South East Scotland Cancer Network (SCAN), West of
Scotland Cancer Network (WoSCAN), Information Services Division (ISD), and Healthcare
Improvement Scotland. The QPIs are published on the Healthcare Improvement Scotland
website.
These indicators, used to drive quality improvement in cancer care across NHSScotland are
kept under regular review; NHS Boards will be required to report against QPIs as part of a
mandatory national cancer quality programme.
ISD support NHS Boards in improving the quality of local data collection and reporting
through the production of data validation specifications, and measurability criteria for QPIs.
The current data sets are outlined on the Cancer Audit website.
A rolling programme of reporting is planned across many tumour sites. National reports will
include comparative reporting of performance against QPIs at NHS Board level across NHS
Scotland, trend analysis and survival analysis (where applicable). This approach will help
overcome existing issues relating to the reporting of small volumes in any one year.
This report assesses performance against 13 Breast Cancer QPIs using clinical audit data
relating to patients diagnosed with breast cancer for the period from January 2015 to
December 2017. An initial report on the first year of data collection (2012) was previously
published in April 2014 and the commentary included in that report may still be applicable
when interpreting this report.

Information Services Division
5
Data collection and analysis
Breast cancer QPI data for patients diagnosed between January 2014 and December 2017
were collected by NHS Boards, supported by the regional cancer networks, and then
analysed against the Breast cancer measurability document. Aggregated analysed data
were then submitted to ISD via a data collection template for collation to allow comparisons
at NHS Board level.
Data quality and completeness
Small numbers:
Where the number of cases meeting the denominator criteria for any indicator is between one
and four, the percentage calculation has not been shown on any associated charts or tables.
This is to avoid any unwarranted variation associated with small numbers and to minimise the
risk of disclosure. Any charts or tables impacted by this are denoted with a dash (-).
However, any commentary provided by NHS Boards relating to the impacted indicators will
be included as a record of continuous improvement.
Baseline Review:
Following baseline review and year 1 publication of breast cancer QPIs data, some changes
were made to measurability in order that the QPIs appropriately measured what they were
intended to. These were positive changes and led to more focussed analysis in year 2.
However, the alterations to measurability mean that year 1 and year 2 results may not be
directly comparable for some QPIs.
Formal Review:
In order to ensure the success of the National Cancer QPIs in driving quality improvement in
cancer care across NHS Scotland it is critical that the QPIs continue to be clinically relevant
and focus on areas which will result in improvements to the quality of patient care.
It was proposed that a formal review of all QPIs should take place following 3 years national
comparative reporting, with tumour specific Regional Clinical Leads undertaking a key role in
determining the need and extent of the review required.

Information Services Division
6
For breast cancer, the initial formal review took place in 2015 and the revised QPIs were
implemented from January 2016. At the formal review, the following QPIs were archived and
are consequently not reported here:
QPI 7 - Negative Axillary Clearance Rate
QPI 12 – Anti HER2 Positive Therapy
The following new QPIs were added post formal review:
QPI 13 – Re-excision Rates
QPI 14 – Referral for Genetics Testing
QPI 15 – 30 Day Mortality following Chemotherapy
A second formal review for breast cancer QPIs is currently underway and will report later in
2019.
Survival Analysis:
For future tumour specific survival analyses, it has been agreed to use the Cancer Audit QPI
dataset rather than the Cancer Registry dataset that has been used in the past. This should
provide benefits in terms of improved accuracy and more specific and detailed analysis. Due
to time limitations and availability of data in time for this release, therefore, it has been
agreed to undertake breast cancer survival analysis at a later date. Historic survival analysis
figures using Cancer Registry data are available here for reference

Information Services Division
7
Key Points
• There were 4807 women diagnosed with Breast Cancer in Scotland in 2017. This is
similar to previous years where 4797 were diagnosed in year 2016 and 4853 in 2015.
• At a Scotland level for 2017, the target was met in fourteen of the seventeen indicators
(i.e. including sub parts of some indicators) with three below target. This is an
improvement from previous years where 4 of the indicators did not meet the target.
• For those QPIs where the target was not met across Scotland, reasons and
appropriate actions are provided from the clinical comments in the Quality
Performance Indicators section of this report.
Met or exceeded target
Target not met

Information Services Division
8
Foreword from Breast Cancer Clinical Leads
The three Regional Cancer Networks (North Cancer Alliance (NCA), South East Scotland Cancer Network (SCAN), and West of Scotland Cancer Network (WOSCAN)) aim to promote the highest standards of cancer care and equity of access to cancer services across Scotland. The development and introduction of national Quality Performance Indicators (QPIs) across Scotland represents a major step forward for patients with Breast Cancer. This report provides information on performance against the Breast Cancer QPIs at a national level and across the three Regional Cancer Networks for patients diagnosed in the period 2015 to 2017. Performance against the Breast Cancer QPIs is discussed annually at the National Breast Cancer Trials Group Meeting, most recently held in November 2018. It is clear from the results that delivery of Breast Cancer services across Scotland is of a high standard overall. The development and reporting of QPIs has helped to drive improvement in performance across a number of areas over recent years with considerable improvements in the number of patients having wide excisions and / or axillary sampling procedures undertaken as day case surgery (QPI 8) and the timely provision of HER2 status results to enable treatment decisions to be made in a timely manner (QPI 9). These data have also acted as a catalyst for meaningful debate in a number of areas of clinical practice leading to a reduction in the use of FNA for non-operative diagnosis (QPI 2) or the use of radiotherapy following breast conservation (QPI 10) while the introduction of new QPIs will encourage the development of clinical practice across Scotland, for example genetic testing of certain groups of patients (QPI 14). The geography of Scotland makes the provision of day case surgery challenging in rural areas where patients may have considerable journey times. There have been improvements in performance against this indicator (QPI 8) over the last three years across each of the three cancer networks and NHS Boards are continuing to work on improving the availability of day case surgery in various ways such as through the use of patient hotels, nurse led discharge and anaesthetic pre-assessments. Several areas for improvement have been identified. Delays in the reporting of HER2 status (QPI 9) are largely due to delays in FISH reporting and these delays are exacerbated where samples need to be sent to another centre for testing. While the Molecular Pathology Evaluation Panel (MPEP) provides recommendations about timescales for reporting FISH results these do not align with this QPI definition. As such the breast cancer leads will work with MPEP to raise awareness of the need for timely reporting. The adjuvant chemotherapy target (QPI 11) may not necessarily reflect patient co-morbidities and can be difficult to achieve. The way in which this QPI is measured is being re-considered in light of updated models and new tests for predicting the benefit of chemotherapy following surgery. There are some areas where new information is changing the provision of breast cancer services and this has affected performance against some QPIs. Recent studies provide evidence that not all patients benefit from radiotherapy following breast conservation surgery. As such the use of radiotherapy following surgery has reduced for some patient groups in recent years, resulting in a decrease in performance against QPI 10. This change in practice is supported by clinical evidence and considered to be clinically appropriate; as such the definition of this QPI is likely to be amended for future years of reporting.

Information Services Division
9
The Breast Cancer QPIs are in the process of being reviewed and it is likely that some of the definitions will be updated to address issues like those highlighted above while others may be made more challenging and new QPIs may be introduced. We are confident that implementation of these revised QPIs will drive further quality improvement. Mr Douglas Brown Consultant Breast Surgeon North Cancer Breast Clinical Director Mr James Mansell Consultant Breast Surgeon WOSCAN Clinical Lead for Breast Cancer Mr Glyn Neades Consultant Breast Surgeon
SCAN Clinical Lead for Breast Cancer

Information Services Division
10
Results and Commentary
Case Ascertainment Case ascertainment is a measure of data quality and is calculated by comparing the number
of new patients captured by the cancer audit with a five year average of the numbers
recorded on the cancer registry*. A five year average is used for registry data as the
information is not available until sometime after the year under examination. This is due to
data collection and verification processes. As the number of cases will vary each year, it is
possible for case ascertainment to be over or under 100%. Therefore, the figures presented
should be seen as an indication only.
The average case ascertainment for breast cancer across Scotland in the year to December 2017 was 95.4%.
- Data not shown due to small numbers
*There are differences in the methodology used in the Cancer Registry and Cancer Audit particularly regarding the counting
of patients with multiple primary cancers. In Cancer Registry each primary cancer is counted independently whereas in
Cancer Audit each patient is only counted once.
No. of Audit
Records Diagnosed
in 2015
Average No. of Cancer
Registrations: 2010-
2014
Estimated
Case
Ascertainme
nt %
No. of Audit Records
Diagnosed in 2016
Average No.
of Cancer
Registrations
: 2011-2015
Estimated Case
Ascertainment %
No. of Audit
Records Diagnosed
in 2017
Average No. of Cancer
Registrations: 2012-2016
Estimated Case
Ascertainment %
NoS 1241 1240 100.1 1295 1243 104.1 1240 1274 97.3
Grampian 479 485 98.8 470 481 97.8 484 492 98.5
Highland 294 275 106.8 260 279 93.2 264 281 94.0
Orkney - - 0.0 - 5 0.0 0 - 0.0
Shetland 8 11 70.2 28 12 241.4 10 13 79.4
Tayside 459 463 99.1 535 466 114.8 482 484 99.5
Western Isles 0 - 0.0 0 - 0.0 0 - 0.0
SCAN 1310 1315 99.7 1226 1337 91.7 1282 1317 97.3
Borders 61 71 85.7 72 73 98.1 80 71 112.0
Dumfries & Galloway 108 107 100.7 92 104 88.6 108 98 110.0
Fife 169 188 89.8 180 188 95.8 182 184 99.1
Lothian 972 948 102.5 882 972 90.7 912 964 94.6
WoSCAN 2302 2422 95.0 2276 2454 92.7 2285 2447 93.4
Ayrshire & Arran 377 415 90.9 399 416 96.0 446 417 106.9
Forth Valley 184 186 98.7 168 194 86.6 175 196 89.4
Greater Glasgow & Clyde 1362 1496 91.1 1285 1511 85.1 1207 1482 81.5
Lanarkshire 379 325 116.5 424 334 127.1 457 352 129.9
Scotland 4853 4976 97.5 4797 5034 95.3 4807 5037 95.4
0
50
100
150
200
250
300
Grampian Highland Orkney Shetland Tayside Western Isles
NoS Borders Dumfries & Galloway
Fife Lothian SCAN Ayrshire & Arran
Forth Valley Greater Glasgow &
Clyde
Lanarkshire WoSCAN Scotland
NoS SCAN WoSCAN Scotland
Estimated Case Ascertainment (%)
2015 2016 2017

Information Services Division
11
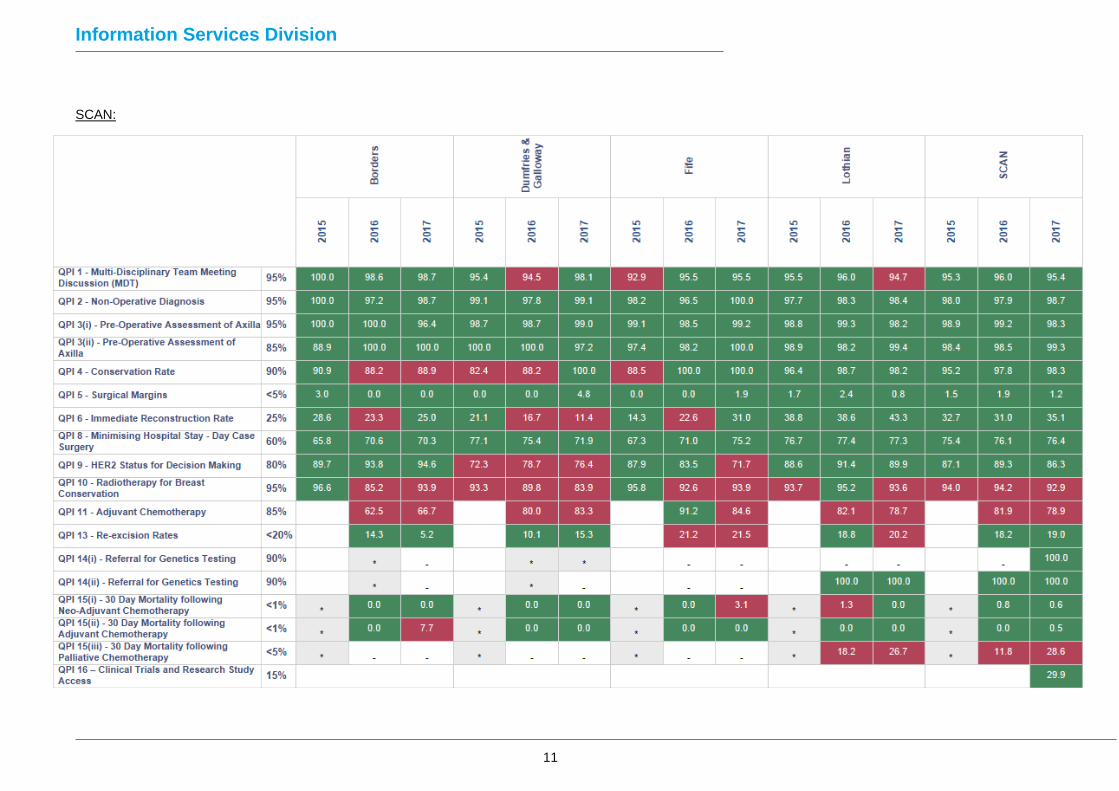
Overall Performance Summary The tables below summarise the overall % performance across the country for each QPI.
NoS:
Information Services Division
11
SCAN:

Information Services Division
12
WoSCAN:
Note: the target for QPI 6 in 2015 was 10%, therefore the colour coding for 2015 is based on this target.

Information Services Division
13
Clinical Trials Summary Table – by Scottish Cancer Research Network (SCRN)
2015
2016
2017
2015
2016
2017
2015
2016
2017
Patients Enrolled - Interventional - > 7.5% 6.2% 7.2% N/A 5.9% 0.0% N/A 4.1% 2.8% N/A
Patients Enrolled - Translational - > 15% 6.2% 8.2% N/A 31.4% 23.0% N/A 0.4% 1.6% N/A
Patients consented for all trials - > 15% N/A N/A 10.0% N/A N/A 29.9% N/A N/A 10.3%
SCRN - West
Breast
Cancer
SCRN - North & East SCRN - South East
N/A – QPI definition not applicable for this reporting period
Target not met
Met or exceeded target

Information Services Division
14
Quality Performance Indicators
The following section includes a detailed summary of each of the thirteen breast cancer QPIs
outlining the variation at NHS Board level. Charts are colour coded by reporting year or by
network if reporting a single year. Where performance at either level is shown to fall below
the target, commentary from the relevant NHS Board is included to provide context to the
variation. Information in this report is shown by either Health Board of diagnosis or Health
Board of surgery as noted. Further information at hospital level is available from the data
tables, where applicable.
QPI 1: Multidisciplinary Team Meeting (MDT)
Evidence suggests that patients with cancer managed by a multidisciplinary team have a
better outcome. There is also evidence that the multidisciplinary management of patients
increases their overall satisfaction with their care.
Numerator: Number of patients with breast cancer discussed at the MDT before definitive
treatment.
Denominator: All patients with breast cancer.
Exclusions:
• Patients who died before first treatment.
Target: 95%
In each of the three reporting years, between 2015 and 2017, the percentage of patients with
breast cancer in Scotland who were discussed at the MDT before definitive treatment, was
above the 95% target. At NHS Board level, over the three years, NHS Dumfries & Galloway
(2016), NHS Fife (2015) and NHS Lothian (2017) narrowly missed the target.

Information Services Division
15
≥95%
0
10
20
30
40
50
60
70
80
90
100
Grampian Highland Orkney Shetland Tayside Western Isles
NoS Borders Dumfries & Galloway
Fife Lothian SCAN Ayrshire & Arran
Forth Valley Greater Glasgow &
Clyde
Lanarkshire WoSCAN Scotland
NoS SCAN WoSCAN Scotland
QPI 1 - Multi-Disciplinary Team Meeting Discussion (MDT) by Health Board of Audit
2015 2016 2017 Target
NHS Board/Region % Performance Numerator Denominator
NR for
Numerator
NR for
Exclusion
NR for
Denominator 2015 2016
Grampian 98.8 474 480 98.7 98.5
Highland 99.2 262 264 99.3 99.2
Orkney * * * - -
Shetland 100.0 10 10 100.0 100.0
Tayside 97.9 472 482 98.9 98.1
Western Isles * * * * *
NoS 98.5 1218 1236 98.9 98.5
Borders 98.7 77 78 100.0 98.6
Dumfries & Galloway 98.1 105 107 95.4 94.5
Fife 95.5 171 179 1 92.9 95.5
Lothian 94.7 859 907 95.5 96.0
SCAN 95.4 1212 1271 1 95.3 96.0
Ayrshire & Arran 98.6 435 441 98.4 99.5
Forth Valley 100.0 174 174 100.0 100.0
Greater Glasgow & Clyde 98.8 1184 1198 96.7 96.6
Lanarkshire 99.3 451 454 97.9 99.3
WoSCAN 99.0 2244 2267 97.5 97.9
Scotland 97.9 4674 4774 1 97.2 97.6
2017 Past % Performance
Source: Cancer audit - Data not shown due to small numbers * No data matching QPI criteria
For those patients not meeting the target in SCAN, all cases were reviewed and it was found
that some patients commenced hormone therapy prior to the MDT, which was regarded as
the most appropriate treatment in these cases.

Information Services Division
16
QPI 2: Non-Operative Diagnosis
Patients with breast cancer should have a non-operative histological diagnosis. Diagnosis of
patients non-operatively allows them to have only one definitive procedure, where possible.
Numerator: Number of patients with invasive or in-situ breast cancer with a non-operative
diagnosis of breast cancer (core biopsy / large volume biopsy).
Denominator: All patients with invasive or in-situ breast cancer.
Exclusions:
• All breast cancer patients with lobular carcinoma in situ (LCIS).
Target: 95%
Across the 3 years, the percentage of patients in Scotland receiving a non-operative
diagnosis of breast cancer was consistently above the 95% target. At NHS Board level, only
NHS Grampian did not achieve the target in any of the 3 years.
≥95%
0
10
20
30
40
50
60
70
80
90
100
Grampian Highland Orkney Shetland Tayside Western Isles
NoS Borders Dumfries & Galloway
Fife Lothian SCAN Ayrshire & Arran
Forth Valley Greater Glasgow &
Clyde
Lanarkshire WoSCAN Scotland
NoS SCAN WoSCAN Scotland
QPI 2 - Non-Operative Diagnosis by Health Board of Audit
2015 2016 2017 Target

Information Services Division
17
Source: Cancer audit
- Data not shown due to small numbers * No data matching QPI criteria
In NHS Grampian a higher proportion of patients were diagnosed by FNA rather than core
biopsy / large volume biopsy, resulting in the QPI target not being met. Some of these
patients declined a core biopsy while others were considered unfit for the procedure.
NHS Board/Region % Performance Numerator Denominator
NR for
Numerator
NR for
Exclusion
NR for
Denominator 2015 2016
Grampian 91.2 437 479 93.7 92.3
Highland 97.7 256 262 99.3 96.5
Orkney * * * - -
Shetland 100.0 10 10 87.5 100.0
Tayside 99.2 478 482 98.9 97.9
Western Isles * * * * *
NoS 95.8 1181 1233 96.8 95.6
Borders 98.7 78 79 100.0 97.2
Dumfries & Galloway 99.1 107 108 1 99.1 97.8
Fife 100.0 166 166 98.2 96.5
Lothian 98.4 886 900 97.7 98.3
SCAN 98.7 1237 1253 1 98.0 97.9
Ayrshire & Arran 96.6 426 441 1 98.1 96.5
Forth Valley 100.0 174 174 98.9 98.8
Greater Glasgow & Clyde 97.7 1174 1202 7 97.6 97.9
Lanarkshire 97.1 443 456 4 97.3 97.8
WoSCAN 97.5 2217 2273 12 97.7 97.7
Scotland 97.4 4635 4759 13 97.6 97.2
2017 Past % Performance

Information Services Division
18
QPI 3(i): Pre-Operative Assessment of Axilla - Ultrasound
Patients with breast cancer should have pre-operative assessment of the axilla. A
preoperative diagnosis of nodal disease enables definitive treatment of the axilla at the time
of initial breast surgery.
Numerator: Number of patients with invasive breast cancer who undergo assessment of the
axilla by ultrasound before surgery.
Denominator: All patients with invasive breast cancer undergoing surgery.
Exclusions:
• No exclusions
Target: 95%
In 2017, 99% of the 3,682 patients with invasive breast cancer undergoing surgery in
Scotland had a pre-operative assessment of the axilla by ultrasound prior to surgery. This
QPI has consistently been above target nationally over the three years.
≥95%
0
10
20
30
40
50
60
70
80
90
100
Grampian Highland Orkney Shetland Tayside Western Isles
NoS Borders Dumfries & Galloway
Fife Lothian SCAN Ayrshire & Arran
Forth Valley Greater Glasgow &
Clyde
Lanarkshire WoSCAN Scotland
NoS SCAN WoSCAN Scotland
QPI 3(i) - Pre-Operative Assessment of Axilla by Health Board of Audit
2015 2016 2017 Target

Information Services Division
19
Source: Cancer audit
- Data not shown due to small numbers * No data matching QPI criteria
NHS Board/Region % Performance Numerator Denominator
NR for
Numerator
NR for
Exclusion
NR for
Denominator 2015 2016
Grampian 97.2 351 361 92.1 97.4
Highland 98.6 204 207 99.6 98.4
Orkney * * * - *
Shetland 100.0 7 7 - 95.5
Tayside 99.5 368 370 95.3 97.5
Western Isles * * * * *
NoS 98.4 930 945 95.1 97.6
Borders 96.4 53 55 100.0 100.0
Dumfries & Galloway 99.0 95 96 98.7 98.7
Fife 99.2 128 129 1 99.1 98.5
Lothian 98.2 707 720 1 8 98.8 99.3
SCAN 98.3 983 1000 2 8 98.9 99.2
Ayrshire & Arran 98.8 338 342 1 100.0 99.3
Forth Valley 100.0 133 133 100.0 98.4
Greater Glasgow & Clyde 98.8 903 914 8 97.9 97.9
Lanarkshire 99.7 347 348 6 98.9 98.8
WoSCAN 99.1 1721 1737 15 98.6 98.3
Scotland 98.7 3634 3682 2 23 97.7 98.4
2017 Past % Performance

Information Services Division
20
QPI 3(ii): Pre-Operative Assessment of Axilla – Ultrasound + FNA or core biopsy
Patients with invasive breast cancer should undergo pre-treatment ultrasound assessment of
the axilla. If morphologically suspicious nodes are identified these should be sampled, using
FNA or core biopsy.
Numerator: Number of patients with invasive breast cancer with suspicious morphology
reported on ultrasound who undergo a FNA/core biopsy of the axilla before surgery.
Denominator: All patients with invasive breast cancer undergoing surgery with suspicious
morphology reported on ultrasound.
Exclusions:
• No exclusions
Target: 85%
There were 910 patients reported on ultrasound with suspicious morphology across Scotland in 2017. Of these, 890 (98%) had a FNA/core biopsy of the axilla before surgery. As per part (i), this has been consistently above target nationally and at NHS Board level (with some exceptions due to small numbers) since 2015.
≥85%
0
10
20
30
40
50
60
70
80
90
100
Grampian Highland Orkney Shetland Tayside Western Isles
NoS Borders Dumfries & Galloway
Fife Lothian SCAN Ayrshire & Arran
Forth Valley Greater Glasgow &
Clyde
Lanarkshire WoSCAN Scotland
NoS SCAN WoSCAN Scotland
QPI 3(ii) - Pre-Operative Assessment of Axilla by Health Board of Audit
2015 2016 2017 Target

Information Services Division
21
Source: Cancer audit - Data not shown due to small numbers * No data matching QPI criteria
NHS Board/Region % Performance Numerator Denominator
NR for
Numerator
NR for
Exclusion
NR for
Denominator 2015 2016
Grampian 99.1 110 111 97.4 100.0
Highland 100.0 45 45 88.0 87.8
Orkney * * * * *
Shetland - - - - -
Tayside 95.8 113 118 97.2 95.7
Western Isles * * * * *
NoS 97.8 270 276 94.6 95.3
Borders 100.0 15 15 88.9 100.0
Dumfries & Galloway 97.2 35 36 100.0 100.0
Fife 100.0 49 49 1 97.4 98.2
Lothian 99.4 166 167 1 98.9 98.2
SCAN 99.3 265 267 2 98.4 98.5
Ayrshire & Arran 95.7 67 70 1 98.7 98.2
Forth Valley 94.1 32 34 94.7 97.5
Greater Glasgow & Clyde 97.3 179 184 2 97.4 96.6
Lanarkshire 97.5 77 79 1 100.0 100.0
WoSCAN 96.7 355 367 4 97.9 97.7
Scotland 97.8 890 910 6 96.9 97.2
2017 Past % Performance

Information Services Division
22
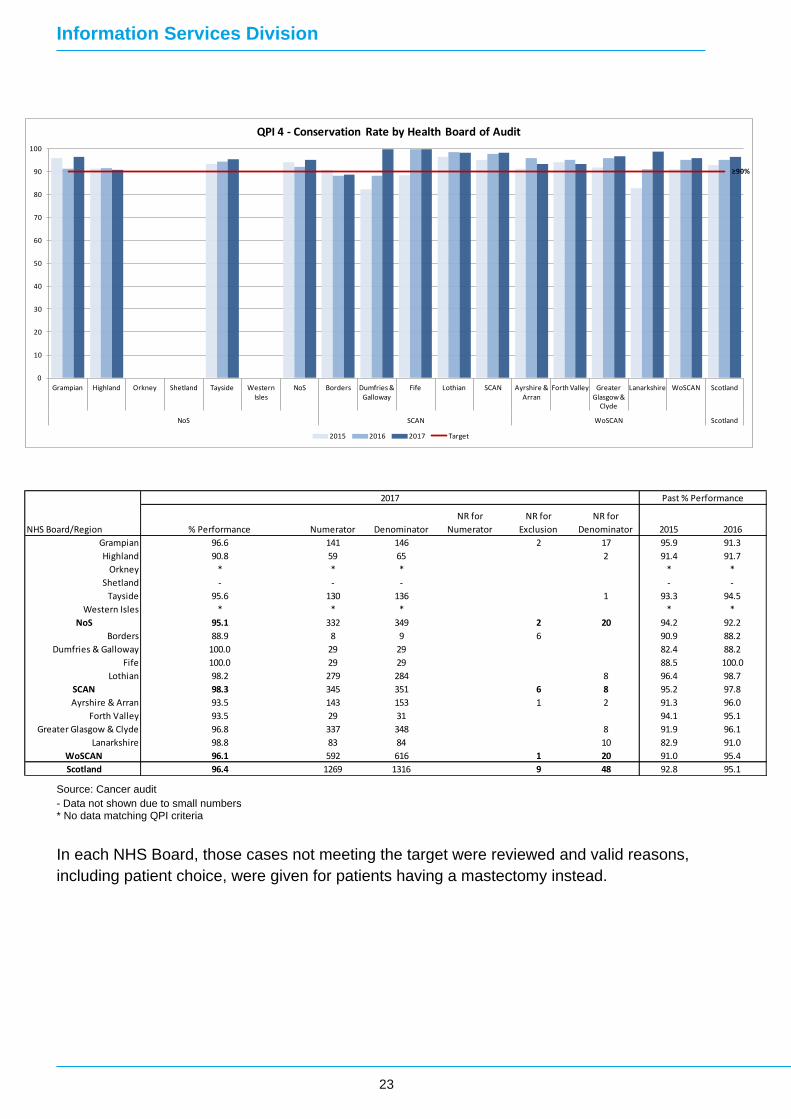
QPI 4: Conservation Rate
Patients with small breast cancers should undergo breast conservation whenever
appropriate. Breast conservation is appropriate for small breast cancers. Randomised trials
have shown no difference in survival for tumours treated by conservation surgery followed by
radiotherapy to mastectomy.
Numerator: Number of surgically treated patients with breast cancer less than 20mm whole
tumour size on histology (invasive plus in situ disease) treated by breast conservation
surgery.
Denominator: All surgically treated patients with breast cancer less than 20mm whole tumour
size on histology (invasive plus in situ disease).
Exclusions:
• Patients with multifocal breast cancer.
• Patients with breast cancer who have received neoadjuvant systemic therapy for ≥6
weeks (hormonal therapy or chemotherapy).
• Patients with high risk
• Patients who have had previous radiotherapy.
• Male patients.
Target: 90%
Across the 3 years, the percentage of patients in Scotland with small breast cancer tumours
undergoing breast conservation surgery was consistently above the 90% target. At NHS
Board level, only NHS Dumfries & Galloway and NHS Lanarkshire did not achieve the target
consistently over the period, although both have seen an increase to above target in 2017.
This increase may be partly due to changes in the exclusion criteria (i.e. patients with high
risk and patients who had previous radiotherapy) introduced in 2016.
Information Services Division
23
Source: Cancer audit
- Data not shown due to small numbers * No data matching QPI criteria
In each NHS Board, those cases not meeting the target were reviewed and valid reasons,
including patient choice, were given for patients having a mastectomy instead.
≥90%
0
10
20
30
40
50
60
70
80
90
100
Grampian Highland Orkney Shetland Tayside Western Isles
NoS Borders Dumfries & Galloway
Fife Lothian SCAN Ayrshire & Arran
Forth Valley Greater Glasgow &
Clyde
Lanarkshire WoSCAN Scotland
NoS SCAN WoSCAN Scotland
QPI 4 - Conservation Rate by Health Board of Audit
2015 2016 2017 Target
NHS Board/Region % Performance Numerator Denominator
NR for
Numerator
NR for
Exclusion
NR for
Denominator 2015 2016
Grampian 96.6 141 146 2 17 95.9 91.3
Highland 90.8 59 65 2 91.4 91.7
Orkney * * * * *
Shetland - - - - -
Tayside 95.6 130 136 1 93.3 94.5
Western Isles * * * * *
NoS 95.1 332 349 2 20 94.2 92.2
Borders 88.9 8 9 6 90.9 88.2
Dumfries & Galloway 100.0 29 29 82.4 88.2
Fife 100.0 29 29 88.5 100.0
Lothian 98.2 279 284 8 96.4 98.7
SCAN 98.3 345 351 6 8 95.2 97.8
Ayrshire & Arran 93.5 143 153 1 2 91.3 96.0
Forth Valley 93.5 29 31 94.1 95.1
Greater Glasgow & Clyde 96.8 337 348 8 91.9 96.1
Lanarkshire 98.8 83 84 10 82.9 91.0
WoSCAN 96.1 592 616 1 20 91.0 95.4
Scotland 96.4 1269 1316 9 48 92.8 95.1
2017 Past % Performance

Information Services Division
24
QPI 5: Surgical Margins
Breast cancers which are surgically treated should be adequately excised. There is an
increased risk of local recurrence if radial surgical excision margins are less than 1mm after
breast cancer surgery.
Numerator: Number of patients with breast cancer (invasive or ductal carcinoma in situ)
having breast conservation surgery with final radial (i.e. superior, inferior, medial or lateral)
excision margins less than 1mm (on pathology report).
Denominator: All patients with breast (invasive or ductal carcinoma in situ) cancer having
breast conservation surgery.
Exclusions:
• LCIS alone
Target: <5%
Over the 3 years, the percentage of patients in Scotland with surgical margins less than 1mm after breast cancer surgery was consistently well below the 5% maximum target. Only NHS Highland in 2016 did not meet the target during the period.
<5%
0
1
2
3
4
5
6
Grampian Highland Orkney Shetland Tayside Western Isles
NoS Borders Dumfries & Galloway
Fife Lothian SCAN Ayrshire & Arran
Forth Valley Greater Glasgow &
Clyde
Lanarkshire WoSCAN Scotland
NoS SCAN WoSCAN Scotland
QPI 5 - Surgical Margins by Health Board of Audit
2015 2016 2017 Target

Information Services Division
25
Source: Cancer audit - Data not shown due to small numbers * No data matching QPI criteria
NHS Highland reviewed those patients not meeting target in 2016 and noted valid reasons
including patients receiving palliative treatment where re-excision was not appropriate.
Similarly in WoSCAN, all patients failing to meet the QPI target were reviewed and detailed
clinical reasons for patients not undergoing further surgery were provided.
NHS Board/Region % Performance Numerator Denominator
NR for
Numerator
NR for
Exclusion
NR for
Denominator 2015 2016
Grampian 2.5 7 280 3.2 4.9
Highland 3.2 5 154 4.6 5.2
Orkney * * * * *
Shetland - - - - 0.0
Tayside 4.8 14 294 3.7 2.5
Western Isles * * * * *
NoS 3.6 26 731 3.7 3.9
Borders 0.0 0 38 3.0 0.0
Dumfries & Galloway 4.8 3 62 1 0.0 0.0
Fife 1.9 2 103 0.0 0.0
Lothian 0.8 5 644 8 1.7 2.4
SCAN 1.2 10 847 1 8 1.5 1.9
Ayrshire & Arran 0.4 1 282 1 1 0.5 0.0
Forth Valley 1.1 1 94 1.1 3.8
Greater Glasgow & Clyde 0.5 4 729 8 0.3 1.5
Lanarkshire 1.7 4 242 1 6 2.2 1.6
WoSCAN 0.7 10 1347 2 15 0.6 1.4
Scotland 1.6 46 2925 3 23 1.6 2.2
2017 Past % Performance

Information Services Division
26
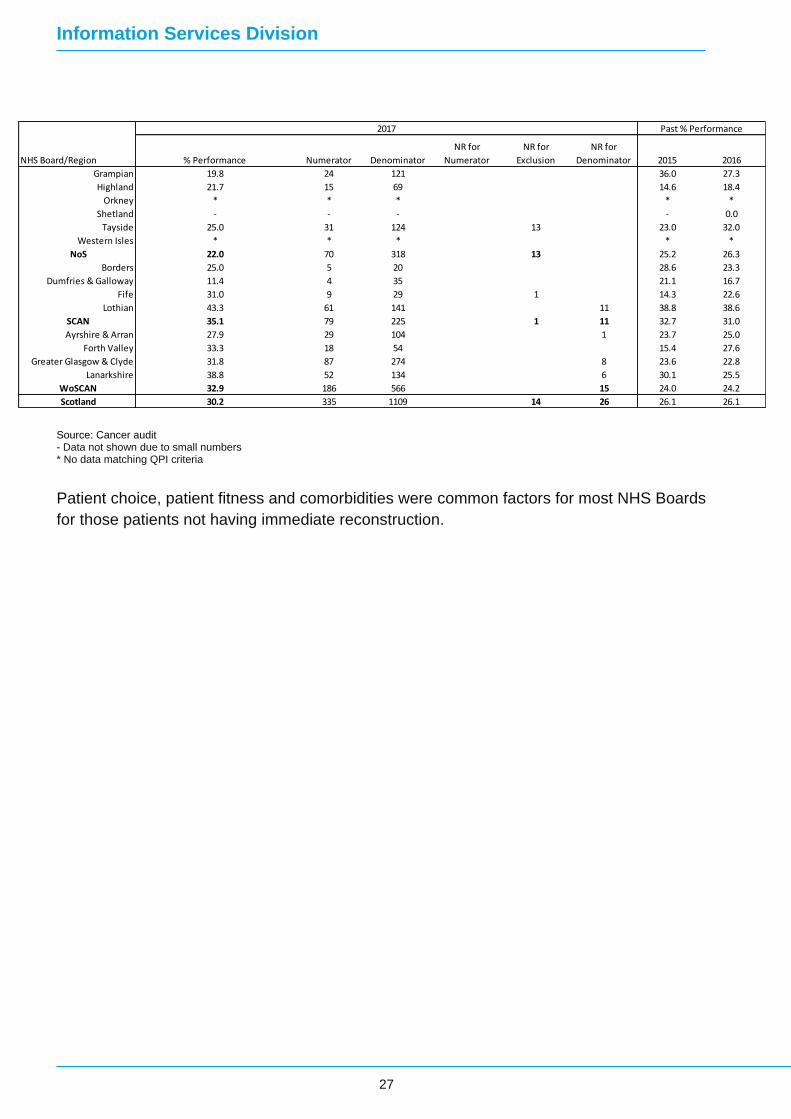
QPI 6: - Immediate Reconstruction Rate
Patients undergoing mastectomy for breast cancer should have access to immediate breast reconstruction. Evidence suggests that breast reconstruction is not associated with an increase in the rate of local recurrence, nor does it affect the ability to detect recurrence and it can yield psychological benefit. Access to immediate breast reconstruction is difficult to measure so uptake is used as a proxy. Numerator: Number of patients with breast cancer undergoing immediate breast reconstruction at the time of mastectomy. Denominator: All patients with breast cancer undergoing mastectomy. Exclusions:
• All patients with M1 disease.
• All male patients. Target: 25%
Of the 1109 patients with breast cancer undergoing mastectomy in Scotland in 2017, 30%
(335 patients) received breast reconstruction at the time of mastectomy. This has been
consistently above target nationally for the past 3 years. At NHS Board and Network level,
performance is more variable with both NHS Highland and NHS Dumfries & Galloway failing
to achieve target in any of the three years and North of Scotland the only network not to
achieve target in 2017.
≥25%
0
5
10
15
20
25
30
35
40
45
50
Grampian Highland Orkney Shetland Tayside Western Isles
NoS Borders Dumfries & Galloway
Fife Lothian SCAN Ayrshire & Arran
Forth Valley Greater Glasgow &
Clyde
Lanarkshire WoSCAN Scotland
NoS SCAN WoSCAN Scotland
QPI 6 - Immediate Reconstruction Rate by Health Board of Audit
2015 2016 2017 Target
Information Services Division
27
Source: Cancer audit - Data not shown due to small numbers * No data matching QPI criteria
Patient choice, patient fitness and comorbidities were common factors for most NHS Boards
for those patients not having immediate reconstruction.
NHS Board/Region % Performance Numerator Denominator
NR for
Numerator
NR for
Exclusion
NR for
Denominator 2015 2016
Grampian 19.8 24 121 36.0 27.3
Highland 21.7 15 69 14.6 18.4
Orkney * * * * *
Shetland - - - - 0.0
Tayside 25.0 31 124 13 23.0 32.0
Western Isles * * * * *
NoS 22.0 70 318 13 25.2 26.3
Borders 25.0 5 20 28.6 23.3
Dumfries & Galloway 11.4 4 35 21.1 16.7
Fife 31.0 9 29 1 14.3 22.6
Lothian 43.3 61 141 11 38.8 38.6
SCAN 35.1 79 225 1 11 32.7 31.0
Ayrshire & Arran 27.9 29 104 1 23.7 25.0
Forth Valley 33.3 18 54 15.4 27.6
Greater Glasgow & Clyde 31.8 87 274 8 23.6 22.8
Lanarkshire 38.8 52 134 6 30.1 25.5
WoSCAN 32.9 186 566 15 24.0 24.2
Scotland 30.2 335 1109 14 26 26.1 26.1
2017 Past % Performance

Information Services Division
28
QPI 8: Minimising Hospital Stay – Day Case Surgery
Patients should have the opportunity for day case surgery wherever appropriate. It is safe to perform wide excision and axillary staging as a short stay procedure in the majority of patients & clinical quality has been shown to be improved utilising this model, resulting in better patient outcomes. Numerator: Number of patients with breast cancer undergoing wide excision and/or axillary sampling procedure (sentinel node biopsy or 4 node sample) as day case surgery. Denominator: All patients with breast cancer undergoing wide excision and/or axillary sampling procedure (sentinel node biopsy or 4 node sample). Exclusions:
• All patients with breast cancer undergoing partial breast reconstruction. Target: 60%
Since 2015, the percentage of patients in Scotland undergoing wide excision and axillary sampling as daycase surgery has steadily increased to 68% in 2017. At network level, only the North of Scotland has not achieved target over this period due to the performance in NHS Grampian and NHS Tayside.
≥60%
0
10
20
30
40
50
60
70
80
90
Grampian Highland Orkney Shetland Tayside Western Isles
NoS Borders Dumfries & Galloway
Fife Lothian SCAN Ayrshire & Arran
Forth Valley Greater Glasgow &
Clyde
Lanarkshire WoSCAN Scotland
NoS SCAN WoSCAN Scotland
QPI 8 - Minimising Hospital Stay - Day Case Surgery by Health Board of Audit
2015 2016 2017 Target

Information Services Division
29
Source: Cancer audit - Data not shown due to small numbers * No data matching QPI criteria
NHS Grampian recognises that achieving this target is challenging although there has been
noticeable improvement over the three years. Improvements in managing patient
expectations, anaesthetic pre-assessments and implementing nurse led discharge have
contributed to this but overall this still remains a challenging indicator.
NHS Forth Valley commented that it is clinical practice for those patients undergoing
mammoplasty to stay within the hospital overnight.
NHS Board/Region % Performance Numerator Denominator
NR for
Numerator
NR for
Exclusion
NR for
Denominator 2015 2016
Grampian 37.5 112 299 11.0 23.0
Highland 72.5 150 207 74.1 79.3
Orkney * * * * *
Shetland - - - - 70.0
Tayside 50.7 170 335 24.3 45.7
Western Isles * * * * *
NoS 51.4 433 843 31.3 45.1
Borders 70.3 26 37 65.8 70.6
Dumfries & Galloway 71.9 41 57 77.1 75.4
Fife 75.2 106 141 67.3 71.0
Lothian 77.3 580 750 76.7 77.4
SCAN 76.4 753 985 75.4 76.1
Ayrshire & Arran 65.9 224 340 37.4 44.3
Forth Valley 58.7 71 121 74.5 64.7
Greater Glasgow & Clyde 72.5 553 763 61.9 67.2
Lanarkshire 85.4 252 295 79.6 82.8
WoSCAN 72.4 1100 1519 61.7 64.9
Scotland 68.3 2286 3347 59.4 63.3
2017 Past % Performance

Information Services Division
30
QPI 9: HER2 Status for Decision Making
HER2 status should be available to inform treatment decision making. HER2 status has a significant impact on survival and so has a significant influence on decisions on neoadjuvant and adjuvant treatment. Numerator: Number of patients with invasive breast cancer for whom the HER2 status (as detected by immunohistochemistry (IHC) and/or FISH analysis) is reported within 2 weeks of core biopsy. Denominator: All patients with invasive breast cancer. Exclusions:
• No exclusions Target: 80%
In 2017, 82% of patients with invasive breast cancer in Scotland had their HER2 status
reported within 2 weeks of core biopsy. This is the second consecutive year that the target
has been met. This is largely due to the improvements over the same period in the WoSCAN
NHS Boards: NHS Greater Glasgow & Clyde, NHS Forth Valley and NHS Lanarkshire. Only
NHS Grampian, NHS Highland, NHS Lanarkshire and NHS Dumfries & Galloway failed to
achieve the target across the three years.
≥80%
0
10
20
30
40
50
60
70
80
90
100
Grampian Highland Orkney Shetland Tayside Western Isles
NoS Borders Dumfries & Galloway
Fife Lothian SCAN Ayrshire & Arran
Forth Valley Greater Glasgow &
Clyde
Lanarkshire WoSCAN Scotland
NoS SCAN WoSCAN Scotland
QPI 9 - HER2 Status for Decision Making by Health Board of Audit
2015 2016 2017 Target

Information Services Division
31
Source: Cancer audit - Data not shown due to small numbers * No data matching QPI criteria
In NHS Grampian, there is evidence of improvement over the three years and they continue to look for ways to improve the turnaround of the FISH (Fluorescence in situ hybridization) results, which is the major cause of the delay. Similarly, in NHS Highland, while it is desirable to reduce delays in the FISH result, patients are re-discussed if the HER2 status is not available at the initial MDT.
The majority of cases not meeting the QPI in NHS Ayrshire & Arran also required FISH
analysis to determine HER2 status. Since FISH analysis is not performed on site this can
lead to delays in HER2 not being reported within 2 weeks of the core biopsy. Similarly, in
NHS Lanarkshire there may be additional delays since HER2 testing is carried out in
Glasgow.
In NHS Fife and NHS Dumfries and Galloway cases involve transportation of the biopsy to
the laboratory in Edinburgh after initial local reporting. If cases require an additional FISH
test, this will add a few working days to the overall process. In a minority of cases, where
there is insufficient invasive material in the core biopsy for adequate assessment, HER2
status determination is deferred until surgery, thus missing the 14 day reporting target.
NHS Board/Region % Performance Numerator Denominator
NR for
Numerator
NR for
Exclusion
NR for
Denominator 2015 2016
Grampian 74.3 297 400 69.0 68.6
Highland 59.7 141 236 73.5 70.9
Orkney * * * - -
Shetland 100.0 10 10 100.0 96.4
Tayside 93.7 399 426 95.3 94.3
Western Isles * * * * *
NoS 79.0 847 1072 79.8 80.7
Borders 94.6 70 74 89.7 93.8
Dumfries & Galloway 76.4 81 106 72.3 78.7
Fife 71.7 124 173 87.9 83.5
Lothian 89.9 742 825 4 88.6 91.4
SCAN 86.3 1017 1178 4 87.1 89.3
Ayrshire & Arran 69.2 270 390 85.2 75.7
Forth Valley 93.6 147 157 1 41.3 76.6
Greater Glasgow & Clyde 85.4 933 1093 72.5 78.7
Lanarkshire 79.1 333 421 67.0 77.4
WoSCAN 81.7 1683 2061 1 71.2 77.8
Scotland 82.3 3547 4311 5 77.6 81.5
2017 Past % Performance

Information Services Division
32
QPI 10: Radiotherapy for Breast Conservation
After wide local excision patients with breast cancer should receive radiotherapy. Trials have demonstrated a significant reduction in local recurrence with the use of radiotherapy after breast conservation. Numerator: Number of patients with invasive breast cancer having conservation surgery receiving radiotherapy to the breast. Denominator: All patients with invasive breast cancer having conservation surgery. Exclusions: • All patients with breast cancer taking part in clinical trials of radiotherapy treatment. • All patients with M1 disease. Target: 95%
Overall in Scotland, the target of 95% of patients having breast conservation surgery who
received radiotherapy was not met in each of the last three years and with a decreasing
trend. Similar patterns were observed at network level with only the North of Scotland
achieving target in any of the three years. At NHS Board level, only NHS Grampian achieved
target consistently across the three year period.
≥95%
0
10
20
30
40
50
60
70
80
90
100
Grampian Highland Orkney Shetland Tayside Western Isles
NoS Borders Dumfries & Galloway
Fife Lothian SCAN Ayrshire & Arran
Forth Valley Greater Glasgow &
Clyde
Lanarkshire WoSCAN Scotland
NoS SCAN WoSCAN Scotland
QPI 10 - Radiotherapy for Breast Conservation by Health Board of Audit
2015 2016 2017 Target

Information Services Division
33
Source: Cancer audit - Data not shown due to small numbers * No data matching QPI criteria
Those cases not meeting target were reviewed in each of the NHS Boards and valid reasons
were provided including patient choice and patient fitness.
It is expected that this QPI will be updated after the next formal review to reflect changes in
clinical practice since some recent studies have shown no benefit to older patients given post
operative radiotherapy.
NHS Board/Region % Performance Numerator Denominator
NR for
Numerator
NR for
Exclusion
NR for
Denominator 2015 2016
Grampian 95.3 202 212 96.2 98.1
Highland 93.9 124 132 95.6 92.4
Orkney * * * * *
Shetland - - - - 83.3
Tayside 93.8 240 256 13 95.8 93.9
Western Isles * * * * *
NoS 94.4 568 602 13 95.9 95.0
Borders 93.9 31 33 96.6 85.2
Dumfries & Galloway 83.9 52 62 1 93.3 89.8
Fife 93.9 92 98 97 95.8 92.6
Lothian 93.6 540 577 1 93.7 95.2
SCAN 92.9 715 770 98 1 94.0 94.2
Ayrshire & Arran 88.1 208 236 2 2 1 91.4 87.7
Forth Valley 87.1 74 85 93.4 73.9
Greater Glasgow & Clyde 90.5 573 633 1 8 92.8 92.3
Lanarkshire 82.3 177 215 1 1 6 90.1 82.9
WoSCAN 88.3 1032 1169 4 3 15 92.3 88.7
Scotland 91.1 2315 2541 4 114 16 93.7 91.9
2017 Past % Performance

Information Services Division
34
QPI 11: Adjuvant Chemotherapy
Patients with breast cancer should receive chemotherapy post operatively where it will provide a survival benefit for patients. Large randomised trials have confirmed that adjuvant systemic therapy improves relapse-free survival and overall survival. Numerator: Number of patients with invasive breast cancer who have a ≥5% overall survival benefit of chemotherapy treatment predicted at 10 years that undergo adjuvant chemotherapy. Denominator: All patients with invasive breast cancer who have a ≥5% overall survival benefit of chemotherapy treatment predicted at 10 years. Exclusions: • All patients with breast cancer taking part in trials of chemotherapy treatment. • All patients with breast cancer who have had neo-adjuvant chemotherapy. • All patients with M1 disease. Target: 85%
This QPI was changed significantly at the formal review and consequently previous years’
data is not comparable, therefore only the last 2 years are reported.
In 2017, 80% of patients in this cohort in Scotland underwent adjuvant chemotherapy. This is
the second consecutive year that the target has not been met nationally. At NHS Board level,
only NHS Grampian, NHS Shetland, NHS Fife, NHS Ayrshire & Arran and NHS Greater
Glasgow and Clyde achieved the target in either 2016 or 2017 with NHS Grampian achieving
target in both years.
For a significant number of patients (as indicated by the ‘not recorded for denominator’
figures in the table below), the overall survival benefit of chemotherapy was not recorded.
This meant that large numbers of patients have been excluded from the results of this QPI,
potentially biasing the results reported. As such caution should be exercised when
comparing performance between NHS Boards and regions.

Information Services Division
35
Source: Cancer audit - Data not shown due to small numbers * No data matching QPI criteria
In the majority of cases that were reviewed across the country it was found that patients declining treatment and patient comorbidities were common reasons for not meeting the target.
≥85%
0
10
20
30
40
50
60
70
80
90
100
Grampian Highland Orkney Shetland Tayside Western Isles
NoS Borders Dumfries & Galloway
Fife Lothian SCAN Ayrshire & Arran
Forth Valley Greater Glasgow &
Clyde
Lanarkshire WoSCAN Scotland
NoS SCAN WoSCAN Scotland
QPI 11 - Adjuvant Chemotherapy by Health Board of Audit
2015 2016 2017 Target
NHS Board/Region % Performance Numerator Denominator
NR for
Numerator
NR for
Exclusion
NR for
Denominator 2015 2016
Grampian 91.7 33 36 41 71.4 94.3
Highland 80.0 16 20 93.0 82.0
Orkney * * * * *
Shetland - - - 1 - 100.0
Tayside 75.6 31 41 4 10 45.8 70.0
Western Isles * * * * *
NoS 82.7 81 98 4 52 70.1 81.7
Borders 66.7 8 12 * 62.5
Dumfries & Galloway 83.3 5 6 7 * 80.0
Fife 84.6 22 26 23 * 91.2
Lothian 78.7 70 89 7 * 82.1
SCAN 78.9 105 133 23 14 * 81.9
Ayrshire & Arran 76.9 30 39 3 * 88.5
Forth Valley 63.8 30 47 * 70.7
Greater Glasgow & Clyde 87.0 114 131 2 * 72.9
Lanarkshire 50.0 3 6 77 * 40.0
WoSCAN 79.4 177 223 82 * 73.8
Scotland 80.0 363 454 27 148 70.1 78.9
2017 Past % Performance

Information Services Division
36
QPI 13: Re-excision Rates Patients undergoing surgery for breast cancer should only undergo one definitive operation where possible. Patients undergoing additional surgical procedures can be subject to unnecessary stress, as well as potential complications and delays in recovery. Numerator: Number of patients with breast cancer (invasive or in situ) having breast conservation surgery who undergo re-excision or mastectomy following initial breast surgery. Denominator: All patients with breast (invasive or in situ) cancer having breast conservation surgery as their initial or only breast surgery. Exclusions:
• LCIS alone Target: <20%
This is a new QPI that was added after the formal review and, therefore, only 2 years worth of data are available. In each of the two years, the percentage of patients undergoing additional surgical procedures following initial breast conservation surgery was comfortably below the target of 20%. Most NHS Boards also achieved the target with only NHS Fife, NHS Lothian and NHS Lanarkshire having re-excision rates above 20% in 2017.
<20%
0
5
10
15
20
25
Grampian Highland Orkney Shetland Tayside Western Isles
NoS Borders Dumfries & Galloway
Fife Lothian SCAN Ayrshire & Arran
Forth Valley Greater Glasgow &
Clyde
Lanarkshire WoSCAN Scotland
NoS SCAN WoSCAN Scotland
QPI 13 - Re-excision Rates by Health Board of Audit
2015 2016 2017 Target

Information Services Division
37
Source: Cancer audit - Data not shown due to small numbers * No data matching QPI criteria
In NHS Lanarkshire, an internal audit of patients not meeting the QPI was conducted – further action may be taken depending on a review of the audit findings.
NHS Board/Region % Performance Numerator Denominator
NR for
Numerator
NR for
Exclusion
NR for
Denominator 2015 2016
Grampian 13.2 54 409 * 12.5
Highland 16.7 38 227 1 * 18.5
Orkney * * * * *
Shetland 0.0 0 7 * 9.5
Tayside 7.6 32 422 * 8.8
Western Isles * * * * *
NoS 11.6 124 1065 1 * 12.0
Borders 5.2 3 58 * 14.3
Dumfries & Galloway 15.3 15 98 * 10.1
Fife 21.5 29 135 * 21.2
Lothian 20.2 134 663 1 7 * 18.8
SCAN 19.0 181 954 1 7 * 18.2
Ayrshire & Arran 13.3 52 392 1 1 * 12.3
Forth Valley 13.3 20 150 * 5.1
Greater Glasgow & Clyde 11.7 118 1012 8 * 12.5
Lanarkshire 20.3 77 380 6 * 16.2
WoSCAN 13.8 267 1934 1 15 * 12.6
Scotland 14.5 572 3953 2 23 * 13.9
2017 Past % Performance

Information Services Division
38
QPI 14(i): Referral for Genetics Testing – patients under 30 years of age
Patients with breast cancer should be offered referral to a specialist genetics clinic where appropriate. Numerator: Number of patients with breast cancer under 30 years of age referred to a specialist clinic for genetic testing. Denominator: All patients with breast cancer who are under 30 years of age. Exclusions:
• No exclusions Target: 90%
This is a new QPI that was added after the formal review and, therefore, only 2 years worth of data are available.
There were very few patients diagnosed with breast cancer under 30 years of age across the 2 years. In 2017, only 1 patient of the 18 diagnosed was not referred to a specialist clinic for genetic testing thus achieving the target. This is a slight improvement over 2016 but, given the small numbers involved, caution is advised when interpreting these figures.
QPI 14(ii): Referral for Genetics Testing – patients with triple negative breast cancer under 40 years of age
Patients with breast cancer should be offered referral to a specialist genetics clinic where appropriate. Numerator: Number of patients with triple negative breast cancer under 40 years of age referred to a specialist clinic for genetic testing. Denominator: All patients with triple negative breast cancer who are under 40 years of age. Exclusions:
• No exclusions Target: 90%
As per QPI14(i), there were very few patients with triple negative breast cancer under 40 years of age. In both years, the percentage of patients in this cohort referred to a specialist clinic for genetic testing was well above the 90% target. Again, due to the small numbers, caution is advised when interpreting these figures particularly when comparing at NHS Board level.

Information Services Division
39
QPI 15: 30 Day Mortality following Chemotherapy
Treatment related mortality is a marker of the quality and safety of the whole service provided by the Multi Disciplinary Team (MDT). Numerator: Number of patients with breast cancer who undergo chemotherapy that die within 30 days of treatment. Denominator: All patients with breast cancer who undergo chemotherapy. Exclusions:
• No exclusions Targets: Neoadjuvant and adjuvant treatment <1% Palliative treatment <5%
This is a new QPI which was added after the initial formal review. Neoadjuvant Chemotherapy In 2017, 3 patients from a total of 540 died within 30 days of receiving neo-adjuvant chemotherapy for breast cancer. This is less than the 1% mortality rate target for this treatment type and the third year in a row that the target has been met since this QPI was introduced. Adjuvant Chemotherapy Similarly, for those patients receiving adjuvant chemotherapy, the mortality rate for Scotland was less than 1% in each year since 2015. Palliative Chemotherapy The percentage of patients dying within 30 days of receiving palliative chemotherapy from breast cancer has increased from 7% in 2015 to 11% in 2017 which is above the target of <5%. It should be noted, however, that the number of patients in this category was relatively small in each year. In each case where a patient died within 30 days of the above treatment types, each NHS Board reviewed the details associated with each case and no further action was required.

Information Services Division
40
Clinical Trials
Access to Clinical Trials is a common issue for all cancer types; therefore, a generic QPI was
developed to measure performance across the country. Further details on the development
and definition of this QPI can be found here. Specifically for breast cancer, the QPI is defined
as follows and Appendix A3 contains a list of breast cancer trials into which patients have
been recruited in Scotland during the reporting period ending December 2017. Information is
shown by each Scottish Cancer Research Network (SCRN).
Clinical Trials Access: Proportion of patients with breast cancer who are consented for a clinical trial / research study.
All patients should be considered for participation in available clinical trials / research studies, wherever eligible. Numerator: Number of patients with breast cancer consented for a clinical trial / research study. Denominator: All patients diagnosed with breast cancer (5 year average of Scottish Cancer Registry data) Exclusions: No exclusions. Target: 15%
At the formal review, this QPI was changed to patients consented for clinical trial (defined as
patients who have given consent to participate in a clinical trial / research study subject to
study specific screening for eligibility) rather than enrolled without the
interventional/translational split and with a target of 15%. This new definition came into effect
in January 2017 and consequently, for breast cancer, year 3 data reflects this new definition
(measurability version 2) whereas years 1 and 2 are measured against version 1. Therefore,
comparison across years is not advised.
Patients enrolled for translational trials / interventional studies (Measurability Version 1.0)
Network Trial Type TargetNo of patients
enrolled
Av cancer
registrations%Enrolled
No of patients
enrolled
Av cancer
registrations %Enrolled
SCRN - North & East 7.5% 77 1240 6.2% 90 1243 7.2%
SCRN - South East 7.5% 77 1315 5.9% 101 1337 7.6%
SCRN - West 7.5% 100 2422 4.1% 143 2454 5.8%
SCRN - North & East 15% 77 1240 6.2% 102 1243 8.2%
SCRN - South East 15% 413 1315 31.4% 307 1337 23.0%
SCRN - West 15% 9 2422 0.4% 39 2454 1.6%
2015 2016
Interventional
Translational

Information Services Division
41
Patients consented for all trials (Measurability Version 2.0)
Network TargetNo of patients
consented
Av cancer
registrations%Consented
SCRN - North & East 15% 127 1274 10.0%
SCRN - South East 15% 394 1317 29.9%
SCRN - West 15% 253 2447 10.3%
2017

Information Services Division
42
List of abbreviations
QPI - Quality Performance Indicator
ISD - Information Services Division
NCA - North Cancer Alliance
NOS - North of Scotland
WoSCAN - West of Scotland cancer network
SCAN - South East Scotland cancer network
MDT - Multidisciplinary team
SCRN - Scottish Cancer Research Network
SIMD - Scottish Index of Multiple Deprivation
SMR01 - Scottish Morbidity Record (Inpatient and Daycase Activity)
CT - Computed Tomography scan
MRI - Magnetic Resonance Imaging scan

Information Services Division
43
List of Tables
File name File and size
Breast Cancer Data Tables Excel 115 Kb

Information Services Division
44
Contact
John Connor
Principal Information Analyst
0141 282 2231
Colin Houston
Senior Information Analyst
0131 275 6397
Further Information
Further information on Cancer Quality Performance Indicators can be found on the Cancer
QPI section of the ISD website.
The next release of this publication will be April 2022.
Rate this publication
Please provide feedback on this publication to help us improve our services.

Information Services Division
45
Appendices
Appendix 1 – Background information The purpose of the cancer quality work programme and the roles and responsibilities of each
organisation are outlined in Chief Executives Letter (CEL 06). This document also provides
details of the data collection, quality assurance and governance processes that are critical to
the reporting of QPIs.
Appendix 2 – Breast Cancer QPIs The tables below show the list of Breast Cancer QPIs applicable to this publication. Please
note that revisions to these QPIs may have been made since the initial data collection – refer
to the Healthcare Improvement Scotland website for the latest version of these QPIs.
QPI Numerator Denominator Exclusions Target
QPI 1: Multidisciplinary
Team Meeting (MDT)
Number of patients with breast cancer discussed at the MDT before definitive treatment.
All patients with breast cancer.
Patients who died before first treatment.
95%
QPI 2: Non-Operative
Diagnosis
Number of patients with invasive or in-situ breast cancer with a non-operative diagnosis of breast cancer (core biopsy / large volume biopsy).
All patients with invasive or in-situ breast cancer.
All breast cancer
patients with lobular
carcinoma in situ
(LCIS).
95%
QPI 3(i): Pre-Operative
Assessment of Axilla -
Ultrasound
Number of patients with invasive breast cancer who undergo assessment of the axilla by ultrasound before surgery.
All patients with invasive breast cancer undergoing surgery.
No exclusions. 95%
QPI 3(ii): Pre-
Operative Assessment
of Axilla - Biopsy
Number of patients with invasive breast cancer with suspicious morphology reported on ultrasound who undergo a FNA/core biopsy of the axilla before surgery.
All patients with invasive breast cancer undergoing surgery with suspicious morphology reported on ultrasound.
No exclusions. 85%
QPI 4: Conservation
Rate
Number of surgically treated patients with breast cancer less than 20mm whole tumour size on histology (invasive plus in situ disease) treated by breast conservation surgery.
All surgically treated patients with breast cancer less than 20mm whole tumour size on histology (invasive plus in situ disease).
Patients with multifocal breast cancer. Patients with breast cancer who have received neoadjuvant systemic therapy for ≥6 weeks (hormonal therapy or chemotherapy). Patients with high
90%

Information Services Division
46
risk Patients who have had previous radiotherapy. Male patients.
QPI 5: Surgical
Margins
Number of patients with breast cancer (invasive or ductal carcinoma in situ) having breast conservation surgery with final radial (i.e. superior, inferior, medial or lateral) excision margins less than 1mm (on pathology report).
All patients with breast (invasive or ductal carcinoma in situ) cancer having breast conservation surgery.
LCIS alone <5%
QPI 6: Immediate
Reconstruction Rate
Number of patients with breast cancer undergoing immediate breast reconstruction at the time of mastectomy.
All patients with breast cancer undergoing mastectomy.
All patients with M1
disease
All male patients.
25%
QPI 8: Minimising Hospital Stay – Day Case Surgery
Number of patients with breast cancer undergoing wide excision and/or axillary sampling procedure (sentinel node biopsy or 4 node sample) as day case surgery.
All patients with breast cancer undergoing wide excision and/or axillary sampling procedure (sentinel node biopsy or 4 node sample).
All patients with breast cancer undergoing partial breast reconstruction.
60%
QPI 9: HER2 Status for Decision Making
Number of patients with invasive breast cancer for whom the HER2 status (as detected by immunohistochemistry (IHC) and/or FISH analysis) is reported within 2 weeks of core biopsy.
All patients with invasive breast cancer.
No exclusions. 80%
QPI 10: Radiotherapy for Breast Conservation
Number of patients with invasive breast cancer having conservation surgery receiving radiotherapy to the breast.
All patients with invasive breast cancer having conservation surgery.
All patients with breast cancer taking part in clinical trials of radiotherapy treatment. All patients with M1 disease.
95%
QPI 11: Adjuvant Chemotherapy
Number of patients with invasive breast cancer who have a ≥5% overall survival benefit of chemotherapy treatment predicted at 10 years that undergo adjuvant chemotherapy.
All patients with invasive breast cancer who have a ≥5% overall survival benefit of chemotherapy treatment predicted at 10 years.
All patients with breast cancer taking part in trials of chemotherapy treatment. All patients with breast cancer who have had neo-adjuvant chemotherapy. All patients with M1 disease.
85%

Information Services Division
47
QPI 13: Re-excision Rates
Number of patients with breast cancer (invasive or in situ) having breast conservation surgery who undergo re-excision or mastectomy following initial breast surgery.
All patients with breast (invasive or in situ) cancer having breast conservation surgery as their initial or only breast surgery.
LCIS alone
<20%
QPI 14(i): Referral for Genetics Testing – Under 30
Number of patients with breast cancer under 30 years of age referred to a specialist clinic for genetic testing.
All patients with breast cancer who are under 30 years of age.
No exclusions 90%
QPI 14(ii): Referral for Genetics Testing – triple negative
Number of patients with triple negative breast cancer under 40 years of age referred to a specialist clinic for genetic testing.
All patients with triple negative breast cancer who are under 40 years of age.
No exclusions 90%
QPI 15: 30 Day Mortality following Chemotherapy
Number of patients with breast cancer who undergo chemotherapy that die within 30 days of treatment.
All patients with breast cancer who undergo chemotherapy.
No exclusions <1% (neoadjuvant & adjuvant)
<5% (palliative)

Information Services Division
48
Appendix 3 – Breast Cancer Clinical Trials
The list of clinical trials open for recruitment during 2015-17 for breast cancer patients in
Scotland across the Scottish Cancer Research Networks is shown below. Further details on
these clinical trials are available from the relevant SCRN.

Information Services Division
49
Appendix 4 – Publication Metadata
Metadata Indicator Description
Publication title Breast Cancer Quality Performance Indicators
Description This report shows the performance of NHS Boards against
seven Breast Cancer QPIs for the period January 2015 to
December 2017. Relevant commentary from NHS Boards
is also included to provide local context to the data.
Theme Health and Social Care
Topic Cancer services
Format PDF Document
Data source(s) Cancer audit, Cancer registry
Date that data are acquired September 2018
Release date April 9th 2019
Frequency Every 3 years
Timeframe of data and
timeliness
Data covering patients diagnosed between January 2015
and December 2017.
Continuity of data First published 29th April 2014
Revisions statement It is expected that QPI definitions and measurability
documents will evolve and therefore future publications
may contain revisions to previously published information.
Revisions relevant to this
publication
Not applicable
Concepts and definitions QPI definitions and measurability criteria are available from
the Cancer Audit section of the ISD website.
Relevance and key uses of
the statistics
The reporting of performance against these national QPIs is
underpinned by a national governance framework that aims
to use these data to improve cancer services in Scotland.
Accuracy Information on the accuracy of some of the national
datasets used within this publication is available on the ISD
website.
ISD only receives aggregate data from each NHS Board to
populate these indicators (with the exception of SMR based
indicators and case ascertainment). Derivations of the
figures and data accuracy are matters for individual NHS

Information Services Division
50
Boards.
Completeness For the reporting period, information based on the SMR01
data completeness can be found here. 100% of QPI
aggregate data was returned.
Comparability The national dataset and data definitions in conjunction with the final quality performance indicators and the accompanying measurability document were agreed in public engagement to ensure data collection is comparable across the country.
Accessibility It is the policy of ISD Scotland to make its web sites and
products accessible according to published guidelines.
Coherence and clarity Statistics for each QPI are presented consistently in chart and table format at NHS Board level, with national figures and performance targets included for comparison and clarity.
Value type and unit of
measurement
The units of measure include numbers and percentages.
Disclosure The ISD protocol on Statistical Disclosure Protocol is
followed.
Official Statistics designation Official Statistics
UK Statistics Authority
Assessment
Not currently put forward for assessment
Last published April 2014
Next published April 2022
Date of first publication 29/04/2014
Help email [email protected]
Date form completed 9th January 2019

Information Services Division
51
Appendix 5 – Early access details
Pre-Release Access
Under terms of the "Pre-Release Access to Official Statistics (Scotland) Order 2008", ISD is
obliged to publish information on those receiving Pre-Release Access ("Pre-Release Access"
refers to statistics in their final form prior to publication). The standard maximum Pre-Release
Access is five working days. Shown below are details of those receiving standard Pre-
Release Access.
Standard Pre-Release Access:
Scottish Government Health Department
NHS Board Chief Executives
NHS Board Communication leads
Early Access for Management Information
These statistics will also have been made available to those who needed access to
‘management information’, i.e. as part of the delivery of health and care:
Members of the National Cancer Quality Operational Group
Members of the National Cancer Quality Steering Group
Early Access for Quality Assurance
These statistics will also have been made available to those who needed access to help
quality assure the publication:
Members of the National Cancer Quality Operational Group
Members of the National Cancer Quality Steering Group
Regional and NHS Board Breast Cancer Clinical Leads
Network Lead Clinicians

Information Services Division
52
Appendix 6 – ISD and Official Statistics
About ISD
Scotland has some of the best health service data in the world combining high quality, consistency,
national coverage and the ability to link data to allow patient based analysis and follow up.
Information Services Division (ISD) is a business operating unit of NHS National Services
Scotland and has been in existence for over 40 years. We are an essential support service to
NHSScotland and the Scottish Government and others, responsive to the needs of
NHSScotland as the delivery of health and social care evolves.
Purpose: To deliver effective national and specialist intelligence services to improve the
health and wellbeing of people in Scotland.
Mission: Better Information, Better Decisions, Better Health
Vision: To be a valued partner in improving health and wellbeing in Scotland by providing a
world class intelligence service.
Official Statistics
Information Services Division (ISD) is the principal and authoritative source of statistics on
health and care services in Scotland. ISD is designated by legislation as a producer of
‘Official Statistics’. Our official statistics publications are produced to a high professional
standard and comply with the Code of Practice for Official Statistics. The Code of Practice is
produced and monitored by the UK Statistics Authority which is independent of Government.
Under the Code of Practice, the format, content and timing of statistics publications are the
responsibility of professional staff working within ISD.
ISD’s statistical publications are currently classified as one of the following:
• National Statistics (ie assessed by the UK Statistics Authority as complying with the Code of Practice)
• National Statistics (ie legacy, still to be assessed by the UK Statistics Authority)
• Official Statistics (ie still to be assessed by the UK Statistics Authority)
• other (not Official Statistics)
Further information on ISD’s statistics, including compliance with the Code of Practice for
Official Statistics, and on the UK Statistics Authority, is available on the ISD website.