brief communication communication abrégée
TRANSCRIPT
CJS, Vol. 43, No. 1, February 2000 57
Resection of solitary small-bowelmetastases from bronchogeniccarcinoma may be curative in the
absence of residual or other metastaticdisease.1 Although most cases of small-bowel metastases have occurred in pa-tients with advanced disease, in whomsmall-bowel resection is followed by im-minent demise,2 we report a case of iso-lated metachronous jejunal metastasesfrom a squamous cell carcinoma that wereresected for potential cure.
CASE REPORT
A 62-year-old man underwent a rightupper lobectomy for a poorly differenti-ated epidermoid carcinoma with involve-ment of the visceral pleura. The hilar re-section margin was free of carcinoma andthe hilar, interlobar and tracheobronchial-angle lymph nodes were all negative formetastases. Preoperative computed to-mography showed no evidence of spreadto the liver, adrenal glands or otherviscera. Bone scanning was negative formetastatic disease. Ten months later, he complained of
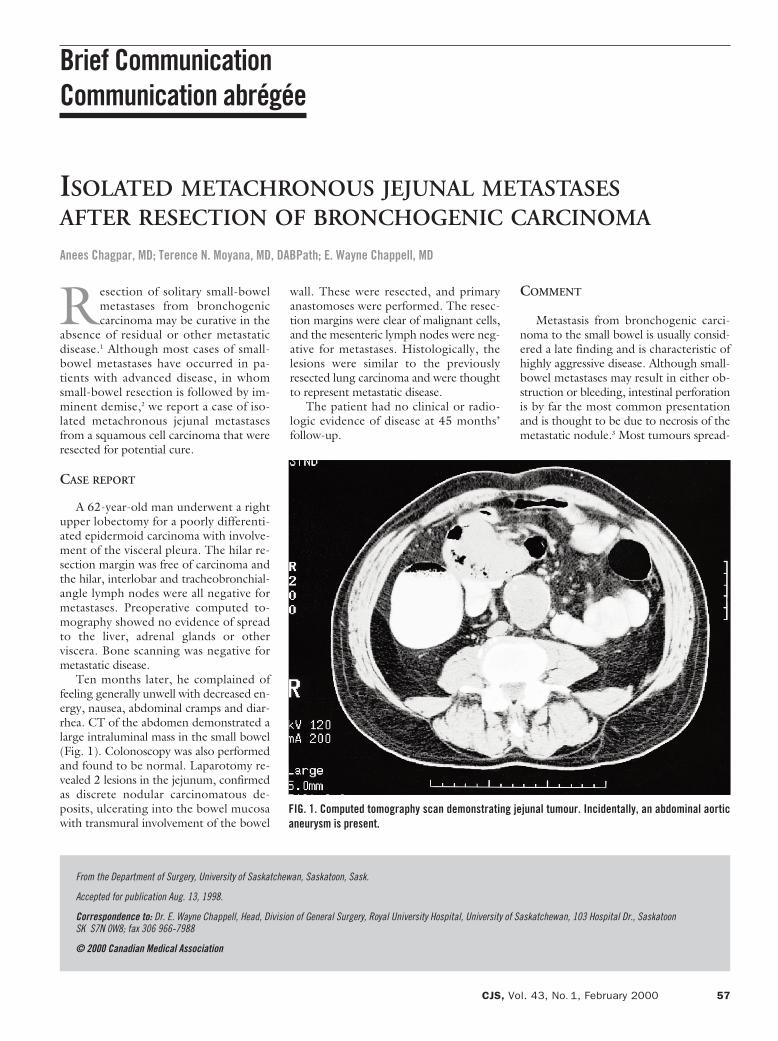
feeling generally unwell with decreased en-ergy, nausea, abdominal cramps and diar-rhea. CT of the abdomen demonstrated alarge intraluminal mass in the small bowel(Fig. 1). Colonoscopy was also performedand found to be normal. Laparotomy re-vealed 2 lesions in the jejunum, confirmedas discrete nodular carcinomatous de-posits, ulcerating into the bowel mucosawith transmural involvement of the bowel
wall. These were resected, and primaryanastomoses were performed. The resec-tion margins were clear of malignant cells,and the mesenteric lymph nodes were neg-ative for metastases. Histologically, thelesions were similar to the previouslyresected lung carcinoma and were thoughtto represent metastatic disease.The patient had no clinical or radio-
logic evidence of disease at 45 months’follow-up.
COMMENT
Metastasis from bronchogenic carci-noma to the small bowel is usually consid-ered a late finding and is characteristic ofhighly aggressive disease. Although small-bowel metastases may result in either ob-struction or bleeding, intestinal perforationis by far the most common presentationand is thought to be due to necrosis of themetastatic nodule.3 Most tumours spread-
Brief CommunicationCommunication abrégée
ISOLATED METACHRONOUS JEJUNAL METASTASESAFTER RESECTION OF BRONCHOGENIC CARCINOMA
Anees Chagpar, MD; Terence N. Moyana, MD, DABPath; E. Wayne Chappell, MD
From the Department of Surgery, University of Saskatchewan, Saskatoon, Sask.
Accepted for publication Aug. 13, 1998.
Correspondence to: Dr. E. Wayne Chappell, Head, Division of General Surgery, Royal University Hospital, University of Saskatchewan, 103 Hospital Dr., SaskatoonSK S7N 0W8; fax 306 966-7988
© 2000 Canadian Medical Association
FIG. 1. Computed tomography scan demonstrating jejunal tumour. Incidentally, an abdominal aorticaneurysm is present.
ing to the small bowel from the lung are ofhigh grade, are poorly differentiated andare non-small cell in type. In the majority of reported cases of
small-bowel metastases, the primary lungtumour was unresectable at the time ofpresentation, was accompanied by wide-spread metastatic disease or was found as aresult of the abdominal complaints. Pallia-tive radiotherapy, chemotherapy and oc-casionally palliative resection were theusual treatment modalities. It is thereforenot suprising that the prognosis in thesepatients was so poor, with most survivingless than 16 weeks after laparotomy. Other primary malignant lesions that
metastasize to the small bowel (e.g., thoseof skin, cervix, colon and ovary) have beenshown to be discrete events in which “vig-orous surgical therapy does not imply ahopeless prognosis,”4 as long as the pri-mary tumour has been adequately resectedand there are no other signs of metastasis.The evidence of this same phenomenonfor bronchogenic carcinoma is less abun-
dant. We are aware of only 2 other case re-ports of previously resected primary bron-chogenic carcinoma in which isolatedsmall-bowel metastases were subsequentlyfound and resected with intent to cure.1,5
In both of these cases, patients were aliveand well at the time of publication (5months and 8 years after laparotomy).This case report adds to the evidence thatperhaps isolated small-bowel metastasisfrom bronchogenic carcinoma, in the ab-sence of other metastatic or residual dis-ease, may have a better prognosis with re-section. This finding should thereforeprompt surgeons to pay close attention tosubtle abdominal complaints in patients inwhom a “curative” pulmonary resectionhas been performed for bronchogenic car-cinoma. As with other extracranial solitarymetastases of non-small cell carcinoma ofthe lung, aggressive treatment with resec-tion of isolated small-bowel metastaseswhen the primary tumour has been re-sected should be considered since this ap-proach may improve long-term survival.6
References
1. Richie RE, Reynolds VH, Sawyers JL. Tumormetastases to the small bowel from extra-abdominal sites. South Med J 1973; 66(12):1383-7.
2. McNeill P, Wagnan L, Neifeld J. Smallbowel metastases from primary carcinomaof the lung. Cancer 1987;8(59):1486-9.
3. Wiedemer H, Godbole M, Appavu SK.Small bowel metastases in bronchogeniccarcinoma. Ill Med J 1981;160:228-30.
4. Farmer RG, Hawk WA. Metastatic tumorsof the small bowel. Gastroenterology 1964;47:496-504.
5. Hubens G, Van Eerdeweg W, Schoofs E,Fierens H, Colpaert C, Van Marck E, et al.Massive intestinal haemorrhage due to asolitary jejunal metastasis of a primary bron-chogenic tumour. Acta Chir Belg 1992;92(4):187-90.
6. Luketich JD, Martini N, Ginsberg RJ, Rig-berg D, Burt ME. Successful treatment ofsolitary extracranial metastases from non-small cell lung cancer. Ann Thorac Surg1995;60(6):1609-11.
CHAGPAR ET AL
58 JCC, Vol. 43, No 1, février 2000
Essential readingfrom CMA Publishing Services
• CMAJ• Canadian Journal of Surgery• Clinical and Investigative Medicine • Journal of Psychiatry & Neuroscience
For information contactCMA Member Service Centre888 [email protected]