brief strategic family therapy
TRANSCRIPT

8/7/2019 Brief Strategic Family Therapy
http://slidepdf.com/reader/full/brief-strategic-family-therapy 1/12
U.S. Department of Justice
Office of Justice Programs
Office of Juvenile Justice and Delinquency Prevention
John J. Wilson, Acting Administrator
From the Administrator
Just as a child is influenced by his or
her family, the child’s family, in turn, is
affected by the culture of which it isan integral part. If we are to succeed
in preventing and combating delin-
quency, we must work to strengthen
the role of the family within the com-
munity in which it resides.
This Bulletin features a family-
strengthening strategybrief strate-
gic family therapythat integrates
theory with decades of research and
practice at the University of Miami in
an intensive, short-term, problem-
focused intervention, generally
lasting 3 months.
The Bulletin also describes the
therapy’s implementation by the
Spanish Family Guidance Center.
The Center, which was established
by the University of Miami’s School
of Medicine, serves the local His-
panic community, consisting largely
of Cuban immigrants. In adapting
brief strategic family therapy to the
needs of its clients, the Center took
into account the strengths and weak-
nesses these minority youth and
families bring to therapy, and those
special risk and protective factors
are also highlighted in these pages.
The needs of families are addressed
most effectively within the social and
cultural milieus of those families.
Brief strategic family therapy is a
time-tested approach to that end.
John J. Wilson
Acting Administrator
April 2000
Brief StrategicFamily Therapy
Michae l S. Robb ins and Jo sé Szapoczn ik
The Office of Juvenile Justice and Delin-
quency Prevention (OJJDP) is dedicated to
preventing and reversing trends of increased
delinquency and violence among adoles-
cents. These trends hav e alarmed the pub-
lic during the past decade and challenged
the juvenile justice system. It is widely ac-
cepted that increases in delinquency and
violence ove r the past decade are rooted ina number of interrelated social problems
child abuse and neglect, alcohol and drug
abuse, youth conflict and aggression, and
early sexual involvem entthat m ay origi-
nate within the family structure. The focus
of OJJDP’s Family Strengthening Series is to
provide assistance to ongoing efforts across
the country to strengthen the family unit by
discussing the effectiveness of family inter-
vention programs and providing resources
to families and com munities.
The 1970’s witnesse d a t remend ous in-
creas e in the numbe r of Hispanic adoles-
cents involved with dr ugs. In resp onse t othis pro blem, th e Univers ity of Miami (FL)
School of Medicine, Department of Psy-
chiatric and Behavioral Sciences, esta b-
lished the Spanish Family Guidance Cen-
ter in Miami to provide ser vices to the
local Hispanic com munity, which was pre-
dominately recent immigrants from Cuba.
The Center was initially funded by th e
U.S. Dep ar tme nt of Health , Educ ation, an d
Welfare, Office of Econom ic Opp or tun ity.
One of the first challenges the Spanish
Family Guidan ce Cent er’s clinical pro gram
encoun tered involved identifying and de-
veloping a culturally appropr iate and ac-
ceptable treatment intervention for Cu-
ban youth with be havior prob lems. To
understand Cuban culture and how it re-
semb led, and differed from, mainstrea m
culture, the Center’s st aff condu cted acomprehensive study on value orienta-
tions. The stud y determined that th e
Cuban comm unity expected a family-
oriented approach in which therapists
take act ive, directive, present -oriented
leaders hip roles (Szapocznik, Scopet ta,
et al., 1978).
The Center’s s econd challenge involved
developing intervent ions to help recent
immigrant Hispanic families work to-
gether to d eal with th e stress of accul-
tura tion. In th ese families, it was q uite
commo n for conflicts to e merge or inten-
sify when the children or ad olescentsbegan to beh ave in ways th at were not
cons istent with t he families’ trad itional
cultural values. Typically, these conflicts
occurred as ch ildren and adolescents as-
similated more rapidly than their parents
to th e bicultural environment in which
the y were living, and o ften involved a clash
between the American value of individual-
ism and the Hispan ic value of familism.
Such intergenerational (parent ver sus
Fam
ilyStr
engthe n i n g S e r i e s

8/7/2019 Brief Strategic Family Therapy
http://slidepdf.com/reader/full/brief-strategic-family-therapy 2/12
2
adolescent) a nd cultur al difference s often
yielded intense conflict within the family
and resulted in parents and adolescents
feeling alienated from one another.
In 1975, the Span ish Family Guidance Center
adopted struct ural family therapy (SFT) as
its core approac h, and SFT has been at the
hear t of the Center ’s effor ts to de velopinterventions for use in culturally diverse
conte xts (Szapocznik and Kurtines, 1993).
Over time, the s truc tur al approa ch of SFT
has bee n refined to meet the need s of theHispan ic comm unity in Miami. For example,
SFT uses treatment met hods th at are both
strategic (i.e., problem focused and prag-
matic) and time limited. Thus, the s tructu ral
approach has evolved into a time-limited,
family-based approach that combines bot h
structu ral and st rategic inter ventions. This
appr oach , called brief strat egic familyther apy (BSFT), has become t he mos t com-
mon intervention used b y the SpanishFamily Guidance Cente r for families tha t
include youth with beha vior p roblems.
BSFT evolved from more than 25 years o f
resea rch and p ract ice at the University of
Miami. The structural orientation of BSFT
dra ws on th e work of Minuchin (Minuch in,
1974; Minuch in an d Fish man , 1981; and
Minuch in, Ros man , and Baker, 1978), andthe stra tegic as pects of BSFT are influenced
by Haley (1976) an d Mada nes (1981). By
integrating theor y, resear ch findings, and
clinical prac tice, BSFT has been continu-
ously refined to impro ve its effectiveness
with youth with behavior prob lems.Since its modes t beginning in a small stor e-
front locat ion, the Span ish Family Guid-
ance Center has grown in response to the
needs of the minority comm unity in Mi-ami. In particular, work with youth with
behavior problems has expanded t o in-
clude minor ity families from a var iety of
backgrounds , including both Hispanic
(from the Caribbe an Islands an d Central
and South America) and African American
youth and families. To accom moda te th is
expansion, th e Center for Family Studieswas estab lishe d as an um brella organiza-
tion to se r ve inner-city minority youthand families in Miami. The m ission of the
Center for Family Stud ies is to iden tify th e
needs of minority families a nd develop
and refine culturally app ropr iate interven-
tions to meet those needs. The Center for
Family Stud ies us es BSFT to h elp ch ildre nand adolescents with conduct, delin-
quency, and other behavior-related prob-
lems, including alcohol and s ubs tance
abuse. To improve youth behavior, BSFT
attem pts to ch ange family intera ctions
and cultur al/contextual factor s tha t influ-
ence youth beh avior prob lems. BSFT is
based on the fundamental assumption
that the family is t he “bed rock” of childdevelopmen t; the family is viewed as the
primar y context in which children learn
to t hink, feel, and b eh ave. Family rela-
tions are th us believed to play a pivotal
role in the evolution of beh avior problems
and, consequently, they are a primary tar-
get for inter vention.
BSFT recognizes t hat the family itself is pa rt
of a larger s ocial system an das a ch ild is
influenced by he r or his familythe family
is influenced b y the larger soc ial syste m
in which it exists . Sens itivity to cont extual
factors begins with an und ers tanding of
the influence o f peer s, scho ols, and neigh-borhood s on the de velopment o f childre n’s
be havior pro blems . However, BSFT also
focuses on pa rents ’ relationships with
children’s peer s, schools, and neighbor-
hoods and on th e unique relationships
that p arents h ave with individuals and
syste ms o utside t he family (e.g., work or
groups s uch as Alcoholics Anonymous).
Program ObjectivesBSFT has been revised to resp ond to t he
unique strengths and weaknesses minor-
ity youth and families in Miami br ing totherap y. Several of these r isk and protec-
tive factor s are d escr ibed below.
Mitigating Risk Factors
Immigration. Many of the families ser ved
by th e Spanish Family Guidance Center
have rece ntly immigrated t o the United
States . The immigration proce ss crea tes
specific problems that m ust be ad dressed
in treatm ent. For examp le, many families
emigrate in stages; it is not unc ommon for
one pare nt, usually the mothe r, to come
to the United States alone to es tablish a
place and econom ic means for t he family
and then bring the children to th is countr y. For m any families, this p roces s is pro
tracted, and they are separ ated for many
years. Moreover, the reunification proce
often fails to m eet family members ’ expe
tations. Children are often disap pointed
when th ey arrive in the United States and
see t hat t hey are living in an impover-
ished, d angerous, inner -city commun ity.
Likewise, parents are often d isappointed
when they are confronted with angry and
emotionally detache d ch ildren. As a re -
sult, treatment often involves attem pting
to reestab lish parent-child bond s and cr
ate new family str ucture s that include thparent who was s eparate d from the famil
High con flict. Intense and persistent
conflict is a com mon cha racter istic of
families of youth with b ehavior p rob-
lems. High levels of conflict inter fere
with parents ’ ability to resolve problem
communicate effectively, nurture, and
guide the ir children. BSFT focuses on
ass ess ing the family’s con flict reso lutio
style and developing specific interven-
tions to help families n egotiate and re -
solve th eir differen ces more effectively.
Inner city. The po werful influenc e of
neighborh oods cann ot be ignored whenworking with inne r-city yout h and fami-
lies. In fact, accu mulating evidence
shows tha t the pos itive changes made in
family ther apy are often overwhelmed
by the harsh and deteriorated condit ion
of the inner city. As a re sult, the focus of
BSFT ha s e xpande d from individua l fami-
lies t o include t he re lationship b etween
families and the multiple systems that in-
fluence ch ildren. Developme nts in the
clinical model have been heavily influence

8/7/2019 Brief Strategic Family Therapy
http://slidepdf.com/reader/full/brief-strategic-family-therapy 3/12
3
by the th eore tical work of Urie Bronfen-
bren ner (1977, 1979, 1986) an d t he
ground bre aking clinical work of Scott
Henggeler and his co lleagues (Henggeler
and Borduin, 1990; Henggeler, Melton,
and Smith, 1992). In p art icular, BSFT has
expanded to include atte ntion to the rela-
tionship between families, on one hand,and s chools, peer s, juvenile justice agen-
cies, and neighborhood s, on the other.
Enhancing ProtectiveFactors
Extended families. One of the mos t effec-
tive protec tive facto rs is th e availability of
stro ng extended family networks. It is not
uncommon, for example, for t reatment to
include grandp arents, aunts, uncles, cous-
ins, or even close friends (“fictive kin”) who
grew up with the child’s parents. Although
these networks may also be s ources of
problems for the family, they a re frequentlysourc es o f strong sup por t. In BSFT, thes e
networks are often used to bolster or ser ve
the importa nt functions of the family. For
example, extend ed family membe rs are
freque ntly engaged in treatmen t to help
monitor the children while parents are at
work. At times, memb ers of the extended
family or fictive kin assume primar y lead-
ersh ip roles in the family when parent s are
unable or unwilling to p erform thes e t asks.
In mos t instanc es, BSFT seeks t o st rengthen
social connections by increasing mutual
support and decreasing tension and con-
flict b etween th e family and the extended
support network.
Family fo cus. A secon d pro tective factor
that has helped minority families in Miami
is the ir str ong se ns e of family unity. High-
lighting the need s of the family above th e
needs of individual family memb ers moti-
vates many adults to participate in inter-
vention s. In fact , the Spa nish Family Guid-
ance Center initially selected a family
approach because of the Cuban (the target
population in the 1970’s) emphasis on fam-
ily values. As th e Center rea ched out t o
many different Hispanic pop ulations in the
1980’s an d t o African Amer icans in the
1990’s, the em phas is on the impor tance of families remained consistent. Minority
groups in the United States generally place
great value on their nat ural reference group
(e.g., family, extended ne twork, or t ribe) .
Target PopulationBSFT targets children and adolescents be-
tween the ages of 8 and 17 who are display-
ing or a re at risk for d eveloping behavior
problems, including substance abuse.
BSFT has b een implemente d as a preven-
tion, early inter vention, and intervent ion
strategy for d elinquent and substance-
abusing adolescents.
Theoretical
UnderpinningsThe goa l of BSFT is to imp rove yo uth
behavior by:
x Improving family relationsh ips t hat
are presumed to be directly related
to youth beh avior prob lems.
x Improving relationships b etween th efamily and other impor tant syste ms that
influence the youth ( e.g., school, peers).
To unde rst and th e sp ecific way in which
BSFT produc es ch anges in thes e relation-
ships and sub sequent ch anges in behavior
problems, it is necessary to under stand
some of the b asic pr inciples on which BSFTis based.
Systems
BSFT ass umes that each family has its
own unique character istics and prop er-
ties that emerge and are ap parent only
when family membe rs interact. This fam-
ily “system” influences all member s o f the
family. Thus, th e family mus t be viewed as
a whole organism r ather than merely as
the co mpos ite sum of the individuals or
group s th at c omp os e it. In BSFT, this view
of the family syste m is evident in the fol-
lowing assump tions:
x The family is a s ystem with interd e-
pendent/ interrelated parts .
x The beh avior of one family membe r can
only be unde rst ood by examining the
context (i.e., family) in which it occur s.
x Interventions must be implemented at
the family level and m ust t ake into ac-
count th e complex relationships within
the family system .
Structure
BSFT also focus es on “str uctu re.” While
the co ncept o f a system is useful, onemust under stand th e system’s b asic
stru cture to recognize the mechanism
through which it operates . Thus, as
noted ab ove, the existence o f a system
explains how th e b ehaviors o f family
members are interdependent. These in-
terdep endent or linked behavioral inter-actions amon g individuals tend to recur
and create pat terns of interac tions
amo ng family me mbe rs . In BSFT, the se
repetitive patterns compos e a family
system’s struc ture. This view of structur
is evident in th e following ass umpt ions:
x Structure refers to th e repetitive pat-
terns of interactions that characterizethe family syste m.
x Repet itive intera ctions (i.e., ways fam
ily members behave with one anotherare either s uccessful or unsucces sful
in ach ieving th e goals of the family or
its individual members .
x BSFT targets repe titive p atter ns of in-
tera ction (i.e., the h abitual ways in
which family memb ers b ehave with
one another ) that are directly relatedto the youth’s behavior problems.
Strategy
BSFT believes in a s trat egic app roach th
uses pragmat ic, prob lem-focused, and
planned interventions. This strategic ap
proach emerged from an explicit focus odeveloping an inter vention that was q uic
and effective in eliminating symptoms. In
BSFT, this str ategic app roach is evident
in the following ass umpt ions:
x Inter ventions are pr actical. That is,
interventions are tailored to th e uniqu
char acteristics of families a nd a re
implemented to achieve attainable
treatment goals.
x Inter ventions are prob lem focuse d. A
problem-focused approach targets fir
those pa tterns of interactions that mo
directly influence the youth’s ps ycho-
social adjustment and ant isocial behaviors and targets one prob lem at a tim
x Interventions are well planned, meanin
that the therapist determines what see
to be the m aladaptive inter actions (i.
interactions that are directly related t
the youth’s b ehavior p roblems), dete
mines which of these might be targete
and estab lishes a plan to help the fam
ily develop more effective patt erns of
interaction.
Process Versus Content
As no ted abo ve, BSFT is prima rily con-
cerne d with ident ifying and ameliorating
patterns of interaction in the family syste
that are p resumed t o be directly related t
beh avioral sympt oms. This focus on pa t
terns of interactions is also referred t o as
“process ” focus. Rath er th an focusing sim
ply on what h app ens in th e family (e.g.,
what dad said when he yelled at the chil
dren), BSFT focus es o n ho w interactions
occur (e.g., who was involved in the con
flict, when it occurred, who resp onded t
whom, what precede d and followed the

8/7/2019 Brief Strategic Family Therapy
http://slidepdf.com/reader/full/brief-strategic-family-therapy 4/12
4
incident ). This important distinction be-
tween process (p atterns of interaction) and
content (spec ific and concrete information)
is a fundam ental conce pt of BSFT. This pro -
cess focus is evident in the following
assumptions:
x Process refers to what beh aviors are
involved in an interaction and howthey o ccur. Second arily, proces s re fers
to the mes sage that is communicated
by the nature of interactions or by th e
style of com munication, including allthat is commu nicated nonver bally,
such as emotion, tone, and the under-
lying power re lationship.
x Content refers to the s pecific and con -
crete facts used in the communication.
Content includes s uch th ings as the
reas ons th at family membe rs offer for
a given intera ction.
x BSFT is proce ss oriented at all times.
The emp has is is on ident ifying the na -ture of the inter actions in the family
and changing those interactions th at
are maladaptive.
Components ofInterventionThere are three intervention compo-
nen ts in BSFT: joining, diagnos is, and
restructuring.
Joining
Individuals from families that include youthwith b ehavior pro blems are very difficult to
engage in treatm ent. For th e pas t 15 years,
the Center’s s taff have focus ed explicitly on
family resistance and h ave developed spe -
cialized p roce dures for engaging families in
treatment. These procedures , which are
descr ibed in more detail below (see “Engag-
ing Hard-To-Reach Families” on page 8), are
based on two fundamental assumptions:
x Engagement o r joining begins from the
very first con tact with the family.
x Resistance can be und erstood in the
same way as any other pattern of
family intera ction.
In BSFT, joining occur s a t two levels. First ,
at the individual level, joining involves es-
tablishing a relationship with each partici-
pating family memb er. Secon d, at t he level
of the family, the th erap ist joins with t he
family system t o create a new ther apeutic
system. Joining thus requires bo th s ensi-
t ivi ty and an ab ili ty to respond to th e
unique cha racteristics o f individuals an d
quickly discer n th e family’s gover ning
processes.
A numb er of spe cific techniques can be
used to join the family, including m aint e-nance (e.g., supp ort ing the family’s s truc -
ture and entering the s ystem by accepting
their rules that regulate beh avior), track-
ing (e.g., using what th e family talks abo ut
(content) and h ow their interactions un-
fold (proces s) to e nter t he family sys-tem), and mimesis (e.g., matching the
temp o, mood, and s tyle of family memb erinteractions).
Diagnosis
In BSFT, diagnos is re fers to identifying inter -
actional patterns (struc ture) that a llow or
encourage problematic youth behavior. Inother words , diagnosis determines how the
nature a nd cha racter istics of family interac -
tions (how family member s beh ave with
one anot her) c ontr ibute to the family’s
failure to meet its ob jective of eliminating
youth p roblems. To derive comp lex diag-noses of the family, therapists carefully ex-
amine family interactions along five interac-tional dimensions (see the tab le on pages
6 and 7): structure, resonan ce, develop-
mental stage, identified patient , and c on-
flict resolution.
Asses sment refers to the s ystematic review
of the detailed or molecular asp ects of fam-
ily interaction to identify specific qualities
in the pa ttern s of interaction of each family
along the five dimensions p resented in the
table. In contrast, clinical formulation refersto the p roces s of integrating the informa-
tion obtained through ass essment intolarger patterns or processes that character-
ize the family’s inte rac tions . In family sys-
tems therapy, clinical formulation explains
the p atient’s pres enting symptom in rela-
tionship to t he family’s ch aract eristic pat-
tern s o f intera ction. For example, a ch ild’sacting out may be s een as resulting from a
lack of parental sup er vision and m onitoring
that, in turn, are influenced by a p oor ma ri-
tal relationship and disagreement about
parenting practices.
In ad dition to t he family interactional factors
tha t are cent ral to BSFT, individual and so-
cial factors must b e considered for a com-plete clinical formu lation. At t he individual
level, psychological factors (e.g., beliefs, atti-tude s, intelligence, and psych opat hology)
and biological factors (e.g., family predispo-
sition toward alcohol abuse or b ipolar dis-
order) must be considered when evaluating
the impact of family interactions o n th e
problems experienced by youth. Moreover,
other social systems that th e family comes
into contact with may have a pro found im-pact on t he family, and cons equently, must
be co nsidered in the clinical formu lation.
For e xample, youth intera ctions at schoo
or with peers a nd the n ature of the neigh-borhood may serve as po werful risk or pro
tective factors. In addition, one’s p arents ,
extended family, friends, or career may
serve as sources of strength or stress that
may or may not contribute to the problem
experienced by the youth.
Restructuring
As t her apists identify what a family’s p at
tern s of inter action are and h ow these fi
with individual and s ocial factor s, they
make judgments ab out the relationship be
tween t he family’s p atter n of interact ion
and th e youth’s prob lem behaviors. Basedon thes e judgments, therapists develop
specific plans for changing the family inter
actions an d individual and s ocial factor s
that a re directly related t o the child’s prob
lem beh avior. The ultimate goal of treat-
men t plans in BSFT is to ch ange familyinteractions that maintain the problems
to more effective and ada ptive intera c-tions th at e liminate th e p roblems. BSFT
therapists use a range of techniques tha
fall within th ree br oad c ategories:
x Working in th e pre sent .
x Reframing.
x Working with bound aries a nd alliance
Working in the present. While some typ e
of couns eling focu s on t he p ast , BSFT fo-
cuses p rimarily on the present interac tion
that occur between family members and
are obser vable to the therapist. For ex-ample, enactments a re a cr itical feature o
BSFT. Enactm ents encou rage, he lp, and/o
allow family membe rs t o beh ave or intera cas th ey would if the th erap ist were not
present. Very frequently, family member
will spontaneously behave in their typica
way when the y fight, interr upt , or criticiz
one a noth er. Therefore, when families be
come r igidly focuse d on s peaking to the
therap ist, the therap ist should systemati
cally redirect comm unication to encour ag
interactions between session participants
There are two reas ons for encour aging en
actments . The first is to per mit the thera-pist to obser ve problematic interactions
directly rath er th an relying on stories
about what happens when the therapist
is not pre sent . Clinical experience sh ows
that families’ stories a bout how they inte
act are o ften ver y different from their ac-
tual interactions.
The second reas on for enactme nts, and
a centr al tenet o f BSFT, is th at th e th erapist is responsible for res tructu ring (or
trans forming) intera ctions. Frequently,

8/7/2019 Brief Strategic Family Therapy
http://slidepdf.com/reader/full/brief-strategic-family-therapy 5/12
5
interactions are tr ansformed when the
ther apist allows family memb ers t o inter-
act and then intervenes in the midst of
these interactions to facilitate the occur-
rence or emergence o f a different, more
positive set of inter actions. It is importa nt
to rem embe r th at in BSFT, therap ists are
not interes ted in having the family simply“talk ab out ” beha ving different ly. Rath er,
they are inter ested in having the family
behave differently during and following
the intervention sessions.
Reframing. Perhaps one of the most inter-
esting, useful, subt le, and power ful tech-
nique s in BSFT is refra ming. Refram ing
create s a different sens e of reality; it gives
family members t he opp ortunity to per-
ceive their inter actions or s ituation from
a different pers pect ive. Reframing is a re-
structuring technique that typically doesnot cause the ther apist to lose his or her
rapp ort with the family. For t his reas on,reframing should b e use d liberally through-
out the treatment process, especially at the
beginning of treatmen t when th e ther apist
needs to br ing about changes bu t is still in
the proces s of building a working relation-
sh ip with t he family. Reframing ser ves two
extremely important functions. First, it is a
tool for changing negative and ap parently
“uncaring” emotions into positive and car -
ing intera ctions. This is ach ieved, for e x-
ample, by redefining anger and frust ration
as the b onds t hat tie a family together; the
thera pist may help a parent recognize that
his or her anger toward a child is based
on love. The oth er impor tant function isto sh ift from a blaming or cas tigating ap-
proach to developing a team s pirit that al-
lows family members to acknowledge that
they are in therapy because they care about
one ano ther. One ma jor goal of all restruc-
turing inter ventions is to create th e oppor -
tunity for t he family to be have in const ruc-
tive new ways. Tha t is, when t he family is
unable to bre ak out of its ma ladaptive inter-
actions, the the rapist’s job is to help th e
family intera ct in a n ew, more p ositive, way.
Working with boundaries and alliances.
The lives of youth who us e dr ugs are likely
to include a comp lex set of alliances th atrequire intervent ion. The a lliances bet ween
the drug user and other users and s ellers
need t o be severed, and alliances with indi-
viduals who can encour age prosocial be-
haviors need to be es tablished.
Boundaries are the social “walls” that exist
around groups of peop le who are allied with
one anothe r and that s tand between indivi-
duals and group s that are not allied with
one ano ther. Shifting boundar ies refers to
changing the p atterns of alliance. A common
situation o f drug-using youth is a s trong alli-ance with only one pare nt. The resulting
alliance may cross generational lines a nd
work against th e trad itional parental hierar-
chy. For examp le, there m ay be a st rong
bond between a youth and her or his
mother (or mother figure). Whenever theyouth is punished by the father (or father
figure) for inapprop riate be havior, theyouth may solicit sympathy and supp ort
from the “mother” to underm ine the
“fathe r’s” authority and r emove th e sanc -
tion. In a single-pare nt family, it may b e th e
grandmother who overprotects the youth
and under mines the parent’s attemp ts at
discipline. Shifting of bound aries involves:
x Creating a more solid bond bet ween
the p arents so the y will make execu-
tive decisions together.
x Removing the inappropriate parent-
child alliance and replacing it with a nappropriate alliance between both p ar-
ents or parent figures and the youth
that meets the youth’s needs for sup -
port and nurturance.
Implementation
Philosophy
BSFT is bas ed on th e assu mption that t he
familyone of the m ost import ant and influ-
ential systems in the lives of children and
adolescents provides t he foundation for
child de velopme nt. As a res ult, BSFT con-
ceptualizes and intervenes to ch ange youth
beh avior pro blems at th e family level. Al-
though BSFT also uses unique interventions
to work with individual family members (see
“One-Person Family Therapy” on page 7), it
attemp ts to include t he en tire family in
treatment. In fact, therap ists are very activin trying to engage relucta nt family mem
bers, particularly during the early phase o
therap y. The basic philosophy is that thera
pists will be able to unders tand family prob
lems and treat youth behavior problems
more effectively if they view the family’spatte rns of interac tion directly.
Although BSFT the rap ists a re ac tive and
directive, they never do what t he family
members can do for themselves. Thether apist’s goal is to m ove in and out of
family interactions, creating opportunitie
in the ses sion th at will prop el the family’s
interactions in a new, more positive direc
tion. Even in these circums tances , the
ther apist mo ves br iefly into a centra lized
role and quickly moves o ut of it. Idea lly,
when the therap ist leaves the system, thfamily will be able to resp ond pos itively t
internal and external cha llenges. Excep-tions are allowed when crises occ ur or
when situations ar ise that require expert
intervention (e.g., suicidal thoughts or be
haviors, family violence/a bus e).
A fundamental assumption of BSFT is that
families enter treatme nt with their own,
natura lly occ urring, informal n etworks,
including friends, extended family membersch ools, and work. BSFT therapists examin
thes e networks to identify potent ial prob
lems or areas o f strength on which to cap
talize in therapy. Thus, rath er th an attem pt
ing to hook family members into formal
systems, like social services, that tend t o btransient in nature, BSFT tries to improve
natura lly occurr ing relationsh ips so th efamily is more likely to mainta in pos itive
changes when the therapist (or s ocial

8/7/2019 Brief Strategic Family Therapy
http://slidepdf.com/reader/full/brief-strategic-family-therapy 6/12
6
ser vices a gency) is no longer involved
with t he family.
Length of Treatment
BSFT is a sho rt -ter m, pro blem-focus ed in-
ter vention. The average treatment includes
appr oximately 12–15 sess ions and lasts
about 3 months. For more severe cases,
such as substance-abusing adolescents, the
average number of sessions and length of
treatment may b e doub led. It is important
to n ote , however, th at BSFT is not a fixed“package.” Treatment continues until the
family achieves changes in key behavioral
criteria rath er th an until it completes a
predetermined number of sessions.
Location of Treatment
Most BSFT work with ch ildren with be hav-
ior prob lems occu rs in the office. How-
ever, some treatment of substance-abusing
adolescents and t heir families is c on-
ducted in the home or community. The
movement to “home-based” treatment re-
sults from many factors; therapists m ust
deal with families tha t are h ighly disorga-nized and/or u nmotivated to attend treat-
ments and families that lack the necessar y
resources (e.g., transp ortat ion, money) to
make it t o t he office. BSFT does n ot b elieve
that h ome- or community-based treatment
is required for all youth with beh avior
problems, but finds t hat it may be re -quired for more severe cases . Therapists
should never allow the location of treat-
ment (e.g., home, office, schoolyard) to
become an obstacle to treatment.
Development of aCulturally SpecificFamily ApproachApplying BSFT to Hispanic families revealed
how profoundly the p rocess of immigration
and a cculturat ion could affect t he family
and eac h mem ber. To meet th is challenge,
an inter vention was s pecifically designed toaddress the special stressors and clinical
prob lems faced by th is population.
Bicultural EffectivenessTraining
The Center for Family Studies d eveloped t he
bicultural effectiveness training inter vention
to enhance b icultura l skills in all family mem-
ber s. Bicultural e ffectiveness training is
specifically des igned to a meliorate the
acculturation-related stress es confronted
by two-generation immigrant families
(Szapocznik et al., 1984).
A clinical t rial1 investigated the relative effe
tiveness of bicultura l effectiveness training
in comp ariso n with BSFT (Szapocznik,
Santisteban, et al., 1986b) in improving be-
havior problems in early adolescence and
family functioning. (Drug-abusing adoles-
cents were excluded from this s tudy becau
they were considered beyond th e reach of
the intervention.) The results of this study
indicated tha t bicultural effectiveness t rain
ing was a s effective as str uctur al family
ther apy in improving adolescent and family
functioning. These findings suggested that
bicultural effectiveness training could ac-
complish the goals of family therapy whilefocusing on the cultural content that made
the t herapy attr active to Hispanic families.
Family Effectiveness Trainin
Subseq uent ly, BSFT and bicultur al effec-
tiveness tr aining were combined into a
Dimensions of Family Functioning* Addressed in Brief Strategic Family Therapy
Hierarchy/Leadership
One parent is more active than t heother.
Child is more p owerful than t he pa rents.
Behavior Control
Parent s are not e ngaging in beh avior
control when needed or are engaging
in ineffective beha vior con trol (e.g.,
inappropriate consequ ences, lack of
followthrough, unclear expectations,
inconsistency, or excess emotion).
Guidance/Nurturance
Parents do not nur ture children.
Parents a re poor role mode ls (e.g.,engaged in illegal activity, substance
abus e, or violence).
Spousal Alliance
Marital relationship is poo r (e.g., high
conflict or d isengagement).
Enmeshment
Emotional, psych ological, or p hysical
boundaries between family members
are exces sively close.
Disengagement
Emotional, psych ological, or p hysical
boundaries between family members
are excess ively distan t.
Structure Resonance
Executive Subsystem
Decisionmaking subsys tem is abs ent.
Sibling Subsystem
Relationship bet ween siblings is po or
(e.g., high conflict or disengagement).
Triangulation
Child is s tuck in the middle of a
conflict between ad ults.
Communication
Family lacks direct verbal co mmunica-
tion or us es ineffective commu nication
(e.g., vagueness , ser monizing, or
excess emotion).
One family memb er ser ves as a
switchboard o perator or gatekeeper.
* Examples of problems in family interaction are listed under each of the five dimensions.
1 This stud y was funded b y National Institut e of Ment
Health (NIMH) gr ant #MN31226.

8/7/2019 Brief Strategic Family Therapy
http://slidepdf.com/reader/full/brief-strategic-family-therapy 7/12
7
Parenting
Parent is immature.
Children
Child is trea ted a s/ac ts to o young (e.g.,
overly restricted, low requireme nt/
opportunity for responsible behavior,
or no negotiation allowed).
Child is trea ted a s/ac ts to o old (e.g.,
overloaded with ad ult tasks or exhibits
paren tlike behavior).
Extend ed Family
Extended family usur ps p arenta l power
or trea ts the p arent like a child.
Negativity
Family membe rs a re critical about andnegative toward the ident ified patient.
Centrality
Identified p atient is almos t always th e
centr al topic of convers ation.
Family membe rs ar e organized around
the identified patient and her /his
problem behaviors.
Support
Family members protect or suppor t
identified p atient.
Denial/Avoidance
Family memb ers d eny or avoidconflict.
Diffusion
Family members jump from conflict to
conflict withou t ach ieving any dep th
regarding one particular issue.
Emergence Without Resolution
Family engages in an indept h d iscus-
sion abou t a par ticular conflict but is
not able to resolve the problem.
Negativity/Conflict
Family inter actions are op enly critical
or hostile.
Developmental Stage Identified Patient Conflict Resolution
package called family effectiveness training
(Szapocznik, Santisteban, et al., 1986a). A
study2 investigated t he value of family
effectivenes s tr aining as a preven tion/
inter vention st rat egy for Hisp anic familiesof children ages 6–11 who pre sent ed emo -
tional and b ehavioral problems (Szapocznik,
Santiste ban, et al., 1989). The r esults of this
stud y indicated t hat families in the family
effectiveness training treatment group
showed significantly greater improvement
than did control families on measures
of family funct ioning, prob lem be haviors,
and child self-concept. Thus, the interven-
tion was able to improve both child
and family funct ioning. The improvem ents
were s till in effect at 6-mont h followup.
Multicultural EffectivenessTraining
Recently, the cultural co ntext in Miami has
becom e more comp lex. When bicultural
effectiveness training and family effective-
ness training were developed in the 1970’s,
the targeted Cuban-born families lived in a
cultural context that was dominated by
Cuban immigrants and Caucas ian Ameri-
can s. However, by th e 1990’s, Miami in-
cluded Cuban Americans , Cuban immi-
grants , Caucas ian Amer icans, LatinAmericans from n early all countries in
the Western Hemisphere, African Ameri-
cans , and Haitian immigrant s. In resp onse
to these changes , the bicultura l effec-
tiveness training intervention was rede-
signed into th e multicultura l effective-
nes s tr aining (Mancilla and Szapocznik,
1994) program that helps non-Cuban
Hispanic paren ts understand the com-
plex cultural conte xt in which they live.
In multicultura l effectivenes s tr aining, the
cha llenges faced by non-Cuba n Hispan ic
families who find t hem selves in a cu lture
tha t is h eavily influenced by Cuban Ameri-
cans are considered for the first time.
One-Person FamilyTherapyEngaging the who le family in tre atment is
one of the mos t challenging aspec ts of
working with youth with be havior prob lems
and their families. Thus, developing a p ro-cedure that can ach ieve the goals of family
ther apy without h aving the whole family
prese nt was an impor tant cha llenge.
To meet t his challenge, it was neces sar y to
question some b asic theoretical assump-
tions of conventional family system s p rac-
tice. Family systems th eory pos tulates th a
the youth’s beha vior prob lems are a symp
tom of flawed patterns of family interactio
As s uch, interventions must change family
interactions that produce problem beh av-
iors in the child. Conventional family sys
tems theorists assume that to change these
interactions, the e ntire family must be
prese nt in ther apy. Thus, the c hallenge in-
volved developing an approach, One-Perso
Family Therap y, that s eeks to change fami
intera ctions wh ile working with o nly on
per son ( Szapoc znik, Kurt ines, et a l.,
1990; Szapocznik and Kurtines, 1989).
One-pers on family ther apy app lies th e pr i
ciple of complementarity, which suggests
that a cha nge in the beh avior of one family
membe r will lead to corresp onding change
in the beh avior of other family member s.
One-pers on family therapy us es th is prin-
ciple d eliberat ely and s trate gically to direc
the identified patient to ch ange his or
her beha vior in ways tha t will lead t o2 This study was funded b y National Institut e on Drug
Abuse (NIDA) gran t #1E0702694.

8/7/2019 Brief Strategic Family Therapy
http://slidepdf.com/reader/full/brief-strategic-family-therapy 8/12
8
adjus tments in the b ehavior of other family
members toward him or h er.
A clinical trial3 examined the effectiveness
of one-pers on family ther apy, comparingthe entire family format with the one-person
format of BSFT (Szapoc znik, Kur tines , et
al., 1983, 1986). Both con ditions were d e-
signed to us e the BSFT frame work so th atonly the nu mber of people would d iffer.
Results indicated that one-per son family
ther apy was as effective as the group for-
mat not only in improving behavior andreducing drug abuse in the youth, but
also in impr oving and m aintaining signifi-
cant improvements in family functioning.
The results of this stud y demonstrated
that it is po ssible to c hange family inter-
actions even when th e whole family is not
present at most ses sions. It is important
to not e, however, that one-person familyther apy was mos t effective when it was
implemented b y expert BSFT therap ists.To implement one-person family therap y,
ther apists m ust b e proficient with family
and individual BSFT technique s. One-
person t echniques are very complex and
sophisticated and thus require a therap ist
with exten sive training and experience in
changing family inter actions.
Engaging Hard-To-Reach FamiliesAlthough it is possible to conduct family
thera py through one p erson , getting indi-
viduals to begin treatment co ntinues to be aproblem. For example, in the clinical trial
discusse d a bove, only 250 of approximately
650 families who met intake criteria on the
basis of a telepho ne screen ing began the
intake process. Of this number, 145 com-
pleted the intake proced ure and on ly 72
completed treatment. Clearly, a very large
propor tion of families who initially seek
treatment never participate in therapy.
Strategic Structural SystemsEngagement
Strate gic struc tural systems en gagement
was de veloped to more effectively engagedrug abus ers and their families in treatment
(Szapo czn ik, Perez-Vidal, et al., 1990;
Szapocznik and Kurtines , 1989). It is ba sed
on the p remise that resistance to change
within the family results from two systems
prop er ties. First , the family is a self-
regulatory systemthat is, the family will
attemp t to maintain struct ural equilibrium
(status quo) which, in the case of drug-
abus ing youth with behavior prob lems, can
be a ccomplished by avoiding therapy. Sec-
ond, while the pre senting symptom may be
drug ab use, the initial obst acle to cha nge is
resistance to treatment. The same struc-
tur al principles that ap ply to family
functioning and t reatment also apply to
und ers tand ing and hand ling the family’s
resistance to treatment (Szapocznik,
Per ez-Vida l, et a l., 1990). The solution to
overcoming the undes irable “symptom ” of
resistance is to r estr ucture th e family’s pa t-terns of interaction that permit the symp-tom of resistance to cont inue to exist. It is
here th at one-pers on family ther apy tech-
niques become useful because the pers on
requesting help becomes the person
through whom ther apy can work to im-
prove the family’s p attern of intera ction.
Having accomp lished the first phas e of
the th erapeutic process in which resis-tance h as been overc ome and th e family,
including the drug-abus ing youth , have
agreed to p art icipate in therapy, the
ther apist may sh ift the focus of the inter-
vention toward the r emoval of beh avior
problems and drug abuse.
Clinical work suggests t hat t he pa ttern s
of interaction that permitted the symp-
toms to exist may be the same patt erns
of inter action th at keep the families from
ente ring trea tmen t. Hence, to have the
oppor tunity to intervene in these h ard-to-
reach families, the therap ist using strate-
gic struct ural systems engagement must
begin the intervention with th e first phone
call rather th an th e first office session.
To tes t th e effectiveness of strategic struc
tural system s engagement in engaging an
retaining Hispanic families with drug-
abusing youth in treatm ent, a major clini
cal trial4 was con ducted (Szapocznik,
Per ez-Vidal, et al., 1988). In t his s tu dy,strate gic struct ural systems engagement
was comp ared to an engagement-as-usual
cont rol condition. Clients in the contr ol
condition were approac hed in a way that
resembled as closely as p ossible the kind
of engagement that usually takes place in
outpatient center s. There were two basicfindings from th e st udy (Szapocznik, PereVidal, et al., 1988). Firs t, as figure 1 sh ow
the e ffects of the experimenta l condition
were dram atic. More tha n 57 perce nt of
the families in the engagement-as-usual
condition failed to par ticipate in treat-
ment. In contr ast, on ly 7.15 percent (fou
families) in the st rate gic stru ctur al sys-
tems e ngagement cond ition failed to participate in treatm ent. The differences in
the ret ention rates were also dr amatic. I
the engagement-as-usual cond ition, 41
percent of cases did not comp lete treat-
ment; whereas, in the t reatment condition
17 percen t of cases d id not complete
treat ment. Thus, of all cases ass igned to
ther apy, 25 percen t in the e ngagement-as-usual condition and 77 perce nt in the
strategic structural systems engagement
condition were succes sfully comp leted.
For families that co mpleted t reatme nt in
both conditions, behavioral improvemen
4 This st udy wa s funde d b y NIDA grant #DA2059.
Percentage of Families
0
20
40
60
80
100
Engagement
Engagement-as-Usual Control Group
Strategic Structural Systems Engagement Experimental Group
Retention
Figure 1: Differential Engagement and Retention Rates for Strategic
Structural Systems Engagement Experimental Group andEngagement-as-Usual Control Group
3 This st udy wa s funde d b y NIDA grant #DA0322.
8/7/2019 Brief Strategic Family Therapy
http://slidepdf.com/reader/full/brief-strategic-family-therapy 9/12
9
by adoles cent s were highly significant an d
these improvements were not significantly
different across th e engagement conditions.
The critical distinction between th e con-
ditions was in the rates o f par ticipation
and completion.
A sec ond m ajor finding of the p roject
(Szapoczn ik et al., 1988) was t he ide ntifi-cation of a numbe r of resistant family
types and the d evelopment of interven-
tion st rategies for e ngaging the se families
(Szapocznik and Kurtines, 1989).
Replication Study
An ad ditional study5 was des igned t o repli-
cate th ese findings and to further explore
the elements of effective interventions
(Santisteb an e t al., 1996). This st udy, which
included a large multicultural s ample, dem-
onstr ated t he overall effectiveness of the
specialized engagement inter ventions dis-
cussed abo ve. Significant d ifferences inrates of engagement were found between
the treatment group and the control group.
In the treatme nt group, 81 percent of the
families were successfully brought intotreatme nt. In contr ast, 60 percent of the
families ass igned to th e two c ontrol groups
were succes sfully brought into treat ment.
In addition to inves tigating the over all effec-
tiveness of the specialized engagement
intervention, the st udy also investigated
the influence o f culture/e thnicity on the
multicultura l Hispanic samp le. The d ata
suggested var ying rates of engagement
acros s Hispa nic groups. Among the n on-Cuban Hispanics (primarily Nicaraguan, but
also including Colombian, Puerto Rican,
Peruvian, and Mexican) as signed to the
treatment group, the rate of intervention
failure was extrem ely low (3 percen t). Fully
97 percent of the n on-Cuban Hisp anic fami-
lies were successfully treated. In contrast,
among the Cuban Hispanic sample ass igned
to the treat ment group, the rate of inter ven-
tion failure was relatively high at 36 percent ,
with 64 per cent o f the Cuba n Hispan ic
families succe ssfully treat ed.
Comparing StructuralFamily Therapy WithOther Types of TherapyEarlier research concentrated on the de-
velopment, refinemen t, and tes ting of
BSFT theor y and s trat egies. The next
challenge was to com pare th e relative
effect ivenes s of BSFT with t hat of othe r
widely used clinical interventions. Two
such studies are des cribed below.
BSFT Versus IndividualPsychodynamic ChildTherapy
The first stud y6 compare d th e effective-
ness of a str uctur al family ther apy group
(Minuc hin, 1974; Minuch in and Fish man ,
1981) with a n individual ch ild th erap y
group and a recr eational activity contro l
group for children with beha vior prob-
lems. In ad dition, this stu dy investigated
the mechanisms for ch ange used by each
type of ther apy. Both t heore tical ap-
proach es assu me underlying causes of
symptoms an d try to eliminate or reduce
symptoms. However, each form of therapy
uses a different app roach to reducing
symptoms . The individual child a pproach
postulates that the child’s internal (i.e.,
emotional, cognitive) functioning needs tobe mod ified to eliminate the s ymptoms.
BSFT, on the oth er ha nd, post ulates th at
family interactions need to be modified
to eliminate the symptoms. Because of
these important theoretical differences,
this stud y explored th e impact of each
form of thera py on child psychod ynamic
functioning and family interactions.
The analysis revealed se veral impor tant
findings. First, memb ers o f the rec reationa l
activity (contro l) group were significant ly
more likely to drop out th an member s of
the two treatm ent conditions, with more
than two-thirds o f dropouts belonging tothe c ontrol group. Second, th e two forms
of thera py were eq ually effective in reduc
ing behavior and em otional problems.
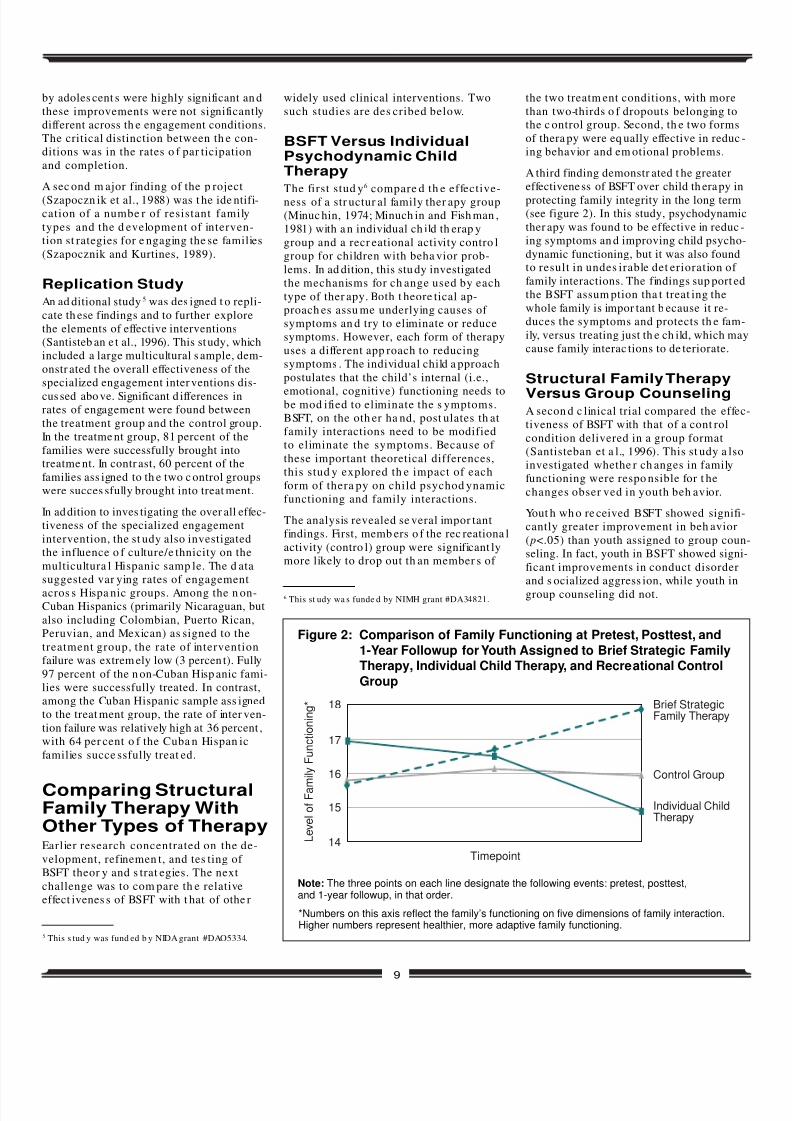
A third finding demonstr ated t he greater
effectiveness of BSFT over child th erapy in
protecting family integrity in the long term(see figure 2). In this study, psychodynami
ther apy was found to be effective in reduc
ing symptoms an d improving child psycho
dynamic functioning, but it was also foundto result in undes irable det erioration of
family interactions. The findings sup port e
the BSFT assum ption tha t treat ing the
whole family is impor tant b ecause it re-
duces the symptoms and protects th e fam
ily, versus treating just th e ch ild, which ma
cause family interac tions to de teriorate.
Structural Family Therapy
Versus Group CounselingA secon d c linical trial compared the effe
tiveness of BSFT with that of a cont rol
condition delivered in a group format
(Santisteban et a l., 1996). This st udy a lso
investigated whethe r ch anges in family
functioning were respo nsible for t he
changes obser ved in youth beh avior.
Yout h wh o re ceived BSFT showed signifi
cantly greater improvement in beh avior
(p<.05) than youth assigned to group cou
seling. In fact, youth in BSFT showed sign
ficant improvements in conduct disorder
and s ocialized aggress ion, while youth in
group counseling did not.
Figure 2: Comparison of Family Functioning at Pretest, Posttest, and
1-Year Followup for Youth Assigned to Brief Strategic FamilyTherapy, Individual Child Therapy, and Recreational Control
Group
Note: The three points on each line designate the following events: pretest, posttest,and 1-year followup, in that order.
5 This s tud y was fund ed b y NIDA grant #DAO5334.
6 This st udy wa s funde d by NIMH grant #DA34821.
Level of Fam
ily Functioning*
15
16
17
18
Timepoint
Brief StrategicFamily Therapy
Control Group
Individual ChildTherapy
14
*Numbers on this axis reflect the family’s functioning on five dimensions of family interaction.Higher numbers represent healthier, more adaptive family functioning.

8/7/2019 Brief Strategic Family Therapy
http://slidepdf.com/reader/full/brief-strategic-family-therapy 10/12
10
A Structural Approachto Changing the SocialContext of FamiliesAs th e need s of families ch ange, the
the oret ical and clinical work of the Cen-
ter for Family Studies continues to
evolve. The Center h as expand ed andadjusted its interventions in response to
dec lining inner -city social cond itions, the
multiple prob lems faced by m inority
families, and the complex contextual fac-
tors t hat affect beh avior problems. The
Center is developing a struct ural ap-
proach for ch anging the social context of
families th at wor ks mor e effectively with
minority youth with beh avior pr oblems
and their families.
Theoretical Background
The Center for Family Stud ies us es
the theoretical work of Bronfenbrenner(1977, 1979, 1986) and the multisystemic,
ser vice-oriented approa ch o f Henggeler a nd
colleagues ( Henggeler an d Borduin, 1990;
Henggeler, Melton , and Smith, 1992).
Bronfenbrenner examined the complexity
of contexts, espe cially the re lationships
between various systems th at affect an
individual. In do ing so, he iden tified a nd
defined “microsystems” as those systems
that h ave direct contact with th e individual.
For a child, microsys tems include the family,
scho ol, and pe ers . He defined “mesos ys-
tems” as those systems that occur when
microsyste ms intera ct. One example of a
mesosystem occurs when the parents and
scho ol collaborat e on a child’s educ ation.
Another example of a mes osystem occur s
when parents and peer s interact (e.g., when
parents organize and sup ervise peer a ctivi-
ties). “Exosystem s” are defined a s th ose
system s that affect family memb ers an d,
throu gh their impac t on family memb ers,
affect the child. Examples of exosyst ems
are a mother ’s workplace or h er natural
suppor t network.
Bronfenbrenner’s theor y highlights the
pivotal role of cont ext in th e life of a
child and her o r his family memb ers.
Moreover, this t heor y helps to explain
how culture influences all other social
contexts and provides a framework for
developing culturally s ensitive interven-
tions that take into account the comp lex
influence that cultural factors have on
minority families.
Most of the cur rent work at the Center
for Family Stud ies reflects an increas ing
under stand ing of ecosyste mic influences
on youth beha vior p roblems. In fact,
several ongoing ecosystemic prevention
and intervention projects are b eingimplemented in schools and neighbor -
hood s to addre ss ch ildren’s beh avior
pro blems . In place of a review of each of
these p rograms, one program th at exem-
plifies the e cosystem ic philosop hy is de-
scribed below.The Family Alliance Project. 7 The Fam-
ily Alliance Pro ject s tud y is invest igat-
ing the e ffectiveness of ecosys temic
family thera py compa red with tra di-tional family ther apy and a co mmun ity
control group. The experimental inter-
vention, structur al ecosystems ther apy,
organizes the life context of the dru g-
abu sing youth using Bronfenbre nner ’s
social ecology framework and the theo-
retical p rinciples o f BSFTthat is, p at-
terns of interaction are examined withinand o uts ide the family. Stru ctur al eco-
systems therap y includes a full dose of BSFT (e.g., alliance , hiera rch y, com mu ni-
cation flow, personal and subsystem
boundar ies, developmental s tage, iden-
tified pa tient, conflict re solution s tyle,
and abilities). However, interven tions go
beyond t he family to t arget other cri t i-
cal youth intera ctions. In par ticular, the
youth’s relationships with school au-
thori t ies and p rosocial versus antisocial
peers are examined. At the mesosystem
levels, the relat ionships between pa r-
ents and s chool, parents and t heir
children’s peers , and parents and the
juvenile just ice system are cons idered.
At th is mesosyste m level, the extent towhich the different system s sup port one
anothe r, or are in co nflict with one an-
oth er, is cr itical. For e xample, in the
parents -peers meso system, parents may
know the peer s, organize super vised
peer a ctivi t ies, and know the parents of
their ch ild’s p eers. Parents may par t ici-
pate in community organizations that
provide organized, super vised peer
activities.
Results of the inter ventions suggest that
i t is possible to a ffect youth conduct
problems at home and school by correct-
ing patterns of inter action in the familyand sc hool microsystems a nd the family-
school mesosystem; reducing youth drug
abuse also requires improving inter-
actions in the p eer microsystem and
family-peer meso syste m.
ConclusionIn t he evolution of BSFT, the Center for Fam
ily Studies h as sou ght to integrate th eor
app lication, and research . The Center ’s wor
began in the 1970’s to addres s an issue of
growing concern: promoting culturally
competent therapists and therapies to ad
dress b ehavior and drug abuse problems
amon g Miami’s Hispanic youth. Since th e
the Center has ach ieved important b reak
throughs in assessment, engagement, trea
ment, and p revention, which have provide
a solid founda tion from which to pur sue ne
advanc es in th e field. Refineme nt of str uc
tur al family the or y stra tegies and goals in
BSFT, in turn , enab led th e Center to m odif
these s trategies to achieve the same goal
without h aving the ent ire family in th erap
thus making one-person family therap y pos
sible. Changing family intera ctions by wor
ing primar ily with one person led to a break
thro ugh in e ngaging ha rd-to-reach familiein treatment.
The wor k of th e Center for Family Stud ie
will help ther apists de velop new strate-
gies t o su ppor t minor ity families. As th e
nee ds of families ch ange, work in the fiel
needs to continue to evolve to address
the multiple p roblems minority families
will continue to confront. The Center op e
ates under the assump tion that “it takes
village to r aise a c hild.” It is nec essa ry
bot h to create a “village,” or comm unity,
that can support healthy child develop-
ment and to mod ify policies an d s ystems
that provide ser vices to the community.Bronfenbrenner (1979) wrote, “Seldom is
atten tion paid to the pers on’s beha vior in
more than one setting or t o th e way in
which relations b etween se ttings can af
fect what hap pen s within them” (p. 18).
He su ggested t hat an individual’s en viron
ment is compos ed of a complex set of
nested struc tures. Scientists involved in
intervention must cons ider the social and
cultural context in which treate d families
live. The Center for Family Stud ies’ devel-
opment of theory, research, and ser vices
within the com plex community is bas ed
on th is priority.
ReferencesBronfenbre nne r, U. 1977. Toward an ex-
per imental ecology of human develop-ment. American Psychologist 32:513–531.
Bronfenbre nne r, U. 1979. The Ecology of
Human Development. Cambridge, MA:
Harvard University Press.
7 This study was or iginally funded as a t reatmen t de-
velopment p roject by Center for Substance Abuse
Treatment grant #1 HD7 TI00417; it is currently funded
by NIDA grant #1 RO1 DA10574.

8/7/2019 Brief Strategic Family Therapy
http://slidepdf.com/reader/full/brief-strategic-family-therapy 11/12
11
Bronfenbre nne r, U. 1986. Ecology of t he
family as a co ntext for human develop-
ment: Research perspectives. Develop-
mental Psychology 22(6):723–742.
Haley, J. 1976. Problem -Solving Therapy.
San Franc isco, CA: Joss ey-Bass.
Henggeler, S.W., an d Bordu in, C.M. 1990.Family Therapy and Beyond: A Multi-
systemic Approach to Treating the Be-
havior Problems of Children and Adoles-
cents. Pac ific Grove, CA: Brooks /Cole.
Henggeler, S.W., Melton , G.B., and Smith ,
L.A. 1992. Family p res er vation using
multisystemic th erap y: An e ffective alter -
native to incarcer ating serious juvenile
offenders. Journal of Consulting and Clini-
cal Psychology 60:953–961.
Madanes, C. 1981. Strategic Family
Therapy. San Francisc o, CA: Joss ey-Bass.
Mancilla, Y., and Szapo czn ik, J. 1994. AManual for a Community Based, Multifam-
ily Strategic Structural System s Interven tion
for Strengthen ing Hispanic Imm igrant Fami-
lies of Behavior Problem Adolescents at
Risk for Gang Involvement. Technical Re-
port. Miami, FL: University of Miami,
Spanish Family Guidan ce Cente r.
Minuch in, S. 1974. Families and Family
Therapy. Cambr idge, MA: Har vard Univer-
sity Press.
Minuchin, S., and Fishman, H.C. 1981.
Family Therapy Techniques. Cambridge,
MA: Har vard Univers ity Pres s.Minuch in, S., Rosma n, B.L., and Baker, L.
1978. Psychosomatic Families: Anorexia
Nervosa in Context. Cambridge, MA:
Harvard University Press.
Santiste ban , D.A., Szapo cznik, J., Perez-
Vidal, A., Kurtines, W.M., Murray, E.J., and
LaPer riere , A. 1996. Engaging b eh avior
problem drug abusing youth and th eir
families into treatment: An investigation
of the efficacy of spe cialized e ngagement
interventions and factors that contr ibute
to differential effectiveness. Journal o f
Family Psychology 10(1):35–44.
Szapo czn ik, J., and Kurt ines , W.M. 1989.
Breakthroughs in Family Treatment. NewYor k, NY: Spr inge r.
Szapo czn ik, J., and Kurt ines , W.M. 1993.
Family psychology and cultural diversity:Opportunities for theory, research and
application. American Psychologist
48(4):400–407.
Szapocznik, J., Kurtines, W.M., Foote, F.,
Perez-Vidal, A., and Hervis, O.E. 1983.
Conjoint versus one person family
therap y: Some evidence for the effect ive-
nes s o f conducting family therap y through
one person. Journal of Consulting and Clini-
cal Psychology 51:889–899.
Szapo czn ik, J., Kur tine s, W.M., Foote, F.,
Per ez-Vida l, A., and Hervis , O.E. 1986.
Conjoint versus o ne per son family
ther apy: Furth er evidence for th e effec-
tiveness o f conducting family ther apy
through one person. Journal of Consulting
and Clinical Psychology 54:395–397.
Szapocznik, J., Kurtines, W.M., Perez-
Vidal, A., Her vis, O.E., and Foote , F. 1990.
One per son family therap y. In Handbook
of Brief Psychotherapies, edite d b y R.A.
Wells an d V.A. Giane tt i. New Yor k, NY:
Plenum , pp . 493–510.
Szapocznik, J., Perez-Vidal, A., Brickman,
A.L., Foote, F.H., Sant ist eb an , D.A., Her vis,
O.E., and Kur tine s, W.H. 1988. Engaging
adolescent drug abusers and their fami-lies into treat ment: A str ategic struct ural
systems approach. Journal of Consulting
and Clinical Psychology 56: 552–557.
Szapo czn ik, J., Per ez-Vida l, A., Her vis,
O.E., Brickma n, A.L., an d Kur tine s, W.M.
1990. Inno vations in Family Ther apy:
Overcoming Resistan ce to Treatment .
Handbook of Brief Psychotherapy, edited
by R.A. Wells and V.A. Gianetti. New York,
NY: Plenu m, p p. 93–114.
Szapocznik, J., Rio, A.T., Murray, E.J.,
Cohen, R., Scope tt a, M.A., Rivas -Vas qu ezA., Her vis, O.E., Posa da , V., and Kur tine s
W.M. 1989. Stru ctu ral family vers us ps y-
chodynamic child therapy for problem-
atic Hispa nic boys. Journal of Consulting
and Clinical Psychology 57(5):571–578.
Szap ocznik, J., Sant isteb an, D., Kur tines ,W.M., Perez-Vidal, A., and Hervis, O.E.
1984. Bicultur al Effectivenes s Training
(BET): A treatm ent intervent ion for en-
hancing intercultural adjustment. His-
panic Journal of Behavioral Sciences
6(4):317–344.
Szapo czn ik, J., San tist eb an , D., Rio, A.T.,
Per ez-Vidal, A., and Kur tine s, W.M. 1986a
Family Effectivenes s Tra ining for Hisp an
families: Strategic Structural Systems In-
ter vention for th e Prevention of Drug
Abuse. In Cross Cultural Training for Men
tal Health Profession als, edite d b y H.P.
Lefley and P.B. Pedersen. Springfield, IL:Char les C. Thomas .
Szapoc znik, J., Santist eban, D., Rio, A.T.,
Pere z-Vidal, A., Kur tines, W.M., and Hervis
O.E. 1986b. Bicultura l effectiveness trainin
(BET): An int er vention mod ality for familie
experiencing intergenerat ional/intercultur
conflict. Hispanic Journal of Behavioral
Sciences 8(4):303–330.
Szapo czn ik, J., San tist eb an , D., Rio, A.T.,
Per ez-Vidal, A., and Kur tine s, W.M. 1989.
Family effectiveness training: An interve
tion to prevent p roblem beh aviors in His
panic adolescents. Hispan ic Journal of Behavioral Sciences 11:4–27.
Szap ocznik, J., Scopet ta, M.A., Aran alde,
M.A., and Kur tine s, W.M. 1978. Cuban
value s truct ure: Clinical implications.
Journal of Consulting and Clinical Psychol
ogy 46(5):961–970.
Acknowledgments
This Bulletin was written by Michael S. Robbins, Ph.D., Research AssistantProfessor, and José Szapocznik, Ph.D., Professor and Director, Center for Family
Studies, Affiliation University of Miami School of Medicine, Department of
Psychiatry and Behavioral Sciences.
Photograph page 2 copyright © 1999 Artville; photograph page 5 copyright © 1999
PhotoDisc, Inc.
Points of view or op inions expres sed in this
document are those of the authors and do no
neces sarily represent the official position or
policies o f OJJDP or t he U.S. Depa rtm ent of
Justice.
The Office of Juvenile Justice and Delin
quency Prevention is a component of the Of
fice of Justice Programs, which also includes
the Bureau of Justice Assistance, the Bureau
of Justice Statistics, the National Institute of
Justice, an d the Office for Victims o f Crime.

8/7/2019 Brief Strategic Family Therapy
http://slidepdf.com/reader/full/brief-strategic-family-therapy 12/12
PRESORTED STANDAR
POSTAGE & FEES PAID
DOJ/OJJDP
PERMIT NO. G–91
NCJ 179285Bulletin
U.S. Department of Justice
Office of Justice Programs
Office of Juvenile Justice and Delinquency Prevention
Washington, DC 20531
Official Business
Penalty for Private Use $300