bringing up baby - key concerns - american college of ... · acofp intensive board review you are...
TRANSCRIPT

The American College of Osteopathic Family Physicians is accredited by the American Osteopathic Association Council to sponsor continuing medical education forosteopathic physicians.
The American College of Osteopathic Family Physicians designates the lectures and workshops for Category 1-A credits on an hour-for-hour basis, pending approval bythe AOA CCME, ACOFP is not responsible for the content.
I N N O V A T I V E • C O M P R E H E N S I V E • H A N D S - O N
INTENSIVE UPDATE& BOARD REVIEW
AUGUST 24 - 26, 2018Loews Chicago O’Hare Hotel
Rosemont, IL
Bringing Up Baby - Key Concerns
Sarah Hall, DO


8/3/2018
1
Sarah Hall, D.O.
August 24, 2018
ACOFP Intensive Board Review
You are seeing a newborn at 72 hours for an initial newborn visit in your office. The baby was born at 37 weeks after a prolonged spontaneous vaginal delivery and is exclusivelybreastfeeding. APGARS were 7/9. Discharge papers indicate that at 24 hours, the baby’s Total bilirubin level was 8 mg/dL and the direct bilirubin level was 0.2 mg/dL. The baby is urinating and sleeping well. Baby is nursing every 3-4 hours for 10 minutes but falls asleep at the breast. +3 stools in the last 24 hours. On exam, the infant is afebrile and has lost 13 percent of birth weight. The baby’s eyes, tongue, and skin appear yellow down to the umbilicus. Anterior fontanelle is open and flat. The infant is alert and has a 3 cm cephalhematoma located on the left parietal area. A STAT Total serum bilirubin level is 17 mg/dL at 72 hours.
8/3/2018
2
A. Reassure parents that this is normal. And follow up in 2 days.
B. Repeat total and direct bilirubin levels in 24 hours.
C. Admit the infant and initiate exchange transfusion.
D. Initiate home phototherapy and follow up in 24 hours.
E. Admit the infant and start IVIG and phenobarbital.
Unconjugated hyperbilirubinemia
Peak values occur at 48-96 hours
Resolves within 1-2 weeks after birth
Pathologic if noted in the first 24 hours of life
Different nomograms for determination of risk, phototherapy treatment and exchange transfusion

8/3/2018
3
Bryon J. Lauer, and Nancy D. Spector
Pediatrics in Review 2011;32:341-349
Phototherapy
24 hrs-bilirubin > 10 mg/dL
48 hrs-bilirubin>13 mg/dL
72 hrs-bilirubin>15 mg/dL
24 hrs-bilirubin >16.5 mg/dL
48 hrs-bilirubin > 19 mg/dL
72 hrs- bilirubin> 21 mg/ dL
Exchange transfusion
8/3/2018
4
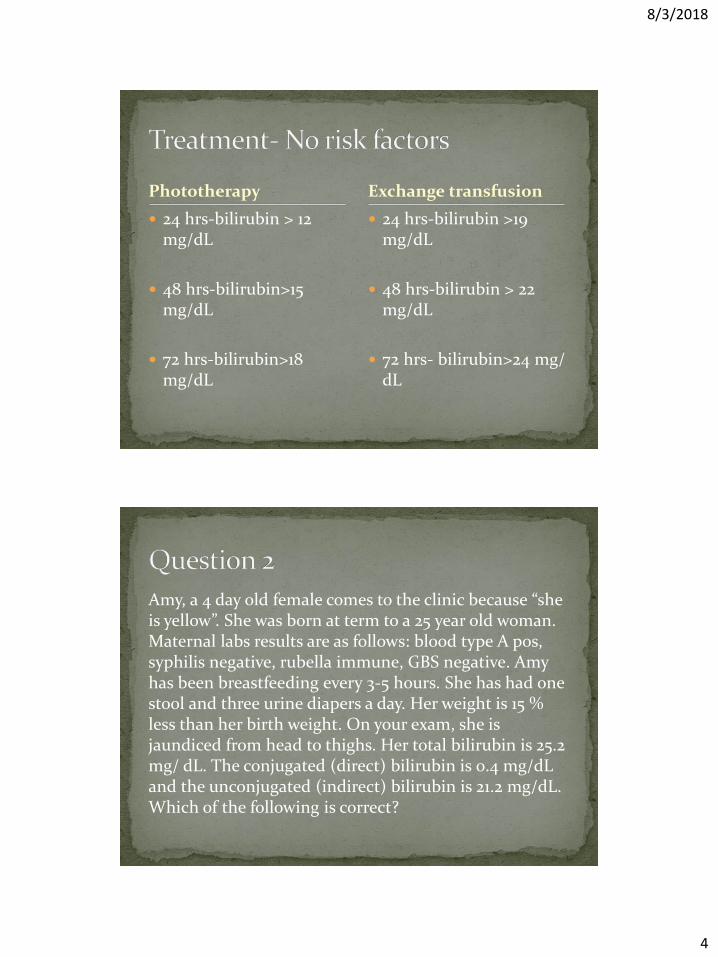
Phototherapy
24 hrs-bilirubin > 12 mg/dL
48 hrs-bilirubin>15 mg/dL
72 hrs-bilirubin>18 mg/dL
24 hrs-bilirubin >19 mg/dL
48 hrs-bilirubin > 22 mg/dL
72 hrs- bilirubin>24 mg/ dL
Exchange transfusion
Amy, a 4 day old female comes to the clinic because “she is yellow”. She was born at term to a 25 year old woman. Maternal labs results are as follows: blood type A pos, syphilis negative, rubella immune, GBS negative. Amy has been breastfeeding every 3-5 hours. She has had one stool and three urine diapers a day. Her weight is 15 % less than her birth weight. On your exam, she is jaundiced from head to thighs. Her total bilirubin is 25.2 mg/ dL. The conjugated (direct) bilirubin is 0.4 mg/dL and the unconjugated (indirect) bilirubin is 21.2 mg/dL. Which of the following is correct?

8/3/2018
5
A. she has breastfeeding failure jaundice
B. she has physiologic jaundice
C. she has biliary atresia; you must consult pediatric gastroenterology
D. There is an ABO incompatibility between the mother and the child
E. she has pathologic jaundice
Develops within the first few days of life as opposed to breast milk jaundice which develops later
Due to inadequate breastmilk production
8/3/2018
6
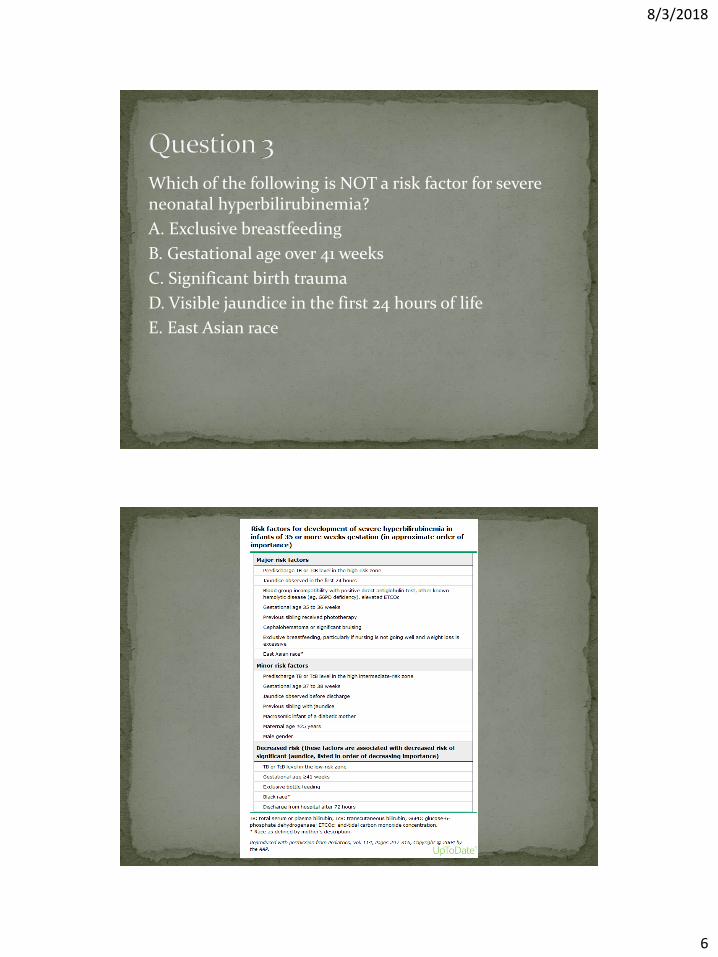
Which of the following is NOT a risk factor for severe neonatal hyperbilirubinemia?
A. Exclusive breastfeeding
B. Gestational age over 41 weeks
C. Significant birth trauma
D. Visible jaundice in the first 24 hours of life
E. East Asian race

8/3/2018
7
Amy’s CBC is unremarkable and blood type is A pos.
Which of the following is the most appropriate initial therapy for this patient. Her total bilirubin is 25.2 mg/ dL. The conjugated (direct) bilirubin is 0.4 mg/dL and the unconjugated (indirect) bilirubin is 21.2 mg/dL.
A. admit for exchange transfusion
B. admit for fluids to improve hydration
C. admit for phototherapy
D. discharge home encourage formula feeding, light exposure, and follow up bilirubin tomorrow
Severe neonatal bilirubinemia TB> 25 mg/ dLBilirubin induced neurologic dysfunction (BIND) Acute bilirubin encephalopathy (ABE)
Chronic and permanent sequela of BIND=kernicterus
***Treated with exchange transfusion

8/3/2018
8
You admit Amy for further management. You confirm Amy’s current weight, which is down 15 % from birth weight. Beyond what point in time is it considered problematic if the patient has not returned to his or her birth weight?
A. 5 days
B. 7 days
C. 10 days
D. 14 days
E. None of the above
By 14 days-regain birth weight
By 6 months-double birth weight
By 12 months-triple birth weight

8/3/2018
9
The current recommendation for the treatment of breast milk jaundice is:
A. Continue to breastfeed
B. Stop breastfeeding and change to cow’s milk formula
C. Stop breastfeeding and change to soy milk formula
D. Stop breastfeeding and treat with rehydration solution
Continuation of breastfeeding, increase frequency, formula supplementation
Phototherapy
Exchange transfusion
8/3/2018
10
A 2 week old infant presents to the office with mom and complaint of poor feeding for the last 2 days. She has noted that the infant has been more fussy and has been sleeping more. The baby has been formula feeding 2 ounces/ 3-4 hours until 2 days ago at which time the infant would only take 1 ounce every 6-8 hours. Urine output has decreased from 8 wet diapers to 3 wet diapers/ day. Vitals-T101 ° F, HR-167, RR-60-fontanelle is sunken and MM dry. Heart is tachycardic without Murmurs. Lungs are clear without wheezes or rhonchi. Abdomen is soft, no masses or erythema noted at umbilicus. Decreased bowel sounds in all quadrants.
A. Administer acetaminophen and obtain labs.
B. Administer ceftriaxone and follow up in 24 hours.
C. Admit the infant for work up and empiric antibiotics.
D. Arrange for home health to assist with improved feeding.
E. Obtain prenatal history and birth history.
8/3/2018
11
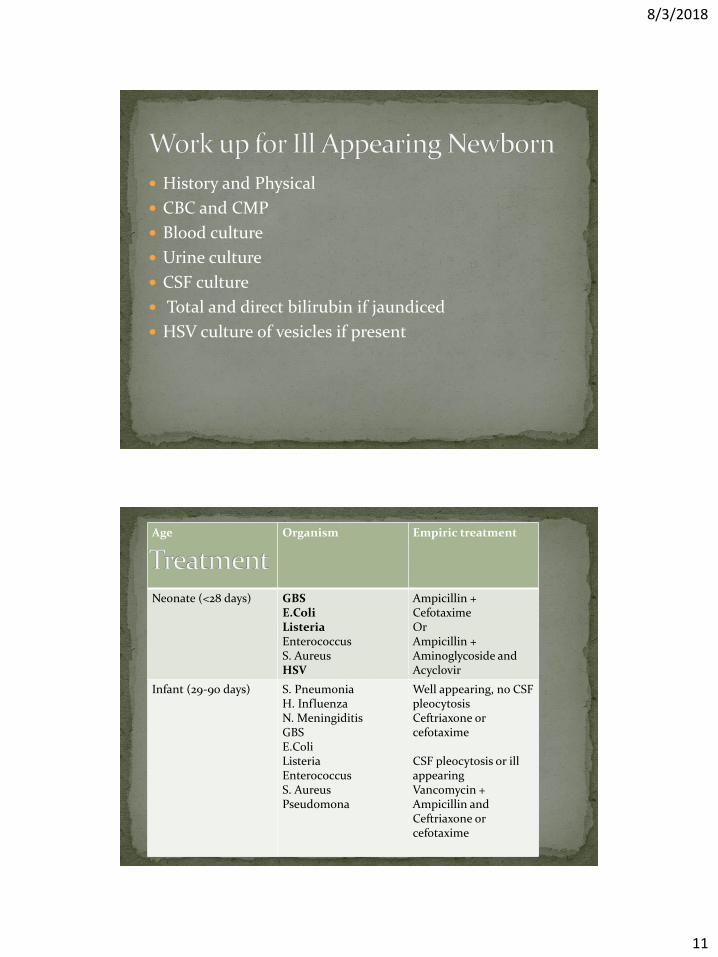
History and Physical
CBC and CMP
Blood culture
Urine culture
CSF culture
Total and direct bilirubin if jaundiced
HSV culture of vesicles if present
Age Organism Empiric treatment
Neonate (<28 days) GBSE.ColiListeriaEnterococcusS. AureusHSV
Ampicillin + Cefotaxime OrAmpicillin + Aminoglycoside and Acyclovir
Infant (29-90 days) S. PneumoniaH. InfluenzaN. MeningiditisGBSE.ColiListeriaEnterococcusS. AureusPseudomona
Well appearing, no CSFpleocytosisCeftriaxone or cefotaxime
CSF pleocytosis or ill appearingVancomycin + Ampicillin and Ceftriaxone or cefotaxime
8/3/2018
12
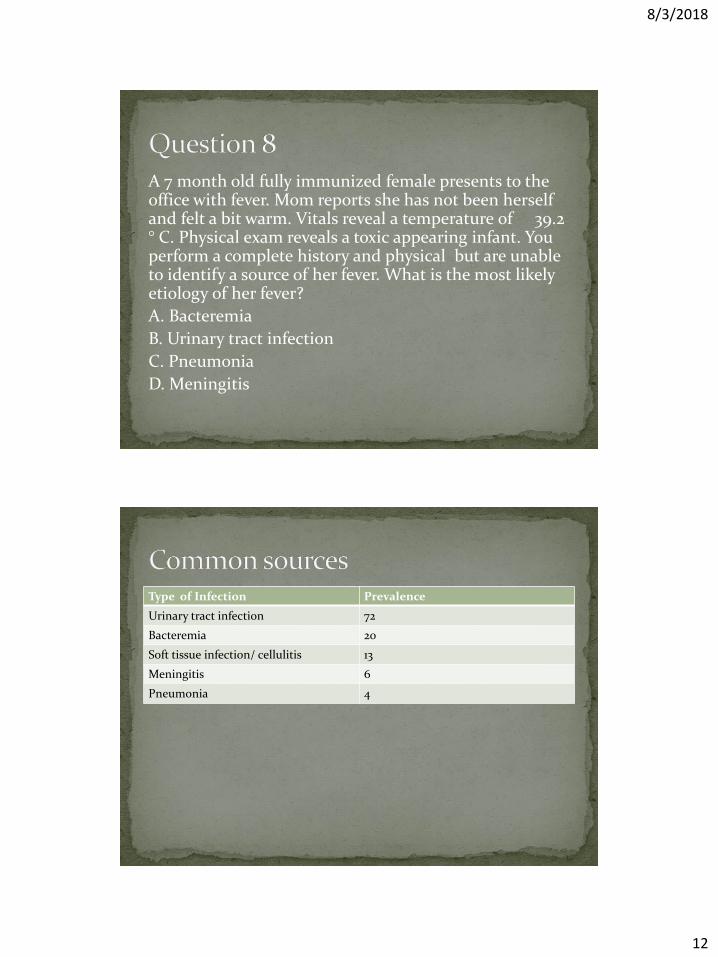
A 7 month old fully immunized female presents to the office with fever. Mom reports she has not been herself and felt a bit warm. Vitals reveal a temperature of 39.2 ° C. Physical exam reveals a toxic appearing infant. You perform a complete history and physical but are unable to identify a source of her fever. What is the most likely etiology of her fever?
A. Bacteremia
B. Urinary tract infection
C. Pneumonia
D. Meningitis
Type of Infection Prevalence
Urinary tract infection 72
Bacteremia 20
Soft tissue infection/ cellulitis 13
Meningitis 6
Pneumonia 4

8/3/2018
13
Age younger than 28 days
Maternal infection in pregnancy or labor
Temperature over 40° C (104 F)
Unimmunized
Prematurity
Chronic illness
Antibiotic administration with in 7 days
Social barriers to follow up
An 18 month old male presents to your office for well child check. His weight has dropped from 30th
percentile to 5th percentile since his last well check 6 months ago. Father reports that he is a picky eater and mainly consumes apple juice and rice cereal. He has refused milk and his mother believes he is lactose intolerant and therefore has not been receiving any. He has 6 wet diapers/ day and 4-5 loose stools/ day. On physical exam you note symmetric bruising on the upper arms and healed circular burns on the buttocks and lower back.

8/3/2018
14
A. Contact a pediatric dietician for outpatient consultation
B. Inpatient admission for work up and initiation of nutritional support
C. Notify local authorities to escort the father out of the clinic
D. Perform labs to screen for underlying medical disorder
E. Perform skeletal survey for inherited bone disease

8/3/2018
15
Nutritional
Medical
Developmental/behavioral
Psychosocial factors
Interdisciplinary approach is critical to success
Indication for Hospitalization Severe malnutrition
Dehydration
Serious illness
Child at risk for harm
Failed OP management
Severe parental mental health disorders
Loss of follow up due to location or transportation
8/3/2018
16
A family has moved into the area and brings their 12 month old girl in for a well child check. They bring her medical records with them. Her parents have no concerns, and she has been healthy. Her growth chart reveals her length tracks along at 25 th % and her weight has decreased from 50th % at 6 months to 10th% at 9 months and now is at the 5th %. Which of the following most likely explains her pattern of growth?
A. Normal
B. Familial short stature
C. Prenatal insult such as exposure to drugs or infection
D. Hypothyroidism
E. Inadequate nutrition

8/3/2018
17
FTT is a sign not a diagnosis
Occurs in 5-10 % of children in primary care
Also called weight faltering, failure to gain weight appropriately, or undernutrition
Weight loss across two standard deviations on the growth chart
Weight less than 80 percent ideal weight for age
Weight below the 2nd percentile
Rate of daily weight gain less than expected
Taking more history you discover that she eats mostly rice and fruit. She does not like meat. Her parents endorse that she is very picky. She drinks about 12 oz or whole milk and 12 oz apple juice each day. She is active and developmentally appropriate. Her ROS is negative as is her past medical history. What is the least appropriate way to proceed with evaluation and management of this patient?

8/3/2018
18
A. Allow the child to feed herself whenever she is hungry or thirsty.
B. Obtain cbc, iron studies and urinalysis
C. Limit juice
D. Consult a nutritionist
E. Prescribe a multivitamin
A 14 month old female presents to the ED with mom and chief complaint of emesis and diarrhea for the last 48 hours. She cannot tell if the child has had urine output because of the watery diarrhea. On examination, her temperature is 102.5 ° F, heart rate is 180 bpm, blood pressure is 80/50 mm HG. Her weight is 8 kg. She is lying very still in her mother’s lap. She has dry, cracked lips and dry skin. Her capillary refill is about 4 seconds and you note mottling of the extremities. What is the most appropriate next step in the management of this patients condition?

8/3/2018
19
A. Evaluate for underlying bacterial infection with blood, urine and stool cultures.
B. Admit to an inpatient pediatric until and begin maintenance IV fluids
C. Infuse 20 mL/kg normal saline over 20 minutes
D. begin oral rehydration with Pedialyte
E. Infuse 10mL/kg D5 ½ NS over 2 hours
Finding Mild Moderate Severe
Pulse Normal Rapid Rapid, weak, orabsent
Systolic pressure Normal Normal to low Low
Respirations Normal Deep, may be ↑ Deep, ↑ or ↓
Buccal mucosa Normal Sunken Markedly sunken
Anterior fontanelle
Normal Sunken Markedly sunken
Eyes Normal Sunken Markedly sunken
Skin turgor Normal Reduced Tenting
Skin Normal Cool Cool, mottled, acrocyanosis
Urine output Normal Markedly reduced
Anuria
Systemic signs Increased thirst Listlessness, irritability
Grunting, lethargy, coma

8/3/2018
20
A 3 year old female presents with her mother with a complaint of productive cough over the last 3 days. The sputum is described as copious and is yellowish white in color. She does go to day care and there have been several kids out due to some respiratory illness. Vitals T 102°F, HR 150, RR 65. She is ill appearing and clinging to her mother. Heart is tachycardic without murmur. Lungs reveal rhonchi in the right lower lung field. Retractions are noted.
A. Group B streptococcus
B. Klebsiella pneumonia
C. Listeria monocytogenes
D. Pseudomonas aeruginosa
E. Streptococcus pneumonia

8/3/2018
21
Age Organism Treatment
<1mo Group B strep, E. Coli, Klebsiella, Pseudomonas, Listeria
Amp + Aminoglycoside OR Amp + Cefotaxime
1-3 moH. influ, S. pneumonia, Grp A or B strep, pertussis
Amp + Cefotax
3mo- 5 yrS. pneumonia, H. influ, Staph aureus, Grp A Strep, pertussis
Cephalosporin + anti-staph or pertussis if indicated
>5yo S. pneumonia, H. influ, Grp A Strep
PCN OR Amp OR Cephalosporin + anti-staph or pertussis if indicated
The parents of a 2 month old present with concerns that their daughter vomits at least 2 ounces of formula with every feed. There is no blood in the vomit and the baby appears to be hungry after she vomits. She has no respiratory symptoms. They burp her for 5-10 minutes after each feeding. She is at the 70th percentile for height, 50th percentile for weight, and 60th percentile for head circumference which is consistent with her growth measurements since birth. Physical exam reveals a cheerful infant otherwise unremarkable.
8/3/2018
22
A. Order lab tests to rule out underlying medical condition
B. Counsel the parents regarding lifestyle modifications.
C. Refer the baby to a gastroenterologist
D. Prescribe ranitidine
E. Prescribe omeprazole
Conservative therapy Lifestyle changes
Upright position after feedings
Small frequent feedings
Thickening formula or breastmilk

8/3/2018
23
Proton pump inhibitors Omeprazole (Prilosec)
Lansoprazole (Prevacid)
Rabeprazole (Aciphex)
Esomeprazole (Nexium)
Hydrogen 2 blockers
Ranitidine (Zantac)
Nizatidine (Axid)
A two year old male presents to your office with his father complaining that the patient has had intermittent crying followed by episodes of profound lethargy during which he is difficult to arouse. The father further describes the episodes explaining the patient will sometimes clutch his abdomen and roll into the fetal position. This started about 4 hours prior to presenting to your office. He denies any fever, vomiting, or diarrhea. He denies any sick contacts. He is developmentally normal and has a negative past medical history. His examination reveals an afebrile non toxic appearing male. His abdominal exam is unremarkable.

8/3/2018
24
A. Meningitis
B. Renal Colic
C. Intussusception
D. Gastric outlet obstruction
E. Appendicitis
Section of intestine telescopes into the adjoining bowel leading to bowel obstruction
Often presents with non bilious vomiting, colicky abdominal pain, passage of blood and mucus “currant jelly” stools, lethargy and a palpable abdominal mass in the right

8/3/2018
25
A. CBC
B. UA
C. Glucose
D. Serum lactate
E. None of the above
Lab analysis in intussusception is generally not helpful in aiding the diagnosis
Later in the disease course may see leukocytosis, evidence of dehydration, and electrolyte imbalance

8/3/2018
26
A. Upper GI with barium
B. A plain film of the abdomen
C. An air enema
D. An abdominal ultrasound
E. CT scan of the abdomen with oral contrast
“Bull’s eye” appearance on ultrasound confirms the diagnosis of intussusception
Air enema is the preferred non surgical treatment
8/3/2018
27
A 7 year old male presents to your clinic with his mother with the complaint of enuresis. The child has never been continent at night, wetting his bed several times per night. This is becoming a problem for him and the family. He denies any urge or overflow problems. UA was unremarkable. Physical exam reveals a well developed, well nourished child. Abdominal exam is unremarkable.
Which of the following recommendations would be the initial treatment for primary enuresis?
A. Patient education and motivational training
B. Over-learning
C. Enuresis alarm
D. Nasal desmopressin (DDAVP)
E. Oral desipramine

8/3/2018
28
Initial treatment
Behavioral modification
Education
Patient and caring paternal attitude
Normal daytime voiding and stooling pattern
After 3 months: may consider alarm therapy or pharmacologic therapy
Oral DDAVP – 6 years or older, 0.2-0.6 mg q hs, restrict fluid intake for 1 hour or more before administration
If initial treatment fails
8/3/2018
29
Questions:
Sarah Hall, D.O.
OSU Center for Health Sciences
Associate Professor of Family Medicine
1. Muchowski, KE. Evaluation and Treatment of Neonatal Hyperbilirubinemia. Am Fam Physician, 2014 June 1; 89(11):873-878.
2. Jardine, LA., Woodgate, P. Neonatal Jaundice, Am Fam Physician. 2012 Apr 15;85(8):824-825.
3. Woodgate P, Jardine LA. Neonatal jaundice: phototherapy. Systematic review 319. BMJ Clinical Evidence. 2015 May. http://clinicalevidence.bmj.com/x/systematic-review/0319/overview.html. essed July 6, 2015.
4. BiliTool www.bilitool.org
5. AMERICAN ACADEMY OF PEDIATRICS: Management of Hyperbilirubinemia in the Newborn Infant 35 or More Weeks of Gestation. Subcommittee on Hyperbilirubinemia. Pediatrics 2004; 114:1 297-316; doi:10.1542/peds.114.1.297. Downloaded at Columbia University on July 7, 2015.
6. Centers for Disease Control and Prevention. Kernicterus in Full Term Infants.http://www.cdc.gov/ncbddd/jaundice/hcp.html.
7. American Academy of Pediatrics. Jaundice picture. www.healthychildren.org. Jaundice picture.
8. Lauer, BJ, Spector, ND. Hyperbilirubinemia in the Newborn. Pediatrics in Review 2011; 32:341-349; (doi:10.1542/pir.32-8-341).
8/3/2018
30
9. Lewis, ML. A Comprehensive Newborn Exam. Am Fam Physician. 2014 Sep 1;90(5):289-296.
10. Gastroesophageal Reflux. Pediatrics in Review Vol. 33 No. 6 June 1, 2012. pp. 243 -254 (doi: 10.1542/pir.33-6-243).
11. Lightdale, JR. Gremse, DA. Gastroesophageal Reflux: Management Guidance for the Pediatrician. SECTION ON GASTROENTEROLOGY, HEPATOLOGY, AND NUTRITION. Pediatrics Vol. 131 No. 5 May 1, 2013. pp. e1684 -e1695 (doi: 10.1542/peds.2013-0421). Last accessed July 7, 2015.
12. Pediatric Gastroesophageal Reflux Clinical Practice Guidelines: Joint Recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) and the European Society for PediatricGastroenterology, Hepatology, and Nutrition (ESPGHAN) Journal of Pediatric Gastroenterology and Nutrition. 49:498–547#2009 by European Society for Pediatric Gastroenterology, Hepatology, and Nutrition and North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition. http://www.naspghan.org/files/documents/pdfs/position-papers/FINAL%20-%20JPGN%20GERD%20guideline.pdf.
13. Canares, T et al. Going with the Flow: Respiratory Care in the Pediatric Emergency Department. Pediatric Emergency Medicine. Rhode Island Medical Journal. January 2014. 23-26.
14. Immunization Action Coalition. http://www.immunize.org/catg.d/p4211.pdf.
15.e http://phil.cdc.gov/phil/details.asp?pid=3168. L accessed July 9, 2015.ters for Disease
Control and Prevention. Immunization Schedule. http://www.cdc.gov/vaccines/schedules/downloads/child/0-18yrs-ined-schedule.pdf . Last accessed July 9, 2015.
8/3/2018
31
16. Cole S and Lanham J. Failure to Thrive: An Update. Am Fam Physician. 2011 Apr 1;83(7):829-834.
17. Kirkland, R, Motil K, Duryea, T. Poor weight gain in children younger than two years: Etiology and Evaluation. Up to Date. Last Updated June 28, 2018.
18. Kirkland, R, Motil K, Duryea, T. Poor weight gain in children younger than two years : Management. Up to Date. Last Updated June 28, 2018.
19. Smitherman H and Macias J. Febrile infant (younger than 90 days of age): Outpatient evaluation. Up to Date. Last Updated June 13, 2018.
20. Scarfone R and Cho C. Approach to the ill appearing infant. Up to Date. Last Updated Feb 15, 2018.
21. Barson W. Community-acquired pneumonia in children: Clinical features and diagnosis. Up to Date. Last Updated March 30, 2018 .
22. Barson W. Pneumonia in children: Inpatient treatment. Up to Date. Last Updated Jul 17, 2018.
23. Stuckey-Schrock K, and Hayes B. Community-Acquired Pneumonia in Children. Am Fam Physician. 2012 Oct 1;86(7):661-667.
24. Weiner D. Acute respiratory distress in children: Emergency evaluation and initial stabilization. Up to Date. Last Updated Dec 12, 2016.
25. Nurko S and Zimmerman L. Evaluation and Treatment of Constipation in Children and Adolescents. Am Fam Physician. 2014 Jul 15;90(2):82-90.
26. Sood M. Constipation in infants and children: Evaluation. Up to Date. Last Updated April 10, 2018.
27. Kliegman S. Nelson Textbook of Pediatrics 20th ed. Ch 41 Failure to Thrive.2016.
28. Kliegman S. Nelson Textbook of Pediatrics 20th ed. Ch 102 Digestive System Disorders. 2016.
8/3/2018
32
29. Kliegman S. Nelson Textbook of Pediatrics 20th ed. Ch 109 Infections of the Neonatal Infant. 2016.
30. Kliegman S. Nelson Textbook of Pediatrics 20th ed. Ch 306 Major Symptoms and Signs of Digestive Tract Disorders. 2016.
31. Kliegman S. Nelson Textbook of Pediatrics 20th ed. Ch 172 Immunization practices. 2016.
32. Kliegman S. Nelson Textbook of Pediatrics 20th ed. Ch 176 Fever. 2016.
33. Kliegman S. Nelson Textbook of Pediatrics 20th ed. Ch 98 Clinical Manifestations of Diseases in the Newborn Period. 2016.
34. Kliegman S. Nelson Textbook of Pediatrics 20th ed. Ch 102.3 Jaundice and Hyperbilirubinemia in the Newborn. 2016.
35. Kliegman S. Nelson Textbook of Pediatrics 20th ed. Ch 71 Respiratory Distress and Failure. 2016.
36. Kliegman S. Nelson Textbook of Pediatrics 20th ed. Ch 329 Pyloric Stenosis and Other Congenital Anomalies of the Stomach. 2016.
37. Kliegman S. Nelson Textbook of Pediatrics 20th ed. Ch 355 Manifestations of Liver Disease. 2016.
38. Kliegman S. Nelson Textbook of Pediatrics 20th ed. Ch 323 GERD. 2016.
39. Graber and Wilbur’s Family Medicine Examination and Board Review, 4th edition, 2017.
40. Nghia Jack Vo, MD, Sato Thomas, MD. Intussusception in children. Up to Date. Last updated June 29, 2018.