building a preventive ethics program mary beth foglia rn phd ma integratedethics manager: preventive...
TRANSCRIPT

Building a Preventive Building a Preventive Ethics ProgramEthics Program
Mary Beth Foglia RN PhD MA
IntegratedEthics Manager: Preventive Ethics, and Senior Staff, Ethics Evaluation Group
National Center for Ethics in Health Care (VHA)
Catholic Health East
August 5, 2009

Learning objectivesLearning objectives
Describe IntegratedEthics modelDescribe IntegratedEthics modelIdentify key elements of Preventive Identify key elements of Preventive EthicsEthics
Describe how to get started in Describe how to get started in developing a preventive ethics developing a preventive ethics approachapproach
What Is IntegratedEthics?What Is IntegratedEthics?
A national education and A national education and organizational change initiative organizational change initiative
A comprehensive, systematic A comprehensive, systematic approach to ethics in health approach to ethics in health care care
Perceived Quality GapsPerceived Quality Gaps
Lack of adequate training Lack of adequate training 96%96%
Lack of a systematic approach Lack of a systematic approach 88%88%Ethics program not well integratedEthics program not well integrated 80%80%Ethics program lacks standardsEthics program lacks standards 71%71%Ethics program not improvement-orientedEthics program not improvement-oriented 68%68%Ethics program too narrowly focused Ethics program too narrowly focused 64%64%Ethics program not data-drivenEthics program not data-driven 64%64%Lack of leadership support/accountabilityLack of leadership support/accountability 60%60%

The IntegratedEthics The IntegratedEthics ModelModel

DecisionsDecisionsand actionsand actions
SystemsSystemsand processesand processes
EnvironmentEnvironmentand cultureand culture
What Is Ethics Quality?What Is Ethics Quality?

Three Core FunctionsThree Core Functions
Ethics ConsultationEthics Consultation Responding to ethics questions in health careResponding to ethics questions in health care
The CASES ApproachThe CASES Approach
Preventive EthicsPreventive Ethics Addressing ethics quality gaps on a systems Addressing ethics quality gaps on a systems
levellevel The ISSUES ApproachThe ISSUES Approach
Ethical LeadershipEthical Leadership Fostering an ethical environment and cultureFostering an ethical environment and culture
The Four Compass pointsThe Four Compass points

Ethics Ethics ConsultationConsultation
Preventive Preventive EthicsEthics
EthicalEthicalLeadershipLeadership
Three Core FunctionsThree Core Functions

Domains of ethics in Domains of ethics in health carehealth care
Shared decision making with patientsShared decision making with patients Ethical practices in end-of-life careEthical practices in end-of-life care Patient privacy and confidentialityPatient privacy and confidentiality Professionalism in patient careProfessionalism in patient care Ethical practices in resource allocationEthical practices in resource allocation
Domains of ethics Domains of ethics –– continuedcontinued
Ethical practices in business and Ethical practices in business and managementmanagement
Ethical practices in government serviceEthical practices in government service Ethical practices in researchEthical practices in research Ethical practices in the everyday Ethical practices in the everyday
workplace workplace IntegratedEthics programIntegratedEthics program

Introduction to Introduction to Preventive Ethics Preventive Ethics

Preventive ethics Preventive ethics defineddefined
Activities performed by an individual or group on behalf of a health care organization to identify, prioritize, and address systemic ethics issues

Goal of Preventive Goal of Preventive EthicsEthics
Produce Produce measurablemeasurable and and sustainablesustainable improvements in improvements in an organization’s ethics an organization’s ethics practicespractices

Difference between Difference between best practicebest practice and and current practicecurrent practice
Difference between what staff Difference between what staff oughtought to to do and what staff do and what staff isis doing doing
What is an Ethics What is an Ethics Quality Gap?Quality Gap?
Preventive ethics (PE) seeks to reduce gaps through a quality improvement approach
Preventive ethics seeks to reduce gaps through a quality improvement approach
Preventive Ethics Preventive Ethics RReduces Variation in educes Variation in Ethics PracticesEthics Practices

““Treat equals equally and Treat equals equally and unequals unequallyunequals unequally…”…”
From: Aristotle, Nicomachean Ethics. translated by Weldon, J.E.C. Prometheus Books (Buffalo, NY:1987).
PE Promotes Organizational Justice
1616

Traditional case-based ethics Traditional case-based ethics consultation services don’t address consultation services don’t address systems-level obstacles to ethical systems-level obstacles to ethical practicespractices
Developing individual virtue through Developing individual virtue through training and education alone can’t training and education alone can’t ensure ethical practiceensure ethical practice
Key assumptions of Key assumptions of preventive ethicspreventive ethics

The primary causes of ethics quality gaps The primary causes of ethics quality gaps lie in organizational systems and lie in organizational systems and processesprocesses——not the behavior of not the behavior of individualsindividuals
Ethical practices in health care can be Ethical practices in health care can be measured and improvedmeasured and improved
Key assumptions of Key assumptions of Preventive Ethics Preventive Ethics – – continuedcontinued

Introduction Introduction to ISSUESto ISSUES
ISSUES approach to ISSUES approach to reducing ethics reducing ethics quality gapsquality gapsIIdentify an issuedentify an issue
SStudy the issuetudy the issue
SSelect a strategyelect a strategy
UUndertake a planndertake a plan
EEvaluate and adjustvaluate and adjust
SSustain and spreadustain and spread

A systematic, step-by-step process A systematic, step-by-step process to narrow the gap between “best to narrow the gap between “best practice” and “current practice”practice” and “current practice”
Marries principles and methods of Marries principles and methods of quality improvement with quality improvement with principles and methods of ethical principles and methods of ethical analysis analysis
Targets the systems and Targets the systems and processes that influence ethical processes that influence ethical practices in a facilitypractices in a facility
ISSUES approach to ISSUES approach to reducing ethics quality reducing ethics quality gaps gaps – overview– overview

Identify an issue Find an opportunity for improvement(Core team + ad hoc members) Organize a teamStudy the issue Clarify processes and problemsSelect a strategy Understand root causesSelect a strategy Select improvementUndertake a plan PlanUndertake a plan DoEvaluate and adjust StudySustain and spread Act
ISSUES FOCUS-PDSA
Crosswalk Crosswalk – ISSUES and – ISSUES and FOCUS-PDSAFOCUS-PDSA

Indications for PE : Indications for PE : Examples from the Examples from the FieldField
DOMAINDOMAIN NN %%
Shared Decision MakingShared Decision Making 12/3012/30 4040
Professionalism Professionalism 5/305/30 1717
Resource AllocationResource Allocation 4/304/30 1313
End-of-Life CareEnd-of-Life Care 4/304/30 1313
Business & ManagementBusiness & Management 2/302/30 77
Everyday Work PlaceEveryday Work Place 1/301/30 33
Privacy and ConfidentialityPrivacy and Confidentiality 1/301/30 33
IntegratedEthics ProgramIntegratedEthics Program 1/301/30 33

Shared Decision Shared Decision MakingMakingExamples:Examples: Advance directives of dialysis patients are not Advance directives of dialysis patients are not
accurate, or updatedaccurate, or updated Advance care planning is not addressed in Advance care planning is not addressed in
primary careprimary care Advance care planning processes do not Advance care planning processes do not
include elicitation of mental health treatment include elicitation of mental health treatment preferences preferences
Electronic informed consent is not utilizedElectronic informed consent is not utilized ‘‘Gurney consent’ is obtained for non-emergent Gurney consent’ is obtained for non-emergent
casescases Organ donation screening practices are Organ donation screening practices are
inconsistent with policyinconsistent with policy

ProfessionalismProfessionalism
Examples:Examples: Patients discharged AMA are Patients discharged AMA are
denied follow-up appointments, denied follow-up appointments, discharge medicines and discharge medicines and discharge instructionsdischarge instructions
Adverse events are not Adverse events are not consistently reported, disclosed or consistently reported, disclosed or documented in the health recorddocumented in the health record
Resource AllocationResource Allocation
Examples:Examples: Practice of “Discharge by noon” results in Practice of “Discharge by noon” results in
avoidable readmissions, burdensome rework, avoidable readmissions, burdensome rework, and patient dissatisfactionand patient dissatisfaction
TCU patients requiring/requesting palliative TCU patients requiring/requesting palliative care are transferred to ED and then to care are transferred to ED and then to inpatient careinpatient care
The process for referring Veterans for services The process for referring Veterans for services outside of VHA is inconsistent and perceived outside of VHA is inconsistent and perceived to be arbitrary and unfairto be arbitrary and unfair
Care processes for “difficult” patients are Care processes for “difficult” patients are inconsistent and lack coordinationinconsistent and lack coordination

End-of-Life End-of-Life
Examples:Examples: Process to address requests for portable Do Not Process to address requests for portable Do Not
Attempt Resuscitation (DNAR) orders is lackingAttempt Resuscitation (DNAR) orders is lacking Processes for eliciting patient preferences and Processes for eliciting patient preferences and
goals of care are inconsistent resulting in “futile” goals of care are inconsistent resulting in “futile” carecare
Attending physicians routinely disapprove Attending physicians routinely disapprove requests for ethics and palliative care consultsrequests for ethics and palliative care consults
Clinical warnings (CWAD) are inconsistently Clinical warnings (CWAD) are inconsistently updated leading to staff mistrust of DNAR status updated leading to staff mistrust of DNAR status

Everyday WorkplaceEveryday Workplace
Examples:Examples: Inconsistencies exist in emergency-related Inconsistencies exist in emergency-related
facility closures/time and leave policies facility closures/time and leave policies across VISN causing staff and labor partners across VISN causing staff and labor partners moral distress (“unfair and arbitrary”)moral distress (“unfair and arbitrary”)

Privacy and Privacy and ConfidentialityConfidentialityExamples:Examples: Food service workers note that personal food Food service workers note that personal food
items (food brought in for patients by items (food brought in for patients by family/friends) are labeled with full name, family/friends) are labeled with full name, DOB and social security numberDOB and social security number

Select OutcomesSelect Outcomes
DomaiDomainn
IssueIssue ProcessProcess
ChangeChangeMeasureMeasure
ssResultResult
SDMSDM Advance Advance directives of directives of dialysis dialysis patients are not patients are not accurateaccurate
Revised Revised job job description description of SW to of SW to coordinate coordinate processprocess Simplified Simplified and clarified and clarified process process Developed Developed quality quality check prior check prior to scanningto scanning Instituted Instituted routine routine patient patient educationeducation
% of % of advance advance directives directives that are that are accurateaccurate
Increase Increase from 58% of from 58% of advance advance directives to directives to 96%96%

Select OutcomesSelect Outcomes
DomaiDomainn
IssueIssue ProcessProcess
ChangeChangeMeasureMeasure
ssResultResult
SDMSDM Utilization rates Utilization rates for for iMedConsent iMedConsent were well were well below national below national averageaverage
Local Local leadership leadership mandated mandated useuse Trained AD Trained AD PACs to PACs to address address routine routine systems systems failuresfailures Used pay Used pay for for performanceperformance Increased Increased wireless wireless capability on capability on unitsunits
% of % of informed informed consents consents documented documented in iMed in iMed
Increased Increased from 20% from 20% across 5 across 5 specialties specialties to nearly to nearly 100% across 100% across same same specialties specialties

Select OutcomesSelect Outcomes
DomaiDomainn
IssueIssue ProcessProcess
ChangeChangeMeasureMeasure
ssResultResult
SDMSDM Organ donation Organ donation screening screening practices are practices are inconsistent inconsistent with policy and with policy and non-compliant non-compliant with The Joint with The Joint Commission Commission (TJC)(TJC)
Identified Identified responsible responsible service and service and single single processprocess Screening Screening template & template & note note developed developed ROI ROI revised to revised to remain in remain in effect unless effect unless revoked by revoked by patientpatient New New patient patient orientationorientation
% of new % of new admissions admissions screened for screened for organ organ donationdonation
Increase Increase from 57% of from 57% of new new admissions admissions to 88%to 88%

Select OutcomesSelect Outcomes
DomainDomain IssueIssue ProcessProcess
ChangeChangeMeasureMeasure
ssResultResult
ProfessionalisProfessionalismm
Inconsistent Inconsistent documentatidocumentation of on of adverse adverse event event disclosuredisclosure
Updated Updated MCMMCM Developed Developed standard standard documentation documentation template with template with auto alert to auto alert to risk risk managementmanagement Just in time Just in time disclosure disclosure training training CMO/CNO set CMO/CNO set clear clear expectations expectations with Service with Service Chiefs & Nurse Chiefs & Nurse managersmanagers
% of adverse % of adverse events that events that require require disclosure disclosure that are that are documented documented
IncreaseIncreased from d from 10% to 10% to 90%90%
Select OutcomesSelect Outcomes
DomainDomain IssueIssue ProcessProcess
ChangeChangeMeasureMeasure
ssResultResult
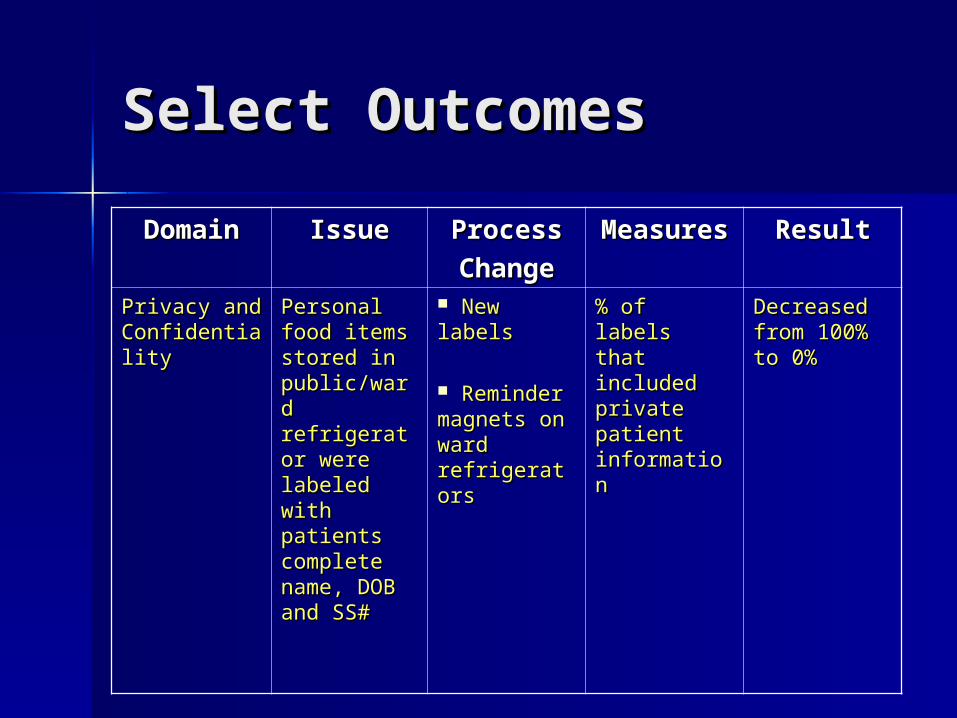
Privacy and Privacy and ConfidentialiConfidentialityty
Personal Personal food items food items stored in stored in public/ward public/ward refrigerator refrigerator were labeled were labeled with with patients patients complete complete name, DOB name, DOB and SS#and SS#
New labelsNew labels
Reminder Reminder magnets on magnets on ward ward refrigeratorsrefrigerators
% of labels % of labels that that included included private private patient patient informationinformation
Decreased Decreased from 100% from 100% to 0%to 0%
Getting Getting StartedStarted

Models of Organizing Models of Organizing PE PE Core function of IntegratedEthics Core function of IntegratedEthics
programprogram– Reports to facility leadership through the Reports to facility leadership through the
IntegratedEthics facility councilIntegratedEthics facility council Part of Ethics ProgramPart of Ethics Program
– Subcommittee of organizational ethics with Subcommittee of organizational ethics with strong linkages to ethics consultationstrong linkages to ethics consultation
Part of Quality Management ProgramPart of Quality Management Program

Core membersCore members– PE coordinator PE coordinator
with dedicated with dedicated timetime
– Team members Team members – Responsible for Responsible for
ongoing work ongoing work of PE functionof PE function
Ad hoc membersAd hoc members– Issue specificIssue specific– Time-limited Time-limited
commitmentcommitment– Most often Most often
content or content or process experts process experts and ownersand owners
Assembling your Assembling your team: Get the Right team: Get the Right PeoplePeople

Proficiencies required to Proficiencies required to perform PEperform PE
Quality improvement principles, Quality improvement principles, methods, and practicesmethods, and practices
– Numeric or statistical (basic) literacyNumeric or statistical (basic) literacy
Working knowledge of health care Working knowledge of health care delivery system; systems thinking delivery system; systems thinking
Knowledge of routine data sources to Knowledge of routine data sources to identify ethics quality gaps and baseline identify ethics quality gaps and baseline measuresmeasures
Ability to use or develop data tracking Ability to use or develop data tracking toolstools

Proficiencies Proficiencies – – continuedcontinued
Practical grasp of how to promote Practical grasp of how to promote sustained organizational changesustained organizational change
Knowledge of common ethics Knowledge of common ethics topics and concepts topics and concepts
Skill in moral reasoningSkill in moral reasoning

IE Performance Measures: IE Performance Measures: Preventive EthicsPreventive Ethics
Measure of Success FY10Measure of Success FY10
Preventive EthicsPreventive Ethics Each facility, with input from the IE Council, will Each facility, with input from the IE Council, will
complete a minimum of 2 preventive ethics QI complete a minimum of 2 preventive ethics QI cyclescycles
Each Network will address at least one Network Each Network will address at least one Network wide cross-cutting issue identified through IE wide cross-cutting issue identified through IE resources (e.g., Facility Workbooks, IE Staff Survey, resources (e.g., Facility Workbooks, IE Staff Survey, QI logs, ECWeb reports, recurrent cases)QI logs, ECWeb reports, recurrent cases)

Award Award Programs/Leadership Programs/Leadership MandatesMandates Prioritize high priority and cross Prioritize high priority and cross
cutting ethics quality gapscutting ethics quality gaps Teams chartered to address Teams chartered to address
ethics quality gapethics quality gap Disseminate results to foster an Disseminate results to foster an
organizational learning organizational learning environmentenvironment

Contact UsContact Us
www.ethics.va.govwww.ethics.va.gov– Download publicly available materialsDownload publicly available materials
Mary Beth FogliaMary Beth FogliaPreventive Ethics ManagerPreventive Ethics [email protected]@va.gov(206) 277-5121(206) 277-5121

Questions?