building an effective population health team: stepping towards the
TRANSCRIPT

Building an Effective Population Health Team: Stepping towards
the Triple AimAmy M. Sitapati, M.D.
Chief Medical Information Officer of Population HealthClinical Professor Department of MedicineUniversity of California San Diego Health

2
UC San Diego Health

AGENDA• The triple aim as it pertains to Population
Health• Roles, Team, Oversight and Governance• Scaling for value in the MACRA era• Continuous cohesion – gluing together
programs and resources
Culture, Incentives, Leadership, Management, Business Model,
Structure – Tackling local problems to build outcomes, operations, and
infrastructure
Image: Sandiego.org
Operational
Reporting Application
4
Working Towards the Triple AIM-Improving
www.ihi.org
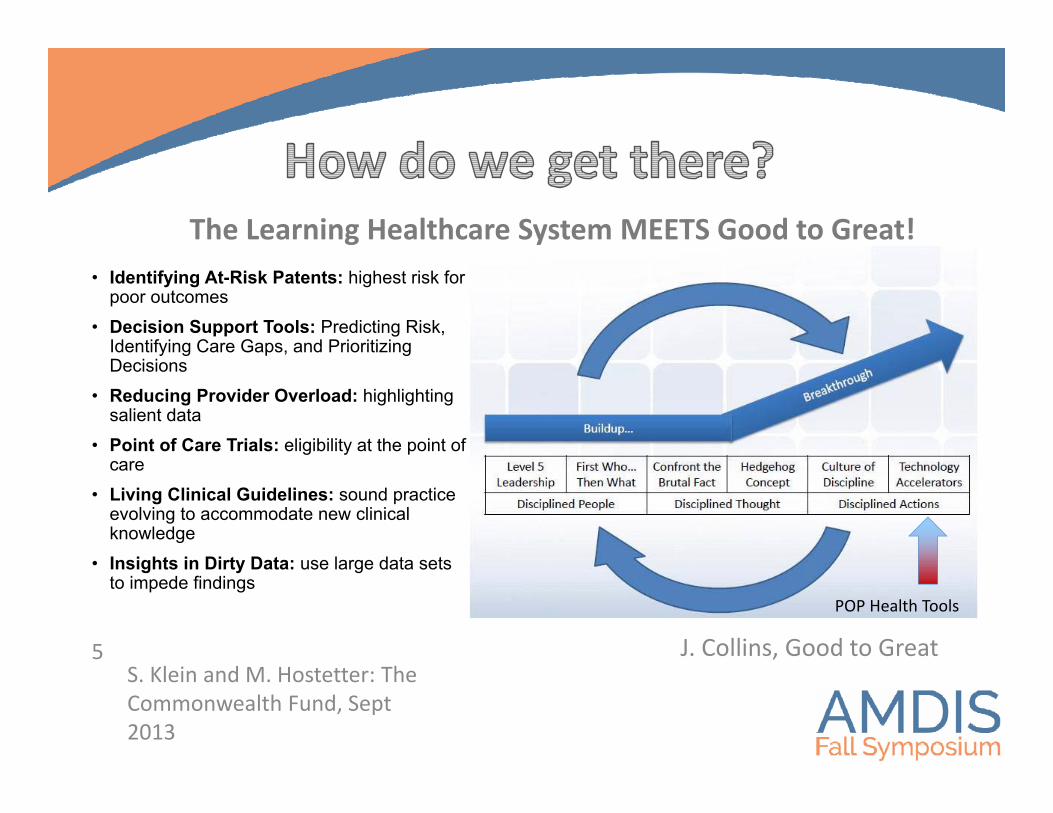
• Identifying At-Risk Patents: highest risk for poor outcomes
• Decision Support Tools: Predicting Risk, Identifying Care Gaps, and Prioritizing Decisions
• Reducing Provider Overload: highlighting salient data
• Point of Care Trials: eligibility at the point of care
• Living Clinical Guidelines: sound practice evolving to accommodate new clinical knowledge
• Insights in Dirty Data: use large data sets to impede findings
S. Klein and M. Hostetter: The Commonwealth Fund, Sept 2013
5 J. Collins, Good to Great
POP Health Tools
The Learning Healthcare System MEETS Good to Great!
• Care Management (Outreach Navigator)• Risk Acuity (Predict Risk)• Provider Decision Support (Disease Based Print Group)• Patient Centered Goals (Include Patients in their Care
MyChart)• Performance Review and Accountability (Dashboard)
6
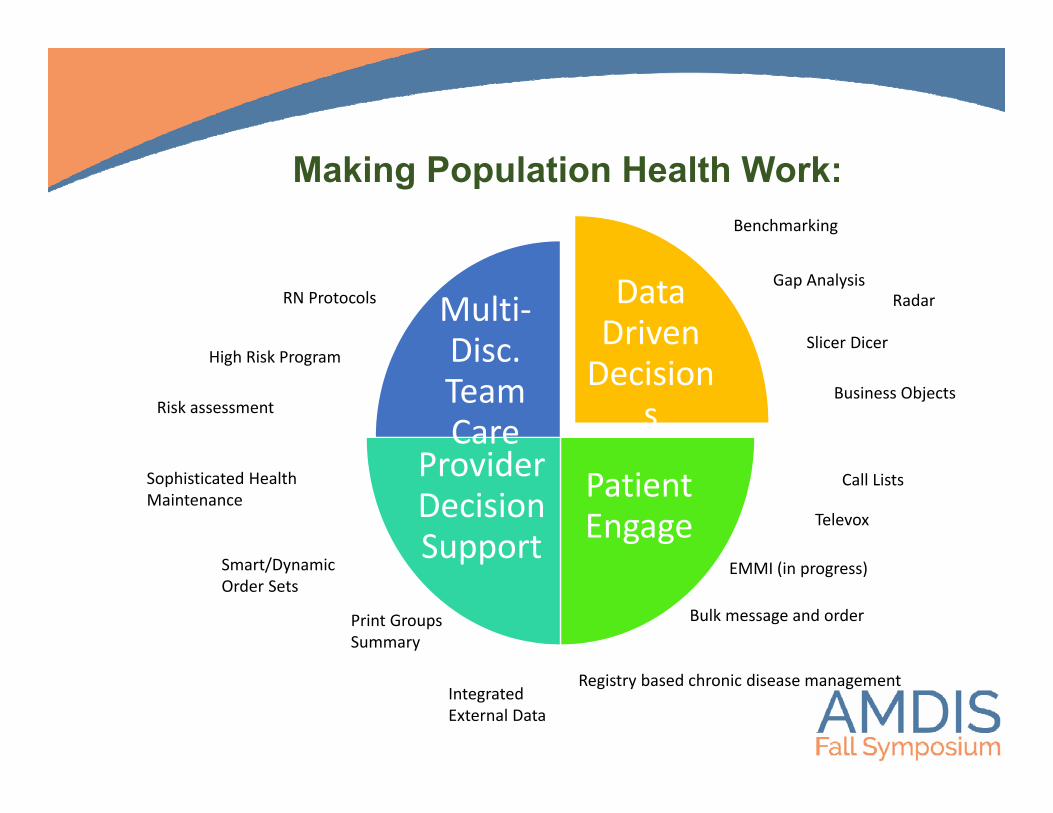
Making Population Health Work:
Data Driven Decision
s
Patient Engage
Provider Decision Support
Multi‐Disc. Team Care
RN Protocols
High Risk Program
Sophisticated HealthMaintenance
Smart/DynamicOrder Sets
Print GroupsSummary
Radar
Benchmarking
Gap Analysis
Call Lists
Televox
EMMI (in progress)
Bulk message and order
Registry based chronic disease management
Risk assessment
Slicer Dicer
Business Objects
IntegratedExternal Data
The STORY of our Journey Includes:
Sisters Jewel Thief Superheroes!Image: Pinterest
Population Health Team
Our Visionis to deliver outstanding population health through innovative use of the electronic health record
Our Mission is to create a healthier population through:· Actionable patient registries · Operational reporting for patient care and coordination· Tools that help patients and providers achieve health goals· Population-based performance measurement and quality improvement
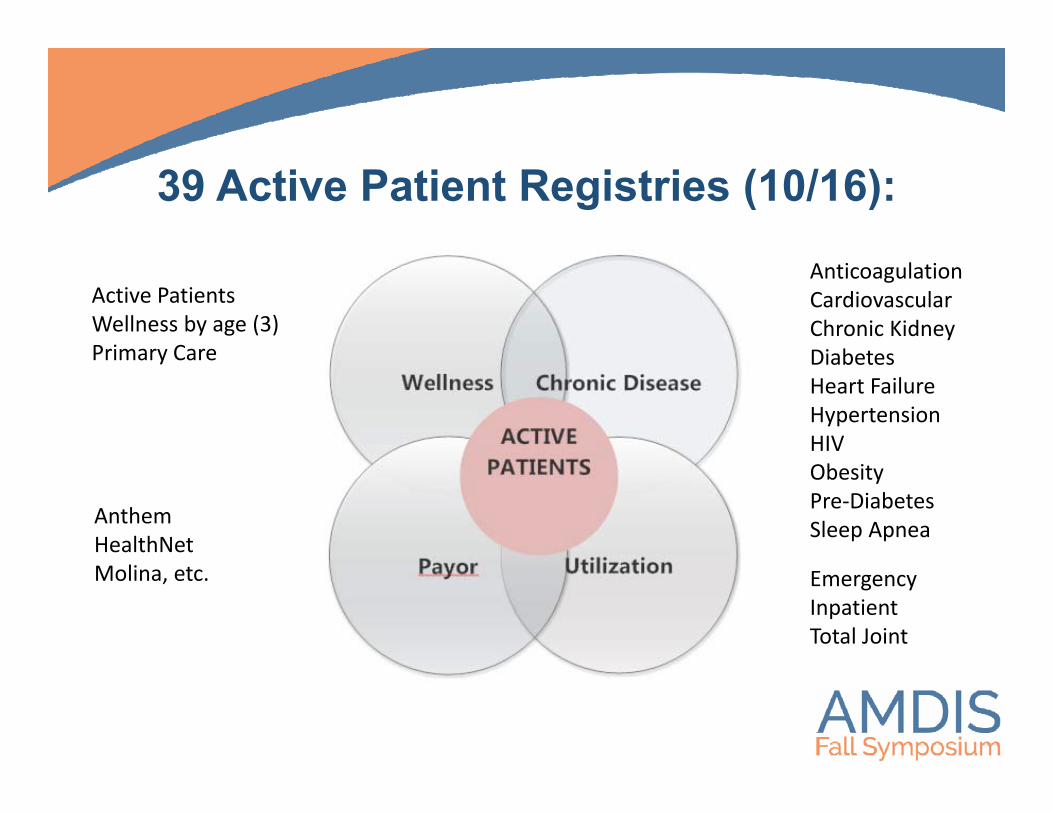
39 Active Patient Registries (10/16):
Active PatientsWellness by age (3)Primary Care
AnticoagulationCardiovascularChronic KidneyDiabetesHeart FailureHypertensionHIVObesityPre‐DiabetesSleep Apnea
EmergencyInpatientTotal Joint
AnthemHealthNetMolina, etc.
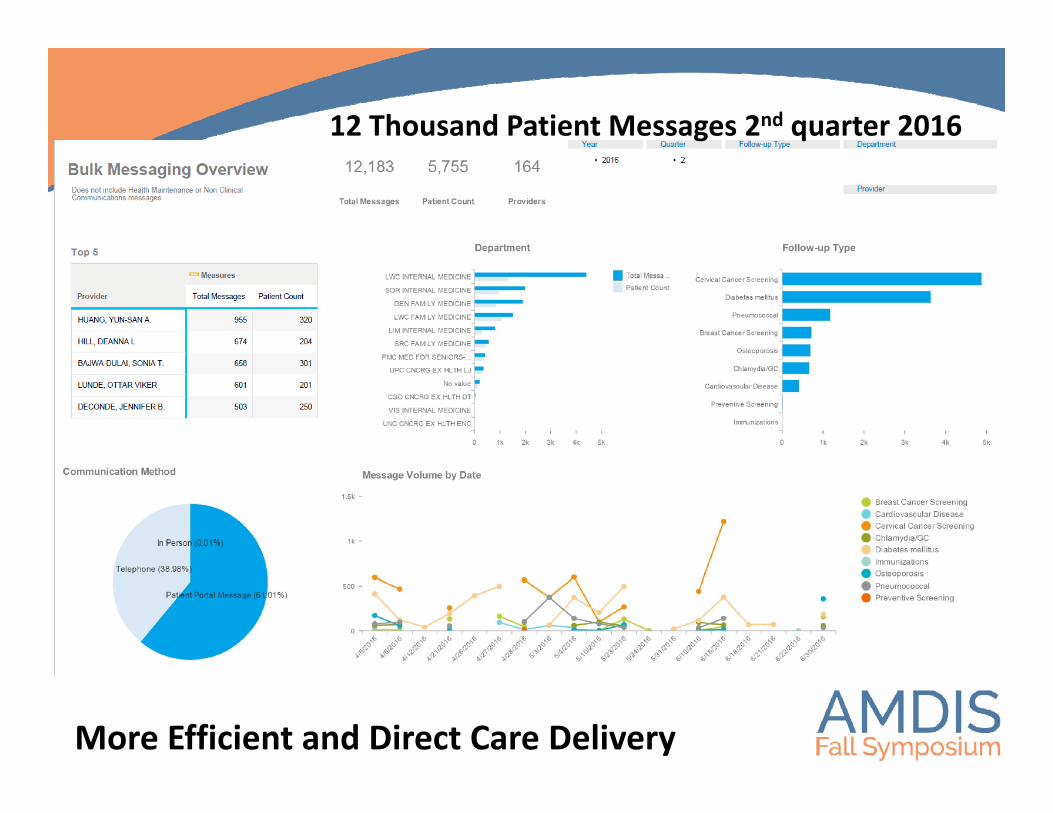
12 Thousand Patient Messages 2nd quarter 2016
More Efficient and Direct Care Delivery

• Develop Operational Teams that can implement change with accountability and governance
12
“who” Two Core Concepts for PEOPLE:
• Technical Teams should be cross-fit and diversely functional responsive to the operational needs

Governance “who decides”

Partial Overview of Governance“who decides”
PRIME Executive
PRIME Steering
Workgroups
ACO/RISK Executive
ACO Steering
Workgroups
CIN Executive
CIN Steering
Workgroups
Medical Group Quality
Division based QM & Managed Care Teams
Quality Council(Operations)
Physician Led ChampsBy domain area
UCI/UCSD Executive
Workgroup Steering
Workgroups
IS Clinical Council (Coming Soon)
Physician Informatics
Workgroups
Information Services Executive (IS)

Health Care Reform

0123456
Level
Level
16
Work on the right projectsConsider a matrix scoring
Average registry or risk score might take $50-100k
Level Patient #Healthcare worker # FTE Safety Quality/Value
Incentive/Risk ($)
1 <100 <50 Minimal Harm <5% or <25th % <1 k2 101‐1,000 50‐200 Mild Harm 5‐10% or 50th 1‐10 k3 1,001‐10,000 201‐500 Moderate Harm 11‐15% or 75th 10k‐100 k4 10,001‐100,000 501‐1,000 Significant Harm 16‐20% or 80th 100,k‐ 1 m5 >100,000 >1,000 Catastrophic >20% or 90th % >1m
Try to prioritize projects“what matters”
Scaling for Value with Forward Vision
PRIME P4P PQRS ACO & MSSP
Other
GE healthcare

Developing the Organizational Teams to Deliver better Care
18
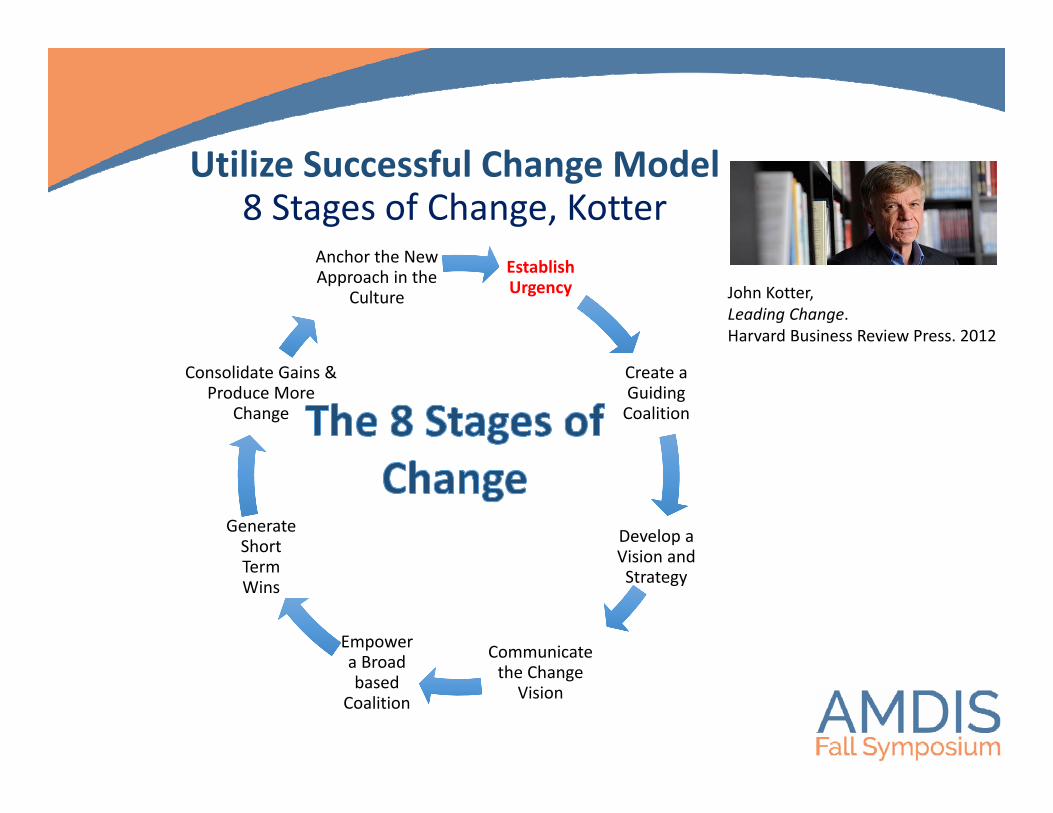
Utilize Successful Change Model8 Stages of Change, Kotter
Establish Urgency
Create a Guiding Coalition
Develop a Vision and Strategy
Communicate the Change
Vision
Empower a Broad based
Coalition
Generate Short Term Wins
Consolidate Gains & Produce More
Change
Anchor the New Approach in the
Culture John Kotter, Leading Change.Harvard Business Review Press. 2012
20
Operational: Supersize the Stakeholders:
expert to front line
A. Division Lead MD: Endo/MetabolicB. Primary Care Lead MDC. Managed Care RND. Pre‐diabetes stakeholder/sE. PharmDF. Diabetes EducatorsG. Patients/MyChart
Diabetes Educators
Pharmacists

Superheroes! Develop technical teams that excel.

EpicCare AmbulatoryEpic Inpatient
MyChartCadence
Healthy Planet
ClarityCrystalReporting WorkbenchRadarCaboodle/Star
Span the Clinical and Reporting Department/s
Physician Led: CMIO Population HealthClinical Analyst, Registry Reporting AnalystReporting Analyst, CIN Reporting Analyst
Clinical Systems Reporting
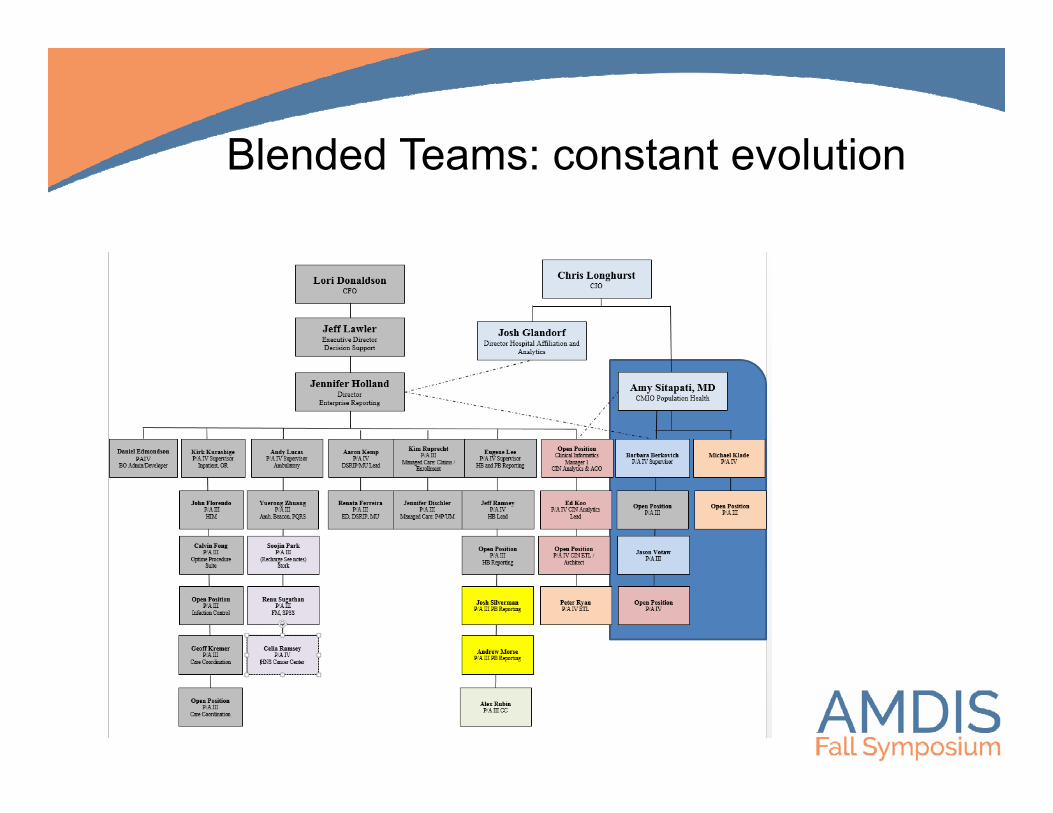
Blended Teams: constant evolution
Model “Swiss Cheese” –Integrated Pop Health Team
Population Health
Patient Portal /Ambulatory/HM
Managed Care/Care
Coordination
Dashboard & Reporting
Registry & Operational Reporting
Integrated Data Warehouse

Building an Olympic TeamNeed good structure!
Using version of Agile Scrum Methodology to share work

2 week SPRINT: Starts Fridays
(QOF)Finish line and Start line for
projects
FINISH LINE: 10 min demo of DONE each
analyst

START LINE: 1 hour of Project Planning

28
A Shared active work board for project work –SWIM LANES for active work
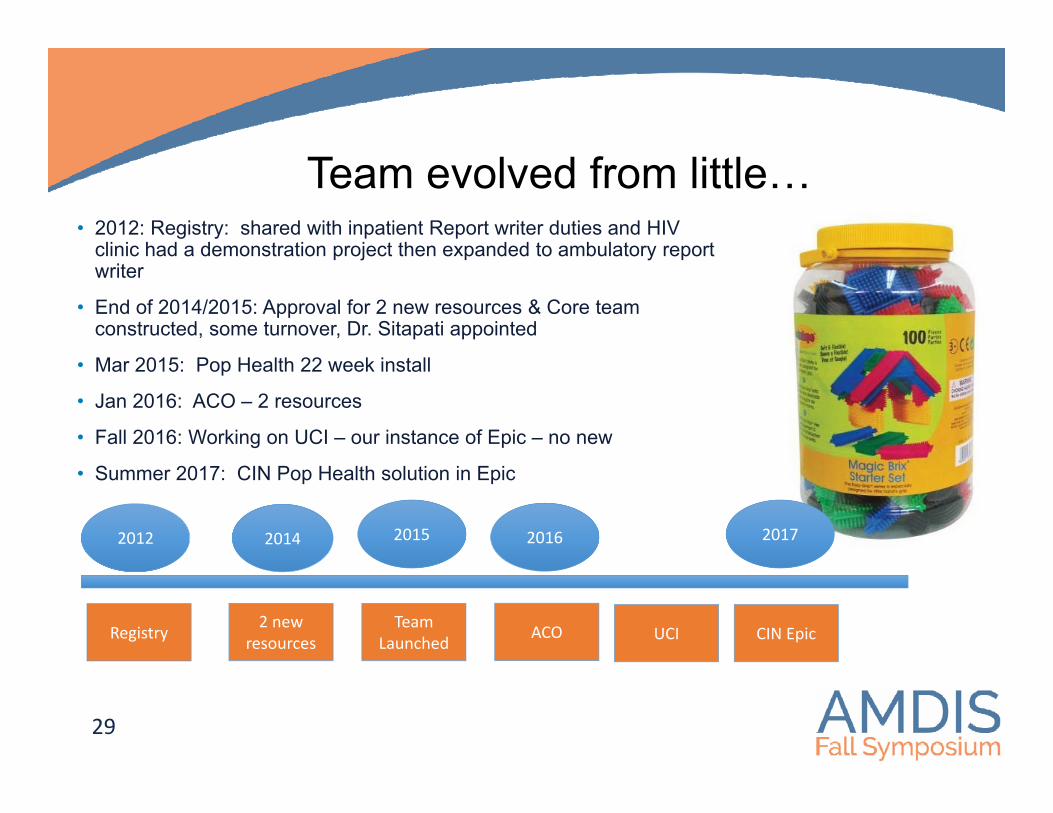
• 2012: Registry: shared with inpatient Report writer duties and HIV clinic had a demonstration project then expanded to ambulatory report writer
• End of 2014/2015: Approval for 2 new resources & Core team constructed, some turnover, Dr. Sitapati appointed
• Mar 2015: Pop Health 22 week install
• Jan 2016: ACO – 2 resources
• Fall 2016: Working on UCI – our instance of Epic – no new
• Summer 2017: CIN Pop Health solution in Epic
29
Team evolved from little…
2012 2014 2016
ACO
2015
Team Launched
2 new resources
2017
CIN EpicRegistry UCI

Sisters: Find new collaborators and partners
UC San Diego Clinically Integrated Network
Jewel Thief! Seek experts that you wouldn’t usually partner with
Leverage robust Research Infrastructure including-OMOP-Data Harmonization Experience
-Relationships

32
Challenges: Lots of Work! Needs
prioritization, vision, and strategy!training,
project management, right sizing,
organizational structure with growth, talent,
lexicons,clinical and technical
overlap

Value in patient outcomes:
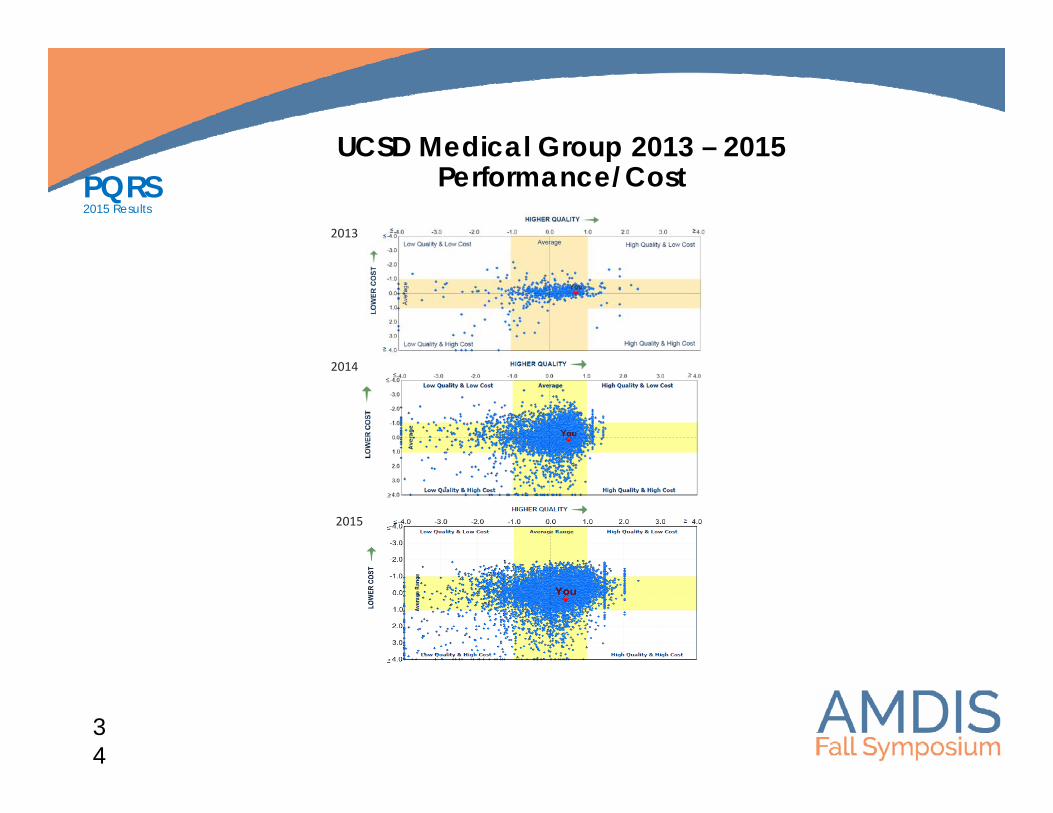
UCSD Medical Group 2013 – 2015 Performance/Cost
2013
2014
2015
PQRS2015 Results
34

PQRS2015 Results
35
PQRS GPRO Measures 2014 Rate 2015 Rate YoY Change
IVD User of Aspirin 87.43% 83.39% -4.04%
CAD-7 ACE or ARB Therapy 85.17% 84.03% -1.14%
HTN-2 Controlling High Blood Pressure 63.67% 62.79% -0.88%
PREV-12 Screening for Clinical Depression and Follow-Up Plan 22.83% 22.15% -0.68%
DM-2 A1c >9% Poor Control 11.59% 11.04% -0.55%
PREV-10 Tobacco Use Screening and Cessation Intervention 94.14% 94.29% 0.15%
PREV-5 Breast Cancer Screening 75.25% 75.82% 0.57%
PREV-7 Influenza Immunization 71.50% 72.21% 0.71%
CARE-2 Screening for Future Fall Risk 98% 99.51% 1.46%
PREV-9 BMI screening and follow-up plan 53.09% 55.14% 2.05%
HF Beta-Blocker Therapy for LVSD 94.67% 97.75% 3.08%
PREV-8 Pneumonia Vaccination 77.36% 81.37% 4.01%
PREV-6 Colorectal Cancer Screening 58.52% 65.63% 7.11%
PREV-11 Screening for High Blood Pressure and Follow-up Documented 26.43% 38.50% 12.07%
CARE-3 Documentation of Current Medications in the Medical Record n/a 81.33% N/A
DM-7 Diabetes Eye Exam n/a 50.33% NEW
MH-1 Depression at Twelve Months n/a 23.53% NEW
36
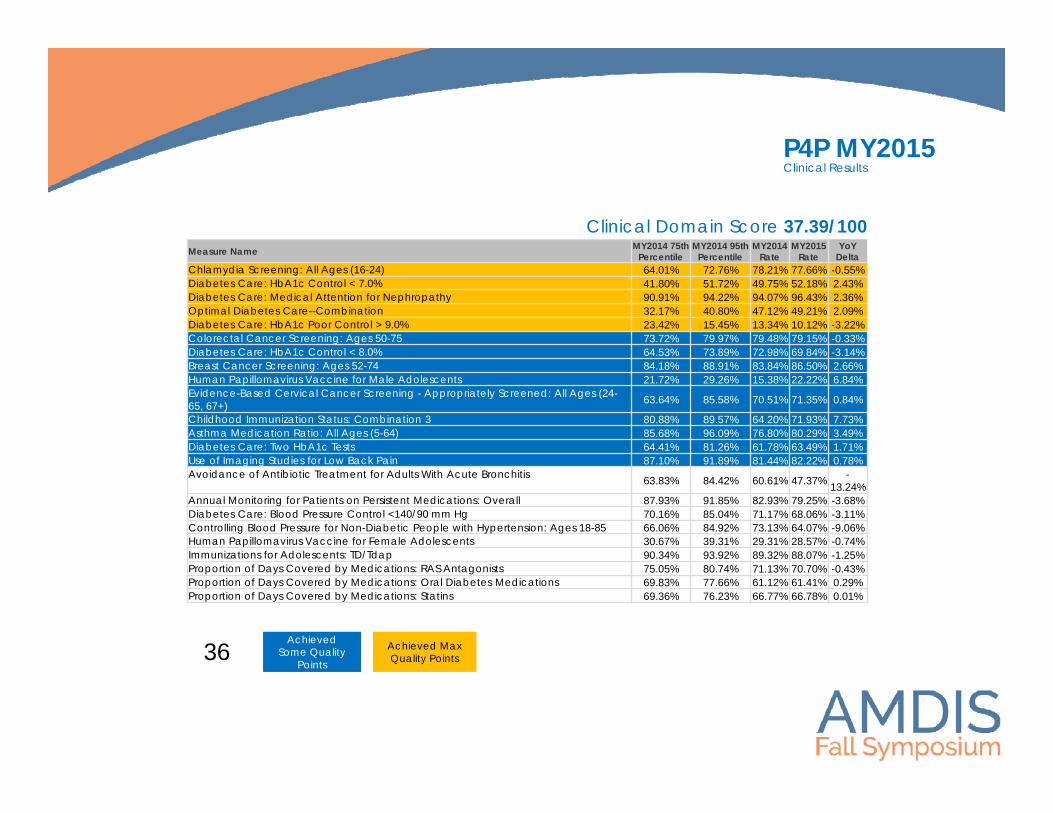
Clinical Domain Score 37.39/100
P4P MY2015 Clinical Results
Achieved Some Quality
Points
Achieved Some Quality
Points
Achieved Max Quality Points
Achieved Max Quality Points
Measure Name MY2014 75th Percentile
MY2014 95th Percentile
MY2014 Rate
MY2015 Rate
YoY Delta
Chlamydia Screening: All Ages (16-24) 64.01% 72.76% 78.21% 77.66% -0.55%Diabetes Care: HbA1c Control < 7.0% 41.80% 51.72% 49.75% 52.18% 2.43%Diabetes Care: Medical Attention for Nephropathy 90.91% 94.22% 94.07% 96.43% 2.36%Optimal Diabetes Care--Combination 32.17% 40.80% 47.12% 49.21% 2.09%Diabetes Care: HbA1c Poor Control > 9.0% 23.42% 15.45% 13.34% 10.12% -3.22%Colorectal Cancer Screening: Ages 50-75 73.72% 79.97% 79.48% 79.15% -0.33%Diabetes Care: HbA1c Control < 8.0% 64.53% 73.89% 72.98% 69.84% -3.14%Breast Cancer Screening: Ages 52-74 84.18% 88.91% 83.84% 86.50% 2.66%Human Papillomavirus Vaccine for Male Adolescents 21.72% 29.26% 15.38% 22.22% 6.84%Evidence-Based Cervical Cancer Screening - Appropriately Screened: All Ages (24-65, 67+) 63.64% 85.58% 70.51% 71.35% 0.84%
Childhood Immunization Status: Combination 3 80.88% 89.57% 64.20% 71.93% 7.73%Asthma Medication Ratio: All Ages (5-64) 85.68% 96.09% 76.80% 80.29% 3.49%Diabetes Care: Two HbA1c Tests 64.41% 81.26% 61.78% 63.49% 1.71%Use of Imaging Studies for Low Back Pain 87.10% 91.89% 81.44% 82.22% 0.78%Avoidance of Antibiotic Treatment for Adults With Acute Bronchitis 63.83% 84.42% 60.61% 47.37% -
13.24%Annual Monitoring for Patients on Persistent Medications: Overall 87.93% 91.85% 82.93% 79.25% -3.68%Diabetes Care: Blood Pressure Control <140/90 mm Hg 70.16% 85.04% 71.17% 68.06% -3.11%Controlling Blood Pressure for Non-Diabetic People with Hypertension: Ages 18-85 66.06% 84.92% 73.13% 64.07% -9.06%Human Papillomavirus Vaccine for Female Adolescents 30.67% 39.31% 29.31% 28.57% -0.74%Immunizations for Adolescents: TD/Tdap 90.34% 93.92% 89.32% 88.07% -1.25%Proportion of Days Covered by Medications: RAS Antagonists 75.05% 80.74% 71.13% 70.70% -0.43%Proportion of Days Covered by Medications: Oral Diabetes Medications 69.83% 77.66% 61.12% 61.41% 0.29%Proportion of Days Covered by Medications: Statins 69.36% 76.23% 66.77% 66.78% 0.01%

37
MUHIT Domain Score 86.82/100
P4P MY2015 Patient Experience & Meaningful Use Results
Patient Experience Domain Score 25/100Measure Name
MY2014 75th
Percentile
MY2014 95th
Percentile
MY2014 Rate
MY2015 Rate YoY Delta
Doctor-Patient Interaction Composite 80.90% 84.67% 84.21% 81.30% -2.91%Coordination of Care Composite 63.38% 68.21% 68.35% 65.55% -2.80%Overall Ratings of Care Composite (Rating of Doctor & Rating of All Healthcare) 70.79% 75.30% 75.98% 73.21% -2.77%Health Promotion Composite (One-Year) 64.96% 71.52% 65.49% 59.46% -6.03%Office Staff Composite 72.92% 76.74% 74.85% 69.82% -5.03%Timely Care and Service Composite 59.96% 64.42% 55.55% 55.69% 0.14%
Measure Name MY2014 Rate MY2015 Rate YoY Deltae-Measure: Controlling High Blood Pressure 67.85% 58.10% -9.75%e-Measure: Controlling High Blood Pressure (Percent Reportable) 100.00% 90.91% -9.09%e-Measure: Screening for Clinical Depression and Follow-up 19.15% 3.57% -15.58%e-Measure: Screening for Clinical Depression and Follow-up (Percent Reportable) 100.00% 90.91% -9.09%Percent of Providers Paid Meaningful Use Incentive by Medi-Cal or CMS 97.65% 86.00% -11.65%
Achieved Some Quality
Points
Achieved Some Quality
Points
Achieved Max Quality Points
Achieved Max Quality Points
• Defining modifiable factors that occur before new EVENT OUTCOMES through chart review
• What do I predict?
38
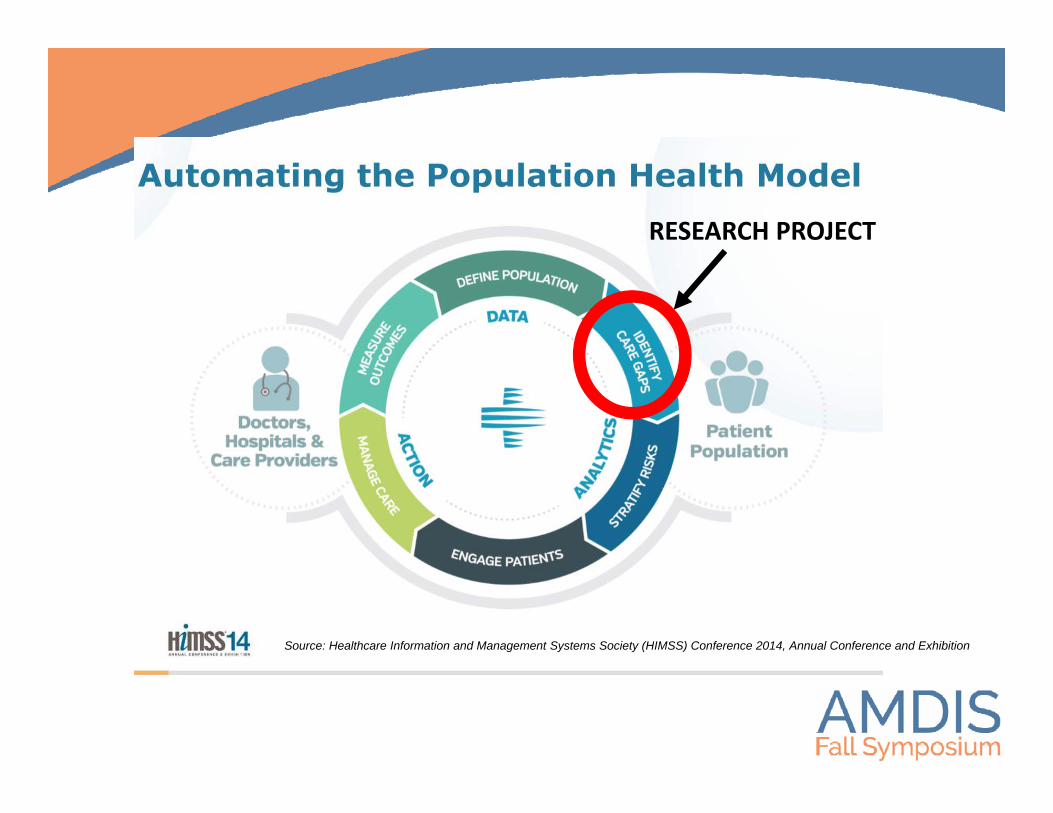
RESEARCH PROJECT
Source: Healthcare Information and Management Systems Society (HIMSS) Conference 2014, Annual Conference and Exhibition

Active in healthcare system
Disease/ risk factor recognition
Disease/ risk factor control
Disease/ risk factor treatment
CARE GAPS IN CVD RISK MANAGEMENT
Missing visitsMissing lab tests
Pill burdenCompliance
Tailoring Adequate dosing
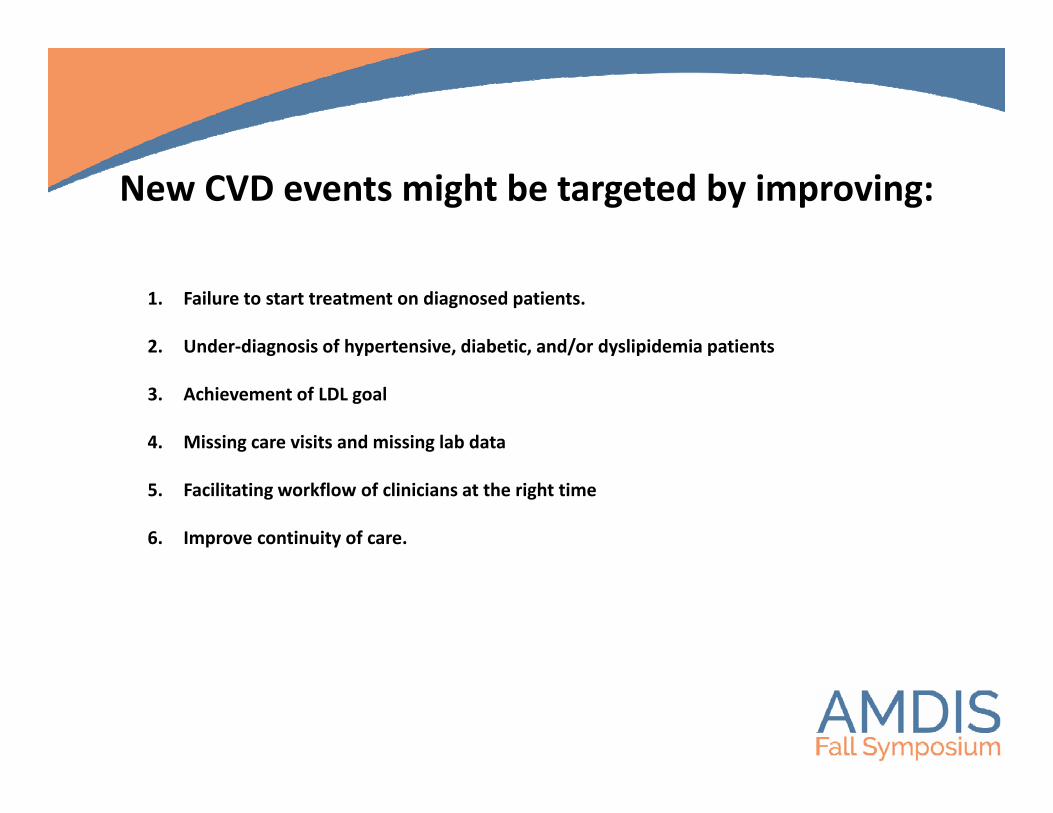
New CVD events might be targeted by improving:
1. Failure to start treatment on diagnosed patients.
2. Under‐diagnosis of hypertensive, diabetic, and/or dyslipidemia patients
3. Achievement of LDL goal
4. Missing care visits and missing lab data
5. Facilitating workflow of clinicians at the right time
6. Improve continuity of care.

Become by intersecting , with , and
PASSION
BEST in the world
Makes/Saves Money
J. Collins, Good to GreatA. Flynn et.al. Tell it Like it Seems 2015.42
15% Healthcare spend is waste
Aim for high quality
Our passion is to change patient lives
UC San Diego HealthAmy Sitapati, MDContact Phone: 858-249-0112Email: [email protected]