by anita wiese, m.a., ccc-slp and audra a. amreihn, m.a ... · pdf fileone bite/sip at a time...
TRANSCRIPT
By Anita Wiese, M.A., CCC-SLP and
Audra A. Amreihn, M.A., CCC-SLP
} SLP’s are trained to: ◦ assess and treat a variety of diagnoses that cause
communication and swallowing disorders
◦ work with families and staff to improve communication skills and decrease the risk of aspiration caused by the swallowing disorder
} Dysphagia means the difficulty or inability to swallow
} There are 3 phases: oral, pharyngeal and esophageal
} The Speech-Language Pathologist’s main focus is the first two phases
} If there is a malfunction with any of these 3 phases the person will have a swallowing disorder or dysphagia
} Oral Phase ◦ Lips ◦ Teeth ◦ Tongue ◦ Cheeks ◦ Hard and Soft palate ◦ Velum
} Pharyngeal Phase ◦ Pharyngeal muscles ◦ Valleculae ◦ Epiglottis ◦ Pyriform Sinuses ◦ Upper Esophageal
Sphincter
} Lip seal to keep food in the oral cavity } Adequate dentition for mastication } Tongue mobility and coordination for bolus
control and transportation posteriorly } Adequate jaw mobility to assist in
mastication, bolus manipulation and transport
} Cheek tone to reduce pocketing } Soft palate moves superiorly to close off the
nasal cavity
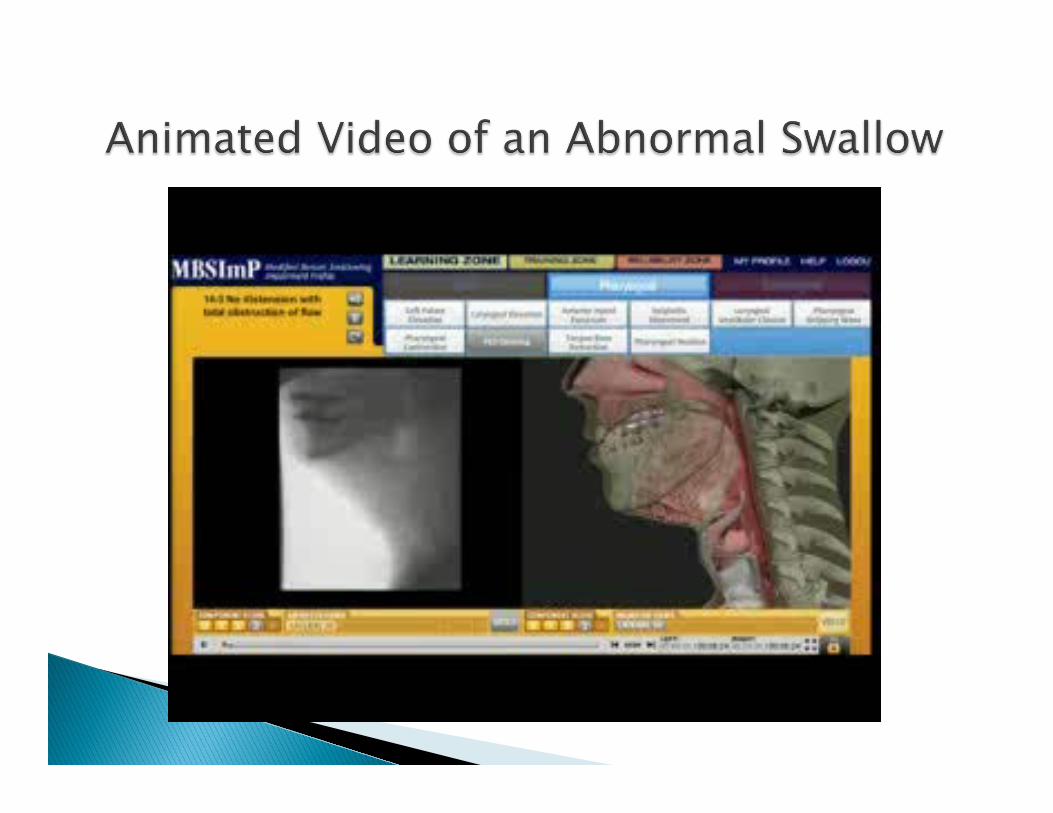
} The bolus passes into the pharynx where the pharyngeal constrictor muscles squeeze to propel the bolus as the posterior tongue elevates to invert the epiglottis to close off the airway
} Simultaneously the vocal folds close and the larynx raises up and tilts forward providing extra closure of the airway
} The upward and forward movement of the larynx is what helps to open the cricopharyngeal muscle (UES) in order for the bolus to pass into the esophagus.
} Intellectual and Developmental Disabilities in conjunction with neurological and psychological disorders
} Down’s Syndrome } Cerebral Palsy } Spina Bifida } Stroke } Dementia } Deconditioning and Debility } Prolonged intubations } Lung/respiratory disorders } Cancer with radiation to the surrounding swallowing
mechanism } Neurological disorders } And many more…
} Open mouth while swallowing } Head thrown back for swallowing } Pocketing of food } GERD } Tongue thrust } Prolonged chewing } Abnormal length of time to complete meals } Coughing or choking on their own saliva } Excessive drooling } Pneumonia } Repeated swallowing } Delay in swallowing } Holding food in mouth for too long
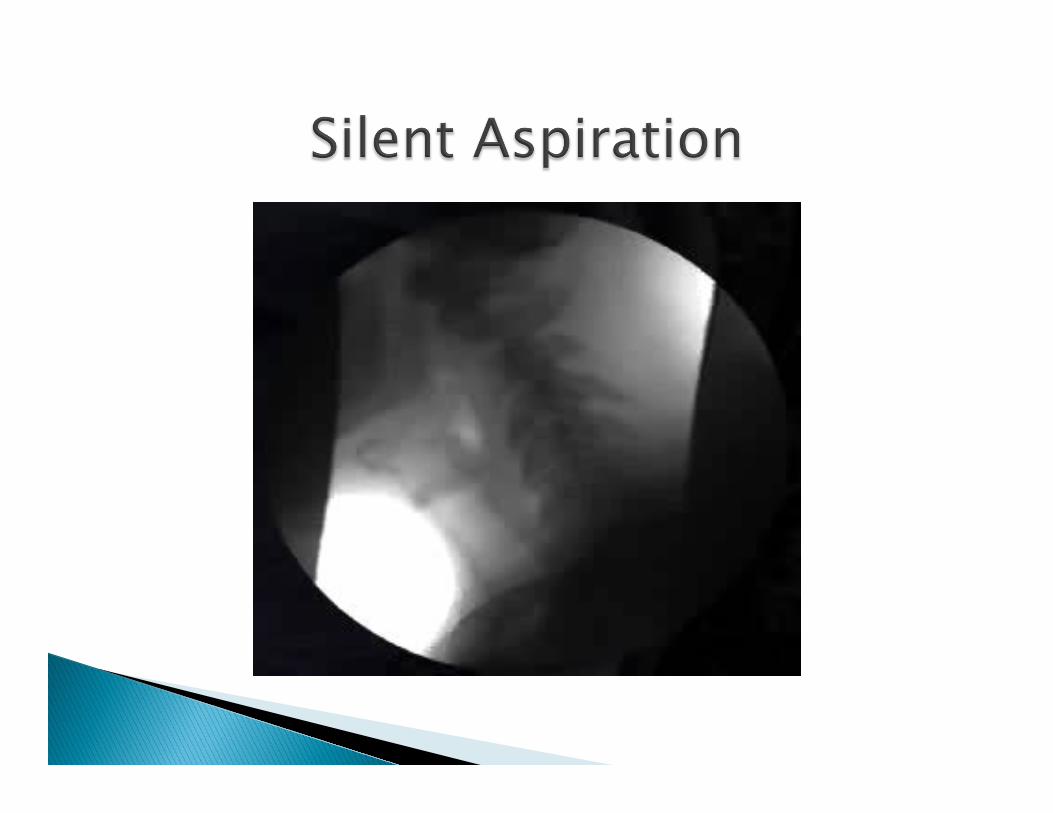
} Aspiration is food and liquid that enters the airway below the vocal folds from either an impaired swallow or refluxing contents from the esophagus or stomach.
} Silent aspiration is the same as above, however, the individual does NOT cough or choke when contents enter the airway… silent
} Coughing } Choking } Elevated temperature } Increased WBC } Lung sound changes typically in the right
lower lobe. } Chest x-ray may not show aspiration for up
to 72 hours after the aspiration event. } Aspiration can occur in the left lower lobe if a
person typically leans to the left.

} Enlarged tongue } Short frenulum (tongue tied) } Cleft palate } Vaulted palate } Lack of tone in the lips, tongue and cheeks } Poor dentition } Sensory issues for texture } Lack of sensory awareness of the bolus
} Bedside/Clinical Swallow Evaluation
} Modified Barium Swallow Study
} Dysphagia Therapy/Swallow Strategies/Diet Modifications
} Traditional dysphagia therapy } Diet modification analysis to food textures
and liquids } Swallowing strategies or techniques } NMES (Neuromuscular Electrical Stimulation)
Vital Stimulation } DPNS (Deep Pharyngeal Neural Stimulation)
} Oral care is important to: ◦ Keep the mouth moist and clean ◦ Keep bacteria in saliva from being aspirated ◦ Keep food particles from being aspirated after
meals } A client who is on thickened liquids is at risk
for dehydration and dry mouth, therefore, oral care is especially important.
} Optimal body positioning is having a client sitting up at 90 degrees and head in neutral position.
◦ If in bed, boost or pull the client up toward the
head of the bed, then raise the head of the bed. ◦ If in chair, reposition the client so that the hips are
flexed at 90 degrees.
} This position maximizes: ◦ Bolus control in the oral cavity ◦ Anterior to posterior movement of the bolus ◦ Cricopharyngeal opening ◦ Bolus propulsion into the esophagus
} Meals at the table } Tilt the wheel chair } Recline bed for a person with kyphosis } Place pillow behind the head } Straws versus no straws } Chin tuck versus head in neutral position } Soft cervical collar or neck brace
} If head is not in proper position the risk of aspiration may increase.
◦ When airway is lengthened the muscles used to
close off the airway are less effective. ◦ Individuals with Cerebral Palsy, Tardive Dyskinesia,
etc. have a tendency to be in constant motion and traditional head placement may be too difficult… in that case texture modifications may need to be considered.
} If the person is reclined, reflux symptoms may increase. ◦ Be aware if medications are working properly ◦ Stay upright for at least 60 min after meals ◦ Smaller more frequent meals may need to be provided
} Other conditions that may cause or increase reflux: ◦ hiatal hernia ◦ Medications ◦ Poor esophageal motility.
� These can also be affected by poor positioning.
} 5-6 small meals } One bite/sip at a time } Alternate solid then
liquid } Minimize distractions } Small bite/sip size } Reduce rate of intake } Large handled utensils
} Chin tuck } Swallow hard } Hold then swallow } Swallow twice } Clear the throat or
cough and re-swallow

} Provale Cup ◦ 5cc and 10 cc bolus size ◦ Works with thin and nectar ◦ Increases independences ◦ Decreases cues ◦ One, two or no handles
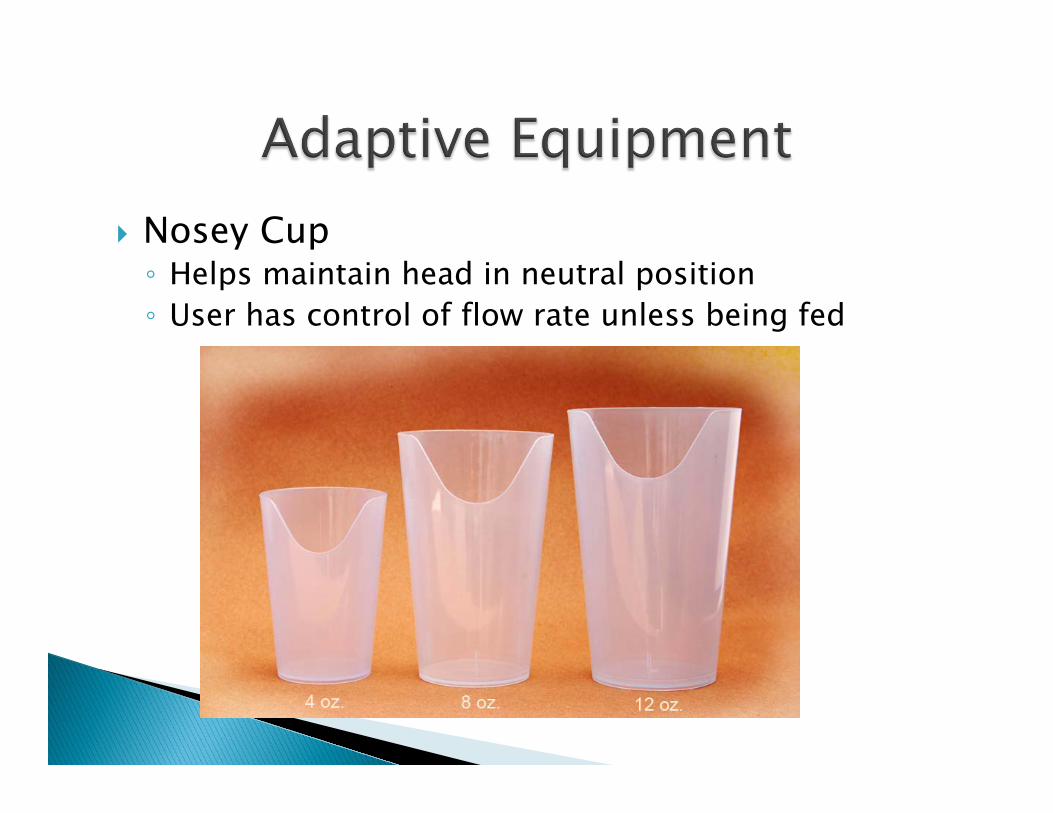
} Nosey Cup ◦ Helps maintain head in neutral position ◦ User has control of flow rate unless being fed

} Novo Cup ◦ User is in control of flow
rate when cap plug is in place ◦ Ideal for clients with
restricted head and neck movements ◦ Must be able to suck
through a straw

} Maroon spoon } Baby spoon with long handle } Cocktail fork } Weighted spoons } Foam handles for utensils } Weights on wrists
} Puree Diet: ◦ Smooth in texture ◦ No chewing required. ◦ Easy to form and swallow bolus. ◦ Examples: custard, blended yogurt, oatmeal, cream
of wheat and pureed foods.
} Ground Diet: ◦ All food is ground into tiny pieces and should be
moist. Chopped Diet: ◦ All food is chopped/cut into small pieces.
} Mechanically Altered Diet: Ground Meats Diet: ◦ Moist ◦ Soft-textured foods ◦ Easily formed into a bolus. ◦ Some chewing is required. ◦ Examples: fruit with yogurt, soft veggies, canned
fruit, lasagna, macaroni and cheese, moist ground meats, soft flaky fish.
} Regular Diet: ◦ No food texture restrictions. Example: raw
vegetables, meat, crunchy foods, nuts etc.
} Thin Liquid: ◦ It will not coat the spoon. ◦ It moves very quickly. ◦ It is anything that will liquefy in the mouth within a few
seconds. Examples: water, tea, hot chocolate, coffee, milk, juice, milkshakes, ice cream, sherbet, gelatin etc.
} Nectar Thick Liquid: ◦ Liquid will coat the spoon or sides of cup/glass. ◦ It will pour freely in small rapid drops. ◦ If spilled, it will splash. Examples: tomato juice, plain
nectars, creamed soups, smoothies made with yogurt, any liquid with the correct amount of thickener added.
} Honey Thick Liquids: ◦ Will pour more slowly like honey from a honeycomb. ◦ A straw will stand up. ◦ If spilled, it will spread rather than splash. Examples:
any beverage correctly thickened to honey-thick consistency
} Pudding Thick Liquid: ◦ It will fall off the spoon in a glob. ◦ If the cup is turned upside down, the beverage should
still move. If it doesn’t it is too thick! Examples: any beverage correctly thickened to pudding-thick consistency.
} If too little or too much powder is used it will not be accurate.
} Stir and pour the thickener at the same time
to avoid getting lumps. } Stir briskly for 30 to 45 seconds. ◦ Let set for 3 minutes for water, coffee, tea, juice. ◦ 10 minutes for milk, creamed soups, Ensure, Boost.
◦ Use the correct amount of thickener. ◦ Pour and stir at the same time. ◦ Let set for the allotted time. ◦ Have all the required thickener ready before you
start adding it to the beverage. (lumps) ◦ Liquid medications need to be thickened. ◦ When thickening soda only add a small amount of
thickener to dissipate some of the carbonation. ◦ Place thickener in cup before adding supplement.
(lumps) ◦ Stir beverages one more time before serving.
} Chill the beverage ahead of time. } Add ice to the beverage to chill, remove
before thickening. } Add lemon or lime juice flavoring to water. } Do not over thicken. } Add ginger ale to juices. } For a tasty treat make Kool-Aid, add
thickener and then freeze into popsicles.
} Beverages have been known to loose their thickness over time for no known reason. ◦ Soda pop ◦ Warm liquids ◦ Water � Irrespective of type of thickener
} Supplements require extra time to thicken. } Enzymes in saliva can break down thickeners
and some foods. (wipe spoon)
} Thickened liquids allow for normal hydration } Digestible } Doesn’t bind fluid } 98% of free water is released after consumption } Offer beverages through out the day } Offer foods with high water content such as: ◦ carrots, broccoli, cantaloupe, watermelon, peaches,
strawberries, oranges, grapes, apples, blueberries, kiwi, pears, pineapple, plums, cabbage, cooked pasta, kidney beans. � These items need to be pureed and thickened.
*made w/Xanthan gum More natural flavor
} Thick-It } Thick-It 2 concentrated } ThickenUp } ThickenUP Clear* } Simply Thick (gel) } Thick & Easy } Thick & Easy Clear* } Thik & Clear (Cellulose
gum, more natural flavor) } Hydra-aid (gel) } AquaCare H2O* } Aqua Thick
} Baby cereal } Instant pudding } Jell-O } Pureed fruit in juice } Dehydrated potato
flakes } Bread crumbs } Prethickened liquids ◦ Novartis, Sysco,
Walgreens, CVS, WalMart
} The following recipe is good for clients with esophageal scarring, hiatal hernia and dysmotility issues. ◦ Box of Jell-O according to package directions ◦ Refrigerate until it begins to gel ◦ Remove from fridge - add a ¼ cup of cold liquid for
every cup of Jell-o the recipe makes ◦ Mix and refrigerate ◦ Client eats bite of their food, swallow, then bite of
slick diet } May add thickener during first step
} There are many medications that may affect the swallow function from the oropharyngeal to the esophageal phase.
◦ Anti anxiety/Benzodiazepines drugs ◦ Antipsychotic/Neuroleptic drugs ◦ Antiepileptic drugs ◦ Narcotics ◦ Muscle relaxants
} Multiple medications can cause dry mouth ◦ give sips of water before giving medications or
meal. � ACE inhibitors, anti-nausea, antihistamines and
decongestants, calcium channel blockers, diuretics, antidepressants
} Medications not given with enough water can lay in the esophagus and cause damage
� antibiotics, aspirin, iron pills, bronchodilators, NSAID’s, potassium supplements, vitamin C
◦ Dry mouth – food sticks at base of tongue, throat and possibly the esophagus. ◦ Muscle impairments in the face and tongue leading
to discoordinated swallows such as Tardive Dyskinesia ◦ Reflux that can cause damage to the peristaltic
movement of the esophagus ◦ Lethargy (increases risk for aspiration, dehydration
and poor nutrition)
} Client is always awake and alert for all meals and medication passes
} Oral hygiene } Proper body and head positioning for the
individual client } Provide proper diet texture and liquid
consistency } Follow any swallow strategies } Plenty of water to wash medications into the
stomach } Conduct a quarterly review of medications
} Radionz. (2010, August 9). The Intra-Swallow Aspiration [Video file]. Retrieved from http://youtu.be/1sFNMk87558
} Northern Speech. (2012, March 29). MBSImP Sample Animation: Penetration & Aspiration [Video file]. Retrieved from http://youtu.be/sowo87vxxxM
} Killphil08. (2012, January 26). Dysphagie [Video file]. Retrieved from http://youtu.be/BevsLki9IU8
} Griffin, Maggie. (2012, November 19). Swallow Inservice: If You Could See What I See. [Video file]. Retrieved from http://youtu.be/3XkkBvJ_cYo
} Alanswatches. (2013, January 2). Aspiration. [Video file]. Retrieved from http://youtu.be/huZ6ymeKFd4
} Ferguson, Neina. (2011, May 25). Normal Swallow. [Video file]. Retrieved from http://youtu.be/Cwy5Wfdf8nY
} Cork, Alejandra. (2012, July 17). Swallowing. [Video file]. Retrieved from http://youtu.be/pNcV6yAfq-g
} Logemann, J. A. (1997) Evaluation and Treatment of Swallowing Disorders. Austin, TX: Pro-Ed.
} Balzer, KM, PharmD, “Drug-Induced Dysphagia”, International Journal of MS Care, page 6, Volume 2 Issue1, March 2000. (http://www.mscare.com/a003/page_06.htm)
} http://www.ct.gov/dds/lib/health/attacha_med_dysphagia_swallowing_risks.pdf.
} http://www.speechmedconsults.com/medications---affecting-swallowing.html
} Slick Jell-O recipe http://dysphagia.com/maillist/2009-May/msg00013.html
} Dysphagia Resource Center www.dysphagia.com