by: jeanette caddell, rn - alabamanurses.org · gillespie bm, chaboyer wp, mcinnes e, kent b,...
TRANSCRIPT
Evidence Based Practice Pressure Ulcer
Prevention Strategies: To Reposition or
Turn
By: Jeanette Caddell, RN
No Conflict of Interest
I have received no support or funding for this
presentation and bibliography will be provided at
the end of the presentation.
Objectives
At the completion of the presentation participants will:
Be able to identify EBP pressure ulcer prevention strategies.
Be able to verbalize the importance of a pressure ulcer prevention
program.
PICOT Question
How does repositioning or turning the client with
decreased mobility at frequent intervals as compared to
not repositioning or turning reduce the development of
pressure ulcers over a 90 day period?
Thesis Statement
Implementation of repositioning or turning will prevent
development of pressure ulcers along with providing
incontinent care, proper nutrition, and skin assessments.
BACKGROUND
Pressure ulcers (PU) common findings in healthcare
Occur when pressure is applied to an area for long periods of time
Staged from 1-4 with stage 1 being the least worst and 4 being the
worst
Measured in centimeters (cm)
Now called Pressure Injury
Stage 1
Non-blanchable erythema of intact skin
Skin is discolor or dark
Color doesn’t return when pressure is applied

Stage 1
Stage 2
Partial-thickness skin loss with exposed dermis
Similar to an abarasion
Top layer of skin isn’t present
May have a intact blister present

Stage 2
Stage 3
Full-thickness skin loss
Top layer of skin is removed
Fatty tissue is visible

Stage 3

Stage 4
Full-thickness skin and tissue loss
Worst of the worst
All layers of the skin are removed
Bone, ligament, or muscle may be visible

Stage 4

Pressure Ulcers/Injury

Significance
In critically ill infants and children is 18% to 27%
3.55 million hospital admissions in Australia each year 10% or
more will develop an ulcer
Estimated cost to treat full thickness PU is about $70,000
Yearly cost to treat PU in U.S. is about $11 billion
Proposed Interventions
Implemented at a skilled nursing home w/ licensed nursing staff
Repositioning or turning every 2 hours
Side to side to back
Even hours turn
90 day intervention
Complete head to toe assessment each shift
Incontinent care after each incontinent episode
Pressure reduction mattress
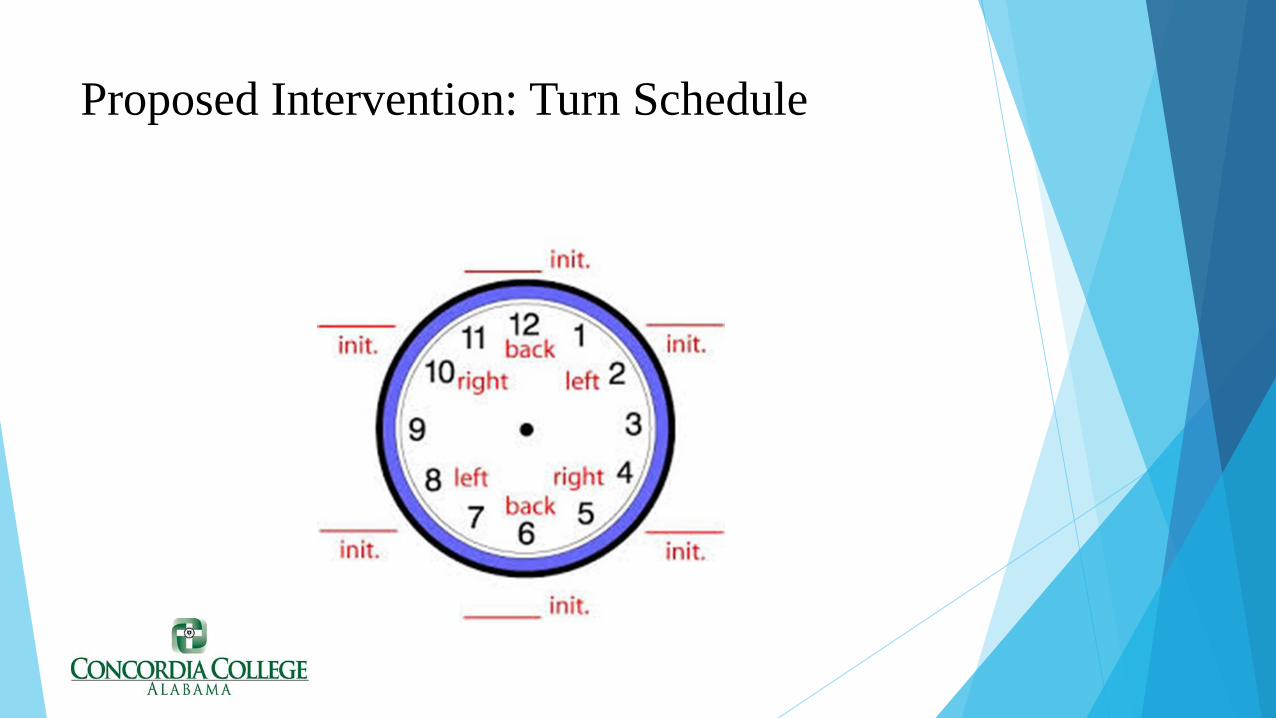
Proposed Intervention: Turn Schedule

Methods
Documentation of meal intake each meal
Offer supplement if refused meal or oral intake less than 50%
Documentation of fluid intake every shift
Skin assessment
Provide incontinence care
Ethical Considerations
Obtain signed consent forms
Privacy of clients
No harm to clients

Pressure Ulcer Module

Pressure Ulcer Module

Examples of Measurement

Examples cont.
Importance of Preventing Pressure Ulcers
It puts the client at risk for infection
Increases client’s length of stay
Decreases client’s life expectance
Perceives the facility as an unfit place of business
Increases costs at healthcare facility
Possibility of survey by Joint Commission or State


Bibliography Berloqwitz, D., VanDeusen Lukas, C., Parker, V., Niederhauser, A., Silver, J., Logan, C., Ayello, E., Zulkowski,
K. (2014). Preventing pressure ulcers in hospitals. Agency for Healthcare Research and Quality. https://www.ahrq.gov/professionals/systems/hospital/pressureulcertoolkit/index.html
Nancy Bergstrom, N. (2013). Repositioning as a pressure ulcer prevention strategy: a multi-site clinical trial. http://www.npuap.org/wp-content/uploads/2012/01/NPUAP.Keynote.2.2013.all_edits.2.3.13_1.pdf
Gillespie BM, Chaboyer WP, McInnes E, Kent B, Whitty JA, Thalib L. (2013) Repositioning for pressure ulcer prevention in adults. Cochrane Database of Systematic Reviews 2014, Issue 4. Art. No.: CD009958. DOI: .10.1002/14651858.CD009958.pub2
Hall, K and Clark, R. (2016). A prospective, descriptive, quality improvement study to investigate the impact of a turn-and-position device on the incidence of hospital-acquired sacral pressure ulcers and nursing staff time needed for repositioning patients. Ostomy Wound Management 2016; 62(11):40–44. http://www.o-wm.com/article/prospective-descriptive-quality-improvement-study-investigate-impact-turn-and-position
Manzano F1, Colmenero M, Pérez-Pérez AM, Roldán D, Jiménez-Quintana Mdel M, Mañas MR, Sánchez-Moya MA, Guerrero C, Moral-Marfil MÁ, Sánchez-Cantalejo E, Fernández-Mondéjar E. (2013). Pressure ulcer prevention in ventilated patients using two repositioning regimens (PUPPAS). https://clinicaltrials.gov/ct2/show/results/NCT00847665?term=pressure+ulcers+and+turning&rank=3§=X01256
Rich, S. E., Margolis, D., Shardell, M., Hawkes, W. G., Miller, R. R., Amr, S., & Baumgarten, M. (2011). Frequent manual repositioning and incidence of pressure ulcers among bedbound elderly hip fracture patients. Wound Repair and Regeneration: Official Publication of the Wound Healing Society [and] the European Tissue Repair Society, 19(1), 10–18. http://doi.org/10.1111/j.1524-475X.2010.00644.x
Schindler, S, Mikhailov, T, Kuhn E, Christopher, J, Conway P, Ridling, D, Scott, A and Simpson, V. (2011). Protecting fragile skin: nursing interventions to decrease development of pressure ulcers in pediatric intensive care. American Association of Critical-Care Nurses. http://ajcc.aacnjournals.org/content/20/1/26.full.pdf+html

