by: jennifer knight pa-s lock haven university february 2009 acute otitis media in children
TRANSCRIPT

BY: JENNIFER KNIGHT PA-S
LOCK HAVEN UNIVERSITYFEBRUARY 2009
Acute Otitis Media in Children
The Facts
Acute otitis media is a common disease in the pediatric setting, the most commonly diagnosed condition in the United States,
and the most common indication for antibiotic use in children!

By the Book Definition
A non-specific inflammation of the middle ear
Clinically: rapid onset of symptoms including persistent/severe ear pain, fever, nausea, vomiting, conductive hearing loss, and diarrhea
Otoscopy: inflammation of the middle ear, bulging tympanic membrane that is opaque with erythema, and prominent vessels

www.medscape.com/viewarticle/408727_3
A Closer Look…

The Culprit
Viral: RSV, parainfluenza, human rhinovirus, enterovirus,
adenovirusBacteriaMost common:
Streptococcus pneumoniae Haemophilus influenzae Moraxella catarrhalis Streptococcus pyogenes Staphylococcus aureus

Pathophysiology
Poor drainage of the Eustachian tube due to the anatomy leading to blockage
Inflammation/edema
Congenital deformity
http://content.revolutionhealth.com/contentimages/images-image_popup-ww5rp36.jpg
Treatment Guidelines
Defer antibacterial therapy in children with nonsevere AOM by limiting management given to symptomatic relief for the first 48 to 72 hours
Antibiotic treatment is only to be initiated if the child remains symptomatic at 72 hours

Summary Table
Antibiotic Therapy
When required, these are the first line antibiotics: Amoxicillin Erythromycin/sulfonamide Clavulanic acid/amoxicillin Trimethoprim/sulfamethoxazole Cefaclor
* PCN allergy: erythromycin or clarithromycin

The basis of my question:
1. Despite current therapy guidelines, antibiotics continue to be prescribed immediately
2. Antibiotic resistance is increasing in the bacterial pathogens responsible for AOM
3. There is a need for healthcare costs to be decreased
4. Are parents truly unsatisfied if they don’t receive an antibiotic at their visit?
PICO Question
In the pediatric population, from birth to 18 years of age, with nonsevere acute otitis media, which excludes those with fevers > 39 C/severe pain/recurrent infection/recent antibiotic use within 30 days/ toxic appearance/immune-compromised/>48 hours of otalgia and fever/history of myringotomy and/or tympano-tubes, would withholding antibiotic treatment when compared with the standard treatment of antibiotic use, lead to resolution of the symptoms without harm and increased discomfort to the child/adolescent?

“ A randomized, double-blind, placebo-controlled noninferiority trial of amoxicillin for clinically
diagnosed acute otitis media in children 6 months to 5 years of age”
512 children who presented to clinics or the ER with a new episode of AOM from 6 months to 5 years of age were randomized to receive amoxicillin or placebo for 10 days. The primary outcome was clinical resolution of symptoms without receipt of an antimicrobial agent. Secondary outcomes were the presence of pain/fever and activity level in the first 3 days and the presence of middle ear effusion in 1-3 months. Patients were followed for 3 months. Conclusion:
At 14 days, 84.2% that received placebo and 92.8% that received amoxicillin had clinical resolution of symptoms. No statistical difference in adverse events between the groups nor recurrence rates or middle ear effusions at 1 and 3 months.
The results “did not support the hypothesis that placebo was noninferior to amoxicillin,” however; “delayed treatment was associated with resolution of clinical signs and symptoms in most of the children.

Table 1
Cumulative clinical resolution rates in the per-protocol analysis at 14 days
Group; no. (and %) of patients
Age group Amoxicillin Placebo Absolute difference, %(and 95% CI) All children 232/250 (92.8) 202/240 (84.2) –8.6 ( –14.4 to –3.0) 6–23 mo 76/89 (85.4) 73/92 (79.3) –6.1 ( –17.1 to 5.2) 2–5 yr 156/161 (96.9) 129/148 (87.2) –9.7 ( –16.3 to –3.8)

“Antibiotics for acute otitis mediaIn children”
Through the Cochrane Database of Systematic Reviews, 10 trials were used. The trials were randomized controlled clinical trials that compared antimicrobial drugs with placebo. Outcomes were based solely on patient relevant outcomes.
ConclusionBy 24 hours, 2/3 children recovered from pain no matter what treatment they had. In 2-7 days, 80% children spontaneously recovered. No differences in hearing preservation was found. Reduced contra-lateral otitis media was found in the antibiotic group but an increase in GI side affects/rash in this group. Few serious complications occurred in either and only 1 in 2,000 children developed mastoiditis. Recurrences of otitis media was not significantly different in the two groups.
Antibiotics were found to provide a small benefit for AOM in children. Most cases were found to resolve spontaneously and the benefits must be weighed against the possible adverse reactions. Antibiotics may reduce the risk of mastoiditis in populations where it is common.
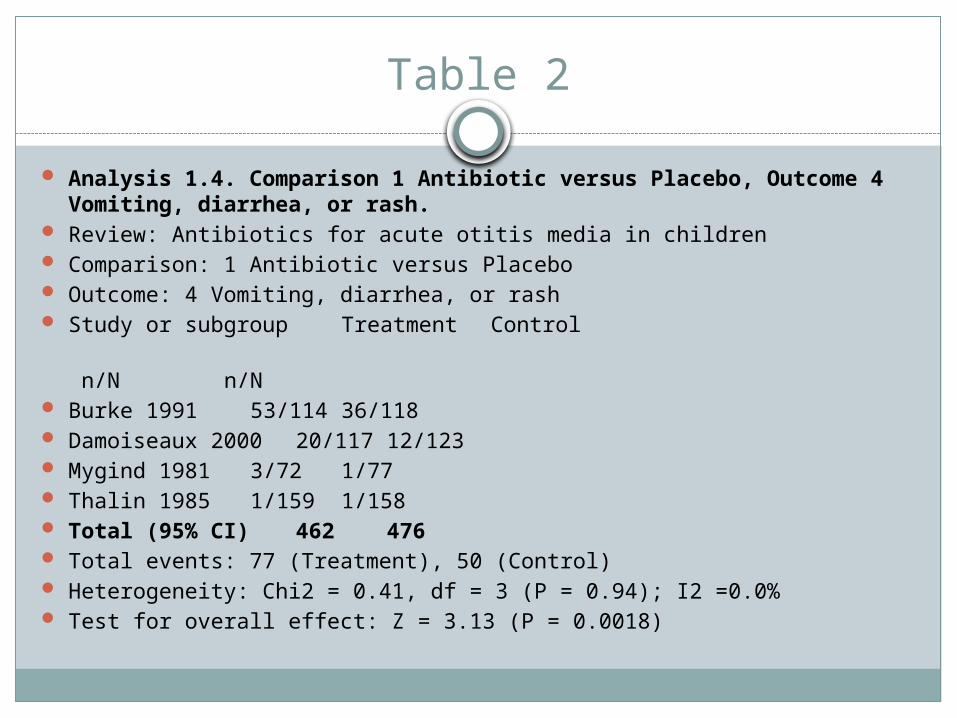
Table 2
Analysis 1.4. Comparison 1 Antibiotic versus Placebo, Outcome 4 Vomiting, diarrhea, or rash.
Review: Antibiotics for acute otitis media in children Comparison: 1 Antibiotic versus Placebo Outcome: 4 Vomiting, diarrhea, or rash Study or subgroup Treatment Control
n/N n/N Burke 1991 53/114 36/118 Damoiseaux 2000 20/117 12/123 Mygind 1981 3/72 1/77 Thalin 1985 1/159 1/158 Total (95% CI) 462 476 Total events: 77 (Treatment), 50 (Control) Heterogeneity: Chi2 = 0.41, df = 3 (P = 0.94); I2 =0.0% Test for overall effect: Z = 3.13 (P = 0.0018)
“Comparison of two approaches to ObservationTherapy for Acute Otitis Media in the
Emergency Department”117 children were randomly assigned to observation therapy and 100 children were randomly assigned to observation therapy with a prescription. A prospective randomized trial was conducted with the primary outcome of examining adherence to observation therapy for AOM in a PED when given an antibiotic and advised not to fill it in 2-3 days. Secondary outcomes were satisfaction with the visit and predictability of parental adherence.
Conclusion87 % in the observation group reported no abx usage within the 3 days observation, and 66% respectively for the group that received an antibiotic prescription upon leaving the PED.
Observation therapy with and without a prescription were both accepted by parents. Adherence was better when an antibiotic was not given at all.
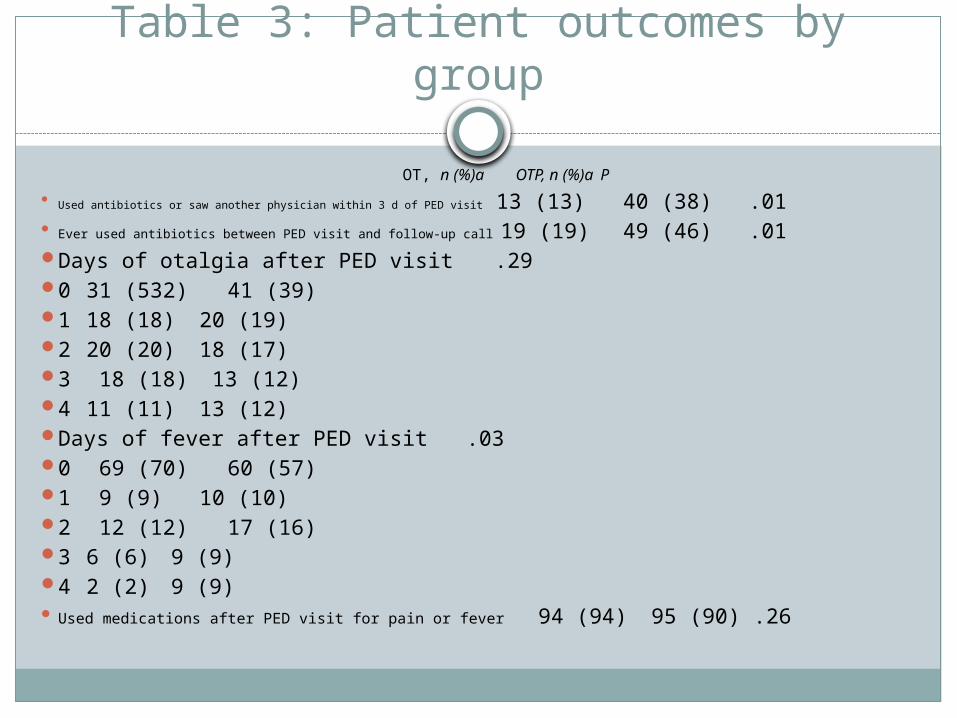
Table 3: Patient outcomes by group
OT, n (%)a OTP, n (%)a P Used antibiotics or saw another physician within 3 d of PED visit 13 (13) 40 (38) .01 Ever used antibiotics between PED visit and follow-up call 19 (19) 49 (46) .01 Days of otalgia after PED visit .29 0 31 (532) 41 (39) 1 18 (18) 20 (19) 2 20 (20) 18 (17) 3 18 (18) 13 (12) 4 11 (11) 13 (12) Days of fever after PED visit .03 0 69 (70) 60 (57) 1 9 (9) 10 (10) 2 12 (12) 17 (16) 3 6 (6) 9 (9) 4 2 (2) 9 (9) Used medications after PED visit for pain or fever 94 (94) 95 (90) .26
“Pediatric Acute Otitis Media: The Case for Delayed Antibiotic Treatment”
A literature review was conducted for this article based on recent literature suggesting that antibiotics are not needed in many children with AOM. The goal of the article was to review the current guidelines as far as therapeutic options and to secondly summarize the approach to management options in the ED.
ConclusionReview of the guidelines showed that birth-2 years with a certain diagnosis requires antibiotic therapy. 6 months-2 years with uncertain diagnosis requires antibiotics if it is severe or observation if nonsevere. Greater than 2 years of age merits antibiotic treatment for severe cases only. Otherwise, defer antibiotic treatment for 48-72 hours and treat symptomatically.
Judicious use of antibiotics in the ER is supported in nonsevere cases as a way to reduce the amount of antibiotics prescribed, decrease cost, increase parental satisfaction, and lower rates of antibiotic resistance while producing an equal amount of cases with resolved AOM.
“NONSEVERE ACUTE OTITIS MEDIA:A CLINICAL TRIAL COMPARING OUTCOMES
OF WATCHFUL WAITING VERSUSIMMEDIATE ANTIBIOTIC TREATMENT”
233 subjects were used. 112 were randomized to antibiotic treatment and 111 were randomized to watchful waiting. The investigators, but not the parents, were blinded to enrollment status. The primary outcome of this study was to evaluate the acceptability, efficacy, and costs of watchful waiting for children with nonsevere AOM.
CONCLUSION66% of subjects in WW completed the study without needing abx. Patient satisfaction was the same for both groups. Immediate abx treatment showed decreased numbers of treatment failures and improved symptom control, but increased abx adverse events and a higher percentage of multidrug resistant strep pneumoniae strains on day 12. Costs were also found to be decreased in the WW group.
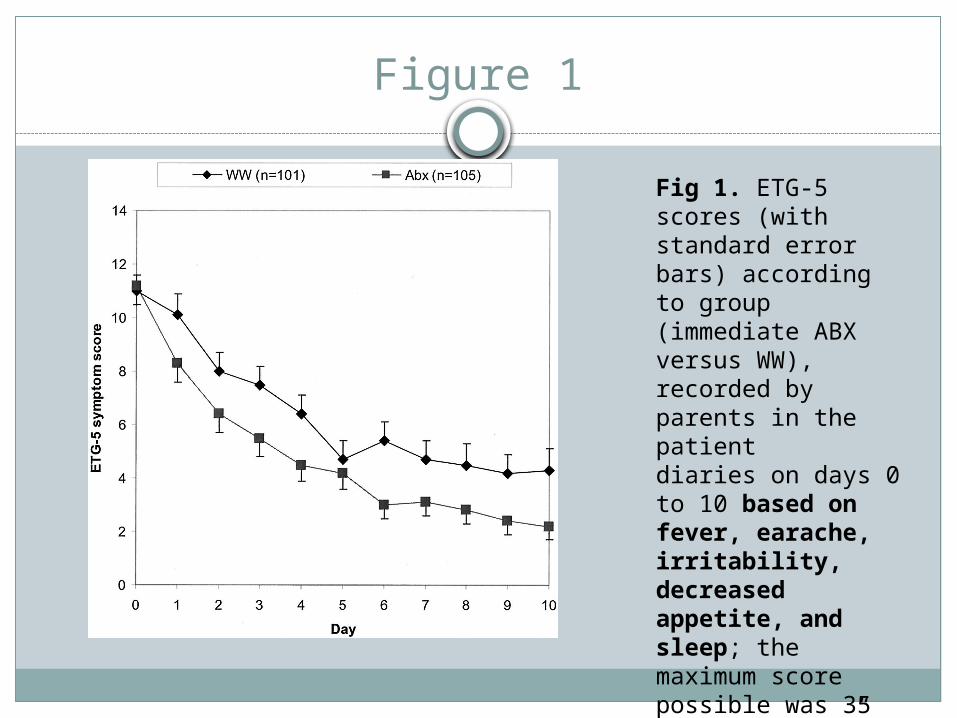
Figure 1
Fig 1. ETG-5 scores (with standard error bars) according to group(immediate ABX versus WW), recorded by parents in the patientdiaries on days 0 to 10 based on fever, earache, irritability, decreasedappetite, and sleep; the maximum score possible was 35(see “Methods”).

In summary:
1. The WW approach often leads to spontaneous resolution of clinical signs and symptoms.
2. Antibiotics have been shown to only provide a small benefit on nonsevere cases of AOMnonstatistically significant differences between WW and ABX treatment have been shown.
3. WW has not been shown to cause harm.
4. Contrary to popular belief, WW is an acceptable management plan for parents when given the proper patient education.
5. WW decreases healthcare costs.

References
Chao, J. H., Kunkov, S., Reyes, L. B., Lichten, S., & Crain, E. F. (2008). Comparison of Two Approaches to Observation Therapy for Acue Otitis Media in the Emergency Department. Pediatrics , 121 (5), 1352-1356.
Glasziou, PP., Del Mar, C., Sanders, S., & Hayem, M. (2004). Antibiotics for acute otitis media in children. Cochrane
Database of Systemic Reviews 2004, Issue 1. Art No.: CD000219. DOI: 10.1002/14651858.CD000219.pub2.
Johnson, N. C., & Holger, J. S. (2007). Pediatric Acute Otitis Media: The Case for Delayed Antibiotic Treatment. The Journal of Emergency Medicine , 32 (3), 279-284.
Leibovitz, Eugene. (2003) Acute Otitis Media in Pediatric Medicine: Current Issues in Epidemiology, Diagnosis, and Management. Pediatric Drugs. 5 (Suppl 1), 1-12.
Le Saux, N., Gaboury, I., Baird, M., Klassen, T. P., MacCormick, J., Blanchard, C., et al. (2005). A randomized double- blind, placebo controlled noninferiority trial of amoxicillin for clinically diagnosed acute otitis media in children 6 months to 5 years of age. Canadian Medical Association Journal , 172 (3), 335-341.
McCormick, D. P., Chonmaitree, T., Pittman, C., Saeed, K., Friedman, N. R., Uchida, T., et al. (2005).Nonsevere
Acute Otitis Media: A Clinical Trial Comparing Outcomes of Watchful Waiting Versus Immediate Antibiotic Treatment. Pediatrics , 115 (6), 1455-1464.
O'Connell, C. B., & Zarbock, S. F. (2007). A Comprehensive Review for the Certification and Recertification Examinations for Physician Assistants. Philadelphia: Lippincott Williams and Wilkins.
Thank you
Questions?