by: mahmood a. khwaja and s.waqar ali
TRANSCRIPT

Policy Brief # 45
Regulating Mercury Amalgam Use at
Private Dental Clinics in Pakistan
By:
Mahmood A. Khwaja and S.Waqar Ali
All rights reserved. No part of this paper may be reproduced or transmitted in any form or by any
means, electronic or mechanical, including photocopying, recording or information storage and
retrieval system, without prior written permission of the publisher.
A publication of the Sustainable Development Policy Institute (SDPI).
The opinions expressed in the papers are solely those of the authors, and publishing them does not
in any way constitute an endorsement of the opinion by the SDPI.
Sustainable Development Policy Institute is an independent, non-profit research institute on
sustainable development.
First edition: November 2015
© 2015 by the Sustainable Development Policy Institute
Mailing Address: PO Box 2342, Islamabad, Pakistan.
Telephone ++ (92-51) 2278134, 2278136, 2277146, 2270674-76
Fax ++(92-51) 2278135, URL: www.sdpi.org

Table of Contents
1. Introduction: ................................................................................................................................... 1
2. Methodology: .................................................................................................................................. 2
3. Results and Discussion: ................................................................................................................... 2
4. Recommendations: ......................................................................................................................... 3
References: ............................................................................................................................................. 4
Annexes ................................................................................................................................................... 6

1
1. Introduction:
Mercury, one of the most hazardous chemicals, has become a growing issue of global concern
because of its adverse environmental and health impacts (ATSDR 2011). Despite its toxic properties,
mercury is widely used in dental amalgams for filling cavities caused by caries (SOU 2003). Dental
amalgam is typically composed of approximately 50% mercury, 34.5% silver, 9% tin, 6% copper, and
0.5% zinc by weight (Alt Inc. 2005). The dentist’s occupational exposure to mercury vaporus occurs
to a large extent during direct clinical work with preparation of dental amalgam restorative material,
as well as during cutting, filling and polishing operations (Morton et al. 2004; Ely, 1997). It is
estimated that in human, 60 per cent of Mercury exposure results from dental amalgam in the oral
cavity via inhalation of mercury vapours and 40 per cent of mercury exposure is via ingestion
(Spencer 2000). A person having dental mercury amalgam filling on the average absorbs about 3-
17micrograms of mercury (Weinberg 2010). Mercury poisoning may damage the nervous system,
lungs, and kidneys. Exposure to mercury of vulnerable population (dental professionals, healthcare
workers, children, pregnant women, and elderly) is of particular concern. The nervous system is
most sensitive to mercury exposure (OPH 2008). Children are more at risk from mercury poisoning,
which affects their neurological development and brain. According to the World Health
Organization, dentists are among the health professionals with higher occupational exposure to
mercury vapours (World Health Organization 1991; Morton et al. 2004).
Very few investigations on mercury amalgam use in the dentistry sector have been carried out in
South Asia (including Pakistan) and there is little data reported on mercury contamination of
indoor/outdoor air at dental healthcare sites, dental teaching institutions, hospitals & private dental
clinics. In Pakistan, mercury emission and transfer are mainly from extraction and use of fuels,
intentional use of mercury in industrial processes, and in others, such as dental mercury-amalgam
fillings, medical equipment’s, waste deposition/land fillings and waste water-treatment (MoE 2000).
Studies on dental amalgam use and mercury contaminated waste disposal practices by dental
professionals in Pakistan have been reported by Rubina et al. (2010) and Iqbal et al. (2011). SDPI
studies indicated alarmingly high mercury levels in the air (indoor as well as outdoor) at 11 of the 34
visited dental sites (17 dental teaching institutions, 7 general hospitals & 10 dental clinics) in five
main cities of Pakistan (Khwaja & Maryum 2014; Khwaja et al. 2014). Responses from dental
professionals at 38 dental institutions in Pakistan showed general unawareness among dental
professionals regarding mercury containing wastes and lack of awareness about health hazards of
mercury exposure to human health (Khwaja & Sadaf 2014). A recent study carried out by Gul (2015)
at Peshawar University, Pakistan on appropriate handling of mercury/mercury amalgam,
environmentally unsound management of biological samples (RBCs, plasma, urine, hair & nails) of
individuals with mercury dental amalgam (n=30) and controlled samples (n=30)) have shown
mercury concentration 6 – 8 times higher than the controlled samples (individuals without dental
mercury amalgam).
In view of the earlier SDPI studies mentioned above, indicating high indoor air mercury levels within
private dental clinics and lack of awareness among dental professionals regarding mercury related
occupational health and safety issues, the present study was conducted to assess the status of
mercury amalgam use in private dental clinics. In the light of the findings described and discussed in
the following pages to safeguard public health and for the protection of environment, it is strongly
recommended that since mercury amalgam use cannot be banned immediately in the country, its use

2
may be regularized and allowed subject to use of “Amalgam Separators,” “Capsulated Mercury” and
“Mechanized Mixing ban on use of mercury amalgam for children (below 12 years age) and pregnant
women. A review/revision of the curriculum currently being taught at medical and dental colleges in
the country should be conducted to ensure adequate training towards minimizing mercury exposure,
and mercury amalgam use in dentistry.
2. Methodology:
Over 90 private dental clinics were visited in Gilgit, Hunza, Peshawar, Rawalpindi & Islamabad and
dental professionals/private clinics in-charge interviewed during June – July 2015. Dental
professionals (qualified medical graduate) interviewed were 79% male and 21% female. A
questionnaire based assessment was undertaken to evaluate the mercury/mercury amalgam related
issues at private dental clinics (Annex 1). The focus areas were Hg amalgam toxicity, its waste
management practices and safety measures practiced among the dental practitioners. The lists of
private dental clinics of each visited is given in Annex II. Summarized results are shown in Table 1.
3. Results and Discussion:
According to an earlier SDPI study report, the levels of mercury in air at private dental clinics were
observed to be lower as compared to general hospitals and dental teaching institutions (Khwaja et
al. 2014). The highest levels were observed at some clinics in Islamabad, which was considered to be
due to insufficient ventilation and improper waste disposal and proportionately larger number of
visited patients, treated with mercury amalgam fillings at these clinics. All the visited private clinics
were having higher concentrations of mercury vapours in indoor air than the permissible limits of
300 ng/m3 of air (Khwaja et al. 2014)
In view of the very high mercury vapours in air at private dental clinics, i.e. 1800 – 333 ng/m3
(Khwaja et al. 2014), this survey was carried out to know the extent of mercury dental amalgam use
at private dental clinics and other related issues in five selected cities. Summarized data of
responses to four priority questions (out of 15 questions/Annex I) is given in Table 1.
3
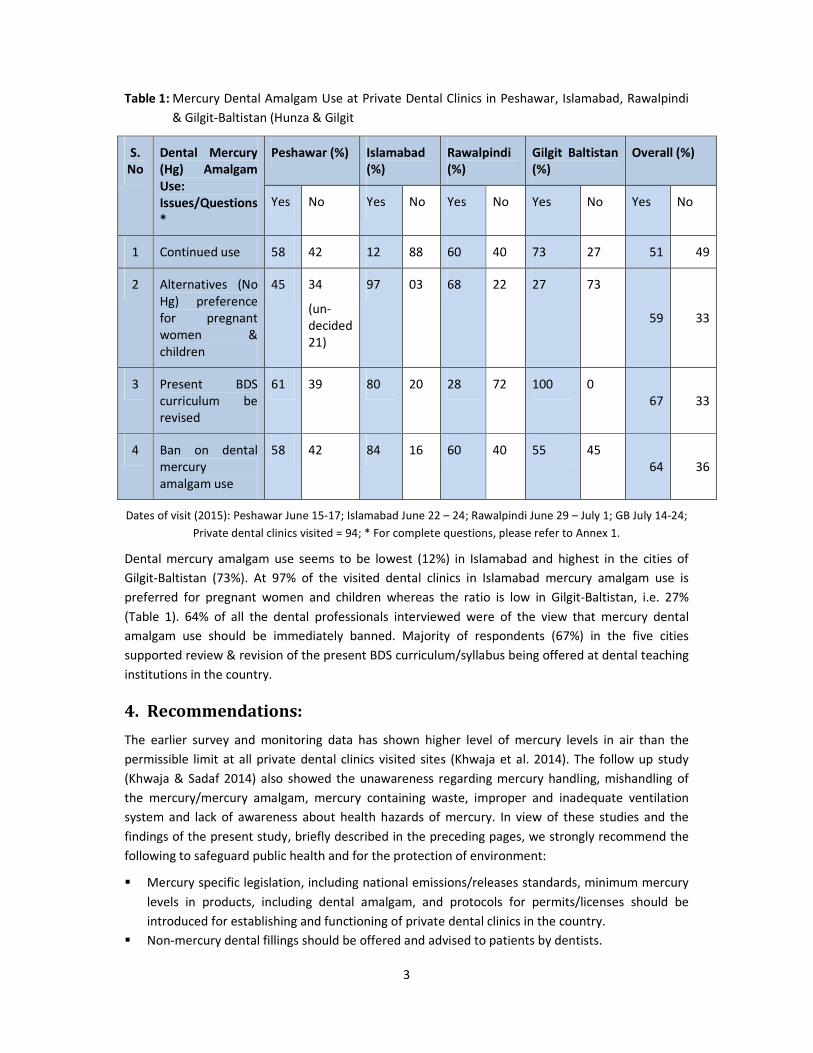
Table 1: Mercury Dental Amalgam Use at Private Dental Clinics in Peshawar, Islamabad, Rawalpindi
& Gilgit-Baltistan (Hunza & Gilgit
S.
No
Dental Mercury
(Hg) Amalgam
Use:
Issues/Questions
*
Peshawar (%) Islamabad
(%)
Rawalpindi
(%)
Gilgit Baltistan
(%)
Overall (%)
Yes No Yes No Yes No Yes No Yes No
1 Continued use 58 42 12 88 60 40 73 27 51 49
2 Alternatives (No
Hg) preference
for pregnant
women &
children
45 34
(un-
decided
21)
97 03 68 22 27 73
59 33
3 Present BDS
curriculum be
revised
61 39 80 20 28 72 100 0
67 33
4 Ban on dental
mercury
amalgam use
58 42 84 16 60 40 55 45
64 36
Dates of visit (2015): Peshawar June 15-17; Islamabad June 22 – 24; Rawalpindi June 29 – July 1; GB July 14-24;
Private dental clinics visited = 94; * For complete questions, please refer to Annex 1.
Dental mercury amalgam use seems to be lowest (12%) in Islamabad and highest in the cities of
Gilgit-Baltistan (73%). At 97% of the visited dental clinics in Islamabad mercury amalgam use is
preferred for pregnant women and children whereas the ratio is low in Gilgit-Baltistan, i.e. 27%
(Table 1). 64% of all the dental professionals interviewed were of the view that mercury dental
amalgam use should be immediately banned. Majority of respondents (67%) in the five cities
supported review & revision of the present BDS curriculum/syllabus being offered at dental teaching
institutions in the country.
4. Recommendations:
The earlier survey and monitoring data has shown higher level of mercury levels in air than the
permissible limit at all private dental clinics visited sites (Khwaja et al. 2014). The follow up study
(Khwaja & Sadaf 2014) also showed the unawareness regarding mercury handling, mishandling of
the mercury/mercury amalgam, mercury containing waste, improper and inadequate ventilation
system and lack of awareness about health hazards of mercury. In view of these studies and the
findings of the present study, briefly described in the preceding pages, we strongly recommend the
following to safeguard public health and for the protection of environment:
� Mercury specific legislation, including national emissions/releases standards, minimum mercury
levels in products, including dental amalgam, and protocols for permits/licenses should be
introduced for establishing and functioning of private dental clinics in the country.
� Non-mercury dental fillings should be offered and advised to patients by dentists.

4
� Capsulated mercury use and adaptation of mechanical mixing instead of motor and pestle for
preparation of mercury amalgam be adopted.
� Following the best preventive approach - Waste Reduction at Source, mercury
emissions/releases streams through an environmental waste audit, be identified within dental
sites, so that accordingly, control measures for the same be designed and implemented at the
earliest.
� Best in-house environmental practices (BEPs) and use of best environment-friendly technology
be encouraged; standard operating procedures for mercury handling, transport & use and
mercury contaminated waste management be developed and implemented. An institutional
mercury waste management plan be put in place at all mercury related sites and the same be
periodically monitored and evaluated by the management.
� Minamata Convention on mercury (2013) be ratified by Pakistan and other countries at the
earliest time possible.
� In the revised BDS curriculum the topics need to included are a brief on the need, objectives and
the relevant provisions of “Minamata Convention on Mercury,” with reference to mercury in
products (dental amalgam); health and environment; the toxicity and health hazards resulting
from mercury/mercury amalgam use and protection and control measures for the same,
minimization of mercury exposure and guidelines for environmentally sound mercury
contaminated waste management; promotion of cost and clinically effective mercury free
alternatives dental filling materials such as glass ionomers and resin composites.
(Full report accessible at www.sdpi.org)
References:
Alt Inc. Dental amalgam composition. Dispersalloy. Available at: http://www. Altcorp. Com/Dental
Information/ amalgamcomp. Feb, 24, 2005
(ATSDR): Agency for toxic substances and diseases registry. (2011). Detailed Data table for priority
list of hazardous substances
http://www.atsdr.cdc.gov/spl/resources/ATSDR_2011_SPL_Detailed_Data_Table.pdf
Gul, Nayab (2015) Mercury Exposure and Health Effects in Occupational Workers, Dental Amalgam
and Whitening Creams Users, PhD Thesis, Environmental Sciences Department, University of
Peshawar, Peshawar. Pakistan
Ely, B.M., (1997). The future of dental amalgam: a review of the literature. Part 2: Mercuryexposure
in dental practice. Br. Dent. 182 (8), 293–297.
Iqbal, K.I, Maria, Z., Majid, J., Sana, M., Afreen, M., Fareed, A., Sajid, S., Adel, A., Iftikhar, A., Yawar
and Kaleem, M. 2011, “ Dental Amalgam Effects of Alloy/Mercury mixing uses and Waste
Management,” J. Ayub Med. College, Abottabad, 23 (4)
5
Khwaja, M.A., Abbasi, M.S.. Mahmood, F. and Jahangir, S. 2014, ‘Study of High Levels Indoor Air
Mercury Contamination from Mercury Use in Dentistry’, Journal of Science, Technology and
Development, Pakistan Council for Science and Technology, vol.33, no. 2, pp.94-106.
Khwaja, M.A. and Abbasi, M.S. 2014, ‘Mercury Poisoning Dentistry’, Reviews on Environment Health,
New York Academy of Sciences, vol. 29, nos.1/2, pp.29 – 31.
Khwaja, M.A. and Nawaz, S. 2014, ‘Toxic Mercury and Mercury Amalgam Use in Dentistry – The
Need to Review and Revise Current BDS Curriculum at Dental Teaching Institutions’, SDPI Policy
Brief Series # 43, Sustainable Development Policy Institute, Islamabad, Pakistan.
MoE preliminary report on Mercury Inventory in Pakistan, (2000) Government of Pakistan/UNEP
Chemical Branch, Ministry of Environment, Islamabad
Morton J, Mason HJ, Ritchie KA, White M. (2004) Comparison of hair, nails and urine for biological
monitoring of low level inorganic mercury exposure in dental workers. Biomarkers, 9(1):47–55.
Office for Public Health, (2008), Information for health care professionals Mercury exposure and
toxicity, Louisiana Department of Public Health and Hospitals
http://new.dhh.louisiana.gov/assets/oph/CenterEH/envepi/Mercury_for_Health_Provider_Hg_a.
Final.pdf
Rubina, M., Khan, A.A.. Noor, N. and Humayun 2010, “Amalgam Use and Waste Management by Pak.
Dentist, EMHU, 16 (3)
SOU (2003) Dentala material och halsa (Dental materials and health), (in Swedish; English summary
and an overview of scientific literature by Maths Berlin). Swedish Government Official Reports
Series. Stockholm, Sweden: Ministry of Health and Social Affairs
http://social.regeringen.se/propositionermm/sou/ sou 2003.htm.
Spencer, A.J. (2000). Dental amalgam and mercury in dentistry. Australian Dental Journal 45(4): 224-
234
Weinberg, J. (2010). An NGO Introduction to Mercury Pollution. International POPs Elimination
Network.
WHO World Health Organization, 1991. Environmental Health Criteria 118 Inorganic Mercury
International Program in Chemical Safety. World Health Organization, Geneva.

6
Annexes
Annex 1: SDPI Survey Form
7
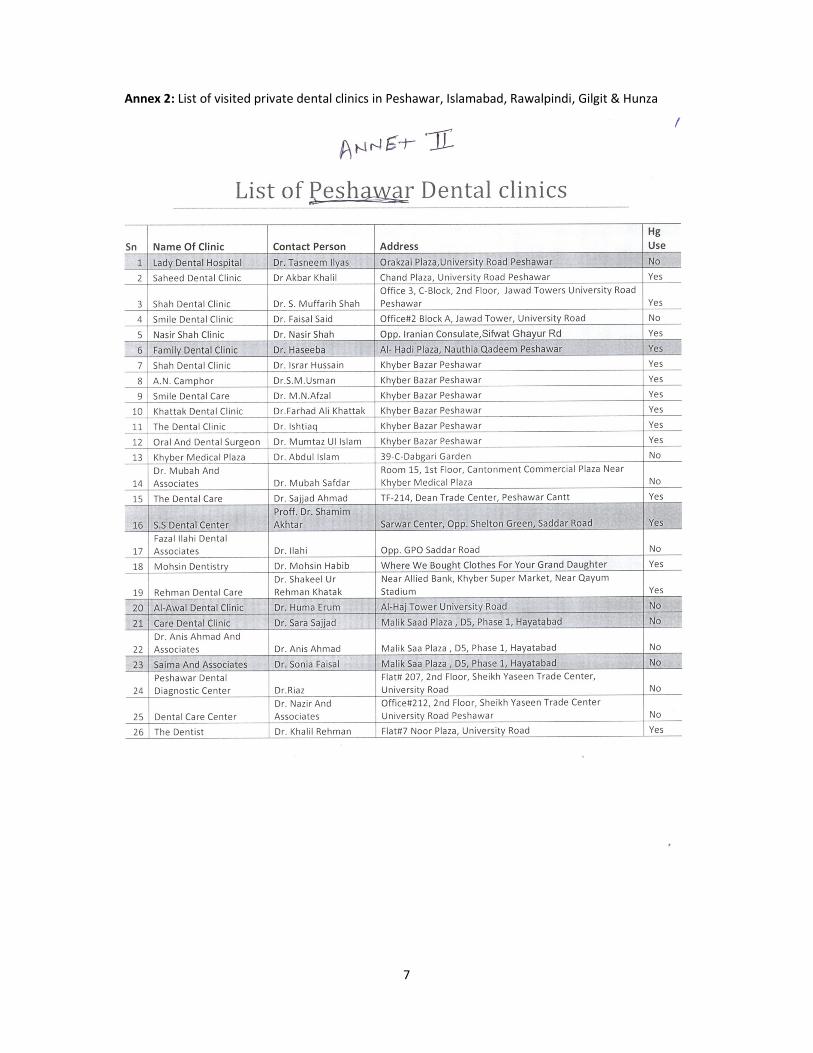
Annex 2: List of visited private dental clinics in Peshawar, Islamabad, Rawalpindi, Gilgit & Hunza
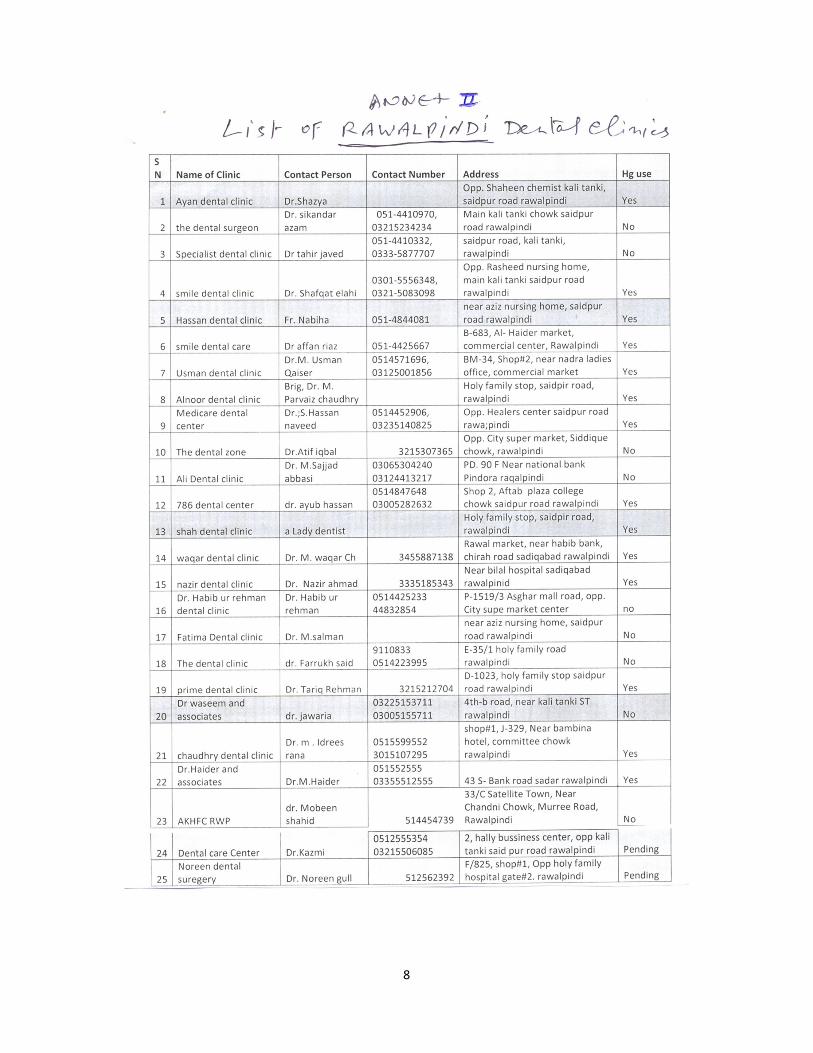
8
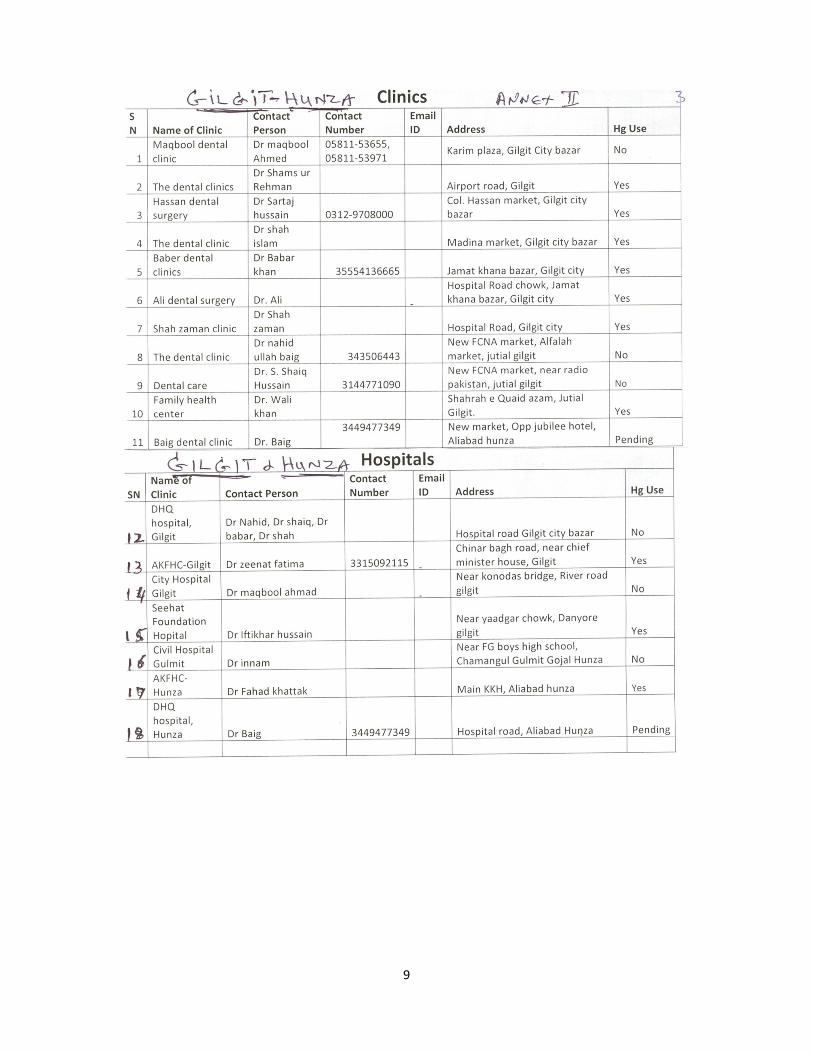
9
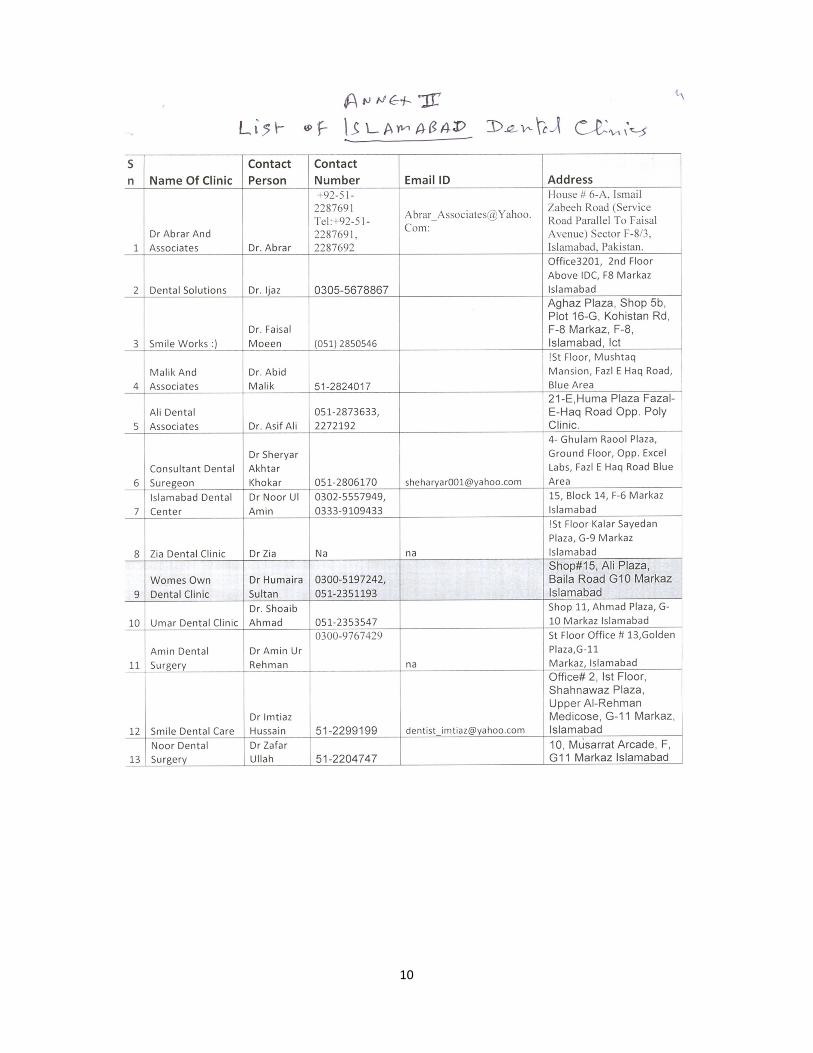
10
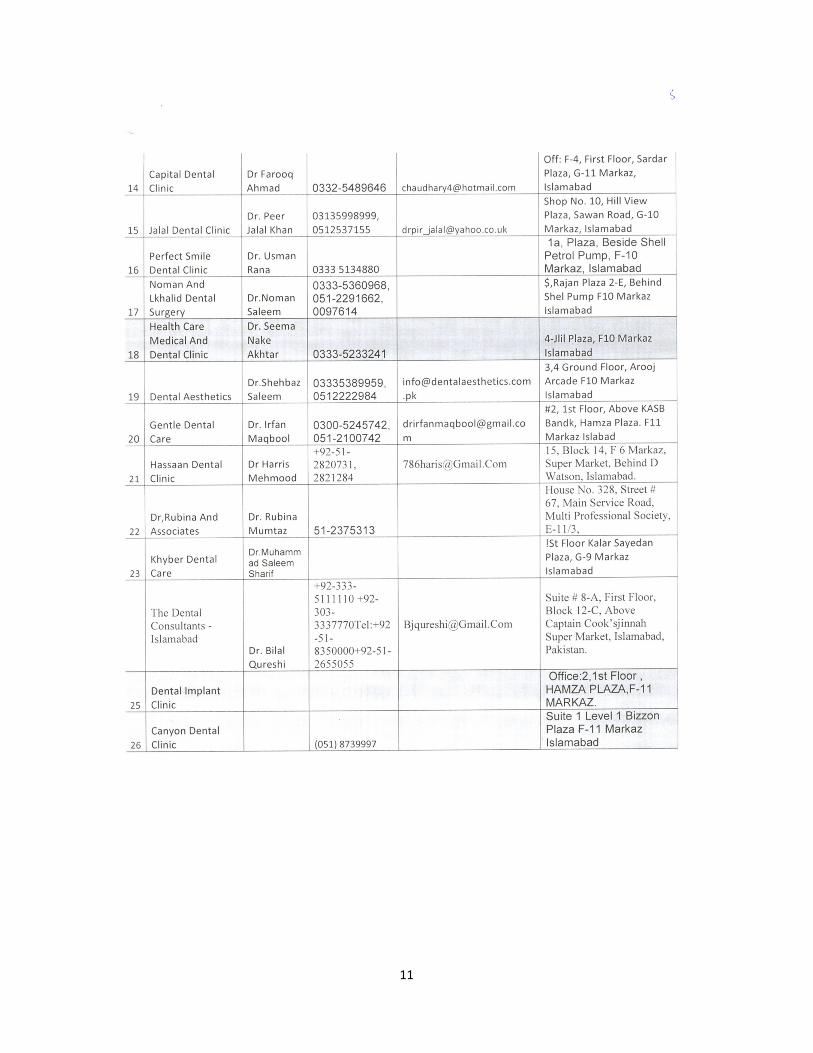
11