cadaver study of medial neurovascular structures following percutaneous calcaneal displacement...
TRANSCRIPT
CADAVER STUDY OF MEDIAL NEUROVASCULAR
STRUCTURES FOLLOWING PERCUTANEOUS CALCANEAL
DISPLACEMENT OSTEOTOMIES
Authors:
Joseph M. Anain Jr. DPM, FACFAS (Catholic Health System, Buffalo, NY)
Lawrence DiDomenico DPM, FACFAS (Forum Health Northside Medical Center, Youngstown, OH)
Trang Mai Duong DPM
INTRODUCTION:
• Flatfoot deformity is a very common foot problem with clinical manifestation of posterior tibial tendon dysfunction (PTTD.) Flatfoot deformity is characterized by progressive colapsing of the medial longitudinal arch, forefoot abduction, and hindfoot valgus.
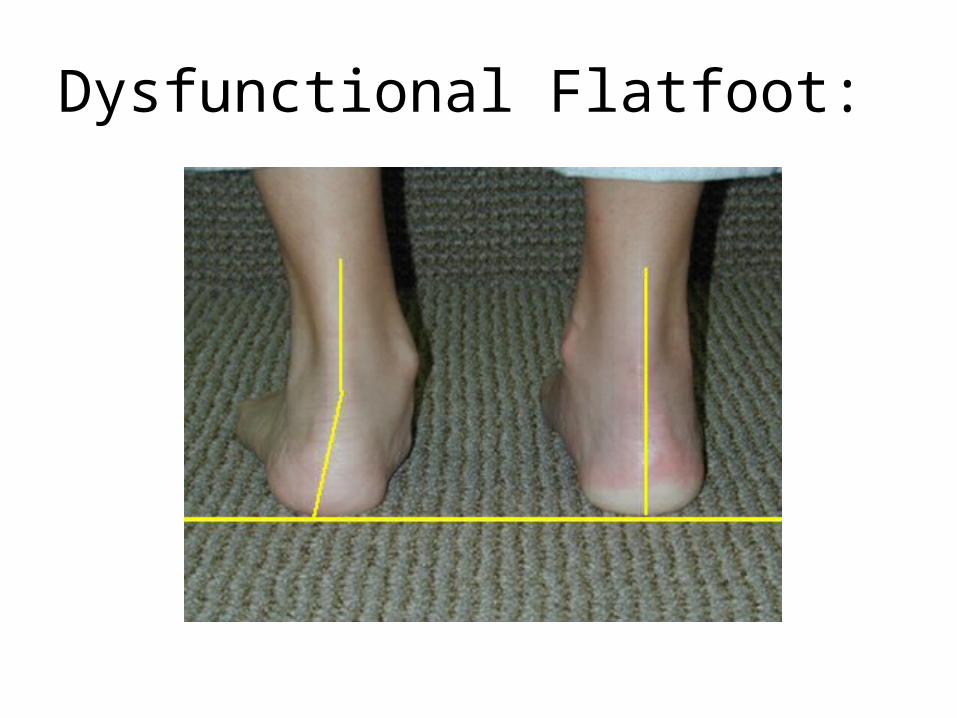
Dysfunctional Flatfoot:
Terminology
• Flatfoot
• Pes planus
• Hypermobile flatfoot
• Pes plano-valgus
• Tilipes calcaneal valgus
• Peroneal spastic flatfoot
Etiologies:
• congenital-ligamentous laxity, veritical talus, coalition, equinus
• Acquired:• Biomechanical-torsional,hypermobility• Systemic disease: arthritis, neuromuscular • Trauma- coalition fx, PT damage, lisfranc
dislocation
Treatment goals:
• Relieve pain
• Reduce deformity
• Improve function
• Prevent progression of deformity
• Decrease postural symptoms
Medial displacement osteotomy of the Calcaneus:
• Medial displacement osteotomies of the calcaneus is commonly performed for stage II posterior tibial tendon dysfunction to correct the valgus deformity of the hindfoot. These procedures in conjunction with other soft tissue procedures can lead to restoration of the height of the hindfoot, and reposition the Achilles tendon, plantar fascia and the calcaneus.

• Medial displacement of the calcaneus redirects the pull of the gastrocnemius-soleus muscle group slightly medial to the STJ , increasing varus on the hindfoot. The medial displacement osteotomies of the calcaneus thus play a significant role in restoring normal biomechanic in the flexible pes planovalgus deformity.
HISTORY:
• Gleich first introduced the calcaneal osteotomy in 1893 as an attempt to restore the calcaneal pitch angle.
• Subsequently, operative management of stage II posterior tibial tendon dysfunction takes many forms using medial displacement osteotomy, lateral column lengthening, calcaneocuboid joint distraction arthrodesis, and soft tissue balancing procedures.
Open calcaneal Osteotomies:
• While performing open calcaneal osteotomies in association with other soft tissue repositioning few patients develop post-operative medial hindfoot pain which radiates distally and wound complications. These can range from hindfoot pain, numbness, hematoma, and wound dehiscence.
• Greene et al studied the anatomical relation to open calcaneal osteotomy and this anatomical study concluded the extensive dissection of open calcaneal osteotomies can traumatize the medial neurovascular structures which may result in post-operative complications. The authors recommended breaking medial cortex of the calcaneus should be done in a control manner to minimize post-op complictions.

PURPOSE:
• The purpose of our cadaver study is to prove medial neurovascular structures at the rearfoot can be safely protected after percutaneous calcaneal displacement osteotomies (PCDO.) The PCDO minimizes soft tissue and subperiosteal dissection to help prevent trauma to the medial neurovascular structures and post-operative wound complications.
PCDO:
• PCDO is an extra-articular calcaneal osteotomy in which violation of medial neurovascular structures can be prevented by subperiosteal tunneling, and minimized soft tissue dissection using four stab incisions.
ANATOMY: posterior tibial tendon
• Origin: interosseous membrane and proximal adjacent surfaces of the tibia and fibula.
• Insertion: navicular tuberosity, medial naviculocuneiform and plantar base of 2nd, 3rd, 4th metatarsals.
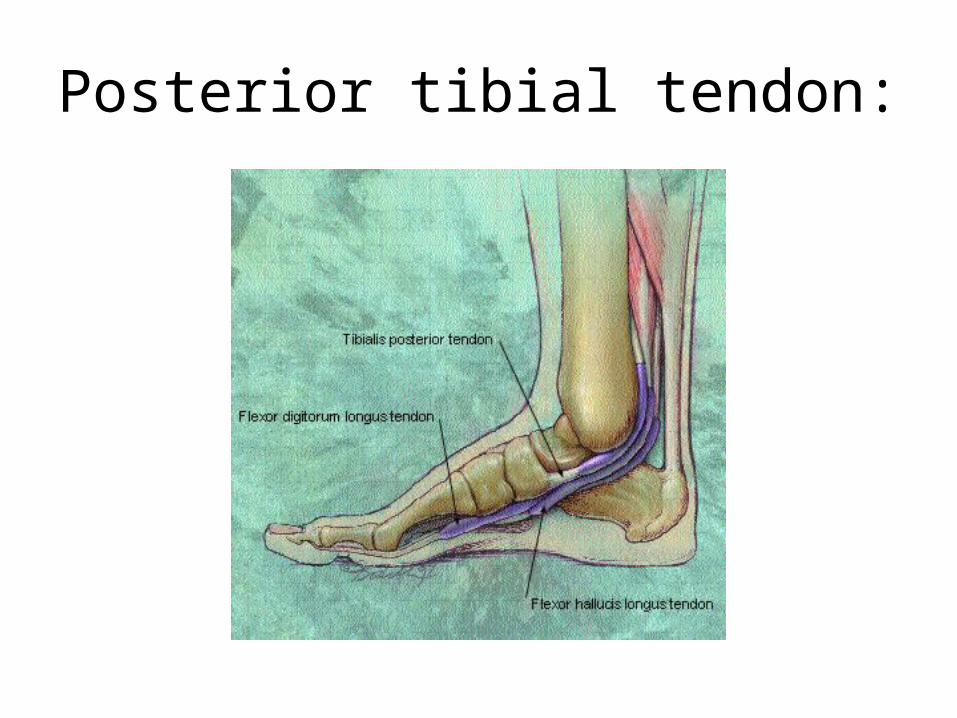
Posterior tibial tendon:
Blood Supply:
• Proximal area is supplied by branches of the posterior tibial artery
• Distal is the bone-tendon interface supplied by branches of posterior tibial and dorsalis pedis arteries
Nerve supply:
• Tibial nerve
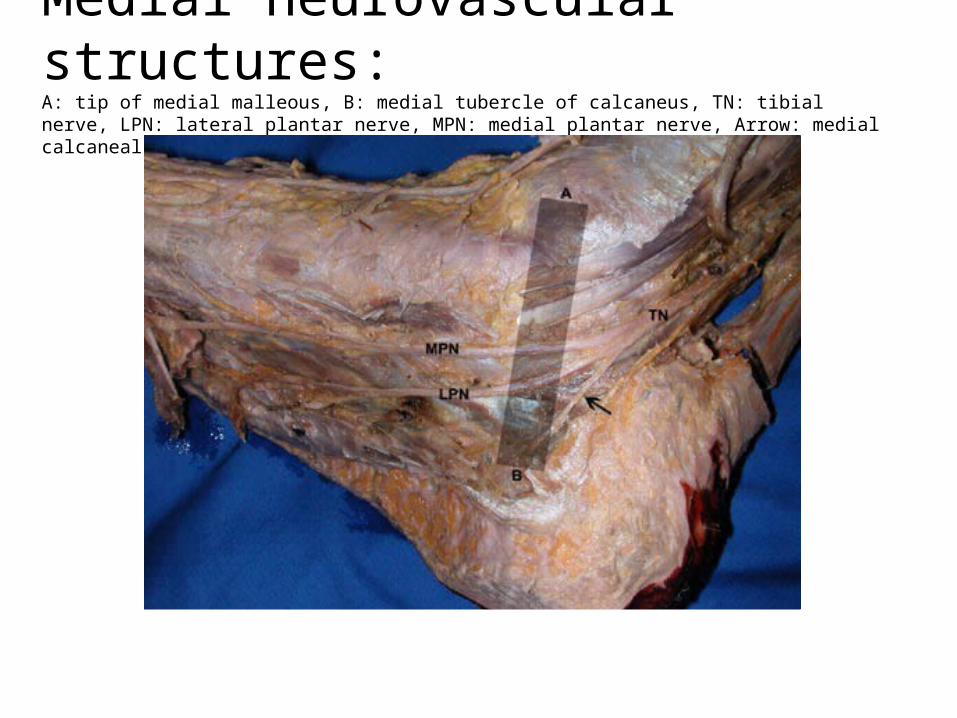
Medial neurovascular structures:A: tip of medial malleous, B: medial tubercle of calcaneus, TN: tibial nerve, LPN: lateral plantar nerve, MPN: medial plantar nerve, Arrow: medial calcaneal branch.
Ligaments:
• Spring ligament
• Deltoid ligament
• Plantar fascia
• Short plantar ligament

CLINICAL EVALUATION:
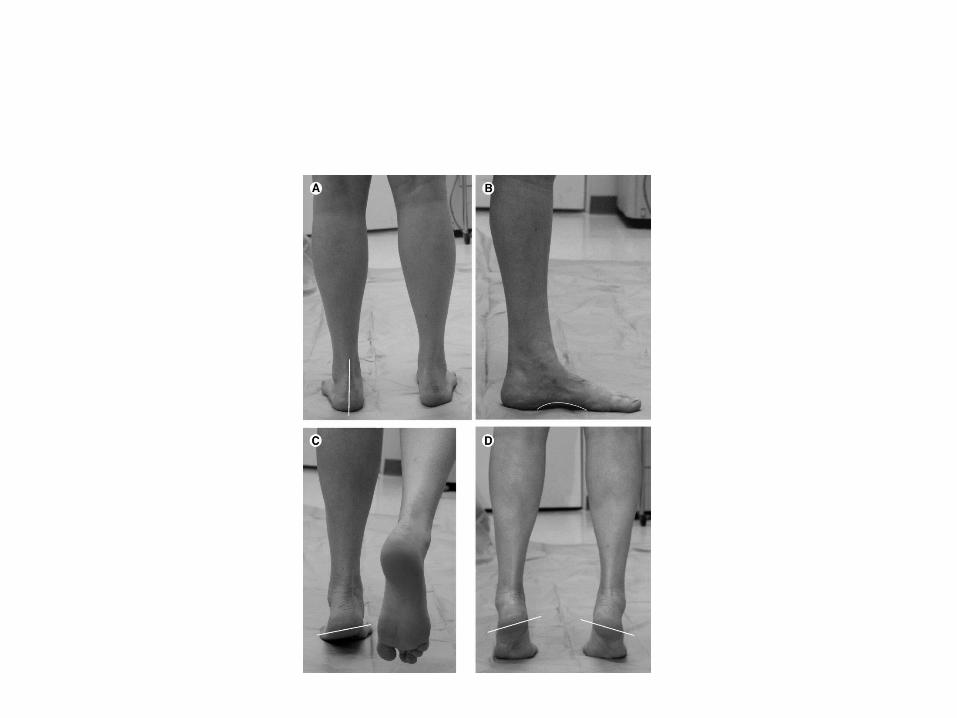
• Non weight bearing and weight bearing LE examination
• Dorsal view: evaluate for malleolar position. If symptomatic, will see posterior displacement of the medial malleoli and internally rotated position of the malleoli.
• Can compare medial and lateral borders (medial bulging of at the talo-navicular joint and lateral concavity at the C-C joint
• Posterior view: hindfoot valgus with medial displacement of the rearfoot
• While patient is standing:• Single heel rise test: holding one foot off the floor, raise
up the ball of the other foot, lifting heel off the floor. PTTD will cause unstability at midtarsal joint
• Hubscher maneuver test: passively DF the patient’s hallux to end range of motion. Through the windlass mechanism and dependent upon ligamentous integrity of the hindfoot, DF of hallux causes PF of first ray, supination of the STJ and external rotation of the tibia. Attenuation of ligaments will cause no external rotation of the tibia
• Non weight bearing: test for heel cord tightness with knee flexed and extended
• Non weight bearing: standard biomechanical examination including range of motion and muscle testing

DIAGNOSTIC TESTING:
Radiographic evaluation: AP, lateral of foot and AP of the ankle
AP view: Forefoot (FF) abduction and navicular sliding laterally on the head of the talus
Lateral view: dislocation of the TN joint, evaluation of calcaneal inclination angle
Ankle view: Osteoarthritis

Normal and flatfoot
• MRI: evaluation of integrity of ligaments and posterior tibial tendon
• CT scan: coalition
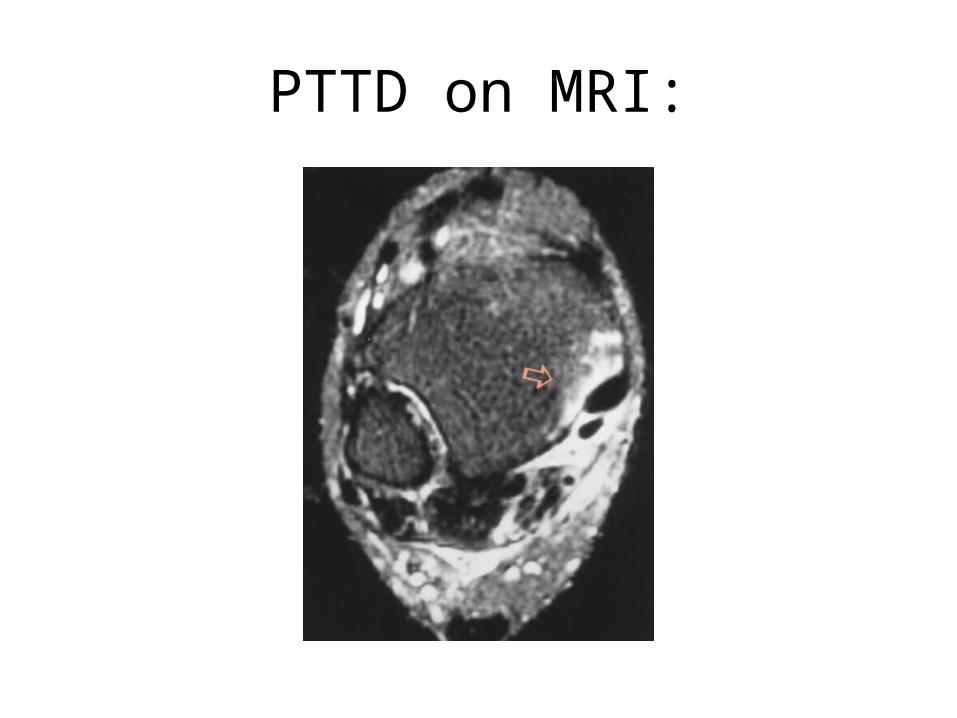
PTTD on MRI:

CLASSIFICATION:
• Johnson and Strom, 1989
• Described the three clinical stages of PTTD
Johnson and Strom Classification:
• Stage I: normal PT tendon length with some degenerative changes and peritendonitis
• Stage II: attenuation and elongation of PT tendon, flexible STJ, RF valgus, FF abduction
• Stage III: Rigid hindfoot, degeneration of the PT tendon, deformity is severe
TREATMENT:
• Stage I: Conservative treatment
• Stage II: calcaneal osteotomies in conjunction with other soft tissue procedures
• Stage III: Arthrodesis
MATERIALS AND METHODS:
Our study utilized 18 fresh frozen cadaver.
Meticulous dissection at medial aspect of
the rearfoot after completion of the PCDO was performed to examine the integrity of the medial neurovascular structures
• PCDO requires four stab incisions and subperiosteal tunneling
• PCDO was performed with the podiatric assistant while the foot was stabilized and following sequential steps of the PCDO with fluoroscopic imaging
• Initially, plantar medial tubercle of the calcaneus was palpated and a stab incision made along the orientation of the planned osteotomy just distal to the calcaneal tubercle at inferior medial aspect of the calcaneus. The incision is deepened bluntly to the bone using a curved hemostat and a subperiosteal tunneling was made toward the medial superior aspect of the calcaneus and tenting of the skin was visualized. Another stab incision was made parallel with the plantar aspect of the foot in the natural skin resting crease at the tented skin (Figure 1) and a 12 inch Gigli saw was introduced to the tip of the same curved hemostat and pulled through the tunnel in retrograded fashion exiting through the same inferior medial incision (Figure2).


Figure #2
• Attention was then redirected to the superior medial stab incision where a straight hemostat was used to make another transverse subperiosteal tunnel at the superior aspect of the calcaneus and anterior to the Achilles tendon. Another stab incision was made to the tented skin parallel to the plantar aspect of the foot within a resting skin crease posterior to the peroneal tendons and sural nerve. The tip of the straight hemostat was visualized at the lateral superior border of the calcaneus (Figure3). The straight hemostat was removed upon completion of tunneling from superior lateral to superior medial of the calcaneus. A straight hemostat was again inserted into the original tunneling from superior lateral of the calcaneus to superior medial aspect of the calcaneus. The free end of the Gigli saw was introduced to the tip of the straight hemostat and pulled from superior medial to superior lateral aspect of the calcaneus.
Figure #3
• The final stab incision was made at the lateral inferior aspect of the calcaneus in line with the proposed osteotomy. A curved hemostat was used to deepen the lateral inferior incision to the level of the bone and the curved hemostat was advanced from inferior lateral to lateral superior connecting the tunnels to create the final subperiosteal tunneling. The free end of the Gigli saw was clamped to the tip of the curved hemostat and pulled in retrograde fashion from lateral superior to lateral inferior aspect of the calcaneus (Figure 4).

Figure #4
• Fluoroscopy imaging was used to assess the placement of the Gigli saw and to confirm the final position of the proposed calcaneal osteotomy (Figure 5&6). The handles were hooked to the loops of the gigli saw at the two ends. The osteotomy was performed at approximately 45 degree from the plantar surface of the foot with the foot stabilized and dorsiflexed by the assistant.

Figure #5
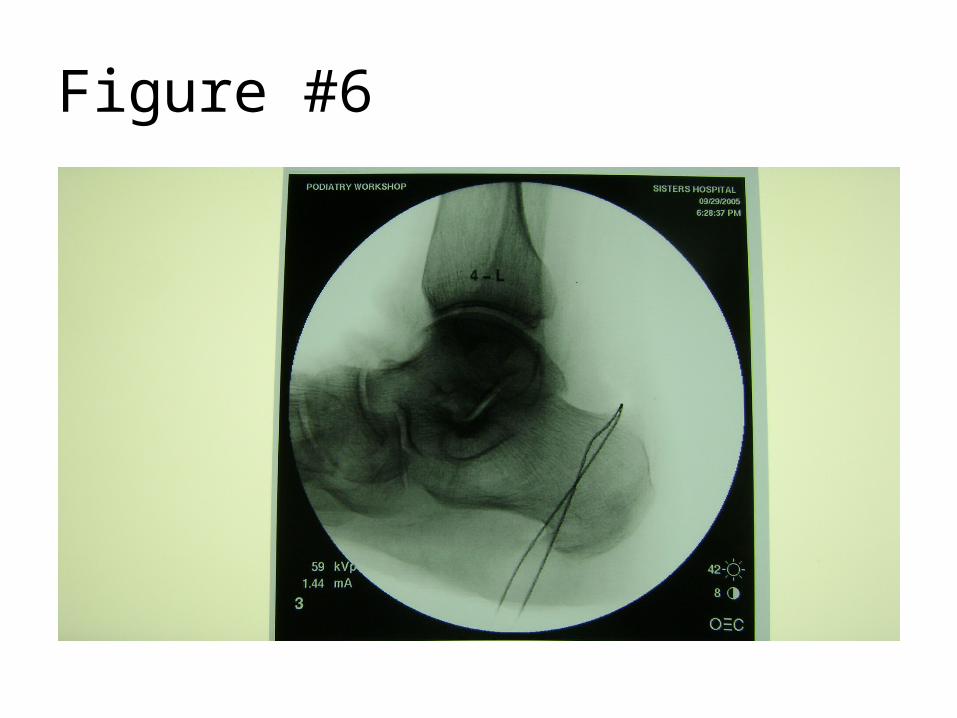
Figure #6
• It is extremely important that the surgical assistant dorsiflexes the ankle and the digits of the foot as this act as dynamic stabilization. Regarding the pull of the Gigli saw, the arms of the surgeon start out close together and quickly fan out while performing the osteotomy (Figure7). As the saw goes from the superior calcaneus to the inferior aspect of the calcaneus, the gigli saw goes from an arced position over the superior posterior calcaneus to a straight position when it exits the inferior cortices of the calcaneous

Figure #7
• Care was taken to prevent kinks in the Gigli saw and to protect soft tissue prior to completion of the osteotomy and to protect soft tissue while the Gigli saw exiting toward the inferior medial and inferior lateral stab incisions. The Gigli saw was transected at inferior lateral end and the remaining of the Gigli saw was pulled down from the medial inferior incision.
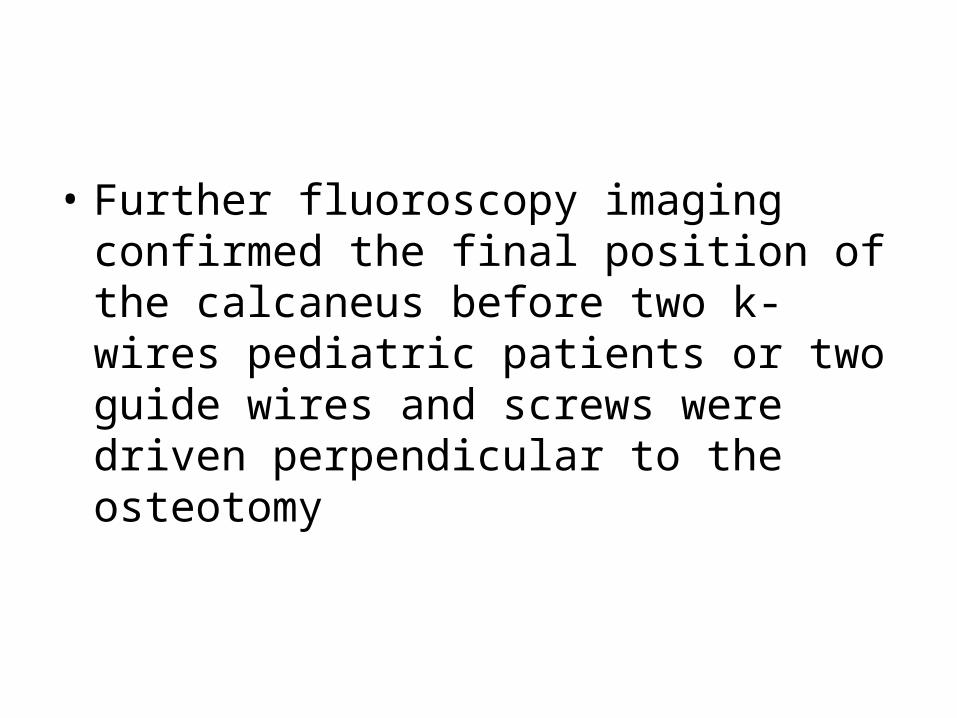
• Further fluoroscopy imaging confirmed the final position of the calcaneus before two k-wires pediatric patients or two guide wires and screws were driven perpendicular to the osteotomy
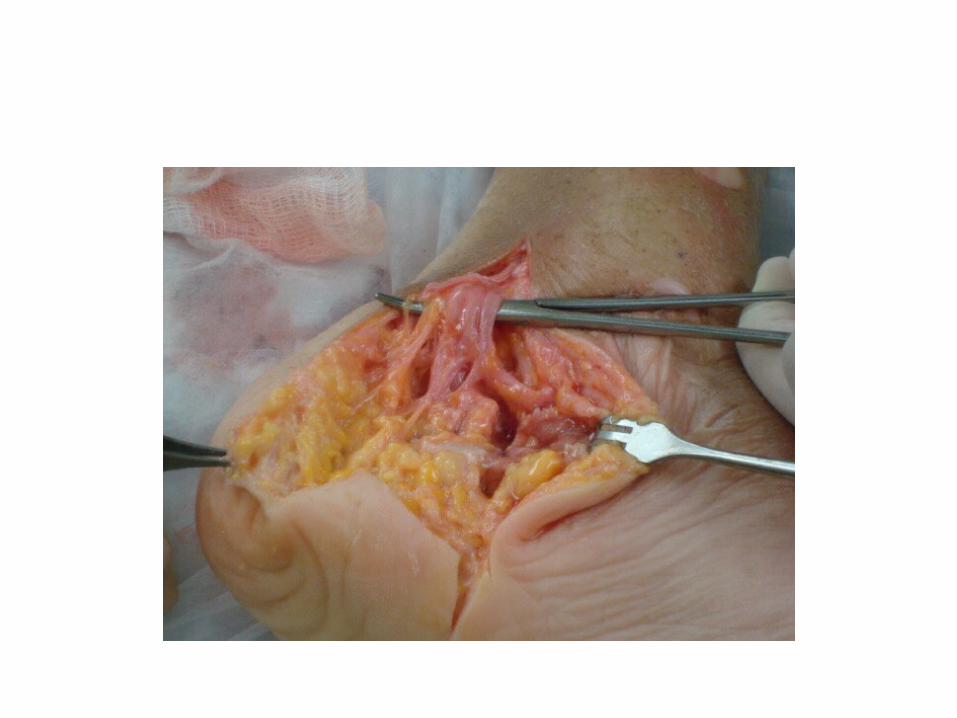
RESULTS:
• The cadavers were further examined after each meticulous dissection at the posteromedial aspect of the heel. Each neurovascular structure was identified and followed distally. The medial plantar nerve, the lateral plantar nerve, the calcaneal sensory branch of the lateral plantar nerve, the posterior tibial artery and its branches were studied in detail at the medial aspect of the calcaneus after PCDO performance. All of the mentioned structures were found to be intact and were able to bluntly dissect distally without signs of trauma (Figures 11-16).


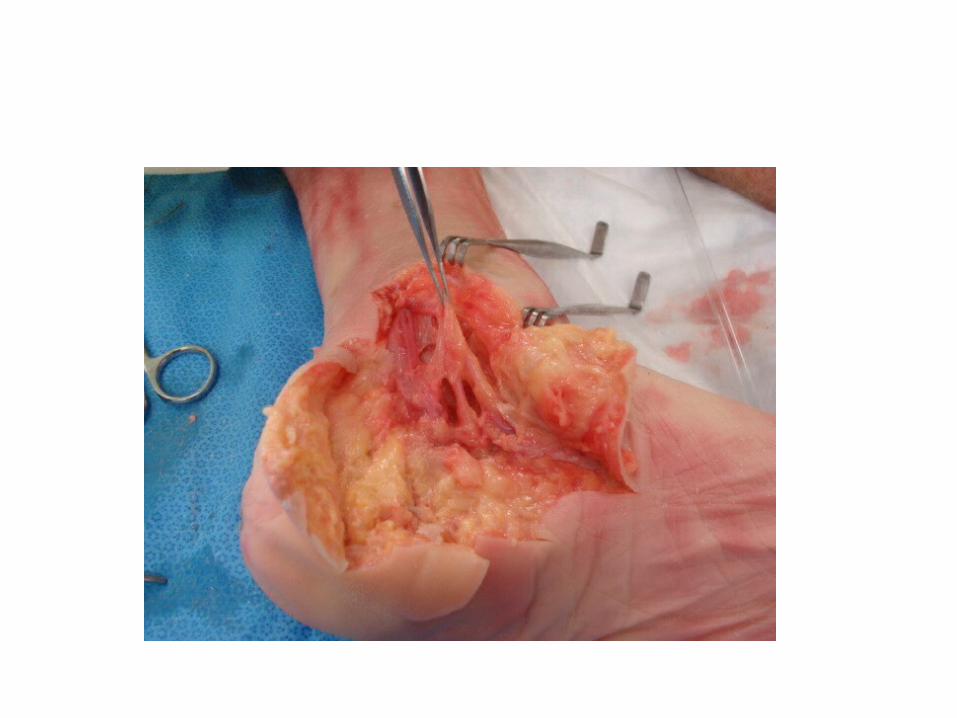
Discussion:
• Our anatomic dissection at the medial aspect of the hindfoot confirms that PCDO is a powerful osteotomy 2,4 which minimizes trauma to the medial neuromuscular structures and soft tissues. This surgical procedure can help to reduce post-operative complications as mentioned earlier.
• The surgeon should be well versed in rearfoot anatomy and rearfoot procedures to perform the PCDO. Fluoroscopy should be utilized to perform the osteotomy, to confirm final placement of the Gigli saw, and to evaluate the correction post-operatively.
•
CONCLUSION:
• The use of percutaneous calcaneal osteotomy is advocated to correct flatfoot deformities and to prevent further progression of the deformity. Our anatomical cadaver study confirms that soft tissue and medial neurovascular structures are well protected after PCDO. Thus, post-operative complications can be prevented in order to achieve pleasing results. It is the surgeon’s choice and proficiency that will dictate the successful outcomes after PCDO procedure.
REFERENCES:• Dull J, DiDomenico L. Percutaneous Displacement Calcaneal Osteotomy. Journal of Foot and Ankle Surgery 43(5): 336-337,2004.• Greene DL, Thompson MG, Gesink DS, Graves SC. Anatomic study of the medial neurovascular structures in relation to calcaneal
osteotomy. Foot Ankle Int 22:569-571, 2001.• Koutsogiannis E: Treatment of Mobile Flat foot by Displacement Osteotomy of the Calcaneus. JBJS, 53B(1), Feb 1971, 96-100.• Didomenico L. A closer look at the Percutaneous calcaneal Displacement Osteotomy. Podiatry Today ISSN: 1045-7860, Vol 19, May
2006.• Mosier-LaClair S, Pomeroy G, Manoli A 2nd: Operative treatment of the difficult stage 2 adult acquired flatfoot deformity. Foot Ankle Clin,
6(1):95-119, 2001.• Bluman E, Title C, Myerson M. Posterior Tibial Tendon Rupture: A Refined Classification System. Foot Ankle Clin N Am 12: 233-249,
2007.• Sammarco J, Hockenbury T. Treatment of Stage II Posterior Tibial Tendon Dysfunction with Flexor Hallucis Longus Transfer and Medial
Displacement Calcaneal Osteotomy. Foot Ankle Int 2001:22: 305-311.• Mendicino SS: Posterior tibial tendon dysfunction. Diagnosis, evaluation and treatment. Clin Podiatr Med Surg, 17(1):33-54, 2000.• Myerson MS, Corrigan J: Treatment of posterior tibial tendon dysfunction with flexor digitorum longus tendon transfer and calcaneal
osteotomy. Orthopedics, 19(5):383-8, 1996.• Myerson MS, Corrigan J, Thompson F, Schon LC: Tendon transfer combined with calcaneal osteotomy for treatment of posterior tibial
tendon insufficiency: a radiological investigation. Foot Ankle Int, 16(11):712-8, 1995.• Myerson MS: Adult Acquired flatfoot Deformity. JBJS, 78A(5) May 1996, 780-792.• Arangio G, Salathe E. A Biomechanical analysis of posterior tibial tendon dysfunction, medial displacement calcaneal osteotomy and
flexor digitorium longus transfer in adult acquired flat foot. Clinical Biomechanics, 24: 385-390, 2009.• Vora AM, Tien TR, Parks BG, Schon LC. Correction of severe and moderate flexible flatfoot with medializing calcaneal osteotomy and
flexor digitorium longus transfer. J Bone Joint Surg 88A:1726-1734, 2006.• Dollard MD, Marcinko DE, Lazerson A, Elleby DH: The Evans calcaneal osteotomy for correction of flexible flatfoot syndrome. J Foot
Surg, 23(4):291-301, 1984.
• THANK YOU