cadth 2015 a3 ramji
TRANSCRIPT

CADTH SYMPOSIUM : HCV:
NATURAL HISTORY AND THERAPEUTICS
Alnoor RamjiGastroenterology & HepatologyClinical Associate ProfessorDivision of GastroenterologyUniversity Of British ColumbiaSt. Paul’s Hospital [email protected]

Company Name Relationship
Abbvie Investigator, consultant
BI Investigator, Consultant
BMS Investigator, Consultant, Speaker
Gilead Sci. Inc Investigator, Consultant, Speaker
Hoffman LaRoche Investigator, Consultant, SpeakerNursing Support
Janssen (J. & J.) Investigator, Consultant, Speaker
Novartis Investigator
Merck & Co. Investigator, Consultant, SpeakerNursing Support
Vertex Pharmaceuticals Investigator, Consultant, Speaker
Disclosures

Objectives
• Review the natural history of hepatitis C and its complications.
• Understand Treatment options for hepatitis C– Pegylated-interferon + ribavirin +/- Direct acting
anti-virals (DAA’s).
– Combination DAA’s

1a, 1b 2a, 2b,
3a
1a, 1b 2a, 2b,
2c, 3a
4
5a
1b
1b, 6
1b, 3a
1b, 3a
3b
4
Fang et al. Clin Liver Dis. 1997.
HCV Infection: Worldwide Genotype Distribution
1a, 1b, 2b, 3a
2a

5HCC: hepatocellular carcinoma.1. Alter and Seeff. Semin Liver Dis. 2000;20:17-35; 2. Pinette et al. Public Health Agency of Canada. Available from: http://www.phac-aspc.gc.ca/hepc/pubs/pdf/hepc_guide eng.pdf; 3.Myers et al. Can Gastroenterol. 2012;26:359-75.
Projection of Lifetime Outcomes1
100 patients with acute HCV infections
100 patients with acute HCV infections
24 patientschronic, nonprogressive
24 patientschronic, nonprogressive
24 patientssevere progressive hepatitis
24 patientssevere progressive hepatitis
32 patientsvariable progression
32 patientsvariable progression
20 patients recover20 patients recover 80 patientspersistent infection
80 patientspersistent infection
All patients should seek antiviral therapy2,3All patients should seek antiviral therapy2,3
End-stage disease, HCC, liver transplantation,
death
End-stage disease, HCC, liver transplantation,
death
Treatment failureTreatment failureSustained response/cureSustained response/cure
Outcomes:Outcomes:
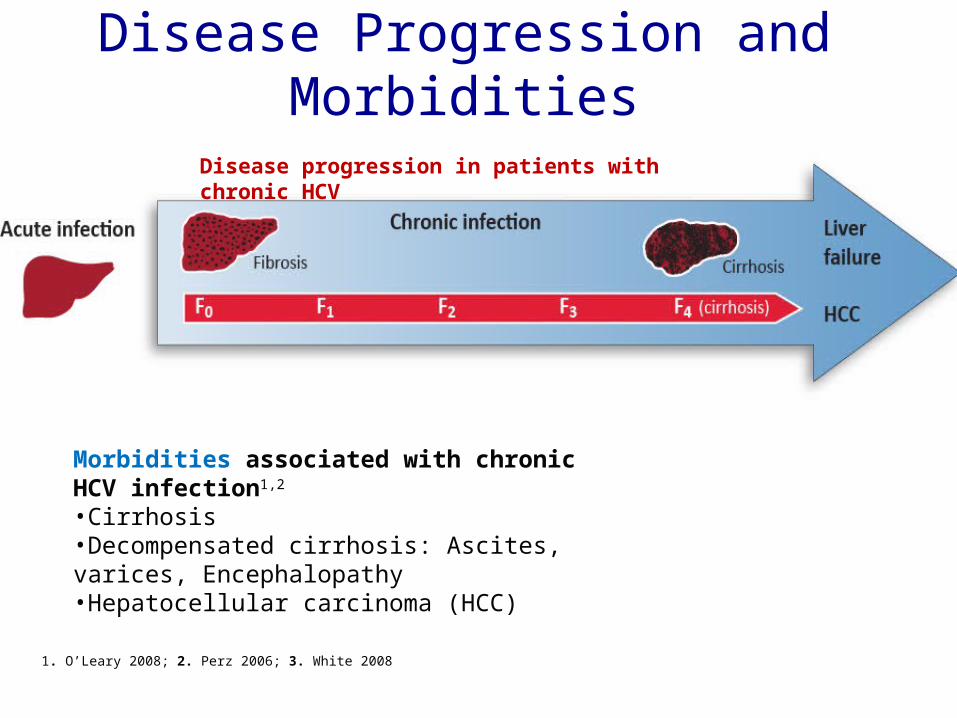
Disease Progression and Morbidities
6Pre-Submission Briefing Meeting | July 2014 | Company Confidential © 2014 AbbVie
1. O’Leary 2008; 2. Perz 2006; 3. White 2008
Disease progression in patients with chronic HCV
Morbidities associated with chronic HCV infection1,2
•Cirrhosis•Decompensated cirrhosis: Ascites, varices, Encephalopathy•Hepatocellular carcinoma (HCC)

• 312 patients with initially compensated cirrhosis of viral aetiology
Cirrhotic patients at risk of serious morbidity
Benvegnù L, et al. Gut 2013; 53: 744‒9
Patients at riskHCC 312 311 310 303 297 268 226 189 153 129 94 65 45 27 11 5
Variceal bleeding 312 312 312 309 301 269 237 190 163 131 97 71 44 29 13 7
Ascites 312 311 312 305 296 259 223 181 152 125 93 60 48 30 15 9
Encephalopathy 312 312 312 309 300 270 235 192 161 127 95 65 43 30 13 7
Cu
mu
lati
ve r
isk
(%)
Years of follow-up
HCCVariceal bleedingAscitesPortal-systemic encephalopathy
50
40
30
20
10
00 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15

Variceal Hemorhage

Adapted from the US Food and Drug Administration, Antiviral Drugs Advisory Committee Meeting, April 27-28, 2011, Silver Spring, MD.
SV
R (
%)
IFN6 mos
PegIFN/ RBV 12 mos
IFN12 mos
IFN/RBV12 mos
PegIFN12 mos
2001
1998
2011
StandardIFN
RBV
PegIFN
1991
DAAs
PegIFN/RBV/DAA
IFN/RBV6 mos
6
16
3442 39
55
70+
0
20
40
60
80
100
The Advancing Present
2014/590-98
PegIFN/RBV/DAAOr DAA+RBV

Viral Eradication Improves All-Cause Mortality
10References: 1. Ravazi 2012; 2. Burra 2009; 3. Guillouche 2011; 4. Van der Meer 2012
• Cure = SVR = reduced risk of — All-cause mortality; Liver-related mortality; HCV-related complications:-
Progression to HCC or liver failure4
Pat
ien
t su
rviv
al o
utc
om
es
wit
h a
nd
wit
ho
ut
SV
R
Pre-Submission Briefing Meeting | July 2014 | Company Confidential © 2014 AbbVie

HCV Lifecycle and DAA Targets
Adapted from Manns MP, et al. Nat Rev Drug Discov. 2007;6:991-1000.
Receptor bindingand endocytosis
Fusion and
uncoating
Transportand release
(+) RNA
Translation andpolyprotein processing
RNA replication
Virionassembly
Membranousweb
ER lumen
LD
LDER lumen
LD
NS3/4 protease inhibitors
NS5B polymerase inhibitors
*Role in HCV lifecycle not well defined
NS5A* inhibitors

0
20
40
60
80
100S
VR
(%
)
PegIFN/RBVBOC or TVR + PegIFN/RBV
38-44
67-81
Poordad F, et al. N Engl J Med. 2011;364:1195-1206. Jacobson IM, et al. N Engl J Med. 2011;364:2405-2416.
2012 – 2014: SVR Rates: Boceprevir or Telaprevir with PEG-INF + Ribavirin in Genotype 1 Treatment-Naive
Patients: upto 48 Weeks
F0-2 F3-4
52-62

Boceprevir Triple therapy Safety Profile 48 PR
n=363
BOC RGT
n=368
BOC/PR48
n=366
Median treatment duration, days 203 197 335
Deaths N=4 N=1 N=1
Serious AEs 9% 11% 12%
Discontinued due to AEs 16% 12% 16%
Dose modification due to AEs 26% 40% 35%
Hematologic parameters
Neutrophil count (<750 to 500/mm3 / <500/mm3)
14% / 4% 24% / 6% 25% / 8%
Hemoglobin (<10 to 8.5 g/dL / <8.5 g/dL)
Discontinuation due to anemia
Dose reductions due to anemia
Erythropoietin use
Mean (median) days of use
26% / 4%
1%
13%
24%
121 (109)
45% / 5%
2%
20%
43%
94 (85)
41% / 9%
2%
21%
43%
156 (149)

Adverse Event Arm 1 (PR48); n=363 (%) Arm 2 (RGT); n=368 (%) Arm 3 (BOC/PR48); n=366 (%)
Fatigue 59 52 57
Headache 42 45 43
Nausea 40 46 42
Anemia 29 49 49
Dysgeusia 18 37 43
Chills 28 36 33
Pyrexia 32 33 30
Insomnia 32 31 32
Alopecia 27 20 28
Decreased Appetite 25 26 24
Pruritis 26 23 25
Neutropenia 21 25 25
Influenza Like Illness 25 23 22
Myalgia 26 21 24
Rash 22 24 23
Irritability 24 22 22
Depression 21 23 19
Diarrhea 19 19 23
Dry Skin 18 18 22
Dyspnea 16 18 22
Dizziness 15 21 17
Boceprevir Triple: Common Treatment-Related Adverse Events*
*Reported in >20% of patients in any treatment arm and listed by decreasing overall frequency

0
20
40
60
80
100S
VR
(%
)
Simeprevir
85%
90%
2014 /2015 :Virologic Response to PEG-INF + RBV + Simeprevir or Sofosbuvir in Genotype 1
Treatment-Naive Patients
80%
CirrhosisNoCirrhosis
60%
Sofosbuvir
CirrhosisNo Cirrhosis
Jacobson I, et al. EASL 2013. Abstract 1425. Reproduced with permission.Lawitz E, et al. EASL 2013. Abstract 1411. Reproduced with permission.

0
20
40
60
80
100S
VR
(%
)
SOF/ LDV +/-RBV x 8-12 wks
97-100% 93-100%
Feld JJ, et al. N Engl J Med. 2014;370:1594-1603. Afdhal N, et al. N Engl J Med 2014; 2014 Apr 12Poordad F, et al. EASL 2014. Abstract O163
2015 /2016 :Virologic Response to Non-interferon based therapy: Genotype 1 :Treatment-Naive Patients:
Non-cirrhotic and cirrhotic sub-groups
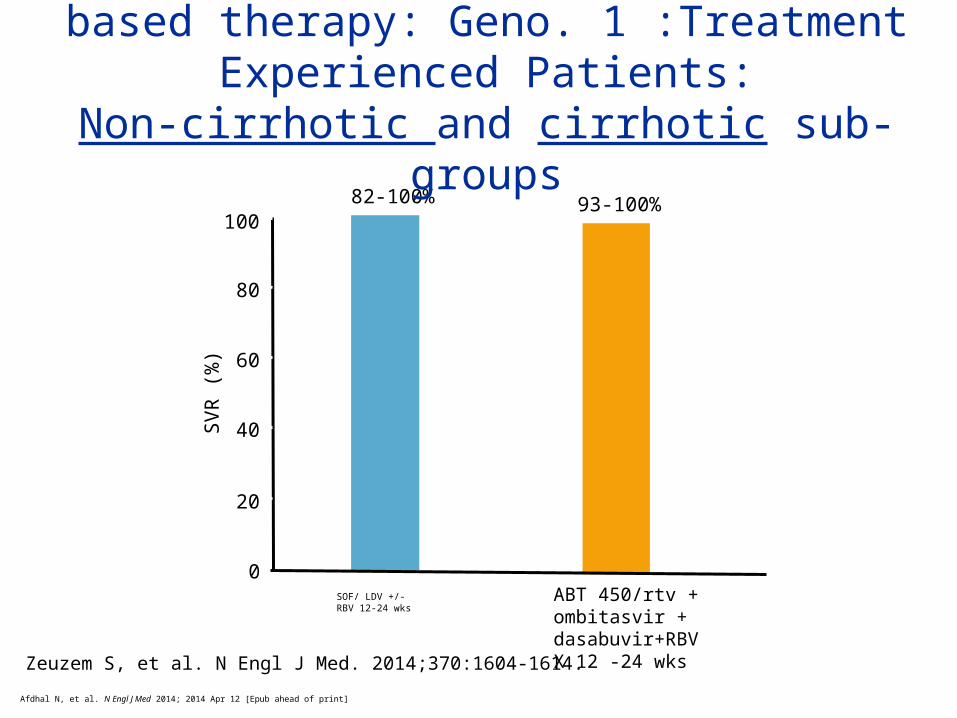
ABT 450/rtv + ombitasvir + dasabuvir+RBVX 12 wks
0
20
40
60
80
100S
VR
(%
)
SOF/ LDV +/-RBV 12-24 wks
82-100% 93-100%
2015 /2016 :SVR to Non-interferon based therapy: Geno. 1 :Treatment Experienced Patients:
Non-cirrhotic and cirrhotic sub-groups
ABT 450/rtv + ombitasvir + dasabuvir+RBVX 12 -24 wks
Afdhal N, et al. N Engl J Med 2014; 2014 Apr 12 [Epub ahead of print]
Zeuzem S, et al. N Engl J Med. 2014;370:1604-1614.

AEs
SAPPHIRE I SAPPHIRE II
3 DAA + RBV(n = 473)
Placebo(n = 158)
3 DAA + RBV(n = 297)
Placebo(n = 97)
Any AE, n (%) 414 (87.5) 116 (73.4) 271 (91.2) 80 (82.5)
AE leading to D/C, n (%) 3 (0.6) 1 (0.6) 3 (1.0) 0
Any serious AE, n (%) 10 (2.1) 0 6 (2.0) 1 (1.0)
Grade 3/4 lab events, n/N (%)
ALT 4/469 (0.9) 7/158 (4.4) 5/296 (1.7) 3/96 (3.1)
AST 3/469 (0.6) 3/158 (1.9) 3/296 (1.0) 1/96 (1.0)
Alkaline phosphatase 0 0 0 0
Creatinine – – 2/297 (0.7) 0
Total bilirubin 13/469 (2.8) 0 7/296 (2.4) 0
Hemoglobin < 8 g/dL 0 0 1/296 (0.3) 0
Hemoglobin < 10 to 8 g/dL, % 5.8 0 4.7 0
Feld JJ, et al. N Engl J Med. 2014;370:1594-1603. Zeuzem S, et al. N Engl J Med. 2014;370:1604-1614.
ABT 450/rtv + ombitasvir + dasabuvir+RBV(Holkira) with RBV in Non-cirrhotic GT1 Pts: Tolerance
compared to placebo
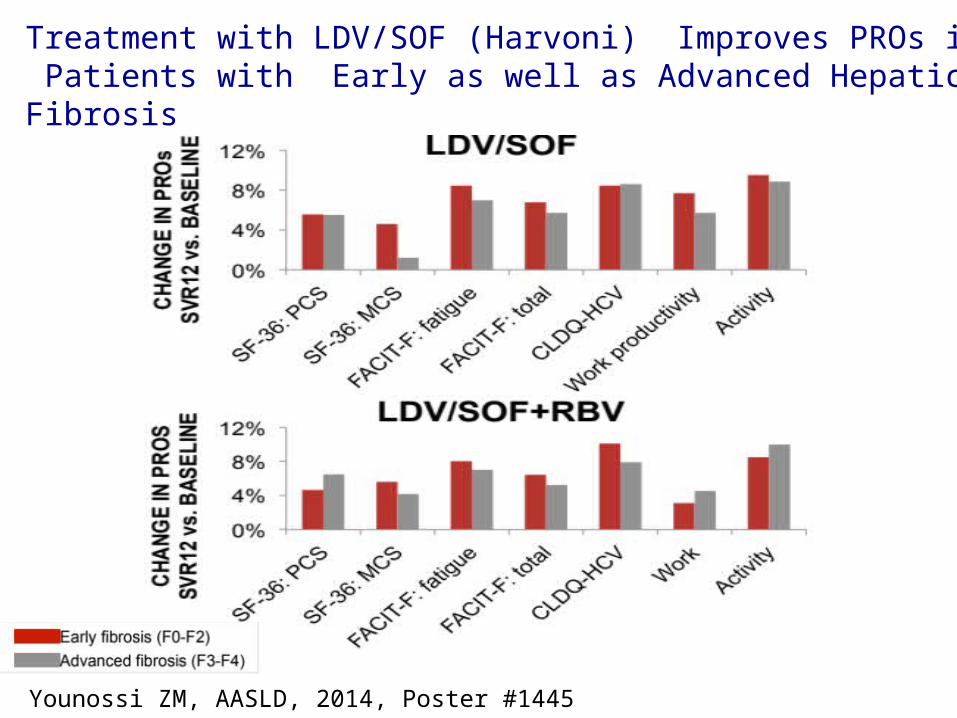
Younossi ZM, AASLD, 2014, Poster #1445
Treatment with LDV/SOF (Harvoni) Improves PROs in CHC Patients with Early as well as Advanced Hepatic Fibrosis

0
20
40
60
80
100S
VR
(%
)
PegIFN/RBVX 24 wks
70-80%
97%
Poordad F, et al. N Engl J Med. 2011;364:1195-1206. Jacobson IM, et al. N Engl J Med. 2011;364:2405-2416.
2014 /2015 :Virologic Response to PEG-INF + RBV vs. Sofosbuvir + RBV (all-oral) in Genotype 2 and 3
Treatment-Naive Patients
Geno 2SOF+RBVX 12 wks
92-94%
Geno 3SOF+RBVX 24 wks
Gane E, et al. J Hepatol. 2013;58(suppl 1):S3. Abstract 5.Lawitz E, et al. N Engl J Med. 2013;368:1878-1887.

LDV/SOF (Harvoni) + RBV for HCV Patients with Decompensated Cirrhosis: SVR-12
SOLAR-1: LDV/SOF + RBV in Decompensated Cirrhosis
CTP B CTP C
SV
R12
(%
)
26/30 19/22 18/2024/27
Error bars represent 90% confidence intervals.
LDV/SOF + RBV 12 Weeks LDV/SOF + RBV 24 Weeks
SVR rates were similar with 12 or 24 weeks of LDV/SOF + RBV
Flamm, AASLD, 2014, Oral #239
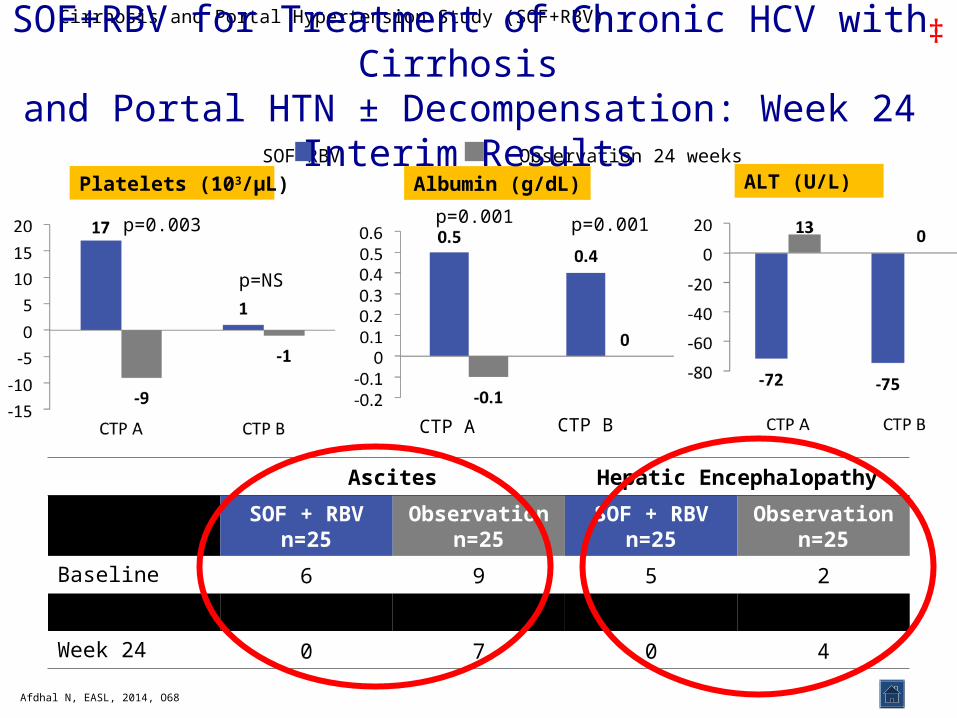
Ascites Hepatic Encephalopathy
Patients, nSOF + RBV
n=25Observation
n=25SOF + RBV
n=25Observation
n=25
Baseline 6 9 5 2
Week 12 5 8 3 3
Week 24 0 7 0 4
Cirrhosis and Portal Hypertension Study (SOF+RBV)
Platelets (103/µL) Albumin (g/dL)
SOF+RBV Observation 24 weeks
ALT (U/L)
CTP A CTP B
Afdhal N, EASL, 2014, O68
p=0.003
p=NS
p=0.001 p=0.001
‡SOF+RBV for Treatment of Chronic HCV with Cirrhosis
and Portal HTN ± Decompensation: Week 24 Interim Results

Hepatitis C: Summary
• HCV has a slowly progressive course to cirrhosis, with complications of decompensated disease.
• Newer regimen: all-oral, efficacious, well tolerated
• Viral eradication / cure in 70-98%
• Viral eradication has a mortality benefit

CADTH SYMPOSIUM : HCV:
NATURAL HISTORY AND THERAPEUTICS
Alnoor RamjiGastroenterology & HepatologyClinical Associate ProfessorDivision of GastroenterologyUniversity Of British ColumbiaSt. Paul’s Hospital [email protected]