can surgery improve neurological function in penetrating ... · spinal cord injury from spinal gsws...
TRANSCRIPT

Neurosurg Focus / Volume 28 / May 2010
Neurosurg Focus 28 (5):E4, 2010
1
Patients with PSIs present very complex, multi-disciplinary management challenges for military surgeons. Not only can the patient have immedi-
ate and delayed life-threatening damage to organs along the path of the projectile, the spinal column and possibly the neurological structures contained within can also, by definition, suffer injury, the severity of which depends on multiple factors. Spinal cord injury from spinal GSWs is more often a complete lesion with a decreased poten-
tial for neurological recovery than with closed trauma.43 There are a number of potential surgical indications, the most controversial of which is whether decompressive laminectomy has any effect on neurological recovery. Medical civilian and military literature is replete with opinions for and against the use of surgery.
Although missile characteristics such as size, compo-sition and design are important, the major determinant of the destructive ability of a projectile is velocity at impact and thus the kinetic energy imparted to the surrounding tissue.10 Energy is calculated based on mass and velocity as follows: energy = 1/2mv2. Therefore, velocity has a sig-nificantly greater effect on energy than projectile mass.
Can surgery improve neurological function in penetrating spinal injury? A review of the military and civilian literature and treatment recommendations for military neurosurgeons
Paul Klimo Jr., m.D., m.P.H.,1 Brian T. ragel, m.D.,2 micHael rosner, m.D.,3 Wayne gluf, m.D.,4 anD ranDall mccafferTy, m.D.5
188th Medical Group, Wright-Patterson Air Force Base, Ohio; 2Department of Neurological Surgery, Oregon Health & Science University, Portland, Oregon; 3Division of Neurosurgery, Walter Reed Medical Center, Washington, DC; 4Naval Medical Center, San Diego, California; and 5Wilford Hall Medical Center, Lackland Air Force Base, Texas
Object. Penetrating spinal injury (PSI), although an infrequent injury in the civilian population, is not an infre-quent injury in military conflicts. Throughout military history, the role of surgery in the treatment of PSI has been controversial. The US is currently involved in 2 military campaigns, the hallmark of both being the widespread use of various explosive devices. The authors reviewed the evidence for or against the use of decompressive laminectomy to treat PSI to provide a triservice (US Army, Navy, and Air Force) consensus and treatment recommendations for military neurosurgeons and spine surgeons.
Methods. A US National Library of Medicine PubMed database search that identified all literature dealing with acute management of PSI from military conflicts and civilian urban trauma centers in the post–Vietnam War period was undertaken.
Results. Nineteen retrospective case series (11 military and 8 civilian) met the study criteria. Eleven military articles covered a 20-year time span that included 782 patients who suffered either gunshot or blast-related projectile wounds. Four papers included sufficient data that analyzed the effectiveness of surgery compared with nonoperative management, 6 papers concluded that surgery was of no benefit, 2 papers indicated that surgery did have a role, and 3 papers made no comment. Eight civilian articles covered a 9-year time span that included 653 patients with spinal gunshot wounds. Two articles lacked any comparative data because of treatment bias. Two papers concluded that decompressive laminectomy had a beneficial role, 1 paper favored the removal of intracanal bullets between T-12 and L-4, and 5 papers indicated that surgery was of no benefit.
Conclusions. Based on the authors’ military and civilian PubMed literature search, most of the evidence suggests that decompressive laminectomy does not improve neurological function in patients with PSI. However, there are serious methodological shortcomings in both literature groups. For this and other reasons, neurosurgeons from the US Air Force, Army, and Navy collectively believe that decompression should still be considered for any patient with an incomplete neurological injury and continued spinal canal compromise, ideally within 24–48 hours of injury; the patient should be stabilized concurrently if it is believed that the spinal injury is unstable. The authors recognize the highly controversial nature of this topic and hope that this literature review and the proposed treatment recommenda-tions will be a valuable resource for deployed neurosurgeons. Ultimately, the deployed neurosurgeon must make the final treatment decision based on his or her opinion of the literature, individual abilities, and facility resources avail-able. (DOI: 10.3171/2010.2.FOCUS1036)
Key WorDs • penetrating spinal injury • spinal gunshot wound • blast injury • military • decompression • laminectomy • outcome
1
Abbreviations used in this paper: GSW = gunshot wound; IED = improvised explosive device; PSI = penetrating spinal injury; SCI = spinal cord injury; VB = vertebral body.
Report Documentation Page Form ApprovedOMB No. 0704-0188
Public reporting burden for the collection of information is estimated to average 1 hour per response, including the time for reviewing instructions, searching existing data sources, gathering andmaintaining the data needed, and completing and reviewing the collection of information. Send comments regarding this burden estimate or any other aspect of this collection of information,including suggestions for reducing this burden, to Washington Headquarters Services, Directorate for Information Operations and Reports, 1215 Jefferson Davis Highway, Suite 1204, ArlingtonVA 22202-4302. Respondents should be aware that notwithstanding any other provision of law, no person shall be subject to a penalty for failing to comply with a collection of information if itdoes not display a currently valid OMB control number.
1. REPORT DATE MAY 2010 2. REPORT TYPE
3. DATES COVERED 00-00-2010 to 00-00-2010
4. TITLE AND SUBTITLE Can surgery improve neurological function in penetrating spinal injury?A review of the military and civilian literature and treatmentrecommendations for military neurosurgeons
5a. CONTRACT NUMBER
5b. GRANT NUMBER
5c. PROGRAM ELEMENT NUMBER
6. AUTHOR(S) 5d. PROJECT NUMBER
5e. TASK NUMBER
5f. WORK UNIT NUMBER
7. PERFORMING ORGANIZATION NAME(S) AND ADDRESS(ES) 88th Medical Group,Wright-Patterson AFB,OH,45433
8. PERFORMING ORGANIZATIONREPORT NUMBER
9. SPONSORING/MONITORING AGENCY NAME(S) AND ADDRESS(ES) 10. SPONSOR/MONITOR’S ACRONYM(S)
11. SPONSOR/MONITOR’S REPORT NUMBER(S)
12. DISTRIBUTION/AVAILABILITY STATEMENT Approved for public release; distribution unlimited
13. SUPPLEMENTARY NOTES
14. ABSTRACT
15. SUBJECT TERMS
16. SECURITY CLASSIFICATION OF: 17. LIMITATION OF ABSTRACT Same as
Report (SAR)
18. NUMBEROF PAGES
11
19a. NAME OFRESPONSIBLE PERSON
a. REPORT unclassified
b. ABSTRACT unclassified
c. THIS PAGE unclassified
Standard Form 298 (Rev. 8-98) Prescribed by ANSI Std Z39-18
P. Klimo et al.
2 Neurosurg Focus / Volume 28 / May 2010
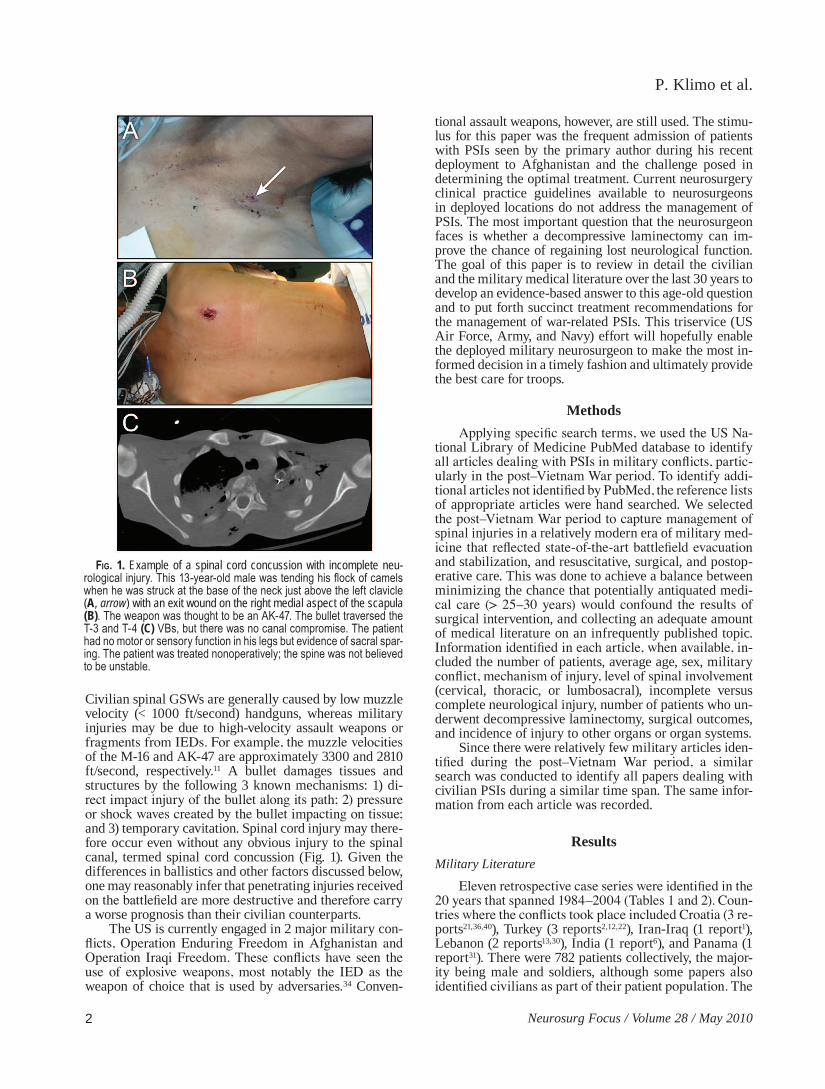
Civilian spinal GSWs are generally caused by low muzzle velocity (< 1000 ft/second) handguns, whereas military injuries may be due to high-velocity assault weapons or fragments from IEDs. For example, the muzzle velocities of the M-16 and AK-47 are approximately 3300 and 2810 ft/second, respectively.11 A bullet damages tissues and structures by the following 3 known mechanisms: 1) di-rect impact injury of the bullet along its path; 2) pressure or shock waves created by the bullet impacting on tissue; and 3) temporary cavitation. Spinal cord injury may there-fore occur even without any obvious injury to the spinal canal, termed spinal cord concussion (Fig. 1). Given the differences in ballistics and other factors discussed below, one may reasonably infer that penetrating injuries received on the battlefield are more destructive and therefore carry a worse prognosis than their civilian counterparts.
The US is currently engaged in 2 major military con-flicts, Operation Enduring Freedom in Afghanistan and Operation Iraqi Freedom. These conflicts have seen the use of explosive weapons, most notably the IED as the weapon of choice that is used by adversaries.34 Conven-
tional assault weapons, however, are still used. The stimu-lus for this paper was the frequent admission of patients with PSIs seen by the primary author during his recent deployment to Afghanistan and the challenge posed in determining the optimal treatment. Current neurosurgery clinical practice guidelines available to neurosurgeons in deployed locations do not address the management of PSIs. The most important question that the neurosurgeon faces is whether a decompressive laminectomy can im-prove the chance of regaining lost neurological function. The goal of this paper is to review in detail the civilian and the military medical literature over the last 30 years to develop an evidence-based answer to this age-old question and to put forth succinct treatment recommendations for the management of war-related PSIs. This triservice (US Air Force, Army, and Navy) effort will hopefully enable the deployed military neurosurgeon to make the most in-formed decision in a timely fashion and ultimately provide the best care for troops.
MethodsApplying specific search terms, we used the US Na-
tional Library of Medicine PubMed database to identify all articles dealing with PSIs in military conflicts, partic-ularly in the post–Vietnam War period. To identify addi-tional articles not identified by PubMed, the reference lists of appropriate articles were hand searched. We selected the post–Vietnam War period to capture management of spinal injuries in a relatively modern era of military med-icine that reflected state-of-the-art battlefield evacuation and stabilization, and resuscitative, surgical, and postop-erative care. This was done to achieve a balance between minimizing the chance that potentially antiquated medi-cal care (> 25–30 years) would confound the results of surgical intervention, and collecting an adequate amount of medical literature on an infrequently published topic. Information identified in each article, when available, in-cluded the number of patients, average age, sex, military conflict, mechanism of injury, level of spinal involvement (cervical, thoracic, or lumbosacral), incomplete versus complete neurological injury, number of patients who un-derwent decompressive laminectomy, surgical outcomes, and incidence of injury to other organs or organ systems.
Since there were relatively few military articles iden-tified during the post–Vietnam War period, a similar search was conducted to identify all papers dealing with civilian PSIs during a similar time span. The same infor-mation from each article was recorded.
ResultsMilitary Literature
Eleven retrospective case series were identified in the 20 years that spanned 1984–2004 (Tables 1 and 2). Coun-tries where the conflicts took place included Croatia (3 re-ports21,36,40), Turkey (3 reports2,12,22), Iran-Iraq (1 report1), Lebanon (2 reports13,30), India (1 report6), and Panama (1 report31). There were 782 patients collectively, the major-ity being male and soldiers, although some papers also identified civilians as part of their patient population. The
Fig. 1. Example of a spinal cord concussion with incomplete neu-rological injury. This 13-year-old male was tending his flock of camels when he was struck at the base of the neck just above the left clavicle (A, arrow) with an exit wound on the right medial aspect of the scapula (B). The weapon was thought to be an AK-47. The bullet traversed the T-3 and T-4 (C) VBs, but there was no canal compromise. The patient had no motor or sensory function in his legs but evidence of sacral spar-ing. The patient was treated nonoperatively; the spine was not believed to be unstable.

Neurosurg Focus / Volume 28 / May 2010
Can surgery improve neurological function in PSIs?
3
mean age ranged from 20 to 39 years, the latter being the average from a group of injured citizens included in one report.21 Gunshot wounds were clearly identified as the mechanism in 333 patients and fragmentation from an explosive device in 378. One paper did not make the distinction between the two mechanisms.13 Two papers specified the kinetics of the weapon used (low velocity vs high velocity).6,12 The thoracic spine was most com-monly involved (317 [41%] of 782 patients), followed by lumbosacral (285 [36%] of 782 patients) and cervical (180 [23%] 782 patients). Of the 606 patients in whom their admission neurological function was known, 306 (50%) had a complete SCI. Decompressive laminectomy was performed in 382 patients, 31 of whom underwent stabili-zation as well. Associated organ injuries occurred in 45% of patients (350 of 775).
Only 4 papers had sufficient data to allow any conclu-sion to be drawn regarding the efficacy of decompressive surgery compared with conservative management (Table 2). The other papers either did not present adequate pre- and postoperative neurological data or were biased in their treatment (that is, they treated all patients either surgically or nonoperatively), thus rendering any comparison impos-sible. Despite presenting inadequate supportive data, the authors of 4 other papers rendered a position statement on the role of surgery. Overall, 6 papers concluded that decom-pressive surgery was of no benefit, 2 indicated that surgery was a benefit in all patients with a neurological deficit (1 report) or only in those with an incomplete or cauda equina injury (1 report), and 3 papers made no comment.
Civilian LiteratureEight retrospective case series met our search crite-
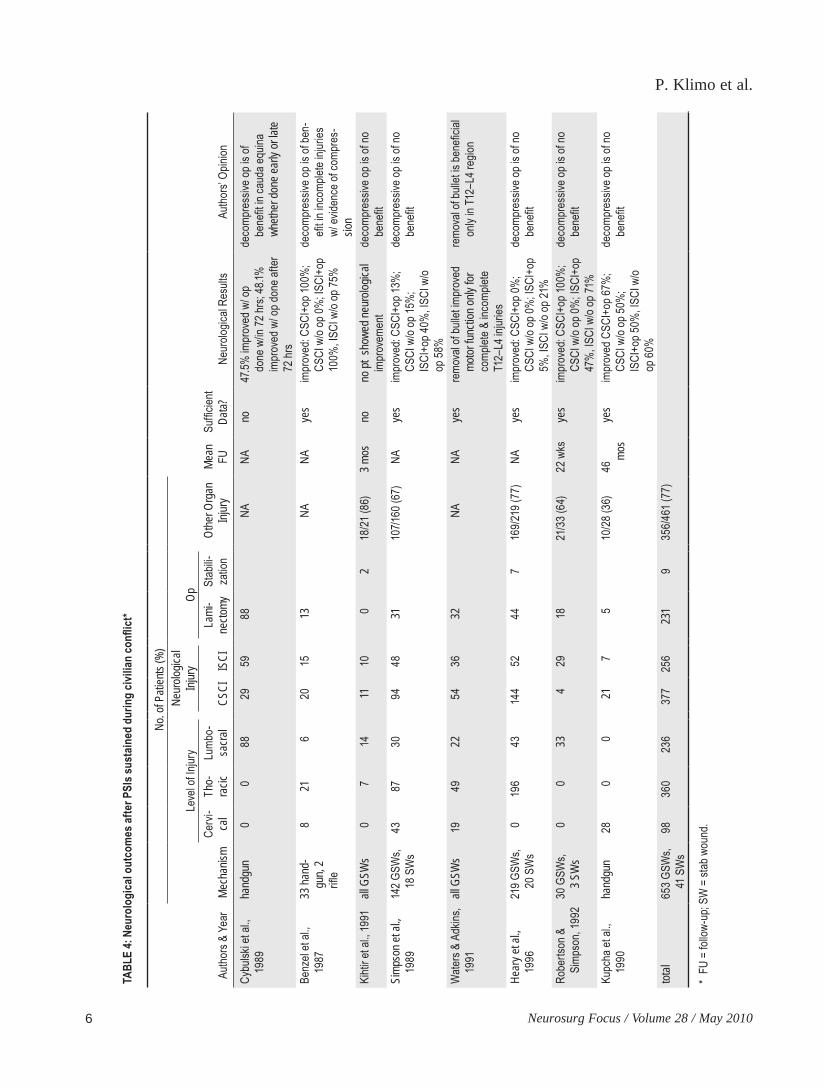
ria in the 9 years that spanned 1987–1996 (Tables 3 and 4). Although 2 papers were published in the post–Viet-nam War era, their data collection occurred during the Vietnam War era and thus were excluded.17,41 Metropoli-tan trauma centers included Philadelphia (2 reports16,25),
Houston (2 reports35,38), Los Angeles (1 report45), Shreve-port (1 report5), Chicago (1 report9), and The Bronx (1 report23). There were 694 patients collectively, the vast majority being male (639 patients). The mean age ranged from 24.7 to 32 years. Gunshot wounds from low-velocity handguns were the most common mechanism. Although some series also included patients with stab wounds, the neurological data in Table 4 reflect only those patients with GSWs, but some of the demographic data in Table 3 includes the stab wound victims. The thoracic spine was again the most commonly involved region (360 [52%] of 694), followed by lumbosacral (236 [34%] of 694), and cervical (98 [14%] of 694). Of the 633 patients in whom the admission neurological function was known, 377 (60%) had a complete SCI. Decompressive laminectomy was performed in 231 patients, and only 9 underwent con-current stabilization. Associated organ injuries occurred in a high percentage of patients (356 [77%] of 461).
Only 2 papers had sufficient data to draw any conclu-sion on the efficacy of decompressive surgery compared with conservative management (Table 4). This was due to treatment bias. Cybulski et al.9 operated on all patients; Kihtir et al.23 did not operate on any patient. Despite lack of comparative data in these 2 papers, the authors of all papers rendered an opinion on the role of surgery based on their experience. Overall, 2 papers concluded that de-compressive surgery had a beneficial role (in cauda equina or incomplete lesions [1 report each]), 1 paper indicated that removal of the bullet was of benefit between T-12 and L-4 in either incomplete or complete SCI, and 5 papers indicated that there was no evidence to support the use of decompressive laminectomy.
DiscussionHistory
An early and one of the most well-known fatalities due to a PSI was that of the great British naval Vice Ad-
TABLE 1: Demographics of patients with PSIs in military conflicts*
Authors & Year Conflict No. of Patients Mean Age (yrs)
Janković et al., 1998 Croatian War 96 (86 soldiers, 10 civilians [4 F, 6 M]) 28.3 (soldiers), 38.8 (civilians)Alaca et al., 2002 terrorism in Turkey 105 25Splavski et al., 1996 Croatian War 21 (10 soldiers, 11 civilians [7 M, 4 F]) 30.7Aarabi et al., 1996 Iran-Iraq War 205 (145 w/ follow-up) NAKahraman et al., 2004 terrorism in Turkey 106 21.2Ohry & Rozin, 1984 Lebanon War 12 (7 soldiers, 5 civilians) 19.7Duz et al., 2008 terrorism in Turkey 129 20.3Rukovansjki, 1996 Croatian War 20 (16 M, 4 F) NABhatoe & Singh, 2003 India 22 30.7Hammoud et al., 1995 Lebanon War 64 25Parsons et al., 1993 Operation Just Cause
(Panama)2 (M) 23
total 782 19.7 (soldiers), 38.8 (civilians)
* NA = not available.
P. Klimo et al.
4 Neurosurg Focus / Volume 28 / May 2010
TABL
E 2:
Neu
rolo
gica
l out
com
e of P
SIs s
usta
ined
dur
ing
mili
tary
confl
ict*
No. o
f Pati
ents
(%)
Mec
hanis
mLe
vel o
f Injur
y Ne
urolo
gical
Injur
y Op
Auth
ors &
Ye
arGS
WEx
pl/Bl
ast
Cer-
vical
Tho-
racic
Lum
-ba
rSa
cral
CSCI
ISCI
Lami
nec-
tomy
Stab
ili-za
tion
Othe
r Org
an
Injur
y (%)
Suffic
ient
Data?
†Ne
urolo
gical
Resu
ltsAu
thor
s’ Op
inion
Jank
ović
et al.
, 199
849
4719
2156
NANA
276
50/9
6 (52
)no
NAde
comp
ress
ive op
is
of no
bene
fitAl
aca e
t al.,
2002
987
268
305
8817
5672
/105 (
69)
noNA
NA
Splav
ski e
t al.
, 199
612
38
82
1011
171
10/21
(48)
nono
CSC
I pt im
prov
ed; a
ll ISC
I pts
impr
oved
all pt
s w/ n
euro
logica
l de
ficit s
hould
un-
derg
o dec
ompr
es-
sive o
p imm
ediat
elyAa
rabi
et al.
, 19
9660
138
4010
263
90/14
5
(62)
55/14
5
(38)
87/14
5
(60)
49/2
05 (2
4)ye
sim
prov
ed: C
SCI+
op 24
%; C
SCI
w/o o
p 27.5
%; IS
CI+o
p 91%
, IS
CI w
/o op
100%
deco
mpre
ssive
op is
of
no be
nefit
Kahr
aman
et
al., 2
004
868
3525
4623
8365
49/10
6 (46
)ye
s36
/53 (
68%)
w/ o
p imp
rove
d; 17
/28 (
60%)
w/o
op im
prov
edde
comp
ress
ive op
is
of no
bene
fitOh
ry &
Roz
in,
1984
11
14
53
75
25/1
2 (42
)no
1 pt im
prov
ed w
/ op;
2 pts
impr
oved
w/o
opde
comp
ress
ive op
is
of no
bene
fitDu
z et a
l., 20
08
53 (3
7 high
ve
l, 16
low ve
l)
7639
3159
2410
574
2454
/129 (
41.9)
yes
56.9
% im
prov
ed w
/ op;
57.5%
im
prov
ed w
/o op
deco
mpre
ssive
op is
of
no be
nefit
Ruko
vans
jki,
1996
118
84
NANA
1213
/20 (
65)
nono
preo
p dat
a; po
stop 8
wer
e Fr
anke
l Gra
de A
or B
, 10
were
Gra
de C
or D
, 1 w
as
Grad
e E
NA
Bhato
e &
Sing
h, 20
03
4 (a
ll low
ve
l)
186
123
115
717
10/17
(59)
nono
CSC
I pt im
prov
ed; a
ll ISC
I pts
impr
oved
deco
mpre
ssive
op
is of
bene
fit in
pts
w/ in
comp
lete o
r ca
uda e
quina
injur
yHa
mmou
d et
al., 1
995
NANA
2437
347
1723
38/6
4 (59
)ye
sim
prov
ed: C
SCI+
op 0%
; CSC
I w/
o op 3
.7%; IS
CI+o
p 100
%;
ISCI
w/o
op 8
0%
deco
mpre
ssive
op is
of
no be
nefit
Pars
ons e
t al.
, 199
32
22
NAno
CSCI
pts d
id no
t impr
ove
NA
total
333
378
180
317
277
830
630
038
231
350/
775 (
45)
* CS
CI =
comp
lete S
CI; E
xpl =
explo
sion;
ISCI
= in
comp
lete S
CI; p
t = pa
tient;
vel =
veloc
ity.
† Th
e stu
dy w
as c
onsid
ered
to h
ave
suffic
ient d
ata
if th
e pa
per h
ad n
euro
logica
l outc
ome
data
for p
atien
ts wh
o un
derw
ent a
dec
ompr
essiv
e lam
inecto
my a
nd th
ose
that
were
trea
ted n
onop
era-
tively
.
Neurosurg Focus / Volume 28 / May 2010
Can surgery improve neurological function in PSIs?
5
miral Lord Horatio Nelson. A French sharpshooter felled him during the epic naval battle of Trafalgar.14 He was hit in the left shoulder, experienced immediate paraplegia, and died of his injury shortly thereafter. Other notable fatalities from spinal GSWs in history include the 20th President of the US James A. Garfield47 and the assas-sin of the 16th President of the US (Abraham Lincoln), John Wilkes Booth.39 Throughout the military conflicts of the 19th century such as the American Civil War and the Crimean, Boer, and Balkan Wars, PSIs were relatively rare, but came with a very high mortality rate, typically greater than 50%, which discouraged many from per-forming any surgical intervention.14
This reluctance to render treatment to these patients based on their grim prognosis continued into the Great War (World War I, 1914–1918). For example, during the brief but bloody American involvement, 0.4% of the in-jured had compound spinal injuries with a mortality rate of 56%.14 After the war, the British Medical Research Council, in a review of World War I spinal cord injuries, concluded that the only indication for a laminectomy was an incomplete lesion with progressive neurological loss, which admittedly was quite a rare scenario.42 At the onset of World War II (1939–1945), surgeons were faced with another onslaught of PSIs with little treatment to offer as a result of the continuation of the fatalistic attitude born through the previous conflicts. As stated by Dr. Milton Tinsley, “This was the confusion existing when we began
to care for compound spinal injuries in World War II.”42
Before becoming one of the founding fathers of pediatric neurosurgery, then Major Donald Matson28 summarized the feelings of many surgeons: “This has always been a difficult and discouraging group of cases to treat and per-haps for this reason they have been neglected.”
During the early American land campaigns of World War II such as Africa and Sicily, surgeons initially man-aged PSI using the same pessimistic philosophy of World War I. However, this was becoming increasingly unac-ceptable to surgeons. As stated by Dr. Walter Haynes,15
consultant neurosurgeon for the American First Army, “No one of us was ever satisfied with the defeatist attitude prevalent as to the prognosis of cord wounds. Yet, in light of previous experience of such men as Cushing, and the results of surgery in hardly comparable closed cord inju-ries, it seemed foolhardy to laminectomize more of those patients.”
As World War II progressed, the pendulum of opinion swung sharply in favor of aggressive surgical de bride ment, decompression of the spinal canal, and often intradural ex-ploration through a laminectomy in virtually all patients with compound spinal wounds, even those with complete neurological injuries.15,28,29,37,42 Previously unheard of results were being reported. In Pool’s series32 of 57 pa-tients treated during the years 1943–1944, 35 underwent a laminectomy and 57% showed a marked neurological improvement, compared with 4.5% spontaneous improve-
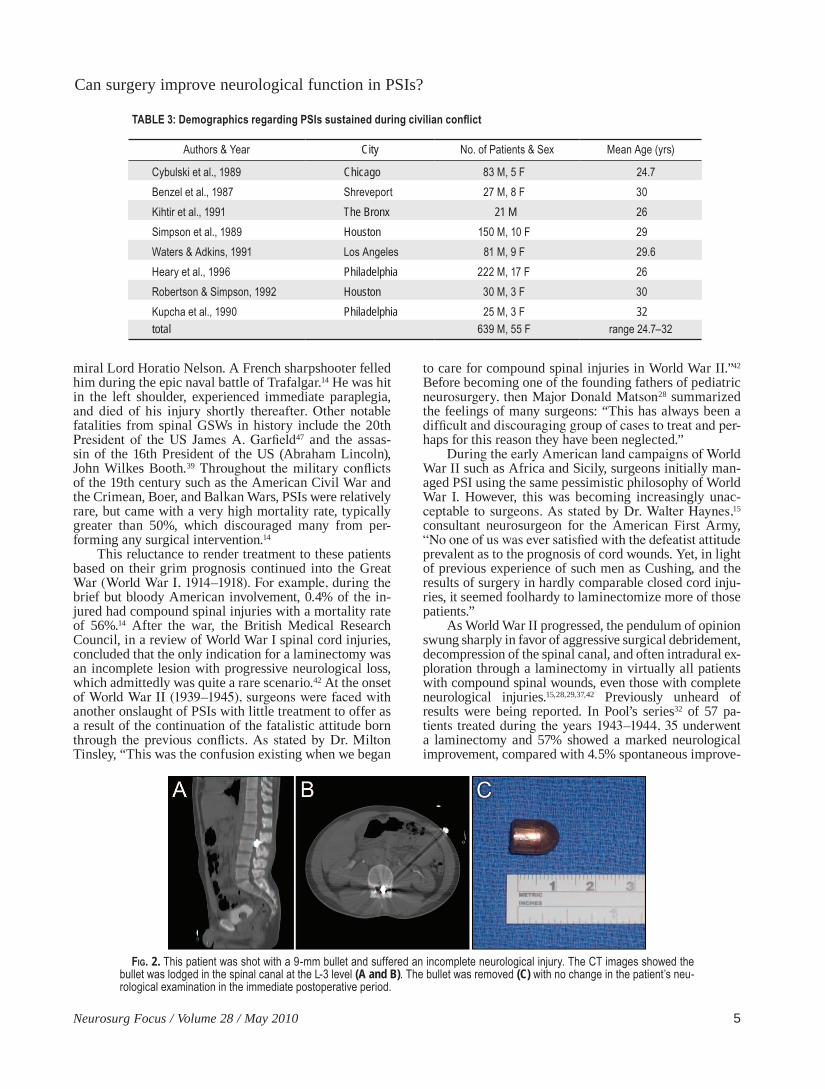
Fig. 2. This patient was shot with a 9-mm bullet and suffered an incomplete neurological injury. The CT images showed the bullet was lodged in the spinal canal at the L-3 level (A and B). The bullet was removed (C) with no change in the patient’s neu-rological examination in the immediate postoperative period.
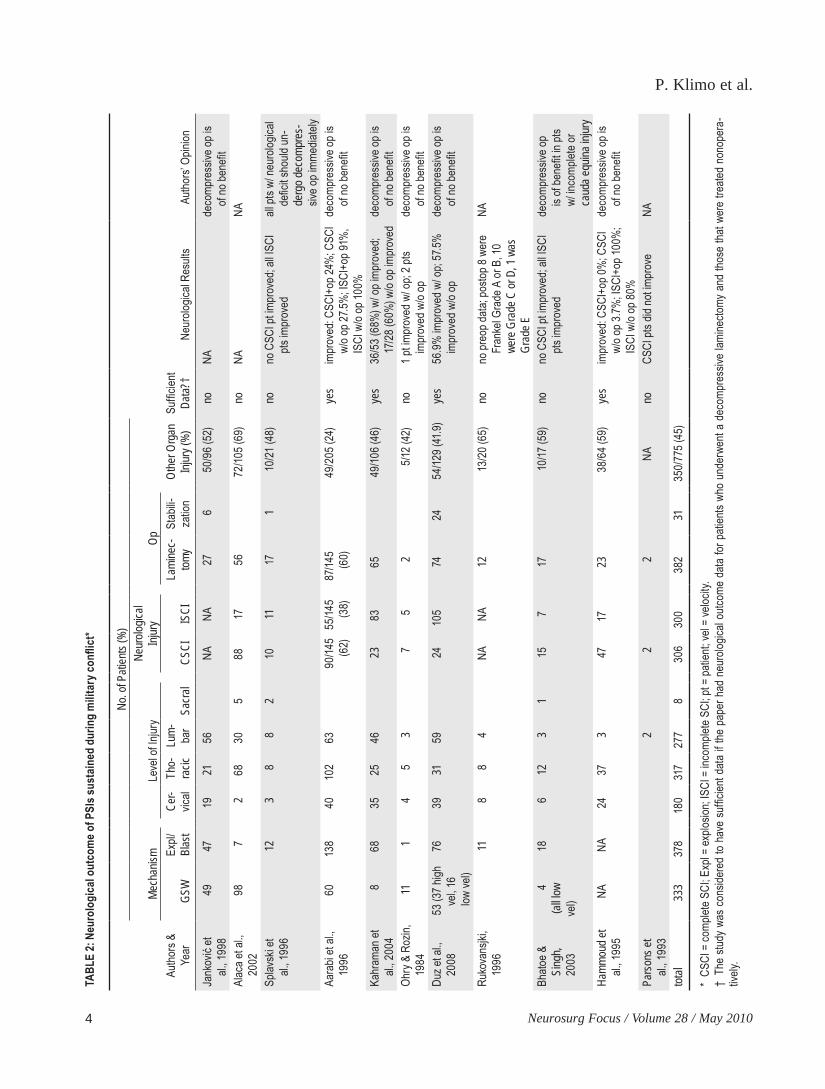
TABLE 3: Demographics regarding PSIs sustained during civilian conflict
Authors & Year City No. of Patients & Sex Mean Age (yrs)
Cybulski et al., 1989 Chicago 83 M, 5 F 24.7Benzel et al., 1987 Shreveport 27 M, 8 F 30Kihtir et al., 1991 The Bronx 21 M 26Simpson et al., 1989 Houston 150 M, 10 F 29Waters & Adkins, 1991 Los Angeles 81 M, 9 F 29.6Heary et al., 1996 Philadelphia 222 M, 17 F 26Robertson & Simpson, 1992 Houston 30 M, 3 F 30Kupcha et al., 1990 Philadelphia 25 M, 3 F 32total 639 M, 55 F range 24.7–32
TABL
E 2:
Neu
rolo
gica
l out
com
e of P
SIs s
usta
ined
dur
ing
mili
tary
confl
ict*
No. o
f Pati
ents
(%)
Mec
hanis
mLe
vel o
f Injur
y Ne
urolo
gical
Injur
y Op
Auth
ors &
Ye
arGS
WEx
pl/Bl
ast
Cer-
vical
Tho-
racic
Lum
-ba
rSa
cral
CSCI
ISCI
Lami
nec-
tomy
Stab
ili-za
tion
Othe
r Org
an
Injur
y (%)
Suffic
ient
Data?
†Ne
urolo
gical
Resu
ltsAu
thor
s’ Op
inion
Jank
ović
et al.
, 199
849
4719
2156
NANA
276
50/9
6 (52
)no
NAde
comp
ress
ive op
is
of no
bene
fitAl
aca e
t al.,
2002
987
268
305
8817
5672
/105 (
69)
noNA
NA
Splav
ski e
t al.
, 199
612
38
82
1011
171
10/21
(48)
nono
CSC
I pt im
prov
ed; a
ll ISC
I pts
impr
oved
all pt
s w/ n
euro
logica
l de
ficit s
hould
un-
derg
o dec
ompr
es-
sive o
p imm
ediat
elyAa
rabi
et al.
, 19
9660
138
4010
263
90/14
5
(62)
55/14
5
(38)
87/14
5
(60)
49/2
05 (2
4)ye
sim
prov
ed: C
SCI+
op 24
%; C
SCI
w/o o
p 27.5
%; IS
CI+o
p 91%
, IS
CI w
/o op
100%
deco
mpre
ssive
op is
of
no be
nefit
Kahr
aman
et
al., 2
004
868
3525
4623
8365
49/10
6 (46
)ye
s36
/53 (
68%)
w/ o
p imp
rove
d; 17
/28 (
60%)
w/o
op im
prov
edde
comp
ress
ive op
is
of no
bene
fitOh
ry &
Roz
in,
1984
11
14
53
75
25/1
2 (42
)no
1 pt im
prov
ed w
/ op;
2 pts
impr
oved
w/o
opde
comp
ress
ive op
is
of no
bene
fitDu
z et a
l., 20
08
53 (3
7 high
ve
l, 16
low ve
l)
7639
3159
2410
574
2454
/129 (
41.9)
yes
56.9
% im
prov
ed w
/ op;
57.5%
im
prov
ed w
/o op
deco
mpre
ssive
op is
of
no be
nefit
Ruko
vans
jki,
1996
118
84
NANA
1213
/20 (
65)
nono
preo
p dat
a; po
stop 8
wer
e Fr
anke
l Gra
de A
or B
, 10
were
Gra
de C
or D
, 1 w
as
Grad
e E
NA
Bhato
e &
Sing
h, 20
03
4 (a
ll low
ve
l)
186
123
115
717
10/17
(59)
nono
CSC
I pt im
prov
ed; a
ll ISC
I pts
impr
oved
deco
mpre
ssive
op
is of
bene
fit in
pts
w/ in
comp
lete o
r ca
uda e
quina
injur
yHa
mmou
d et
al., 1
995
NANA
2437
347
1723
38/6
4 (59
)ye
sim
prov
ed: C
SCI+
op 0%
; CSC
I w/
o op 3
.7%; IS
CI+o
p 100
%;
ISCI
w/o
op 8
0%
deco
mpre
ssive
op is
of
no be
nefit
Pars
ons e
t al.
, 199
32
22
NAno
CSCI
pts d
id no
t impr
ove
NA
total
333
378
180
317
277
830
630
038
231
350/
775 (
45)
* CS
CI =
comp
lete S
CI; E
xpl =
explo
sion;
ISCI
= in
comp
lete S
CI; p
t = pa
tient;
vel =
veloc
ity.
† Th
e stu
dy w
as c
onsid
ered
to h
ave
suffic
ient d
ata
if th
e pa
per h
ad n
euro
logica
l outc
ome
data
for p
atien
ts wh
o un
derw
ent a
dec
ompr
essiv
e lam
inecto
my a
nd th
ose
that
were
trea
ted n
onop
era-
tively
.
P. Klimo et al.
6 Neurosurg Focus / Volume 28 / May 2010
TABL
E 4:
Neu
rolo
gica
l out
com
es af
ter P
SIs s
usta
ined
dur
ing
civili
an co
nflic
t*
No. o
f Pati
ents
(%)
Leve
l of In
jury
Neur
ologic
al Inj
ury
Op
Auth
ors &
Yea
rM
echa
nism
Cerv
i-ca
lTh
o-ra
cicLu
mbo-
sacr
alCS
CIIS
CILa
mi-
n ecto
mySt
abili-
zatio
nOt
her O
rgan
Inj
ury
Mea
n FU
Suffic
ient
Data?
Neur
ologic
al Re
sults
Auth
ors’
Opini
on
Cybu
lski e
t al.,
1989
hand
gun
00
8829
5988
NANA
no47
.5% im
prov
ed w
/ op
done
w/in
72 hr
s; 48
.1%
impr
oved
w/ o
p don
e afte
r 72
hrs
deco
mpre
ssive
op is
of
bene
fit in
caud
a equ
ina
wheth
er do
ne ea
rly or
late
Benz
el et
al.,
1987
33 ha
nd-
gun,
2 rifl
e
821
620
1513
NANA
yes
impr
oved
: CSC
I+op
100%
; CS
CI w
/o op
0%; IS
CI+o
p 10
0%, IS
CI w
/o op
75%
deco
mpre
ssive
op is
of be
n-efi
t in in
comp
lete i
njurie
s w/
evide
nce o
f com
pres
-sio
nKi
htir e
t al.,
1991
all G
SWs
07
1411
100
218
/21 (8
6)3 m
osno
no pt
sho
wed n
euro
logica
l im
prov
emen
tde
comp
ress
ive op
is of
no
bene
fitSi
mpso
n et a
l., 19
8914
2 GSW
s, 18
SW
s43
8730
9448
3110
7/160
(67)
NAye
sim
prov
ed: C
SCI+
op 13
%;
CSCI
w/o
op 15
%;
ISCI
+op 4
0%, IS
CI w
/o op
58%
deco
mpre
ssive
op is
of no
be
nefit
Wate
rs &
Adk
ins,
1991
all G
SWs
1949
2254
3632
NANA
yes
remo
val o
f bull
et im
prov
ed
motor
func
tion o
nly fo
r co
mplet
e & in
comp
lete
T12–
L4 in
juries
remo
val o
f bull
et is
bene
ficial
on
ly in
T12–
L4 re
gion
Hear
y et a
l., 19
96
219 G
SWs,
20 S
Ws
019
643
144
5244
716
9/21
9 (77
)NA
yes
impr
oved
: CSC
I+op
0%;
CSCI
w/o
op 0%
; ISCI
+op
5%, IS
CI w
/o op
21%
deco
mpre
ssive
op is
of no
be
nefit
Robe
rtson
&
Simp
son,
1992
30 G
SWs,
3 SW
s0
033
429
1821
/33 (
64)
22 w
ksye
sim
prov
ed: C
SCI+
op 10
0%;
CSCI
w/o
op 0%
; ISCI
+op
47%
, ISCI
w/o
op 71
%
deco
mpre
ssive
op is
of no
be
nefit
Kupc
ha et
al.,
1990
hand
gun
280
021
75
10/2
8 (36
)46
mos
yes
impr
oved
CSC
I+op
67%
; CS
CI w
/o op
50%
; IS
CI+o
p 50%
, ISCI
w/o
op 6
0%
deco
mpre
ssive
op is
of no
be
nefit
total
653 G
SWs,
41 S
Ws
9836
023
637
725
623
19
356/4
61 (7
7)
* FU
= fo
llow-
up; S
W =
stab
wou
nd.
Neurosurg Focus / Volume 28 / May 2010
Can surgery improve neurological function in PSIs?
7
ment in the nonoperative group. His mortality rate was 7%. Haynes reported a 39.4% neurological improvement in laminectomized patients compared with virtually zero in nonoperated patients with a mortality rate of 9.8%.15 He strongly believed that all patients with incomplete cord injuries and static or progressive neurological deficits should undergo exploration and decompression, and also that those with a complete physiological lesion should be treated if there was any suspicion that the spinal cord was intact.
This aggressive and early surgical management car-ried over into the Korean and Vietnam conflicts. Of the 300 patients with spinal injuries treated at the Tokyo Army Hospital between September 1950 and May 1952, 254 were penetrating and only 46 were closed.44 It was believed that unless other associated injuries required life-saving surgery, laminectomy was to be performed as soon as possible. Thus, 249 of the 254 open spinal injured patients underwent a laminectomy, 44 of them within 24 hours of injury, with only 3 deaths (1.2%). Neurological improvement or complete recovery was seen in 121 pa-tients (48%), although 130 (51%) did not have improve-ment. Amazingly, neurological improvement in those with complete injuries was best observed in the group with cervical cord injuries. Between 1965 and 1966 at the Neu-rosurgical Treatment Center in Saigon, Jacobs and Berg18
operated on all 32 patients with penetrating wounds, but had dismal short-term outcomes—none of the patients with complete injuries improved and only 2 patients with incomplete injuries showed any improvement prior to evacuation. In the series by Jacobson and Bors,19 all but one of their 90 patients with an open spinal injury from the Vietnam conflict had a laminectomy. However, during this time, reports from civilian trauma centers were rais-ing questions about the effectiveness of indiscriminate use of laminectomy for patients with a PSI.
Between 1966 and 1973, Stauffer et al.41 treated 185 pa-tients with GSWs of the spine from low-velocity missiles, 106 with complete lesions and 79 with incomplete lesions. None of the patients with complete lesions showed any im-provement regardless of whether they underwent a lamine-ctomy. Of the patients with incomplete lesions, 71% showed measureable neurological improvement after a laminecto-my compared with 76.5% who did not have surgery. Yashon et al.48 also found similar equivocal results between surgery
and nonoperative care and concluded the following: 1) the final neurological outcome was most closely related with the initial neurological status rather than with surgery; and 2) surgery should only be performed in grossly contami-nated wounds or in patients with progressive neurological decline. Surgery also appeared to be ineffective in the series of patients with cervical GSWs presented by Heiden et al.,17
in contrast to the Korean War experience described previ-ously. They too believed that the sole indication for surgery was progressive neurological deficit. Chronologically, this leads into our literature review.Current Literature
The purpose of this review was to evaluate the evi-dence for or against decompressive laminectomy use to treat PSIs since the Vietnam War. We started by review-ing the military medical literature and found that there were a number of issues with the quality of the data and the conclusions put forth by the authors as stated in Re-sults. Although a large number of total patients (782) have been reported from these studies, only 4 papers had a reasonable amount of operative and nonoperative data within their studies to make a legitimate statement about the efficacy of surgery. Only 2 papers asserted that sur-gery was beneficial, and neither one of these had data to support this conclusion. Despite having a bias toward surgery (17 of 21 patients had a decompressive laminec-tomy and did not report the outcomes on those who did not have surgery), Splavski et al.40 made the inappropri-ate conclusion that all patients with PSIs and a neurologi-cal deficit be treated with immediate surgery. The same flaws (bias toward surgery and lack of nonoperative data) marred the paper by Bhatoe and Singh6 in which they similarly concluded that surgery was beneficial. One paper correctly stated in their abstract the lack of ben-efit for surgery based on their observed data, but then contradictorily concluded that patients with incomplete or cauda equina injury have a better prognosis for func-tional recovery when surgery is performed.22 The highest quality papers in the military medical literature were by Aarabi et al.1 and Hammoud et al.13 In both papers, there were sufficient numbers of nonoperative and operative patients and within each, complete and incomplete neu-rological deficits, for data analysis. In both, surgery was not found to improve neurological functional recovery.
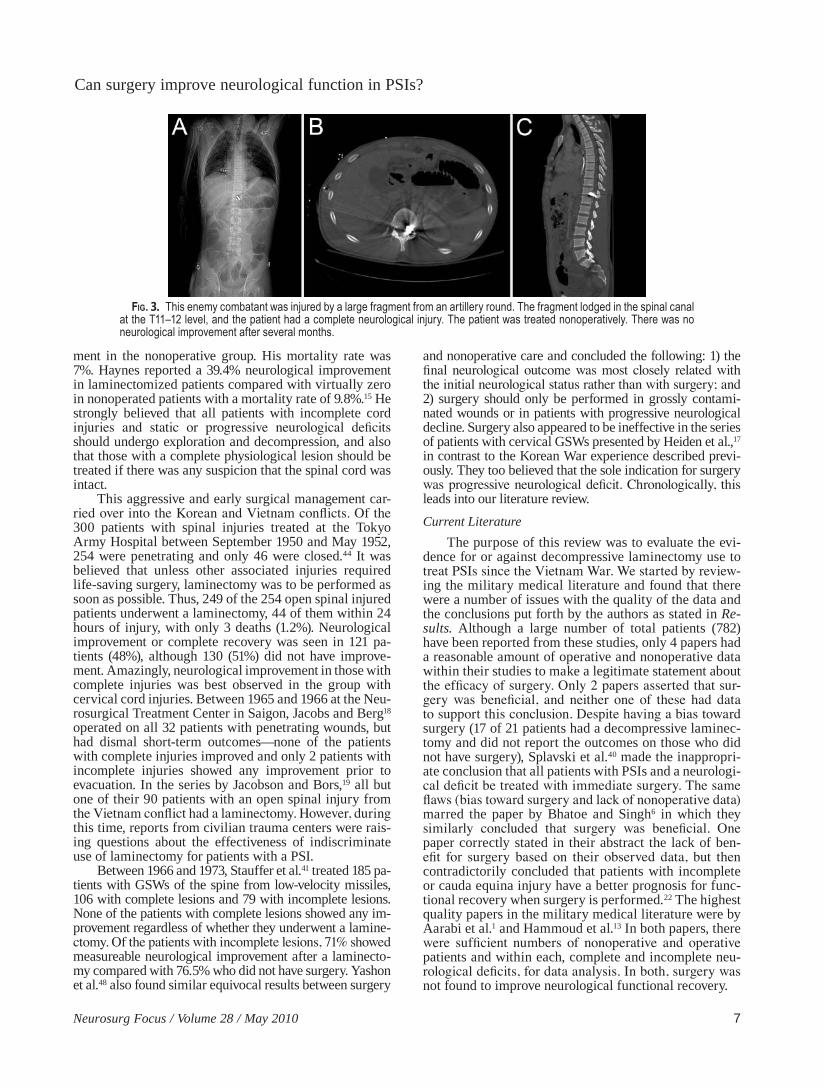
Fig. 3. This enemy combatant was injured by a large fragment from an artillery round. The fragment lodged in the spinal canal at the T11–12 level, and the patient had a complete neurological injury. The patient was treated nonoperatively. There was no neurological improvement after several months.
P. Klimo et al.
8 Neurosurg Focus / Volume 28 / May 2010
Given the aforementioned methodological deficien-cies in existing military medical literature, we performed a similar search in the civilian medical literature. Here, the quality of the literature was superior. Eight papers were identified, and of these 3 advocated a role for sur-gery. Cybulski et al.9 only evaluated patients with inju-ries of the cauda equina and concluded that surgery was of benefit whether done early (< 72 hours) or late (> 72 hours), but there were no control data (nonoperative) to support their conclusion. Benzel et al.5 concluded that surgery was indicated in those patients with incomplete injury and evidence of continued compression of neuro-logical structures within the spinal canal. In a multicenter study, Waters and Adkins45 found that bullet removal ben-efited those with complete or incomplete lesions between T-12 and L-4 (Fig. 2), but there was no effect in those between T-1 and T-11. Four papers in which there was complete preoperative, postoperative, and nonoperative data, containing patients with both complete and incom-plete neurological injury, strongly concluded that surgery was of no benefit.16,25,35,38
Our Recommendations for Deployed Military Neurosurgeons
A deployed military neurosurgeon works in an envi-ronment devoid of many administrative responsibilities,
family support responsibilities, and other issues that com-prise life. Thus, they are able to focus all of their energy on providing the best care for the casualties of war even though it may be in less than an ideal clinical setting. Repetitively facing injured soldiers and civilians with a clinical problem not often encountered in civilian prac-tice and with limited guidance is extremely unsettling. As described by World War II surgeons in the preced-ing section, the motivation to act and provide maximal intervention, regardless of whether such intervention is known to provide actual benefit, is strong. Such has been the dilemma with patients with PSI, for whom recom-mendations have not appreciably changed in more than 100 years of military conflicts.
The literature thus far for PSI has provided some an-swers to other questions.7,8,16,20,24 It is quite clear that the strongest prognostic predictor of future neurological func-tion is the initial neurological grade. There is no need to perform exploratory surgery or bullet or fragment removal as a means to reduce infection beyond local wound care unless there is gross contamination of the wound.13,43,46 A minimum of 3 days but more typically a 7–14-day course of broad-spectrum intravenous antibiotics with coverage of gram-positive, gram-negative, and anaerobic bacterial flora is effective at preventing most infections, including those in patients with transcolonic wounds.7,27,33 There is no need to operate to remove bullet fragments to prevent lead or copper toxicity as this is an extremely rare com-plication even in the new era of IEDs. There is also no role for the administration of trauma-dose Solu-Medrol in these patients.26 The only absolute indications for surgery are to repair a CSF-cutaneous/pleural fistula or if the pa-tient has progressive neurological decline correlated with compression of neural elements on imaging studies.
The question that has always been of greatest impor-tance is whether decompressive laminectomy can provide the patient a better chance at regaining neurological func-tion compared with nonoperative supportive measures. The gravity of this question is obvious when considering that the vast majority of patients who sustain PSIs in the military are young, healthy, physically active individuals, many of whom have spouses and children eagerly awaiting their return home from deployment. Does surgery work? The literature reviewed here is inconclusive, but the data reported to date suggest it does not, especially in those with complete lesions. Most of the military and civilian literature does not support surgery. Furthermore, the find-ings in the civilian literature are particularly important when one considers that the differences between civilian and military injuries make the argument for nonopera-tive treatment even stronger. Civilian injuries are almost universally caused by low-velocity projectiles that impart only a fraction of the energy to the tissue on impact in comparison with what is found in high-velocity injuries. The associated organ injuries are less severe and the wounds are less contaminated. Civilian patients can often be transported to a trauma center and can rapidly start re-ceiving advanced care. Despite significant advancement in battlefield resuscitation and transport, the process of getting a wounded warrior to a Level III Air Force The-ater Hospital, which may have neurosurgical assets, can
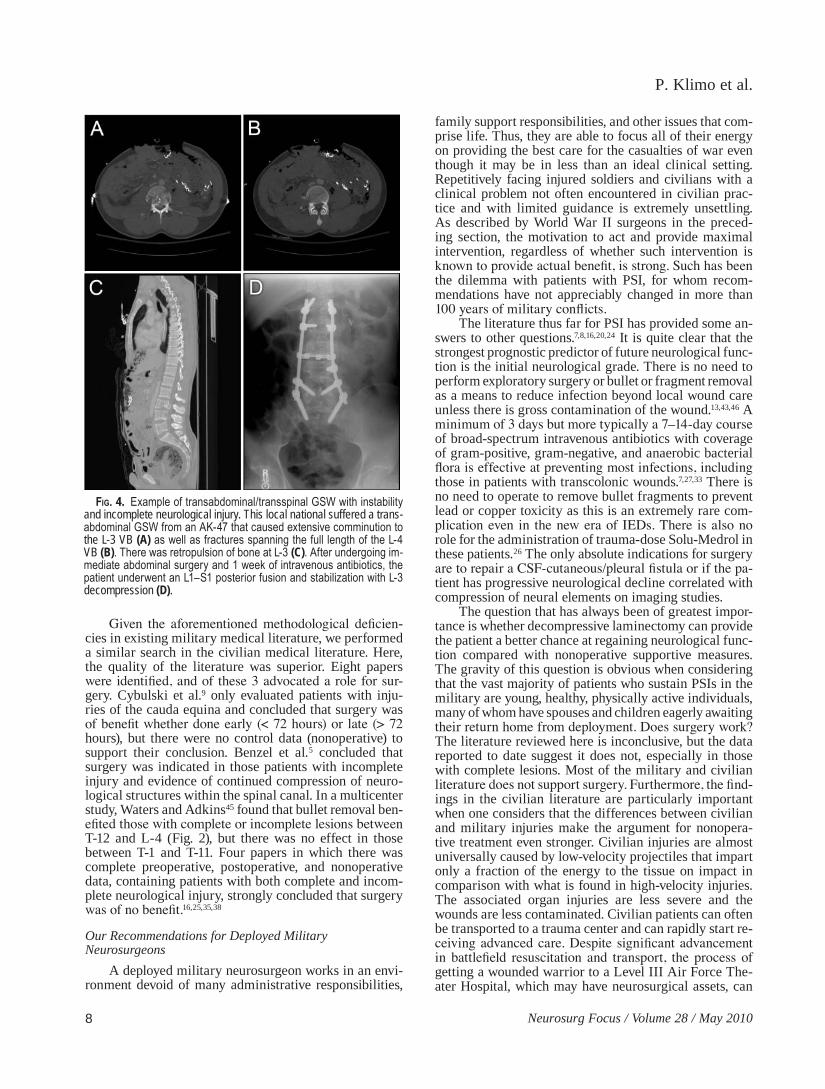
Fig. 4. Example of transabdominal/transspinal GSW with instability and incomplete neurological injury. This local national suffered a trans-abdominal GSW from an AK-47 that caused extensive comminution to the L-3 VB (A) as well as fractures spanning the full length of the L-4 VB (B). There was retropulsion of bone at L-3 (C). After undergoing im-mediate abdominal surgery and 1 week of intravenous antibiotics, the patient underwent an L1–S1 posterior fusion and stabilization with L-3 decompression (D).

Neurosurg Focus / Volume 28 / May 2010
Can surgery improve neurological function in PSIs?
9
be lengthy. If there is merit to the argument that early de-compression leads to better outcomes, patients extracted from a battlefield may be at a disadvantage.
However, we believe that decompressive laminectomy may be indicated for patients with penetrating SCI beyond those patients requiring repair of a CSF fistula or expe-riencing progressive neurological decline. We stress that these recommendations are the collective opinions of the authors and in no way should be interpreted as treatment standards or guidelines; each neurosurgeon or spine sur-geon must make their own clinical decision based on their opinion of the literature, their abilities, resources available at their deployment location, and each individual patient scenario:
1. Laminectomy is to be considered only if the patient is stabilized from other life-threatening injuries, most notably abdominal, thoracic, or intracranial injury.
2. Laminectomy should not be performed in patients with complete neurological injury (Fig. 3), with the possible excep-tion of patients with a cervical injury who demonstrate clear compressive pathology on imaging and arrive early after sus-taining their injury. Here, the recovery of even one spinal seg-ment is highly significant in their rehabilitive function.
3. Laminectomy should be considered in all patients with an incomplete neurological deficit (especially if the lesion is in the cauda equina) and there is evidence on imaging of signifi-cant spinal canal compromise (for example, bone or metal). Surgery should be performed as soon as possible, ideally within 24–48 hours. Segmental instrumentation and fusion should be considered at the same time if the injury is deemed unstable.
We offer these recommendations for several reasons. The available medical literature as we have detailed is far from conclusive. All the components to provide timely surgical intervention in-theater are currently in place: a well-integrated, rapid, military medical evacuation sys-tem, in-theater neurosurgeons, and medical facilities that are able to provide all aspects of perioperative care. There has been a significant change in the paradigm for delivery of neurosurgical care for the wounded military service member over the past 2 decades. Since the first Gulf War, neurosurgeons are now deployed directly in the combat theater, often quickly accessible via helicopter evacuation with times comparable to those seen at major civilian trauma centers. This previously unseen access to neuro-surgical evaluation and treatment should be considered when establishing a treatment algorithm in current and future military conflicts. Additionally, many military spinal cord and cauda equina injuries are the result of IEDs, which are low velocity shrapnel wounds similar to injuries sustained in civilian GSW injuries. Direct in-jury from a high-velocity military firearm, such as from a sniper attack, is fortunately less frequent than low-veloc-ity shrapnel wounds. Another point we believed was an important consideration was the transportation of these patients out of the operational theater to other medical facilities, typically in Europe and North America. These are long (commonly 8 or more hours) transcontinental and transoceanic flights aboard military aircraft, which may encounter significant turbulence with additional risk for further neurological injury. A similar rationale is used to support the use of decompressive craniectomy
in patients with severe head injury.4 There are several ad-ditional issues with these recommendations that require further discussion and clarification.
Perioperative ComplicationsA number of authors have cited an increased rate of
complications in patients who undergo surgery and use this finding to strengthen their argument against perform-ing surgery.1,7,16,35,38 This finding, however, has not been supported by others.12 Complications that have been re-ported include CSF leak, postoperative instability, neuro-logical decline, epidural hematoma, meningitis, and local infection. If such a difference truly exists, it would not be surprising and in fact expected, but we believe that these complications are manageable and should not dis-suade the surgeon from rendering potentially beneficial treatment.
Transgastrointestinal InjuriesProjectiles that pass through the abdomen and in
particular the colon before striking the spinal column are particularly ominous injuries. These patients typically require a life-saving laparotomy as the initial treatment. These patients are often too critically ill or have other issues such as an open abdominal wound that precludes them from being placed prone for several hours to per-form a laminectomy. Furthermore, several authors have found that the risk of developing a postoperative spinal wound infection is significantly higher in those patients with transcolonic injuries.16,33 Therefore, whether to per-form a laminectomy in patients with transgastrointestinal injuries needs a careful analysis of all issues, neurologi-cal and nonneurological. We believe that if the patient has an incomplete injury with continued canal compro-mise from bone or foreign objects, and it is thought the patient could tolerate a laminectomy, and the patient has been placed on appropriate broad-spectrum intravenous antibiotics, then a laminectomy should be performed as soon as possible. We believe that the potential of achiev-ing neurological recovery outweighs the risk of devel-oping an infection that should be readily treatable with appropriate antibiotics.
If it is thought that the patient has an unstable spine (see Instability), then the decompression and instrumenta-tion should be delayed until the patient has completed a full course of antibiotics (Fig. 4). Alternatively, the decompres-sion may be performed initially and the instability treated with segmental instrumentation in a delayed fashion or with prolonged immobility and bracing. In this circum-stance, stabilization for coalition personnel would most likely occur at a medical facility out of theater because nonnative patients would most likely have been transferred before completion of their course of antibiotics.
InstabilityAs seen in this literature review, few patients in either
the military or the civilian articles required stabilization. In general, low-velocity injuries typically seen in civil-ian casualties rarely create an unstable spine.3 However, high-velocity injuries, which are more common in mili-

P. Klimo et al.
10 Neurosurg Focus / Volume 28 / May 2010
tary patients, probably have a higher risk of instability because of the greater destructive capability of the pro-jectile. Some of the cases of instability in the literature were associated with overly aggressive laminectomy.41
The largest series of military patients with PSI requiring stabilization was recently published by Duz et al.12 Of 129 patients, 24 required stabilization, 17 of them for what the authors classified as a Type III or side-to-side injury in which the bullet passed through both facet joints and/or pedicles.
In the area of operation, spinal imaging is accom-plished with plain radiographs and CT scanning. Mag-netic resonance imaging is not available until the patient reaches medical centers in either Europe or North Amer-ica. In addition, MR imaging is often contraindicated in the wounded warrior due to retained fragments from the IEDs. Computed tomography with reconstructed images in the coronal and sagittal planes is adequate for deter-mining the integrity of the VB, spinal canal, facets, and overall alignment of the spine in the area of the injury. Severely comminuted anterior and posterior elements with evidence of segmental deformity can be indicative of instability. Furthermore, a laminectomy in the presence of an anterior or middle column injury may produce an unstable spine.
Instrumentation should be performed if deemed nec-essary as part of the decompression operation if possible. Although coalition soldiers do not typically have perma-nent orthopedic or spinal implants placed in-theater for fear of infection, the state of the major in-theater medical centers, for example the Craig Joint Theater Hospital in Bagram, Afghanistan, is such that all the intraoperative equipment and spinal instrumentation needed to perform a fusion and stabilization are available. The decision to perform an instrumented fusion must take into account the risks of a potentially increased infection rate, which can be highly variable depending on the maturity of the deployed facility versus the risks of neurological decline during a long and complicated transport in a turbulent environment. In the more than 2 years that Air Force neu-rosurgeons have been deployed to Afghanistan, a number of spinal stabilization surgeries have been performed and, to date, there have been no deep or superficial wound in-fections. However, we stress that the final determination on whether to pursue instrumentation must be made by the deployed on-site neurosurgeon or spine surgeon as he or she will have the most accurate assessment of all fac-tors that need to be taken into account when making such a decision.
ConclusionsThe treatment of patients with PSIs continues to be a
great challenge to all involved and may present considerable uncertainty for the in-theater neurosurgeon with regard to treatment. Despite the numerous conflicts of today and yes-terday, there is still ambiguity as to the role of decompres-sive laminectomy in regaining lost neurological function. It is clear that the most important factor that determines fu-ture neurological function is the initial neurological status. Surgery may or may not have a beneficial role. However, the medical literature, both civilian and military, is inad-
equate at answering this question. This underscores the great need for future studies that are currently underway. Based primarily on the lack of conclusive evidence, we be-lieve that there is a role for surgery when it is done with the hope of restoring neurological function. Despite more than 60 years of amazing advancement in medical treat-ment and technology, our recommendations are hauntingly similar to the opinions expressed by Dr. Matson28 in 1946 as a result of his experience in treating these injuries in the European Theater of Operations from 1944 to 1945:
Patients who exhibit a neurological picture consistent with an incomplete transection of the spinal cord where this picture has altered since the time of injury, especially where the neuro-logical deficit is increasing.…
Patients with a neurological picture of incomplete cord transection where x-rays reveal clear-cut encroachment on the spinal canal by a foreign body or reveal definite fracture of a lamina or pedicle with or without depressed bone fragments.…
Patients who have sizable wounds directly over or near the spinal column and are leaking spinal fluid profusely.…
Disclosure
The authors report no conflict of interest concerning the mate-rials or methods used in this study or the findings specified in this paper.
Author contributions to the study and manuscript preparation include the following. Conception and design: P Klimo, B Ragel, M Rosner, W Gluf, RR McCafferty. Acquisition of data: P Klimo, B Ragel, M Rosner, W Gluf, RR McCafferty. Analysis and interpreta-tion of data: P Klimo, B Ragel, M Rosner, W Gluf, RR McCafferty. Drafting the article: P Klimo, B Ragel, M Rosner, W Gluf, RR McCafferty. Critically revising the article: P Klimo, B Ragel, M Rosner, W Gluf. Reviewed final version of the manuscript and approved it for submission: P Klimo, B Ragel.
The opinions or assertions contained herein are the private views of the authors and are not to be construed as official or as reflecting the views of the United States Army, United States Navy, United States Air Force, or Department of Defense. The authors are employees of the United States government. This work was prepared as part of their official duties and as such, there is no copyright to be transferred.
Acknowledgment
The authors thank Shirley McCartney, Ph.D., for editorial assistance.
References
1. Aarabi B, Alibaii E, Taghipur M, Kamgarpur A: Compara-tive study of functional recovery for surgically explored and conservatively managed spinal cord missile injuries. Neuro-surgery 39:1133–1140, 1996
2. Alaca R, Yilmaz B, Goktepe AS, Yazicioglu K, Gunduz S: Military gunshot wound-induced spinal cord injuries. Mil Med 167:926–928, 2002
3. Aryan HE, Amar AP, Ozgur BM, Levy ML: Gunshot wounds to the spine in adolescents. Neurosurgery 57:748–752, 2005
4. Bell RS, Vo AH, Neal CJ, Tigno J, Roberts R, Mossop C, et al: Military traumatic brain and spinal column injury: a 5-year study of the impact blast and other military grade weaponry on the central nervous system. J Trauma 66 (4 Suppl):S104–S111, 2009
5. Benzel EC, Hadden TA, Coleman JE: Civilian gunshot wounds to the spinal cord and cauda equina. Neurosurgery 20:281–285, 1987
Neurosurg Focus / Volume 28 / May 2010
Can surgery improve neurological function in PSIs?
11
6. Bhatoe HS, Singh P: Missile injuries of the spine. Neurol In-dia 51:507–511, 2003
7. Bono CM, Heary RF: Gunshot wounds to the spine. Spine J 4:230–240, 2004
8. Buxton N: The military medical management of missile in-jury to the spine: a review of the literature and proposal of guidelines. J R Army Med Corps 147:168–172, 2001
9. Cybulski GR, Stone JL, Kant R: Outcome of laminectomy for civilian gunshot injuries of the terminal spinal cord and cauda equina: review of 88 cases. Neurosurgery 24:392–397, 1989
10. DeMuth WE Jr: Bullet velocity and design as determinants of wounding capability: an experimental study. J Trauma 6:222–232, 1966
11. DeMuth WE Jr: Bullet velocity as applied to military rifle wounding capacity. J Trauma 9:27–38, 1969
12. Duz B, Cansever T, Secer HI, Kahraman S, Daneyemez MK, Gonul E: Evaluation of spinal missile injuries with respect to bullet trajectory, surgical indications and timing of surgical intervention: a new guideline. Spine 33:E746–E753, 2008
13. Hammoud MA, Haddad FS, Moufarrij NA: Spinal cord mis-sile injuries during the Lebanese civil war. Surg Neurol 43:432–442, 1995
14. Hanigan WC, Sloffer C: Nelson’s wound: treatment of spinal cord injury in 19th and early 20th century military conflicts. Neurosurg Focus 16 (1):E4, 2004
15. Haynes WG: Acute war wounds of the spinal cord. Am J Surg 72:424–433, 1946
16. Heary RF, Vaccaro AR, Mesa JJ, Balderston RA: Thora-columbar infections in penetrating injuries to the spine. Or-thop Clin North Am 27:69–81, 1996
17. Heiden JS, Weiss MH, Rosenberg AW, Kurze T, Apuzzo ML: Penetrating gunshot wounds of the cervical spine in civilians. Review of 38 cases. J Neurosurg 42:575–579, 1975
18. Jacobs GB, Berg RA: The treatment of acute spinal cord inju-ries in a war zone. J Neurosurg 34:164–167, 1971
19. Jacobson SA, Bors E: Spinal cord injury in Vietnamese com-bat. Paraplegia 7:263–281, 1970
20. Jallo GI: Neurosurgical management of penetrating spinal in-jury. Surg Neurol 47:328–330, 1997
21. Janković S, Busić Z, Primorac D: Spine and spinal cord war injuries during the war in Croatia. Mil Med 163:847–849, 1998
22. Kahraman S, Gonul E, Kayali H, Sirin S, Duz B, Beduk A, et al: Retrospective analysis of spinal missile injuries. Neuro-surg Rev 27:42–45, 2004
23. Kihtir T, Ivatury RR, Simon R, Stahl WM: Management of transperitoneal gunshot wounds of the spine. J Trauma 31:1579–1583, 1991
24. Kitchel SH: Current treatment of gunshot wounds to the spine. Clin Orthop Relat Res (408):115–119, 2003
25. Kupcha PC, An HS, Cotler JM: Gunshot wounds to the cervi-cal spine. Spine 15:1058–1063, 1990
26. Levy ML, Gans W, Wijesinghe HS, SooHoo WE, Adkins RH, Stillerman CB: Use of methylprednisolone as an adjunct in the management of patients with penetrating spinal cord in-jury: outcome analysis. Neurosurgery 39:1141–1149, 1996
27. Lin SS, Vaccaro AR, Reisch S, Devine M, Cotler JM, Reich SM: Low-velocity gunshot wounds to the spine with an as-sociated transperitoneal injury. J Spinal Disord 8:136–144, 1995
28. Matson D: Treatment of compound spine injuries in forward army hospitals. J Neurosurg 3:114–119, 1946
29. McCravey A: War wounds of the spinal cord. A plea for ex-ploration of spinal cord and cauda equina injuries. JAMA 129:152–153, 1945
30. Ohry A, Rozin R: Acute spinal cord injuries in the Lebanon War, 1982. Isr J Med Sci 20:345–349, 1984
31. Parsons TW III, Lauerman WC, Ethier DB, Gormley W, Cain JE, Elias Z, et al: Spine injuries in combat troops—Panama, 1989. Mil Med 158:501–502, 1993
32. Pool JL: Gunshot wounds of the spine. Surg Gynecol Obstet 81:617–622, 1945
33. Quigley KJ, Place HM: The role of debridement and antibiot-ics in gunshot wounds to the spine. J Trauma 60:814–820, 2006
34. Ramasamy A, Harrisson SE, Clasper JC, Stewart MP: Inju-ries from roadside improvised explosive devices. J Trauma 65:910–914, 2008
35. Robertson DP, Simpson RK: Penetrating injuries restricted to the cauda equina: a retrospective review. Neurosurgery 31:265–270, 1992
36. Rukovansjki M: Spinal cord injuries caused by missile weap-ons in the Croatian war. J Trauma 40 (3 Suppl):S189–S192, 1996
37. Schneider RC, Webster JE, Lofstrom JE: A follow-up report of spinal cord injuries in a group of World War II patients. J Neurosurg 6:118–126, 1949
38. Simpson RK Jr, Venger BH, Narayan RK: Treatment of acute penetrating injuries of the spine: a retrospective analysis. J Trauma 29:42–46, 1989
39. Sloffer CA, Hanigan WC: A gunshot wound to the cervical spine: the case of the presidential assassin. J Am Coll Surg 204:168–174, 2007
40. Splavski B, Vranković D, Sarić G, Blagus G, Mursić B, Ruko-vanjski M: Early management of war missile spine and spinal cord injuries: experience with 21 cases. Injury 27:699–702, 1996
41. Stauffer ES, Wood RW, Kelly EG: Gunshot wounds of the spine: the effects of laminectomy. J Bone Joint Surg Am 61:389–392, 1979
42. Tinsley M: Compound injuries of the spinal cord. J Neuro-surg 3:306–309, 1946
43. Velmahos GC, Degiannis E, Hart K, Souter I, Saadia R: Changing profiles in spinal cord injuries and risk factors influencing recovery after penetrating injuries. J Trauma 38:334–337, 1995
44. Wannamaker GT: Spinal cord injuries; a review of the early treatment in 300 consecutive cases during the Korean Con-flict. J Neurosurg 11:517–524, 1954
45. Waters RL, Adkins RH: The effects of removal of bullet fragments retained in the spinal canal. A collaborative study by the National Spinal Cord Injury Model Systems. Spine 16:934–939, 1991
46. Waters RL, Sie IH: Spinal cord injuries from gunshot wounds to the spine. Clin Orthop Relat Res (408):120–125, 2003
47. Weiner BK: The case of James A. Garfield: a historical per-spective. Spine 28:E183–E186, 2003
48. Yashon D, Jane JA, White RJ: Prognosis and management of spinal cord and cauda equina bullet injuries in sixty-five civil-ians. J Neurosurg 32:163–170, 1970
Manuscript submitted January 21, 2010.Accepted February 16, 2010.Address correspondence to: Paul Klimo Jr., M.D., 88th Medical
Group, 4881 Sugar Maple Drive, Wright-Patterson Air Force Base, Ohio 45433. email: [email protected].