can user fee in cbrh model for fp/rh be practical and ensure
TRANSCRIPT

ODA’s Practical Field Experience
SOMALI
OROMIA
SNNP
AMHARAAFAR
TIGRAY
GAMBELLA
BENISHANGUL-GUMUZ
DIRE-DAW AADDIS ABABA
EthiopiaOromia
N
50 0 50100150200250 Kilometers
Adiministrative Regions of Ethiopia

ODA a membership local CSO (>500,000 members); working : health, education, agriculture & rural water supply)
Oromia Development Association (ODA) initiated and run ICBRH /FP Program for 9 years; starting in 2000
The David and Lucile Packard Foundation supported the project
BALE
GUJI
BORENA
ARSIJIMMA
EaAST HARERGE
ILUBABOR
WEST ARSI
WEST SHEWA
WES
T
HARE
RGE
EAST
SHEWA
EAST
WEL
LEG
AWEST WELLEGAKELEM WELLEGA
NORTH SHEWA
HORO GUDURU
S/WEST SHEWA
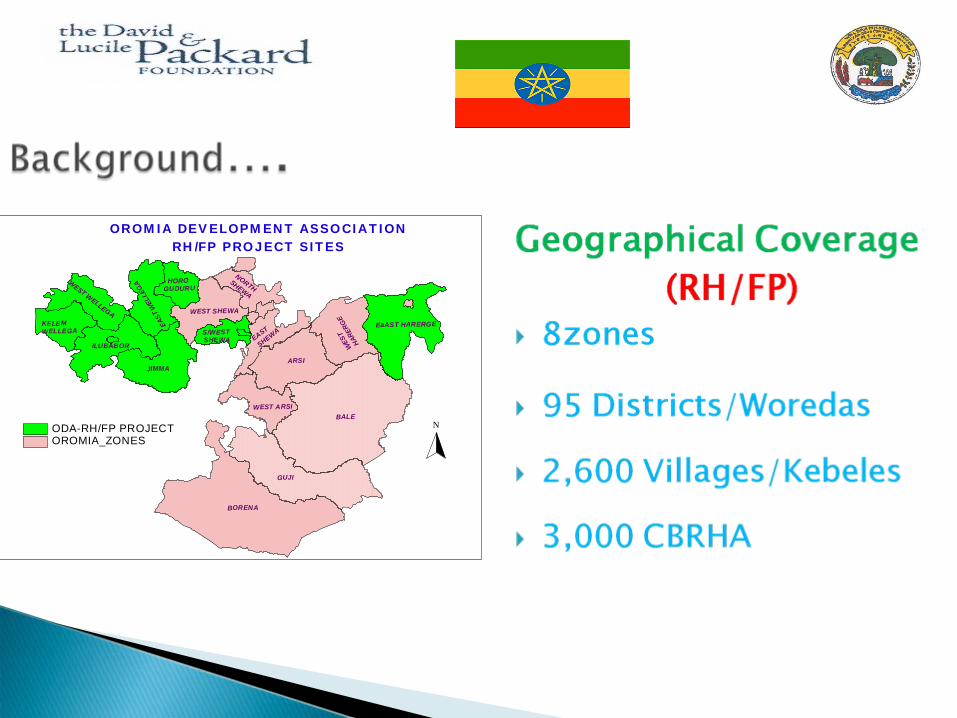
OROMIA_ZONESODA-RH/FP PROJECT N
OROMIA DEVELOPMENT ASSOCIATIONRH/FP PROJECT SITES
To ensure the availability and accessibility of range of contraceptive choices
To fill in the gaps whenever short acting contraceptives run out of stock (Public sector)
Main source of incentives for CBRHA; besides recognition, provision of uniforms and training
To enable CBRHA continue to serve communities; even when the project phases out

Compensation for CBRHA has enabled project managers:
to undertake rigorous supervision, to standardize schedules, to implement the project rapidly and to maintain service quality
To make the client a more responsible contraceptive userTo use as a revolving fund to procure contraceptives To become less reliant on donors (to ensure sustainability)

The communities were consulted on the amount of user fee
Cost sharing was based on what clients could pay or are already paying for services they are receiving
Ability to pay was determined based on: research findings, participatory rural appraisal (PRA),

For those who could not pay; ◦
Referral to the near by public health facilities
◦
If the health facility was far from CBRHA service delivery point and the clients were very poor, services were provided free of charge

The fee collection system was made simpleRegistry books instead of receipts Minimal additional work for CBRHA
The price set was communicated to communities through community support committees
Sixty percent was paid for CBRHA & 40% was deposited in block account
Internal financial controls/ auditing carried out
1.
MOH assessment of CBRH program (2002-2003),
◦
76% of clients knew and were willing to pay for the services provided by CBRHA, While it was:◦
81% for Oromia region &
◦
90% in areas where ODA-CBRH program was operating
2. ODA project sites Experience: Project sites were divided into two◦
In East Wollega, clients were asked to pay 50% less ◦
In West Wollega clients paid the amount agreed
Finding◦
The number of clients could not increase◦
Even the number of clients decreased over time
More than 98% of 900,000 Clients had been paying
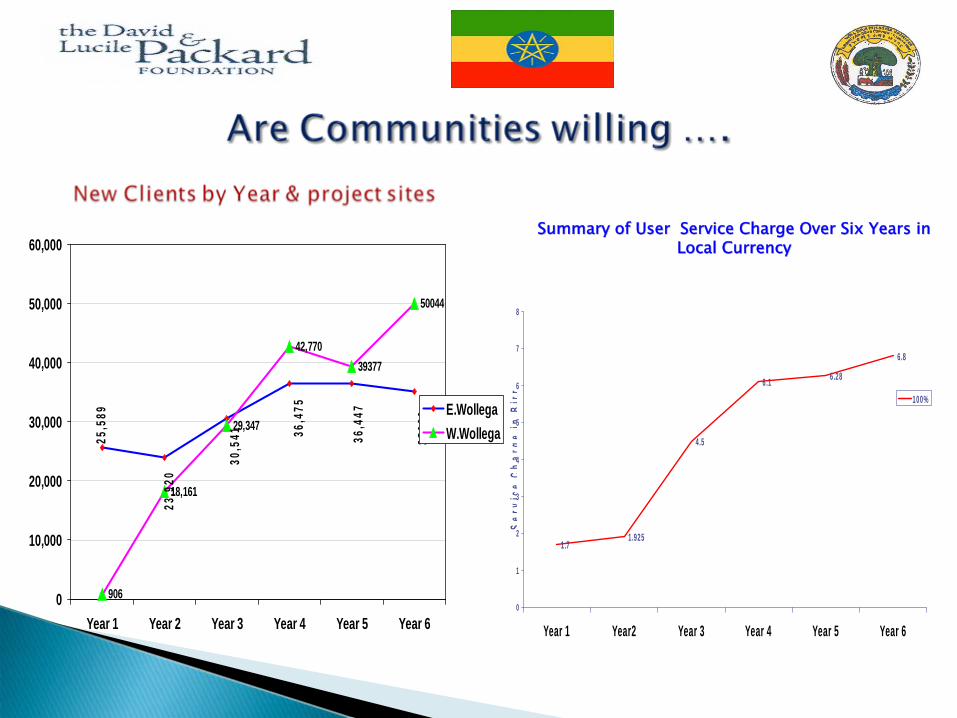
906
18,161
29,347
42,77039377
50044
36,4
47
36,4
75
30,5
41
23,9
20
25,5
89
3503
9
0
10,000
20,000
30,000
40,000
50,000
60,000
Year 1 Year 2 Year 3 Year 4 Year 5 Year 6
E.WollegaW.Wollega
1.71.925
4.5
6.1 6.28
6.8
0
1
2
3
4
5
6
7
8
Year 1 Year2 Year 3 Year 4 Year 5 Year 6
Ser
vice
Ch
arge
inB
irr
100%
Summary of User Service Charge Over Six Years in Summary of User Service Charge Over Six Years in Local CurrencyLocal Currency

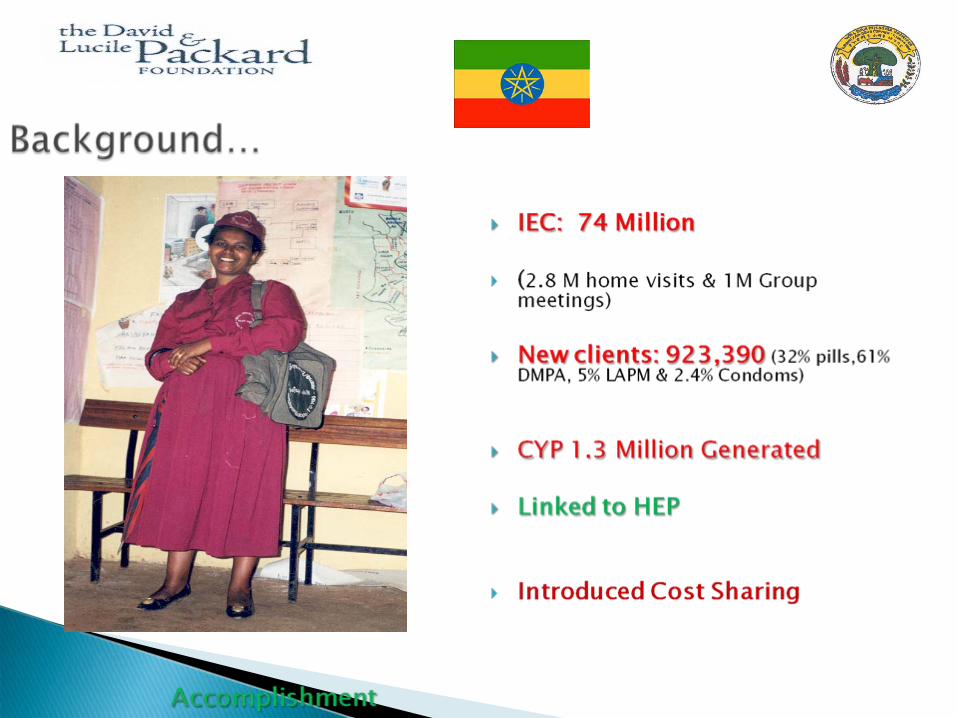
As a result of the service charge the project was able to motivate community health agents to allocate their spare time to render services for their community
The money collected was used as a revolving fund to procure contraceptives through social marketing to ensure continuity of service whenever the public facility runs out of stock
Up to now 23 CBRHA Associations have been established and making use of the money collected as revolving fund for income generating activities and has continued to serve their communities after the project has closed out.

In countries with low health service coverage CBRHA model has been proved as the most successful approach to mobilize communities and to increase contraceptive uptake
Clients who pay fee for service are more likely to value the services they receive and demand high quality services
Advocacy for service charge and enhancing voluntary CBRH model approaches should be encouraged as part of ensuring contraceptive security efforts
The Packard Foundation
CBRHA & Communities
ODA staff
Conference organizers

Thank you!