can we trust the xpert? - home page - fidssa...fakulteit geneeskunde en gesondheidswetenskappe •...
TRANSCRIPT

Fakulteit Geneeskunde en Gesondheidswetenskappe
•
Faculty of Medicine and Health Sciences
Can we trust the Xpert?
An evaluation of the Xpert MRSA/SA BC System and
an assessment of potential clinical impact
Dr Kessendri Reddy
Division of Medical Microbiology, NHLS Tygerberg

2
Background
▪ S. aureus is a common cause of bacteraemia
▪ Rapid differentiation has several benefits▪ Undirected antibiotic use, including vancomycin
▪ Appropriate antimicrobial treatment
▪ Source identification and control
▪ Infection control precautions
Positive blood cultures with Gram positive
cocci in clusters (GPCC) Coagulase-negativestaphylococcus
(CoNS)
Staphylococcus aureus
Methicillin-sensitive S. aureus (MSSA)
Methicillin-resistant S. aureus (MRSA)
The Test
▪ Xpert MRSA/SA BC System (Cepheid, Sunnyvale, CA) ▪ Real-time
▪ Semi-automated
▪ MRSA vs MSSA vs CoNS within ~1h▪ Traditional biochemical-based methods require overnight
incubation
3

The Test
4
spa mecA SCCmec-orfX
MRSA + + +
MSSA + - +/-
CoNS - +/- -
Interpretation

Research Question
▪ How does the Xpert MRSA/SA BC assay perform in a real-world setting?
▪ What is the potential impact of implementation of this test in Cape Town, South Africa?
5

Study Design
▪ Prospective, observational study
▪ Setting and population▪ BacT/Alert 3D Microbial Identification System (bioMérieux, Marcy
L’Étoile, France)
▪ January – June 2016: adults from January – March, then inclusive of paediatric patients
▪ Blood cultures submitted at clinician’s discretion
▪ Ethics▪ Waiver of informed consent
▪ SU Health Research Ethics Committee, reference S14/10/201
6

7
Study Design
▪ Performance▪ Aerobic, anaerobic and paediatric blood culture bottles with
monomorphic GPCC on Gram stain
▪ Operator blinded to culture result
▪ Potential impact▪ Clinician-based interviews
▪ Xpert result not conveyed

Methods: Performance
8
BC positive with GPCC
Traditional:
MSA, DNAse, BA, MCC, Kirby-
Bauer disk diffusion
Discrepant results resolved
by PastorexStaph Plus kit
(Bio-Rad)
Xpert:
Stored at 37°C, Xpert MRSA/SA BC assay within
80h
Further identification using Vitek 2 GP ID and/or
AST-P603 (bioMérieux) as
needed

Methods: Potential Impact
▪ Standard practice for calling out positive BCs with GPCC on Gram stain▪ Clinical information available suggested S. aureus sepsis
▪ Previous S. aureus on BC
▪ ICU patient
▪ S. aureus isolated provisionally or on final result
▪ For the study▪ Clinicians contacted in all included cases, when final culture result
indicated CoNS
▪ Basic data and demographic information
▪ Case-by-case assessment of whether earlier knowledge of result would have impacted antibiotic management
9

Results: Performance
▪ 231 bottles → 6 failed assays▪ Invalid (loss of SPC): 2
▪ Error (signal loss after initial amplification): 4
▪ Repeat testing: 3 → Resolution of error: 2
▪ Conservative error rate 1.7% (95% CI 0.7-4.4%)
▪ 227 bottles included
10
57%
8%
35%
Distribution of BC bottles, in %
FAN Aerobic Plus
FAN Anaerobic Plus
Paediatric FAN Plus
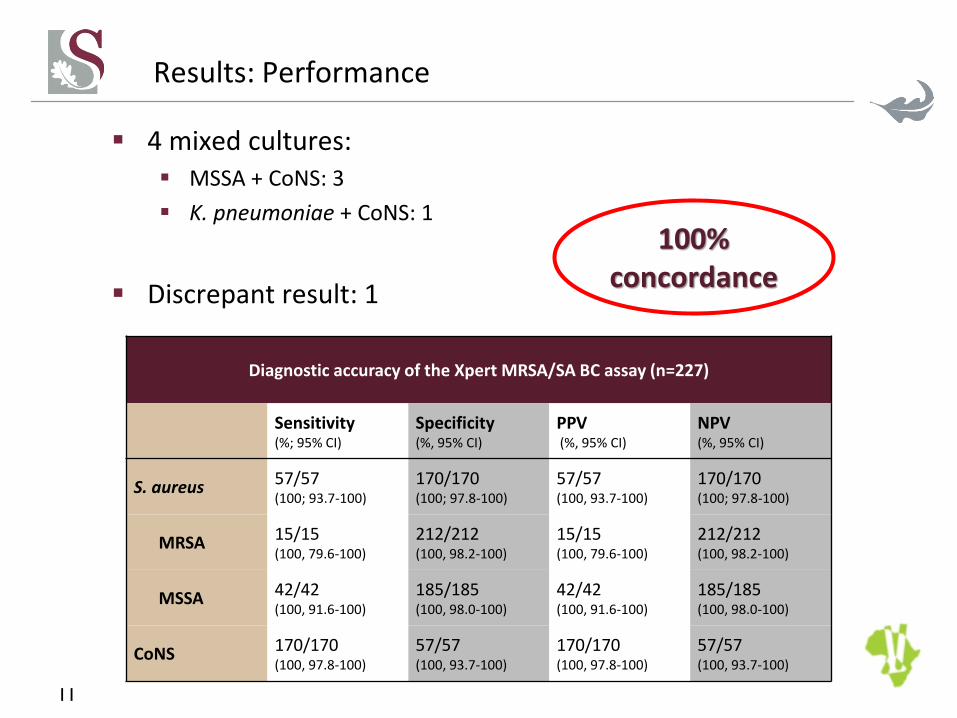
Results: Performance
▪ 4 mixed cultures: ▪ MSSA + CoNS: 3
▪ K. pneumoniae + CoNS: 1
▪ Discrepant result: 1
11
Diagnostic accuracy of the Xpert MRSA/SA BC assay (n=227)
Sensitivity(%; 95% CI)
Specificity(%, 95% CI)
PPV(%, 95% CI)
NPV (%, 95% CI)
S. aureus 57/57 (100; 93.7-100)
170/170 (100; 97.8-100)
57/57 (100, 93.7-100)
170/170 (100; 97.8-100)
MRSA 15/15 (100, 79.6-100)
212/212 (100, 98.2-100)
15/15 (100, 79.6-100)
212/212 (100, 98.2-100)
MSSA 42/42(100, 91.6-100)
185/185 (100, 98.0-100)
42/42(100, 91.6-100)
185/185 (100, 98.0-100)
CoNS 170/170 (100, 97.8-100)
57/57 (100, 93.7-100)
170/170 (100, 97.8-100)
57/57 (100, 93.7-100)
100% concordance

Results: Potential Impact
▪ Clinical information in 181 (79.7%)▪ 87.8% started antibiotics at the time of culture collection
▪ β-lactam-based in 150/181 (94.3%)
▪ MSSA-active agent in 125/150 (83.3%)
▪ Targeted antistaphylococcal therapy in 24/181 (13.3%)
▪ S. aureus bacteraemia with known antibiotic history: 46
▪ Targeted antistaphylococcal empiric therapy in 10 (21.7%)12
Demographic data, in % (n = 227)
Age/Ward
Adult (>18y) 66.5
ICU, high care and burns unit (% of adults) 16.6
Paediatric 33.5
ICU (% of paediatric patients) 13.0
Gender
Male 50.6
51,138,3
10,6
Onset of sepsis, in %
Community-acquired
Hospital-acquired
Not known

Results: Potential Impact
▪ Escalation▪ change from an ineffective to a more effective agent, or the addition
of a semisynthetic penicillin (MSSA) or glycopeptide (MRSA)
▪ De-escalation ▪ change in antibiotic to a narrower-spectrum, targeted
antistaphylococcal agent, or cessation of some or all antibiotics
▪ Unclassified: MSSA 1, CoNS 313
Evolution of antimicrobial therapy on Gram stain and culture result availability
MRSA (n=11) MSSA (n=35) CoNS (n=135)
On Gram On Final On Gram On Final On Gram On Final
Escalation 2 6 2 7 7 1
De-escalation 0 7 0 18 0 12
No action 9 3 32 9 125 119

Results: Potential Impact
▪ CoNS▪ Antibiotics stopped in 12/135, additional patient changed from
broad-spectrum β-lactam to alternative agent
▪ 9.6% (95% CI 5.7-15.8% )
▪ Total▪ Potential reduction in antibiotic use in 38/181 (21.0%, 95% CI 15.7-
27.5%)
▪ Further exposure to a broad-spectrum β-lactam in 30 (16.6%, 95% CI 11.9-22.7%)
▪ Further exposure to vancomycin in 4 (2.2%, 95% CI 0.9-5.5%)
▪ >30h potential time saving to final result
▪ Average time between between BC positivity and authorisation of final result 31.3h (IQR 20.7-42.5h)
14

Discussion
▪ Patients with unsuspected S. aureus bacteraemia▪ 34/46 patients with known histories (73.9%) changed antibiotics
on release of the final result
▪ >50% of the patients with MRSA bacteraemia and +-22% of all patients with S. aureus bacteraemia could have initiated appropriate therapy earlier
▪ Reduction in broad spectrum agents in 16.6% of the cohort with known antibiotic history
▪ β-lactam-β-lactamase inhibitor combinations
▪ extended-spectrum cephalosporins
▪ carbapenems
▪ vancomycin
15

Conclusion
▪ Xpert MRSA/SA BC assay performed well in differentiating between S. aureus and CoNS, and demonstrated a low error rate
▪ Conventional culture should still be performed in parallel
▪ Significant potential benefit of introduction of the assay▪ Appropriate therapy for S. aureus bacteraemia
▪ Modest reduction in antibiotics prescribed
16

Acknowledgements
▪ Professor Andrew Whitelaw
▪ NHLS Tygerberg Microbiology Laboratory
▪ NHLS Research Trust
▪ Cepheid
▪ Dr Shima Abdulgader
17