canadian diabetes association clinical practice guidelines acute coronary syndromes and diabetes...
TRANSCRIPT

Canadian Diabetes Association Clinical Practice Guidelines
Acute Coronary Syndromes and Diabetes
Chapter 26
Jean-Claude Tardif, Phillipe L. L’Allier,
David H. Fitchett

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Acute Coronary Syndrome Checklist
SCREEN for DM among patients with ACS
USE anti-platelet therapies, prasugrel or ticagrelor,
instead of clopidogrel in patients with DM undergoing
percutaneous coronary intervention (PCI)
AVOID both hyper- and hypoglycemia among
patients with DM admitted with ACS
2013

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Screen for DM Among Patients with ACS
• Diabetes is a strong risk factor for cardiovascular disease
• A significant proportion of patients with ACS have undiagnosed DM
• Screening for DM is essential among patients with ACS– Can use FPG, A1C or 75g OGTT– Consider standardized order sets

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Radke P W ,et al. Eur Heart J 2010;31:2971-3.
ACS Mortality in Diabetes vs. No Diabetes: Changes Across the Eras

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
All patients with DM and ACS should receive
the same treatments as those without DM …
with some differences
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Dual Anti-platelet Therapy in Patients with DM
• Diabetes ↑ risk of recurrent atherothrombotic events, including stent thrombosis
• Low dose ASA (75-150 mg) is effective for secondary prevention
• Dual anti-platelet therapy (ASA + clopidogrel) has been standard of care for non-ST elevation acute coronary syndrome (NSTE ACS) but recurrent events continue to occur, especially in diabetes

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
TRITON Study: Prasugrel vs. Clopidogrel
Days
% o
f Pa
tien
ts
0
5
10
15
0 30 60 90 180 270 360 450
HR: 0.81(0.73-0.90)
p <.001
Prasugrel (n=6813)
12.1%
9.9%
NNT = 46
Modified from Wiviott SD, et al. N Engl J Med. 2007;357(20):2001-2015.
CV Death/MI/Stroke at 15 monthsn =13,608: ACS (STEMI or NSTE ACS) and Planned PCI
CLOPIDOGREL300 mg LD/ 75 mg MD
PRASUGREL60 mg LD/ 10 mg MD
CV Death / MI / Stroke
ACS = Acute Coronary Syndrome; STEMI = ST-elevation Myocardial Infarction; NSTE ACS = Non-ST-elevation Acute coronary Syndrome; PCI = Percutaneous Coronary Intervention; LD = Loading Dose; MD = Maintenance Dose; NNT = Number Needed to Treat; CV = Cardiovascular
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
0
2
4
6
8
10
12
14
16
18
0 30 60 90 180 270 360 450Days
En
dp
oin
t (%
)
CV Death / MI / Stroke
TIMI Major Non CABG Bleeds
17.0%
12.2%
Modified from Wiviott SD et al. Circulation 10-14-2008;118:1626-1636
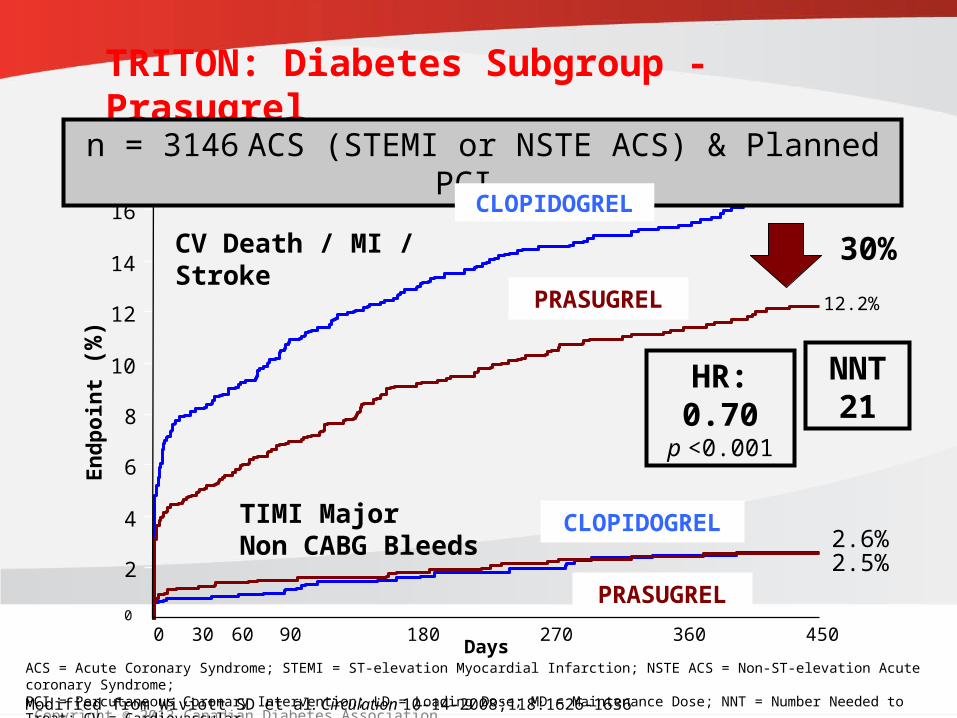
TRITON: Diabetes Subgroup - Prasugrel
30%
n = 3146 ACS (STEMI or NSTE ACS) & Planned PCI
PRASUGREL
PRASUGREL
2.6%2.5%
CLOPIDOGREL
CLOPIDOGREL
HR: 0.70p <0.001
NNT 21
ACS = Acute Coronary Syndrome; STEMI = ST-elevation Myocardial Infarction; NSTE ACS = Non-ST-elevation Acute coronary Syndrome; PCI = Percutaneous Coronary Intervention; LD = Loading Dose; MD = Maintenance Dose; NNT = Number Needed to Treat; CV = Cardiovascular

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Days after Randomisation0 60 120 180 240 300 360
12
11
10
9
8
7
6
5
4
3
2
10
Cu
mu
lati
ve in
cid
ence
(%
)
9.8%
11.7%
TICAGRELOR
Modified: Wallentin et al. New Eng J Med 2009; 361(11): 1045-1057
PLATO Study: Ticagrelor vs. Clopidogrel
n = 18,624 ACS
CLOPIDOGREL
NNT = 56HR: 0.84
(0.77-0.92) p <0.001
CV Death / MI / Stroke
ACS = Acute Coronary Syndrome; PCI = Percutaneous Coronary Intervention; NNT = Number Needed to Treat; CV=Cardiovascular
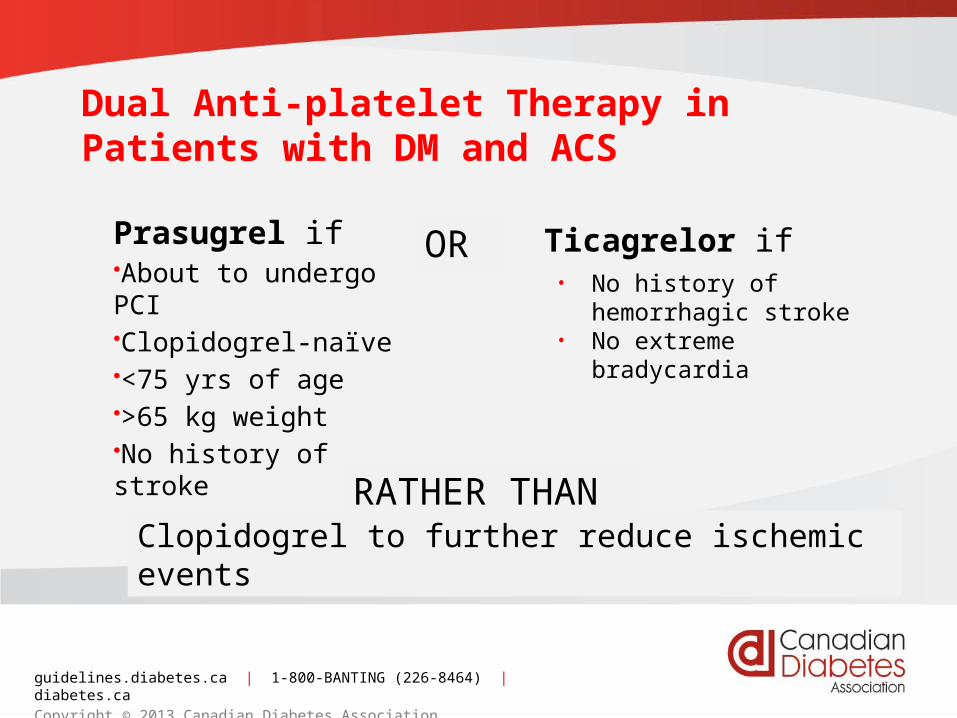
Dual Anti-platelet Therapy in Patients with DM and ACS
Prasugrel if•About to undergo PCI•Clopidogrel-naïve•<75 yrs of age•>65 kg weight•No history of stroke
OR
RATHER THAN
Ticagrelor if
Clopidogrel to further reduce ischemic events
• No history of hemorrhagic stroke
• No extreme bradycardia
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
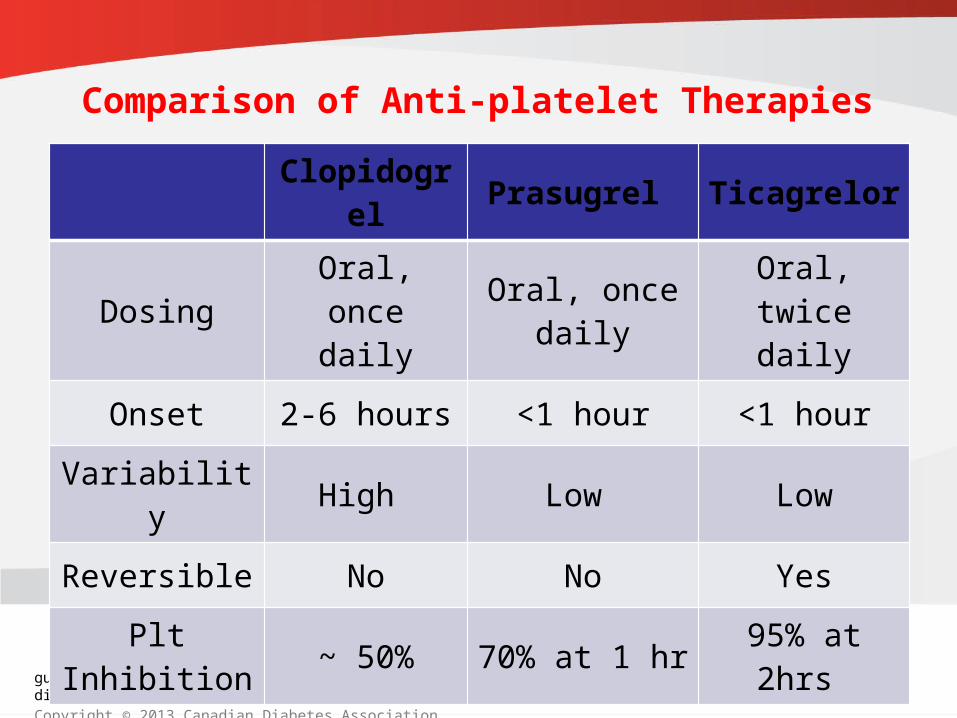
Clopidogrel Prasugrel Ticagrelor
Dosing Oral, once daily
Oral, once daily
Oral, twice daily
Onset 2-6 hours <1 hour <1 hour
Variability High Low Low
Reversible No No Yes
Plt Inhibition ~ 50% 70% at 1 hr 95% at 2hrs
Comparison of Anti-platelet Therapies

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Glycemic Control Among Patients with ACS
• Hyperglycemia during the first 24 to 48 hours after admission ↑ early mortality in patients with ACS
• Evidence to support treatment of elevated blood glucose after ACS = inconclusive
• Patients with acute MI and blood glucose (BG) on admission of >11 mmol/L likely benefit from maintaining BG 7.0 -10.0 mmol/L
– Insulin therapy may be required – Helpful to have protocols
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Recommendation 1
1. Patients with ACS should be screened for
diabetes with a fasting plasma glucose, A1C or
75 gram OGTT prior to discharge from
hospital. [Grade D consensus]
2013

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Recommendation 2
2. All patients with diabetes and ACS should receive
the same treatments that are recommended for
patients with ACS without diabetes since they
benefit equally [Grade D, consensus].
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Recommendation 3
3. Patients with diabetes and ACS undergoing PCI
should receive antiplatelet therapy with prasugrel
(if clopidogrel-naïve, <75 years of age, weight
>65kg and no history of stroke) [Grade A, Level 1] or
ticagrelor [Grade B, Level 1], rather than clopidogrel, to
further reduce recurrent ischemic events.
Patients with DM and non-STE ACS and higher risk
features, destined for a selective invasive strategy
should receive ticagrelor, rather than clopidogrel [Grade B level 2]
2013
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Recommendation 4
4. Patients with diabetes and non-STE ACS and
high risk features should receive an early
invasive strategy rather than a selective invasive
approach to revascularization to reduce recurrent
coronary events, unless contraindicated [Grade B
Level 2].
2013
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Recommendation 5
5. In patients with diabetes and STE-ACS, the
presence of retinopathy should not be a
contraindication to fibrinolysis [Grade B, Level 2].

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Recommendation 6
6. In-hospital management of diabetes in ACS should
include strategies to avoid both hyperglycemia and
hypoglycemia:– Blood glucose should be measured on admission and
monitored throughout the hospitalization [Grade D, Consensus]
– Patients with acute MI and blood glucose on admission of
>11 mmol/L may receive glycemic control in the range of
7.0 to 10.0 mmol/L followed by strategies to achieve
recommended glucose targets long term [Grade C, Level 2]

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Recommendation 6 (continued)
6. In-hospital management of diabetes in ACS
should include strategies to avoid both
hyperglycemia and hypoglycemia:– Insulin therapy may be required to achieve these targets
[Grade D, consensus]. A similar approach may be taken in those
with diabetes and admission blood glucose <11.0 mmol/L [Grade D, consensus]
– An appropriate protocol should be developed and staff
trained to ensure the safe and effective implementation of
this therapy and to minimize the likelihood of hypoglycemia [Grade D, Consensus].
CDA Clinical Practice Guidelines
www.guidelines.diabetes.ca – for professionals
1-800-BANTING (226-8464)
www.diabetes.ca – for patients
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association