cancer ecology in kerala, india
TRANSCRIPT
This article was downloaded by: [University of Auckland Library]On: 08 October 2014, At: 15:54Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number:1072954 Registered office: Mortimer House, 37-41 Mortimer Street,London W1T 3JH, UK
International Journal ofEnvironmental StudiesPublication details, including instructions forauthors and subscription information:http://www.tandfonline.com/loi/genv20
Cancer ecology in Kerala,IndiaRais Akhtar aa Dept. of Geography , University of Kashmir ,Srinagar, J and K, 190 006, IndiaPublished online: 24 Feb 2007.
To cite this article: Rais Akhtar (1998) Cancer ecology in Kerala, India,International Journal of Environmental Studies, 55:4, 345-355, DOI:10.1080/00207239808711190
To link to this article: http://dx.doi.org/10.1080/00207239808711190
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of allthe information (the “Content”) contained in the publications on ourplatform. However, Taylor & Francis, our agents, and our licensorsmake no representations or warranties whatsoever as to the accuracy,completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views ofthe authors, and are not the views of or endorsed by Taylor & Francis.The accuracy of the Content should not be relied upon and should beindependently verified with primary sources of information. Taylor andFrancis shall not be liable for any losses, actions, claims, proceedings,demands, costs, expenses, damages, and other liabilities whatsoeveror howsoever caused arising directly or indirectly in connection with, inrelation to or arising out of the use of the Content.
This article may be used for research, teaching, and private studypurposes. Any substantial or systematic reproduction, redistribution,
reselling, loan, sub-licensing, systematic supply, or distribution in anyform to anyone is expressly forbidden. Terms & Conditions of accessand use can be found at http://www.tandfonline.com/page/terms-and-conditions
Dow
nloa
ded
by [
Uni
vers
ity o
f A
uckl
and
Lib
rary
] at
15:
54 0
8 O
ctob
er 2
014
Intern. J. Environmental Studies, 1998, Vol. 55, pp. 345-355 © 1998 OPA (Overseas Publishers Association) N.V.Reprints available directly from the publisher Published by license underPhotocopying permitted by license only the Gordon and Breach Science
Publishers imprint.Printed in India.
CANCER ECOLOGY IN KERALA, INDIA
RAIS AKHTAR
Dept. of Geography, University of Kashmir,Srinagar (J and KJ-190 006 (India)
(Received in final form 14 June 1997)
Studies carried out on the spatial distribution of cancer in India reveal a high intensityzone of cancer in Kerala, especially in"respect of tumours of the oral cavity, pharynx andrespiratory system. It is suggested that an ecological approach involving the study ofenvironmental deficiencies or overloads of minerals and radio-active elements in the soiland dietary habits, could provide useful guidelines for the control of cancer in Kerala.
Keywords: Cancer; Kerala; ecological approach; radio-activity
INTRODUCTION
The geographical association between geochemical variables and theoccurrence of certain human diseases, including cancer, has beenstudied for quite some time. The association between the distributionof elements of soils and the distribution of mortality from car-diovascular disease, multiple sclerosis and certain types of cancers hasbeen particularly strong and persistent. Howe's work on stomachcancer and lead in Wales in the United Kingdom is a pioneeringattempt in the study of geocancerology [1]. Armstrong's work on soiland cancer [2], Warren's study on geology and health [3], and Voisin'spioneering effort, So/7 Grass and Cancer [4] are important contribu-tions on the subject. An attempt has been made in the present paper tostudy the geoecological condition of Kerala in relation to theoccurrence of cancer (Fig. 1).
Studies carried out on the spatial distribution of cancer in Indiareveal a high intensity zone of cancer in Kerala, particularly in thesouthern region, also known as Malabar.
345
Dow
nloa
ded
by [
Uni
vers
ity o
f A
uckl
and
Lib
rary
] at
15:
54 0
8 O
ctob
er 2
014
346 R. AKHTAR
FIGURE 1 Location of Kerala State in India.
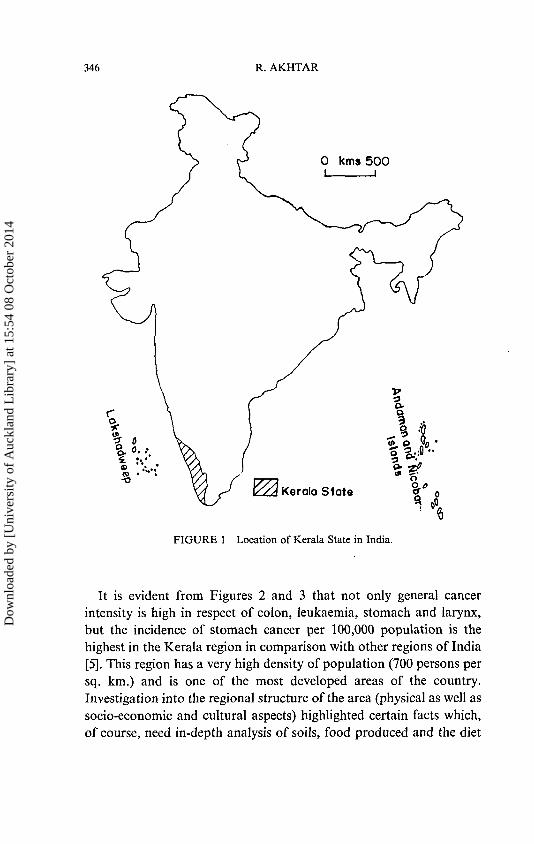
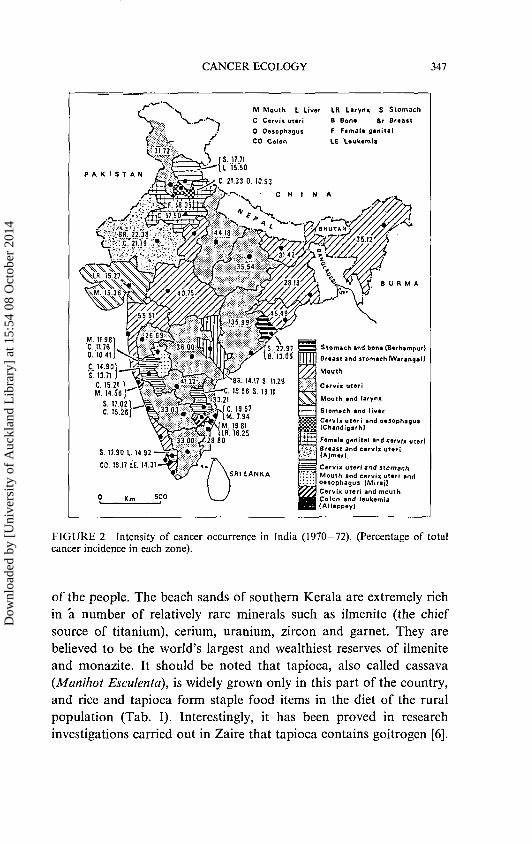
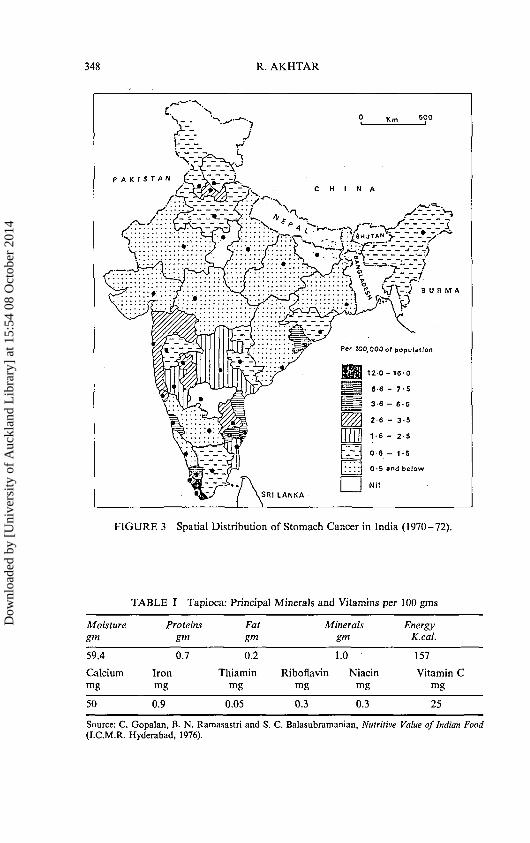
It is evident from Figures 2 and 3 that not only general cancerintensity is high in respect of colon, leukaemia, stomach and larynx,but the incidence of stomach cancer per 100,000 population is thehighest in the Kerala region in comparison with other regions of India[5]. This region has a very high density of population (700 persons persq. km.) and is one of the most developed areas of the country.Investigation into the regional structure of the area (physical as well associo-economic and cultural aspects) highlighted certain facts which,of course, need in-depth analysis of soils, food produced and the diet
Dow
nloa
ded
by [
Uni
vers
ity o
f A
uckl
and
Lib
rary
] at
15:
54 0
8 O
ctob
er 2
014
CANCER ECOLOGY 347
M Mouth L Liver LR Larynx S Stomach
C Cervix uteri B Bon* 8r Breast
0 OesophagusCO Colon
F F»mal« genital
LE Leukemia
P A K I S T A N
M. 11.981C. 11.760. 10.41)
C. 14.901! 13.71 )
Stomach and bone (Berhampur)
Sraast and stomach (Warangal)
Mouth
SR. 14.17 S. 11.29•C. 13.66 S. 1311
3.21C. 19.57M. 7.94
M. 19.81, . .IB".'16.25' 2 9 8 0 Female genital and cervix uteri
(Ajmerl7 " : '
Cervix uteri and stomachMouth and cervix uteri ana1
oesophagus IMira j !Cervix uteri and mouthColon and leukemiaAlleppey)
FIGURE 2 Intensity of cancer occurrence in India (1970-72). (Percentage of totalcancer incidence in each zone).
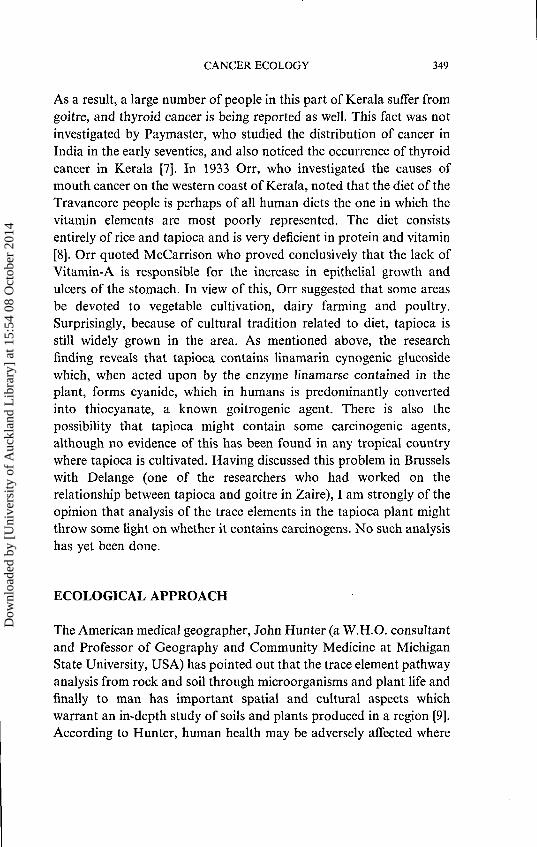
of the people. The beach sands of southern Kerala are extremely richin a number of relatively rare minerals such as ilmenite (the chiefsource of titanium), cerium, uranium, zircon and garnet. They arebelieved to be the world's largest and wealthiest reserves of ilmeniteand monazite. It should be noted that tapioca, also called cassava{Manihot Esculenta), is widely grown only in this part of the country,and rice and tapioca form staple food items in the diet of the ruralpopulation (Tab. I). Interestingly, it has been proved in researchinvestigations carried out in Zaire that tapioca contains goitrogen [6].
Dow
nloa
ded
by [
Uni
vers
ity o
f A
uckl
and
Lib
rary
] at
15:
54 0
8 O
ctob
er 2
014
348 R. AKHTAR
P A K I S T A N
FIGURE 3 Spatial Distribution of Stomach Cancer in India (1970-72).
TABLE I Tapioca: Principal Minerals and Vitamins per 100 gms
Moisturegm
59.4
Calciummg
50
Proteinsgm
0.7
Ironmg
0.9
Fatgm
0.2
Thiaminmg
0.05
Mineralsgm
1.0
Riboflavin Niacinmg mg
0.3 0.3
EnergyK.cal.
157
Vitamin Cmg
25
Source: C. Gopalan, B. N. Ramasastri and S. C. Balasubramanian, Nutritive Value of Indian Food(I.C.M.R. Hyderabad, 1976).
Dow
nloa
ded
by [
Uni
vers
ity o
f A
uckl
and
Lib
rary
] at
15:
54 0
8 O
ctob
er 2
014
CANCER ECOLOGY 349
As a result, a large number of people in this part of Kerala suffer fromgoitre, and thyroid cancer is being reported as well. This fact was notinvestigated by Paymaster, who studied the distribution of cancer inIndia in the early seventies, and also noticed the occurrence of thyroidcancer in Kerala [7]. In 1933 Orr, who investigated the causes ofmouth cancer on the western coast of Kerala, noted that the diet of theTravancore people is perhaps of all human diets the one in which thevitamin elements are most poorly represented. The diet consistsentirely of rice and tapioca and is very deficient in protein and vitamin[8]. Orr quoted McCarrison who proved conclusively that the lack ofVitamin-A is responsible for the increase in epithelial growth andulcers of the stomach. In view of this, Orr suggested that some areasbe devoted to vegetable cultivation, dairy farming and poultry.Surprisingly, because of cultural tradition related to diet, tapioca isstill widely grown in the area. As mentioned above, the researchfinding reveals that tapioca contains linamarin cynogenic glucosidewhich, when acted upon by the enzyme linamarse contained in theplant, forms cyanide, which in humans is predominantly convertedinto thiocyanate, a known goitrogenic agent. There is also thepossibility that tapioca might contain some carcinogenic agents,although no evidence of this has been found in any tropical countrywhere tapioca is cultivated. Having discussed this problem in Brusselswith Delange (one of the researchers who had worked on therelationship between tapioca and goitre in Zaire), I am strongly of theopinion that analysis of the trace elements in the tapioca plant mightthrow some light on whether it contains carcinogens. No such analysishas yet been done.
ECOLOGICAL APPROACH
The American medical geographer, John Hunter (a W.H.O. consultantand Professor of Geography and Community Medicine at MichiganState University, USA) has pointed out that the trace element pathwayanalysis from rock and soil through microorganisms and plant life andfinally to man has important spatial and cultural aspects whichwarrant an in-depth study of soils and plants produced in a region [9].According to Hunter, human health may be adversely affected where
Dow
nloa
ded
by [
Uni
vers
ity o
f A
uckl
and
Lib
rary
] at
15:
54 0
8 O
ctob
er 2
014
350 R. AKHTAR
essential trace elements, such as iodine, copper or zinc, are regionallydeficient, or where non-essential minerals, such as lead or arsenic (orradio-active elements in the case of Kerala), occur in high concentra-tions. Environmental deficiencies or overloads of health-related min-erals are mediated through the consumption of drinking water andlocally-grown foodstuffs (tapioca in the context of Kerala) reflectingthe customary dietary pattern.
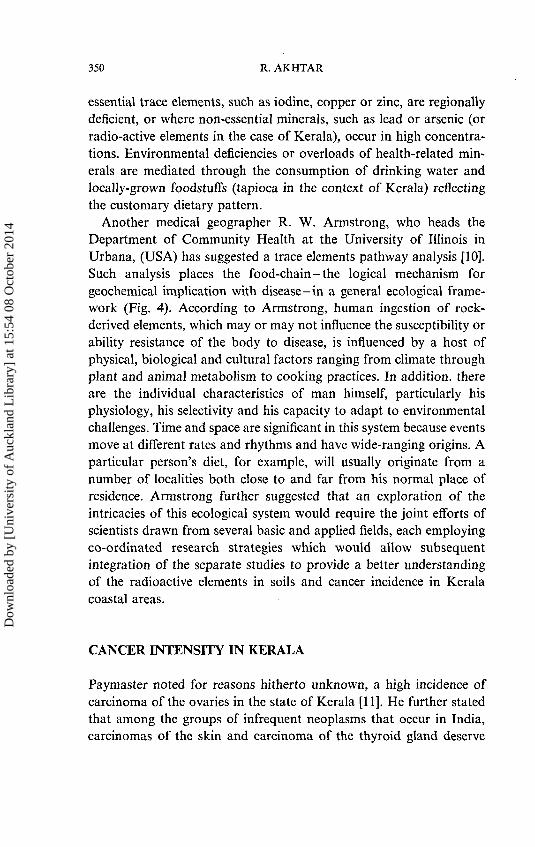
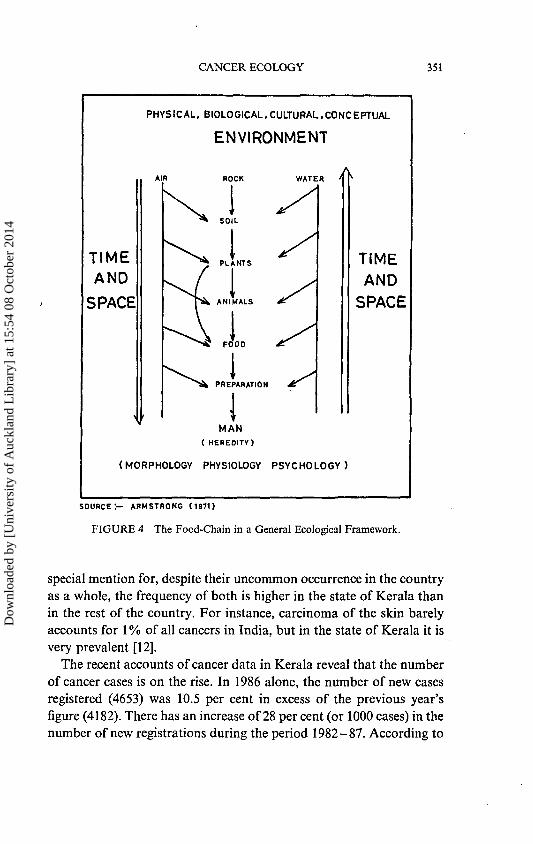
Another medical geographer R. W. Armstrong, who heads theDepartment of Community Health at the University of Illinois inUrbana, (USA) has suggested a trace elements pathway analysis [10].Such analysis places the food-chain-the logical mechanism forgeochemical implication with disease-in a general ecological frame-work (Fig. 4). According to Armstrong, human ingestion of rock-derived elements, which may or may not influence the susceptibility orability resistance of the body to disease, is influenced by a host ofphysical, biological and cultural factors ranging from climate throughplant and animal metabolism to cooking practices. In addition, thereare the individual characteristics of man himself, particularly hisphysiology, his selectivity and his capacity to adapt to environmentalchallenges. Time and space are significant in this system because eventsmove at different rates and rhythms and have wide-ranging origins. Aparticular person's diet, for example, will usually originate from anumber of localities both close to and far from his normal place ofresidence. Armstrong further suggested that an exploration of theintricacies of this ecological system would require the joint efforts ofscientists drawn from several basic and applied fields, each employingco-ordinated research strategies which would allow subsequentintegration of the separate studies to provide a better understandingof the radioactive elements in soils and cancer incidence in Keralacoastal areas.
CANCER INTENSITY IN KERALA
Paymaster noted for reasons hitherto unknown, a high incidence ofcarcinoma of the ovaries in the state of Kerala [11]. He further statedthat among the groups of infrequent neoplasms that occur in India,carcinomas of the skin and carcinoma of the thyroid gland deserve
Dow
nloa
ded
by [
Uni
vers
ity o
f A
uckl
and
Lib
rary
] at
15:
54 0
8 O
ctob
er 2
014
CANCER ECOLOGY 351
PHYSICAL, BIOLOGICAL,CULTURAL.CONCEPTUAL
ENVIRONMENT
TIMEAND
SPACE
ROCK WATER
PREPARATION
TIMEAND
SPACE
(MORPHOLOGY PHYSIOLOGY PSYCHOLOGY)
SOURCE:- ARMSTRONG (1971)
FIGURE 4 The Food-Chain in a General Ecological Framework.
special mention for, despite their uncommon occurrence in the countryas a whole, the frequency of both is higher in the state of Kerala thanin the rest of the country. For instance, carcinoma of the skin barelyaccounts for 1% of all cancers in India, but in the state of Kerala it isvery prevalent [12].
The recent accounts of cancer data in Kerala reveal that the numberof cancer cases is on the rise. In 1986 alone, the number of new casesregistered (4653) was 10.5 per cent in excess of the previous year'sfigure (4182). There has an increase of 28 per cent (or 1000 cases) in thenumber of new registrations during the period 1982-87. According to
Dow
nloa
ded
by [
Uni
vers
ity o
f A
uckl
and
Lib
rary
] at
15:
54 0
8 O
ctob
er 2
014
352 R. AKHTAR
recent information some 6209 cases have been registered during theyear 1993. In Trivandrum City, the incidence of oral (mouth andthroat) cancer is the highest (i.e., 25 per 100,000 population or 33 percent of all types of cancers). This figure is similar to that of incidencerates in Singapore, U.K. and the U.S.A. [13]. In Kerala the generalmorbidity rate is also rising [14].
According to Krishnan Nair, two major factors which contribute tothe relative increase in cancer incidence are (1) control of communic-able diseases and (2) subsequent increases in life expectancy. The aver-age life expectancy in Kerala is estimated to be 63.5 years for malesand 63 years for females (which is about 12 years longer than theaverage national figures [15].
The work carried out by Ermans and his colleagues in Zaire showedthat the development of goitre in Ubangi is critically linked to theconditions of the nutritional micro-environment and specifically to thebalance between iodine and thiocyanate. Tapioca is the basic foodstuffand it contains large quantities of cyanide. If it is not correctlydetoxified during preparation, the food ingested contains significantamounts of residual cyanide causing an increase in thiocyanate. In thepresence of iodine deficiency or even with normal amounts of iodine,thiocyanate leads to the development of goitre.
Several examples can be cited in support of such analysis of thepresence of radioactive elements in soils and the occurrence of cancer.For example, in 1957 two small villages in the Apennines in Italyshifted to a new source of water supply. Within a few years, almosthalf of the population had been operated upon for various types ofcancers, mainly stomach and intestine. It was only in 1965 that a localpractitioner traced the trouble to this newly developed water supplywhich was found to contain more than 50 times the radioactivity of thewater previously being used in the villages [16].
In India, Sarma has suggested that the cancer of larynx in thenorth-eastern part of the country is due to betal nut chewing [17]. Hefurther argued that the betal nut grown in the north-eastern regionmay absorb some carcinogenic agents from the oil bearing soils andthus become more irritant. Betal chewing is also common in Kerala,and people use lime available in the area near Trivandrum.
In order to strengthen the hypothesis of ecological relation with thecancer incidence, a detailed study of the incidence of some cancer types
Dow
nloa
ded
by [
Uni
vers
ity o
f A
uckl
and
Lib
rary
] at
15:
54 0
8 O
ctob
er 2
014
CANCER ECOLOGY 353
in Kerala and a comparative study with Bombay and Delhi regionswould be appropriate.
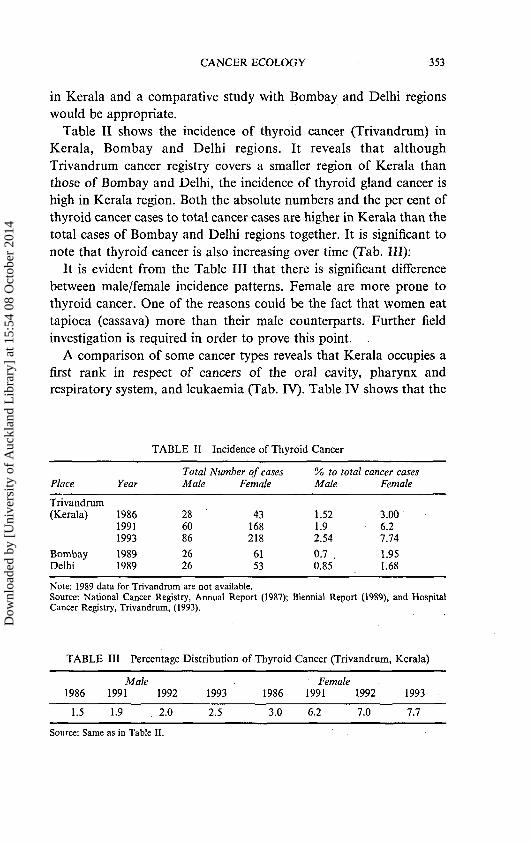
Table II shows the incidence of thyroid cancer (Trivandrum) inKerala, Bombay and Delhi regions. It reveals that althoughTrivandrum cancer registry covers a smaller region of Kerala thanthose of Bombay and Delhi, the incidence of thyroid gland cancer ishigh in Kerala region. Both the absolute numbers and the per cent ofthyroid cancer cases to total cancer cases are higher in Kerala than thetotal cases of Bombay and Delhi regions together. It is significant tonote that thyroid cancer is also increasing over time (Tab. Ill):
It is evident from the Table III that there is significant differencebetween male/female incidence patterns. Female are more prone tothyroid cancer. One of the reasons could be the fact that women eattapioca (cassava) more than their male counterparts. Further fieldinvestigation is required in order to prove this point. .
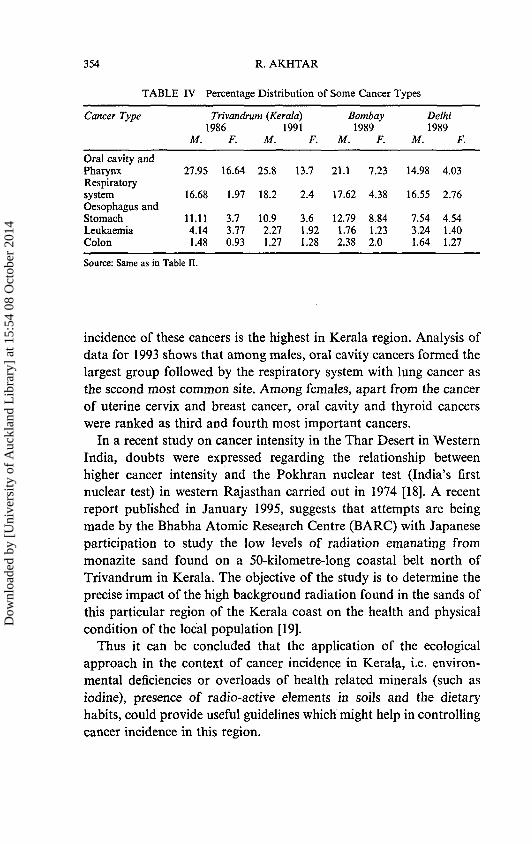
A comparison of some cancer types reveals that Kerala occupies afirst rank in respect of cancers of the oral cavity, pharynx andrespiratory system, and leukaemia (Tab. IV). Table IV shows that the
TABLE II Incidence of Thyroid Cancer
Total Number of cases % to total cancer casesPlace Year Male Female Male Female
Trivandrum(Kerala)
BombayDelhi
198619911993
19891989
286086
2626
43168218
6153
1.521.92.54
0.7 .0.85
3.006.27.74
1.951.68
Note: 1989 data for Trivandrum are not available.Source: National Cancer Registry, Annual Report (1987); Biennial Report (1989), and HospitalCancer Registry, Trivandrum, (1993).
TABLE
1986
1.5
111 Percentage
Male1991 1992
1.9 2.0
Distribution
1993
2.5
of Thyroid
1986
3.0
Cancer (Trivandrum,
Female1991 1992
6.2 7.0
Kerala)
1993.
7.7
Source: Same as in Table II.
Dow
nloa
ded
by [
Uni
vers
ity o
f A
uckl
and
Lib
rary
] at
15:
54 0
8 O
ctob
er 2
014
354 R. AKHTAR
TABLE IV Percentage Distribution of Some Cancer Types
Cancer Type
Oral cavity andPharynxRespiratorysystemOesophagus andStomachLeukaemiaColon
Trivandrum (Kerala)1986
M.
27.95
16.68
11.114.141.48
F.
16.64
1.97
3.73.770.93
M.
25.8
18.2
10.92.271.27
1991F.
13.7
2.4
3.61.921.28
Bombay1989
M. F.
21.1 7.23
17.62 4.38
12.79 8.841.76 1.232.38 2.0
Delhi1989
M.
14.98
16.55
7.543.241.64
F.
4.03
2.76
4.541.401.27
Source: Same as in Table II.
incidence of these cancers is the highest in Kerala region. Analysis ofdata for 1993 shows that among males, oral cavity cancers formed thelargest group followed by the respiratory system with lung cancer asthe second most common site. Among females, apart from the cancerof uterine cervix and breast cancer, oral cavity and thyroid cancerswere ranked as third and fourth most important cancers.
In a recent study on cancer intensity in the Thar Desert in WesternIndia, doubts were expressed regarding the relationship betweenhigher cancer intensity and the Pokhran nuclear test (India's firstnuclear test) in western Rajasthan carried out in 1974 [18]. A recentreport published in January 1995, suggests that attempts are beingmade by the Bhabha Atomic Research Centre (BARC) with Japaneseparticipation to study the low levels of radiation emanating frommonazite sand found on a 50-kilometre-long coastal belt north ofTrivandrum in Kerala. The objective of the study is to determine theprecise impact of the high background radiation found in the sands ofthis particular region of the Kerala coast on the health and physicalcondition of the local population [19].
Thus it can be concluded that the application of the ecologicalapproach in the context of cancer incidence in Kerala, i.e. environ-mental deficiencies or overloads of health related minerals (such asiodine), presence of radio-active elements in soils and the dietaryhabits, could provide useful guidelines which might help in controllingcancer incidence in this region.
Dow
nloa
ded
by [
Uni
vers
ity o
f A
uckl
and
Lib
rary
] at
15:
54 0
8 O
ctob
er 2
014
CANCER ECOLOGY 355
A cknowledgement
I am grateful for the useful comments made by Dr. Keith Ball andProf. R. W. Armstrong. I am also thankful to Dr. M. Krishanan Nair,Director, Regional Cancer Centre, Trivandrum, for providingnecessary data.
References
[1] G. M. Howe, "The geography of lung-bronchus cancer and stomach cancer in theUnited Kingdom", Scottish Geographical Magazine 87, 202-220 (1971).
[2] R. W. Armstrong, "Cancer and soil: Review and councel", The ProfessionalGeographer 14(3), 7 -13 (1962).
[3] H. V. Warren, "Some aspects of the relationship between health and geology",Can. J. Public Health 52, 157-164 (1961).
[4] A. Voisin, Soil, Grass and Cancer (Crosby, Lockwood and Sons., PhiosophicalLibrary, New York, 1959).
[5] R. Akhtar, "Human cancer in Orient-India", In: (G. M. Howe, ed.) GlobalGeocancerology: A World Geography of Human Cancer (Churchill Livingstone,Edinburgh, 1986) pp. 261-271.
[6] P. Bourdoux, et al. "Cassava toxicity: The role of linemarin", In: (A. M. Ermans,N. M. Mbulamoko, F. Delange and R. Ahluwalia, eds.) Role of Cassava in theEtiology of Endemic Goiter and Cretinism (IDRC, Ottawa, 1980) pp. 15-28.
[7] J. C. Paymaster, "Cancer and its distribution in India", Cancer 17, 1026-1034(1964).
[8] I. M. Orr, "Oral cancer in betal-nut chewers in Travancore", Lancet 2, 575-580(1933).
[9] J. M. Hunter, "The challenge of medical geography", In: (J. M. Hunter, ed.) TheGeography of Health and Disease. (University of North Carolina at Chappel Hill,Department of Geography, Studies in Geography, 1974) No. 6, pp. 1 — 31.
[10] R. W. Armstrong, "Medical geography and its geological substrate", In: (H. L.Cannon and H. C. Hopps, eds.) Environmental Geochemistry in Health and Disease(Boulder, Col., Geological Society of America, 1971). No. 123, pp. 211-219.
[11] J. C. Paymaster, op. cit., p. 1032.[12] J. C. Paymaster, op. cit., p. 1034.[13] "Cancer on the rise in Kerala", The Times of India, New Delhi, 8 (16 August, 1988).[14] "Blot on health map: Morbidity rate in Kerala has gone up".77;e Pioneer, New
Delhi, 9, (20 July, 1992).[15] The Times of India, op. cit.[16] H. V. Warren, "Geology and health", In: (R. Akhtar, ed.) Environment and
Health: Themes in Medical Geography, (Ashish Publishing Housing, New Delhi,1990)pp.299-313.
[17] S. N. Sarma, "A study into the incidence and etiology of cancer of Iarnyx andadjacent parts in Assam", Indian J. Medical Research 46, 525-533 (1958).
[18] Y. Goyal, "Cancer: A health hazard in the Thar desert", The Hindustan Times,New Delhi 13 (7 November, 1993).
[19] "Research on sand radiation", The Hindustan Times, New Delhi, (9 January,1995).
Dow
nloa
ded
by [
Uni
vers
ity o
f A
uckl
and
Lib
rary
] at
15:
54 0
8 O
ctob
er 2
014