cancer immunotherapy - ceconcepts.com pocket guide.pdf · response kinetics recist vs irrc factor...
TRANSCRIPT

CANCER IMMUNOTHERAPY
Pocket Guide

Unique Clinical Features
Tumor Response Kinetics
• Response patterns associated with immune checkpoint blockade may differ from those associated with conventional therapies, which has prompted the development of immune-related response criteria (irRC)a
Immune-Related Adverse Events (irAEs)
• By enhancing immune system function, immune checkpoint blockade can lead to autoinflammatory side effects called irAEsb
a. Wolchok JD, et al. Clin Cancer Res. 2009;15(23):7412-7420.b. Weber JS, et al. J Clin Oncol. 2015;33(18):2092-2099.
1
Disclaimer: The information in this pocket guide is intended as reference material and should not replace clinical judgment or updated recommendations that may supersede those provided here.

Response KineticsRECIST vs irRC
Factor RECIST irRCMeasurement
of tumor burden
• Unidimensional • Bidimensional
CR • Disappearance of all target and non-target lesions
• Lymph nodes must regress to <10mm short axis
• No new lesions• Requires confirmation
• Same as RECIST
PR • ≥30% decrease in tumor burden compared to baseline
• Requires confirmation
• ≥50% decrease in tumor burden compared to baseline
• Requires confirmation
PD • ≥20% plus 5mm absolute increase in tumor burden compared with nadir
• Progression of non-target lesions and/or appearance of new lesions (at any single time point)
• ≥25% increase in tumor burden compared to most recent prior evaluation
• New lesions added to tumor burden
• Requires confirmation
SD • Any response pattern that does not meet criteria for CR, PR, or PD
• Same as RECIST
RECIST = response evaluation criteria in solid tumors; CR = complete response; PR = partial response; PD = progressive disease; SD = stable disease
Agarwala SS. Semin Oncol. 2015;42Suppl 3:S20-S27.
2

Key Points About Evaluating Activity
• Antitumor activity may appear delayed compared with cytotoxic therapies
• Patients may experience response after apparent progressive disease
• Development of new small lesions in the presence of other shrinking lesions may be clinically insignificant
• Durable stable disease may indicate response
• Development of progressive disease should be confirmed before discontinuing therapy
Agarwala SS. Semin Oncol. 2015;42 Suppl 3:S20-S27.
3
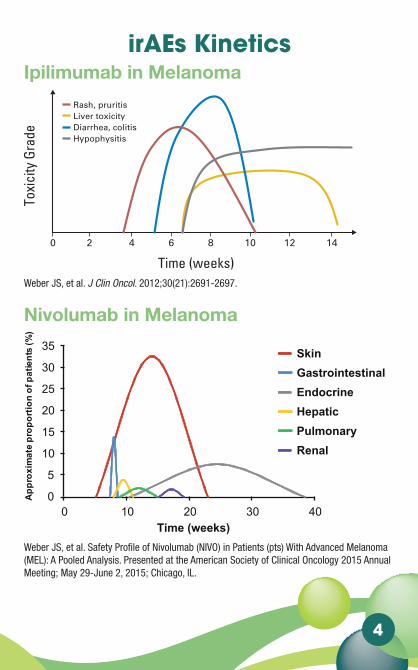
irAEs Kinetics
Ipilimumab in Melanoma
Weber JS, et al. J Clin Oncol. 2012;30(21):2691-2697.
Nivolumab in Melanoma
Weber JS, et al. Safety Profile of Nivolumab (NIVO) in Patients (pts) With Advanced Melanoma (MEL): A Pooled Analysis. Presented at the American Society of Clinical Oncology 2015 Annual Meeting; May 29-June 2, 2015; Chicago, IL.
endocrinologic AEs only after an average of 9 weeks. Frequencies ofdose-limiting ipilimumab-related irAEs increased with dose; no grade3 to 4 irAEs were observed at 0.3 mg/kg, 7% at 3 mg/kg, and 25% at 10mg/kg.8 The frequency of irAEs increased with dose but not the qualityor type of irAE,8 suggesting that experience with toxicity at 10 mg/kgwill be useful for the clinician treating patients at the FDA-approvedipilimumab dose of 3 mg/kg.
Currently, algorithms help clinicians manage and treat the mostcommon irAEs. These algorithms18present detailed managementguidelines that depend on the severity of the particular irAE.
ORGAN-SPECIFIC IRAES OF IPILIMUMAB
Skin and MucosaIn 47% to 68% of patients receiving ipilimumab, a diffuse, pre-
dominantly maculopapular rash that can be intensely pruritic wasobserved after an average of 3.6 weeks.8-10 In 4% of patients, it wasconsidered to be severe. Histologically, a perivascular lymphocyticinfiltrate extending deep into the dermis and up into the epidermiswas evident. Immunohistochemical staining showed that CD4� andmelan-A–specific CD8� T cells were in close proximity to apoptoticmelanocytes,19 suggesting that anti-CTLA-4 antibodies stimulated animmune response directed against melanocytes. This is supported byan 11% rate of vitiligo in a phase II trial with ipilimumab.8 Skineruptions and pruritus are generally managed symptomatically andusually do not require skipping a dose or discontinuation. The use oftopical glucocorticosteroids (eg, betamethasone 0.1% cream) or urea-containing creams in combination with oral antipruritics (eg, diphen-hydramine HCl or hydroxyzine HCl) are recommended. In case ofgrade 3 dermatologic irAEs, withholding a dose and treating with a4-week tapering course of oral steroids is recommended, starting with1 mg/kg prednisone once per day. One should withhold a scheduleddose for persistent grade 2 or for grade 3 skin toxicity but permanentlydiscontinue ipilimumab for life-threatening toxicity. Rare occur-rences of toxic epidermal necrolysis, as well as Stevens-Johnson syn-drome have been reported with ipilimumab, several of which haveresulted in death. Ipilimumab should be permanently discontinued inpatients with grade 4 skin toxicity, and steroids should be initiated at 1to 2 mg/kg prednisone or equivalent, tapering over not less than30 days.
Diarrhea/ColitisDiarrhea was observed in 44% of patients receiving ipilimumab
at 10 mg/kg.7 Severe diarrhea (grade 3 or 4; at least six diarrheal bowelmovements above baseline in 24 hours) was reported in approxi-mately 18% of patients.7 Diarrhea can also be associated with signs andsymptoms of colitis, which can lead to obstruction and bowel perfo-ration, potentially requiring colostomy. The rate of bowel perforationis less than 1%,5,7 including five occurrences in a cohort of 511 patientsnoted in the ipilimumab package insert and in one of 177 patients inanother long-term follow-up series.20 IrAE-related colitis involves thedescending colon more often than the sigmoid colon, ascending co-lon, or rectum.8 Histologically, a neutrophilic infiltrate in 46% ofpatients, a lymphocytic infiltrate in 15%, and a mixed neutrophilic-lymphocytic infiltrate in 38%2 have been observed.
In low-grade diarrhea (grade 1, an increase of two diarrhealbowel movements over baseline in 24 hours), purely symptomatictreatment with loperamide, oral hydration, and electrolyte substitu-tion can be instituted. The American Dietary Association colitis diet isrecommended. With persistent or grade 2 or higher diarrhea, GIinfection or inflammatory bowel disease can be ruled out by examina-tion for stool leukocytes, stool cultures, and a Clostridium difficile titer.Oral diphenoxylate hydrochloride and atropine sulfate four times perday and budesonide 9 mg once per day has been used by the authors totreat grade 2 diarrhea. Sigmoidoscopy or colonoscopy to confirm orrule out colitis is indicated for persistent grade 2 diarrhea or rectalbleeding. Although there are concerns over the possibility of perfora-tion, those procedures can generally be done safely. The presence ofcolitis may change the therapeutic approach, since unexpected diffuseulceration and bleeding with grade 2 diarrhea may mandate a courseof oral steroids and represents an increased risk for the development ofa bowel perforation. With grade 3 or 4 diarrhea (an increase of sevendiarrhealbowelmovementsormoreoverbaselinein24hours),treatmentshould be discontinued, and intravenous steroids and replenishment offluid and electrolytes should be given. Intravenous methylprednisolone125 mg should be given. Oral prednisone 1 to 2 mg/kg once per day ordexamethasone 4 mg every 4 hours is indicated thereafter, followed bya taper over the next 4 weeks. Generally, this leads to significantimprovement of symptoms within 1 to 2 weeks. It is important totaper steroid therapy over at least 4 weeks to ensure complete resolu-tion of symptoms. In patients with diffuse and severe ulcerationand/or bleeding, a taper of up to 6 to 8 weeks is reasonable, since rapidtapering can result in recurrence or worsening of symptoms. The useof opiates and other analgesics may mask the pain associated withcolitis induced by ipilimumab. A low threshold for concern about GIcomplications, including perforation and obstruction, should bemaintained by physicians using ipilimumab, and imaging with plainfilms or computed tomography scans may be useful.
For patients in whom intravenous steroids followed by high-doseoral steroid therapy does not lead to initial resolution of symptomswithin 48 to 72 hours, treatment with infliximab at 5 mg/kg once every2 weeks similar to the therapeutic approach for inflammatory boweldisease is an alternative.17 Once relief of symptoms is achieved withinfliximab, which can be rapid and dramatic, it should be discontin-ued, and a prolonged steroid taper over 45 to 60 days should beinstituted. There may be a waxing and waning of the GI adverse effectsof ipilimumab. As steroids are tapered, there can be a recrudescence ofsymptoms, mandating a retapering of steroids starting at a higher doseof 80 or 100 mg, a more prolonged taper, and the use of infliximab.
Rash, pruritisLiver toxicityDiarrhea, colitisHypophysitis
Toxi
city
Gra
de
Time (weeks)
6420 8 10 12 14
Fig 2. Kinetics of appearance of immune-related adverse event.
Management Guidelines for Ipilimumab
www.jco.org © 2012 by American Society of Clinical Oncology 2693Downloaded from jco.ascopubs.org by Kathleen Tulley on June 17, 2013 from 207.138.251.2
Copyright © 2012 American Society of Clinical Oncology. All rights reserved.
Weber JS, et al. ASCO. 2015.
Nivolumab in Melanoma
Skin
0
5
10
15
20
25
30
35
0 10 20 30 40
Approximate proportion of patients (%)
Time (weeks)
GastrointestinalEndocrineHepaticPulmonaryRenal
4

irAEs DistributionGrade 1-2 irAEs
Grade 3-5 irAEs
Michot JM, et al. Eur J Cancer. 2016;54:139-148. Reprinted with permission.
irAEs Distribution Grade 1-‐2 irAEs
Michot JM, et al. Eur J Cancer. 2016.
Grade 3-‐5 irAEs
Michot JM, et al. Eur J Cancer. 2016.
5

Ipilimumab vs Nivolumab vs Combo irAEs Reported in ≥10% of Patients
Patients Reporting Event %
NIVO + IPI (n=313)
NIVO (n=313) IPI (n=311)
Any Grade
Grade 3–4
Any Grade
Grade 3–4
Any Grade
Grade 3–4
Skin 59.1 5.8 41.9 1.6 54.0 2.9
Pruritus 33.2 1.9 18.8 0 35.4 0.3
Rash 28.4 2.9 21.7 0.3 20.9 1.6
Rash maculo-papular
11.8 1.9 4.2 0.3 11.9 0.3
Gastrointestinal 46.3 14.7 19.5 2.2 36.7 11.6
Diarrhea 44.1 9.3 19.2 2.2 33.1 6.1
Colitis 11.8 7.7 1.3 0.6 11.6 8.7
Hepatic 30.0 18.8 6.4 2.6 7.1 1.6
Increase in alanine amino-transferase
17.6 8.3 3.8 1.3 3.9 1.6
Increase in aspartate amino- transferase
15.3 6.1 3.8 1.0 3.5 0.6
Endocrine 30.0 4.8 14.4 0.6 10.9 2.3
Hypothyroidism 15.0 0.3 8.6 0 4.2 0
Wolchok J, et al. Efficacy and safety results from a phase III trial of nivolumab (NIVO) alone or combined with ipilimumab (IPI) versus IPI alone in treatment-naive patients (pts) with ad-vanced melanoma (MEL) (CheckMate 067). Presented at American Society of Clinical Oncology 2015 Annual Meeting; May 29-June 2, 2015; Chicago, IL.
6

Management of Selected irAEs
General Principles
• Responsibility of all health care providers
• Early reporting by patients with close monitoring, and early intervention by health care providers
• Provide thorough and continuous patient education about the signs and symptoms of irAEs
• Assess for signs and symptoms of irAEs before each cycle of immunotherapy
• Know management algorithm specific to each irAE
− Safety profiles of immunosuppressants
• Monitor and manage toxicities of immunosuppressants
− Hyperglycemia and diabetes
− Opportunistic infection
7

CTCAE Severity Grade
Severity CTCAE Grade
Type of Patient Care
Steroids
Other immuno-
suppressive drugs
Immuno- therapy and subsequent approach
1 AmbulatoryNot recommended
Not recommended
Continue
2 Ambulatory
Topical steroids or oral systemic steroids 0.5-1 mg/kg/d
Not recommended
Suspend** temporarily
3 Hospitalization
Systemic steroids (oral or IV) 1-2 mg/kg/d for 3 d then reduce to 1 mg/kg/d
To be considered for patients with unresolved symptoms after 3-5 days of steroid course.Organ specialist advised
Suspend and discuss resumption based on risk/benefit ratio with patient
4
Hospitalization; consider the intensive care unit
Systemic steroids IV methylpred- nisolone 1-2 mg/kg/d for 3 d and then reduce to 1 mg/kg/d
To be considered for patients with unresolved symptoms after 3-5 days of steroid course.Organ specialist advised
Discontinue permanently
**Outside skin or endocrine disorders, where immunotherapy can be maintained.
CTCAE = common terminology criteria for adverse events
Michot JM, et al. Eur J Cancer. 2016;54:139-148.
8

Diarrhea and Colitis
Grade 1 (mild)
<4 bowel actions per day over baseline: supportive measures such as increasing oral fluid and anti-motility agents such as loperamide
Grade 2 (moderate)
4–6 bowel actions per day over baseline: withhold immune checkpoint inhibitor. As per Grade 1 if patient is well. If no improvement in 5 days, or if worsening of symptoms, commence steroids at a dose of 0.5–1 mg/kg per day of prednisolone (or IV equivalent) and continue until symptoms improve to Grade 1. If no improvement occurs, manage as per Grade 3. Steroids can be tapered over 2–4 weeks. Sigmoidoscopy and biopsy can be considered and may assist in determining the duration of steroid taper based on the macroscopic and microscopic inflammation evident
Grade 3 (severe)
>7 bowel actions per day over baseline: admit patient to hospital for intravenous hydration and clinical observation as appropriate. Commence steroids at 1–2 mg/kg prednisolone or IV equivalent. If no improvement in 2–3 days, commence infliximab 5 mg/kg and continue steroids. Infliximab is contraindicated in patients with sepsis or a perforation. Sigmoidoscopy and biopsy recommended to exclude other causes. Once symptoms resolve to Grade 1, taper steroids over a minimum of 1 month (up to 3 months for severe cases). Infliximab may be re-administered at 2 and 6 weeks if symptoms persist or recur. Dietitian input recommended
Grade 4 (life threatening)
Urgent intervention indicated: management as per Grade 3. Involve gastroenterologist and surgeon in management. Permanently discontinue immune checkpoint inhibitor
Spain L, et al. Cancer Treat Rev. 2016;44:51-60. Reprinted with permission.
9

Hepatitis
Grade 1 (mild)
ALT/AST up to 3 times ULN: continue immune checkpoint inhibitor. Send viral serology looking for hepatitis A, B, C, and CMV and iron studies to look for underlying haemochromatosis. Advise against excessive alcohol intake
Grade 2 (moderate)
3 to 5 times ULN: withhold immune checkpoint inhibitor. Product information (Ipi, Nivo, Pembro) recommends initiation of steroids with prednisolone 1–2 mg/kg/day or IV equivalent. If patient is well, it is reasonable to re-check liver function every 2 days and initiate steroids if no improvement or worsening. Taper steroids over 4 weeks once liver function is at Grade 1 or at baseline
Grade 3 (severe)
5 to 20 times ULN: as per Grade 2 except that steroids should be initiated immediately. Ipilimumab should be permanently discontinued. Consider permanent discontinuation of anti-PD-1 drugs
Grade 4 (life threatening)
>20 times ULN: as per Grade 3. Permanently discontinue immune checkpoint inhibitor
Spain L, et al. Cancer Treat Rev. 2016;44:51-60.
Rash
Grade 1 (mild)
<10% BSA: symptomatic management with antihistamines for pruritus and topical steroid cream for localized pruritus and rash; continue immune checkpoint inhibitor if responding or stable
Grade 2 (moderate)
0–30% BSA: if tolerable, as per Grade 1; if intolerable, initiate systemic steroids (eg, oral prednisolone 0.5–1 mg/kg daily with a 1–2 week wean) and delay treatment until Grade 1 and steroids <10 mg. If symptoms persist or recur, consider skin biopsy and withholding drug
Grade 3 (severe)
>30% BSA: obtain a skin biopsy and dermatology consult. Initiate systemic steroids with 1 mg/kg of prednisolone or IV equivalent, with a 4 week taper. Withhold treatment until Grade 1
Grade 4 (life threatening)
No formal definition. Management as per Grade 3. Permanently discontinue immune checkpoint inhibitor
Spain L, et al. Cancer Treat Rev. 2016;44:51-60. 10

Pneumonitis
Grade 1 (mild)
Asymptomatic; clinical or diagnostic observations; no intervention needed: delay drug administration. Consider steroids (eg, prednisone 1 mg/kg/day PO or methylprednisolone 1 mg/kg/day IV). Follow-up: reassess management after 3 weeks. If completely resolved or non-drug related, continue treatment. If worsens, treat as Grade 2 or 3/4
Grade 2 (moderate)
Symptomatic; medical intervention indicated; limits instrumental activities of daily living (ADLs): delay drug administration. Consider hospitalization and daily monitoring of symptoms. Steroids recommended (eg, prednisone 1–2 mg/kg/day PO or methylprednisolone 1–2 mg/kg/day IV). Consider empiric antibiotics (if suspicious for concurrent infection). Follow-up: reassess management every 1–3 days. If improving, taper steroids and continue treatment if symptoms resolve completely. If worsens, treat as Grade 3/4
Grade 3 (severe)
Limits self-care ADLs; oxygen indicated: discontinue drug administration. Hospitalization. High dose steroids with methylprednisolone (eg, 1 g/day IV). Add prophylactic antibiotics for opportunistic infections. Consider bronchoscopy with biopsy. Reassess management daily. If not improving after 48 h or worsening, administer additional immunosuppressive therapy (eg, infliximab, mycophenolate, immunoglobulins). If improving, taper steroids. Discontinue treatment permanently
Grade 4 (life threatening)
Urgent intervention indicated (eg, intubation): as per Grade 3. Intensive care support required
Spain L, et al. Cancer Treat Rev. 2016;44:51-60.
11

Thyroid DysfunctionGrade 1 (mild)
Asymptomatic, no intervention needed: monitor only
Grade 2 (moderate)
Symptomatic or intervention indicated: for hypothyroidism, commence levothyroxine. For hyperthyroidism, seek endocrinology input and start propranolol or atenolol for symptoms; steroids or carbimazole may be indicated pending underlying mechanism
Grade 3 (severe)
As per Grade 2: Hospitalization and specialist input are recommended. Initiate prednisolone 1–2 mg/kg or IV equivalent
Grade 4 (life threatening)
As per Grade 3
Spain L, et al. Cancer Treat Rev. 2016;44:51-60.
Nephritis
Grade 1 (mild)
Creatinine >1–1.5 x baseline; proteinuria 1+, <1.0g/24 h: monitor renal function, promote hydration and cessation of nephrotoxic drugs
Grade 2 (moderate)
Creatinine >1.5–3.0 x baseline; proteinuria 2+, 1.0–3.4 g/24 h: exclude non-immune causes, commence prednisolone 0.5–1 mg/kg. If worsens, manage as per Grade 3 and discontinue immune checkpoint inhibitor
Grade 3 (severe)
Creatinine >3.0 x baseline; ≥3.5 g/24 h: initiate prednisolone 1–2 mg/kg or IV equivalent. Consider renal biopsy. Discontinue immune checkpoint inhibitor
Grade 4 (life threatening)
Creatinine >6.0 x ULN: as per Grade 3
Spain L, et al. Cancer Treat Rev. 2016;44:51-60.
12

Hypophysitis
• Discontinue immune checkpoint inhibitor
• High-dose corticosteroid administration with a taper over 4 weeks
• Obtain endocrine consult
• Replace deficient hormones
• Symptoms will resolve with treatment
• Slow return of some endocrine function
• Most patients require life-long hydrocortisone supplement
• Use stress dose hydrocortisone in perioperative period and critical illness
Postow M. ASCO Educational Book. 2015:76-83; Fecher LA, et al. Oncologist. 2013;18:733-743.
13

Neurological Toxicities
• Relatively infrequent (<1% all grades) with IPI or PD-1
• Symptoms:
− Numbness, tingling, foot drop and localized muscle weakness, or generalized ascending motor and diaphragmatic weakness
• Observed so far:
− Myasthenia gravis (MG)-like syndrome
− Peripheral neuropathy
• Management: get a neurology consult!
− For Grade 2 or more, discontinue antibodies, work-up including labs and brain MRI, high dose corticosteroid administration with a prolonged taper, neurology consultation, and EMG, if appropriate
− Hospitalize if MG-like syndrome
− Consider rapidly moving to IVIG and infliximab if Grades 3-4 and without resolution of symptoms within 24-48 hours
Postow M. ASCO Educational Book. 2015:76-83; Fecher LA, et al. Oncologist. 2013;18:733-743.
14
Patient and Caregiver Education
Evaluate Education Needs
• Assess both patient and caregiver
− Knowledge of therapy and the disease process
− Educational level and preferred learning methods
• Develop a plan
• Implement teaching, using a variety of materials and methods
• Evaluate patient and caregiver for continued educational needs related to the therapy and disease process
15
Educate
• Describe signs and symptoms, including complications if not treated promptly
• Emphasize early recognition and prompt reporting of worsening condition
• Discuss preventative measures, if applicable
• Instruct patient to present agent-specific wallet card to all healthcare providers
• Stress compliance with corticosteroid therapy
• Provide supportive care instructions
• Explain that benefits of therapy outweigh potential risks, particularly when irAEs are recognized early and treated quickly
Provide Contact Information
• Whom to call
• Why to call
• When to call
• Where to call (MUST HAVE 24/7 clinician
availability)
16

When to Call the Sub-Specialist
Skin
Grades 1-2 No, manage the symptoms
Grades 3-4 Yes, consider a biopsy
GI
Grades 1-2 Only if scoping changes the management
Grades 3-4 Only if therapy-refractory, or Grade 4
Hepatic
Grades 1-2 No
Grades 3-4 Only if therapy-refractory, or Grade 4
Endocrine
Grades 1-2 Yes, if symptomatic
Grades 3-4 Yes, always
17
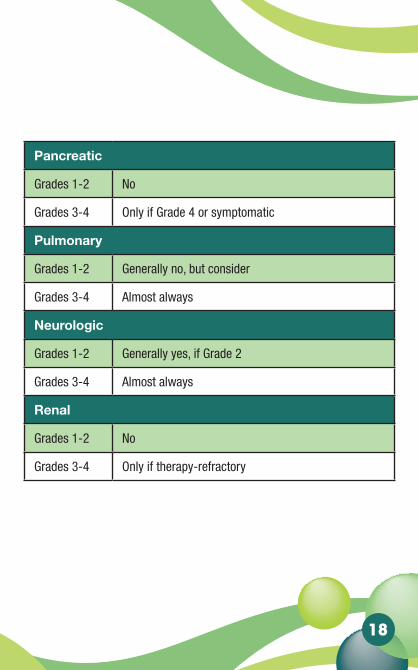
When to Call the Sub-Specialist
Skin
Grades 1-2 No, manage the symptoms
Grades 3-4 Yes, consider a biopsy
GI
Grades 1-2 Only if scoping changes the management
Grades 3-4 Only if therapy-refractory, or Grade 4
Hepatic
Grades 1-2 No
Grades 3-4 Only if therapy-refractory, or Grade 4
Endocrine
Grades 1-2 Yes, if symptomatic
Grades 3-4 Yes, always
Pancreatic
Grades 1-2 No
Grades 3-4 Only if Grade 4 or symptomatic
Pulmonary
Grades 1-2 Generally no, but consider
Grades 3-4 Almost always
Neurologic
Grades 1-2 Generally yes, if Grade 2
Grades 3-4 Almost always
Renal
Grades 1-2 No
Grades 3-4 Only if therapy-refractory
18

Creative Educational Concepts, Inc.1792 Alysheba Way, Suite 100
Lexington, KY 40509859-260-1717 • Toll-Free 866-360-1717 • Fax 859-276-6118
www.ceconcepts.com
© March 2016. CEC. All rights reserved.