candidacidal activity of crohn's disease neutrophils
TRANSCRIPT

Gut, 1991, 32, 55-605
Candidacidal activity of Crohn's disease neutrophils
F T Curran, D J Youngs, R N Allan, M R B Keighley
AbstractThe ability of normal and Crohn's diseaseneutrophils to kill Candida albicans has beenstudied using neutrophils isolated fromperipheral blood and suspended in phosphatebuffered saline at 5x 106 cells per ml. C albicanswas grown to a stationary phase in brothculture and suspended in phosphate bufferedsaline at 107 organisms/ml. Neutrophils andCandida were then incubated together at 37°Cin a shaking water bath in the presence of freshserum. At 30 and 60 minutes samples werewithdrawn, neutrophils lysed, and Candidasurvival assessed by colony counting. Resultswere compared with control suspensions ofCandida incubated with serum alone. After 30and 60 minutes in the presence of autologousserum normal neutrophils had killed signific-andy more Candida than Crohn's diseaseneutrophils (mean (SD) 61-0 (16.7)% v 40 5(16-2)% at 30 minutes, p<00001; 83*2 (7)% v70-8 )16)% at 60 minutes, p<0005). Theresults did not alter significantly when nonnalneutrophils were incubated with Candida inthe presence of Crohn's disease serum insteadof normal serum. When Crohn's diseaseneutrophils were incubated with Candida inthe presence of normal serum instead of auto-logous serum there was some improvement incandidacidal ability at 30 minutes (48.9 (20.6)%v 40 5 (16.2)%, p<003) but not at 60 minutes.Phagocytosis, measured using a radiometricassay, was normal. Neutrophils from patientswith Crohn's disease have an impaired abilityto kill this granuloma provoking organism. It isnot due to serum inhibitors or defectivephagocytosis.
Departments of Surgeryand Gastroenterology,The General Hospital,BirminghamF T CurranD J YoungsRNAllanM R B KeighleyCorrespondence to:Mr F T Curran, QueenElizabeth Hospital,Edgbaston, Birmingham B 15.
Accepted for publication19 March 1990
The inactivation of invading micro-organisms isthe most important function of the neutrophil.Although various abnormalities of neutrophilfunction have been reported in Crohn's disease,'their capacity to kill granuloma provokingorganisms has not been evaluated.
This study was designed to investigate theability of Crohn's disease neutrophils to killCandida albicans. The organism was chosen forstudy because it is present in the gastrointestinaltract of 14-47% of the healthy population2 3 andcauses chronic inflammatory diseases, such aschronic mucocutaneous candidiasis, and leadsto granuloma formation.3 It may also causeenteritis4 and allergic colitis.56 It is a convenientorganism to culture compared to other organismsresponsible for causing chronic inflammatoryconditions. Whereas C albicans can be culturedin two to three days, mycobacteria, for example,require four to 12 weeks. It is a relatively safeorganism to handle and is the species mostresistant to killing by neutrophils.7
Phagocytosis was studied using a sensitive
radiometric assay to determine whether impair-ment of candidacidal activity could be a result ofthis.
Methods
PREPARATION OF ORGANISMSC albicans from the same source were used in allexperiments. The organisms were isolated fromthe faeces of a healthy woman who was taking nodrugs. The organism was maintained in stockculture on a slope of malt extract agar (Oxoid) atroom temperature. When required, a sample ofthe organisms was inoculated into approximately50 ml Sabouraud liquid medium (Oxoid) andgrown to a stationary phase for three to five daysat 30°C. The organisms were washed twice inDulbecco's B phosphate buffered saline (PBS),centrifuged at 1500 g for 10 minutes after eachwash, counted in an improved Neubauerhaemocytometer, and suspended in PBS at aconcentration of 107 organisms per ml. Freshlycultured organisms were used in all tests.
PREPARATION OF NEUTROPHILSNeutrophils were isolated from fresh venousblood using discontinuous density gradients ofPercoll (Pharmacia) as follows. An iso-osmoticstock solution of Percoll was made by adding 1part 1-5 M saline to 9 parts Percoll (resultingdensity 1-123 g/ml). Stock Percoll was furtherdiluted with 0 15 M saline to densities of 1-070 g/ml' and 1-097 g/ml9 for the separation of whitecells. In a sterile universal container was placed6 ml Percoll of density 1-097 g/ml, then 4 mlPercoll of density 1 070 g/ml was carefullylayered on top avoiding mixing at the interphase.
Five ml heparinised blood was diluted with anequal volume of 0 15 M saline and carefullylayered on top of the Percoll in the same way.The tube was centrifuged at 200g for 25 minutes,to ensure isopycnic banding of cells at therelevant interphases; granulocytes were sus-pended between the two layers of Percoll. Theywere removed with a pipette and washed twice inPBS and centrifuged at 1500 g for 10 minutesafter each wash. Any contaminating erythrocyteswere lysed by hypotonic shock treatment byresuspending the cells in tris-ammoniumchloride for 10 minutes before the second wash.Neutrophils were counted in an improvedNeubauer chamber and resuspended in PBS atconcentrations of 5 x 106 cells per ml. All neutro-phil suspensions were at least 95% pure andviability, assessed by trypan blue exclusiontests,7 was 98%.
CANDIDACIDAL ASSAYThe study was performed in two parts using
55

Curran, Youngs, Allan, Keighley
TABLE I Subject data - candidacidal assay
Healthy subjects Crohn's disease
Autologous serum:No 20 30Mean (SD) age (years) 47 (18) 45 (16)Sex 13M,7F 10M,20FDisease activity - Quiescent 19
Active 11No taking steroid treatment - 4'Crossed' serum:No 15 25Mean (SD) age (years) 45 (18) 49 (14)Sex 8M,7F 8M, 17FDisease activity - Quiescent 15
Active 10No taking steroid treatment - 4Phagocytosis assay:No 20 20Mean (SD) age (years) 40 (15) 38 (13)Sex 9M, 11 F 14M,6FDisease activity - Quiescent 12
Active 8No taking steroid treatment 1
fresh serum, either autologous or 'crossed' - thatis, normal neutrophils with Crohn's diseaseserum and vice versa. With autologous serum, 20healthy subjects and 30 patients with Crohn'sdisease were studied; with crossed serum therewere 15 and 25 respectively. Details of subjectsare summarised in Table I. Four patients were
taking steroids; none was taking sulphasalazine.Crohn's disease activity was assessed using themethod of Harvey and Bradshaw."'A 0-5 ml neutrophil suspension, 0-25 ml C
albicans, and 0-25 ml fresh serum were broughtto 37°C and mixed in a stoppered polystyrene testtube. Tubes were laid on their sides in a shakingwater bath at 37°C so that the contents flowedcontinually from one end of the tube to the otherduring each cycle. A control tube containingC albicans, fresh serum, and 0-5 ml PBS insteadof neutrophils was included in each test.At time 0 (immediately after mixing) a 10 ,ul
aliquot was withdrawn from the control tube foran initial colony count, so that the exact numberof viable organisms used in each test was known.Two time points were included for each assay.
At 30 and 60 minutes 10 1t aliquots were
Figure 1: Candida albicans on agar plates after 3 days' incubation: 1. At time 0; 2. After 30minutes with normal neutrophils; 3. After 60 minutes with normal neutrophils; 4. After 30minutes with Crohn's neutrophils; 5. After 60 minutes with Crohn's neutrophils.
withdrawn from each tube (control, normal, andCrohn's disease) and allowed to stand for at least10 minutes in 10 ml sterile distilled water to lyseneutrophils and release ingested organisms. Thistime was adequate to lyse all neutrophils, whichwas confirmed microscopically on severaloccasions - after centrifuging the water noneutrophils could be identified in the deposit.Each aliquot was serially diluted to 1x 104 andlx 105 of the initial concentration using steriledistilled water and sterile glass containers. Oneml ofboth the 104 and 105 dilutions was spread onmalt extract agar and incubated at 30°C for two tothree days. The number of colonies ofC albicanson the plates (Fig 1) was counted using anilluminated colony counter. The 104 dilutionplate was normally counted but if the number ofcolonies was excessive the 105 dilution plate wasused instead. Any 105 plate used contained atleast 15 colonies.The percentage killing was calculated using
the formula:
% of yeast killed=
1(No of colonies at 30 or 60 minutes)x 100
\0o~~( (No ofcolonies at time 0)The percentage of Candida remaining on controlplates at 30 and 60 minutes was also calculated toensure that neither normal nor Crohn's diseaseserum alone had candidacidal activity, using theformula:% candida remaining on control plate=(No of 'control' colonies at 30 or 60 minutes)
x(No of colonies at time 0)
:100
INTERASSAY VARIABILITYThree assays were performed in triplicate on
different days. The numbers of Candida colonieson each plate are given in Table II. The variance,calculated using the formula:
standard deviationvariance=- x 100,
meanwas 9 5% at 30 minutes and 114% at 60 minutes.
PHAGOCYTOSIS ASSAYTwenty healthy subjects and 20 patients withCrohn's disease were studied. Details are sum-marised in Table I. Neutrophils were suspendedat 8x 10' cells/ml PBS and C albicans at 4x 106organisms/ml PBS, a Candida:neutrophil ratio of5:1. A 0 5 ml neutrophil suspension, 0 5 mlCandida suspension, and 50 ,ul autologous
TABLE II Interassay variability
No ofCandida colonies
30 minutes 60 minutes
Assay 1 71 5180 5173 47
Assay 2 44 3040 2752 32
Assay 3 71 2769 1960 19
56
Candidacidal activity ofCrohn's disease neutrophils
serum were incubated at 37°C in a shaking waterbath. The tubes were laid on their sides so thatthe contents continually flowed from one end ofthe tube to the other during each cycle. Allexperiments were performed in duplicate and acontrol tube containing 0 5 ml PBS instead ofneutrophils was included in each assay. Duringthis incubation Candida were phagocytosed byneutrophils.
After incubation 0-2 ml aliquots were with-drawn from each tube, tests, and controls, andtransferred into microtitre wells containing 3-6R1 [5,6-3H] uridine (specific activity 46 Ci/mmol,Amersham International) made up to 20 >d withPBS. The microtitre plate was incubated at 37°Cfor one hour. During this time Candida whichhad not been phagocytosed incorporated 3H-uridine.
After the second incubation 0- 1 ml aliquotswere withdrawn from each microtitre well aftermixing and transferred to aWhatman GF-B filter(pore size 1 rim) prewetted with PBS. Each filterwas washed with approximately 8 ml steriledistilled water under suction from a stream ofwater to remove free radioactivity, so as to leaveonly Candida-associated radioactivity on thefilter. To confirm that the wash was sufficient toremove all free radioactivity, 3H-uridine wasplaced on four filters and washed precisely asdescribed; only background radioactivity couldbe detected on them.The filters were dried overnight, placed in
scintillation fluid, and the radioactivity counted.To check that no Candida passed through thefilter the filtrate was centrifuged and the pelletexamined under a microscope; it contained a fewfragments of glass fibre from the filter but noorganisms.The mean number of Candida phagocytosed
per neutrophil (the phagocytic index), was calcu-lated using the following formula:
Phagocytic index=
1- (dpm for Candida+neutrophils) x(dpm for Candida alone)
100-
90.
80-
70.._
( 6a
50
30-
20-
10I
n
p < 005
p<0-03,
O
NS
p < 0-0001 p < 0-005| wr--~~~~~
00
3.
3 0
10 I
* 0
,
*.0
0;
0.
.0
0
.0
0
*3o
*0
Normal cells Crohn's cells Normal cells Crohn's cellsNormal serum Crohn's serum Crohn's serum Normal serum(n = 20) (n = 30) (n = 1 5) (n = 25)
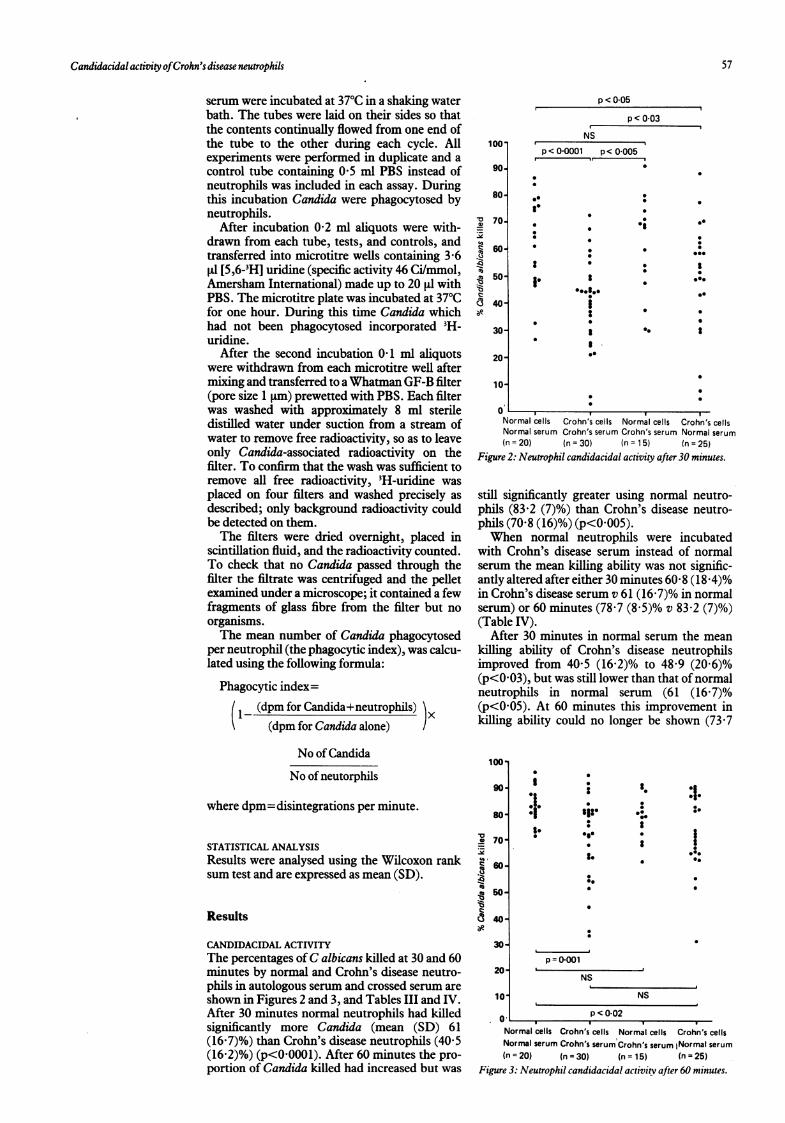
Figure 2: Neutrophil candidacidal activity after 30 minutes.
still significantly greater using normal neutro-phils (83-2 (7)%) than Crohn's disease neutro-phils (70-8 (16)%) (p<0 005).When normal neutrophils were incubated
with Crohn's disease serum instead of normalserum the mean killing ability was not signific-antly altered after either 30 minutes 60 8 (18 4)%in Crohn's disease serum v 61 (16-7)% in normalserum) or 60 minutes (78-7 (8 5)% v 83-2 (7)%)(Table IV).
After 30 minutes in normal serum the meankilling ability of Crohn's disease neutrophilsimproved from 405 (16-2)% to 48-9 (20 6)%(p<003), but was still lower than that of normalneutrophils in normal serum (61 (16-7)%(p<0O05). At 60 minutes this improvement inkilling ability could no longer be shown (73-7
No of Candida
No of neutorphils
where dpm=disintegrations per minute.
STATISTICAL ANALYSISResults were analysed using the Wilcoxon ranksum test and are expressed as mean (SD).
Results
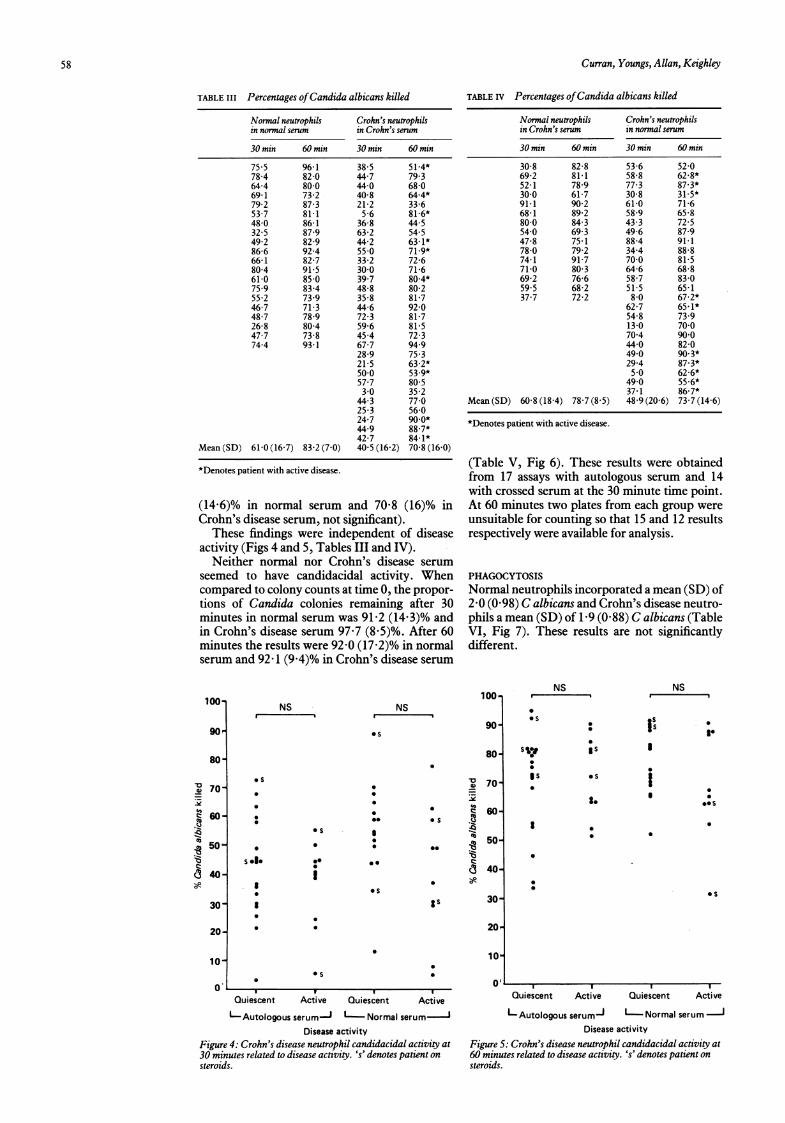
CANDIDACIDAL ACTIVITYThe percentages ofC albicans killed at 30 and 60minutes by normal and Crohn's disease neutro-phils in autologous serum and crossed serum areshown in Figures 2 and 3, and Tables III and IV.After 30 minutes normal neutrophils had killedsignificantly more Candida (mean (SD) 61(16-7)%) than Crohn's disease neutrophils (40 5(16-2)%) (p<0 0001). After 60 minutes the pro-portion of Candida killed had increased but was
100o
90-
80~
70-
, 60-
-C 50-
c3 40-
30-
20-
1.
I
si:0*0
S.
p=0.001
NS. .~~~~~~~~~~~~~~~~~~~~~~~~~~~
0
:1.:0
I0000.
10, NS
0 p<0-02Normal cells Crohn's cells Normal cells Crohn's cellsNormal serum Crohn's serum Crohn's serum iNormal serum(n = 20) (n = 30) (n = 15) (n = 25)
Figure 3: Neutrophil candidacidal activity after 60 minutes.
57
Curran, Youngs, Allan, Keighley
TABLE III Percentages ofCandida albicans killed
Normal neutrophils Crohn's neutrophilsin normal serum in Crohn's serum
30 min 60 min 30 min 60 min
75-5 96-1 38 5 51-4*78-4 82-0 44-7 79.364-4 80-0 44-0 68-069-1 73-2 40-8 64-4*79-2 87-3 21-2 33-6537 81-1 56 81*6*48-0 86-1 36-8 44 532 5 87-9 63-2 54-549-2 82-9 44-2 63- 1*86-6 92-4 550 71-9*66-1 82-7 33-2 72-680-4 91-5 30 0 71-661-0 850 39-7 80-4*75 9 83-4 48-8 80-255 2 739 35 8 81-746-7 71-3 44-6 92-048-7 78-9 72-3 81-726-8 80-4 59 6 81-547-7 73-8 45-4 72-374-4 93-1 67-7 949
28-9 75 321-5 63-2*50 0 53.9*57-7 80-530 35 2
44-3 77025 3 56 024-7 90.0*44 9 88-7*42-7 84- 1*
Mean (SD) 61-0 (16-7) 83-2 (7 0) 40 5 (16-2) 70-8 (16-0)
*Denotes patient with active disease.
(14-6)% in normal serum and 70-8 (16)% inCrohn's disease serum, not significant).
These findings were independent of diseaseactivity (Figs 4 and 5, Tables III and IV).
Neither normal nor Crohn's disease serumseemed to have candidacidal activity. Whencompared to colony counts at time 0, the propor-tions of Candida colonies remaining after 30minutes in normal serum was 91[2 (14"3)% andin Crohn's disease serum 97"7 (8-5)%. After 60minutes the results were 92-0 (17-2)% in normalserum and 92-1 (9 4)% in Crohn's disease serum
TABLE IV Percentages ofCandida albicans killed
Normal neutrophils Crohn's neutrophilsin Crohn's serum in normal serum
30 min 60 min 30 min 60 min
30-8 82-8 53-6 52-069-2 81-1 58-8 62-8*52-1 78-9 77-3 87-3*30 0 61-7 30-8 31-5*91*1 90 2 61-0 71-668-1 89-2 58-9 65-880-0 84-3 43-3 72 554-0 69-3 49-6 87-947-8 75 1 88-4 91.178-0 79-2 34-4 88-874-1 91-7 70 0 81-571-0 80-3 64-6 68-869-2 76-6 58 7 83-0595 68-2 51-5 65-137-7 72-2 8-0 67-2*
62-7 65-1*54-8 73 913-0 700704 900440 82-049 0 90.3*29-4 87-3*5 0 62-6*490 55.6*37-1 86-7*
Mean (SD) 60-8 (18-4) 78-7 (8 5) 48-9 (20 6) 73-7 (14-6)
*Denotes patient with active disease.
(Table V, Fig 6). These results were obtainedfrom 17 assays with autologous serum and 14with crossed serum at the 30 minute time point.At 60 minutes two plates from each group wereunsuitable for counting so that 15 and 12 resultsrespectively were available for analysis.
PHAGOCYTOSISNormal neutrophils incorporated a mean (SD) of2 0 (0 98) C albicans and Crohn's disease neutro-phils a mean (SD) of 1-9 (0-88) C albicans (TableVI, Fig 7). These results are not significantlydifferent.
NSI.
100oNS
*s90
80-
* s
0
sea.
0 S
*e
i
.- s
**-
*s
Ss
570-._
C 60-
.a350-:M
CZ(3 40-
30'
20r
10'
* S
NS
0
Os
S
as
NSI sIs
asa.
*. 1
9_ I*SO
I
*S
u I I I I
Quiescent Active Quiescent Active
L-Autologous serum-1 I Normal serum
Disease activityFigure 4: Crohn's disease neutrophil candidacidal activity at30 minutes related to disease activity. 's' denotes patient onsteroids.
Quiescent Active Quiescent Active
Autologous serumj Normal serum 1Disease activity
Figure 5: Crohn's disease neutrophil candidacidal activity at60 minutes related to disease activity. 's' denotes patient onsteroids.
100-
90
.0 70-ye
c 60-
(50
c3 40-o1-
30"
20-
10-
O'
58
.

Candidacidal activity ofCrohn's disease neutrophils
TABLE V Candidacidal activity ofserum
Normal serum Crohn's serum
30 min 60 min 30 min 60 min
84-1 76-4 108-0 88-470 0 78-0 96-9 90 076-8 56-4 94 7 105-395 5 67-7 96-7 100-896-9 94-2 107-1 107-183 2 87-4 962 97 7100-0 97-2 87-7 859975 111-6 95 1 91*3119-6 107-7 87-1 91.098 5 1100 91-3 90-495 3 83-0 100 0 84-1101-2 101-7 89-9 73 578-8 91-3 99-1 NA100-0 100-4 117-8 NA104-2 116-588-3 NA60-1 NA
Mean (SD) 91-2 (14-3) 97 7 (8 5) 92-0 (17-2) 92-1 (9 4)
NA=Not available.
TABLE VI Phagocytic index
Normal Crohn's disease
2 5 1.11-5 1-01-8 1-31-7 1-41-4 1-22-0 2-42-7 1.92-5 2-31-8 2-23.5 1-30-8 3-307 2-61-6 3-204 3-707 032-3 1 53-9 2-82-3 1-52-7 1-93.5 1-3
Mean (SD) 2-0 (0 98) 1-9 (0-88)
DiscussionTwo previous studies have investigated micro-bicidal activity in Crohn's disease with con-flicting results. Lamster et all' reported onepatient whose neutrophils showed an enhancedability to phagocytose and lyse Escherichia colicompared to a single control subject. Worsaae etall2 investigated nine patients and found an'increased intracellular survival' of Staphylo-coccus aureus in Crohn's disease neutrophils. Theimportance of this finding is uncertain sincestaphylococci do not form granulomas andpatients with Crohn's disease are not unusuallysusceptible to bacterial infections.
Lehrer and Cline'3 first showed in vitro thephagocytosis and killing of C albicans by humanneutrophils and monocytes. The process israpid; more than 90% of C albicans injected intothe bloodstream of rabbits is removed within 10minutes'4 and more than 70% is removed withinfive minutes from the blood stream of rats.'5 Theyeast are killed intracellularly by the phagocyteperoxide/myeloperoxidase system'""' and a non-oxidative fungicidal mechanism. 1618 There are noreports of candidacidal activity in patients withinflammatory bowel disease, but neutrophilmyeloperoxidase is probably normal in Crohn'sdisease. '9A Candida/neutrophil ratio of 1: 1 was used in
120
o 110-
.* 100-0
a 90-
a
E0c 80-
-M70--16
60
the assay, as recommended by Babior andCohen,7 since the number of Candida presentedto neutrophils and the number killed is linear upto a ratio of 5:1.20These results suggest that neutrophils from
patients with Crohn's disease have a significantlyimpaired candidacidal activity in vitro, even inquiescent disease, implying that patients withCrohn's disease are less able to inactivateorganisms which can cause chronic inflamma-tory diseases. The results are not due to a seruminhibitor since adding Crohn's disease serum towashed normal neutrophils did not impair theircandidacidal activity. The temporary improve-ment in killing by Crohn's disease neutrophils inthe presence of normal serum at 30 minutes butnot at 60 minutes may suggest some replenish-ment of a deficient plasma factor important forkilling. If it was due to poor opsonisation theimprovement should have been sustained andCrohn's disease serum should have impaired thecandidacidal activity of normal neutrophils.
Phagocytosis was studied because any impair-ment in opsonisation or the ability of Crohn's
4-0.
3.5
30-
t
S
*. 0
*.
x
& 2-5.._
.2
4-
15-
1*0-
u I I I
Normal Crohn's disease Normal Crohn's diseaseserum serum serum serum(n= 17) (n 14) (n= 15) (n=12)
30 minuus 60 mienuasFigure 6: Candidacidal activity ofnormnal and Crohn'sdisease serum.
0 5-
.
00
0
*0
000*0-
:000000
0
S
0*
S.
0*000
000
0
NS
r h diNormal Crohn's disease(n - 20) (n = 20)
.Figure 7: Neutrophil phagocytosis ofCandida albicans.
59
40
0
i
.

60 Curran, Youngs, Allan, Keighley
disease neutrophils to phagocytose would resultin impaired killing ability. A radiometric assaywas used,20"2 based on the observations that theuptake of 3H-uridine by Candida is an index ofphagocytic function, that there is linear correla-tion between uridine incorporation and yeastnumbers, and that neutrophils do not take upuridine in short term cultures so that candidawithin neutrophils have no access to uridine.2'The assay is one of the best available for measur-ing phagocytosis and opsonisation,2223 and noabnormality was found.
There was no evidence that normal or Crohn'sdisease serum alone had candidacidal activity, amean of 92% of C albicans remaining after onehour. This confirms the findings of Wilkinson,24who reported that less than 10% of organismsshould be dead after one hour. Some counts weregreater than 100%, presumably because Candidacontinued to multiply during the assay - serumat 37°C is a good stimulant ofCandida germ tubeformation.2526 A few counts in normal serumwere quite low at 30 and 60 minutes, due eitherto a sampling error or to the presence in serum ofantibodies to Candida which result from thehost's immune response to infection. There is nogood published evidence for true fungistasis ofC albicans by serum.3Many factors can affect neutrophil function
and in patients with Crohn's disease malnutri-tion is an important consideration. We, how-ever, found similar results in patients withquiescent and active disease and know ofno datasuggesting that patients in a quiescent phase oftheir disease are malnourished. Hill et al foundthat malnutrition was unlikely to be presentwhen patients with inflammatory bowel diseasewere in remission or during the early stages ofanacute attack.27 Deficiency of micronutrients,such as iron, necessary for normal neutrophilfunction is unlikely to have caused the impairedkilling since iron is an essential growth factor forC albicans. Iron deficiency offers a competitiveadvantage to the host rather than the organismbecause iron binding to transferrin and lacto-ferrin renders the level of free ionic iron toolow for microbial growth.28 9 The growth ofC albicans in human serum is direcdly related tothe percentage of iron saturation30 and irondeficiency increases resistance to C albicans invivo.3' If our patients were iron deficient thekilling of Candida would have been greater thanthat in normal subjects.An unexplained finding is that some patients
had normal neutrophil candidacidal activity, asshown by the overlapping results in Figures 2and 3. The reason is not clear but the resultsimply that the defect is either intermittent oroccurs only in certain patients, but these werenot necessarily patients with quiescent disease orthose on a particular treatment.
Neutrophils from many patients with Crohn'sdisease have an impaired ability to killC albtcans,an organism known to cause chronic inflamma-tory diseases. There was no evidence of a seruminhibitor, defective opsonisation, or impaired
phagocytosis, and a cellular defect is the mostlikely explanation. Further work is needed todetermine the reason for these findings andwhether they are disease specific.1 Hermanowicz A, Gibson PR, Jewell DP. The role of phago-
cytes in inflammatory bowel disease. Clin Sci 1985; 69:241-9.
2 Finegold SM, Sutter VL, Mathisen GE. Human intestinalmicroflora in health and disease. London: Academic Press,1983.
3 Odds FC. Candida and candidosis. 2nd ed. London: BailliereTindall, 1988.
4 Kozinn PJ, Taschdjian CL. Enteric candidiasis: diagnosis andclinical considerations. Pediatrics 1962; 30: 71-85.
5 Alexander JG. Allergy in the gastrointestinal tract. Lancet1975; ii: 1264.
6 Holti G. Candida allergy. In: Winner HI, Hurley R, eds.Symposium on candida infections. London: Livingstone,1966: 73-81.
7 Babior BM, Cohen HJ. Measurement of neutrophil function.In: Cline MJ, ed. Leukocyte function. London: ChurchillLivingstone, 1981: 1-38.
8 Giddings JC, Piovella F, Ricetti M, Jarvis A, Peake IR, BloomAL. Characterization of procoagulant activity produced bycultures ofhuman monocytes and lymphocytes separated incolloidal silica-polyvinyl-pyrrolidone gradients. Clin LabHaematol 1980; 2: 121-8.
9 Jepsen LV, Skottun T. A rapid one-step method for theisolation of human granulocytes from whole blood. ScandJClin Lab Invest 1982; 42: 235-8.
10 Harvey RF, Bradshaw JM. A simple index of Crohn's-diseaseactivity. Lancet 1980; i: 514.
11 Lamster I, Sonis S, Hannigan A, Kolodkin A. An associationbetween Crohn's disease, periodontal disease and enhancedneutrophil function.J Periodontol 1978; 49: 475-9.
12 Worsaae N, Staehr Johansen K, Christensen KC. Impaired invitro function of neutrophils in Crohn's disease. Scand JGastroenterol 1982; 17: 91-6.
13 Lehrer RI, Cline MJ. Interaction of Candida albicans withhuman leukocytes and serum. J Bacteriol 1969; 98: 996-1004.
14 Baine WB, Koenig MG, Goodman JS. Clearance of Candidaalbicans from the bloodstream ofrabbits. InfectImmun 1974;10:1420-5.
15 Jeunet FS, Meuwissen HJ, Good RA. Fate ofCandida albicansin neonatally thymectomized rats. Proc Soc Exp Biol Med1970; 133: 53-6.
16 Brune K, Schmid L, Glatt M, Minder B. Correlation betweenantimicrobial activity and peroxidase content of leukocytes.Nature 1973; 245: 209-10.
17 Klebanoff SJ. Myeloperoxidase: contribution to the micro-bicidal activity of intact leukocytes. Science 1970; 169:1095-7.
18 Lehrer RI. Measurement of candidacidal activity of specificleukocyte types in mixed cell populations. I. Normal,myeloperoxidase-deficient, and chronic granulomatousdisease neutrophils. InfectImmun 1970; 2: 42-7.
19 Renz M, Ward M, Eastwood MA, Harkness RA. Neutrophilfunction and myeloperoxidase activity in inflammatorybowel disease. Lancet 1976; ii: 584.
20 Bridges CG, Dasilva GL, Yamamura M, Valdimarsson H. Aradiometric assay for the combined measurement of phago-cytosis and intracellular killing ofCandida albicans. Clin ExpImmunol 1980; 42: 226-33.
21 Yamamura M, Boler J, Valdimarsson H. Phagocytosismeasured as inhibition of uridine uptake by Candidaalbicans. J Immunol Methods 1977; 14:19-24.
22 Axtell RA. Evaluation ofthe patient with a possible phagocyticdisorder. Hematol Oncol Clin North Am 1988; 2: 1-12.
23 Rajkovic IA, Williams R. Rapid microassays of phagocytosis,bacterial killing, superoxide and hydrogen peroxide produc-tion by human neutrophils in vitro. J ImmunolMethods 1985 -
78: 35-47.24 Wilkinson PC. In: Thompson RA, ed. Techniques in clinical
immunology. 2nd ed. London: Blackwell, 1981: 273-93.25 Barlow AJE, Aldersley T, Chattaway FW. Factors present in
serum and seminal plasma which promote germ-tubeformation and mycelial growth of Candida albicans. J GenMicrobiol 1974; 82: 261-72.
26 Dolan CT, Ihrke DM. Further studies of the germ-tube testfor Candida albicans identification. AmJI Clin Pathol 1971;55: 733-4.
27 Hill GL, Blackett RL, Pickford IR, Bradley JA. A survey ofprotein nutrition in patients with inflammatory boweldisease - a rational basis for nutritional therapy. Br J Surg1977; 64: 894-6.
28 Finkelstein RA, Sciortino CV, McIntosh MA. Role of iron inmicrobe-host interactions. Rev Infect Dis 1983; 5: S759-77.
29 Weinberg ED. Iron witholding: a defence against infectionand neoplasia. Physiol Rev 1984; 64: 62-102.
30 Elin RJ, Wolff SM. Effect of pH and iron concentration ongrowth of Candida albicans in human serum. J Infect Dis1973; 127: 705-8.
31 Elmn RJ, Wolff SM. The role of iron in nonspecific resistance toinfection induced by endotoxin. J Immunol 1974; 112: 737-45.