cape breton region, nova scotia -...
TRANSCRIPT

CAPE BRETON REGION, NOVA SCOTIA


Cape Breton Region, Nova Scotia
© 2013 CAMH
3
Cape Breton Region, Nova Scotia
For more information, please contact:
Joanna Henderson, Ph.D.
Clinician Scientist
Gloria Chaim, MSW
Deputy Clinical Director
Child, Youth and Family Services
Centre for Addiction and Mental Health
80 Workman Way, Toronto, ON M6J 1H4
Production of this report has been made possible through a financial contribution from Health Canada.
The views expressed herein do not necessarily represent the views of Health Can

Cape Breton Region, Nova Scotia
4
Acknowledgments
The National Youth Screening Project Team would like to acknowledge the commitment, dedication
and hard work of the many people representing agencies in the Cape Breton Region, Nova Scotia,
one of the ten participating communities across Canada. Sincere thanks are due to the Cape Breton
network lead, Samantha Hodder, who advocated for Cape Breton to participate in this project, as well
as to the network coordinator, Brandy MacNeill, who spearheaded the project and worked tirelessly to
ensure full implementation of the project protocol; to the agency leads who were prepared to commit
to participate in a cross-sectoral collaboration, adapt agency protocols to integrate consistent
administration of a screening tool and dedicate staff time to participate in the project; and to front-line
service providers who were willing to take the time to explore new practices, and to engage youth in a
screening process for clinical and research purposes; and, most of all, to the youth who participated in
completing the screeners and consented to sharing them for project purposes. We would also like to
thank Health Canada for their commitment to capacity building, data collection and knowledge
exchange, demonstrated by providing the funding support that made this project and dissemination of
the findings possible.
National Youth Screening Project Partner Agencies: Cape Breton Region
The following agencies participated in one or more of the four key project activities: Capacity Building,
Network Development, Screening Implementation and Data Collection (Refer to Appendix A for
agency descriptions and Appendix B for key project activity descriptions).
Partner Agencies Agency Leads
Cape Breton District Health Authority:
Addictions Services:
o Community Based Services
o Health Promotion and Prevention
o Inpatient Withdrawal Management
o Opiate Recovery Program
Brandy MacNeill
Barry McNeil
Samantha Hodder
Priscilla McIntyre
Sharon MacKenzie
Mental Health Services:
o Adult Mental Health
o Child and Adolescent Mental Health
o Emergency Crisis and Community
o Inpatient Mental Health
Youth Health Centre
Karen Shea
Julie MacDonald
Linda Parris
Corinna Simon
Mary Beth Leblanc
Cape Breton Victoria Regional School Board Cathy Viva
Cape Breton Region, Nova Scotia
5
Department of Justice, Community Corrections Brad Furey
Family Service of Eastern Nova Scotia Bridget Revell & Mary-Jo Church
Department of Community Services, Child Welfare John Janega & David Tunney
Network Leads
Cape Breton District Health Authority (CBDHA)
Samantha Hodder, Network Lead
Brandy MacNeill, Network Coordinator
Project Team: Centre for Addiction and Mental Health (CAMH)
Project Leads
Joanna Henderson
Gloria Chaim
Project Coordinators
Eleanor Liu
Megan Anne Tasker
Administrative Support
Stephanie Schultz
Research Analysts
Andra Ragusila
Dave Summers
Carly Clifton
Vivian Zhang
GAIN SS License
Chestnut Health Systems – Copyright holder for all Global Appraisal of Individual Needs instruments,
including Global Appraisal of Individual Needs - Short Screener (GAIN SS)

Cape Breton Region, Nova Scotia
6
Table of Contents
List of Figures 7
National Youth Screening Project 9
Overview 9
Context 9
Objectives 12
National Youth Screening Project: Cape Breton Region 13
Summary 13
Development 13
Partners 14
Roles 14
Implementation Process 15
Materials 17
Findings 21
Background Information about Youth 23
Clinical Needs of Youth Based on the GAIN SS 36
Other Clinical Needs 46
Concurrent Substance Use and Mental Health Concerns 47
Service Provider Survey 54
Feasibility and Utility of the GAIN SS 55
Summary of Findings 57
Discussion 58
Recommendations 60
Appendix A: Cape Breton Region Network Member Agency Descriptions 65
Appendix B: Key Project Activity Descriptions 69
Appendix C: Agency Project Activity Participation 70
Appendix D: Project Timeline 71
Appendix E: Project Flow Chart 72
Appendix F: References 73

Cape Breton Region, Nova Scotia
7
List of Figures
Figure 1: Age Distribution of Participants 24
Figure 2: Age Distribution by Service Sector 25
Figure 3: Sex Distribution of Participants 26
Figure 4: Sex Distribution of Participants by Service Sector 27
Figure 5: Service History by Service Sector 28
Figure 6: Ethnicity Distribution of Participating Youth 29
Figure 7: Current Living Arrangements 30
Figure 8: Current Living Arrangements by Sex 31
Figure 9: Current Living Arrangements by Age Categories 32
Figure 10: Current Living Arrangements by Service Sector 33
Figure 11: Number of Concerns Endorsed by GAIN SS Domain 37
Figure 12: Recent Clinical Needs Using Moderate Threshold by Service Sector 38
Figure 13: Recent Clinical Needs Using High Threshold by Service Sector 39
Figure 14: Recent Internalizing Concerns by Age and Sex Categories 40
Figure 15: Recent Externalizing Concerns by Age and Sex Categories 41
Figure 16: Recent Substance Use Concerns by Age and Sex Categories 42
Figure 17: Recent Crime and Violence Concerns by Age and Sex Categories 43
Figure 18: Recent Suicide Concerns by Sex Category 44
Figure 19: Recent Suicide Concerns by Age and Sex Categories 45
Figure 20: Rates of Recent Additional Concerns by Sex Categories 46
Figure 21: Rates of Endorsement of Concurrent Disorders 47
Figure 22: Rates of Endorsement of Concurrent Disorders by
Service Sector and Sex 49
Figure 23: Rates of Endorsement of Concurrent Disorders by Age and Sex 50
Figure 24: Rates of Endorsement of Concurrent Disorders by
Legal System Involvement 51
Figure 25: Complexity of Needs 52
Figure 26: Service Provider Perceptions of GAIN SS Utility and Feasibility 55
Cape Breton Region, Nova Scotia
8

Cape Breton Region, Nova Scotia
9
National Youth Screening Project
Overview
The National Youth Screening Project (NYSP), Enhancing Youth-Focused, Evidence-Informed
Treatment Practices through Cross-Sectoral Collaboration, was funded under Health Canada’s Drug
Treatment Funding Program (DTFP) to work collaboratively with youth-serving agencies in seven
communities across Canada to implement a common screening tool for youth substance use and
mental health concerns. Each network was to include a range of agencies representing three or more
sectors, including substance use, mental health, justice, child welfare, education, housing, outreach
and primary health care. Each of the agencies was to participate in one or more of four key project
activities: Capacity Building, Network Development, Screening Implementation and Data Collection
(See Appendix B). Through this process, the project would have the opportunity to examine rates of
co-occurring substance use and mental health concerns (frequently referred to as concurrent or co-
occurring disorders (CD)) in different service sectors, across the adolescent and emerging adulthood
age spectrum, and to examine the extent to which rates of CD are consistent with service provider
expectations. As well, the project aimed to explore service provider perceptions of inter-agency
referrals, perceived interagency collaboration and youth CD attitudes, knowledge, and practices at
different time points in the project.
The overall objective of the NYSP was to enhance service provider CD capacity, increase early
intervention opportunities and improve pathways to treatment for youth aged 12-24 years with
substance use concerns and CD. This was done through building sustainable stakeholder
collaborations and providing CD-related capacity development opportunities.
Context
Background
Youth with CD experience difficulties in many areas of functioning, resulting in vulnerability to
increased risk-taking behaviour, poor academic/vocational performance, increased suicide risk, and
adverse health effects, including increased risk for substance dependency and psychiatric disorders
continuing into adulthood (Rush, Castel & Desmond, 2009). Unfortunately, effective, developmentally-
informed interventions have yet to be established. From a public health perspective there is a
desperate need to develop integrated models of service delivery across the continuum of care to
improve outcomes and reduce the high individual and societal costs associated with CDs (Rush et al.,
2009). Evidence suggests that universal screening for mental health and/or substance use disorders

Cape Breton Region, Nova Scotia
10
should be a routine part of client care in adults (Rush et al., 2009). However, effective and efficient
screening, assessment and treatment approaches, especially for youth, are only beginning to emerge.
At the same time, concerns about co-occurring substance use and mental health issues in youth have
been identified in services across sectors including child welfare, youth justice, mental health,
addictions, education, health care, housing and other social service agencies (Chaim & Henderson,
2009). There is a strong rationale for effective, consistent screening in youth service delivery settings
(Rush et al., 2009).
In Canada, there have traditionally been separate service delivery systems for health, mental health,
substance use treatment and social services rather than integrated or collaborative models of service
delivery. With recent calls to develop integrated models of service delivery in Canada (Health Canada,
2002), some agencies are beginning to offer integrated CD services, although little information is
available about types and accessibility of these services. Emerging evidence suggests that cross-
discipline collaborations may have particular benefits for improving access and meeting youth and
family needs (McElheran, Eaton, Rupcich, Basinger, & Johnson, 2004; Murphy, Rosenheck,
Berkowitz, & Marans, 2005). There are many barriers, however, to cross-discipline approaches,
especially if the disciplines involved differ substantially in organizational culture, philosophy, values
and practices (Oliver & Dykeman, 2003; Robillard, Gallito-Zaparaniuk, Kimberly, Kennedy, Hammett,
& Braithwaite, 2003). It has been argued that these barriers can be addressed through
communication, relationship-building, joint educational opportunities and practice-based initiatives,
although the specific impacts of these strategies have not been established (McElheran et al., 2004;
Murphy et al., 2005; Oliver & Dykeman, 2003; Henderson, MacKay, & Peterson-Badali, 2010).
Although it is well known that youth presenting for service often have multiple co-occurring needs, the
fragmented system is generally not set up to address them. There are many challenges including
stigma, lack of resources, lack of knowledge and lack of attention to youth-specific needs, as well as a
frequent lack of collaboration and limited integration. The work of the Canadian Mental Health
Commission (2006) and the National Treatment Strategy Working Group (2008) highlighted these
issues and provided some fundamental principles to be considered and followed in planning new
initiatives. Themes and recommendations identified across these documents including “every door is
the right door,” the need to improve access, the importance of attending to population specific needs,
the need to collaborate within and across sectors, the importance of generating solid data to inform
investments and making knowledge exchange a priority, have informed this project as well as our
previous collaborative screening network projects (GAIN Collaborating Network, 2009; Concurrent
Disorders Support Services Screening Project, 2011).
Choosing a Screening Tool for Youth
The importance of screening for both mental health and substance use concerns across sectors has
been identified through a number of initiatives. From 2002 to 2006, the emphasis was primarily on the
Cape Breton Region, Nova Scotia
11
identification of useful adult tools and practices (Health Canada, 2002; Centre for Addiction and
Mental Health, 2006).
In 2006, Rush and colleagues initiated a process to identify youth screening tools and processes and
conducted a comprehensive review and synthesis of screening tools for substance use and mental
health disorders among children and adolescents (Rush et al., 2009).
Through these initiatives, the Global Assessment of Individual Needs Short Screener (GAIN SS) was
identified as an ideal first stage screening tool for substance use and mental health concerns for youth
and adults. In particular, it was recommended because it:
Screens for both substance use and mental health issues
Is reliable and valid
Is brief (five to seven minutes to complete)
Can be self-administered
Has been validated for individuals aged 10 years and older (including adults)
Is low cost
Can be used in different service settings (e.g., treatment, primary care, etc.)
Collaborative Screening Initiatives 2003 - 2010
In 2003, CAMH merged its children’s mental health and youth substance use services into the Child,
Youth and Family Program (CYFP) and in 2005 a project was initiated to identify and implement a
common screening tool for substance use and mental health concerns across the merged program.
Based on the work of Rush and colleagues, the GAIN SS was chosen and implemented. In addition,
substance use and mental health-related staff attitudes, knowledge and practices were measured and
staff feedback was gathered. Findings from that project demonstrated that many youth endorsed co-
occurring substance use and mental health concerns, regardless of “presenting problem” and initial
service request. As well, participating staff indicated that implementing a consistent substance use
and mental health screening tool was feasible across diverse services and provided clinically useful
information (Henderson, Chaim & Rush, 2007; Skilling, Henderson, Root, Chaim, Bassarath & Ballon,
2007).
Discussion about this project at workshops, conferences and network meetings generated interest in
the Toronto-based Mental Health and Addiction Youth Network (MAYN) in replicating the project
within their own agencies. In 2008, a cross-sectoral network of 10 Toronto-based youth serving
agencies, all members of MAYN, led by Gloria Chaim and Joanna Henderson committed to
administer the GAIN SS, along with a standardised background information form to the youth (aged
12 – 24 years) seeking service at their agencies for a 6-month period. The GAIN Collaborating
Network research findings resulted in a report describing youth needs across sectors and about the
feasibility and utility of consistent screening and the GAIN SS in particular. Stakeholder discussion

Cape Breton Region, Nova Scotia
12
about the findings generated a number of service, system and research initiatives and suggested that
the GAIN SS is a feasible and useful clinical instrument (Chaim & Henderson, 2009).
Upon completion of the GAIN Collaborating Network project, findings were presented to local
stakeholders including service providers, agency leaders and policy makers as well as at multiple
international, national and local conferences, meetings, and forums, most notably the Annual
Convention of the American Psychological Association (2009) and Issues of Substance (2009).
Through these knowledge sharing opportunities, interest in implementing the GAIN SS in youth
serving agencies and in participating in collaborative research was generated in communities across
Canada. In 2009, the Health Canada, Drug Treatment Funding Program had a call for proposals.
With interest and stakeholder support from several provinces, Chaim and Henderson submitted a
proposal to engage youth-serving agencies in participating in a national youth screening project.
In 2010, while awaiting acceptance of their DTFP proposal, Chaim and Henderson, in collaboration
with the Toronto Concurrent Disorders Support Services Network, supported by the Toronto Central
Local Health Integration Network, launched another screening project, working with a cross-sectoral
group of 10 Toronto-based health and social service agencies focused on youth and adults seeking or
receiving service at their agencies. Similar to the GAIN Collaborating Network Project, service
providers’ attitudes regarding feasibility and utility of the GAIN SS were positive and stakeholders
reported that the research results were useful in identifying gaps in service and training needs for staff
(Hillman et al., 2011).
The National Youth Screening Project: Enhancing Youth-Focused, Evidence-Informed Treatment
Practices through Cross-Sectoral Collaboration was granted DTFP funding in 2010.
Objectives
Promote, facilitate and evaluate implementation of evidence-based screening procedures and tools
in cross-sectoral youth-serving agencies
Establish network protocols for referral and intervention to improve pathways to care for youth
Promote and facilitate collaboration and knowledge exchange amongst service providers through
the establishment of local cross-sectoral networks of youth-serving agencies
Increase use of reliable and valid tools across agencies and sectors
Evaluate and compare youth service needs across jurisdictions
Evaluate and compare pre-post service provider capacity re: evidence-based practices for youth
substance use with or without co-occurring mental health concerns
Promote a standardised screening protocol for youth concurrent disorders

Cape Breton Region, Nova Scotia
13
National Youth Screening Project: Cape Breton Region, Nova Scotia
Summary
The Cape Breton Network was the first of ten networks to launch the National Youth Screening
Project. Discussion about collaboration began in June 2010, followed by several meetings throughout
the summer and fall, resulting in five agencies committing to participate in the project. All necessary
Research Ethics Board (REB) submissions were approved and agreements were signed by March
2011.
Over a staggered six month period, commencing in April 2011, a cross-sectoral group of five youth-
serving agencies in and around Sydney, Nova Scotia undertook this collaborative project to
administer the GAIN SS and a demographic information form to youth aged 12 to 24 years seeking
service at their agencies. Service providers participated in training about youth substance abuse and
CD, with an emphasis on evidence-based screening practices, clinical use of the GAIN SS and
implementation of the project protocol. Service providers completed pre/post surveys about their own
knowledge, attitudes and practices related to youth substance use and mental health concerns. They
also provided feedback about their perceptions of the feasibility and utility of implementing the
screening tool in their practices and the impact of screening in particular and project participation
more generally on their referral practices. Presented in this report are the background and service
needs of youth who participated in this study as well as service provider perceptions of the screening
tool and related processes.
Development
In 2010, the Cape Breton District Health Authority (CBDHA) expressed interest in participating in the
National Youth Screening Project in response to broad national dissemination of information about the
project prior to the submission of the proposal as well as following the funding announcement. In
collaboration with CBDHA, a cross-sectoral network of five local agencies that serve youth was
formed and CBDHA took on the role of “Lead Agency”. Similar to the pilot screening projects
described above, the agencies expressed interest in participating in a project to build capacity to
identify and address the complex needs of the youth who access their services as well as in having
the opportunity to document the needs of youth seeking service in their respective agencies, sectors
and community.
Cape Breton Region, Nova Scotia
14
In January 2011, CBDHA formally agreed to lead and coordinate a local collaborative network to
implement the GAIN SS1 with youth seeking service at the participating agencies. The project team
held a one-day training workshop for service providers, repeated on two consecutive days to allow for
all agency staff to be trained, in Sydney, Nova Scotia, January 18-19, 2011. Service providers
attended from all five participating agencies. Prior to the training, the service providers were surveyed
regarding their attitudes, knowledge and practices related to youth substance use, mental health and
co-occurring concerns. In March and April, four of the agencies launched the six-month data
collection phase. Two agencies were unable to participate in the data collection activity of the project.
The Department of Community Services - Child Welfare and the Cape Breton Victoria Regional
School Board participated only in capacity building and network development due to staff turnover.
The Cape Breton Region Network was established based on shared interests and concerns, including
interest in the opportunity to work together in a research-community collaboration. Furthermore, the
network members expressed a desire to lay the groundwork for on-going partnerships and
collaboration through their participation in the NYSP. The network was interested and committed to
ensuring that knowledge gained through this collaborative effort be shared locally, provincially and
nationally.
Partners
The Cape Breton Region Network includes representation from the addictions, child welfare,
education, family services, health (i.e Youth Health Centres), justice, and mental health sectors, with
both hospital and community-based agencies and services included (see Appendix A for agency
descriptions). Two thirds of the agencies participated in all four project activities, which included:
Capacity Building, Network Development, Screening Implementation, and Data Collection. Please
refer to Appendix B for a description of key project activities and Appendix C for description of the
respective agency participation.
Roles
National Project Team:
Provide resources for and support meetings of youth-serving agencies to support all aspects of
project participation;
Provide training to staff in identifying and addressing substance use and/or CD concerns in youth,
implementing the GAIN SS and the data collection protocol;
1Chestnut Health Systems granted a license to CBDHA to use the GAIN SS (CAMH Version) and gave permission to CBDHA to include all the participating agencies in the network in its licensing agreement.

Cape Breton Region, Nova Scotia
15
Provide all necessary screening and project-related materials;
Provide templates and support for developing response, resource and referral guides customised
for each community;
Obtain ethics approval through Health Canada and CAMH and support each agency to comply with
their ethics approval processes.
Lead Agency: CBDHA
Identify local organizations, representing a minimum of 3 sectors to participate in the project as a
participating agency;
Vet prospective participating agencies for suitability;
Act as a liaison between CAMH and participating agencies during the term of the project;
Identify and facilitate agency leads to obtain local REB approval for the project;
Obtain licenses from Chestnut Health Systems Inc. for use of the GAIN SS for participating
agencies;
Support training provided by the project leads and facilitate provision of consultation as needed
throughout the project;
Facilitate pre and post service provider surveys of staff attitudes, knowledge and practices to all
agency staff involved in the project;
Facilitate data collection by the participating agencies.
Participating Agencies:
Comply with the agreed upon protocol by obtaining participant and parental consents, administering
GAIN SS and submitting the data to the lead agency for review;
Ensure staff participation in project-related training;
Maintain and store original data from participants as per REB policies and in accordance with legal
requirements;
Ensure that as many eligible youth as possible have the opportunity to be included in the project
and that the rates of eligibility and consent are tracked.
Implementation Process
(See Appendix D for Project Timeline)
Prior to initiating project activities, two separate agreements were signed:
1. A two-party agreement between CAMH and the CBDHA, the network lead agency.
2. A three-party agreement between CAMH, CBDHA and each of the respective participating
agencies.

Cape Breton Region, Nova Scotia
16
Each agreement described the project, roles, responsibilities, activities and commitments, as well as
the data collection protocol. These agreements were developed and signed by five of the agencies.
Two of the agencies, Department of Community Services - Child Welfare and Cape Breton Victoria
Regional School Board were unable to participate in all four of key activities of the project, however,
both participated in the Capacity Building and Network Development activities, and Cape Breton
Victoria Regional School Board also participated in Screening Implementation in its schools.
A collaborative process was used throughout the project to develop joint goals, materials and
processes as well as research questions and data analyses. The lead agency, CBDHA, was involved
with the project throughout each stage of the project from initiation to completion. Once the agency
level training was completed and data collection was underway, the lead agency, along with the
project team at CAMH, was involved in communicating with the participating agencies to maintain
engagement, momentum, and compliance with the project protocol and problem-solving of issues
arising.
Implementation Process
1. May - November, 2010 – Networking:
a. Identified interested agencies
b. Established cross-sectoral network
2. September 2010 - March 2011 – Agreements and REB:
a. Developed 2-party agreement between CAMH and CBDHA
b. Developed 3-party agreement between CAMH, CBDHA and all
participating agencies
3. January 18 – 19, 2011 – Capacity building
a. Capacity building across sites was delivered using the package
developed by the project leads
b. Project leads administered service provider consents and the Service
Provider Survey at the beginning of the training day
c. Each Agency identified a lead to act as a “point person” for
communication with the Network Lead, including receiving and
distributing project packages to the participating service providers in their
respective agencies
4. April 2011 – Project launch:
a. Distributed project packages i.e. Project Instruction Sheets, Consent
forms, GAIN SS, Background Information forms, Tracking Sheets
5. April – September 2011 – Project actively underway:
a. Service providers obtained consent from youth seeking service at their

Cape Breton Region, Nova Scotia
17
agencies, administered the GAIN SS and Background Information Form
b. Anonymous copies of the completed measures and tracking sheets were
submitted to the network coordinator on a monthly basis, and delivered to
CAMH at month 1, 3 and 6
c. Consultation was provided as needed by the network coordinator and/or
project coordinator/project leads
d. Staff feedback forms were collected on completion of the data collection
6. February 22, 2012 – Preliminary data analysis meeting:
Discussed:
a. Data analysis questions
b. Preliminary findings
c. Fit with expectations and experiences of the community
d. Lessons learned, including staff feedback provided on utility and
feasibility of administering the GAIN SS to youth in their agencies
e. Feedback from network and agencyleads
f. Potential recommendations based on findings
g. Report dissemination plan
Materials
Service Provider Project Package
Service Provider Consent Form
The consent form described the project, confidentiality and plans for data management. Service
providers’ initials only were required to ensure anonymity.
Service Provider Survey
The Service Provider Survey is a self-report questionnaire that combines measures of service
providers’ 1) service-related knowledge, attitudes and practices regarding youth substance use,
mental health, co-occurring disorders, and screening; 2) perceptions of co-occurring disorders-
informed practices; 3) estimates of current use of CD-informed practices; and 4) experiences with
inter-agency referrals and collaboration.
Cape Breton Region, Nova Scotia
18
Project Flow Chart (See Appendix E)
A step-by-step one page project flow chart was developed for use by all service providers to facilitate
consistency across providers.
Instructions for GAIN SS Use
A step-by-step one page protocol was developed for use by all service providers to facilitate
consistency across providers.
Referral Resource Guide
Customised templates listing local resources for consultation and referrals for follow-up to
endorsement of concerns on the GAIN SS were provided to each participating service provider.
GAIN SS Tracking Sheet
Tracking sheets were used to document rates of youth eligibility for project participation, consent/non-
consent, participation/reasons for non-participation, and data collection completion and submission for
each youth seeking service in each agency.
Feedback Survey
The feedback survey was designed to gather information from participating service providers
regarding their perceptions of the feasibility and utility of administering the GAIN SS to youth in their
setting and about the impact of the screening process on their practices.
Youth Project Package
Youth Consent Form
The consent form described the project, confidentiality and plans for data management. Youth initials
only were required to ensure anonymity.
Parental Consent Form
The consent form described the project, confidentiality and plans for data management. Parental
consent was required in addition to youth consent only where parental consent was required to obtain
services for youth under 16 years of age. Parent’s initials only were required to ensure anonymity.
Background Information Form
The Background Information Form is a one-page questionnaire used to gather demographic
information about the participating youth. The questions seek information about the determinants of
health frequently cited in the literature as associated with youth substance use and mental health
concerns including age, sex, education, employment, income support, housing, legal involvement,
ethno-racial identification, and language diversity.

Cape Breton Region, Nova Scotia
19
GAIN SS (CAMH Version)
The GAIN SS is a brief screening tool validated for use with individuals aged 10 years and older to
quickly identify those who may be experiencing difficulties in one or more of four dimensions: 1)
internal mental distress (e.g., depression, anxiety); 2) behavioural complexity (externalizing
behaviours e.g., ADHD); 3) substance use problems; and 4) crime and violence (Denis, Chan & Funk,
2006). The tool was developed by Chestnut Health Systems and copyrighted in 2005. Chestnut
Health Systems permitted CAMH’s Child, Youth and Family Program to modify the GAIN SS in 2006,
by adding seven items (not part of the original validation) at the end to screen for: eating-related
issues, trauma-related distress, disordered thinking and gambling, gaming and internet misuse
concerns.

Cape Breton Region, Nova Scotia
20

Cape Breton Region, Nova Scotia
21
Findings
Cape Breton Region, Nova Scotia
22
Cape Breton Region, Nova Scotia
23
Background Information about Youth
Who participated?
In total, 483 youth participated:
188 (39%) from addictions sector
21 (4%) from family services sector
150 (31%) from health sector2
19 (4%) from justice sector
105 (22%) from mental health sector
How representative is the sample of youth who participated in the project?
Service providers were asked to use tracking sheets to record each youth eligible to participate.
Information collected on the tracking sheets included sex, age, consent response, and any comments
on why individual youth may not have been approached or refused to consent. All participating
agencies used this approach to track participation rates.
According to the tracking sheets provided by the service providers 604 youth presented for service to
the participating programs and agencies over the course of the six-month project timeframe. Of these
youth 90% were eligible for the project (n = 544). Reasons for ineligibility included the GAIN SS had
already been administered (39%), immediate mental health concerns (e.g., psychosis) (33%),
cognitive limitations (23%), and the youth were not yet clients of the agency (5%). In addition, for 21
cases information was not provided. Of the youth who were eligible to participate in the project, 530
(97%) were approached for participation. Reasons for youth not being approached included clinician-
based reasons (judgment, forgot) (56%), no forms were available (19%), youth was unavailable (e.g.,
left, no show) (13%), and lack of time (13%). Of the youth who were approached, 86% completed the
GAIN SS. Based on the tracking sheets, 14% of youth who were asked to complete the GAIN SS
refused. Of the youth who completed the GAIN SS, 95% consented to have a copy used for the
purposes of this project. Overall then, based on these tracking sheet numbers, 79% of eligible youth
contributed screeners for this report. Some of the youth who did not contribute refused to participate
(17%), either through refusing to complete the GAIN SS (14%) or through declining to provide consent
(3%), while others were not approached (3%).
Please note: Based on the number of completed consents and screeners we received, we estimate
that approximately 89% of eligible youth were captured on tracking sheets.
2 In Cape Breton, the ‘health sector’ was represented by Youth Health Centres.

Cape Breton Region, Nova Scotia
24
What are the demographics of the youth who participated?
AGE
FIGURE 1: AGE DISTRIBUTION OF PARTICIPANTS
The participating youth ranged in age from 12 to 24 years with an average age of 16.6 years and a
median age of 16.0 years. In Figure 1, the ages of participating youth are presented using age
categories commonly used in service provision. As can be seen, more youth were in the 12-15 years
age range than other age categories.
42%
35%
21%
2%
12-15 years old
16-18 years old
19-24 years old
Missing
Cape Breton Region, Nova Scotia
25
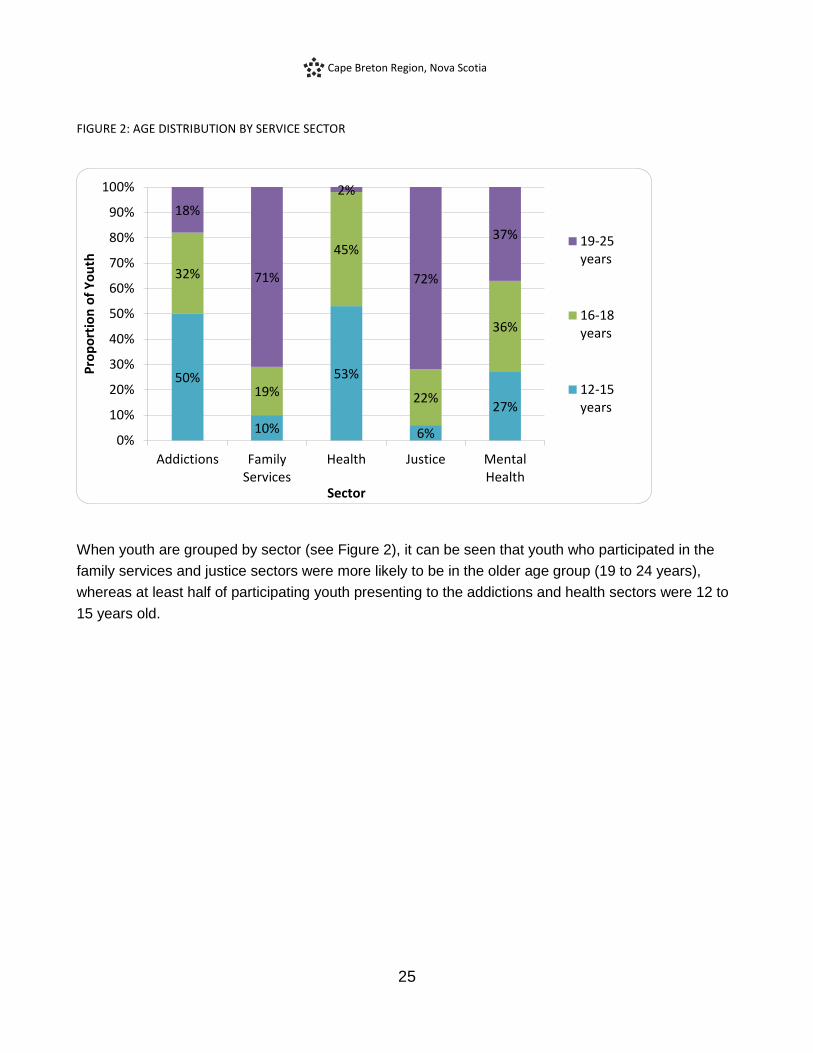
FIGURE 2: AGE DISTRIBUTION BY SERVICE SECTOR
When youth are grouped by sector (see Figure 2), it can be seen that youth who participated in the
family services and justice sectors were more likely to be in the older age group (19 to 24 years),
whereas at least half of participating youth presenting to the addictions and health sectors were 12 to
15 years old.
50%
10%
53%
6%
27%
32%
19%
45%
22%
36%
18%
71%
2%
72%
37%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Addictions FamilyServices
Health Justice MentalHealth
Pro
po
rtio
n o
f Y
ou
th
Sector
19-25years
16-18years
12-15years

Cape Breton Region, Nova Scotia
26
Sex
FIGURE 3: SEX DISTRIBUTION OF PARTICIPANTS
There are significantly more female youth than male youth in the group who participated in the project
(p <.05). Almost two-thirds of participating youth were female (62%), while 36% were male, 0.4%
identified as trans, and 1.7% did not provide this information. In order to protect the privacy of
participants, only those who identified as male or female are included in subsequent analyses related
to sex.
36%
62%
0.4% 1.7%
Male
Female
Trans
Missing

Cape Breton Region, Nova Scotia
27
FIGURE 4: SEX DISTRIBUTION OF PARTICIPANTS BY SERVICE SECTOR
Comparing the five sectors revealed that the male to female ratio differs between sectors. Health
services had a greater proportion of female participants than other sectors (85% female) whereas the
male to female ratio did not differ as significantly across the remaining sectors.
49% 43%
15%
61%
40%
51% 57%
85%
39%
60%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
AddictionsSector
FamilyServices
Health Justice MentalHealth
Pro
po
rtio
n o
f Y
ou
th
Sector
Female
Male

Cape Breton Region, Nova Scotia
28
Service History
FIGURE 5: SERVICE HISTORY BY SERVICE SECTOR
Most youth (76%) participating in the project had been involved with the participating service for less
than one month, although there was a fair amount of variability across sectors. For example, the
majority of youth from the mental health and health sectors completed the GAIN SS on their first visit
(71% for mental health service sector and 75% for health service sector), while the majority of youth
who did the questionnaire in the addictions sector had been involved with their respective services for
one month or less (69%) and in the family services and justice sectors, the majority of youth had been
involved for more than two months (52% family services, and 58% for justice).
19% 14%
75%
26%
71%
50%
33%
17%
16%
8% 21%
33%
6%
21%
14%
10% 19%
2%
37%
7%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Addictions FamilyServices
Health Justice MentalHealth
Pro
po
rtio
n o
f Y
ou
th
Sector
More thana year ago
2-12MonthsagoIn the pastmonth
Today
Cape Breton Region, Nova Scotia
29
Ethnicity
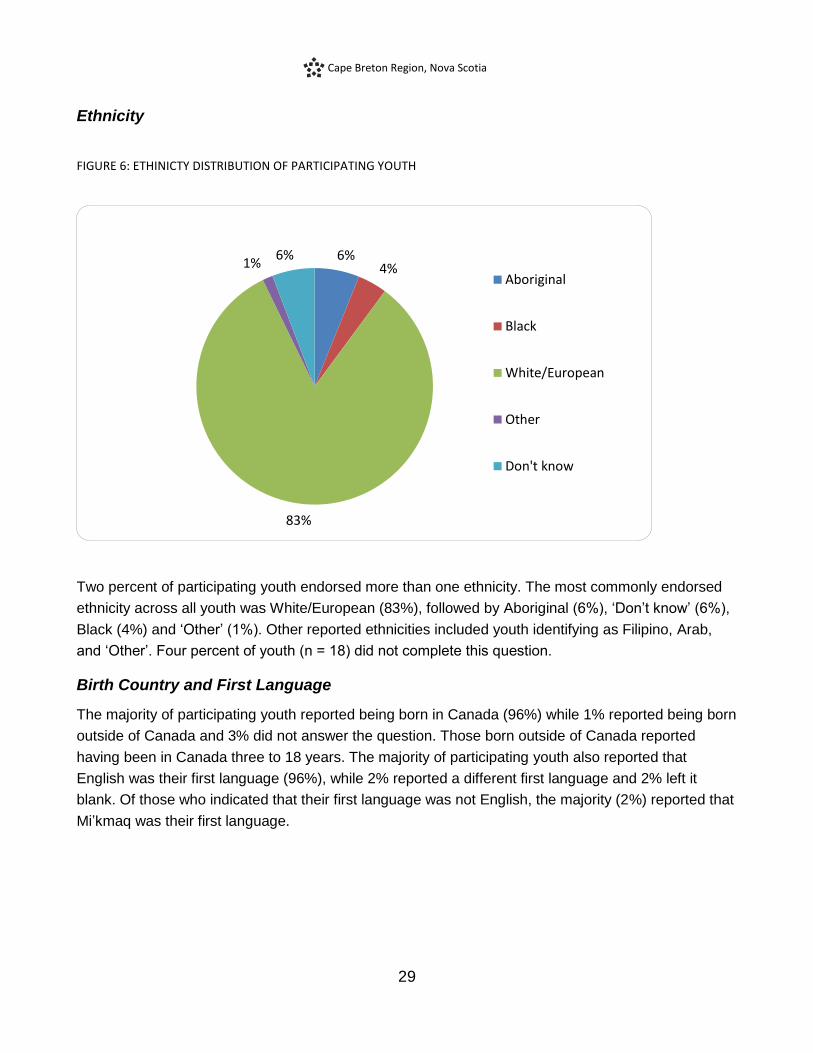
FIGURE 6: ETHINICTY DISTRIBUTION OF PARTICIPATING YOUTH
Two percent of participating youth endorsed more than one ethnicity. The most commonly endorsed
ethnicity across all youth was White/European (83%), followed by Aboriginal (6%), ‘Don’t know’ (6%),
Black (4%) and ‘Other’ (1%). Other reported ethnicities included youth identifying as Filipino, Arab,
and ‘Other’. Four percent of youth (n = 18) did not complete this question.
Birth Country and First Language
The majority of participating youth reported being born in Canada (96%) while 1% reported being born
outside of Canada and 3% did not answer the question. Those born outside of Canada reported
having been in Canada three to 18 years. The majority of participating youth also reported that
English was their first language (96%), while 2% reported a different first language and 2% left it
blank. Of those who indicated that their first language was not English, the majority (2%) reported that
Mi’kmaq was their first language.
6% 4%
83%
1% 6%
Aboriginal
Black
White/European
Other
Don't know

Cape Breton Region, Nova Scotia
30
Living Arrangements
FIGURE 7: CURRENT LIVING ARRANGEMENTS
Most participating youth (78%) reported that they were living with parents, while 8% were living on
their own or with friends, 7% were living with other family members, 1% reported living in supportive
housing (e.g. “group home”, “treatment facility”) and 2% reported living in unstable housing (e.g.
“shelter”, “on street”, “couch surfing”).
78%
8%
7%
1% 2% 4% Parental/Family Home
Own/With Friends
Other Family/Relative
Supportive Housing
Unstable
Missing
Cape Breton Region, Nova Scotia
31
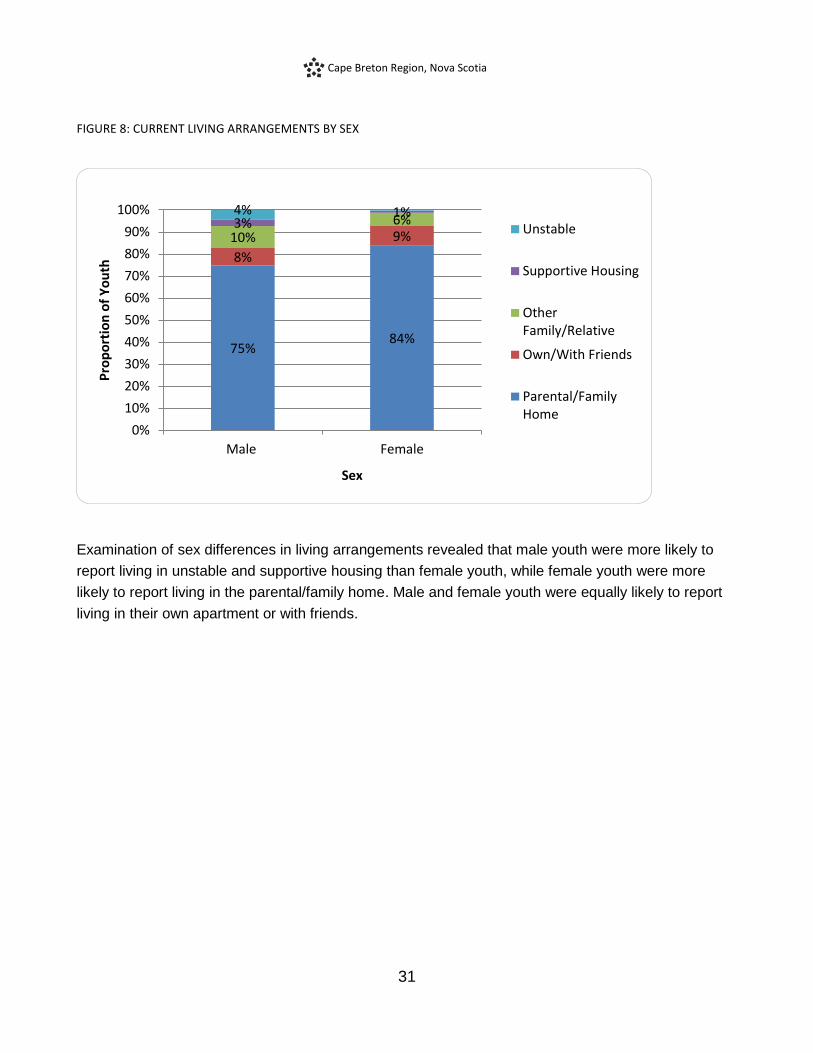
FIGURE 8: CURRENT LIVING ARRANGEMENTS BY SEX
Examination of sex differences in living arrangements revealed that male youth were more likely to
report living in unstable and supportive housing than female youth, while female youth were more
likely to report living in the parental/family home. Male and female youth were equally likely to report
living in their own apartment or with friends.
75% 84%
8%
9% 10% 6% 3% 1% 4%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Male Female
Pro
po
rtio
n o
f Y
ou
th
Sex
Unstable
Supportive Housing
OtherFamily/Relative
Own/With Friends
Parental/FamilyHome
Cape Breton Region, Nova Scotia
32
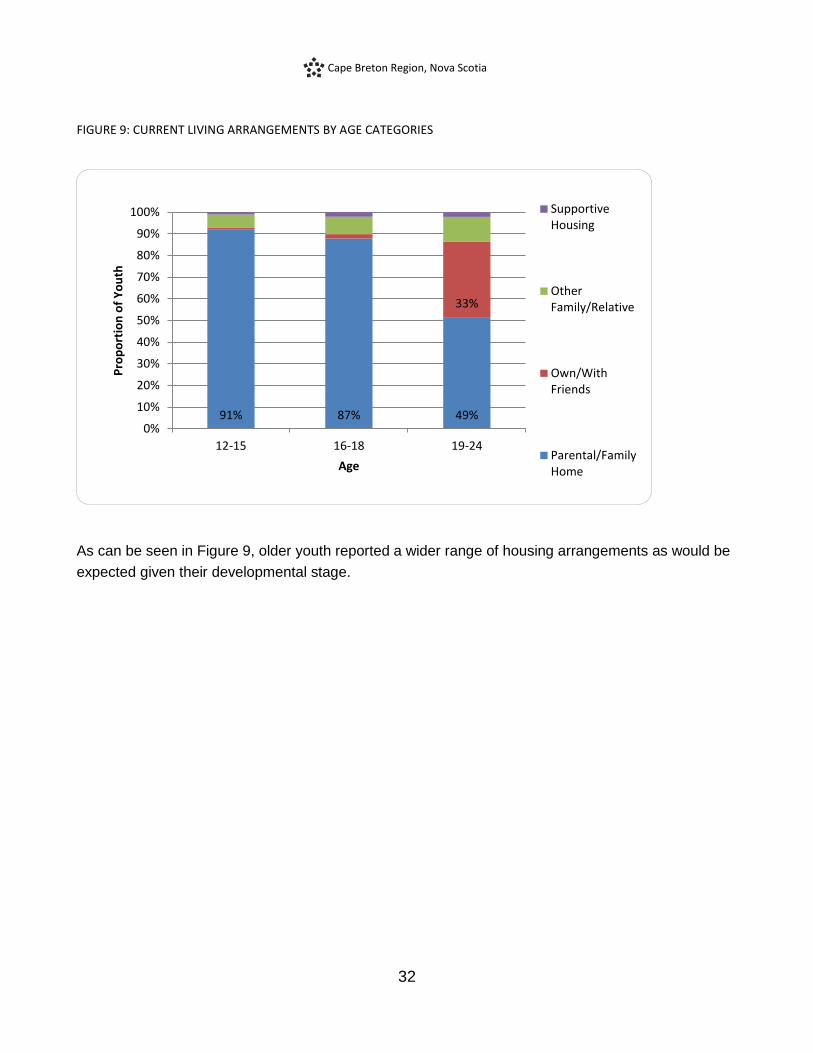
FIGURE 9: CURRENT LIVING ARRANGEMENTS BY AGE CATEGORIES
As can be seen in Figure 9, older youth reported a wider range of housing arrangements as would be
expected given their developmental stage.
91% 87% 49%
33%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
12-15 16-18 19-24
Pro
po
rtio
n o
f Y
ou
th
Age
SupportiveHousing
OtherFamily/Relative
Own/WithFriends
Parental/FamilyHome

Cape Breton Region, Nova Scotia
33
FIGURE 10: CURRENT LIVING ARRANGEMENTS BY SERVICE SECTOR
As would be expected given their age, older youth presenting for service to the family services sector
reported a wider variety of housing arrangements than youth presenting for service to other sectors.
83%
40%
88%
72% 77%
5%
35%
3%
17% 15%
6%
15%
8% 11% 8%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Addictions FamilyServices
HealthServices
Justice MentalHealth
Pro
po
rtio
n o
f Y
ou
th
Sector
Unstable
SupportiveHousing
OtherFamily/Relative
Own/WithFriends
Parental/FamilyHome
Cape Breton Region, Nova Scotia
34
Legal Involvement
The majority of participating youth reported never having any legal involvement (67%), while the
remaining youth reported legal involvement in the past 12 months (18%), more than a year ago
(11%), or did not answer the question (4%).
Education, Employment and Income
Overall just over half of participating youth identified as students. Of those who did not identify as
students, 47% indicated that they were unemployed, 25% indicated part-time employment, 10%
indicated that they were engaged in volunteer activities, and 8% indicated they had full-time
employment.
Age was related to educational, employment and income status. For youth aged over 18 years (n =
101), they indicated that their employment situations were as follows: unemployed (48%), working
part-time (22%), attending school (18%), working full-time (14%) or volunteering (6%) (not mutually
exclusive). In contrast youth aged 18 years or younger (n = 372) indicated that they were students
(62%), unemployed (23%), working part-time (18%), volunteering (12%) and working full-time (1%).
Similarly, the most commonly reported income sources for youth over 18 were as follows: welfare
(43%), employment (27%), no income (14%), employment insurance (12%), and parents/spouse
(11%), while youth aged 18 years and younger reported their income sources to be parents/spouse
(47%), no income (25%), employment (12%), family benefits (6%), and welfare (2%).
For youth over 18 years, educational attainment was also examined revealing a broad range of
educational achievements, including 4% of youth participants reporting grade 8 completion as their
highest educational achievement, 40% indicating grades 9-11 as their highest achievement, 4%
reporting achievement of high school completion without diploma, 27% indicating completion of high
school with diploma, 14% completing some non-university post-secondary education and 10%
completing some university studies.
Cape Breton Region, Nova Scotia
35
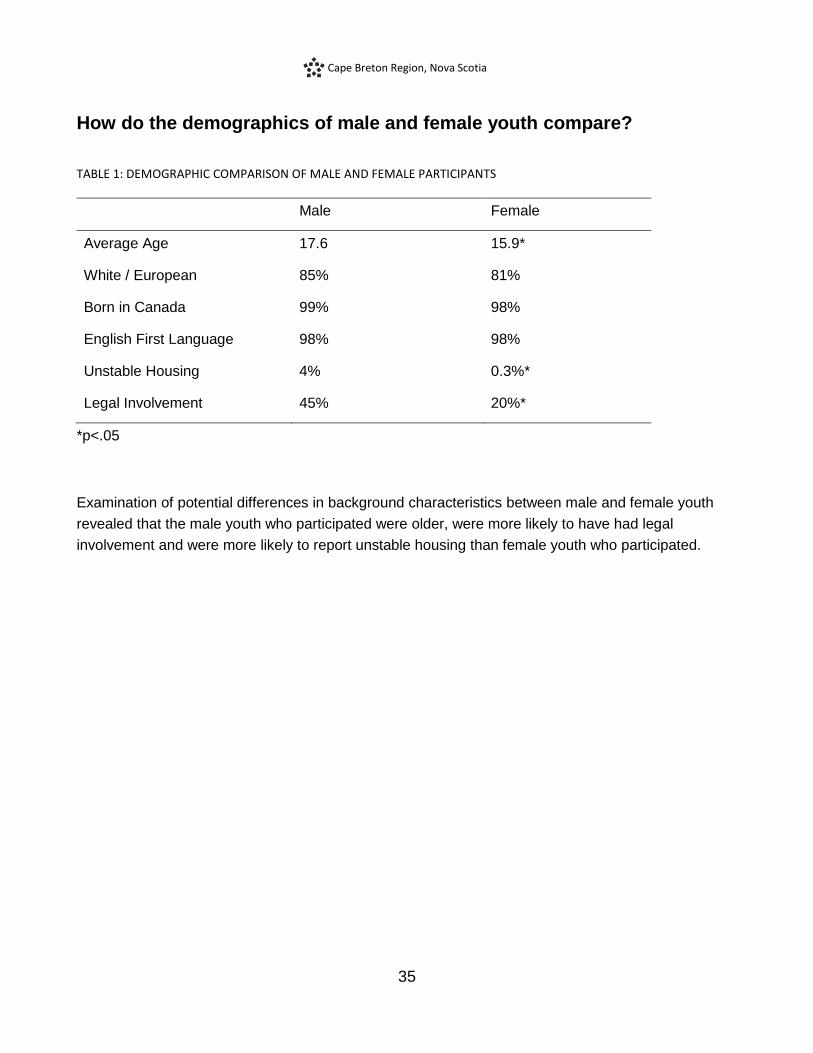
How do the demographics of male and female youth compare?
TABLE 1: DEMOGRAPHIC COMPARISON OF MALE AND FEMALE PARTICIPANTS
Male Female
Average Age 17.6 15.9*
White / European 85% 81%
Born in Canada 99% 98%
English First Language 98% 98%
Unstable Housing 4% 0.3%*
Legal Involvement 45% 20%*
*p<.05
Examination of potential differences in background characteristics between male and female youth
revealed that the male youth who participated were older, were more likely to have had legal
involvement and were more likely to report unstable housing than female youth who participated.

Cape Breton Region, Nova Scotia
36
Clinical Needs of Youth Based on the GAIN SS
The GAIN SS is a well-validated and reliable screener for mental health and substance use concerns
in youth and adults. It has four 5-item subscreeners embedded within the overall measure to screen
across four domains: Internalizing (INT) disorders (e.g., mood, anxiety disorders), Externalizing (EXT)
disorders (e.g., attention deficit/hyperactivity disorder), Substance Use disorders (SUB), and
engagement in Crime/Violence (CV). In order to fully understand the findings presented in this report,
it is important to understand the scoring decisions that informed the analyses. The GAIN SS has been
shown to have excellent sensitivity and specificity. These rates change, however, depending on how
the GAIN SS is scored and analyzed.
Within each subscreener using a moderate threshold of at least one recent (2-12 months ago) or
current (past month) concern has excellent sensitivity (94-98%) for identifying youth who will meet
diagnostic criteria for disorder, but lower (71-76%) specificity, i.e. lower accuracy in ruling out youth
who will not meet diagnostic criteria for disorder. Using a high threshold of three or more recent or
current concerns within one domain improves the specificity to 96-100%, but results in decreases in
sensitivity (49-68%). Using a threshold of three or more current or recent concerns endorsed across
all domains (total) will identify 91% of youth who will meet diagnostic criteria for a disorder and will
rule out 90% of youth who will not have a disorder (Dennis et al., 2006).
Depending on the service setting, use of each threshold may be more appropriate. For example, in
settings where the rates of clinically significant mental health and substance use problems are
expected to be low (e.g. primary care), use of the moderate threshold may be most appropriate. In
settings where individuals are seeking service for mental health and substance use concerns, use of
the high threshold may be more informative.
For this project, a modified version of the GAIN SS was used (GAIN SS CAMH Modified Version)
which includes 7 additional items following the original subscreeners. These additional items provide
information about eating behavior, thinking-related issues, traumatic distress, and gambling, gaming
and internet overuse. Sensitivity and specificity data for these items are not yet available and these
items are not scored.
Cape Breton Region, Nova Scotia
37
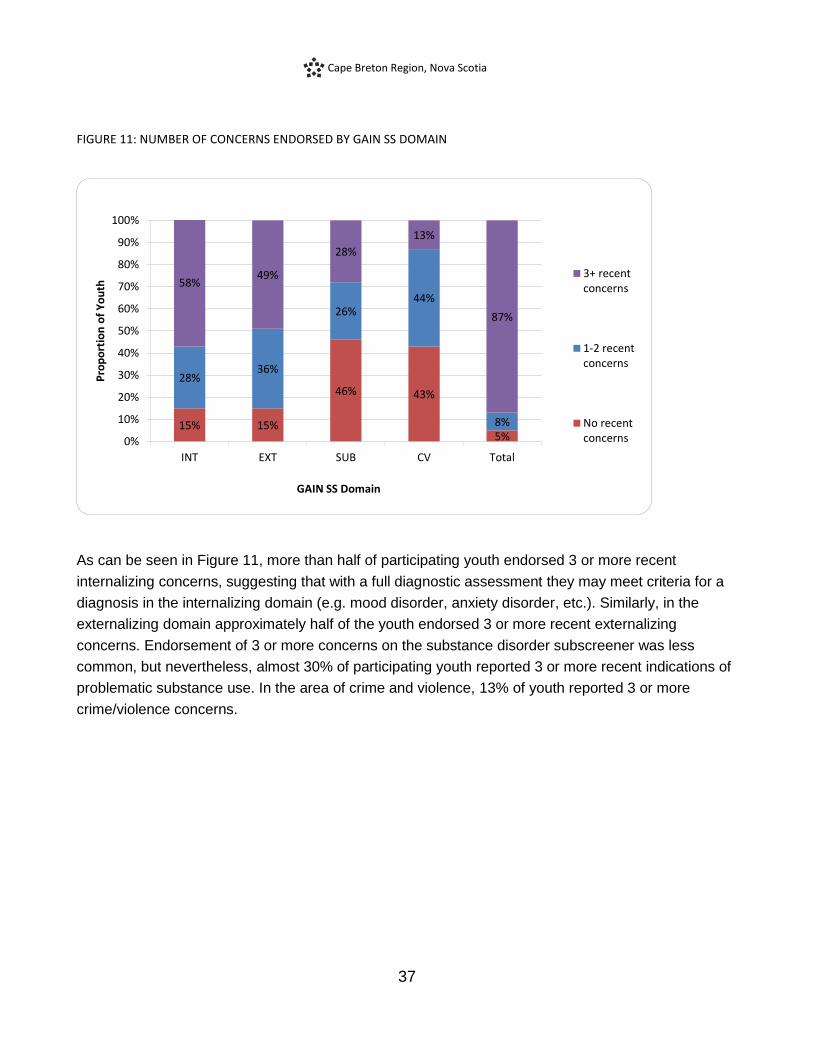
FIGURE 11: NUMBER OF CONCERNS ENDORSED BY GAIN SS DOMAIN
As can be seen in Figure 11, more than half of participating youth endorsed 3 or more recent
internalizing concerns, suggesting that with a full diagnostic assessment they may meet criteria for a
diagnosis in the internalizing domain (e.g. mood disorder, anxiety disorder, etc.). Similarly, in the
externalizing domain approximately half of the youth endorsed 3 or more recent externalizing
concerns. Endorsement of 3 or more concerns on the substance disorder subscreener was less
common, but nevertheless, almost 30% of participating youth reported 3 or more recent indications of
problematic substance use. In the area of crime and violence, 13% of youth reported 3 or more
crime/violence concerns.
15% 15%
46% 43%
5%
28% 36%
26% 44%
8%
58% 49%
28%
13%
87%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
INT EXT SUB CV Total
Pro
po
rtio
n o
f Y
ou
th
GAIN SS Domain
3+ recentconcerns
1-2 recentconcerns
No recentconcerns
Cape Breton Region, Nova Scotia
38
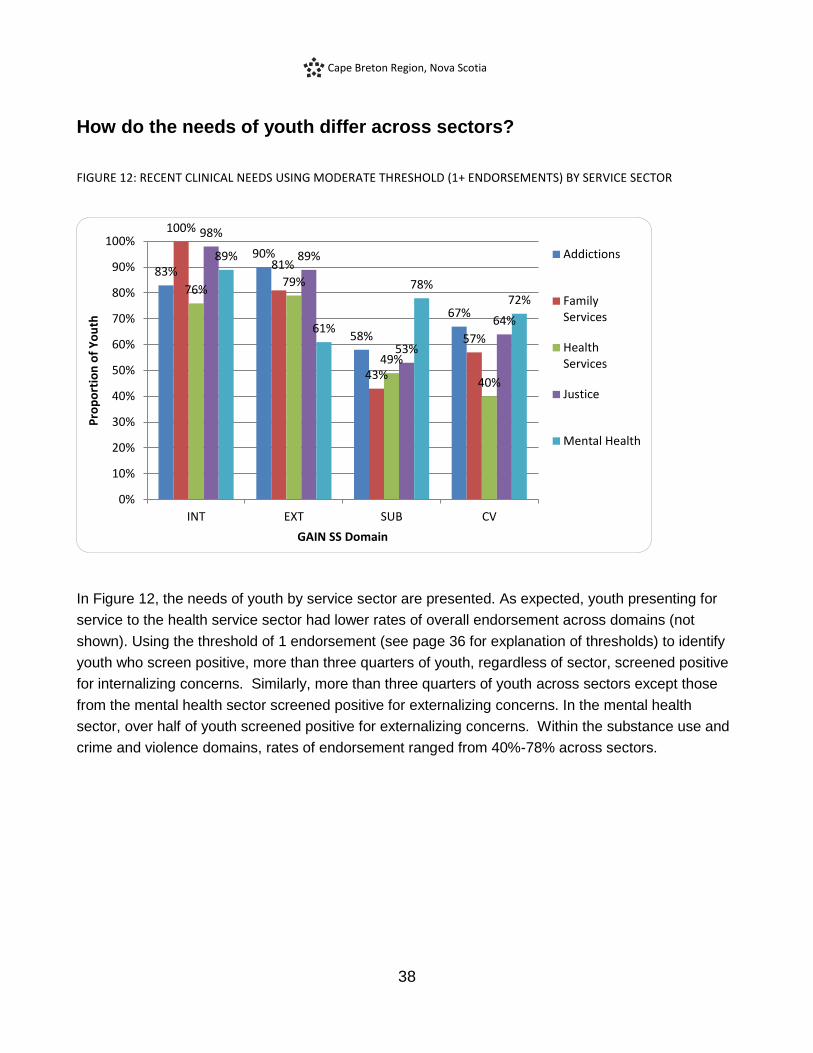
How do the needs of youth differ across sectors?
FIGURE 12: RECENT CLINICAL NEEDS USING MODERATE THRESHOLD (1+ ENDORSEMENTS) BY SERVICE SECTOR
In Figure 12, the needs of youth by service sector are presented. As expected, youth presenting for
service to the health service sector had lower rates of overall endorsement across domains (not
shown). Using the threshold of 1 endorsement (see page 36 for explanation of thresholds) to identify
youth who screen positive, more than three quarters of youth, regardless of sector, screened positive
for internalizing concerns. Similarly, more than three quarters of youth across sectors except those
from the mental health sector screened positive for externalizing concerns. In the mental health
sector, over half of youth screened positive for externalizing concerns. Within the substance use and
crime and violence domains, rates of endorsement ranged from 40%-78% across sectors.
83%
90%
58%
67%
100%
81%
43%
57%
76% 79%
49%
40%
98%
89%
53%
64%
89%
61%
78% 72%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
INT EXT SUB CV
Pro
po
rtio
n o
f Y
ou
th
GAIN SS Domain
Addictions
FamilyServices
HealthServices
Justice
Mental Health

Cape Breton Region, Nova Scotia
39
FIGURE 13: RECENT CLINICAL NEEDS USING HIGH THRESHOLD (3+ ENDORSEMENTS) BY SERVICE SECTOR
Using a threshold of three or more recent or current concerns within one domain improves the
specificity (i.e. fewer false positives) of the GAIN SS screener and allows identification of youth with
higher severity of needs.
As can be seen in Figure 13, the majority of youth presenting for service across sectors have high
internalizing concerns, with the exception of health sector where a lower but still concerning rate of
42% of youth reported high severity internalizing concerns.
Youth presenting for service to the family services and mental health sectors had particularly high
rates of endorsement with over 80% indicating that they had been experiencing 3 or more
internalizing symptoms in the past year. Within the externalizing domain, a third to half of youth
across sectors reported experiencing high severity externalizing difficulties.
In the substance use domain, youth in the justice sector had the highest rates of endorsement of
problematic substance use with just over half of participating youth indicating experiencing 3 or more
symptoms of problematic substance use in the past year. Though lower, a substantial proportion
(24%-36%) of youth presenting for service to addictions, family services, and mental health sectors
also indicated experiencing 3 or more symptoms of problematic substance use in the past year.
Although rates of endorsement were substantially lower in the area of crime and violence than other
domains, 1 in 5 youth presenting to the addictions sector still endorsed 3 or more crime and violence
problems.
52% 56%
36%
21%
81%
33%
24%
5%
42% 39%
13% 5%
61%
39%
56%
17%
83%
54%
31%
12%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
INT EXT SUB CV
Pro
po
rtio
n o
f Y
ou
th
GAIN SS Domain
Addictions
FamilyServices
HealthServices
Justice
MentalHealth
Cape Breton Region, Nova Scotia
40
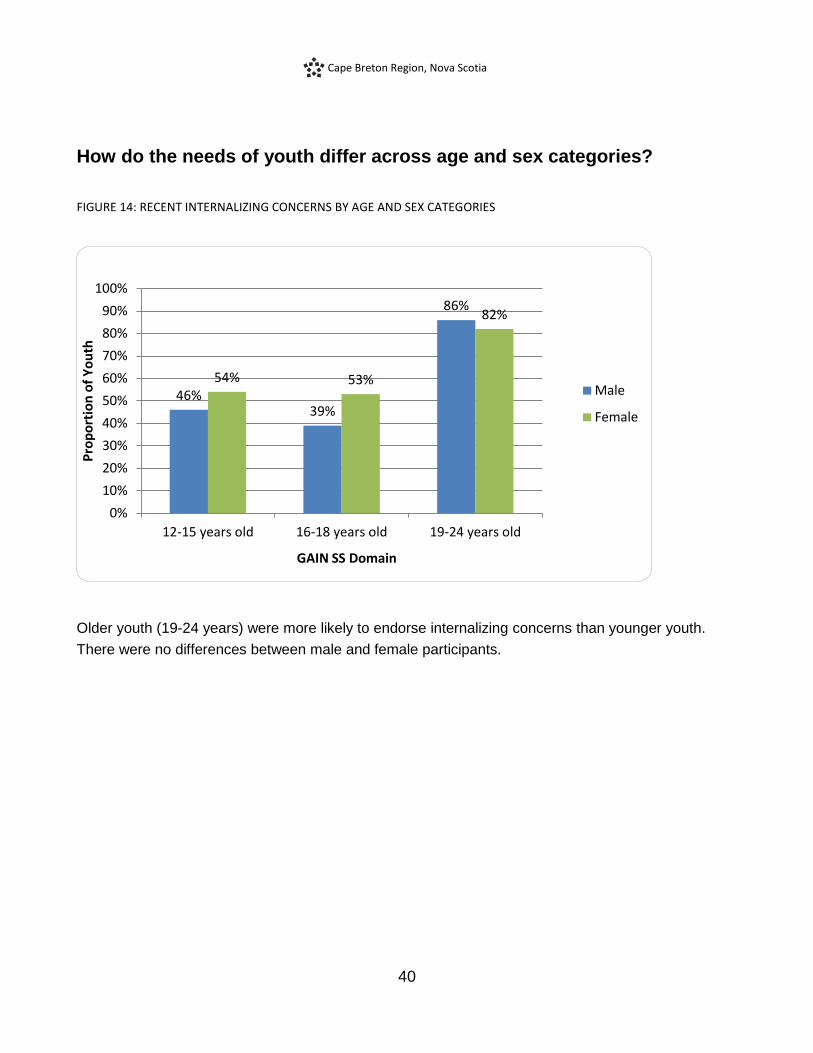
How do the needs of youth differ across age and sex categories?
FIGURE 14: RECENT INTERNALIZING CONCERNS BY AGE AND SEX CATEGORIES
Older youth (19-24 years) were more likely to endorse internalizing concerns than younger youth.
There were no differences between male and female participants.
46% 39%
86%
54% 53%
82%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
12-15 years old 16-18 years old 19-24 years old
Pro
po
rtio
n o
f Y
ou
th
GAIN SS Domain
Male
Female
Cape Breton Region, Nova Scotia
41
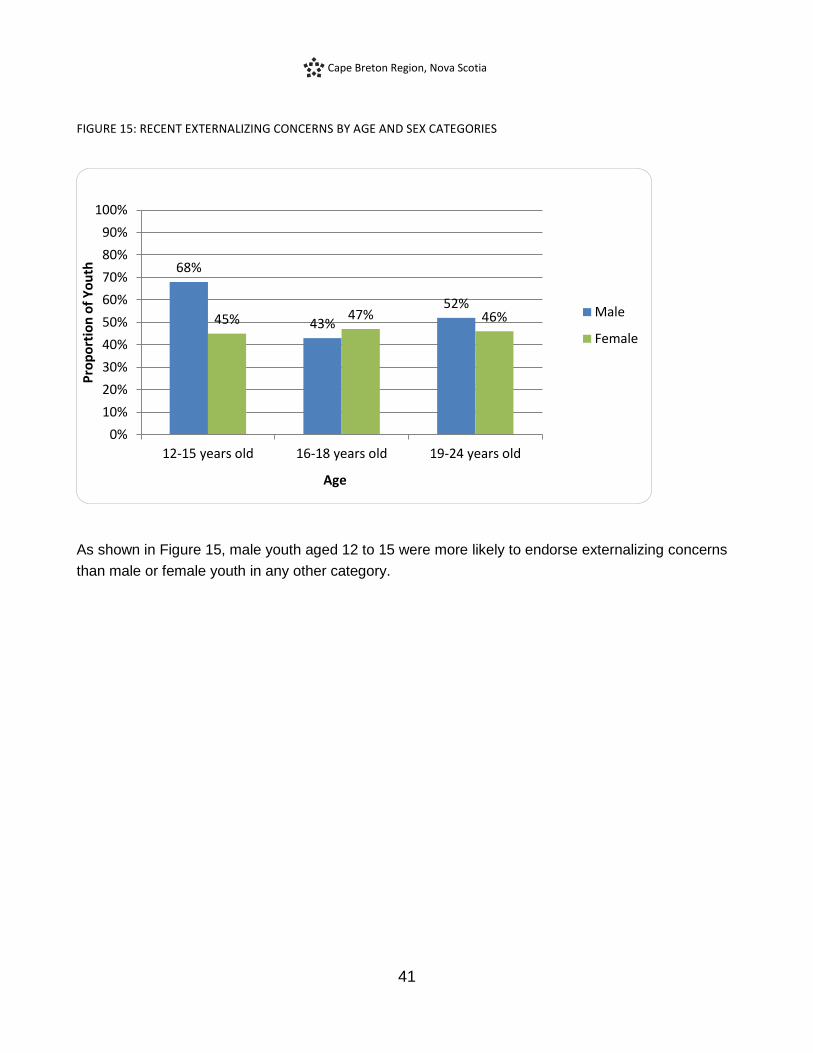
FIGURE 15: RECENT EXTERNALIZING CONCERNS BY AGE AND SEX CATEGORIES
As shown in Figure 15, male youth aged 12 to 15 were more likely to endorse externalizing concerns
than male or female youth in any other category.
68%
43%
52% 45% 47% 46%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
12-15 years old 16-18 years old 19-24 years old
Pro
po
rtio
n o
f Y
ou
th
Age
Male
Female

Cape Breton Region, Nova Scotia
42
FIGURE 16: RECENT SUBSTANCE USE CONCERNS BY AGE AND SEX CATEGORIES
Male youth aged 19 to 24 were more likely to endorse problematic substance use concerns than
same aged female youth. Older youth were also more likely to endorse substance use concerns than
younger youth.
21% 26%
67%
13%
25%
43%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
12-15 years old 16-18 years old 19-24 years old
Pro
po
rtio
n o
f Y
ou
th
Age
Male
Female

Cape Breton Region, Nova Scotia
43
FIGURE 17: RECENT CRIME AND VIOLENCE CONCERNS BY AGE AND SEX CATEGORIES
Crime and violence problems were more commonly endorsed by male youth than female youth,
especially male youth in the oldest age category.
17% 19% 27%
7% 11%
7%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
12-15 years old 16-18 years old 19-24 years old
Pro
po
rtio
n o
f Y
ou
th
Age
Male
Female
Cape Breton Region, Nova Scotia
44
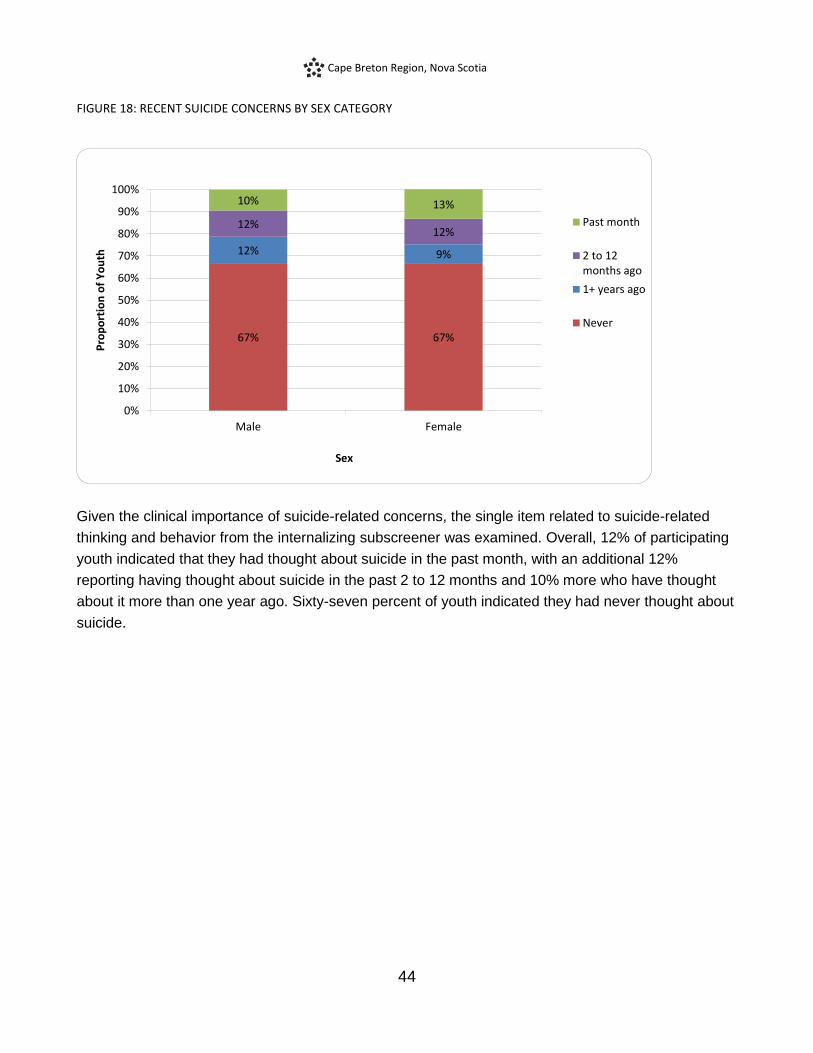
FIGURE 18: RECENT SUICIDE CONCERNS BY SEX CATEGORY
Given the clinical importance of suicide-related concerns, the single item related to suicide-related
thinking and behavior from the internalizing subscreener was examined. Overall, 12% of participating
youth indicated that they had thought about suicide in the past month, with an additional 12%
reporting having thought about suicide in the past 2 to 12 months and 10% more who have thought
about it more than one year ago. Sixty-seven percent of youth indicated they had never thought about
suicide.
67% 67%
12% 9%
12% 12%
10% 13%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Male Female
Pro
po
rtio
n o
f Y
ou
th
Sex
Past month
2 to 12months ago
1+ years ago
Never

Cape Breton Region, Nova Scotia
45
FIGURE 19: RECENT SUICIDE CONCERNS BY AGE AND SEX CATEGORIES
When we examined rates of endorsement by sex and age category, it was revealed that male youth
aged 19 to 24 were more likely to endorse suicide concerns than younger male youth. Also, in the 16-
18 age group, female youth were more likely to report recent thoughts of suicide than same aged
male youth.
18% 13%
34%
24% 25% 28%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
12-15 years old 16-18 years old 19-24 years old
Pro
po
rtio
n o
f Y
ou
th
Age
Male
Female

Cape Breton Region, Nova Scotia
46
Other Clinical Needs
How many youth endorsed additional areas of concern?
As part of the process of meeting the needs of service sector stakeholders, and with the permission of
Chestnut Health Systems, the copyright holders of the GAIN SS, we added 7 items to the end of the
GAIN SS. The items that were added were not part of the original GAIN SS nor the validation study
(Dennis et al., 2006), and as a result their reliability, validity, and utility are unknown. Nevertheless, it
was identified by stakeholders that it would be important to ask about other areas of concern expected
to be important for the youth participants so that these areas could be explored further if youth
indicated any concerns. The items were from the areas of eating concerns (2 items), traumatic stress
(1 item), disordered thinking concerns (2 items), gambling concerns (1 item) and gaming/internet
concerns (1 item).
FIGURE 20: RATES OF RECENT ADDITIONAL CONCERNS BY SEX CATEGORIES
Across male and female youth, the distressing memories/dreams (traumatic distress) item was
endorsed by approximately half of youth and was the most commonly endorsed additional item. Youth
were least likely to endorse concerns about gambling. Female youth were significantly more likely to
endorse eating concerns and traumatic distress compared to male youth.
8% 12%
39% 34%
15%
25%
4%
29% 28%
50%
34%
15% 17%
1% 0%
10%20%30%40%50%60%70%80%90%
100%
Pro
po
rtio
n o
f Y
ou
th
Additional Concerns
Male
Female
Cape Breton Region, Nova Scotia
47
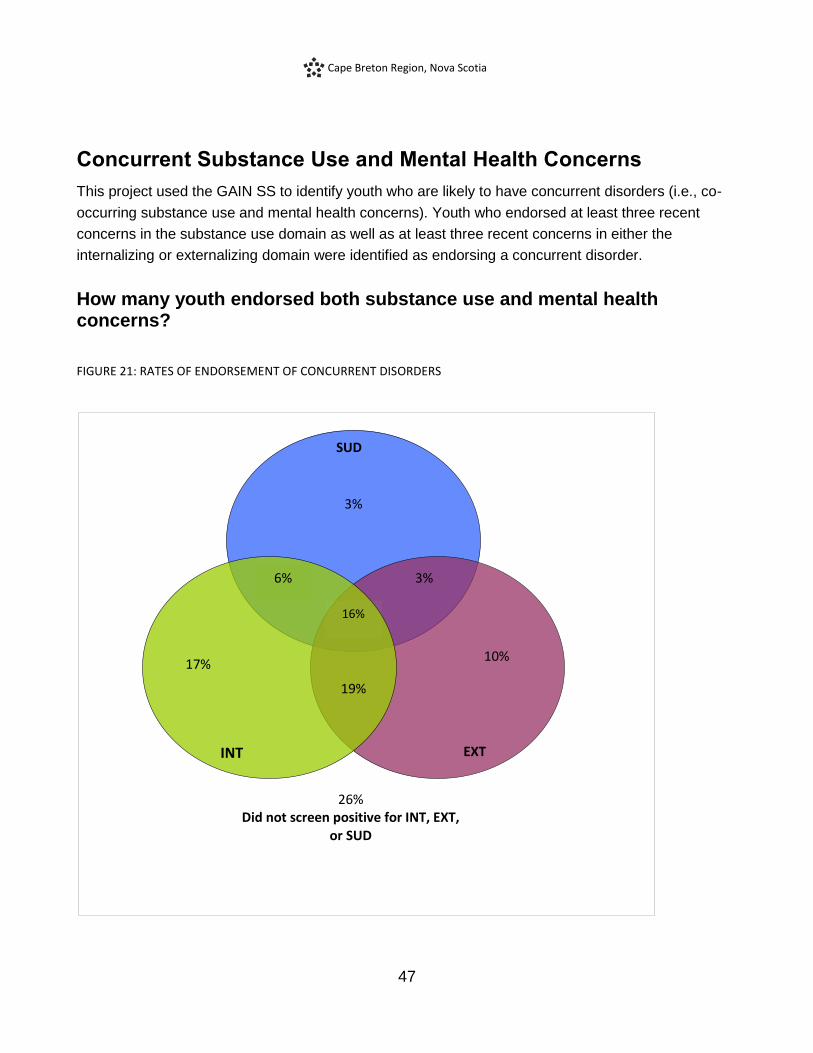
Concurrent Substance Use and Mental Health Concerns
This project used the GAIN SS to identify youth who are likely to have concurrent disorders (i.e., co-
occurring substance use and mental health concerns). Youth who endorsed at least three recent
concerns in the substance use domain as well as at least three recent concerns in either the
internalizing or externalizing domain were identified as endorsing a concurrent disorder.
How many youth endorsed both substance use and mental health concerns?
FIGURE 21: RATES OF ENDORSEMENT OF CONCURRENT DISORDERS
SUD
EXT
6%
17% 10%
19%
3%
16%
26% Did not screen positive for INT, EXT,
or SUD
3%
INT

Cape Breton Region, Nova Scotia
48
Overall, 44% of youth screened positive for more than one area of concern, and 25% of participating
youth screened positive for possible concurrent (substance and mental health) disorders (i.e.
excluding the 26% who did not screen positive for internalizing, externalizing, or substance use
disorders). As can be seen in the Figure 21, 16% of all participating youth screened positive for co-
occurring internalizing, externalizing and substance use concerns, 6% endorsed concurrent
internalizing and substance use concerns, and 3% indicated concurrent externalizing and substance
use concerns. When we examined just those youth who screened positive we found that 88%
screened positive for internalizing concerns and problematic substance use, 76% screened positive
for externalizing concerns and problematic substance use, and 64% screened positive for both
internalizing and externalizing concerns, as well as significant substance use concerns.
Cape Breton Region, Nova Scotia
49
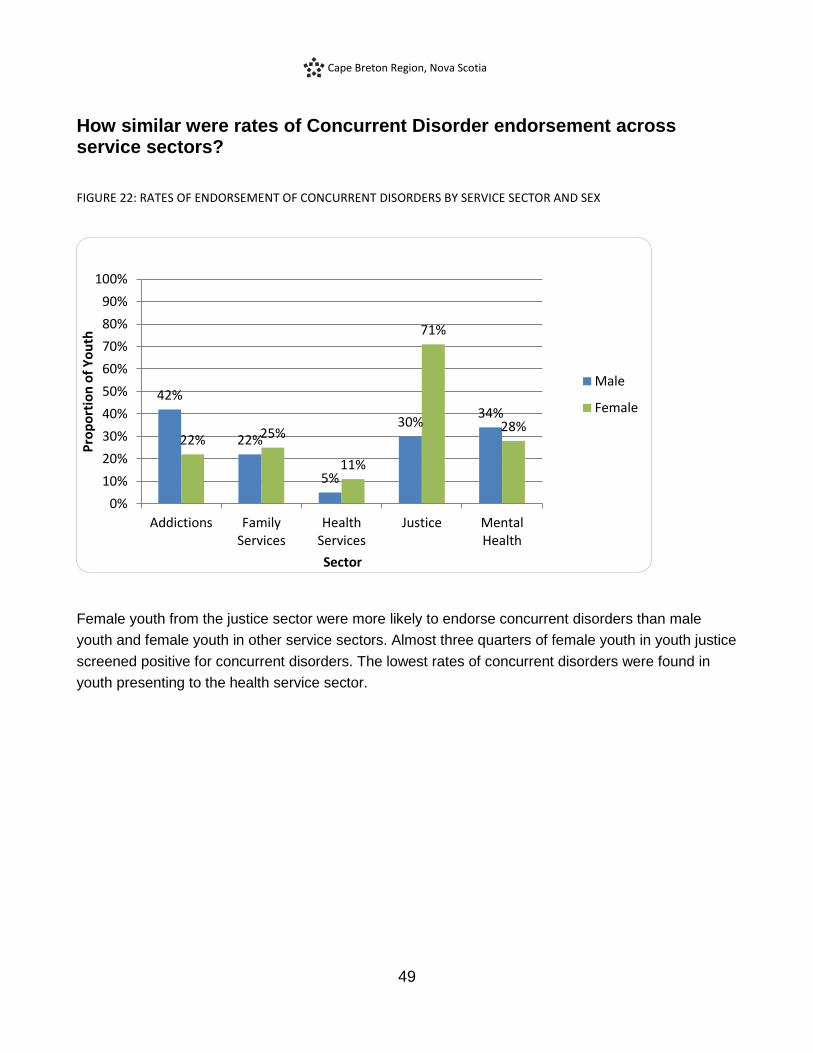
How similar were rates of Concurrent Disorder endorsement across service sectors?
FIGURE 22: RATES OF ENDORSEMENT OF CONCURRENT DISORDERS BY SERVICE SECTOR AND SEX
Female youth from the justice sector were more likely to endorse concurrent disorders than male
youth and female youth in other service sectors. Almost three quarters of female youth in youth justice
screened positive for concurrent disorders. The lowest rates of concurrent disorders were found in
youth presenting to the health service sector.
42%
22%
5%
30% 34%
22% 25%
11%
71%
28%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Addictions FamilyServices
HealthServices
Justice MentalHealth
Pro
po
rtio
n o
f Y
ou
th
Sector
Male
Female
Cape Breton Region, Nova Scotia
50
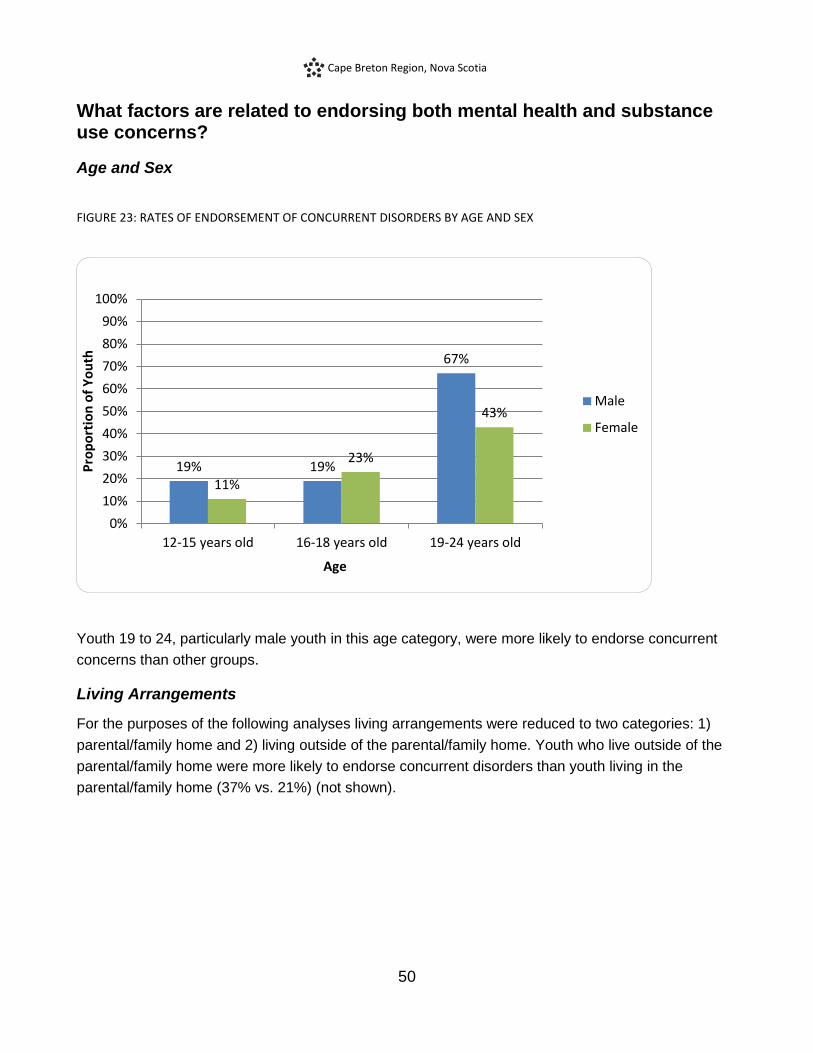
What factors are related to endorsing both mental health and substance use concerns?
Age and Sex
FIGURE 23: RATES OF ENDORSEMENT OF CONCURRENT DISORDERS BY AGE AND SEX
Youth 19 to 24, particularly male youth in this age category, were more likely to endorse concurrent
concerns than other groups.
Living Arrangements
For the purposes of the following analyses living arrangements were reduced to two categories: 1)
parental/family home and 2) living outside of the parental/family home. Youth who live outside of the
parental/family home were more likely to endorse concurrent disorders than youth living in the
parental/family home (37% vs. 21%) (not shown).
19% 19%
67%
11%
23%
43%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
12-15 years old 16-18 years old 19-24 years old
Pro
po
rtio
n o
f Y
ou
th
Age
Male
Female

Cape Breton Region, Nova Scotia
51
Legal Involvement
FIGURE 24: RATES OF ENDORSEMENT OF CONCURRENT DISORDERS BY LEGAL SYSTEM INVOLVEMENT
For the purposes of the following analyses, legal involvement was reduced to two categories: 1) no
legal involvement and 2) previous legal involvement. Youth who reported past legal involvement were
more likely to endorse concurrent disorders (46%) than youth who reported no previous involvement
with the legal system (16%) and indeed, more than half of youth (54%) who screened positive for
concurrent disorders reported previous legal involvement. Male youth who reported legal involvement
were more likely to endorse concurrent disorders than female youth who reported legal involvement.
Educational Status
When we compared youth who identified as students to those who did not, it was revealed that while
18% of students endorsed concurrent substance use and mental health concerns, almost a third
(32%) of non-students screened positive for concurrent disorders.
55%
45%
80%
20%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
No legal involvement Previous legal involvement
Pro
po
rtio
n o
f Y
ou
th
Legal Involvement
Male
Female
Cape Breton Region, Nova Scotia
52
Which factors are most important in understanding the Concurrent Disorder needs of youth presenting for service in Cape Breton Region?
Given that a number of factors were found to be related to endorsing both problematic substance use
and mental health concerns, and that a number of these factors were related to each other (e.g., age
and living arrangements), we examined all of these factors together in one model to understand which
factor(s) are most important in understanding who screens positive for concurrent disorders. The
factors included in this analysis were age, sex, service sector, living arrangements, legal involvement
and educational status. When all of these factors were considered together age, service sector, and
legal involvement were shown to be most important in understanding which youth are more likely to
endorse both substance use and mental health concerns. More specifically, older youth, particularly
youth aged 19 to 24 were more likely to endorse both substance use and mental health concerns. In
addition, even when we controlled for differences associated with age and the other factors, youth
who presented to the health services sector were significantly less likely to endorse mental health and
substance use concerns. Lastly, even after controlling for the impact of other factors like age and sex,
youth who had legal involvement were more likely to endorse concurrent concerns.
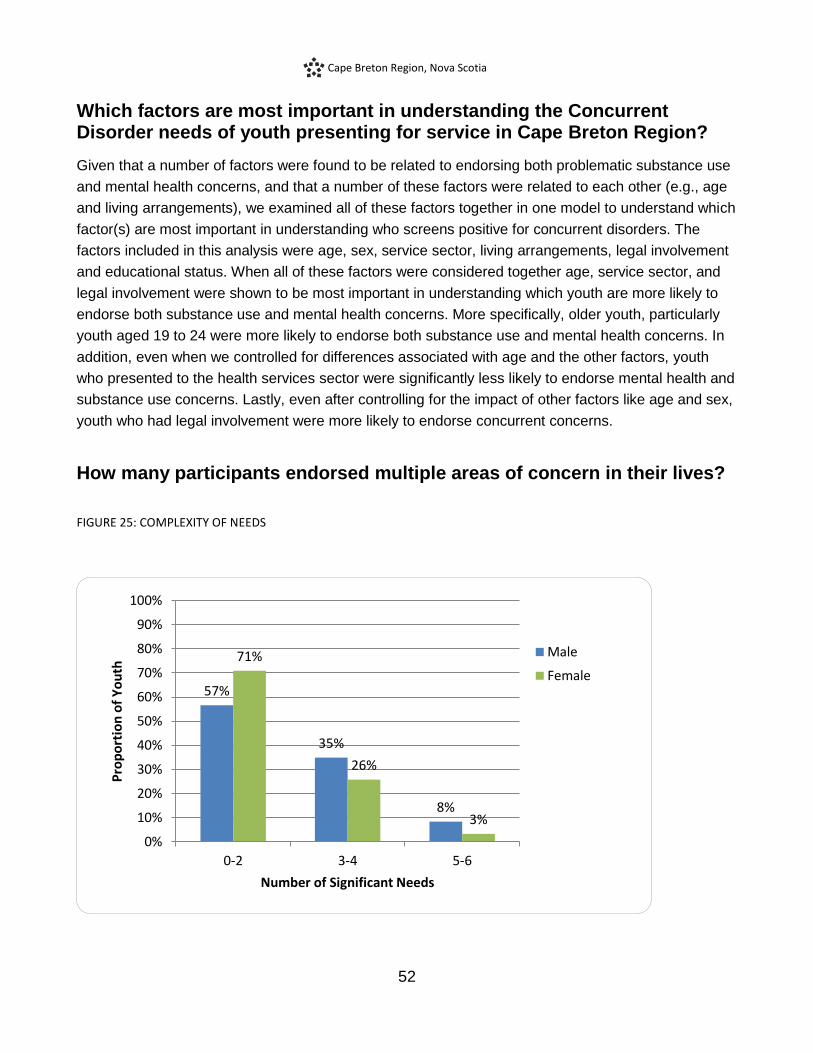
How many participants endorsed multiple areas of concern in their lives?
FIGURE 25: COMPLEXITY OF NEEDS
57%
35%
8%
71%
26%
3%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0-2 3-4 5-6
Pro
po
rtio
n o
f Y
ou
th
Number of Significant Needs
Male
Female
Cape Breton Region, Nova Scotia
53
In order to understand how many participants experience multiple areas of concern we also examined
the following social determinants of health, along with mental health and substance use concerns: 1)
housing (unstable or supportive), 2) education/occupation (under 18 and not a student or 18 and older
and not a student and not employed), 3) legal involvement (past or current legal involvement), 4)
internalizing concerns (high severity), 5) externalizing concerns (high severity), and 6) substance use
problems (high severity). Notably, 34% of participants reported having 3 or more factors and 5% of
participants reported experiencing 5 or more of the 6 factors. These findings highlight the complexity
of the needs of the individuals who are presenting for service and participated in this project.
Cape Breton Region, Nova Scotia
54
Service Provider Survey
This project included a survey about service providers’ attitudes, knowledge, and practices regarding
youth substance use, mental health, and concurrent disorders. Questions about interagency
collaboration and interagency referral practices were also included in the survey. In addition, the
project included a feedback survey that gathered information regarding the feasibility, utility, and
impact of using the GAIN SS.
Service providers in the Cape Breton Region (n = 120) completed the service provider survey prior to
participating in the project’s capacity building training event and then again with the feedback survey
(n = 39) approximately one year after training took place. Detailed results for the service provider
survey can be found in the National Youth Screening Project national report.The results from the
feedback survey of Cape Breton Region service providers are presented following.
Service provider comments about administering the GAIN SS:
“I liked that the tool was brief but still covered a range of behavioral issues. Also
it is effective in that it helps link the individual to the appropriate service,
regardless of their entry point.”
“Concern reflecting on screening tool being (for) the purposes of research
probably resulted in lack of participation by service providers in the data
collection phase”
“GAIN-SS was a great addition to services’ intake systems and youth were willing
to complete the screening tool.”
Cape Breton Region, Nova Scotia
55
Feasibility and Utility of the GAIN SS
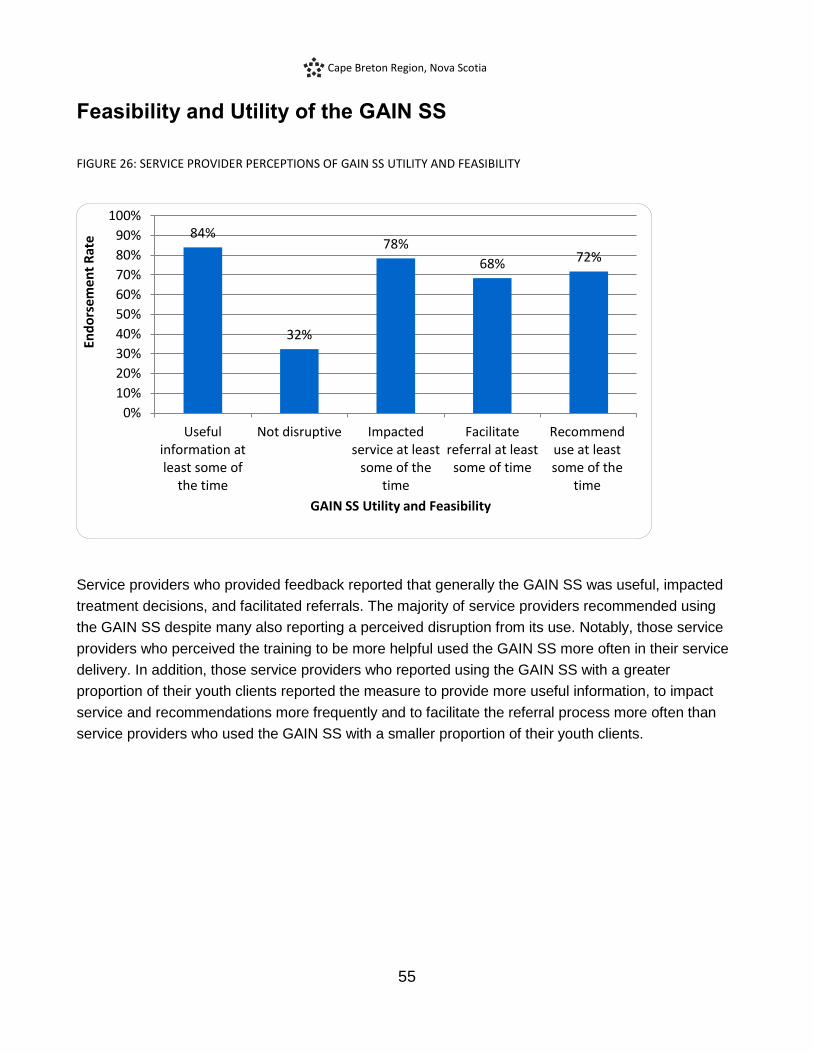
FIGURE 26: SERVICE PROVIDER PERCEPTIONS OF GAIN SS UTILITY AND FEASIBILITY
Service providers who provided feedback reported that generally the GAIN SS was useful, impacted
treatment decisions, and facilitated referrals. The majority of service providers recommended using
the GAIN SS despite many also reporting a perceived disruption from its use. Notably, those service
providers who perceived the training to be more helpful used the GAIN SS more often in their service
delivery. In addition, those service providers who reported using the GAIN SS with a greater
proportion of their youth clients reported the measure to provide more useful information, to impact
service and recommendations more frequently and to facilitate the referral process more often than
service providers who used the GAIN SS with a smaller proportion of their youth clients.
84%
32%
78%
68% 72%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Usefulinformation atleast some of
the time
Not disruptive Impactedservice at least
some of thetime
Facilitatereferral at leastsome of time
Recommenduse at leastsome of the
time
End
ors
emen
t R
ate
GAIN SS Utility and Feasibility

Cape Breton Region, Nova Scotia
56
Service provider comments about the feasibility and utility of the GAIN SS in their
practices
Agency context, service provider role and mandate impacted perception of
feasibility and utility, disruption and clinical benefit of administering the GAIN SS:
“If use of the GAIN could have been disruptive, I didn't use it. Rarely did any
additional information result from the completed GAIN”
“Easy to administer - very useful screening tool”
“The GAIN-SS has been an asset to the work I do with youth. It is a great tool to
facilitate dialogue with youth as well as direct referrals.”
“I found it very helpful - great segue into resources available; over time youth
more open to referral.”
“I have found this tool useful in getting a sense of where our youth are at in their
lives and also in assisting us in providing the best and most relevant service to
them”
“I found it to be a good tool for screening of concurrent disorders in the youth
population and it helped me to generate further discussions related to their
responses.”
Cape Breton Region, Nova Scotia
57
Summary of Findings
Approximately 79% of eligible youth presenting to participating services and agencies contributed to
this report.
95% of youth who completed the GAIN SS gave consent for it to be included in this report.
Youth presenting for services from addictions, family services, health, justice and mental health
service sectors contributed information to this report.
Youth from the whole age range (12-24 years) participated, with differences in age being apparent
across service sectors.
The majority of participants were female, and the health sector had significantly more female
participants than other sectors.
The majority of participants identified their ethnicity as White/European, reported being born in
Canada and having English as their first language.
Male youth, older youth and youth presenting for service to the family services sector endorsed a
wider variety of current living arrangements and were less like to live in the parental/family home.
Almost half of male youth and one fifth of female youth indicated that they had experienced legal
involvement.
The majority of participating youth screened positive for significant internalizing or externalizing
mental health concerns and/or problematic substance use. Moreover, substantial numbers of youth
from each sector endorsed significant difficulties.
Age and sex are related to rates of endorsement across domains.
Almost one quarter of participating youth reported significant suicide-related concerns in the past
year.
Almost half of participating youth (44%) screened positive for more than one disorder and 25% of
youth screened positive for co-occurring mental health and substance use concerns.
Factors found to be significantly related to experiencing co-occurring mental health and substance
use concerns for youth participating in the project include age, sex, service sector, living
arrangements, legal involvement, and student status. Of these the most important appear to be age,
legal involvement and service sector. Younger youth, youth presenting for service to health
services, and those without previous legal involvement were less likely to endorse concurrent
mental health and substance use concerns.
The majority of service providers reported that they found the GAIN SS provided useful information,
impacted service delivery and facilitated referrals. Higher ratings in these areas were associated
with service provider perceptions of the capacity building activities and their use of the GAIN SS.
Those service providers who found the training more helpful and those who used the tool with more
of their youth clients, found the GAIN SS more useful and perceived it to impact service and
facilitate referrals more frequently.

Cape Breton Region, Nova Scotia
58
Discussion Youth Needs
The findings of this project in Cape Breton Region, Nova Scotia suggest that many youth presenting
for service, regardless of which sector they present to, are experiencing significant substance use
and/or mental health concerns. Moreover, almost half of participating youth endorsed significant
concerns in more than one domain, and one quarter of youth screened positive for co-occurring
substance and mental health concerns. These findings suggest that recent efforts to improve capacity
to address co-occurring substance use and mental health problem are warranted.
The findings of this report also support the need for gender-sensitive and developmentally-informed
approaches with youth. The concerns and needs of male and female youth differed, as did the needs
and concerns of younger and older youth. For example, 16 to 18 year old girls were more likely to
report suicide-related concerns than boys, but in the older age category males and females did not
differ significantly, with older male youth experiencing significantly more suicide-related concerns than
younger male youth. Also, the health sector saw a greater proportion of female youth than other
sectors and the justice sector had more male youth than other sectors.
These, and other findings from the project, have implications for service delivery, both in terms of
thinking about issues such as access, but also in terms of what services might be most applicable at
different ages and for male and female youth. Unfortunately the number of youth who identify as trans
who participated was too small to allow for meaningful analyses. Future projects should aim to better
understand the needs of this often overlooked group of youth.
Project and Implementation Processes
As described in this report there were several essential steps required to initiate, carry out and
complete this project. First and foremost, local leadership was required to build a network through
identifying, engaging and supporting partners from various youth service sectors. In the Cape Breton
Region, the interest, support, and enthusiasm of the network lead and ultimately the sustained hard
work of the network coordinator resulted in Cape Breton being the first community to launch and
complete the project. They exceeded their initial agreement to enlist partners representing three
service sectors; rather, enlisting seven (addictions, mental health, health, youth justice, family service,
child welfare and education). Service providers from all seven sectors participated in the network
development and capacity building activities. Ultimately, due to administrative challenges including
staff turnover, agencies representing five sectors, excluding child welfare and education, participated
in all the project activities (See Appendix C).

Cape Breton Region, Nova Scotia
59
Providing more than one capacity building event, including teleconference training options for those
who could not attend the “live” events, provided greater opportunity for all agency staff to receive
training directly from the project leads. This helped to ensure that all aspects of the protocol were
clearly and consistently communicated. Agencies decided to send staff who would participate in the
full project as well as staff who might use the screening tool with populations that were not part of this
project (e.g., adults older than 24 years), as well as staff who would not be administering the
screener, given their role in the agency but might receive youth who had been screened. As such, the
capacity building component of the project had a broader reach than initially anticipated.
Staff concerns about potential challenges in engaging youth in screening and research processes are
a common barrier to engaging service providers and community-based agencies in projects such as
this one. The findings in Cape Breton from this project indicate that most youth who completed the
screener, also agreed to participate in the research component of the project. This is very
encouraging with respect to the feasibility of such initiatives and the potential of projects such as this
to learn more about youth needs.
Following completion of data collection, through the project coordinator, the project team learned that
GAIN SS administration was continuing in some agencies beyond the six month project data
collection phase. Some agencies and services (e.g. CBDHA Addictions and Mental Health services),
were planning to implement policies and protocols to establish on-going consistent implementation of
the GAIN SS in their services. As well, some of the agencies that didn’t participate in the formal data
collection portion of the project, nonetheless, had implemented the GAIN SS in their agencies. This
highlights the importance of considering unanticipated consequences and suggests that an initiative
such as this project may have the potential to significantly impact agency policy and protocol.
Limitations
The findings of this project are limited by a few important factors. The system to capture the extent to
which the sample is representative of youth typically presenting to the participating services (service
provider completed tracking sheets) has limitations and the data indicate that some tracking sheets
were not completed, although the extent of the problem is not clear. As a result, the relevance of the
findings to youth who did not participate is not clear. Secondly, the screening tool is a high level
screening tool intended to identify youth who would be likely to have a diagnosis with a full
assessment and who thus would benefit from assessment and service planning. As a result, it does
not provide detailed information about the areas of concern that are identified. Lastly, different service
providers and services engaged with the project to differing extents which may have impacted the
findings in unknown ways.

Cape Breton Region, Nova Scotia
60
Recommendations
Gender-informed and gender-specific services should be considered to ensure that links to all
necessary services are available where male and female youth are more likely to present for service
and to ensure that once accessed, the services that are delivered are designed to address the
different types of difficulties male and female youth experience. Further research is needed to address
the needs of youth who identify as trans or other youth who do not identify as solely male or female.
Developmentally informed and responsive services are indicated in order to meet the needs of
transitionally aged youth (19 to 24 years), especially those who are seeking and/or receiving services
in the adult service sector.
Continued capacity building regarding concurrent disorders across sectors is warranted given that
almost half of participants endorsed significant concerns in two or more domains. This project aimed
to improve early identification and pathways to care through evidence-based practice in the form of
screening using a standardized tool. Subsequent projects should consider the importance of capacity
building regarding interventions to address concurrent disorders.
Building capacity for trauma-informed care across sectors is also suggested, given that
approximately half of the youth endorsed concerns related to traumatic distress.
The finding that one of the strongest predictors of screening positive for concurrent disorders was
previous legal involvement highlights the importance of early screening and follow-up for youth who
come in contact with the justice sector. Consideration of strategies such as screening youth who have
early police contact for emerging substance use and/or mental health difficulties may identify
opportunities for earlier intervention, rather than waiting for serious legal problems and/or for serious
substance use and/or mental health problems.
The impact of social determinants of health on the manner and type of services available to youth
should continue to be explored. For example, youth who had living arrangements outside the
parental/family home had higher rates of screening positive for co-occurring substance use and
mental health concerns, but this finding did not hold up when the relationship between older age and
the increased likelihood of concurrent concerns was taken into account. Nevertheless, since this
project only included a relatively small sample of youth with non-family home living arrangements, it
may be the case that with a larger sample of youth with non-family living arrangements more would be
learned and important service needs unique to this group would be identified.
Implementation of consistent screening in sectors such as health where youth have the lowest rates
of screening positive for problematic substance use and mental health concerns provides an excellent
opportunity for early identification and intervention, while not using expensive specialized resources.
Consideration should be given to gathering similar information as was gathered through this project in

Cape Breton Region, Nova Scotia
61
other health care settings such as community based primary care and hospital emergency rooms
and/or in other highly accessible settings such as educational settings.
While this project examined youth needs at one point in time in service delivery, consideration
should be given to the potential utility of repeating administration of the screening tool at subsequent
points in the service delivery process for the purposes of monitoring within treatment progress and
post-treatment outcomes.
Further study is also recommended to examine the relative impacts of training, agency policy,
protocols, monitoring, supervision and administrative support on implementation of new practices,
such as the implementation of a consistent screening tool and process, as was examined in this
project.

Cape Breton Region, Nova Scotia
62

Cape Breton Region, Nova Scotia
63
Appendices

Cape Breton Region, Nova Scotia
64
Cape Breton Region, Nova Scotia
65
Appendix A: Cape Breton Network Member Agency Descriptions
Cape Breton District Health Authority: Addiction Services
Addiction Services provides comprehensive prevention, education and treatment services to
individuals, families and communities affected by substance abuse and/or gambling.
Community Based Services:
Community Based Services provides a comprehensive range of assessment, intervention,
consultation and treatment services. Referrals may be made by family members, professionals,
members of self-help groups or may be self-referrals. Programs offered through CBS include Adult
Counselling, Adolescent Counselling, Women's Services, Problem Gambling Counselling, and
Addiction Day Program.
Health Promotion & Prevention Services: Adolescent Services:
The CBDHA Addictions Adolescent team offers health promotion and addiction prevention for teens.
The team offers individual early intervention counselling with Adolescent Outreach Workers and three
youth group programs on a regular basis throughout the year. Any youth 13 – 18 years of age is
eligible to connect with an adolescent outreach worker who is present both in schools and in the
community.
Inpatient Withdrawal Management Unit:
Inpatient Withdrawal Management (or IWMU) is an 18 bed unit located at the Cape Breton Regional
Hospital. The inpatient unit manages the acute phase of withdrawal in a safe, therapeutic
environment.
Opiate Recovery Program:
The Opiate Recovery Program provides methadone maintenance treatment in a community setting. It
is one component of a comprehensive prevention and treatment strategy to help those struggling with
opiate dependence and related harms. The Opiate Recovery Program offers: Medical evaluation and
ongoing assessment; daily dosing of methadone at a community retail pharmacy; random drug
screening; methadone education and support groups; short and long term outpatient counselling and
ongoing assessment; referrals, collaboration and assistance navigating additional healthcare needs
and social supports.
Cape Breton Region, Nova Scotia
66
Cape Breton District Health Authority: Mental Health Services
Mental Health Services is a district-wide program that offers a broad range of general and specialized
inpatient, outpatient and community-based mental health services to residents of all ages across the
continuum of care.
Adult Mental Health:
Adult Outpatient Mental Health Services serves a population within the following mental disorders:
Major Mental Disorders, Neurodevelopment Disorders, Adjustment Disorders, and Personality
Disorders, and it works with communities to provide appropriate, compassionate and integrated
emergency outpatient mental health services. The MHS services focus on quality of life through
prevention, early identification and intervention, treatment, support, consultation, community
partnerships, education and research. Referrals are accepted from any source, including self
referrals. The intake nurse screens all intakes to ensure appropriateness of the referral based on the
target population and the catchment area of the particular clinic.
Child and Adolescent Services:
Child and Adolescent Services is an outpatient service involving a multidisciplinary team approach
including psychology, psychiatry, social work and in-home behavioural interventionists. The service
provides assessment and treatment for children up to age 19 and their families, for a wide range of
mental health disorders. The service includes the Intensive Community-Based Treatment Team, the
N.S. Initiative for Sexually Aggressive Youth and the Autism Intervention Program as well as part-time
clinical services in North Sydney, Glace Bay, Baddeck and Neil's Harbour.
Emergency Crisis Service:
Through the Emergency Crisis Program at the Cape Breton Regional Hospital, anyone whose life or
well being is at risk and who requires immediate care can receive emergency mental health services
24 hours a day, seven days a week.
Inpatient Mental Health Services:
This service consists of three units located at the Cape Breton Regional Hospital for patients generally over the age of 16 years.
Unit 1C: a short stay, eight-bed unit for patients with an expected length of stay of five to seven days.
It provides comprehensive assessment and stabilization for individuals in crisis who require 24-hour
supervision and care.
Unit 1B: a 22-bed unit for patients with an expected length of stay of one to six weeks, providing a
range of individual and group treatment approaches.
Unit 1D: a 16-bed unit with a rehabilitation focus for patients requiring longer stays to support their
recovery and eventual move back into the community.

Cape Breton Region, Nova Scotia
67
Cape Breton District Health Authority (CBDHA): Youth Health Centres
Youth Health Centre (YHC) provide youth with confidential access, coordination and referral to a
comprehensive range of services available in the community that address their health needs. These
centres provide health education, health promotion, information and referral, follow-up and support, as
well as some clinical services. Although youth health centres provide information on a wide range of
health issues, they are also a key source of sexual health information for youth. Some services
offered through the YHCs include STI testing, education, and support regarding healthy choices,
dating, relationships, bullying, and nutrition. Services are available to youth up to age 19.
Cape Breton Victoria Regional School Board
Cape Breton-Victoria Regional School Board is committed to providing the best educational programs
and services to our children and community. The School Board strives to build strong basic
educational skills and augment these attributes by challenging the most sophisticated learner. It is
noted for its diversity in all programs. Additionally, the board has developed “state of the art”
technology laboratories with a district-wide computer network system.
The Board covers a vast area, encompassing urban and rural settings in two municipalities-Cape
Breton Regional Municipality and Victoria County. CBVRSB provides educational services to over
18,000 students in more than 56 schools, as well as 185 adult learners in four Adult education
Centres. These educational services are provided using a significant commitment of resources. Our
board also has two Learning Centres (Excerpt taken from www.cbv.ns.ca).
Department of Community Services: Child Welfare
This Intake / Investigation Team is the entry point for the Department of Community Service Child
Welfare regarding concerns of child abuse and neglect under the Children and Family Services Act.
The team consists of admin workers, social workers and family support workers. The team determines
if it is ‘fit’ to act, the time needed to respond, and it creates an intervention plan and assigns a social
worker to the case. A case plan is developed in consultation with the parents (caregivers) to reduce
the risk of future harm to the children and to outline the basis of our involvement. In the vast majority
of cases the matters are rectified at the Intake level. More complex cases can be transferred to the
Open Protection Unit, or can lead to court ordered interventions to ensure the protection of the
children.
Department of Justice: Community Corrections
Department of Justice - Community Corrections provides supervision to the youth sentenced to court
ordered community dispositions from the ages of 12-17. Amongst this supervision is support by
referral to outside agencies to address the young person’s needs. Community Corrections also
provides youth with “Options to Anger”, “Girls Circle” and Voices (for female youth). These programs
are offered by staff when operationally possible.

Cape Breton Region, Nova Scotia
68
Family Services of Eastern Nova Scotia
Family Services of Eastern Nova Scotia provides professional counselling services on a wide range of
issues based on their mandate: To promote and strengthen families and individuals in the building of
a just and supportive society, and to preserve the sanctity of the family unit. Family Life programs are
also offered to groups with topics ranging from self-esteem, stress/anger management, parenting,
adolescent issues, and young children. The agency also serves as the provider of Marriage
Preparation Courses throughout the service area.

Cape Breton Region, Nova Scotia
69
Appendix B: Key Project Activity Descriptions
Network Development
Member agencies that participated in the Network Development activity played a foundational role in
building a collaborative network, starting with preliminary discussions regarding project participation.
These agencies participated in several meetings with the project team, in addition to network specific
meetings and training. The agency leads and broader network membership also collaborated with the
project team to carry out the project.
Capacity Building
Service providers and agency leads from interested agencies participated in a half-day evidence-
based youth co-occurring disorders capacity building session and a half-day screening and
intervention protocol training session. During this session, where agencies had committed to full
project participation and had obtained research ethics approval, service providers also completed the
Service Provider Survey. Some agencies that participated in the Capacity Building activities were
interested in participating in the full project but were not able to due to resource or administrative
challenges, such as difficulties completing legal and/or ethics processes in the required network
timeframe.
Screening Implementation
Member agencies that participated in the full project implemented the GAIN SS with youth seeking
services at their agencies. Some agencies chose to implement the GAIN SS with the youth seeking
service for clinical purposes, but did not participate in the full data collection component of the project
(see below).
Data Collection
Member agencies that participated in the full project participated in a six month data collection period.
During this time, the GAIN SS and Background Information Form were administered to youth seeking
service at their agencies and, with consent, a copy was sent to the project team. The data was
prepared by the project team and a local community report was generated through a collaborative
process between the project team and the participating agencies.

Cape Breton Region, Nova Scotia
70
Appendix C: Agency Project Activity Participation
SECTOR Agency name
Project activity
Network Development
Capacity Building
Screening Implementation
Data Collection
Addictions
Cape Breton District Health Authority • Community Based
Services • Health Promotion and
Prevention: Adolescent Services
• Inpatient Withdrawal Management Unit
• Opiate Recovery Program
● ● ● ●
Child welfare
Department of Community Services: Child Welfare
● ●
Education
Cape Breton Victoria Regional School Board
● ●
Family services
Family Services of Eastern Nova Scotia
● ● ● ●
Mental health
Cape Breton District Health Authority • Adult Mental Health • Child and Adolescent
Services • Emergency Crisis
Service • Inpatient Mental Health
Services
● ● ● ●
Health
Cape Breton District Health Authority • Youth Health Centres
● ● ● ●
Justice
Department of Justice: Community Corrections
● ● ● ●

Cape Breton Region, Nova Scotia
71
Appendix D: Project Timeline
Year 1 Year 2 Year 3
2010 2011 2012 2013
Apr - Jun
July - Sept
Oct - Dec
Jan - Mar
Apr – Jun
July - Sept
Oct - Dec
Jan - Mar
Apr - Jun
July - Sept
Oct - Dec
Jan - Mar
Networking: Introduce project to potential participating agencies
Establish cross-sectoral network: REB Approval & Signing of MOU
Training for participating agencies
Project launch
Project actively underway
Preliminary findings presented
Report to stakeholders
Legend
Cape Breton Region, Nova Scotia Timeline
National Youth Screening Project Timeline

Cape Breton Region, Nova Scotia
72
Appendix E: Project Flow Chart

Cape Breton Region, Nova Scotia
73
Appendix F: References
Centre for Addiction and Mental Health. (2006). Navigating screening options for concurrent disorders.
Toronto, ON: Author.
Chaim, G. & Henderson, J. (2009). Innovations in collaboration: Findings from the GAIN Collaborating
Network Project. Toronto, ON: Centre for Addiction and Mental Health.
Dennis, M.L., Chan, Y.F., & Funk, R.R. (2006). Development and validation of the GAIN Short Screener
(GSS) for internalizing, externalizing and substance use disorders and crime/violence problems
among adolescents and adults. American Journal on Addictions, 15, 80-91.
Health Canada (2002). Best practices: Concurrent mental health and substance use disorders. Ottawa,
ON: Author.
Henderson, J., Chaim, G., & Rush, B. (2007). Knowledge, skills and tools: Addressing the mental health
and addiction needs of youth. Symposium presentation, Issues of Substance 2007 Conference,
Edmonton, AB.
Henderson, J., Chaim, G., & Goodman, I. (2009, August). Evaluating youth concurrent disorders across
youth-serving agencies in Toronto, Canada. Paper presentation, 117th Annual Convention of the
American Psychological Association, Toronto, ON.
Henderson, J., MacKay, S., & Peterson-Badali, M. (2010). Interdisciplinary knowledge translation: Lessons
learned from a mental health - fire service collaboration. American Journal of Community
Psychology, 46, 277-288.
Hillman, L., Chaim, G., & Henderson, J. (2011). Cross-sector collaboration in action: Findings from the
Concurrent Disorders Support Services Screening Project. Toronto, ON: Authors
McElheran, W., Eaton, P., Rupcich, C., Basinger, M., & Johnston, D. (2004). Shared mental health care:
The Calgary model. Families, Systems & Health. 22(4), 424–438.
Murphy, R. A., Rosenheck, R. A., Berkowitz, S. J., & Marans, S. R. (2005). Acute service delivery in a
police-mental health program for children exposed to violence and trauma. Psychiatric Quarterly,
76(2), 107-201.
National Treatment Strategy Working Group (2008). A systems approach to substance use in Canada:
Recommendations for a National Treatment Strategy. Ottawa, ON: National Framework for Actions
to Reduce the Harms Associated with Alcohol and Other Drugs and Substances in Canada.
Cape Breton Region, Nova Scotia
74
Oliver, C., & Dykeman, M. (2003). Challenges to HIV service provision: The commonalities for nurses and
social workers. AIDS Care, 15(5), 649-663.
Reid, G.J., Evans, B., Brown, J.B., Cunningham, C.E., Lent, B., Neufeld, R., Vingilis, E., Zaric, G., &
Shanley, D. (2006). Help – I need somebody: The experiences of families seeking treatment for
children with psychosocial problems and the impact of delayed or deferred treatment. Ottawa, ON:
Canadian Health Services Research Foundation.
Robillard, A.G., Gallito-Zaparaniuk, P., Arriola, K. J., Kennedy, S., Hammett, T., & Braithwaite, R. L.
(2003). Partners and processes in HIV services for inmates and ex-offenders. Facilitating
collaboration and service delivery. Evaluation Review, 27, 535-562.
Rush, B., Castel, S., & Desmond, R. (2009). Screening for concurrent substance use and mental health
problems in youth. Toronto, ON: Centre for Addiction and Mental Health.
Skilling, T., Henderson, J., Root, C., Chaim, G., Bassarath, L., & Ballon, B., (2007). Who are our clients?
Comparing the mental and addiction needs of adolescent clients across two CAMH programs.
Poster Presentation, Annual Convention of the Canadian Psychological Association, Ottawa, ON.

