capital bluecross edi operations user's guide - zendesk · capital bluecross edi operations ....
TRANSCRIPT

ELECTRONIC DATA INTERFACE 834 TRANSACTION
Capital BlueCross EDI Operations
USER'S GUIDE
Health care benefit programs issued or administered by Capital BlueCross and/or its subsidiaries, Capital Advantage Insurance Company® and Keystone Health Plan® Central. Independent licensees of the Blue Cross and Blue Shield Association. Communications issued by Capital BlueCross in its capacity as administrator of programs and provider relations for all companies. Delta Dental® of Pennsylvania and National Vision Administrators, LLC (NVA®) are independent companies whose products and services are not Blue products and services. Delta Dental and NVA are solely responsible for the payment of claims and provision of services.

C A P I T A L B L U E C R O S S E D I O P E R A T I O N S
Benefit Enrollment and Maintenance for Insurance Products

Table of Contents
Introduction 1 Chapter 1General Information 2 Contact Information ............................................................................................................................ 2
System Operating Hours .................................................................................................................... 3
Authorization Process ......................................................................................................................... 3
Transaction Size .................................................................................................................................... 4 Testing Policy ........................................................................................................................................ 4
Reports and Acknowledgements ...................................................................................................... 5
Chapter 2Transmission Envelopes 6 Delimiters ............................................................................................................................................... 6
ISA Requirements - Inbound Transactions ................................................................................... 7
GS Requirements - Inbound Transactions ..................................................................................... 8 Chapter 3Detail of the ANSI 834 9 Data Detail ............................................................................................................................................. 9
ST - Transaction Set Header ....................................................................................................10 BGN - Beginning Segment .......................................................................................................10 REF - Transaction Set Policy Number ..................................................................................11 DTP - File Effective Date.........................................................................................................11 N1 - Sponsor Name ...................................................................................................................11 N1 - Payer .....................................................................................................................................12 N1 - TPA /Broker Name .........................................................................................................12 ACT - TPA /Broker Account Information .........................................................................12 INS - Member Level Detail ......................................................................................................13 REF - Subscriber Number........................................................................................................14
REF - Member Policy Number ...............................................................................................14 REF - Member Identification Number .................................................................................15 REF - Prior Coverage Months ................................................................................................16 DTP - Member Level Dates .....................................................................................................16 NM1 - Member Name ..............................................................................................................17 PER - Member Communication Numbers ..........................................................................18 N3 - Member Residence Street Address ...............................................................................18 N4 - Member Residence City, State, Zip Code ....................................................................18 DMG - Member Demographics .............................................................................................19 ICM - Member Income .............................................................................................................19 AMT - Member Policy Amounts ............................................................................................19 HLH - Member Health Information .....................................................................................20 LUI - Member Language ..........................................................................................................20 NM1 - Incorrect Member Name ............................................................................................20 DMG - Incorrect Member Demographics ...........................................................................21 NM1 - Member Mailing Address ............................................................................................21 N3 - Member Mail Street Address ..........................................................................................21 N4 - Member Mail City, State, Zip Code ..............................................................................22 NM1 - Member Employer .......................................................................................................22 PER - Member Employer Communications Numbers .....................................................22 N3 - Member Employer Street Address ................................................................................22 N4 - Member Employer City, State, Zip ...............................................................................23 NM1 - Member School .............................................................................................................23 PER - Member School Communications Numbers ...........................................................23 N3 - Member School Street Address .....................................................................................23 N4 - Member School City, State, Zip .....................................................................................23 NM1 - Custodial Parent ............................................................................................................24 PER - Custodial Parent Communications Number ...........................................................24 N3 - Custodial Parent Street Address ....................................................................................24 N4 - Custodial Parent City, State, Zip ...................................................................................24 NM1 - Responsible Person ......................................................................................................25 PER - Responsible Person Communication Numbers ......................................................25 N3 - Responsible Person Street Address ...............................................................................25 N4 - Responsible Person City, State, Zip ..............................................................................25 DSB - Disability Information ...................................................................................................25 DTP - Disability Eligibility Dates ............................................................................................26 HD - Health Coverage ..............................................................................................................26 DTP - Health Coverage Dates.................................................................................................27

AMT - Health Coverage Policy ...............................................................................................28 REF - Health Coverage Policy Number ................................................................................28 IDC - Identification Card ..........................................................................................................28 LX - Provider Information .......................................................................................................29 NM1 - Provider Name ..............................................................................................................29 N4 - Provider City, State, Zip Code .......................................................................................29 PER - Provider Communication Numbers ..........................................................................30 PLA - PCP Change Reason ......................................................................................................30 COB - Coordination of Benefits .............................................................................................30 REF - Additional Coordination of Benefits Identifiers ......................................................30 N1 - Other Insurance Company Name .................................................................................30 DTP - Coordination of Benefits Eligibility Dates ...............................................................31 SE - Transaction Set Trailer .....................................................................................................31
1
The EDI 834 Transaction User's Guide addresses how Groups, who have signed up as Trading Partners with Capital BlueCross, or their business associates, conduct Benefit Enrollment and Maintenance HIPAA (Health Insurance Portability and Accountability Act of 1996) standard electronic transactions in the ANSI x 12 format.
An Electronic Data Interchange (EDI) Trading Partner is defined as any Capital BlueCross customer that transmits to, or receives electronic data from, Capital BlueCross. The Capital BlueCross EDI transaction system supports transactions adopted under the Health Insurance Portability Act of 1996 (HIPAA).
While Capital BlueCross EDI Operations will accept HIPAA compliant transactions from any covered entity, HIPAA security requirements dictate that proper procedure be established in order to secure access to data. Therefore, Capital BlueCross has a process to establish an Electronic Trading Partner relationship. That process has two aspects:
• A Service Agreement must be agreed to and submitted by the customer. This establishes the legal relationship and requirements for the exchange of EDI transactions. Please refer to the Contact Information section of the guide on who to contact to begin this process.
• Once the agreement is received, the Trading Partner will be sent a logon ID and password combination for use when accessing Capital BlueCross' EDI system for submission or retrieval of transactions.
Introduction
i

2
General Information The following addresses general and specific information in regards to Capital BlueCross accepting and sending the HIPAA-mandated ANSI 834 (Benefit Enrollment and Maintenance). It must be noted that for proper implementation of these transactions, both the HIPAA-named Implementation Guide (004010X095A1 or 005010X220A1) and Capital BlueCross' User Guide must be used.
C O N T A C T I N F O R M A T I O N
Business Contacts: These contacts are to be used to receive authorization to send EDI transactions, questions about the Capital BlueCross User Guide, or the HIPAA Implementation Guide.
Group Leaders, please contact your Marketing Representative.
Technical Contacts: These contacts are to be used when experiencing a technical problem such as when an error is incurred when transmitting files, etc.
Capital BlueCross Support Center
Phone: (717) 541-7200
Hours of Operation: 24 hours a day, 7 days a week
It should be noted that although a problem can be reported 24 hours, 7 days a week, the problem may not actually be resolved until the next normal business day during normal business hours.
Chapter 1
1

3
S Y S T E M O P E R A T I N G H O U R S
Trading Partners can send ANSI 834 files to Capital BlueCross, 24 hours a day/7 days a week. Due to system maintenance, Capital BlueCross will only process ANSI 834 files received prior to 3:00 p.m. Monday through Friday. Any file received after 3:00 p.m. Monday through Friday will process the next business day. Any file received over the weekend, will also process the next business day.
Any changes to the processing hours due to holidays will be sent out in separate communications.
A U T H O R I Z A T I O N P R O C E S S
Prior to sending EDI transactions to Capital BlueCross, a trading partner must first enter into a Service Agreement with Capital BlueCross. The Service Agreement establishes the legal relationship and requirements for the exchange of EDI transactions. Please refer to the Contact Information section for whom to contact to begin the process of setting up a Service Agreement and subsequent steps.
New Trading Partners: The Service Agreement outlines all of the Accounts and transactions that a Trading Partner submits on the behalf of. To become a Trading Partner with Capital BlueCross (CBC): • Contact your Marketing Representative to discuss transactions. • A Service Agreement will be sent to you for your signature. The Service Agreement should
be signed and returned to Capital BlueCross. Signatures at Capital BlueCross will be obtained and a final copy returned to the Trading Partner.
• While the Service Agreements are being routed, technical contacts will be made to establish delivery/receipt of the transactions.
• Once the connectivity has been established, test files can be exchanged. • Once the Trading Partner has passed the testing, a target production date will be established.
Note: the Service Agreement must be completed by the production date.

4
Adding a New Account /Transaction to an Existing Trading Partner: • Contact your Marketing Representative to discuss transactions. • An updated Service Agreement will be sent to you for your signature. Section 7.7 of the
Agreement should be signed and returned to Capital BlueCross. Signatures at Capital BlueCross will be obtained and a final copy returned to the Trading Partner.
• If the request is for a new transaction that the Trading Partner has not previously submitted to Capital BlueCross, testing will be required.
• Once the testing process has been completed and the Trading Partner has been approved for production, a target production date will be established.
• If the request is to add a new account to an existing transaction, Capital BlueCross requests that the first transmission of the new account's data be submitted in a separate file.
• If the first production transmission is processed successfully, the new account may be combined with the regular transmission.
Note: The signed Agreement must be completed by the production date.
T R A N S A C T I O N S I Z E
Capital BlueCross will support the HIPAA Implementation Guide limit of 10,000 INS segments in a single ANSI 834 transaction.
T E S T I N G P O L I C Y
Sending Test Files
When sending a test file, indicate that the file being submitted is a test file by placing a "T" in ISA15.
To insure that a full and proper test is done between Capital BlueCross and its Trading Partners, please make sure that they contain a sampling of each type of scenario that may be seen in the production files. The following is a sample of required Enrollment and Maintenance transactions that must be transmitted when testing the ANSI 834.

5
SAMPLE TRANSACTIONS: Enrollment • Subscriber • Spouse • Child Maintenance • Add Dependent • Change Subscriber Information • Change Dependent Information • Address Change • Cancel Contract • Cancel Dependent • Re-add Canceled Contract • Re-add Canceled Dependent • Change Subscriber Coverage • Change Dependent Coverage • Subgroup Transfer (if applicable) • Class Transfer (if applicable) • Retroactivity • Add Subscriber Provider Data (if applicable) • Add Dependent Provider Data (if applicable)
Moving to Production
For a Trading Partner to move to a production status on the ANSI 834, Capital BlueCross must receive and process ANSI 834 test file(s) with at least 90% accuracy rate, successfully completing all defined testing scenarios.
R E P O R T S A N D A C K N O W L E D G M E N T S
When requested by a Trading Partner, Capital BlueCross will send an ANSI 997 or ANSI 999 to acknowledge receipt of a submitted ANSI 834. During normal operating hours (see System Operating Hours), the ANSI 997 or ANSI 999 will be sent one half hour after submission of an ANSI 834. The ANSI 997 or ANSI 999 will report whether an ANSI 834 was properly received and read by the Capital BlueCross translator. The ANSI 997 or ANSI 999 developed by Capital BlueCross will accept/reject a transmission at the GS/GE level. If an ANSI 834 contains multiple GS/GE levels, and one of those GS/GE levels is rejected by the translator, only that GS/GE level will need to be re-submitted; not the entire transmission.

6
Transmission Envelopes It is expected that the ISA and GS segments be used as outlined in the HIPAA-named Implementation Guides. Capital BlueCross' specific requirements for these segments are detailed in the following information.
D E L I M I T E R S
Capital BlueCross prefers the following delimiters:
Description Character Data Element Separator * (asterisk)
Segment Terminator ~ (tilde)
Composite Data Element Separator : (colon)
I F A T R A D I N G P A R T N E R W I S H E S T O U S E O T H E R D E L I M I T E R S O N T H E T R A N S A C T I O N S T H A T T H E Y W I L L S E N D T O C A P I T A L B L U E C R O S S , T H I S S H O U L D B E A D D R E S S E D D U R I N G T H E I M P L E M E N T A T I O N D I S C U S S I O N S .
Chapter 2
2

7
I S A R E Q U I R E M E N T - I N B O U N D T R A N S A C T I O N S
Element Element Name Usage Note
ISA01 Authorization Information Qualifier
Capital BlueCross supports the use of 00 (No Authorization Information Present)
ISA02 Authorization Information This data element must be space filled.
ISA03 Security Information Qualifier Capital BlueCross supports the use of 00 (No Security Information Present)
ISA04 Security Information This data element must be space filled.
ISA05 Interchange ID Qualifier Capital BlueCross supports the use of the qualifier "ZZ" to designate that a Capital BlueCross-assigned sender id will be used.
ISA06 Interchange Sender ID This data element needs to be filled in with your Capital BlueCross sender ID.
ISA07 Interchange ID Qualifier Capital BlueCross supports the use of qualifier "30" to designate the U.S. Federal Tax ID.
ISA08 Interchange Receiver ID This data element needs to be filled in with the Capital BlueCross tax id of 23-0455154. This field needs to be left justified and space filled. The hyphen should not appear in the transaction.
ISA09 Interchange Date Self explanatory
ISA10 Interchange Time Self explanatory
ISA11 Interchange Control Standards Identifier
Per the v4010 HIPAA Implementation Guide for this transaction, this must be filled in with a "U".
Per the v5010 HIPAA Implementation Guide for this transaction, this must be filled in with a “^”.
ISA12 Interchange Control Version Number
Per the v4010 HIPAA implementation Guide for this transaction, this must be filled in with "00401".
Per the v5010 HIPAA Implementation Guide for this transaction, this must be filled in with “00501”.
ISA13 Interchange Control Number This data element must be filled with a truly unique, incrementing number to insure that Capital BlueCross will not process duplicate files.
ISA14 Acknowledgement Requested
For this transaction, Capital BlueCross would prefer to use an indicator of '0' to indicate that no interchange acknowledgement is requested.
ISA15 Usage Indicator This data element needs to be filled in with a "T" or "P", as appropriate, to indicate whether the transmission is test or production.
ISA16 Component Element Separator
This data element should be filled in with the Composite Data Element Separator indicated on page 6 of the CBC 834 User’s Guide under Delimiters.

8
G S R E Q U I R E M E N T S - I N B O U N D T R A N S A C T I O N S
Element Element Name Usage Notes
GS01 Functional Identifier Code For this transaction, this element will be filled with BE (Benefit Enrollment and Maintenance 834).
GS02 Application Sender's Code This data element needs to be filled in with the Capital BlueCross-assigned trading partner id.
GS03 Application Receiver's Code This data element needs to be filled in with the Capital BlueCross federal tax id 23-0455154. This field needs to be left justified. The hyphen should not be part of the transaction.
GS04 Date Self explanatory
GS05 Time Self explanatory
GS06 Group Control Number Self explanatory
GS07 Responsible Agency Code Per the HIPAA Implementation Guide, this should be populated with "X" (Accredited Standards Committee X12)
GS08 Version/Release/Industry Identifier Code
Per the v4010 HIPAA Implementation Guide, this field will be populated with "004010X095A1".
Per the v5010 HIPAA Implementation Guide, this field will be populated with “005010X220A1”.

9
Data Detail for the ANSI 834
The following information is to serve as an explanation or payer-specific requirements for submitting an ANSI 834 to Capital BlueCross. Every segment has been listed in this chapter, indicating Implementation Guide usage and if the segment is used by Capital BlueCross. Any data element that requires an explanation or specific requirement for submitting to Capital BlueCross, will be listed and include an explanation in the element note. Otherwise, please follow the guidelines outlined in the ANSI 834 Implementation Guide. Capital BlueCross requires the transmission data to be structured as outlined in the ANSI 834 Implementation Guide. Each Transaction Set will include one ST - Transaction Set Header segment and one SE - Transaction Set Trailer record per Transaction Set. Member segments that are to be included in the Transaction Set will begin and loop at the INS - Member Level Detail segment. Member level detail should not loop at the ST - Transaction Set Header and SE - Transaction Set Trailer segments.
Chapter 3
3

10
D A T A D E T A I L
Segment: ST Transaction Set Header Loop: ______ Level: Header Usage: Required Capital BlueCross: Used Segment: BGN Beginning Segment Loop: ______ Level: Header Usage: Required Capital BlueCross: Used
Data Element Summary
Element Designator Element Name
Element Note
BGN01 Transaction Set Purpose Code The standard value is 00 (Original). Capital BlueCross would contact the Sponsor to coordinate sending a file with the following values: 15 (Re-submission) 22 (Information Copy)
BGN08 Action Code The standard value is 2 (Change Update). Value 4 (verify) should be sent when an account submits a change file and wishes to conduct a file match or, when they elect to use the Full File capabilities within 834. A full file for the purpose of conducting a file match will be used to synchronize the Sponsor’s and Capital BlueCross files. This should only be sent on a predefined schedule or on a date agreed to by Sponsor and Capital BlueCross.
11
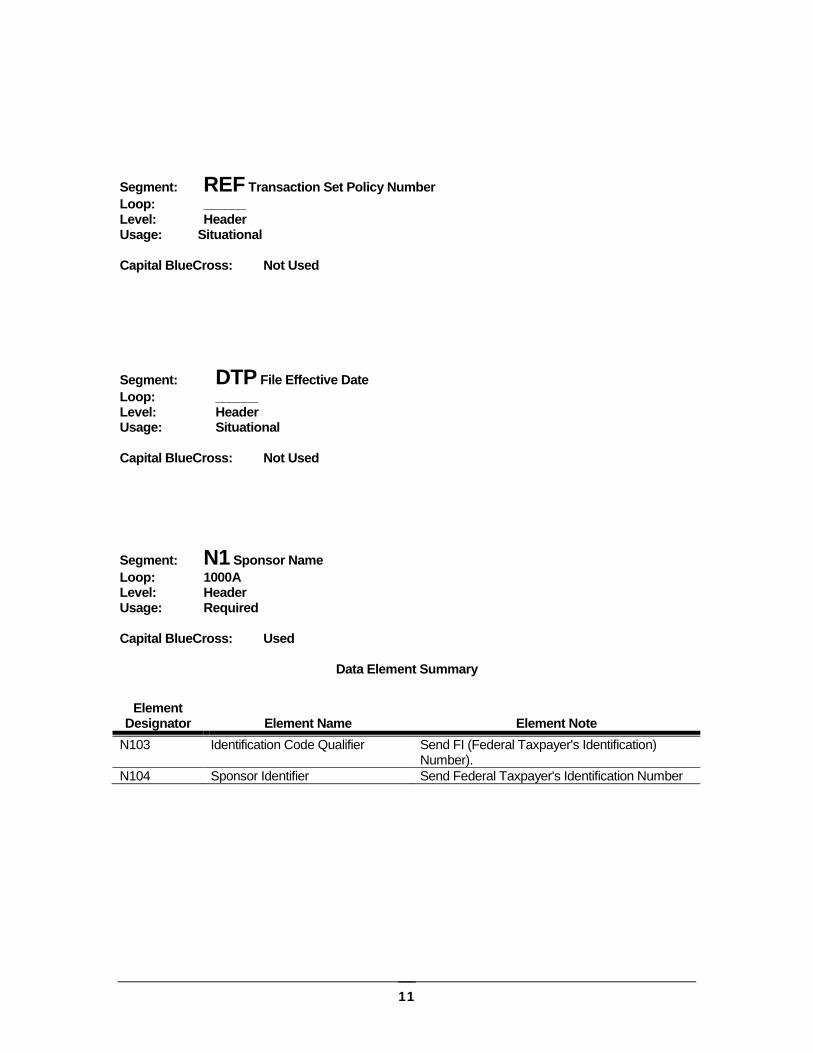
Segment: REF Transaction Set Policy Number Loop: ______ Level: Header Usage: Situational Capital BlueCross: Not Used Segment: DTP File Effective Date Loop: ______ Level: Header Usage: Situational Capital BlueCross: Not Used Segment: N1 Sponsor Name Loop: 1000A Level: Header Usage: Required Capital BlueCross: Used
Data Element Summary
Element Designator Element Name
Element Note
N103 Identification Code Qualifier Send FI (Federal Taxpayer's Identification) Number).
N104 Sponsor Identifier Send Federal Taxpayer's Identification Number

12
Segment: N1 Payer Loop: 1000B Level: Header Usage: Required Capital BlueCross: Used
Data Element Summary
Element Designator Element Name
Element Note
N103 Identification Code Qualifier Send FI (Federal Taxpayer's Identification Number)
N104 Insurer Identification Code Send the Capital BlueCross Taxpayer's Identification Number 23-0455154
Segment: N1 TPA/Broker Name Loop: 1000C Level: Header Usage: Situational Capital BlueCross: Used. Segment is used only if it is necessary to transmit TPA or Broker information for the Sponsor. The Sponsor and Capital BlueCross will discuss any requirements during implementation discussions. Segment: ACT TPA/Broker Account Information Loop: 1100C Level: Header Usage: Situational Capital BlueCross: Not Used

13
Segment: INS Member Level Detail Loop: 2000 Level: Detail Usage: Required
Capital BlueCross: Used Data Element Summary
Element Designator Element Name
Element Note
INS02 Individual Relationship Code Capital BlueCross policy does not cover the following relationships as dependents: 03 – Father or Mother 04 – Grandfather or Grandmother 13 – Mother-in-law or Father-in-law 26 – Guardian 31 – Court Appointed Guardian 32 – Mother 33 – Father 48 – Stepfather 49 – Stepmother
If the Sponsor identifies a requirement to use one of these relationship code values, the Sponsor must contact Capital BlueCross (see contacts).
Any relationship being submitted as a Dependent Child of the Employee must satisfy the age requirements of the Sponsor’s contract.
INS03 Maintenance Type Code Codes ‘001’ (Change), ‘021’ (Addition) & ‘024’ (Cancellation or Termination) are used as defined in Implementation Guide.
Code ‘025’ (Reinstatement) should be used to re-enroll subscriber and dependents previously enrolled with the Sponsor with Capital BlueCross coverage. For a contract reinstatement, the Sponsor must submit the subscriber, dependents and the type of coverage being reinstated. For a dependent reinstatement, the Sponsor must submit the dependent and the type of coverage being reinstated.
Code ‘030’ (Audit or Compare) would be used when a full file is being transmitted for the purpose of conducting a file match between the Sponsor and Capital BlueCross (See additional data in BGN segment/data element BGN08), or when an account is utilizing the 834 Full File process.
INS04 Maintenance Reason Code If the Maintenance Type Code in INS03 is ‘024’ (Cancellation or Termination), a Maintenance Reason Code in INS04 is required.
INS09 Student Status Code Required for dependent students who are over the dependent age requirements in the Sponsor’s benefit program. Capital BlueCross coverage of student dependents requires that the student is a ‘full-time’ student identified by a value of ‘F’ in INS09.
14
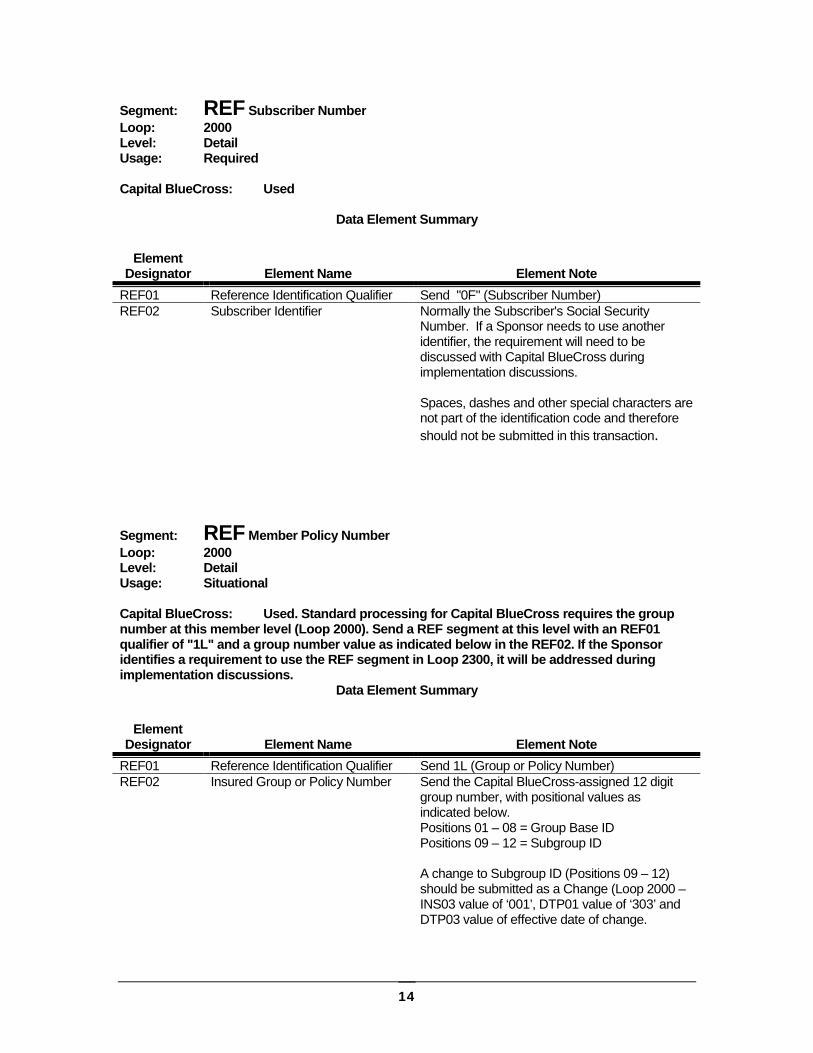
Segment: REF Subscriber Number Loop: 2000 Level: Detail Usage: Required Capital BlueCross: Used
Data Element Summary
Element Designator Element Name
Element Note
REF01 Reference Identification Qualifier Send "0F" (Subscriber Number) REF02 Subscriber Identifier Normally the Subscriber's Social Security
Number. If a Sponsor needs to use another identifier, the requirement will need to be discussed with Capital BlueCross during implementation discussions. Spaces, dashes and other special characters are not part of the identification code and therefore should not be submitted in this transaction.
Segment: REF Member Policy Number Loop: 2000 Level: Detail Usage: Situational Capital BlueCross: Used. Standard processing for Capital BlueCross requires the group number at this member level (Loop 2000). Send a REF segment at this level with an REF01 qualifier of "1L" and a group number value as indicated below in the REF02. If the Sponsor identifies a requirement to use the REF segment in Loop 2300, it will be addressed during implementation discussions.
Data Element Summary
Element Designator Element Name
Element Note
REF01 Reference Identification Qualifier Send 1L (Group or Policy Number) REF02 Insured Group or Policy Number Send the Capital BlueCross-assigned 12 digit
group number, with positional values as indicated below. Positions 01 – 08 = Group Base ID Positions 09 – 12 = Subgroup ID A change to Subgroup ID (Positions 09 – 12) should be submitted as a Change (Loop 2000 – INS03 value of ‘001’, DTP01 value of ‘303’ and DTP03 value of effective date of change.

15
Segment: REF Member Identification Number Loop: 2000 Level: Detail Usage: Situational Capital BlueCross: Used
Data Element Summary
Element Designator Element Name
Element Note
REF01 Reference Identification Qualifier Required for Capital BlueCross: Code ‘17’ (Client Reporting Category) is required by Capital BlueCross. It is used to identify the Employee Classification (Class ID) of the Subscriber. The actual values will be identified during the contract set up. Conditional based on activity: Code ‘F6’ (HIC Number) is required when reporting Medicare eligibility. Code ‘6O’ (Cross-Reference Number) is used to tie the Surviving Insured back to the original Subscriber ID. (Value added in 834 Addenda) Conditional based on Sponsor requirements: Code ‘DX’ (Department/Agency Number) is required if Sponsor is an Association and must submit a Member Firm ID. Used for other Sponsors if there is a need to track other department or location information regarding the Employee not already covered by other segments. Code ‘ZZ’ (Mutually Defined – Title of the members employment position) is used if Sponsor has requirement for Capital BlueCross to capture an Employee ID. Code ‘23’ (Client Number) is used if there is a requirement to store a unique Member Number. Requirements regarding which values a Sponsor will submit will be discussed during the implementation discussions.
REF02 Subscriber Supplemental Identifier Value associated with the qualifier in REF01.

16
Segment: REF Prior Coverage Months Loop: 2000 Level: Detail Usage: Situational Capital BlueCross: Used. Sponsor has benefit program with pre-existing clause. Segment: DTP Member Level Dates Loop: 2000 Level: Detail Usage: Situational Capital BlueCross: Used. As indicated in the Implementation Guide, this segment is used to submit dates for changes not defined in other segments. Any additional uses of these values other than those defined in DTP01 must be addressed with the Sponsor during implementation discussions.
Data Element Summary
Element Designator Element Name
Element Note
DTP01 Date Time Qualifier Capital BlueCross requires the following dates based on these conditions: Code ‘357’ (Eligibility End Date) is required if the Maintenance Code Type in Loop 2000 is ‘024’ – Termination (INS03). Code ‘303’ (Maintenance Effective Date) is required if submitting changes to the following:
Subgroup ID – Loop 2000 – REF/Member Policy Number – Positions 9 – 12. Value changes to Codes 17(Class ID) or DX (Member Firm ID or Department/Location) or ZZ (Employee ID) – Loop 2000 – REF/Member Identification Number. This code is required when submitting an 834 Full File.
Code ‘338’ (Medicare Begin) is required if submitting Medicare Eligibility. The following should be submitted if available to Sponsor: Code ‘286’ (Retirement) should be submitted if changing Employment Status of Employee (Loop 2000 – INS08) from Active to Retired.

17
Code ‘336’ (Employment Begin – Hire Date) should be submitted when enrolling a new employee. Code ‘350’ (Education Begin Date) should be submitted when enrolling a student dependent. Code ‘351’ (Education End Date – Expected Graduation Date) should be submitted when enrolling a student dependent.
DTP02 Date Time Period Format Qualifier Send D8 DTP03 Status Information Effective Date Send Date in CCYYMMDD Format Segment: NM1 Member Name Loop: 2100A Level: Detail Usage: Required Capital BlueCross: Used. As indicated in the Implementation Guide, this segment is used to identify a member being enrolled, changing benefits or changing/correcting member identifier information.
Data Element Summary
Element Designator Element Name
Element Note
NM105 Member Middle Name Capital BlueCross will only store the member’s middle initial.
NM106 Member Name Prefix Not Used by Capital BlueCross NM107 Member Name Suffix Member Suffix values supported by Capital
BlueCross: JR, SR, I, II, III, IV, V, VI, VII, IX, X, MD, DO, DDS, ESQ. Other values can be accommodated if they are needed but not currently defined.
NM108 Identification Code Qualifier Send "34" (Social Security Number) NM109 Subscriber Identifier Until the HIPAA Individual Identifier is available
send SSN

18
Segment: PER Member Communication Numbers Loop: 2100A Level: Detail Usage: Situational Capital BlueCross: Used. Communication numbers must be formatted as specified in the Implementation Guide. Parentheses, hyphens, spaces and special characters must not be sent. Capital BlueCross captures CP/Cellular Phone, HP/Home Phone, WP/Work Phone and EX/Work Phone Extension. If a qualifier of TE/Telephone is submitted, it will be used as a Home Phone Number. Segment: N3 Member Residence Street Address Loop: 2100A Level: Detail Usage: Situational Capital BlueCross: Used. As indicated in the Implementation Guide, ‘Required’ when enrolling a subscriber or changing a subscriber address. Only send this segment for a dependent if the dependent’s address is different from the subscriber's. Segment: N4 Member Residence City, State, Zip Code Loop: 2100A Level: Detail Usage: Situational Capital BlueCross: Used. As indicated in the Implementation Guide, ‘Required’ when enrolling a subscriber or changing a subscriber's address. Only send this segment for a dependent if the dependent’s address is different from the subscriber's.
Data Element Summary
Element Designator Element Name
Element Note
N403 Subscriber Zip Code As specified in the national implementation guide, the hyphen (“-”) is excluded from a complete zip code. That is, a 9-digit zip code typically shown as “11111-1111” must be sent as “111111111”.
N405 Location Qualifier Code ‘CY’ (County) is used to submit County in N406. A requirement to use Code ‘60’ (Area) would need to be discussed with Sponsor during implementation discussions.
N406 Location Identification Code Value for qualifier defined in N405.
19
Segment: DMG Member Demographics Loop: 2100A Level: Detail Usage: Situational Capital BlueCross: Used. As indicated in the Implementation Guide, ‘Required’ when enrolling a new member or when changing a member’s demographic information. This segment is REQUIRED for dependent change records until the National Individual Identifier is mandated. (Birth Date & Gender will be used to identify member.)
Data Element Summary
Element Designator Element Name
Element Note
DMG03 Gender Code As noted in the Implementation Guide, a value of ‘U’/Unknown is not supported in our business systems. If this value is submitted, the Sponsor will be contacted so we can determine what value to assign.
DMG04 Marital Status Code Not Used by Capital BlueCross DMG05 Race or Ethnicity Code Not Used by Capital BlueCross DMG06 Citizenship Status Code Not Used by Capital BlueCross Segment: ICM Member Income Loop: 2100A Level: Detail Usage: Situational Capital BlueCross: Not Used Segment: AMT Member Policy Amounts Loop: 2100A Level: Detail Usage: Situational Capital BlueCross: Not Used

20
Segment: HLH Member Health Information Loop: 2100A Level: Detail Usage: Situational Capital BlueCross: Not Used Segment: LUI Member Language Loop: 2100A Level: Detail Usage: Situational Capital BlueCross: Not Used Segment: NM1 Incorrect Member Name Loop: 2100B Level: Detail Usage: Situational Capital BlueCross: Used. As indicated in the Implementation Guide, this segment is only used if a corrected name is sent in Loop 2100A or if the previously supplied demographics are being changed. If only the demographics (including SSN, Birth Date or Gender) are being changed, the code in NM101 in Loop 2100A will be IL, and the code in NM101 in this Loop will be 70. If using the 834 Full File process this segment should not be sent.
Data Element Summary
Element Designator Element Name
Element Note
NM105 Prior Incorrect Insured Middle Name
Capital BlueCross supports Member Middle Initial.
NM107 Prior Incorrect Insured Name Suffix
Name Suffix of Member. Capital BlueCross supports the following values: JR, SR, I, II, III, IV, V, VI, VII, IX, X, MD, DO, DDS, ESQ.
NM108 Identification Code Qualifier Send 34 (Social Security Number) If value is sent in NM108 then a value must be sent in NM109.
NM109 Prior Incorrect Insured Identifier Identifier previously sent in error. If value is sent in NM109 then a value (qualifier) must be sent in NM108.

21
Segment: DMG Incorrect Member Demographics Loop: 2100B Level: Detail Usage: Situational Capital BlueCross: Used. As indicated in the Implementation Guide, this segment is REQUIRED when there is a change to the previously supplied demographic information. Both the Birth Date and Gender are Required if this segment is sent. If the Birth Date is being changed, this segment will include both the prior/incorrect Birth Date and the current Gender (matches the value in DMG Loop 2100A). If using the 834 Full File process this segment should not be sent. Segment: NM1 Member Mailing Address Loop: 2100C Level: Detail Usage: Situational Capital BlueCross: Used. As indicated in the Implementation Guide, this address should be sent if subscriber has a mailing address different from the residence address sent in Loop 2100A. Only send for a dependent if the dependent’s address if different from the subscriber address. Segment: N3 Member Mail Street Address Loop: 2100C Level: Detail Usage: Situational Capital BlueCross: Used.

22
Segment: N4 Member Mail City, State, Zip Loop: 2100C Level: Detail Usage: Situational Capital BlueCross: Used
Data Element Summary
Element Designator Element Name
Element Note
N403 Subscriber Zip Code As specified in the national implementation guide, the hyphen (“-”) is excluded from a complete zip code. That is, a 9-digit zip code typically shown as “11111-1111” must be sent as “111111111”.
Segment: NM1 Member Employer Loop: 2100D Level: Detail Usage: Situational Capital BlueCross: Not Used Segment: PER Member Employer Communications Numbers Loop: 2100D Level: Detail Usage: Situational Capital BlueCross: Not Used Segment: N3 Member Employer Street Address Loop: 2100D Level: Detail Usage: Situational Capital BlueCross: Not Used

23
Segment: N4 Member Employer City, State, Zip Loop: 2100D Level: Detail Usage: Situational Capital BlueCross: Not Used Segment: NM1 Member School Loop: 2100E Level: Detail Usage: Situational Capital BlueCross: Used. If School Name is available, it should be submitted when enrolling a dependent as a full-time student. Segment: PER Member School Communications Numbers Loop: 2100E Level: Detail Usage: Situational Capital BlueCross: Not Used. Segment: N3 Member School Street Address Loop: 2100E Level: Detail Usage: Situational Capital BlueCross: Not Used Segment: N4 Member School City, State, Zip Loop: 2100E Level: Detail Usage: Situational Capital BlueCross: Not Used

24
Segment: NM1 Custodial Parent Loop: 2100F Level: Detail Usage: Situational Capital BlueCross: Used. As indicated in the Implementation Guide, this loop is REQUIRED when the custodial parent of a minor dependent is someone other than the subscriber.
Data Element Summary
Element Designator Element Name
Element Note
NM108 Identification Code Qualifier Send 34 (Social Security Number) NM109 Custodial Parent Identifier The Social Security Number should be sent, until
the national Identifier for Individual is available. Segment: PER Custodial Parent Communications Numbers Loop: 2100F Level: Detail Usage: Situational Capital BlueCross: Used Segment: N3 Custodial Parent Street Address Loop: 2100F Level: Detail Usage: Situational Capital BlueCross: Used
Segment: N4 Custodial Parent City, State, Zip Loop: 2100F Level: Detail Usage: Situational Capital BlueCross: Used
25
Segment: NM1 Responsible Person Loop: 2100G Level: Detail Usage: Situational Capital BlueCross: Not Used. If Payer has a requirement to submit this segment it must be addressed with Capital BlueCross (Sponsor) during the implementation discussions.
Segment: PER Responsible Person Communication Numbers Loop: 2100G Level: Detail Usage: Situational Capital BlueCross: Not Used. Segment: N3 Responsible Person Street Address Loop: 2100G Level: Detail Usage: Situational Capital BlueCross: Not Used
Segment: N4 Responsible Person City, State, Zip Loop: 2100F Level: Detail Usage: Situational Capital BlueCross; Not Used
Segment: DSB Disability Information Loop: 2200 Level: Detail Usage: Situational Capital BlueCross: Used. As indicated in the Implementation Guide, this segment should only be submitted when enrolling a disabled member or when disability information about an existing member is added or changed.

26
Segment: DTP Disability Eligibility Dates Loop: 2200 Level: Detail Usage: Situational Capital BlueCross: Used Segment: HD Health Coverage Loop: 2300 Level: Detail Usage: Situational Capital BlueCross: Used. As indicated in the Implementation Guide, this segment is REQUIRED when enrolling a new member or when adding, updating or removing coverage from an existing member.
Data Element Summary
Element Designator Element Name
Element Note
HD01 Maintenance Type Code When utilizing an 834 Change File the following values should be sent: ‘001’ – Change ‘021’ – Addition ‘024’ – Cancellation or Termination ‘025’ – Reinstatement When utilizing an 834 Full File the following value should be sent: ‘030’ – Audit or Compare
HD03 Insurance Line Code The following coverages are offered by Capital BlueCross: DEN (Dental) HLT (Health) – Preferred code for Medical Coverage – (Used for PPO, POS, Comprehensive, Traditional, Senior) PDG (Drug) POS (Point of Service) PPO (Preferred Provider Organization) VIS (Vision) Enter the Insurance Line Code value that corresponds to the coverage. If a Payer has a requirement to use one of the other values defined in the Implementation Guide, it must be addressed with Capital BlueCross (Sponsor) during implementation discussions.
HD04 Plan Coverage Description This data element is ‘Required’. Send the Capital BlueCross assigned value (5 to 8 digit value).

27
HD05 Coverage Level Code This data element is ‘Required’ for the Subscriber. The following coverage levels are supported by Capital BlueCross: EMP (Employee Only) ECH (Employee & Children) – Used for both Employee & Children and Employee & Child. ESP (Employee & Spouse) FAM (Family) If the addition or termination of a dependent member changes the Coverage Level Code, then a Subscriber record must be submitted as a Change with the new Coverage Level Code.
Segment: DTP Health Coverage Dates Loop: 2300 Level: Detail Usage: Required Capital BlueCross: Used. As indicated in the Implementation Guide, this segment contains the date that maintenance was performed or effective and the benefit begin and end dates for the coverage.
Data Element Summary
Element Designator Element Name
Element Note
DTP01 Date Time Qualifier Capital BlueCross requires the following dates based on these conditions: Code ‘348’ (Benefit Begin) is required if adding coverage. Code ‘349’ (Benefit End) is required if terminating specific coverage. This code should not be used when a member is terminating all eligible coverage. Code ‘303’ (Maintenance Effective) is required when a change is being made where a member’s coverage is not being added or terminated. Example, if changing the Coverage Level Code (HD05) on a Subscriber because of adding or terminating a dependent member.
DTP02 Date Time Period Format Qualifier Send D8 DTP03 Coverage Period (Date as defined
in DTP01) Send Date in CCYYMMDD Format

28
Segment: AMT Health Coverage Policy Loop: 2300 Level: Detail Usage: Situational Capital BlueCross: Not Used
Segment: REF Health Coverage Policy Number Loop: 2300 Level: Detail Usage: Situational Capital BlueCross: Not Used. If a requirement is identified for use of this segment, it will be addressed during implementation discussions.
Segment: IDC Identification Card Loop: 2300 Level: Detail Usage: Situational Capital BlueCross: Used. This segment should only be sent to request a replacement card when there is no change to data. Capital BlueCross will automatically generate cards based on data changes displayed on cards. Capital BlueCross generates Health cards at the member level. A separate request will be required for each member that requires a replacement card. Drug cards are generated at the subscriber level.
Data Element Summary
Element Designator Element Name
Element Note
IDC01 Plan Coverage Description Capital BlueCross does not require this data. Per Implementation Guide, the field is required and in order to satisfy the requirement send a single zero in the field.
IDC02 Identification Card Type Code Capital BlueCross supports the following values: H (Health) – Health Card is a combined card and will include any coverage for Dental and/or Vision. P (Drug) – Drug is a separate card and a separate request is required if both Health & Drug are being requested.
IDC04 Action Code Capital BlueCross supports the following values: RX (Replace)

29
Segment: LX Provider Information Loop: 2310 Level: Detail Usage: Situational Capital BlueCross: Used. Per Implementation Guide, use this loop to provide information about Primary Care Physician chosen by the enrollee in a managed care plan. Segment: NM1 Provider Name Loop: 2310 Level: Detail Usage: Required Capital BlueCross: Used.
Data Element Summary
Element Designator Element Name
Element Note
NM101 Entity Identifier Code Capital BlueCross supports the following values at this time: P3 (Primary Care Physician)
NM108 Identification Code Qualifier The following value is supported in the 834 4010 Addenda: SV (Service Provider) This code is to be used until a National Provider ID is developed.
NM109 Provider Identifier PCP (Primary Care Physician) Number identified in the Capital BlueCross provider directory.
Segment: N4 Provider City, State, Zip Code Loop: 2310 Level: Detail Usage: Situational Capital BlueCross: Not Used

30
Segment: PER Provider Communications Numbers Loop: 2310 Level: Detail Usage: Situational Capital BlueCross: Not Used Segment: PLA PCP Change Reason Loop: 2310 Level: Detail Usage: Situational Capital BlueCross: Used. As indicated in the Implementation Guide, this segment should be used to report the reason and the effective date that a member changes primary care provider. Segment: COB Coordination of Benefits Loop: 2320 Level: Detail Usage: Situational Capital BlueCross: Used. Segment: REF Additional Coordination of Benefits Identifiers Loop: 2320 Level: Detail Usage: Situational Capital BlueCross: Used Segment: N1 Other Insurance Company Name Loop: 2320 Level: Detail Usage: Situational Capital BlueCross: Used.
31
Segment: DTP Coordination of Benefits Eligibility Dates Loop: 2320 Level: Detail Usage: Situational Capital BlueCross: Used. Segment: SE Transaction Set Trailer Loop: ______ Level: Header Usage: Required Capital BlueCross: Required