capital investment manual - management of construction … · for queries on the status of this...
TRANSCRIPT

For queries on the status of this document contact [email protected] or telephone 029 2031 5512
Status Note amended March 2013
CAPITAL INVESTMENT MANUAL
Management of construction projects
1995
STATUS IN WALES
ARCHIVED


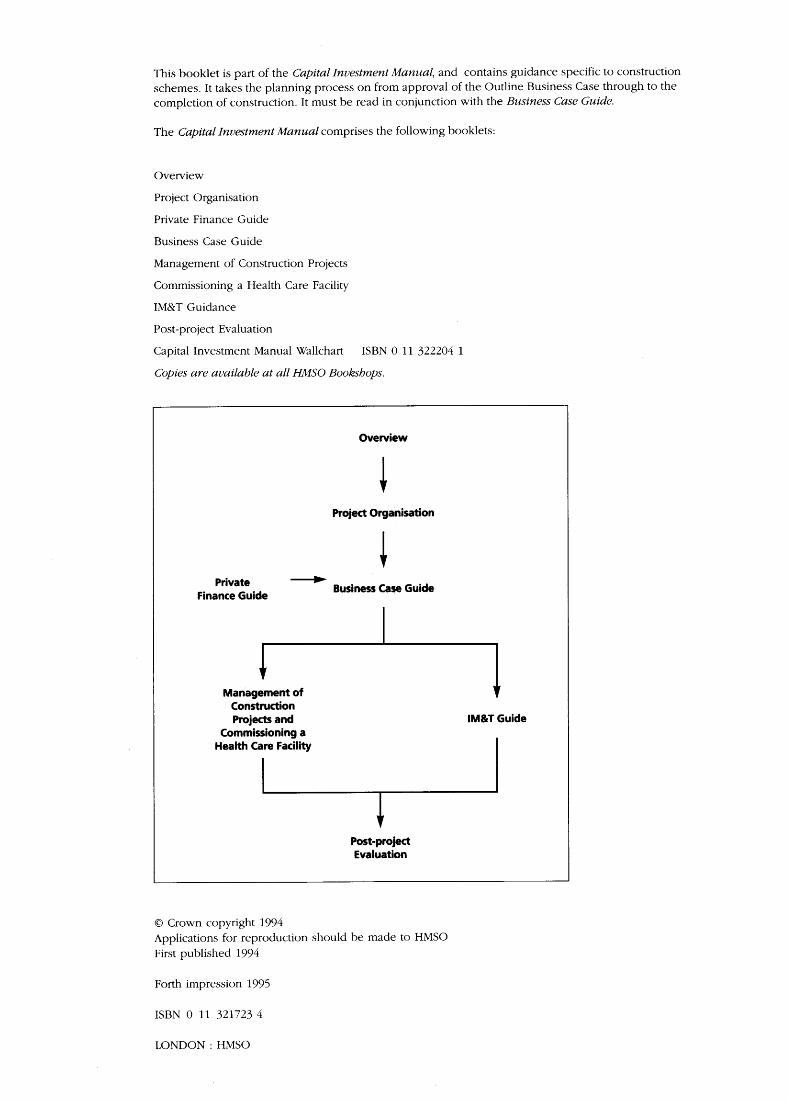
This booklet is part of the Capital Investment Manual, and contains guidance specific to constructionschemes . It takes the planning process on from approval of the Outline Business Case through to thecompletion of construction . It must be read in conjunction with the Business Case Guide.
The Capital Investment Manual comprises the following booklets :
Overview
Project Organisation
Private Finance Guide
Business Case Guide
Management of Construction Projects
Commissioning a Health Care Facility
IM&T Guidance
Post-project Evaluation
Capital Investment Manual Wallchart
ISBN 0 11 322204 1
Copies are available at all HMSO Bookshops .
Overview
Project Organisation
Private
-----
Business Case GuideFinance Guide
Management ofConstructionProjects and
IM&T GuideCommissioning aHealth Care Facility
Post-projectEvaluation
C Crown copyright 1994Applications for reproduction should be made to HMSOFirst published 1994
Forth impression 1995
ISBN 0 11 321723 4
LONDON : HMSO

Contents
Introductory
Foreword
5
Introduction
6
How to Use the Procedures
7
Synopsis of Process for Managing Construction Projects
8
Procedures
Stage 1 : Full Business Case Leading to Approval
15
Stage 2: Design
18
Stage 3: Tender and Contract
21
Stage 4: Construction and Equipment Supply
24
Stage 5: Technical Commissioning and Handover
29
Stage 6: Post Completion
31
Appendices
Appendix 1 : Project Certificates and Full Business Case Forms
35
Appendix 2 : Estimating, Budgets and Risk Assessment
45
Appendix 3: Cost, Risk and Contingency Management
50
Appendix 4: The Brief
55
Appendix 5: The Equipping of Construction Schemes
58
Appendix 6: Project Execution Plan (PEP)
60
Appendix 7: Monitoring and Monthly Progress Reports
63
Appendix 8: Mandatory Reports to the NHS Executive
68
Appendix 9: Assessment of Consultants' and Contractors' Performance
79
Appendix 10 : Glossary of Terms
84
Appendix 11 : Bibliography
87
Index
89

Introductory

Foreword
The NHS capital building programme is one of thelargest of its kind in the world . The National HealthService and Community Care Act 1990 led to thedevolution of responsibility from the centre andregions to the local level NHS Trusts . Thisdevolution applies to the management of majorcapital building projects .
Senior Trust managers should be aware of theprocedures set out in this document and makeevery effort to ensure that they are followed . Theywill be accountable for the performance of staffand external personnel employed in implementingconstruction projects .
The delivery of a major health care facility can becomplex, time-consuming and very costly . If theadvice in this document is followed, it could bestraightforward, efficiently executed andsuccessfully completed. The advice and proceduresin this document are aimed specifically at theneeds of NHS Trusts in discharging theirresponsibilities for managing health care buildingprojects .
The principles underlying the procedures in thismanual are :
Chief executives should be accountable andresponsible for their capital projects with theminimum of rigid and mandatory procedurescompatible with public accountability,compliance with government policies, and theconsequent need for monitoring by the NationalHealth Service Executive .
Trusts' ownership responsibilities should beexercised through an organisational structurewhich places personal responsibility onindividuals . The CEO should normally fulfil therole of project owner and a suitably senior trustemployee should be appointed as projectdirector . Responsibilities are described in theproject organisation booklet .
The objectives of project development are toprovide health care facilities specified in theFull Business Case, obtain best value formoney, and maintain probity .
Trusts should bear in mind that managing aconstruction project is like managing a separateand specialised business, but one which hasdefined start and completion dates . The annual rateof spending on a major project may be measuredin millions of pounds, and justifies the sameattention as a business with the same turnover.The most important tasks for a Trust are to :
- set up an appropriate organisation
adequately staffed by competent andcommitted people, to train them, and to givethem the authority to take decisions ;
- prepare a brief containing all therequirements of the end users of the project,to have it agreed and signed off by them,and to avoid changing it thereafter;
- establish procedures to manage the complexissues involved in a construction project,particularly those affecting cost and progress ;
- monitor performance so that the projectdirector is fully informed and able to takeprompt action if it should become necessary ;and
- identify appropriate contractual arrangementsin order to establish responsibility ofconsultants and contractors .
The principles set out in this document apply to allconstruction projects and trusts are commended tofollow them as much as possible . But theirmandatory application is confined to those whichexceed a threshold to be notified to Trusts fromtime to time by the NHS Executive . For small,simple capital building projects it may not besensible or cost effective to apply the proceduresin full . Trusts should, however, follow theprinciples of good management and propriety forsuch projects, but may simplify the procedures foreconomy and to ease the administrative burden .Trusts remain accountable for their smaller valueprojects and will be expected to complete them ontime, within budget, and to quality standards .
Trust Boards are accountable for a Trust's capitalprojects while the Secretary of State is ultimatelyreponsible for NHS activity . Trusts should thereforereview the progress of projects as a regular item atBoard Meetings . See Project Organisation bookletfor the role of investment decision maker, which isusually undertaken by the Trust board .
In view of problems involving significant time andcost overruns on major building schemes, the NHSExecutive wishes to have mechanisms in place thatwill act aq an early warning device when majorproblems arise and provide assurances on schememanagement . The NHS Executive thereforerequires Trusts to provide regular information onthe progress of schemes . Agreed capital projectaudits will be applied randomly to a proportion ofschemes and specifically to schemes that indicatemajor problems . The monitoring and capital projectaudit procedures will be undertaken by NHSEstates .
Major capital projects attract a great deal of publicattention. and Parliamentary scrutiny . Projectdirectors must be aware of this throughout .

Introduction
This part of the Capital Investment Manual (CIOcovers activities from Outline Business Caseapproval through to the completion ofconstruction .
The procedures are shown in six stages .
Stage 1 : Full Business Case Leading toApproval
Stage 2 : Design
Stage 3 : Tender and Contract
Stage 4 : Supply and Construction
Stage 5 : Technical Commissioning andHandover
Stage 6 : Post Completion
Each stage follows on from the preceding one,with some possible overlap .
Contained within each stage is a description of theprocedures as well as guidance on theirapplication and on good practice . The main tasksare identified with an indication of who shouldperform them and whether they are mandatory .
Trusts should make use of the other guidancedocuments which are referred to, including
CONCODE (see page 7), and should take advicefrom professional advisers and consultants . Beforeundertaking any of the procedures described inthis document, Trusts should first put in place anappropriate organisational structure (see ProjectOrganisation) .
The procedures start with the development of theFull Business Case . The extent of the workrequired for the production of the Full BusinessCase may vary from project to project, and someactivities described in this document may havebeen undertaken already to support the OutlineBusiness Case . This applies particularly to thedevelopment of the brief and the extent of design .Notwithstanding this, the procedures should becarried out as shown, although the work involvedin doing so may be reduced .
In a traditional contract procurement strategy, eachstage is completed before the following stage isstarted . But for fast-track contract procurementstrategies - e.g . Design and Build, ManagementContracts - there is an overlap between the stages .Where this applies, the stage procedures have beendivided into parts to indicate the differencesbetween the contract strategies . The overlap cannotbe defined with precision for every circumstance ;in such cases project directors, on the advice oftheir project managers, should comply with themandatory procedures but adapt the timing to suitthe circumstances of their projects .

How to Use theProceduresTasks should generally follow the stages set out inthis document in sequential order. There is scopefor flexibility when carrying out preliminary or fulldesign work . For example, some forms ofprocurement, such as Design and Build, entail thebulk of design work being carried out from theContract stage - i .e ., the design is part of theconstruction contract .
Finally, if in doubt, or when serious problems areencountered, refer to your NHS Executive contactsfor advice .
MANDATORY PROCEDURESTrusts and other provider units should carry outcertain procedures which apply to the variousstages in a capital scheme from inception toevaluation after completion . These proceduresoccur throughout the CIM and are :
- the establishment of an appropriate projectorganisation (see Project Organisation) ;
- the approval and re-approval requirementsfor funding following submission of businesscases (see below and Business Case Guide) ;
- complying with required tendering andcontract procedures (see below andCONCODE) ;
- complying with such other procedures wherespecified in this document ;
- establishing project control procedures ; and- carrying out post-project evaluation (see
Postproject Evaluation) .
KEY DOCUMENT RECORDThe process should be documented in a way thatwill allow auditors to examine the project . ProjectDirectors should ensure that a key document file ismaintained, which will assist a project audit as wellas being a useful tool in the management of thescheme .
RESUBMISSION OF SCHEME TO NHS EXECUTIVESchemes which are above the Treasury's delegatedlimit for approval will be required to follow at leastone re-approval from the Treasury . For traditionalprocurement methods the Treasury re-approval willbe applied for at the end of the Design Stage, justbefore the issue of the Certificate of Readiness toProceed to Tender . For schemes using non-traditional procurement methods individualjudgments will be made by the NHS Executive onthe precise point at which the re-approval to theTreasury will be made . The procedure forsubmitting a scheme to the Treasury for re-approval will be managed by the NHS Executive inconsultation with the Trust or unit seeking theapproval .
All schemes requiring NHS Executive approvalmust be re-submitted for consideration at any pointduring the lifetime of the project if one of thefollowing conditions apply:
"
The cost of client changes exceeds 5 per centof the approved sum, or
" The contingency allowance is spent at a ratedisproportionate to the stage a project hasreached (unless this was planned), or
"
A significant new risk is identified which wasnot included in the risk assessment on whichthe last approval was based .
OTHER GUIDANCE DOCUMENTSIt is important to read this document in conjunctionwith the other documents in the CIM. Particularattention should be paid to the following :
Project OrganisationBusiness Case GuidePrivate Finance GuideCommissioning a Health Care FacilityPost-Project Evaluation
Another important document to use is CONCODE;this provides guidance on the contracting aspectsof health building projects, including theimplementation of policy and EC directives .CONCODE can help Trusts in the appointment ofworks contractors and consultants and the use ofvarious forms of contract .
Further background material can be obtained fromGuidance Notes produced by the Treasury CentralUnit on Procurement (CUP), which are referred toin this document. They can be obtained free ofcharge by contacting :
HM TreasuryCentral Unit on ProcurementAllington Towers19 Allington StreetLondon SW1E 5EB
Tel : 071-270 1631Fax: 071-270 1639
NB : The CUP documents use the term `ProjectSponsor' to describe the role defined as `ProjectDirector' in CIM documents .
A bibliography is provided in Appendix 11 .

Synopsis of Process forManaging ConstructionProjectsThe project director takes full responsibility for all the main activities listed below . These activities willoften be carried out by others under the supervision of the project director . All these actions aremandatory for schemes that require approval by the NHS Executive, the Treasury or ministers . They areessential for most other schemes and where indicated should be followed in all cases .
STAGE 1 : FULL BUSINESS CASE LEADING TO APPROVAL
Stage Main Activities/Information ParagraphNumber
Review OutlineBusiness Case
Start work on Full Business Case after reviewing approval foroutline business case .
1 .1 .1, 1 .1 .2,1 .1 .4 and 1 .1 .5
Internalproject control
Develop proposals to ensure that effective control procedureswill be in place throughout the project (see Project Organisation) 1''21
Employment ofconsultants
Project Directors to consult CONCODE for advice on theappointment of consultants . 1 .4 .1
Due considerationof private sectorinvolvement
Consider use of private finance .1 .5 .1
Initial brief Preparation of policies and accommodation schedules .See Appendix 4 and NHS Estates Health Building Note 2 . 1 .6 .1
Site investigation Determine physical conditions on existing site . 1 .7 .1-1 .7 .2
Outline design Development of outline design to satisfaction of user panel . 1 .8 .1
Contract procure-ment strategy
Develop preliminary contract strategy. Reference to CONCODEand CUP Guidance Note 36 should be made . 1 .9 .1
Planningpermission
Apply for outline planning consent .1 .10.1-1 .10 .3
Developmentcontrol plan
A development control plan should be developed or existingone reviewed . 1 .11 .1
Equipment strategy Prepare a strategy for procurement of equipment . 1.12.1-1 .12 .3
Risk assessmentand contingencyallowance
Carry out a rigorous risk assessment and determine a suitablecontingency allowance . See Appendices 2 and 3 . 1 .13 .1
Budget costs Refine costings of preferred option . Cost Forms OBI and OB2Business Case Guide (BCG) will assist completion of FormsFB1-FB4 .
1 .14.1-1 .14 .5
Running costs Work up annual running costs . 1 .15 .1-1 .15 .2Planning for post-project evaluation
Initial evaluation activity . See Postproject Evaluation . 1 .16 .1
Obtaining NHSEand Treasuryapproval if required
The project director should be aware of cost thresholdsapplicable to projects . 1 .17 .1-1 .17 .3
Stage completion I Completion of readiness to proceed to design certificate . 11 .18 .1

STAGE 2 : DESIGN
STAGE 3: TENDER AND CONTRACT
Stage Main Activities/Information ParagraphNumber
Quality standards Ensure design team are aware of and take account of standards . 2 .1 .1-2 .1 .4
Brief development Brief should be completed and frozen . Complete Certificate ofBrief Acceptance (see Appendix 1) . 2 .2.1-2 .2 .2
Design managementprocedures
Ensure design conforms with brief; changes, cost controls andprocedures are part of the project execution plan. 2 .3.1-2 .3 .3
Designdevelopment
Development of full brief into sketch plan design, includingspatial layouts . Complete Certificate of Readiness to Proceed toDetailed Design (see Appendix 1) .
24.1-2 .4.2
Equipmentschedules
Prepare equipment schedules for Groups 2 and 3 equipment . 2 .5 .1 andAppendix 5
Detaileddesign
Conversion of sketch plan design into drawings and specifications .The level of detail at this stage depends on the procurementstrategy.
2 .6.1-2 .6.2
Planning consent Full planning consent must be obtained . 2 .7.1-2 .7 .2
Tender documents Bid documents to be prepared according to procurementstrategy used . 2 '8'1
Pre-tenderestimate
A pre-tender estimate must be prepared for the main buildingcontract under any procurement strategy . This will include :- up-to-date risk analysis and contingency;- up-to-date capital cost estimate ;- updated running costs ; and- confirmation that the programme is acceptable.
2 '9'1
Stage completion Treasury re-approval may be required. Certificate of Readinessto Proceed to Tender is required (see Appendix 1) .
4 .10.1-4 .10 .4
Stage Main Activities/Information ParagraphNumber
Generalconsiderations
Need to refer to CONCODE. 3 .1 .1-3 .1 .5
Propriety Tendering should be performed under standing financialinstructions, proper delegations and allow for audit . 3 .2 .1
Tenders Tender lists should be prepared within the appropriate tenderperiod followed by tender assessment and post tendernegotiations as appropriate .
3 .3 .1
Post-tenderestimate
Update risk analysis and contingency, establish approved sum,confirm programme acceptable and check re-approval criteria . 3 .4 .1
Stage completion Confirm validity of tender, complete a Certificate of Readiness toAward Contract, execute contract, complete NHS Estates contractand cost analysis forms where applicable .
3'5'1-3.5 .3

STAGE 4 : CONSTRUCTION AND EQUIPMENT SUPPLY
Stage Main Activities/Information ParagraphNumber
Applicable to allprocurementstrategies
General advice for all forms of procurement . 4 .1.1-4.1 .5
Contractadministrator
Confirm delegations and notify contractor .4 .2 .1
Productioninformation
Ensure necessary information is available to contractors whenneeded :- drawings ;- specifications;- requests for information ; and- approvals .
4.3 .1
Progress monitoring Project director to ensure appropriate monitoring systems are inplace . 4 .4 .1
Programmemanagement
Project manager to : check and monitor progress against contractprogramme . And issue monthly Project Progress Reports . 4 .5 .1
Qualitycontrol
Check work against the specification . Test materials .4 .6 .1
Costmanagement
Project manager to :- Operate change control procedures .- Price variations .- Manage expenditure of contingencies .- Maintain latest estimated cost and cash flow .- Initiate action to avoid overspend .- Issue monthly Financial Status Reports .- Submit NHS Executive Monthly Report Form .
4 .7 .1
Payment Agree interim certificates . Pay sums due on time . 4 .8 .1
Claims Project manager to maintain record of potential claims, assesssubmitted claims and report on circumstances . 4 .9 .1
Record keeping Project manager to :Maintain records of site activities :- daily diary ;- site instructions ;- inspection and test results ; and- contractors' requests .
4 .10 .1
ProceduresApplicable toDesign andBuildContractor'sdesign
Design team :- to check contractor's design drawings, materials andequipment against specification . Accept or requirere-submission .
4.11 .1

STAGE 4 : CONSTRUCTION AND EQUIPMENT SUPPLY (CONT.)
* The Project Buyer performs those duties defined in the Project Execution Plan
STAGE 5: TECHNICAL COMMISSIONING AND HANDOVER
STAGE 6: POST COMPLETION
Stage Main Activities/Information ParagraphNumber
ProceduresApplicable toManagementContractsWork packagesNote : the natureof this type ofprocurementmeans thatcontracts areprogressivelyawarded in phases .Therefore, some ofthese tasks mayoccur in stage 3 aswell as stage 4 .
Approve letting of work package sub-contracts . These cover :- work content ;- contract terms ;- price ;- programme ;- interfaces with other packages ; and- certificates to award contract .After each subcontract, check :- latest estimated cost ;- outstanding contract and design requirement ;- design co-ordination ; and- equipment deliveries .Prepare estimate of prime cost . Submit NHS contract form .
4 .12 .1-4 .12 .4
ProceduresApplicable toEquipment SupplyContracts*
Groups 2, 3 and 4 equipment normally procured duringoperational commissioning . Group 2 equipment may needspecial consideration with design team and contractorat this stage .
4 .13 .1
Stage Main Activities/Information ParagraphNumber
Organisation ofcommissioning
Establish commissioning team .Contractor is responsible for technical commissioning .Commissioning programme required .Check programme and co-ordinate with overall programme .Witness commissioning .
5 .2 .1
Inspection andtesting
Check quality of work, defects, completeness, and performance .Record results .
5 .3 .1
Other deliverables Ensure all specified deliverables are delivered . 5 .4 .1
Certificate ofPracticalCompletion andStage Completion
Issue certificates required on completion . 5 .5 .1
Stage Main Activities/Information ParagraphNumber
Claims and finalaccounts
Settle outstanding claims if possible . 6 .1 .1 andAppendix 3
Defects identify defects found after practical completion .Notify contractor/supplier .Expedite and monitor correction .
6 .2 .1
Final certificates Issue final certificates . Release balance of retention monies . 6 .3 .1
Stage completion Issue a final NHS Executive Report Form .Return all documentation to Trust .
6 .4 .1-6 .4 .2
Procedures

Stage 1 : Full BusinessCase Leading to ApprovalGeneral
1.1 .1 Work should not start on this stage until theOutline Business Case has been approved . Theprimary objective of this stage is to develop a fullycosted preferred option .
1.1.2 Trusts are recommended to consult theNHSE on the scope of work required to produce aFull Business Case if there is any doubt .
Internal Project Control Organisation
1.2.1 It is important that the Full Business Caseexplains project organisation arrangements,showing how Trust management has effectivecontrol over its capital building programme .Guidance on the management arrangements is setout in Project Organisation . It is expected that bythe time an Outline Business Case has beenapproved a project director should have beenappointed by the Trust Chief Executive . Asuggested appointment certificate for the projectdirector is included in Appendix 1 . Theappointment of a project manager will normallyfollow soon after the appointment of the ProjectDirector .
Reviewing the Strategic Context andInvestment Appraisal Undertaken inthe Outline Business Case
1.3.1 The business case must be reviewed toupdate information provided in the OutlineBusiness Case and to develop the justification forthe preferred option . This involves retracing steps1-7 of the Business Case Guide as follows :
' strategic context ;
'
objectives and benefit criteria ;
' generate options ;
' benefits assessment ;
' cost assessment ;
' risk assessment; and
' identify preferred option .
1.3.2 The case for the preferred option mustdemonstrate, on current resources and marketassumptions, that the recommended option can beafforded and how the costs would be met . Thisshould cover both capital and service cash flows
with at least five-year projections of NHS Trustbalance sheets, showing the impact of new assetsand income and expenditure statementsincorporating capital charges . The sources andyearly incidence of cash should be identified,including that from land sales or private financing .
1.3.3 For major investments, alternatives undereach of these headings must also be considered forthe preferred option :
'
In what ways could the option be postponed,accelerated or phased differently?
' Can the option be broken down intocomponents which are each in themselves anoption?
'
If it can be broken down into smaller, phasedschemes, is each component cost-effective onits own?
'
Full assessment of feasibility will includeconsideration of the practical aspect of anysubstantial service charge (such as a change ofuse or an associated hospital closure) . All caseswith substantial workforce implications willneed to address issues of recruitment,professional training, accommodation,redeployment and redundancy .
Employment of Consultants
1.4.1 Trusts need the professional input ofconsultants, including a project manager, designersand a quantity surveyor to develop the FullBusiness Case . The project director should followthe guidance in CONCODE to ensure that his orher duties are properly specified, that a formalagreement is entered into and that propriety ismaintained . At this stage Trusts should not committhemselves to consultants for work beyond thecompletion of outline design . A break clause inconsultants' contracts should be included to allowfor any delay in approval or rejection of the FullBusiness Case, and to cater for alternativeprocurement methods, e .g . where consultants maybe replaced by a contractor's own team or where amanagement contract is used .
Due Consideration of Private-sectorInvolvement
1.5.1 The involvement of the private sector shouldbe considered for all schemes . Use of private-sectorskills and management disciplines may increaseeffectiveness and efficiency and lead to better

managed risks . Further information and examplescan be found in the Private Finance Guide.
Initial brief1.6.1 The development of the brief is described inAppendix 4 and NHS Estates Health Building Note2 . It is prepared by a user panel overseen by theProject Director . The brief should be developed insufficient detail to allow the outline design and thebudget cost to be drawn up . It normally compriseswhole hospital policies, departmental policies andaccommodation schedules .
Site Investigation1 .7.1 Detailed site investigations are necessary todetermine any physical conditions existing on thesite which might have a significant effect on thebudget cost .
1 .7.2 The extent to which this is necessary willdepend on the characteristics of the project . ProjectDirectors should act on the advice of their ProjectManagers and designers .
Outline Design1.8.1 The initial brief should be made available tothe design team which will work up an outlinedesign, normally on the basis of 1:200 roomrelationship drawings, until :
- the user panel is satisfied that all itsrequirements are included in sufficient detail ;and
- the design team are satisfied that all essentialrequirements have been specified to enablethem to proceed to design development instage 2 and prepare the detailed specificationfor the project .
Contract Procurement Strategy1.9.1 A contract strategy is a planned method ofarranging for the work to be done . It determinesthe number and type of construction contracts tobe placed, and, in particular, how much of thedesign should be carried out by consultants andhow much by contractors . The following should beconsidered by the Trust at this stage :
- a preliminary decision on the contract strategyto be used, which may be reviewed at anytime before the tender and contract stage ;
- in reaching a decision on a contract strategy,the project director should rely on the adviceof the project manager, ensuring that risksassociated with the various procurementmethods are addressed ; and
- for more information on selecting anappropriate contract strategy, the projectdirector and his/her team should refer toCONCODE and CUP Guidance Note 36 .
Planning permission1.10.1 Trusts are subject to planning regulations .
The requirements of the local planning authoritycan have a significant effect on the project layout,its design and consequently its cost .
1.10.2 The project director, with the projectmanager and architect, should consult the planningauthority at the earliest possible stage during thedevelopment of the brief, for example at theOutline Business Case . This will enable the brief totake the planning authority's requirements intoaccount . As soon as the brief and theaccompanying design allow, an application shouldbe made for planning consent . The design teamwill prepare the application under the direction ofthe project manager . The status of this applicationand any restriction imposed by planners should beincluded in the Full Business Case .
1.10.3 Late discussions with planning authoritiesand other organisations can cause difficulty infinalising designs or disrupt programmes . Also, aslocal planning committees are democratic bodies,they may override the views of planning officers .The design team should recognise such potentialdifficulties and, where possible, order theprogramme of work and discussions with theauthorities, to ensure that all necessary consultationcan be completed and approvals obtained in goodtime . Local authorities are required to charge feesfor planning applications .
Development Control Plan1.11 .1 The Development Control Plan (DCP) is adocument containing text and drawings showingthe existing configuration of buildings, theirfunctional relationship with each other and thestages of future site development . Any existingDCP should be reviewed and the key drawingsappended to the Full Business Case document .
Equipment Strategy1.12 .1 Equipment is vital to the successfuloperation of the project and often comprises asignificant proportion of the budget . The projectdirector should, therefore, prepare at this stage anequipment strategy, which will outline both theequipment budget and the method of procurement .
1.12 .2 The strategy should identify :
- who will prepare the equipment budget,establish equipment requirements and,subsequently, purchase the equipment . Thisshould normally be an experienced capitalpurchasing officer;
- the policy for the transfer of existingequipment into the new scheme (which willinfluence the budget within the scheme forthe purchase of new equipment);
- the equipment procurement procedures to befollowed to ensure compliance with currentgovernment policies and to maintainpropriety ;
- the reporting procedures of the equippingprocess through to operationalcommissioning ;

- the policy for procuring new equipment forexisting services pending transfer into anynew facilities, i .e . to ensure compatibility -this is especially important for `high tech'equipment ; and
- a risk analysis of the factors which mightlead to an increase in the equipment budgetso that an appropriate contingency sum canbe included within the approved sum .
1.12.3 Detailed advice on the equipping processand the setting of equipment budgets is set out inAppendix 5 .
Risk Assessment and ContingencyProvision1.13.1 A rigorous risk assessment and allowancefor contingencies should be made . See Appendix 2for more detailed advice on preparing these .
Budget Cost1.14.1 The budget cost is prepared on completionof outline design, site investigation and planningconsultation . Cost forms must be submitted for allprojects requiring approval by the NHS Executive .The pro-formas FB1-F134 for this purpose areincluded in Appendix 1 . The supporting costinginformation will have already been set out partly incost forms OB1 and OB2 (see Business Case Guideand supporting costing documentation for theOutline Business Case) .
1.14.2 The budget cost estimate must cover thewhole of the anticipated capital expenditure andVAT on the project including :
- departmental costs ;- on-costs;- works costs (total of departmental and on-
costs) ;- location adjustment ;- fees ;- non-works costs;- equipment; and- contingency .
1 .14.3 Once approved, the total of these costs willform the `Approved Budget Cost' . Appendix 2provides detailed information on the make-up ofthe estimate, including the basis of the riskassessment which will determine the contingencysum . Appendix 5 provides guidance onestablishing the equipment budget .
1.14.4 The NHS Executive will need to estimatethe total outturn cost for the scheme and, for thispurpose will assess an additional amount forinflation . The Approved Budget Cost plus theallowance for inflation and VAT will determine theforecast outturn and should be used for anypublicly-announced cost .
1.14.5 Any financial overspend will have to befinanced within the approved External FinanceLimit (EFL) . No additional funds will be madeavailable .
Running Costs1 .15 .1 Further detailed work in developingrunning cost estimates should be carried out . If acosting model has not previously been developed,this may involve the design of the model oncomputer. Running costs estimates should becorroborated by using alternative methods ofestimating and wide consultation .
1.15.2 Sound estimates for annual running costsare more important than capital costing, becausethey are committed costs which affect prices paidby purchasers in the future . Over the life of ascheme they usually have a more significant effecton net present costs than capital expenditure .
Planning for Post-Project Evaluation1.16.1 Post-project evaluation is mandatory for allbuilding schemes with a total cost exceedingS,1 million, and is an activity recommended for allschemes . Initial work must be undertaken toensure effective evaluation later on . Detailedinformation can be found in the Post-ProjectEvaluation .
Obtaining NHS Executive andTreasury Approval if Required1.17.1 Schemes above the advised cost thresholdshould be formally approved by theNHS Executive (and Treasury where appropriate),before proceeding to the next stage . The costthreshold for schemes which require NHSExecutive and Treasury approval will be advisedby the NHS Executive from time to time .
1.17.2 For all schemes submitted to the NHSExecutive for approval, the scheme name mustremain consistent throughout the life of the project.All schemes approved by the NHS Executive willbe subject to formal monitoring procedures .
1.17.3 Schemes above the Treasury threshold willbe subject to a further approval point . This will beat the end of the design stage when the traditionalprocurement route is followed . For alternativeprocurement strategies, an appropriate point willbe agreed by the NHS when the Full Business Caseis approved .
Stage Completion1.18.1 On receipt of approval, initial projectmonitoring reports should be submitted to NHSEstates (see Appendices 7 and 8) .
Stage 2 : Design
General2.1.1 The purpose of this stage is to convert theinitial brief into a full brief and the outline designthrough sketch design to detailed design . Thedetailed plans and specifications should fulfill therequirements of the brief, be of high qualityaesthetically and be economical to build, maintain,and operate .
2.1.2 The design team should operate under theleadership of the lead consultant, usually thearchitect, who has the responsibility for co-ordinating the input of the rest of the team . Theproject director, through the project manager, mustensure that during this process the integrity of thebrief is maintained, the project remains within thebudget, and the process is completed toprogramme .
2 .1 .3 Quality of design is crucial to the success ofa building and will entail careful consideration ofthe aesthetic appearance, the internal ambience,and the functional efficiency . Simply specifyingfunctional requirements may result in an overallscheme which not only disappoints, but proves tobe costly in the longer term because of poor-quality materials necessitating excessivemaintenance or early replacement together withpossible disruption to the Trust's operations. TheTrust should include in the scheme a provision forinterior design, landscaping and artwork toenhance the quality of the environment .
2 .1 .4 The project director should ensure that thedesign team is familiar with the standards issuedby NHS Estates - Health Building Notes, HealthTechnical Memoranda, Health Facilities Guidance,Equipment Notes, Activity Database, etc . Somestandards, for example those dealing with fireprevention and hygiene, are mandatory. Also, useof a standard design system, such as Nucleus, maybe economic and efficient in producing designsolutions . Project Directors and their consultantsmay obtain advice from NHS Estates on the use ofthe above documents and on the process forchoosing an architect and a design team to ensurethat a building of appropriate quality is delivered .
Brief Development2.2.1 Design development may continue intandem with the development of the full brief . Butany design development to sketch plan stage doneduring the preparation of the full brief must becompleted and checked for compliance with thebrief and other constraints before detail design isundertaken . The brief should be developed to
completion by the user team producing datasheets based on the accommodation schedulesproduced in stage 1 . See Appendix 1 for asuggested format for a brief acceptance certificate .
2 .2 .2 It is important for the user panel torecognise that the brief is now `frozen' and,henceforth, any proposed changes must be subjectto formal change control procedures .
Design Management Procedures2.3.1 The purpose of design management is toensure that :
designs comply with the brief, with the briefitself not being altered except through formalchange control procedures ;
changes are strictly controlled and costed ;
options are considered where practicable andappraised ;
designs are well co-ordinated ;
design is completed to programme ;
cost and progress reports are issued at suitableintervals with a minimum of one at mid-stageand one at stage completion; and
the project director and the user panel are keptinformed through meetings and presentations .
2.3.2 The following will apply particularly fortraditional procurement strategies :
The design team is responsible for thetechnical content of the design .
the project manager has no responsibility forthe technical content except to ensure that itcomplies with the brief, but must haveauthority over the design team in matters ofdesign management .
the procedures for design management areincluded in the project execution plan - seeAppendix 6 .
2 .3 .3 The cost estimate produced by the quantitysurveyor must be regularly updated as the designis progressed, through sketch design and intodetailed design, so that the progress reports reflectthe up-to-date position . Refer to Appendix 3 formore advice on cost management .

Design Development
2.4.1 This involves the development of the fullbrief and outline design into sketch designsthrough the following procedures :
Sketch plan designs should be presented to theuser panel to explain how the brief fulfills theirrequirements . They should be encouraged tosuggest anything which will improveoperability for consideration within the changecontrol procedures . These sketch designsshould include :
(a) updated spatial layouts, includingcirculation and communication spaces androom layouts, inclusive of all exposedengineering services based on theinformation defined in the activity database .
(b) major plant and equipment installation, siteaccess and contractors' areas .
If a project is being developed in stages,design stages will overlap but care must betaken to ensure that interfaces between thestages are co-ordinated .
The range of design options for implementingthe brief should be formally considered by thedesign team . The selection criteria include :estimated construction and running costs, riskfactors, programme constraints, operationalfactors, and quality including aestheticappearance . The project manager shouldensure that the results of the recommendedoptions are recorded by the design team .
Final decisions may be taken by the projectdirector or delegated to the project manager orthe design team depending on theirsignificance . The project manager should drawthe attention of the project director to designoptions which affect whole hospital operations,aesthetic appearance, capital and runningcosts, programme, or operability.
2.4 .2 A Certificate of Readiness to Proceed toDetailed Design, signed by the project managerand project director, must be completed for allprojects . It attests to the completeness, adequacyand integrity of the brief and to the cost estimateand programme based on it . A suggested format isprovided in Appendix 1 .
Equipment Schedules
2.5 .1 Equipment schedules for Groups 2 and 3equipment, based on the agreed room datasheets/layouts, should be prepared at this stage .The items available for transfer should beidentified so that schedules for new equipmentcan be prepared and costed, to ensure that theequipment budget established at the Full BusinessCase stage will not be exceeded .
Detail design
2.6 .1 Detail design comprises converting thesketch plan design into production drawings andspecifications which are in sufficient detail forcontractors to prepare a tender, construct thebuildings, install services and purchase clientequipment . Although the process is the samefor all contract procurement strategies, it isdone by different people and at different times,depending on the strategy selected and mayoverlap stages 3 and 4 . Different procedures willapply in each case .
2 .6 .2 Procedures for this stage are as follows :
For traditional contracts, the detail design mustbe completed before tender .
In fast-track contract strategies, design overlapsconstruction .
(a) For design and build, both the design andconstruction are managed by the contractor.The project manager and the projectdirector or the professional adviser shouldassess the suitability of the contractor'sdesign .
(b) For a management contract, or constructionmanagement contracts, the detail design isundertaken progressively, after theappointment of the management contractor,or construction manager, and released asrequired for each work package . However,it is important that the brief is complete andfrozen before the management contract islet . Where final detailing is done by thecontractor or sub-contractor, it must be clearthat they are financially and contractuallyliable for their own design work .
Poor co-ordination of building services, bothbetween the different services and with thebuilding itself, is a common cause of designchanges, resulting in extra cost and delay . Theproject manager must ensure that the designteam has prepared co-ordination drawings andthat these take into account the requirements ofmajor equipment installations .
The quantity surveyor is normally responsiblefor keeping the cost estimate up to date as thedesign progresses and for producing bills ofquantities . It is recommended that bills ofquantities are also prepared for mechanical andelectrical engineering services, preferably by thequantity surveyor who needs to be suitablyqualified .
Planning consent
2.7.1 obtain full planning consent, buildingregulations and other statutory approvals beforetenders are invited for either the main contract orother significant contracts . Any public enquiry musthave been satisfactorily concluded. The planning

authority should be consulted during designdevelopment so that their requirements can betaken into account .
2.7.2 The contractor is sometimes maderesponsible for obtaining planning consent andother statutory requirements in a design and buildor a management contract. In that case, Trusts mayproceed to stage 3 without consent having beenobtained, so long as the risks of failure to obtainit, or of substantial changes being required, areprovided for in the contract.
Tender Documents2.8 .1 During the preparation of the tenderdocuments, the following should be considered :
The documents should be prepared by thedesign team under the direction of the projectmanager .
The mandatory policies in CONCODE must becomplied with . The project manager anddesign team should recommend to the projectdirector the most appropriate form of contract .
The best practice guidance on contractdocuments given in CONCODE should bereferred to .
The drawings and specifications must beappropriate for the contract strategy .
(a) For a `traditional' contract or `management'contract work package, they will becomplete and comprehensive .
(b) for a `design and build' contract, there willbe performance criteria, standards, andquality requirements, with other detailssuch as layout drawings depending on theextent of contractor design. These must becomprehensive to avoid the risk of thecontractor, who will design for greatesteconomy, producing sub-standard facilities .
The specifications must include whatever tests,samples or mock-ups may be required duringthe course of the work to assure quality andcompliance with the specification. This isparticularly important for Group 1 and 2equipment items, which must be tested forperformance, as part of the commissioningprocedure, before acceptance .
Pre-tender Estimate2.9 .1 Trusts must prepare a pre-tender estimateon completion of the tender documents, beforeproceeding to stage 3, using the followingguidelines :
A formal review of the capital and runningcosts and of the programme must be made,including an update of the risk analysis andcontingency allowance . This should bechecked against any constraints in the FullBusiness Case .
If the review indicates that costs exceed thefigure approved by the NHS Executive, thedesign should be reviewed for savings,otherwise re-approval will be necessary (seepara . 2 .10 .3) .
The pre-tender estimate should be preservedfor future reference (refer to Appendix 3 -Cost Estimating) and included in a progressreport to the NHS Executive (see Appendix 8) .
For management contracts see paragraph4.12 .1 .
Stage Completion2.10.1 For the main construction contract, aCertificate of Readiness to Proceed to Tender isrequired . A suggested format is given in Appendix1, but Trusts may need to modify the form to suitthe particular circumstances of a project,particularly the impact of a non-traditional contractprocurement stategy .
2.10.2 The certificate contains assurances fromthe design team that the design :
has been completed to the degree appropriateto the contract strategy;
complies with Building Regulations and Codesof Practice, including Health Service FireStandards, mandatory standards published byNHS Estates, EC or British Standards, includingthe requirements of environmental authoritieswhere appropriate ; and
fulfills the requirements of the brief .
2.10.3 For schemes using conventional lump sumcontracts in excess of Treasury delegated limits orwhere the estimate exceeds that approved, re-approval on completion of the design stage ismandatory and a submission to the NHS Executiveis necessary . For alternative procurement strategiesabove delegated limits, reapproval will also benecessary, at the point for submission agreed withthe NHSE on completion of stage 1 .
2.10.4 The additional conditions for resubmissionat any stage during the life of a project aredescribed in the introduction section to thisdocument .
Stage 3 : Tender andContractGeneral3.1 .1 The general procedures for tendering andawarding contracts apply to both works contractsand for the purchase and installation of Group 1and the installation of Group 2 equipment . Group2, 3, and 4 equipment should be obtained usingthe Trust's normal purchasing procedures, exceptthat the specification and delivery dates should beestablished by the project team, and the purchaserequisition approved by the project director. Theproject director, on the advice of the projectmanager, should decide which purchases fallwithin this category.
3 .1 .2 Nothing may be charged against the projectbudget unless it has been approved by the projectdirector . Trusts should refer to CONCODE for moredetailed advice on the tendering process, includingmandatory NHS policies, alternative contract forms,and guidance on procedures .
3.1 .3 The same basic procedures apply to allcontract procurement strategies . For managementcontracts the contractor will be placing contracts(or sub-contracts) for work packages after the maincontract has been awarded. (These are dealt within stage 4 Construction and Equipment Supply .)
3.1 .4 There will often be some overlap betweenthe design, tender and contract, and the supplyand construction stages . The project manager andthe design team must integrate the procurement ofboth works and equipment into the overall projectprogramme . For example, it may be necessary toorder some Group 2 equipment early to meetdelivery dates or some equipment contracts may beplaced after the main-works contract .
3 .1 .5 The formal post-tender estimate and themandatory completion of the NHS ExecutiveContracts and Cost Analysis Report (seeAppendices 7 and 8) apply only to the main workscontract .
Propriety3.2 .1 As NHS Trusts are public bodies, the policiesgoverning public procurement will apply and theymust have procurement procedures in placecomplying with those policies, whether they havecapital works projects or not . The two mostimportant policies are the maintenance of proprietyand the award of contracts on the basis of bestvalue for money.
3.2.2 Implementation of these policies should beas follows :
Propriety should be maintained throughcompliance with procedures providing checksand balances, placing the responsibility forcontracts on more than one person, ensuringconfidentiality and equal treatment of bidders .
There should be formal delegations of financialauthority for the approval and letting ofcontracts .
Major works contracts should be approved bythe project investment decision maker (usuallythe Trust Board) ;
Project directors should refer to CONCODE formandatory NHS Executive policies dealing withpropriety.
The project director must ensure that projectmanagers and other consultants maintain thesame high standards of propriety .
The project manager should maintainprocedures, and check those of otherconsultants .
Internal audit of these procedures should be aspecific part of the annual internal and externalaudits of Trusts, not simply a requirement ofone stage of a capital project . As long as arecent audit has confirmed compliance, andthe project director is satisfied regarding theprocedures of consultants, this requirement willhave been fulfilled .
Tenders3.3.1 When considering the tendering process, itis essential to refer to CONCODE and pay regardto the strict codes of practice in the constructionindustry . Tendering can be divided into fourcomponent parts:
(a) Tender lists . These should be compiled withregard to the following :
Subject to EC rules when they apply, Trusts, inconsultation with their professional advisers,should invite appropriate firms to pre-qualifyand draw up a tender list of those firms able tomeet all the requirements .
Only firms with appropriate experience andsufficient financial, technical, and humanresources should be permitted to tender. NHSEstates holds a database of contractors andconsultants who have worked for the NHS onmajor schemes . Their performance on contracts

on which they have been engaged will beavailable on application . It is important forproject directors to complete and send in theassessment forms in Appendix 9 for updatingthis information . Some Trusts may have theirown contractor and consultant registers .
Information on previous performance shouldbe sought prior to interviews or presentations ;technical assessments should always be used,normally involving the project manager and,if appointed, the professional adviser . Poorcontractor performance or bankruptcy canhave a devastating effect on the outcome ofa project .
The project manager and project directorshould prepare tender lists, in accordancewith Trust standing financial instructions andCONCODE procedures, and submit the list tothe investment Decision Maker for approval .
Tender costs are not recoverable from Trusts,except by special agreement for some types ofdesign and build contracts, in which contractorsare required to do a substantial amount ofdesign prior to tendering, or where privatefinance is used .
(b) The tender period . This should be longenough to enable contractors to price the workproperly . The length of time will depend onthe type of contract and its complexity. It willbe longer for design and build than for atraditional strategy because the contractor hasto make preliminary designs before he or shecan estimate the price .
(c) Tender assessment. This should be completedas follows :
Tenders should be assessed by a project tenderboard under the direction of the projectmanager .
An assessment report and recommendationshould be given to the Project Director,including all aspects of the tenders --compliance, technical, programme, price, andresources .
For a major works contract, tenderers areusually asked to provide a method statementdescribing how they plan to set about thework and what resources they will use ; this isa good guide to their capability .
The professional adviser, if one has beenappointed, should be consulted by the projectdirector before the contract is let .
Assessment procedures are described in moredetail in CONCODE.
The principle should be to award the contractto the firm whose tender offers best value formoney . For a traditional contract strategy, thisis usually but not always the same as thelowest price .
The tender documents should specify thecriteria which will be used in the assessment ;these may be restricted by EC rules where forapplicable contracts . If the lowest tender is notrecommended, the reasons must be justifiedand be carefully recorded .
The investment decision maker should approveany large contracts before the contract isawarded .
(d) Post-tender negotiation.
This is a process which can give added valueto a contract . It is essential that it is doneethically and in a controlled way under thedirection of the project director .
A Trust may review the most favoured tenderwith the contractor to see whether there areany changes which are mutually beneficialbefore the contract is awarded . It couldinvolve, for example, removing qualifications inthe tender, or considering suggestions from thecontractor to improve buildability, orimprovements to the programme ; any suchnegotiation must not impair the validity of thetender within the overall competition .
The aim is to make sure that, when thecontract is signed, all matters arising from thetendering process have been financiallyresolved to the satisfaction of both parties . Itmust never be a Dutch auction or just anattempt to beat down the price for the job .Tender reductions may be achieved byreducing the specification, elimination of workfrom the project or seeking more efficientconstruction methods .
Post-tender Estimate3.4.1 This stage should include :
- an update of the cost estimate afterassessment and when the recommendedtender price is known . The risk analysis andcontingency allowance should be reviewedas part of this process, because many of theoriginal risk factors - for example, designdevelopment and tender price levels (whichdepend on the state of the constructionindustry at the time) - will no longer apply.This estimate becomes the formal approvedsum in the construction cost plan;
- checking the project against all the otherconstraints defined in the Full Business Case,including running costs, the discounted cash-flow calculations and re-approval criteria ; and
- identifying any savings necessary to staywithin budget - for example, by simplifyingsome of the design or reducing the scope ofthe project. Significant changes to thecontract should be avoided as this may causeproblems for other aspects of the scheme .Any such steps must be dealt with throughthe change control procedure and agreedwith the user panel if they alter the brief.

(A variation in project scope or a cost abovethat approved, will require re-approval fromthe NHS Executive and this must be donebefore the contract is signed . New tendersmay be required if the scope of work hasbeen altered significantly .)
- establishing the approved sum, based on theagreed tender plus any client contingencyallowance .
Stage Completion3.5 .1 Stage completion entails :
Before the contract is awarded, the projectdirector, through the project manager, mustensure that the contract documents have beenbrought up to date to include any agreed post-tender changes .
The Trust must confirm that it is in a positionto make the site available, and that the contractadministrative arrangements are in place .
The contractor must confirm that the tenderremains valid if the normal acceptance period
stipulated in the contract is exceeded .
0
A Certificate of Readiness to Award Contractmust be completed in accordance with theTrust's standing orders .
The project director must ensure that a totalfunding package is available to meet theapproved sum, including contingency andallowances for inflation . This is particularlyimportant where external funding -or privatefinance is involved and could be cash limited .
3.5.2 When all these arrangements are completed,the contract may be awarded, and the contractformally executed .
3.5.3 Following the award of the contract theproject director, through the project manager asappropriate, should:
- notify unsuccessful bidders ;- place a notice in the EC Journal ;- update the project execution plan ; and- complete the NHS Executive post-tenderreport for all projects exceeding the reportingthreshold (see Appendices 7 and 8) .

Stage 4 : Constructionand Equipment SupplyPart A - Applicable to all ContractProcurement Strategies
General
4.1 .1 The objective of stage 4 is to secure thesatisfactory completion of the project on time,within budget, and to the specified qualitystandards . During this stage, constructionprofessionals carry out their duties . The projectdirector stands back, monitors their performanceand is ready to intervene, through the projectmanager, if it becomes necessary . The projectdirector's main tasks in respect of supply andconstruction are :
- to give decisions and approvals which areabove the delegated limits of the projectmanager ;
- to be aware of cost, progress, and anypotential problems, and ensure thatcorrective action is taken where necessary ;
- to communicate to the project manager anyrequirements or concerns which need to beraised by the Trust, keeping in mind thatchanges to the design or specifications arethe major cause of time or cost overruns ;
- to ensure that no changes are initiated bythe Trust itself, unless they are absolutelyessential . The only changes which should beaccepted without challenge are those due tochanges in legislation, those required onhealth and safety grounds, and those which,if they are not made, would prevent theproject from achieving its objectives .Whenever possible, such changes should beimplemented post contract in order to avoiddisruption to the on-going contract . Otherchanges which are considered desirable butnot essential should also be deferred and re-considered following completion of thecontract . Refer to Appendix 3 for moreinformation on change control procedures .
4.1.2 During this stage the project director mustalso ensure that plans are developed, which willbe available in time for:
- operational commissioning, includingequipping, by the Trust ;
- supply of start-up stocks of operationalconsumables and of spare parts ;
- operations staffing and staff training ;- occupation .
4 .1 .3 Refer to Commissioning ofa Health CareFacility for more detailed guidance .
4.1.4 The general procedures for managingcontracts apply to all procurement strategies, butsome alternative procedures are unique to non-traditional forms of procurement. To take accountof the main alternative methods, stage 4procedures are divided into four parts :
- procedures applicable to all contractprocurement strategies ;
- procedures applicable to design and build ;- procedures applicable to management
contracts ;- procedures applicable to management
contracts ; and- procedures applicable to equipment supply
contracts .
4.1 .5 Project directors should ensure that theproject managers and contractors are familiar withand comply with Health and Safety regulationsapplicable to building sites, such as the Temporaryor Mobile Sites Construction Directive . The Healthand Safety Executive can provide advice on theregulations .
Contract Administrator
4.2.1 Construction contracts are administered onbehalf of the Trust by a person appointed as the`contract administrator' . A similar position - usuallycalled the `engineer' - may apply in civilengineering contracts and in equipment contracts,particularly those for both supply and installation .
4.2.2 Procedures regarding appointment of thecontract administrator and the role of the appointeeare as follows :
The contract administrator's role and duties aredefined in the contract. These are of two kinds :
(a) to inspect work and instruct the contractoron behalf of the Trust, in accordance withthe terms of the contract . Performance ofthese duties is subject to delegatedauthority, and the contract administrator isresponsible through the project manager tothe project director ;
(b) to give decisions in a fair and impartial'quasi-judicial' manner on contract issues .When the contract administrator is acting ina quasi-judicial role, the project directorthrough the project manager may state theTrust's position, but must not issueinstructions with the intention of influencingthe contract administrator's decisions . Thecontract administrator must notify theproject director before issuing a decison

which exceeds his or her delegatedauthority .
'
The lead consultant (usually the architect intraditional procurements) should normally beappointed as contract administrator but theproject manager may undertake the role . Theappointment of the project manager as contractadministrator must not dilute the responsibilityof the design team for the integrity of thedesign and compliance with specifications . Itmeans that changes or instructions initiated bythem are reviewed and issued by the projectmanager.
'
The contractor must be formally notified of thename of the contract administrator by theproject director. The contract administrator'sdelegated authority is confirmed to him or herin writing . The extent of this delegation will beincluded in the project execution plan - seeAppendix 6 - and will include his or herauthority in respect of:
(a) utilisation of provisional sums;(b) ordering changes ; and(c) ordering acceleration to mitigate delays .
' All formal communications with contractorsmust be through the contract administrator .
Production Information
4.3 .1 This is the information required by thecontractor to carry out the contract . The bulk ofthe information is contained in drawings, bills ofquantities and specifications in the contractdocuments but the following will apply :
' In a traditional contract strategy, the detaileddesign should be completed before theinvitations to tender are issued and thecompletion of the Certificate of Readiness toProceed to Tender confirms this ; any drawingsissued after the contract has been let constitutea change and may have cost and timeimplications.
' The project manager should manage the designteam to prevent from initiating unnecessarychanges . Some changes, such as those arisingfrom late equipment details or non-availabilityof components, may be unavoidable andshould be managed through the changecontrol procedure .
' The project director must make sure, throughthe project manager, that :(a) all production information is prepared by
the design team, to meet the contractor'sprogramme requirements so that it isavailable to the contractor in good time ;and
(b) any variations arising from the issue ofproduction information after a contract hasbeen let are managed through the changecontrol procedure .
Progress Monitoring
4.4.1 The project director should ensure thatappropriate systems are in place in order thathe/she is fully informed on time, quality and cost .It will be the primary role of the project manageron a day-to-day basis, reporting to the projectdirector on a formal basis (usually monthly) and byexception where particular issues arise .
Programme Management
4.5.1 Each contract, when awarded, will containits own programme, which will be compatible withthe project programme, and which will list keymilestone dates . The project manager isresponsible for maintaining the overall projectprogramme and for monitoring actual progressagainst it . This should be managed as follows :
'
A contractor will usually be required to submita master programme for the contract workwithin a short period after award of contract,for examination by the project manager. Thismay be used for subsequent monitoring .
' Certain circumstances will entitle a contractorto have an extension to the completion date .These circumstances, which are detailed in thecontract, would be beyond the reasonablecontrol of the contractor, such as force majeureand changes instructed by the contractadministrator. If such circumstances occur, thecontractor will submit a claim for an extensionof time to the contract administrator who willaward such extension as is reasonable in thecircumstances ; this is one of the quasi-judicialfunctions of the contract administrator . Thecontract programme is then amendedaccordingly .
' The project manager must monitor eachcontract against its approved programme, andreport against it in a monthly Project ProgressReport (PPR) to the project director . The PPR,which also includes a monthly cost report, isan important part of the management of theproject. It enforces a discipline on all parties tomake sure that work is proceeding toprogramme, it also enables the project directorand the project manager to take correctiveaction if problems become apparent . Theproject manager should give an executivesummary of it to the chief executive officerand, where appropriate, the Trust Board . (Referto Appendices 7 and 8 for a more detaileddescription of monitoring requirements .)
'
If delays become apparent, the project manageris responsible for initiating corrective action.This action may have cost consequences, to bepriced by the quantity surveyor, and couldaffect the completion date of the project and itsfinancial viability . The project manager shouldconsider the available alternatives and make aformal recommendation to the project director .The consequences must be included in the costestimates .

Quality Control4.6 .1 There are two main requirements :
- to check that all construction work done bycontractors is in accordance with thedrawings and specifications . This is thecontract administrator's résponsibility but inpractice it is carried out by representives ofthe design team, who ask the contractadministrator to issue necessary instructionsto the contractor. There may also be a clerkof works appointed, based on the site, whohas delegated authority to act as inspector onbehalf of the client . The clerk of works hasno authority to change the specifications,only to see that they are complied with ; and
- to ensure that the inspection and testingprocedures in the specification have beencomplied with .
Cost management4.7 .1 Management of the overall cost of a projectis a function of the project manager, who isresponsible to the project director . The proceduresfor this are as follows :
- to operate change control procedures .Although cost reports, estimates, andforecasts are prepared by the quantitysurveyor, the project manager is directlyresponsible for understanding the costconsequences of any decisions and forinitiating corrective actions if necessary ;
- to maintain an up-to-date estimated cost andcash flow ;
- to manage expenditure of contingencies ;- to initiate action to avoid overspend . The
project programme, which includes allcontracts, and the programmes and terms ofpayment for individual contracts, must becompatible with the approved fundingarrangements . If the forecast cash flowshould vary from that approved, the Trustmust notify the NHS Executive immediatelyfor schemes approved by the NHS Executive ;
- to issue a monthly financial status report .This report is prepared by the quantitysurveyor with comments by the projectmanager, and is submitted as an integral partof the Project Progress Report (PPR) . It mustinclude the results of monitoring by theproject manager of the overall cost of theproject, including each individual contract,against the approved budget . Refer toAppendix 3 for information on costmanagement procedures to be included inthe project execution plan and to Appendix 7on monitoring ; and
- to submit the NHS Executive MonthlyProgress Report for all projects exceeding thereporting threshold . The project manager isresponsible for completion of the report forthe approval of the project director, but inpractice it will be prepared by the quantitysurveyor . Refer to Appendix 7 .
Payment4.8 .1 Trusts, as the contracting parties, areresponsible for paying contractors and suppliersthe interim and final payments to which they areentitled. These should be made as follows :
In most construction contracts, the quantitysurveyor will agree valuation of interimpayments due during the course of the work,which the contract administrator will consider,and if agreed will issue a payment certificate.
Trusts should pay the amount certified on time .
The project director, on the advice of theproject manager, should keep the Trust financedepartment aware of future paymentrequirements by means of the updated cashflow forecast .
Claims4.9.1 The terms of the contract allow contractorsto claim additional payments in certaincircumstances defined in the contract conditions .These are generally due to either:
- risks occuring which are client risks underthe contract, such as unforeseeable groundconditions, the ordering of additional orvaried work (when a design and buildcontract is used it is possible for some ofthese risks to be transferred to thecontractor) ;
- failure by the Trust to comply with itsobligations under the contract . This is oftenexpressed as disruption of the contractors'work programme due to changes or lateinformation .
The conditions of these claims, and the way theyshould be dealt with, are as follows :
Assessment of claims, both as to validity andamount, is a responsibility of the contractadministrator.
Contractors are obliged to notify the contractadministrator of a claim within a limited timeafter the occurrence of the events which giverise to it, and to provide full details as soon aspracticable thereafter . The project managershould keep a record both of notified claimsand of expected claims which have not yetbeen notified .
Claims which are valid under the contractshould be ascertained as quickly as possible tofacilitate prompt payment . Circumstances wheninterim payments may be made are describedin CONCODE.
The contract administrator may have to makeextensive and detailed enquiries before thevalidity and cost consequences of a claim canbe determined . However, as soon as a claim orpotential claim is identified, the project
manager must include it in the Financial StatusReport, using the best available estimate of theconsequences .
Whenever recourse to arbitration or litigation iscontemplated or undertaken, this must benoted in the comments section of the NHSExecutive Monthly Progress Report . It isrecommended that the project director formallynotifies the NHS Executive of the situation andseeks advice . Use should be made of theexperience of the professional advisers orsources advised by the NHS Executive .
Record keeping4.10.1 Maintenance of good records of siteactivities is a responsibility of the project manager .The project director should ensure, throughpersonal inspection, that this is carried outthoroughly . These records are necessary to providean audit trail and information for the post-projectevaluation . They are essential for the assessment ofclaims, and particularly for any disputes which goto arbitration or litigation . In any dispute, the sidewith the best and most complete records is in thestrongest position . Records must include :
a daily diary, maintained by the clerk of works ;
all site instructions and change orders ;
inspection and testing results ;
drawing issues and revisions ;
requests for information or instructions by thecontractor;
any circumstances which might give rise to aclaim ; and
other matters which the project managerconsiders significant .
Part B - ProceduresApplicable to Designand BuildGeneral4.11 .1 There are several versions of a design andbuild contract . Trusts should refer to CONCODE fora description of their characteristics and thecircumstances under which they are appropriate .They have the following characteristics :
0
Detailed design is the responsibility of thecontractor, rather than the design team and insome cases the contractor is also responsiblefor part of the conceptual design .
A design and build contract specifies theperformance and quality criteria which thecontractor must meet. The contractor is
responsible for the design meeting thosecriteria .
The Trust's consultant designers, who write theperformance specification to give effect to thebrief, are still necessary during a design andbuild contract, but their responsibilities aredifferent from those for a traditional contract .
The trust's consultant designers examine thecontractor's designs for compliance with thespecifications . This examination should include :
(a) drawings v . specification ;(b) materials v. specification ;(c) equipment v . specification ; and(d) contract sum analysis v . approved sum .
The project director should, through the projectmanager, see that the Trust's consultants do notimpose their design preferences on thecontractor . If any such preferences are to beenforced they must be included in thespecifications .
Part C - ProceduresApplicable toManagement ContractsGeneral4.12.1 Trusts should refer to CONCODE forguidance on management contracts, for thecircumstances when this strategy is appropriate,and the forms of contract:
The construction work is divided into workpackages which are placed as separatecontracts (or sub-contracts) co-ordinated andmanaged by the management contractor .
The management contractor may also providesome common site services, such asaccommodation, cranage and security .
The Trust pays the management contractor'sfee plus the actual cost of the work packages .
The management contractor is responsible fordefining the content of, and interfaces between,the work packages .
The project manager must ensure that thedesign is co-ordinated with the packages, bothas to content and timing, and must check themanagement contractor's proposals .
Each work package is awarded subject to theapproval of the project director on the adviceof the project manager. Each tender is subjectto the general procedures applicable to thisstage, but the aspects mentioned in para . 4 .12 .3must be addressed in particular.

4.12.2 The reason for using a managementcontract is usually that it permits an earlier start toconstruction before the detailed design has beencompleted . The disadvantage may be a lack ofcertainty in the final cost . The consequences arean overlap of the stages of a traditional contractand that :
- the design only has to be completed foreach work package when that package istendered, with separate certificates ofreadiness to proceed to tender provided foreach package;
- the procedures for calling tenders for theindividual work packages and assessingthem is undertaken by the managementcontractor, not the project manager ; and
- the post-tender estimate prepared afteraward of the management contract is lessrobust because the final cost for the workwill only be known after the last workpackage has been let .
4.12.3 The management contractor will preparean Estimate of Prime Cost (EPC) in conjunctionwith the design team . The EPC will be the controlfigure against which the individual work packagetenders will be invited and must be fullyreconcilable with the approved budget cost . Alltenders must be subject to formal recommendationand report . Savings arising from the receipt ofpackage tenders within the EPC will form aseparate reserve out of which any justifiableincreases in the cost of other package tenders canbe offset . Any resultant balance must remain underthe control of the project director . Any increase intotal cost must be subject to formal reporting and
approval procedures and reasons for increasesover the EPC identified . Increases in cost arisingfrom tender indexation should be consistent withpromulgated NHSE guidance .
4.12.4 The availability of funding to meet anyincrease in tender costs must form part of thereporting process .
4.12.5 For a management contract, it is importantthat the monthly financial status reports (see para .4 .7 .1) embrace the complexities of this method ofprocurement involving reporting on a series ofseparate work packages .
Part D - ProceduresApplicable to Group 2,3, and 4 EquipmentContractsEquipment Purchase
4.13.1 The purchase of Group 2, 3 and 4equipment will normally take place during theoperational commissioning period through theTrust's normal purchasing procedures (seeCommissioning a Health Care Facility) . However,care should be taken at this stage to ensure thatGroup 2 equipment which has significant designimplications is discussed fully with the designteam and contractor to ensure compatibility,delivery at the appropriate time and properinspection and testing .

Stage 5 : TechnicalCommissioning andHandoverGeneral5.1 .1 This stage deals with technicalcommissioning of the building, services, andequipment . The project director must co-ordinateall activities to ensure that the Trust is ready whenthe project is handed over. The characteristics ofthis stage are as follows :
There are two different aspects to thecommissioning of a health building project :
(a) technical commissioning of the building,services, and equipment to ensure that itcomplies with the quality and performancespecifications and that all systems operatesatisfactorily. This is normally undertakenunder contract managed by the projectmanager assisted by the design team andwitnessed on behalf of the trust as theclient .
(b) operational commissioning by the Trust,covering the process of preparing tooperate the completed facility, to providethe health care services for which it wasdesigned, and maintain and operate thebuilding services . This is a separate processdescribed in Commissioning a Health CareFacility.
Technical commissioning requirements willhave been considered in the design stage andincluded in the specifications for constructionand equipment contracts . It is particularlyimportant that the performance of equipmentand of M and E services are specifiedadequately, including any tests on completionwhich will form part of the commissioningprocess .
Projects may be taken over in sections if themain contract provides for it . If there areseveral contracts, they may be commissionedand handed over for operation at differenttimes . This will have been stated in the briefand included by the project manager in theproject programme .
Organisation of Commissioning5.2.1 The organisation of commissioning shouldtake account of the following points :
Commissioning is the responsibility of the
contractor, except in the case of Group 2 and 3equipment contracts .
The project manager should require thecontractors and suppliers (if there are morethan one) to provide commissioningprogrammes and method statements indicatingwhen and how they propose to commissiontheir work, in accordance with their contractprogrammes and specifications .
The project manager, supported by the designteam, will check these programmes and co-ordinate them with the overall projectprogramme ; they will be accepted if satisfactoryor returned for amendment if not .
The project director must make sure that theprogramme is co-ordinated with that foroperational commissioning.
The team responsible for supervisingcommissioning will include representativesfrom the design team and from the user panel ;the project director should agree itscomposition with the project manager .
Individual members of the user panel shouldwitness the commissioning of those parts of theproject which they will be responsible foroperating so that they can satisfy themselvesthat it is suitable for operation, and draw theattention of the project director and projectmanager to any concerns ; they must notinstruct the contractor themselves .
Inspection and Testing5.3 .1 The process of commissioning is one ofinspecting the completeness and quality ofbuilding work for compliance with thespecification, and of testing equipment and systemsfor satisfactory operation and compliance withspecified performance criteria . Important elementsof this process are :
- testing integrated systems, which maycomprise components from several sources,to ensure that the system as a wholeperforms satisfactorily ;
- maintaining records of inspections and ofcommissioning test results by the projectmanager to be given to the project directoras a permanent record on completion of theproject;

- listing minor defects which do not preventthe facility from being used satisfactorily on a`snag list' during commissioning. These donot prevent the issue of a Certificate ofPractical Completion, but are left to becorrected later . The project manager mustmake a formal list of these, which is attachedto the Certificate when issued . The projectdirector and user panel should draw anysuch defects which they notice to theattention of the project manager; and
- ensuring that only those items which do notcomply with the specifications are regardedas unacceptable . A standard of performancemay not be required during commissioningwhich was not covered by the contract infulfilment of the brief.
Other Deliverables
5.4 .1 A contract is only complete when all thespecified deliverables have been supplied .Typically these include :
- equipment spare parts ;- operating and maintenance manuals ; and- as-built drawings, including a Health and
Safety file - their technical content should bechecked by the design team to ensurecompleteness .
The following should be observed :
It is recommended that delivery of these itemsshould be included in the contract programmes .
Their receipt should be made a condition of aCertificate of Practical Completion . If they areleft until later, it can affect the efficiency ofoperations, and it may be difficult to persuadethe contractors to give them adequate attention .
Certificate of Practical Completion andStage Completion
5.5 .1 A Certificate of Practical Completion isissued by the contract administrator when thecontract works have been satisfactorily completedand commissioned, subject to a snags list . Theform and term used for this certificate may differdepending on the form of contract used, but theresult is essentially the same :
The issue of a Certificate of PracticalCompletion has important contractual andpractical effects :
(a) It relieves the contractor of his or herobligations under the contract, except thoseof making good defects during the DefectsLiability Period and responsibility for latentdefects .
(b) The Trust takes possession of the contractworks or equipment for operation .
(c) The Trust becomes responsible formaintaining and insuring the facility .
If a part of the works, or a separately supplieditem of equipment, is taken over before thewhole of the works, the same effects apply tothat part and the Trust becomes responsible forits safekeeping .
On practical completion, it is usual for there tobe a payment due to the contractor, todischarge the contractual obligations to releasea part of the retention monies which have beenwithheld during the course of the work. This isincluded in an interim valuation by the quantitysurveyor for certification by the contractadministrator.
Stage : 6 Post Completion
Claims and Final Accounts
6.1 .1 Appendix 3 gives guidance on handlingclaims and completing final accounts at this stage .
Defects
6.2 .1 The Defects Liability Period normallyextends for one year after practical completion .During this period :
The contractor must rectify defects identifiedon the snags list at practical completion, aswell as defects identified subsequently duringthe Defects Liability Period in the course ofoperation . This applies to both constructionand equipment contracts .
The project director, project manager, contractadministrator and design team are responsiblefor ensuring that the defects are rectified bythe constructor/supplier, and that:(a) defects identified by the operating staff are
notified to the contractor through thecontract administrator;
(b) defects are rectified satisfactorily andwithout undue delay ; and
(c) defects are rectified with a minimum ofdisruption to the Trust's operations .
Final Certificates
6.3.1 Procedures and conditions concerning theissue of the final certificates are as follows :
Final certificates are issued by the contractadministrator after the end of the DefectsLiability Period and when all notified defectshave been corrected, and when final accountsclaims have been settled .
The certificate effectively ends the contractor'scontractual liabilities ; except in the case offraud, and except for any outstanding disputesand latent defects .
When the last Final Certificate has been issued(in the case where there are several phases orsections have been handed over to the trust),the project is at an end, except for post-projectevaluation and completion of the last NHSExecutive Project Report Form .
The Final Certificate entitles contractors to thereturn of any retention monies .
Stage Completion
6.4 .1 Stage completion is undertaken as follows :
A final NHS Executive Report Form must besubmitted after all final accounts have beenagreed Final Certificates issued and internalaudit: clearance . This records the final outturncost and achieved programme for the project.
After completion, all consultants should handover their documents on the project to theproject director for retention by the Trust . Thenumber of those documents handed over willvary depending on the project, but shouldinclude those :
(a) which may be required for audit or torespond to Ministerial or Parliamentaryrequests for information, including thoserelating to procurement ; and
(b) which relate to tests of quality or forcompliance with performance specifications .
Handover of documents may be deferred untilafter completion of the post-project evaluation .
6.4.2 The entire scope of the Full Business Caseshould have been implemented, which willidentify :
- the total cost and time for completion of theoverall scheme ; and
- all quality requirements and functionalcontent .

Appendices
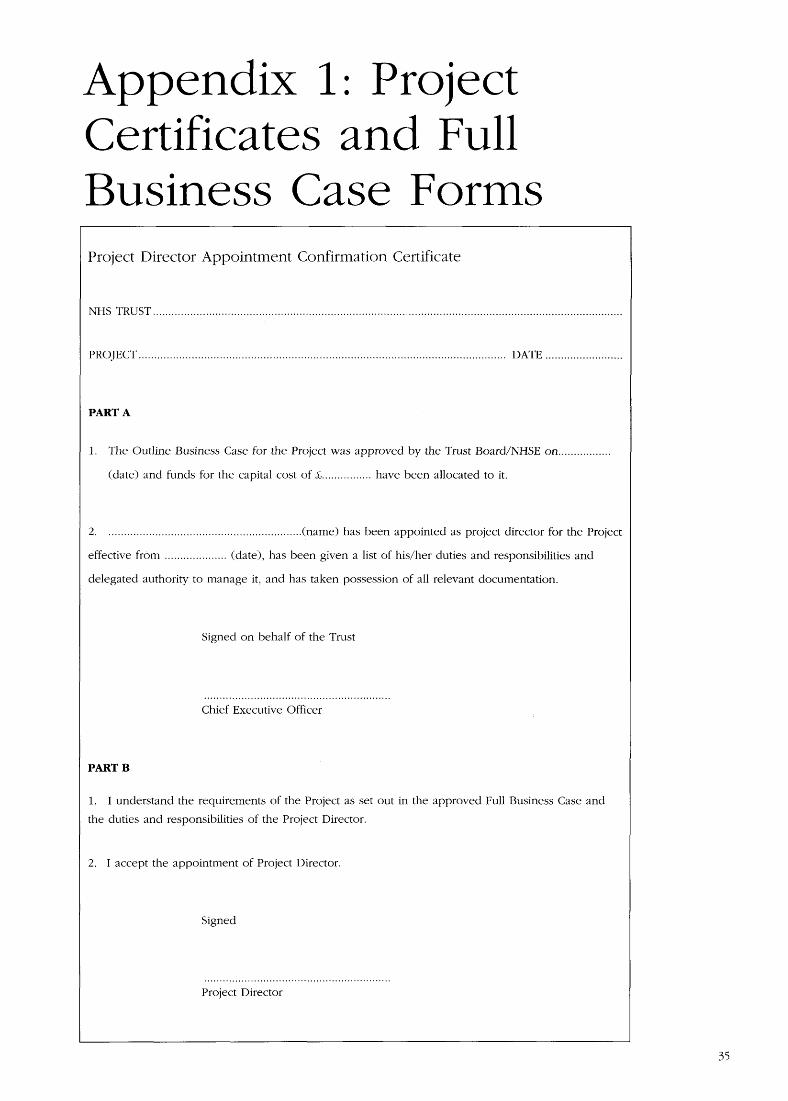
Appendix 1 : ProjectCertificates and FullBusiness Case FormsProject Director Appointment Confirmation Certificate
NHS TRUST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
PROJECT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . DATE . . . . . . . . . . . . . . . . . . . . . . . . .
PART A
1 .
The Outline Business Case for the Project was approved by the Trust Board/NHSE on . . . . . . . . . . . . . . . . .
(date) and funds for the capital cost of £ . . . . . . . . . . . . . . . . have been allocated to it .
2 .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .(name) has been appointed as project director for the Project
effective from . . . . . . . . . . . . . . . . . . . . (date), has been given a list of his/her duties and responsibilities and
delegated authority to manage it, and has taken possession of all relevant documentation .
Signed on behalf of the Trust
Chief Executive Officer
PART B
1 .
1 understand the requirements of the Project as set out in the approved Full Business Case and
the duties and responsibilities of the Project Director .
2 .
1 accept the appointment of Project Director .
Signed
Project Director
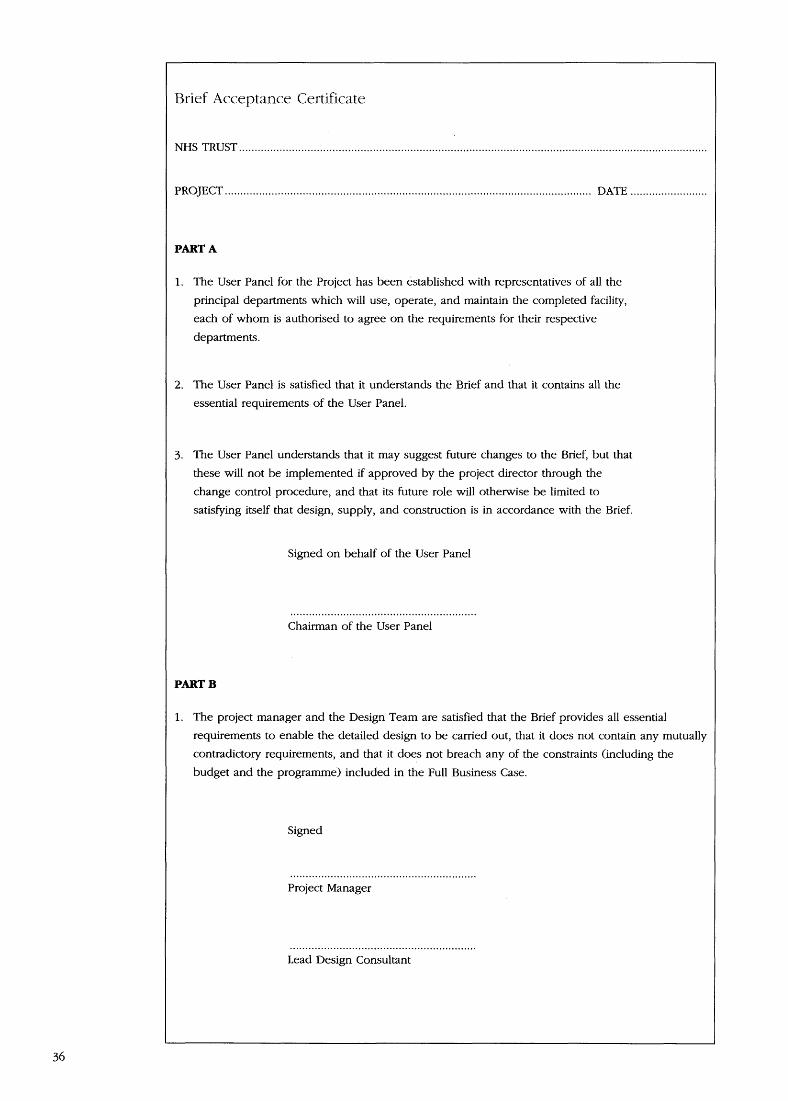
Brief Acceptance Certificate
NHS TRUST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
PROJECT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . DATE . . . . . . . . . . . . . . . . . . . . . . . . .
PART A
1 .
The User Panel for the Project has been established with representatives of all the
principal departments which will use, operate, and maintain the completed facility,
each of whom is authorised to agree on the requirements for their respective
departments .
2 .
The User Panel is satisfied that it understands the Brief and that it contains all theessential requirements of the User Panel .
3 . The User Panel understands that it may suggest future changes to the Brief, but that
these will not be implemented if approved by the project director through the
change control procedure, and that its future role will otherwise be limited to
satisfying itself that design, supply, and construction is in accordance with the Brief.
Signed on behalf of the User Panel
Chairman of the User Panel
PART B
1 .
The project manager and the Design Team are satisfied that the Brief provides all essentialrequirements to enable the detailed design to be carried out, that it does not contain any mutually
contradictory requirements, and that it does not breach any of the constraints (including the
budget and the programme) included in the Full Business Case .
Signed
Project Manager
Lead Design Consultant

Certificate of Readiness to Proceed to Detailed Design
NHS TRUST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
PROJECT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . DATE . . . . . . . . . . . . . . . . . . . . . . . . .
PART A
1 .
The Brief has been completed and a Brief Acceptance Certificate has been signed by the User
Panel, the Project Manager, and the Lead Design Consultant .
2 . The contract procurement strategy has been reviewed and it has been decided to adopt a
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . strategy .
3 . The Project internal organisation is in place and all necessary external consultants have beenappointed . Their duties and delegated authorities are appropriate for the contract procurement
strategy to be used .
4 . The cost estimate and programme have been reviewed, and a risk analysis undertaken and
appropriate contingency allowance made . The latest estimated cost, the programme, and the Brief
are within the constraints provided in the Full Business Case submission or subsequent re-
approval . The Project does not require re-approval .
Signed
Project Director
Approved
Chief Executive Officer
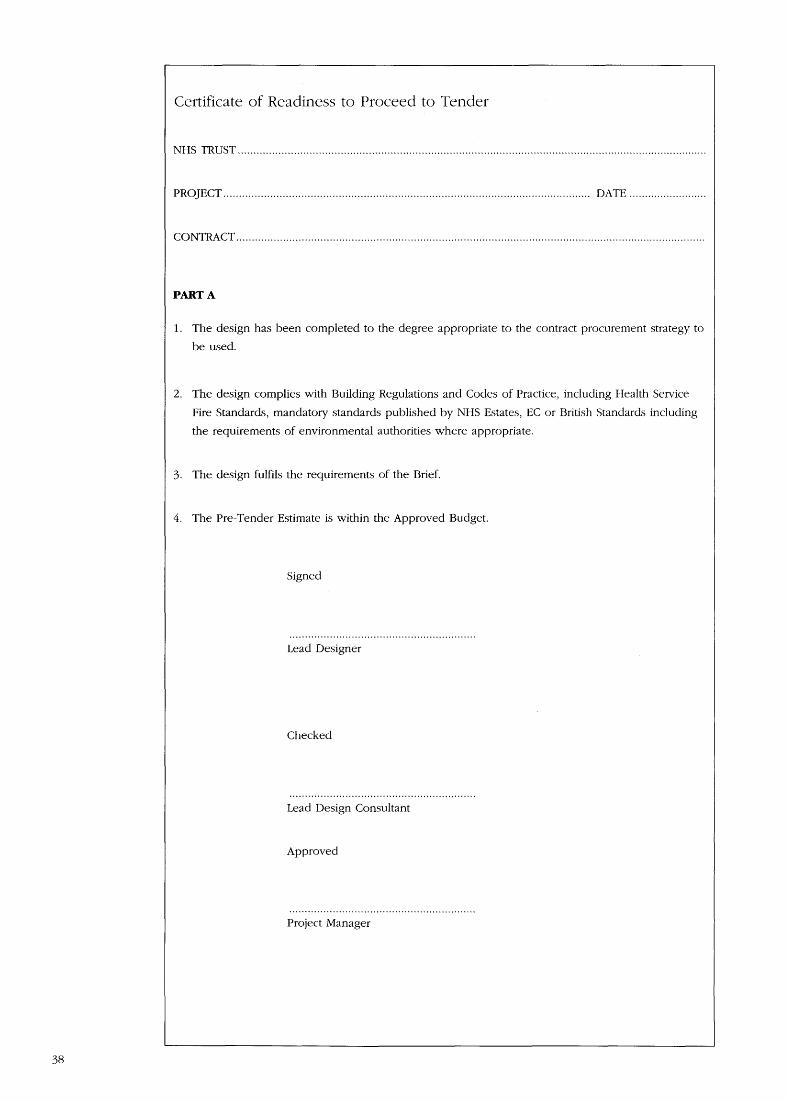
Certificate of Readiness to Proceed to Tender
NHS
TRUST . . . . . . . . . . . . . . . . . . . . . . . . _ . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
PROJECT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
DATE . . . . . . . . . . . . . . . . . . . . . . . . .
CONTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
PART A
1 . The design has been completed to the degree appropriate to the contract procurement strategy to
be used .
2 .
The design complies with Building Regulations and Codes of Practice, including Health Service
Fire Standards, mandatory standards published by NHS Estates, EC or British Standards including
the requirements of environmental authorities where appropriate .
3 .
The design fulfils the requirements of the Brief.
4 . The Pre-Tender Estimate is within the Approved Budget .
Signed
Lead Designer
Checked
Lead Design Consultant
iApproved
Project Manager

FULL BUSINESS CASE FOR PREFERRED OPTION
COST FORM FB1
TRUST/PROVIDER UNIT* . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
ORGANISATIONAL CODE: . . . . . . . . . . . . . . . . . . . . . . . . . . . .
SCHEME : . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
ROME CODE : . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
PHASE : . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
PROJECT DIRECTOR: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
CAPITAL COSTS SUMMARY
Cost Exc.VAT
VAT
Cost Incl.VAT£
1 .
Departmental Costs (from Form FB2)
2 .
On-Costs (a) (from Form FB3)(
% of Departmental Cost)
Works Cost Total (1+2) at . . . . . . . . .FP/VOP*MIPS3 .
(Tender Price index level1975 = 100 base)
4 .
Provisional location adjustment (if applicable)(
% of S,
) (b)
5 .
Sub Total (3+4):
6 . Fees (,)
(a)(
% of sub-total 5)
xxxxxxxxxx
Non-Works Costs (from Form FB4) (e)
7 .
LANDOTHER
8 .
Equipment Cost (from Form FB2)(
% of Departmental Cost)
9 . Contingencies
10 .
TOTAL (for approval purposes)
11 .
Inflation Adjustments (f)
12 .
FORECAST OUTTURN BUSINESS CASETOTAL
Cash Flow:-
SOURCE
£,
Year EFL OTHER PRIVATEGOVERNMENT
Total Cost (as 10 above)
This form completed by : . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Telephone No : . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Address :
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Date :
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Authorised by :
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .PROJECT DIRECTOR
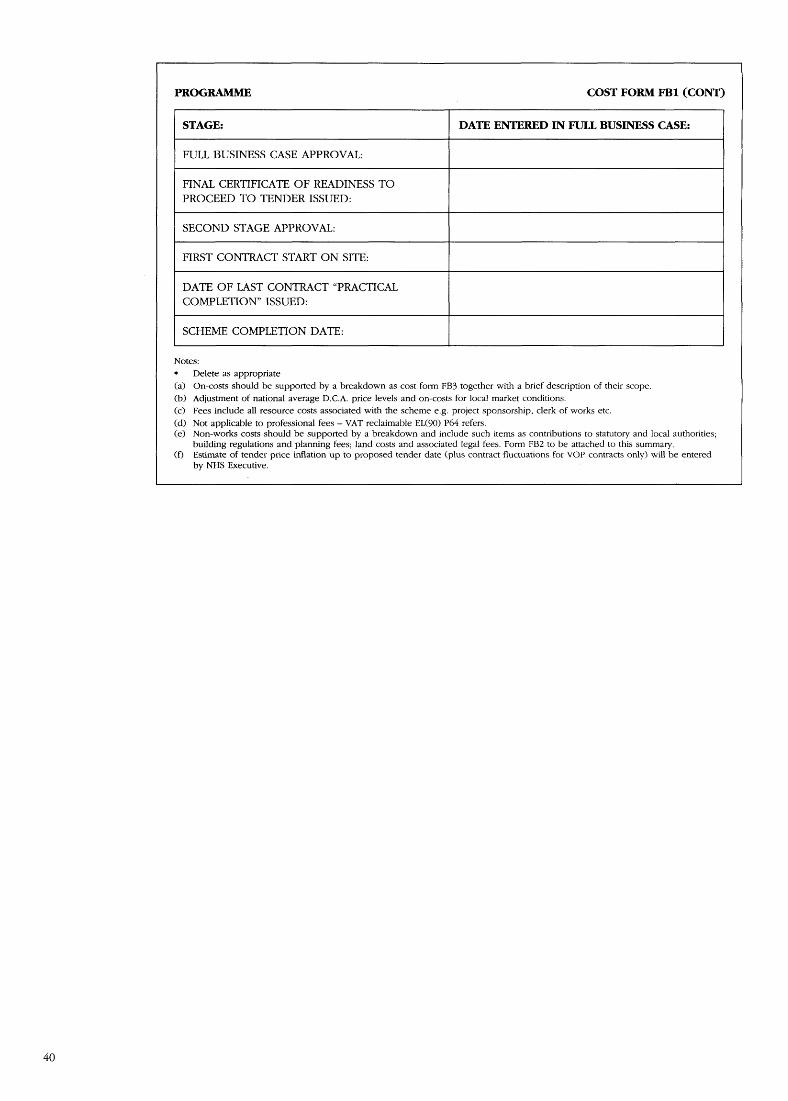
PROGRAMME
COST FORM FBI (CONT)
STAGE:
DATE ENTERED IN FULL BUSINESS CASE:
FULL BUSINESS CASE APPROVAL :
FINAL CERTIFICATE OF READINESS TOPROCEED TO TENDER ISSUED :
SECOND STAGE APPROVAL:
FIRST CONTRACT START ON SITE:
DATE OF LAST CONTRACT "PRACTICALCOMPLETION" ISSUED :
SCHEME COMPLETION DATE :
Notes :*
Delete as appropriate
(a)
On-costs should be supported by a breakdown as cost form FB3 together with a brief description of their scope.(b) Adjustment of national average D .C .A. price levels and on-costs for local market conditions .
(c)
Fees include all resource costs associated with the scheme e .g . project sponsorship, clerk of works etc .
(d) Not applicable to professional fees - VAT reclaimable EL(90) P64 refers .(e) Non-works costs should be supported by a breakdown and include such items as contributions to statutory and local authorities ;
building regulations and planning fees ; land costs and associated legal fees . Form F132 to be attached to this summary .(f)
Estimate of tender price inflation up to proposed tender date (plus contract fluctuations for VOP contracts only) will be enteredby NHS Executive.

FULL BUSINESS CASE FOR PREFERRED OPTION
COST FORM FB2
TRUST/PROVIDER UNIT* . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
SCHEME : . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
PHASE : . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
PROJECT DIRECTOR : . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
CAPITAL COSTS : DEPARTMENTAL COSTS AND EQUIPMENT COSTS
Functional Content
Function Units/Space
N/A/C (2)
Cost Allowance Equipment CostRequirements a>
Version (3) . . . . . .
Version (3) . . . . . .
Less abatement fortransferred equipment ifapplicable ( . . . . . . . . . . .%) (4)
Departmental Costs and Equipment Costs to Summary
£,(Form F131)
See notes overleaf.

COST FORM FB2 (CONT)
This form completed by : . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Telephone No : . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Date : . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Notes :
Cost allowances should be based on Departmental Cost Allowances where appropriate and includeallowances for essential complimentary accommodation and optional accommodation and serviceswhere details not available .Identify separately any proposed adjustment (over or under cost allowances) justifiable in value formoney terms (details to be provided) .
Delete as appropriate
1 .
State area and rate if departmental cost allowance not available2 . Insert:
N for new build,
A for adaptations for alternative use orC for upgrading existing building retaining current use
3 .
Insert relevant version number of CONCISE 4 database listing of Departmental Cost Allowances and
Equipment Cost Allowances4
Provide details where appropriate
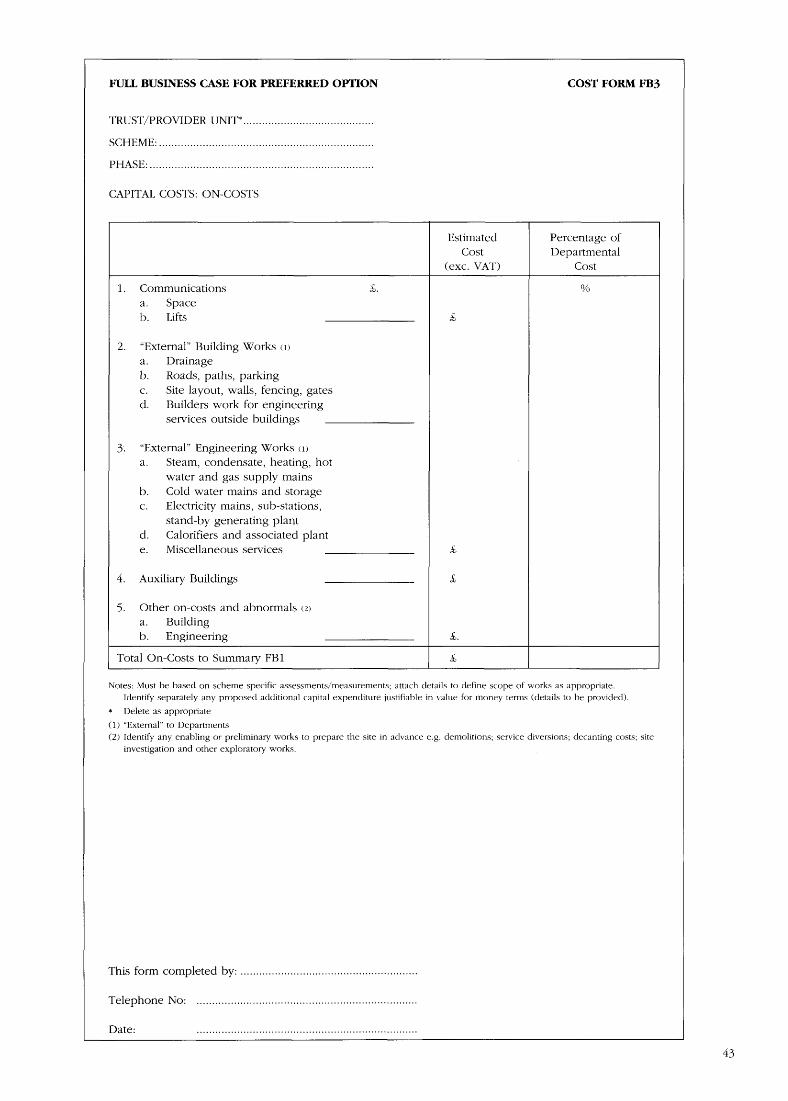
FULL BUSINESS CASE FOR PREFERRED OPTION
COST FORM FB3
TRUST/PROVIDER UNIT* . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
SCHEME : . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
PHASE : . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
CAPITAL COSTS : ON-COSTS
Estimated
Percentage ofCost Departmental
(exc . VAT)
Cost
1 . Communications
£.a. Spaceb. Lifts
£,
2.
"External" Building Works a)a . Drainageb .
Roads, paths, parkingc .
Site layout, walls, fencing, gatesd.
Builders work for engineeringservices outside buildings
3 .
"External" Engineering Works (1)a .
Steam, condensate, heating, hotwater and gas supply mains
b .
Cold water mains and storagec .
Electricity mains, sub-stations,stand-by generating plant
d .
Calorifiers and associated plante .
Miscellaneous services
£,
4.
Auxiliary Buildings
5 .
Other on-costs and abnormals (2)a . Buildingb . Engineering
£.
Total On-Costs to Summary FB1
£
Notes : Must be based on scheme specific assessments/measurements ; attach details to define scope of works as appropriate .Identify separately any proposed additional capital expenditure justifiable in value for money terms (details to be provided).
Delete as appropriate
(1) "External" to Departments(2) Identify any enabling or preliminary works to prepare the site in advance e .g . demolitions; service diversions ; decanting costs ; site
investigation and other exploratory works .
This form completed by: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Telephone No : . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Date :
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
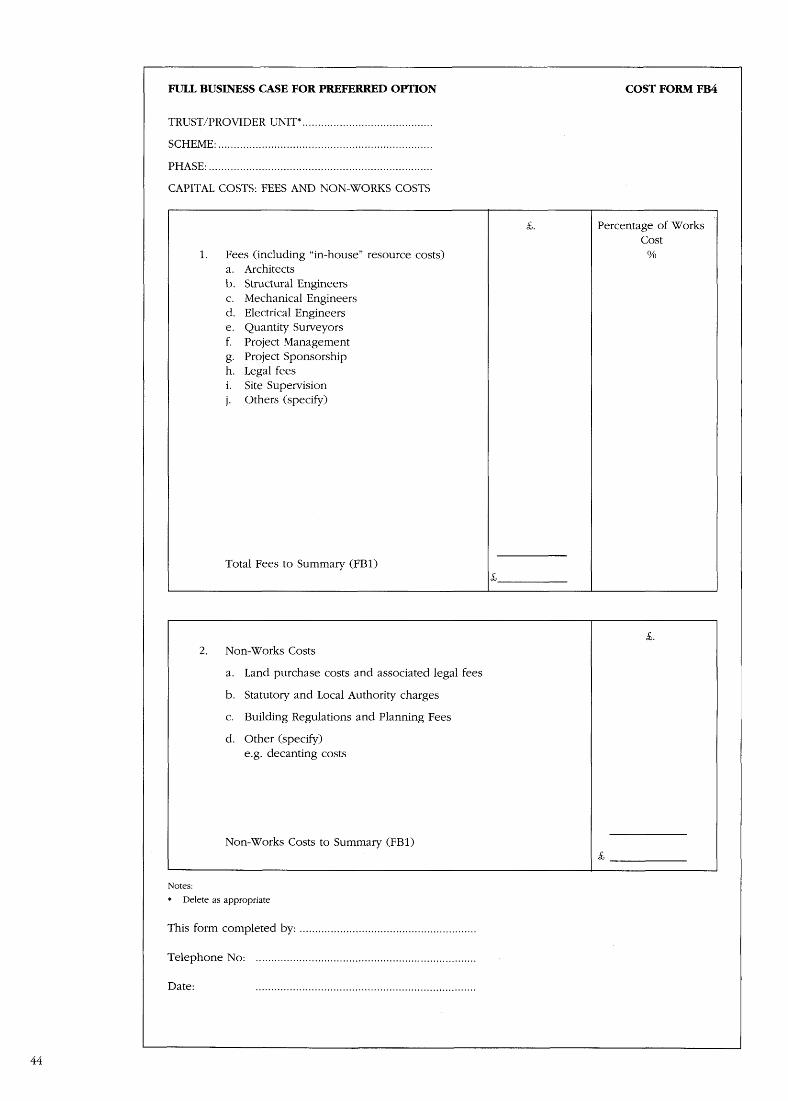
FULL BUSINESS CASE FOR PREFERRED OPTION
COST FORM FB4
TRUST/PROVIDER UNIT* . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
SCHEME : . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
PHASE : . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
CAPITAL COSTS : FEES AND NON-WORKS COSTS
£ .
Percentage of WorksCost
1 .
Fees (including "in-house" resource costs)a . Architectsb . Structural Engineersc . Mechanical Engineersd . Electrical Engineerse . Quantity Surveyorsf.
Project Managementg . Project Sponsorshiph . Legal feesi .
Site Supervisionj .
Others (specify)
Total Fees to Summary (FB1)
à, .2 .
Non-Works Costs
a .
Land purchase costs and associated legal fees
b . Statutory and Local Authority charges
c . Building Regulations and Planning Fees
d . Other (specify)e .g . decanting costs
Non-Works Costs to Summary (FB1)
Notes:*
Delete as appropriate
This form completed by : . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Telephone No : . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Date :
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Appendix 2 : Estimating,Budgets and RiskAssessmentIntroductionA.2.1.1 The following guidance on costingbuilding schemes should be read in conjunctionwith the general principles on identifying andquantifying costs set out in the Business CaseGuide . It aims to expand on the Business Caseguidance, with particular consideration of buildingprojects and how the cost estimates are developedas they progress .
Estimate ClassificationA.2.2 .1 Estimates are usually classified to give anindication of their reliability and accuracy. Thisdepends on the extent of information available,assumptions made about unknowns and the skilland experience of the estimator . Estimates may beclassified on the basis of the probability of a costbeing achieved within a defined band. Thus a90/10 estimate is said to be one which has a 90per cent probability of being achieved within 10per cent .
A.2.2.2 As a project progresses through itsdevelopment and design stages, the assumptionson which its cost estimate is based become morereliable and the degree of uncertainty is reduced .This means that the estimate should becomeprogressively more accurate . However, theprocurement route chosen determines the level ofinformation available at each stage and hence thelikely accuracy of the estimate at a given stage . Arisk analysis will assist in making judgements as tothe accuracy of a given estimate .
A.2.2.3. The table below gives a general guide tothe accuracy that ought to be achieved at eachstage of a typical health care construction project .
Stage
Traditional Design and ManagementBuild
Concept 80/40 80/40 80/40OutlineBusiness 85/15 85/15 80/20CaseFullBusiness 90/10 90/10 85/15CaseDesign 95/5 95/5 90/10*Complete*Assumes major works packages (foundations, external envelope,M&E services design)
A.2.2.4 The table is illustrative only; it shows thatdesign is a significant uncertainty, and as design iscompleted so costs become more certain . In thetraditional procurement approach, design is usuallyfurther advanced at Full Business Case than otherstrategies and, as a result, a greater degree ofcertainty is achieved at that time . Managementforms of contract, which are usually only used forvery large schemes, have greater uncertainty laterin the project as design overlaps construction .Similarly, for Design and Build strategies a highdegree of cost certainty occurs only after contractaward, but at that stage cost is more certain thanother contract forms as the contract is usually alump sum, with the contractor bearing the brunt ofthe risk .
A.2.2.5 There is a greater risk of unknowns inrefurbishment work and where foundations andground conditions are involved . Full andcomprehensive surveys can assist in minimisingsuch risks .
EstimatingA.2.3 .1 All estimates are based on bringingtogether the component parts of the project, withthe cost of each component being establishedfrom past experience . The way the estimate isbroken down into components depends on theobjective of the estimate and its target reliabilityand accuracy . Typically, estimates at an early stageare based on reference costs or cost allowances(see DCAs below) ; then as design is developed,the estimate is related to specific design solutionsbroken down into an elemental cost plan . Finally,estimates during construction are based oncontracts awarded and the drawings forunprocured work . As the project progresses, theproject director will need to compare latestestimates with previous ones and with thecommitment and expenditure already made .
Estimate ComponentsA.2.4.1 The components that make up theestimates normally include:
- departmental costs : based on departmentalcost allowances published by NHS Estatesfor functional units with their recommendedspace and cost allowances . Details to becompiled on form FB2 ;
- on-costs : provides allowances forcommunications and facilities betweendepartments, external building works,external engineering works, auxiliary

buildings and other building or engineeringcosts . Details to be compiled on form FB3 .
- works costs : the total of departmental andon-costs or, where departmental costs arenot used, all contracts for any physical work,including preparatory or enabling works,foundations, drainage, roads and infra-structure, etc . This may include an estimatefor technical commissioning ;
- location : local adjustments may be made tothe national departmental cost allowances ifappropriate ;
- fees : for professional and specialisedservices . Details to be compiled on formFB4 . Sometimes referred to as resource costs;
- non-works costs : for land purchase, statutoryprovision and building regulations orplanning fees . Details to be compiled onform FB4 ;
- equipment : see Appendix 5 . Details to becompiled on form FB2 ; and
- contingencies : see end of this Appendix.
Most of these costs will be subject to VAT (seeform FBI) .
A.2.4.2 These may not all be required in everycase and some projects will require othercategories .
Departmental Cost Allowances
A.2.5.1 In the NHS, past experience ofconstruction costs his been collected and analysedto form a series of reference costs calleddepartmental costs allowances (DCAs) . For eachfunctional element in a hospital scheme, a typicaldesign content has been assumed and a costallowance for that function established . Thisallowance was, in the past, a fixed costing baseagainst which all projects were judged, and servedto control both the design content of the schemeand the approved cost level . With the transfer ofresponsibility for financial management to theTrusts and the establishment of financialjustification procedures, it is no longer appropriateto apply rigid central control of functional content.This is now a matter for justification within theBusiness Case . However, estimates and the controlof cost and value for money remain a centralpriority . For this reason DCAs should at least beused as a reference cost to assist in theestablishment of a control budget .
A.2.5.2 Therefore, DCAs should be used asreference costs at an early planning stage toestablish a cost target that ensures developmentsare designed in an economical manner withoutimpairing their functional requirements . Theyprovide a cost related solely to the work carriedout within the confines of a specific department;to this cost must be added allowances for relatedworks outside the department, such as energy andservices sources, corridors, lifts, other non-usablespace requirements and external works .
A.2.5.3 A full schedule of all current DCAs isavailable from NHS Estates .
Equipment Cost Allowances (ECAGs)
A.2.6.1 ECAGs are the equipment equivalent ofDCAs, i .e . they represent the cost of fullyequipping each department with all necessary newGroup 2 and 3 equipment . As for DCAs, a fullschedule is available from NHS Estates .
A.2.6.2 ECAGs form a valuable role in _ipportingthe development of an appropriate equipmentbudget.
Statistical Indicators
A.2.7 .1 In preparing cost estimates, it is advisableto refer to suitable indices in prices and costmovements throughout the building industry andselected sectors . This is particularly importantwhen costings have to be revised more than ayear after the last calculation was carried out .
A.2.7 .2 NHS Estates produce a Quarterly Briefingdocument which provides regular updates oninformation for investment economics andconstruction project information . The briefingincludes movement in the Median Index of PublicSector Building Tender Prices (MIPS), EquipmentPrice Index and general building costs indices .
Content of the Project Base Estimate
A.2.8.1 The project base estimate is the startingpoint for building up estimates for risk and shouldbe the latest estimate of cost or time (including thecost of risk allocated to other parties), but with nocontingency for risk. The components of a projectbase cost estimate are set out in para A.2 .3 .1 .
Risk Analysis and ContingencyAllowance
A.2.9 .1 A risk analysis is a formal review of theresidual risk exposure at important stages of aproject . Its objectives are to :
- set the contingency sum- identify all potential risks .- identify important risks at each stage of a
project.- identify any unusual risks; and- determine the maximum possible action as
well as the most likely project out-turn .
A.2.9 .2 Risk identification usually cons its of :
- understanding the content of the projectbase estimate ;
- reviewing the likely sources of potential risk ;and
- identifying the potential risks .
Identifying Potential Risks
A.2.10 .1 Methods for identifying potential risksrange from using standard checklists tobrainstorming sessions . The generally establishedmethods include :
- structured meetings with key staff - might be

facilitated by an expert risk manager toencourage all participants to contribute fullyto the exercise ;
- risk audit interviews - may be an alternativeto structured meetings when there is a largenumber óf key staff. An expert managerwould interview staff for the purpose ofidentifying, collating and analysing risk data ;and
- brainstorming sessions - these are not a free-for-all but a structured device led bysomeone with a good knowledge of thistechnique .
A.2.10.2 The outcome of the identificationprocess should be a schedule of potential risksthat could adversely affect the project out-turn .
Risk Assessment
A.2.11.1 Risk assessment may be divided intoqualitative and quantitive assessments . The formerdescribe possible risks and the latter attempts tomeasure them .
A.2.11.2 Qualitative risk assessments should focuson the causes and effects of potential risks .Techniques for doing this include structuralmeetings, risk audit interviews and brainstormingsessions . A suggested pro-forma for this purpose isincluded at the end of this appendix .
A.2.11.3 Quantitive risk assessment attempts toclarify the probability of a risk happening . The riskmay be quantified in terms of:
- increased cost ;- increased time ; and- reduced quality and performance .
A.2.12.1 Among the various methods andtechniques for measuring probability are :
- sensitivity analysis - investigating the effecton the project out-turn of a change in theassumptions of one of the important risks .This technique is mentioned in the BusinessCase Guidewhere it is used for discountedcash-flow calculations . This approach isusually appropriate during the optionappraisal stage ;
- simple risk assessment - considering eachimportant risk separately and investigatingthe possible combined effect by inspection .Usually an estimate is made of the mostlikely consequence of each risk, and theseare added together to give an approximationof the level of risk in the form of themaximum likely and most likely values . Thiswill usually give a good indication of howthe important risks could affect the projectand is most often used for small or mediumsized projects ; and
- probability analysis - calculating the cost ortime consequences of each important risk fora limited number of assumptions . These aresubsequently expressed as a range of valuesof probability with their associated values ofconsequence . Usually each important riskcan only be quantified realistically by
calculating possible values of cost or time forthree reasonably foreseeable cases :
(a) the worst;
(b) the most likely ; and
(c) the best .
A.2.11_5 The risk analysis process, coveringidentification, assessment and quantification, isillustrated as a flow chart at the end of thisappendix . More detailed advice on the issuesinvolved and the way in which a risk analysis iscarried out is contained in CUP Guidance Note 41- `Managing Risk and Contingency for WorksProjects' . A risk analysis flow chart is included atthe end of this appendix .
Estimating Contingency and RiskExposure
A.2.12.1 The contingency sum should be addedto the project base estimate to identify the totalfinancial provision required . If the identified risksare not acceptable, then the contingency shouldnot be set until management action has beentaken to review the risk exposure and to identifyresponses that will reduce the exposure to anacceptable level . A revised risk analysis should becarried out to determine the most likely out-turnand contingency .
A.2.12.2 The provision for contingency mayprovide for :
- the most likely anticipated cost (sometimesreferred to as the average risk estimate) ; or
- the maximum likely risk estimate (sometimesreferred to as tolerance) .
Setting the Contingency Allowances
A.2.13.1 Contingency allowances should reflectthe client's risk exposure . The best way to ensurethat contingency allowances provide for the risksto the project is to determine the size of theallowances from the results of a risk assessment .
A.2.13.2 Three separate allowances arerecommended for :
- the client's contingency, which provides forthe risks of client changes in projectdefinition or inappropriate projectorganisation and management, and risksarising from changes in external factors, suchas availability of funds, statutoryrequirements and force majeure,
- design contingency to allow for use duringthe design process to provide for the risks ofchanges due to design development or inestimating data ; and
- construction contingency to allow for useduring the construction process to providefor the risks of changes due to siteconditions or as a result of construction andcommissioning . CUP Guidance Note 41`Management Risk and Contingency forWorks Projects' gives detailed checklistsunder these headings.

PRO FORMA FOR A QUALITATIVE RISKASSESSMENTRef:
Rev:
Date:
Potential risk :
Importance of the risk :
(a brief description of
Probability :
*high/lowthe risk)
Consequence: *high/low
Stages of the project affected by the risk :
Statement of risk :
(the elements of the project that could be affected)
(the factors that could cause it to occur)
(any relationship or dependency on other risks)
(the likelihood of it occurring)
(how it could affect the project)
*Delete where appropriate .

RISK IDENTIFICATIONUnderstand contentof the base estimate
identify contingency elements for clientdesign and construction elements
identify potential risks
r
r
Structured meetings
Risk audit
Brainstormingwith key staff
interview
session
Qualitative risk assessment
Sensitivity analysis
Simple risk assessment
Probability analysis
Estimate contingency
Most likely risk estimate
Maximum risk estimate

Appendix 3 : Cost,Risk and ContingencyManagementCost Management and Cost Reporting
A.3.1.1 The objectives of cost managementinclude :
- delivering at the lowest cost compatible withthe specified quality, and within the costforecast at the approval stage ; and
- ensuring that throughout the project, full andproper accounts are monitored of alltransactions, payments and changes .
A.3 .1 .2 The principal areas of cost managementare :
- scope - defining what is to be includedwithin the project and limiting expenditureaccordingly ;
- programme - defining the projectprogramme from inception to completion .Estimates and cash flow projections shouldbe consistent with the programme ;
- design - ensuring designs meet the scope,and what quality is appropriate andconforms to the brief.
- commitments - ensuring that orders areproperly authorised and awarded bycompetition ;
- contracts and materials - ensuring that thecontracts provide full and proper control andthat all costs are properly incurred . Ensuringthat materials are properly specified so as tomeet the scope and design, and that theycan be effectively procured ;
- contingency - ensuring all risks areappropriately allocated from contingency andare properly authorised, and monitoring useof contingency funds to forecast overalloutturn cost ;
- cash flow - planning and controlling bothcommitments and expenditure withinbudgets so that unexpected over/under runcost do not result, ensuring that alltransactions are properly recorded andauthorised and where appropriate, decisionsare justified . Regular, consistent and accuratereports are available for different levels ofmanagement . A suggested generalised costreport format is included at the end of thisappendix.
Contingency Management
A.3.2.1 The contingency should be strictlymanaged by the project director with support andadvice from the project manager and the quantity
surveyor . The project director can effectivelydischarge this responsibility if suitable projectcontrol procedures are in place and control allaspects of the project's performance . To supportthis, there must be effective project controlprocedures for :
- cost control ;- time control ;- quality control; and- change control .
Essentially, contingency management consists of aprocedure to move costs out of the allowance forcontingencies into another for the project work .
A.3 .2 .2 Risk and contingency should be reviewedon a regular basis, particularly when formalestimates are prepared, but also throughout thedesign, construction and equipping stages . As morefirm commitments are entered into and work iscarried out, so the risks in future commitments andwork are reduced . The contingency estimateshould reflect this .
Change Control
A.3.3.1 Avoidance of change after the briefing anddesign stages are complete should be a primeobjective of a project management strategy.Changes can be minimised by ensuring that theproject brief is as comprehensive as possible andthe users have signed it off. This might entail:
- early discussions with outside authorities soas to anticipate their requirements ;
- undertaking adequate site investigations, orcondition surveys if existing buildings are tobe renovated;
- ensuring that designs are fully developed andco-ordinated before construction contracts arecommitted ; and
- imposing discipline on users to finalise andsign off their requirements in strictaccordance with the project programme .
If changes are unavoidable, they should be dealtwith as follows .
A.3.3.2 Changes proposed prior to constructionmay either be unavoidable or optional . If they areunavoidable, the project director should, ifsatisfied, authorise a transfer from contingency intothe budget to cover them . If they are optional, theyshould be approved only if it can be demonstrated

that they offer good value for money, or a saving,and that there are sufficient funds available to payfor them .
A.3.3 .3 Changes proposed after the constructioncontract has been let should be avoided if at allpossible . If they are not essential, they should bedeferred until the project is complete and thenreviewed to see if they are necessary andjustifiable economically .
A.3.3.4 When changes do occur, the projectdirector will be responsible for controlling them ;he/she should ensure that the project managerdesigns and implements effective controlprocedures, which include the implementation ofany change (except in emergency situations)before the following factors have been identified :
- the reasons for any changes ;- the full cost and time consequences of the
changes ;- proposals for avoiding and investigating time
overruns ; and- source of funding any cost overrun, e.g .
contingency, savings elsewhere .
A.3.3.5 For reporting purposes, project changesshould be categorised in accordance with theheadings and definitions contained in CUP GuideNo.38 `Approval of Works Projects' .
Cost Profiling
A.3.4.1 An initial cost profiling for the project willhave been quantified for the Business Case . Thiswill have produced a discounted cash flowcalculation, which will include the capital cost forthe life of the project . When financial approval hasbeen given to the Trust for its scheme, an externalfinancing limit (EFL) will be set at a level whichallows for the anticipated scheme costs . If theactual profile of expenditure on the project isgreater than allowed for, the Trust will have tofind the extra resources from within its EFL . If itexceeds its EFL, it will incur a penalty - areduction in its EFL during the next financial year .It is important that project expenditure is properlyand timeously monitored and kept within itsforecast profile .
Elemental Cost Planning
A.3.5.1 The essential feature of `costmanagement', as opposed to `cost recording', isthe reactive nature of design and commitment tothe cost status of the project . Elemental costplanning is a tool that aids this interaction andassists in the control and management of costs .
A.3.5.2 In an elemental cost plan the estimate isbroken down into a series of elements which canthen be compared with later estimates, or withactual costs as the project progresses . For buildingprojects, the most widely used breakdown ofelements is that produced by the BCIS (BuildingCost Information Service), details of which may beobtained from NHS Executive, or from project
quantity surveyors . Typically, each element will betreated as a cost centre, but money may betransferred between elements, provided areasonable balance between elements ismaintained and the overall target budget is notexceeded . The initial cost plan is likely to be basedon approximate figures, which providenevertheless a fair basis for determining the validityof future estimates .
A.3.5.3 Control is achieved by an on-going reviewof estimates for each cost centre against its targetbudget . As design develops and is costed, anyvariance in cost from the cost plan is identified .Decisions are then taken on whether that elementcan be permitted to increase in cost, which wouldnecessitate a corresponding reduction elsewhere,or whether the element must be redesigned inorder to keep within the budget. This provides aflexible degree of cost management control whilstretaining freedom within a control budget for thedesign specialists .
Continuous and Stage Estimates
A.3.6 .1 The quantity surveyor should be asked tocarry out a running review of designs as theydevelop, and to provide advice on costs to boththe design team and the project manager. Usually,authority for a degree of design development willbe delegated to the project manager by the projectdirector; this should be assessed in relation to eachproject and possibly, on complex projects, to eachcost centre . This continuous costing will be ofgreat benefit in assessing individual decisions andis particularly important on large and complexschemes . It does not, however, obviate the needfor a periodic formal assessment of the wholescheme .
Cost Control During DesignDevelopment
A.3.7.1 The project director has overallresponsibility for a project, including the estimatedcost, and will need to be satisfied that appropriatesystems to control cost are in place and operating .Clearly, the non-professional project directorcannot take detailed design decisions, but he/shecan and should require that all such designs whichhave a significant cost attached are properlyreviewed against the budget provision and thatthey are properly authorised . Usually, the projectdirector will delegate a level of financial authorityfor design development decisions to the projectmanager and/or the design team . This level shouldbe assessed in relation to each project and possiblyon complex projects to each cost centre . Theproject director should see that these levels are notexceeded and, with the project manager, set upsystems to review actual costs in relation to theestimate against which a decision was made .
Value Engineering
A.3.8.1 This technique is concerned with howvalue is achieved, rather than what the relativevalues are as defined in a project brief or objective .

A.3.8.2 Value engineering studies are plannedformal reviews of the design philosophy andsolutions at one or more stages of designdevelopment . They are often carried out byindependent agents, who review detailed designsolutions against project objectives and establishwhether they can be achieved in a more cost-effective manner.
A.3.8.3 The benefits of this approach include :
- clarification of the project brief;- design rationalisation; and- minimisation of costs .
Cost Management during ConstructionA.3.9 .1 During construction, instructions issued tothe contractor, whether for change or forclarification of detail, have a much moreimmediate cost . Under the terms of a buildingcontract, such instructions are issued by thecontract administrator, who has the responsibilityfor administering the contract on behalf of theclient . (This may be the project manager or thedesign team leader .) The project director needs toestablish procedures regarding instructions andinformation (similar to those established forcontrol of design development) which ensure that :
Instructions are issued within the authoritydelegated by the project director.
Instructions are costed prior to issue - orwhere this is impracticable - as soonafterwards as possible .
The cost of all instructions is monitored on acontinuous basis and no backlog of work isundertaken without formal instruction .
Specific approval is sought and given wherecosts of an instruction are forecast to beoutside the level of authority delegated to thecontract administrator .
Appropriate authority is sought immediately ifcosts of an instruction issued under delegatedauthority are estimated to rise above thedelegated limit . Effective cost management isdependent on the management systems andprocedures established by the sponsor andmanager.
Final AccountsA.3.10.1 For building contracts :
The quantity surveyor is responsible foragreeing the final account with the contractor.
An agreement should be made as soon aspossible after practical completion; is madeeasier, and faster, if it is done as the work iscarried out during the contract, so that only afew outstanding issues remain at practicalcompletion .
The project director, through the projectmanager, should make sure that the quantitysurveyor agrees quantity and value variationsas the work progresses and does not leavethese until the end .
The monthly Financial Status Report shouldindicate the status of the final accounts .
For Group 2 and 3 equipment contracts :
Responsibility rests on the person nominatedas the `engineer' or the project buyer ratherthan the quantity surveyor .
As for building contracts, outstanding issuesshould be agreed as they occur, instead ofleaving them to the end .
ClaimsA.3.11.1 Claims can vary from a routine requestfor additional time to complete a task to a seriousallegation of breach of contract . Where a claim isnot met in full, or is outside routine procedures, itrepresents a potential preliminary action to adispute over money .
A.3.11.2 The project team should adoptprocedures that will minimise exposure to the riskof claims .
A.3.11.3 The procedures should provide formalreports on a claim, which :
- give details of the claim and why the partiesare in dispute ;
- include an assessment of the extent of theliability ;
- include negotiating proposals ; and- give an assessment of the likely outcome in
financial terms .
A.3.11.4 Detailed advice on handling claims is setout in CONCODE; this should be referred to in theevent of a dispute . In particular it should be notedthat exgratia payments should be made only inexceptional circumstances, in accordance withguidance on financial procedures issued by theNHS Executive .
A.3.11.5 Wherever possible, claims, and matterswhich could give rise to claims, should have beendealt with during the course of the work, but theremay be outstanding contractual claims when theCertificate of Practical Completion is issued . Theseshould be dealt with as follows :
The certificate may not be withheld on accountof such claims .
The contract administrator must settle theseclaims as soon as possible, and before the finalaccount can be agreed.
40 The project director should seek advice fromthe NHS Executive if there are significant

outstanding claims, or if there is a disputeleading to arbitration or litigation . Disputes cancarry on for some time after contracts areotherwise completed .

TYPICAL FORMAT OF COST REPORTProject
Cost Report No .
Date:
Code/
Approved
Expenditure to Date
%
Estimated
VariationDescription
Budget
Complete
Final
+ or (-)Estimated
Actual
Total
Cost

Appendix 4 : The Brief
IntroductionA.4.1 .1 The brief is the document which definesthe owner's requirements, and which forms thebasis of the cost estimates and of all subsequentdesign and construction . Getting it right istherefore of crucial importance ; if it is wrong, theTrust may fail to provide the medical team withwhat they need or the facility may not functionefficiently. The initial brief is prepared for the FullBusiness Case, and is reviewed, further developed,frozen, and implemented during the design stage .
A.4 .1 .2 Getting it right first time is very important .Changes when design is under way, or evenworse during construction, are one of the largestcauses of time and cost overruns, both on healthcare projects and more generally on other publicand private sector projects .
A.4 .1 .3 The preparation of the brief is the timewhen the User Panel representing the end usershave both the opportunity and the obligation tospecify their requirements for the completedfacility .
Content of the Initial BriefA.4.2.1 For detailed information on what shouldbe included in the initial brief, project directorsshould refer to Health Building Note 2 - Briefingand Operational Policies . The content of the briefwill vary depending on the nature of the project,and will need the input of professional hospitalplanners and designers . In its final approved form,however, it should include :
- Trust and whole-hospital policies oncatering, storage, parking, etc ., together withwhole hospital engineering policies;
- departmental policies on matters such asworkload, hours of operation, revenueassumptions and workflow patterns ;
- the financial constraints imposed by theapproved budget, including operating costs ;
- technical constraints imposed by such thingsas the Planning Authority and site conditions ;and
- schedules of accommodation
Full BriefA.4.3.1 The full brief is completed in the designstage by the preparation of room data sheets,setting out in detail the equipment, services,environment, etc ., required in each room in theschedule of accommodation . It should also set outthe performance requirements for the building
services and the equipment to be installed as partof the building contract .
Brief DevelopmentA.4.4 .1 The development of the brief is aniterative process . It starts with the broadest conceptof the Trust's objectives and the scope of thefacility required to meet those objectives, andprogresses, with increasing levels of detail, until allthe essential parameters have been specified . Ateach stage, the requirements are developed byconsultation with the members of the user panelwho are encouraged to describe their ownrequirements so that they can be put down in theform of a simple specification and sketches . Aseach stage is developed, it is reviewed by the userpanel, which is asked to confirm that it accuratelyreflects their needs and to sign it off. That stage isthen frozen, and can be developed in more detailto the next stage . It can be seen that there is anoverlap with design . As the brief develops, itbegins to become a preliminary sketch plan designand at the end it will be a final sketch plan design.It is preferable for final sketch plans to form partof a Full Business Case .
A.4.4.2 As the brief is developed, the projectdirector should be fully aware of the developingcost estimate and the trade-offs which will have tobe made between quality, capital cost, and futurerunning costs, all of which may affect the viabilityof the project . At the same time, the brief ischecked against the agreed policies and principles .If at any time the cost should exceed the approvedbudget the brief must be reviewed to identifysavings and to modify it accordingly . OtherwiseNHSE re-approval will have to be sought . Thisprocess is set out in the flow diagram at the end ofthis Appendix .
A.4.4.3 The final brief, once it has beencompleted and signed off as acceptable, is adocument which can be used by the design team -whether in a traditional contract strategy or a fast-track one - as the basis for the project's detaileddesign and the specification to be used for supplyand construction .
A.4.4.4 This process should be treated as a projectof its own, either managed by the project director,or, if he/she does not have enough experience, byconsultants appointed to develop the brief. Thebrief is finally reviewed by the consultants, whowill be responsible for project implementation andany final development to help it become theapproved design brief and to ensure that tenderdrawings and specifications are prepared .

A.4.4.5 It is likely that the end users will not beable to define easily their requirements or to readdrawings and specifications . Therefore, one of thejobs of the project director and the team whichdevelops the brief is to explain the drawings,layouts, and specifications to the end users interms which a lay person can understand, so as toensure that they fully appreciate what they aregoing to get before their approval is given . Theimportance and implications of each decision, andits timing, must be clear ; the cost impact of somedecisions may be high, but the cost of changingthem later is likely to be far higher .
A.4.4.6 At the conclusion of the process, whenthe brief is signed off, the end users must
understand that it is frozen. They will not haveanother opportunity to change it, but will be ableto see how their requirements are then developedinto the final design.
A.4.4.7 Some projects are developed in stages,with different contracts for each stage, or, under amanagement form of contract, with sub-contractsplaced sequentially . In the latter case, the briefsfor each stage may also be completed and signedoff sequentially . However, care must be taken toensure that completion of the later briefs does notresult in changes to those stages which havealready been frozen .
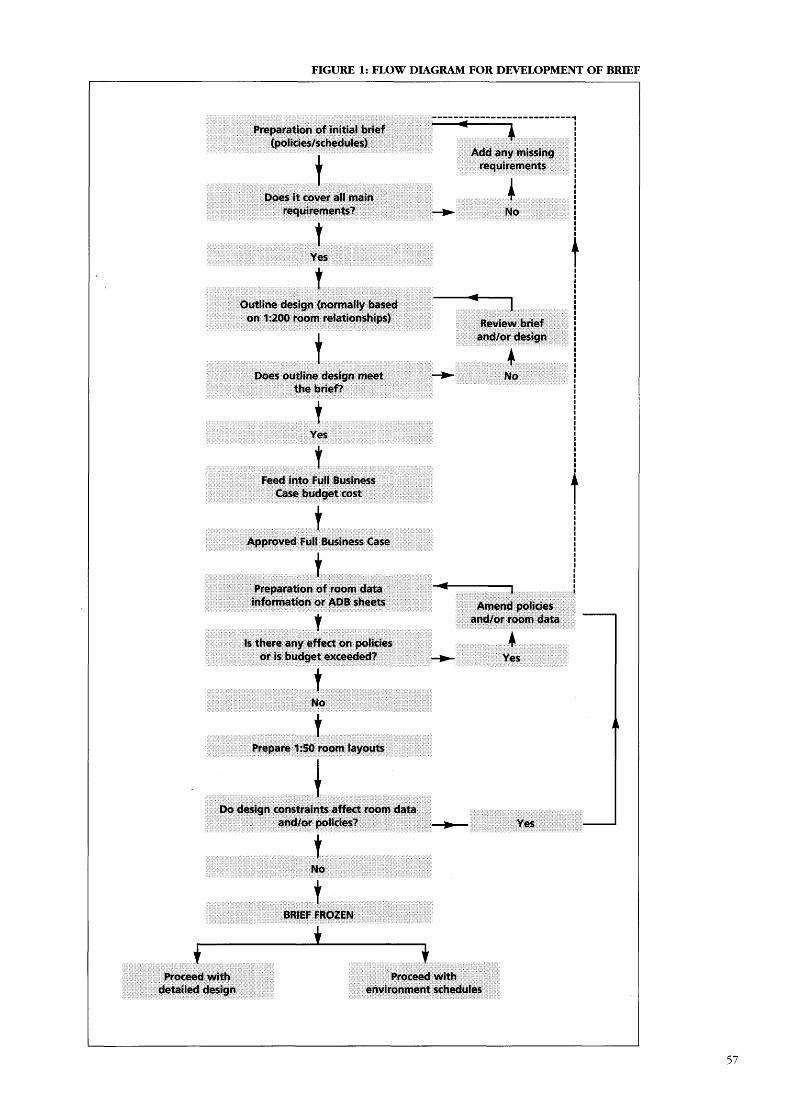
FIGURE 1: FLOW DIAGRAM FOR DEVELOPMENT OF BRIEF
--------------------------PreparationPreparation of initial brief
(policies/schedules)Add any missing
;requirements
Does it cover all mainrequirements?
No
Yes
ioutline design (normally basedon 1:200 room relationships) Review brief
and/or design
;
Does outline design meet
Nothe brief?
Yes
Feed into Full BusinessCase budget cost
i
Approved Full Business Case
;
Preparation of room datainformation or ADB sheets
Amend policiesand/or room data
is there any effect on policiesor is budget exceeded?
.}
Yes
t
Prepare 1:50 room layouts
Do design constraints-affect room dataand/or policies?
10
Yes
tt
BRLEF FROZENi
iProceed with
Proceed withdetailed design
environment schedules

Appendix 5 : TheEquipping ofConstruction SchemesThe role of the projectdirectorA.5.1.1 Equipment is vital to the successfuloperation of a project and often comprises asignificant proportion of the budget . Expertequipping advice and services will be required bythe project director from preparation of the FullBusiness Case to operational commissioning . Theproject director must ensure that :
- the correct equipment budget is set for allGroup 2 and 3 equipment, taking intoaccount the potential for transfer of existingequipment ; and
- all equipment is purchased/transferred,delivered/stored and placed in position inaccordance with the equipment budget, thebuilding contractor's programme and withthe operational commissioning programme(see Commissioning a Health Care Facility) .
Equipment GroupsA.5.2.1 Equipment supplied for a new buildingscheme can be one of four categories :
Group 1A.5.2.2 Items which are supplied and fixed underthe terms of a building/engineering contract andfunded within the works cost . These are generallylarge items of plant and equipment which arepermanently wired/installed . However, thefollowing items are normally excluded from thisgroup :
- items subject to late selection due toconsiderations of technological change, egradiodiagnostic equipment ; and
- specialised equipment items best suited tocentral purchasing arrangements .
A.5.2.3 Group 1 items are specified at designstage in the room (activity data) sheets, togetherwith any associated electrical terminals, etc . andare then included within the working drawings,bills of quantities etc .
Group 2A.5.2.4 Items which have implications in respect
of space/construction/engineering services and areinstalled under the terms of a building/engineeringcontract, but are purchased by the Trust underdirect arrangements and funded out of the separateequipment budget, along with Group 3 items .
A.5.2.5 They include the two categories listedabove as being exclusions from Group 1equipment . The main contract documents mustclearly state any lualification in relation totimescales for delivery of Group 2 equipment andavailability of final installation details . The projectdirector must ensure that responsibility for Group 2equipment is defined at all stages and insurancerequirements confirmed. Further guidance is givenin CONCODE. The project director must ensure thatthese items are procured to the contractor'stimescale and, subsequently, through the projectmanager, ensure its proper installation, inspectionand testing .
Group 3A.5.2.ó Items which have implications in respectof space and/or construction/engineering servicesand are purchased and delivered/installed directlyby the Trust, e.g . furniture, small refrigerators . Theyare funded from the separate equipment budget.
Group 4A.5.2.7 Items which may have storage implicationsbut otherwise have no impact on space orengineering services and are purchased by theclient from normal revenue budgets, e.g . surgicalinstruments, desktop equipment .
Equipment StrategyA.5.3.1 At the commencement of the Full BusinessCase stage the project director must establish anequipment strategy for the scheme, which shouldidentify :
- who will prepare the equipment budget,establish equipment requirements andsubsequently purchase the equipment - thisshould normally be an experienced capitalpurchasing officer or organisation ;
- the policy for transfer of existing equipmentinto the new scheme, which will influencethe budget within the scheme for thepurchase of new equipment;

- the equipment procurement procedures tobe followed to ensure compliance withgovernment policy and with absolutepropriety ;
- the reporting procedures on progress of theequipping process through to operationalcommissioning ;
- the policy for procuring new equipment forexisting services pending transfer into anynew facilities, i .e . to ensure compatibility -this is especially important for `high tech'equipment ; and
- a risk analysis of the factors which mightlead to an increase in the equipment budget,so that an appropriate contingency sum canbe included within the total approved sumfor the scheme .
Setting the EquipmentBudgetA.5.4.1 The equipment budget must beestablished so that it can be incorporated withinthe Full Business Case submission . It will formpart of the scheme's approved budget cost, whichcannot subsequently be exceeded . Becausedetailed equipment schedules are not prepareduntil the Design Stage an experienced capitalpurchasing officer is required to advise on theappropriate Full Business Case equipment budget .This advice would be based on the EquipmentCost Allowance Guidance (ECAG), supplementedby previous experience and knowledge of thisparticular project .
A.5.4.2 ECAG allowances should be used as thebasis of the equipment budget, abated, whereappropriate, for the transfer of existing equipment .
A.5.4.3 The equipment budget should alsoinclude allowances for the costs of:
- equipping staff;- storage of new equipment ; and- transfer (e .g . dismantling, transport and
installation) .
A.5.4 .4 An allowance to cover the risk ofequipment costs increasing during the project(other than by inflationary factors, which will beallowed for automatically) should be included, ifnecessary, within the Full Business Casecontingency sum, based on a proper risk analysis .
Summary of EquippingProcessesA.5.5 .1 At Full Business Case Stage :
- prepare equipment strategy ;- establish the equipment budget ; and- undertake risk analysis and, if necessary,
identify an appropriate contingency sum .
A.5.5 .2 At design stage :
- prepare equipment schedules for Group 2and 3 equipment based on the agreed roomdata sheets/layouts ;
- identify items available for transfer ; and- check costs against budget set at Full
Business Case stage .
A.5.5 .3 At construction and equipment supplystage :
- ensure purchase and delivery of Group 2items in accordance with the buildingcontractor's requirements and timescale,together with proper inspection and testing .
A.5.5.4 At Commissioning Stage :
See Commissioning a Health Care Facility.
Appendix 6 : ProjectExecution Plan (PEP)Introduction
A.6.1 .1 A mandatory requirement is thepreparation of a Project Execution Plan (PEP) forall projects requiring NHS Executive approval .Trusts are recommended to prepare one for lower-value projects as well .
A.6.1 .2 The PEP is the core document for themanagement of a project . It is a statement ofpolicies and procedures defined by the projectdirector, although usually developed by the projectmanager for the project director's approval . It setsout in a structured format the project scope,objectives, and relative priorities . The PEP :
- includes plans, procedures and -controlprocesses for project implementation and formonitoring and reporting progress .
- defines the roles and responsibilities of allproject participants, and is a means ofensuring that everyone understands, acceptsand carries out their responsibilities ; and
- sets out the mechanisms for audit, reviewand feedback, by defining the reporting andmeeting requirements, and, whereappropriate, the criteria for independentexternal review .
A.6.1.3 The PEP will change as a projectprogresses through its design and constructionstages . It should be a dynamic document regularlyupdated and referred to as a communication tool,as well as a control reference .
PEP : Format and Content
A.6.2 .1 Much of a PEP will be standardised, butthe standard will need to be modified to meet theparticular circumstances of each project . A typicalPEP might cover the items listed below, althoughsome matters may appear under a number ofheadings with a cross reference system employedto avoid duplication :
- project definition and brief;- roles, responsibilities and authorities ;- project cost plan and cost management
procedures ;- risk and sensitivity analysis- programme management ;- contracting and procurement- administrative systems and procedures- safety and environmental issues, such as the
construction design and managementregulations ;
- quality assurance ;
- commissioning ; and- post project evaluation .
A.6.2 .2 The following sections describe thecontents of some of these subjects in more detail .
Project Definition and Brief
A.ó.3 .1 The full project definition should bedefined in the brief . The PEP should refer to thebrief, not duplicate it, but should cover :
- the project particulars, ie the Trust name,the project name and reference, and detailsof the Full Business Case approval ;
- the health care objectives ;- operational constraints ;- the construction objectives, ie the overall
budget and programme limits ;- priorities in terms of quality, time, and cost;- location, general arrangement, physicalenvironment, and design constraints ;
- design philosophy; and- contract procurement strategy .
A.6.3.2 The brief will have been prepared for theFull Business Case, but may not be complete andwill not have been finally frozen and signed off .The PEP will cover arrangements for final reviewand approval by the user panel and the proceduresfor keeping the user panel informed of theimplementation of the brief during design andconstruction . It will re-state any priorityrequirements contained in the brief. The controlprocedure for any changes to the brief after it hasbeen signed off should be set out clearly .
Roles, Responsibilities and Authority
A.6.4.1 The PEP should outline the projectorganisation in a formal way, describing :
- the names, addresses, and telephone and faxnumbers of all organisations involved in theproject;
- their roles and relationships with each other;and
- their responsibilities and the authoritydelegated to them as well as the names andresponsibilties of key personnel within eachorganisation .
This should provide a comprehensive directory ofthe project which defines relationships and lines ofcommunication .
A.6.4.2 The ultimate authority for all externalmembers of the project team is the project director,

who is in charge of establishing the responsibilitiesof Project Manager and others in the project team.The PEP should specify financial delegation limitsand those types of decision that the projectdirector wishes to remain responsible for . Aninternal section of the PEP will, similarly, definethe authority of the project director and howhe/she relates to the user panel and the ChiefExecutive Officer and, where established, theProject Board .
A.6.4.3 At stage 1, the roles and responsibilitiesfor planning, design, procurement, construction,equipment, and commissioning should be definedfor :
- the project director ;- the project manager;- the lead designer and the other members ofthe design team ; and
- the quantity surveyor.
A.6.4.4 As the project progresses the roles andresponsibilities of contractor(s), sub-contractors,the Contract Administrator, the Clerk of Works,commissioning staff, etc . should be added to thePEP .
Project Cost Plan and CostManagement ProceduresA.6.5 .1 The PEP should define cost-managementrecording and reporting procedures . Typically,both the budget and recorded costs andcommitments will be subdivided into a series of`cost centres' for administrative, estimating, andcontractual convenience - see Appendix 7, whichshows this and defines the terms used . The PEPwill establish the cost centres and will define thebuild-up of the current control budget; this is theproject cost base line, and performance will bemeasured against achievement of this budget . It isknown as the cost plan .
A.6.5.2 Responsibility for cost management issueson a project will usually be delegated to theproject manager and the quantity surveyor. Theywill propose appropriate control and reportingpractices and procedures which should meet therequirements set out in Appendix 7 ; they mustsatisfy the project director that these are adequateand appropriate for the project .
A.6.5.3 Typical cost management proceduresinclude :
- the cost plan ;- change control ;- risk management ;- cost reporting ;- contingency management ; and- expenditure profile and annuality control .
More detailed advice on these procedures is setout in Appendix 3 .
A.6.5.4 The current control budget build-up willusually be relayed to all members of the designteam, except for contingency, which should bestrictly managed by the project director with thesupport and advice of the project manager and thequantity surveyor.
A.6.5.5 The PEP should also set out theanticipated expenditure profile .
Programme ManagementA.6.6.1 The start and completion dates in theproject programme will have been defined in theFull Business Case . During stage 1 the projectmanager must develop this into a more detailedprogramme, which shows :
- the dates by which milestone events must becompleted ;
- and the interdependancies of events innetwork format, the critical path, and theavailable float .
This task requires considerable experience andeffort . The programme developed must be bothcomprehensive and realistic, as it will form thebasis of all future progress monitoring .
A.6.6.2 Network programmes are difficult tounderstand, so they are converted into bar chartsfor ease of reference . There is a hierarchy ofprogrammes, each in more detail than the oneabove it . The top level programme is the list ofmilestone events which is used for progressreporting .
A.6.6.3 The PEP will not contain the detailednetwork, but should refer to it and include :
- milestone events and a definition of theirmeanings ;
- the amount of detail required;- the frequency of review ; and- how progress is monitored against theprogramme .
Administrative Systems andProceduresA.6.7.1 The PEP will establish the variousadministrative procedures necessary for theeffective and controlled implementation of theproject . Typical procedures will include, amongstothers, those recommended by the projectmanager . These may include :
- document numbering and filing systems ;- drawing numbering systems ;- computer software standards, includingComputer Aided Design (CAD) ;
- project reporting ; and- meetings, including objectives, frequency,
attendance, secretarial, etc .

A.6.7.2 The project manager should specifyadministrative procedures for the project director'sapproval . The systems which the project manageralready has available should be used wheneverthey meet the project director's requirements ; thiswill be more efficient and cost effective thandesigning new systems.
Technical StandardsA.6.8 .1 There may be some specific technicalstandards, not covered by the brief butwhich should be included in the PEP. Examplesare:
- the format of as-built or other permanentrecord drawings,
- plant and equipment numbering systemscompatible with the Trusts's asset register ;and
- requirements relating to the operating andmaintenance instructions for plant andequipment.
A.6.8.2 These are generally related to the futureoperation and maintenance of the facility . Theproject director must identify such requirements byconsultation with the user panel and ensure thatthey are included in the PEP.
Appendix 7 : Monitoringand Monthly ProgressReportsIntroduction and Objectives
A.7.1 .1 It is a mandatory requirement that regularprogress reports be prepared for all projects . Thisappendix describes the objectives, scope, and formof those reports . It also describes how the reportsaffect the management and direction of a project.
A.7.1 . 2 Monitoring of cost and progress isessential for the good management of any project .In the NHS this covers both :
- monitoring by the project director andproject manager to enable them to managecost, time, and quality, and
- monitoring by the NHS Executive to satisfyits accountability to the Department of Healthand ministerial accountability to Parliament .
This appendix covers both requirements .
A.7.1.3 Key decisions need to be based on goodinformation ; that is information which is consistent,accurate, up to date and relevant, and in a formthat can be readily understood and its significanceappreciated. Graphical presentations, for example,may help trends to be better appreciated andunderstood . Progress must be measured against aplan which may change and develop as the projectprogresses, without ever losing sight of the baseline . One principle of a good report is that theposition at the date of a report is compared towhat it should actually be, and the reasons for anydeviation are explained .
A.7.1.4 Progress reports must cover all aspects ofa project, including management processes ; design ;procurement; construction ; cost ; and cash flow.
A.7.1 .5 Progress reports perform five importantfunctions . They are to :
- keep the project director informed of theproject status . They identify problems andoptions for their resolution, and provide theinformation to enable the project director totake key decisions promptly based on themost appropriate information ;
- demonstrate that the project manager andproject team are carrying out theirresponsibilities satisfactorily, and that thenecessary management processes,procedures, and controls are in place and areoperating effectively ;
- provide a discipline for the whole project
team, and establish a time reference forprogress meetings and plans ;
- provide a communication tool in a simple,comprehensive, and consistent format whichcan be distributed to the project team ; and
- permit external monitoring and the gatheringof statistics by the NHS Executive .
A.7.1.6 Reports must be accurate, consistent andon time . They must always be available at a settime and refer to data up to an established date -for example, the end of the previous month . Thecontents of reports, and the dates to which theyrefer should be clearly stated and all information,particularly that relating to cost, must be consistentand as up to date as can practicably be achieved .
Progress Reports
A.7.2 .1 The monthly project progress report (PPR)issued by the project manager to the projectdirector is one of a hierarchy of progress reports,each in more detail than the preceding one, andsummarising the details of the lower-level reports .The Level 1 report is prepared by the projectdirector for the investment decision maker (IDM)and the board, and used for external monitoringby the NHS Executive ; this gives overall progressand cost information in summary form only .Similarly, the various consultants and contractorswill report to the project manager monthly andtheir reports will form the basis of the PPR .
A.7 .2 .2 The table below shows the typicalstructure of such an arrangement and the level ofinformation required at each level .
Level Recipients ScopeLevel 1
Top Management
Overall status trendTrust board external indicators.reports to NHSExecutive
Level 2
Project director
Design,project manager
Constructions,Progress andcost reports, problemsand actions required.
Level 3
Project manager
Information requestsProject team
and responses,contractor progressand resources, designcost/forecasts.
A.7.2.3 The following guidance mainly coversLevel 1 and 2 reports .
A.7.2.4 Each report should summarise the lower-level report and add comment and explanation

where appropriate . It should include anyinformation relevant to the recipient ; if everythingin a particular report is considered relevant, thefull report should be appended as part of the nextlevel . For example, the project director shouldissue the executive summary of the PPR to thechief executive officer, with brief supporting notesas appropriate .
Reports to the TrustA.7.3 .1 It is mandatory for Trusts to establish aregular monthly PPR . The details of therequirement will be set out in the ProjectExecution Plan, but the Project Director mustensure that the requirement is included in theduties of the project manager, the quantitysurveyor, and all other consultants when they areappointed . Reports should be submitted monthlyover the duration of whole project, starting onemonth after the appointment of the projectmanager .
A.7.3 .2 The information required for the PPRshould be only that which the members of theproject team need in order to carry out theirrespective responsibilities . The information mustbe kept in a form which allows the project team togenerate the external report forms .
A.7.3.3 The PPR is a progress report on thedesign and construction of the project . The projectdirector should bear in mind the broader needs ofthe project in the provision of health care, andmay include in the Level 1 reports to the IDM andTrust board a section on the planning for suchoperational matters as :
- staffing and staff training ;- operational management of the facility; and- maintenance of equipment and building
services .
If these issues are not the project director'sresponsibility, the chief executive officer shouldrequire those responsible to prepare reports at thesame frequency and timing as the PPR, so thatthey may be considered together.
Content of Level 2 Reports to theProject DirectorA.7.4 .1 Most project management organisationshave their own standard reporting formats . If these,provide the information required in sufficientdetail, and are well presented, they should form asatisfactory basis for the PPR and need not beamended .
A.7.4.2 The typical contents of a PPR are :
- executive summary ;- project manager's report ;- highlights and changes since previous report;- actions required and plans being developed,- key decisions/information required ;- progress;- design status (if appropriate);
- progress against plan with commentary ;- milestones achieved/anticipated;- key plans for next month ;- changes to plan anticipated orrecommended ;
- procurement ;- tender status ;- contract or order placement ;- equipment inspection and delivery ;- financial status report ;- quality status ; and- staffing report .
These headings and descriptions are notmandatory, and may, require modification to suitthe needs of a particular project and its contractprocurement strategy. The emphasis will changefrom design to construction as the projectprogresses .
Financial Status ReportA.7.5 .1 The Financial Status Report (FSR) forms apart of the PPR . It is usually prepared by thequantity surveyor for the project manager . Itprovides information on:
- the overall cost status ;- current commitments ;- orders placed ;- variation orders ;- estimated cost to complete ;- variations and instructions anticipated;- future provisional sum expenditures;- contract claims ;- contingency status ;- forecast payment profile ;- the status of payments and certificates ; and- final account progress .
The FSR is the formal record of the cost status of aproject. Supporting records must be maintained,which provide a full audit trail of all financialtransactions .
A.7.5.2 A typical FSR is given at the end of thisappendix . A description of the terms used is givenin para A.7 .5 .4 below . It shows the report in twosections, one below the other, for ease ofpresentation on a single page ; in practice, it maybe in one section on larger size paper.
A.7.5.3 The FSR is a statement of the financialsituation of a project at a given point of time ; it isa tool to assist in cost management, but does notof itself provide cost management . Costmanagement, which is the process of managingoften competing demands of scope, quality,programme, and cost to achieve value for moneywithin the approved budget depends onprocedures established by the project director andproject manager and set out in the ProjectExecution Plan (see Appendix 6) .
A.7.5.4 The terms used in the FSR, by referenceto the column numbers, are given below :
A . Approved budget . The capital cost approved inthe Full Business Case.

B . Transfers and adjustments . Transfers out ofcontingency into a cost centre . The total oftransfers out of contingency is equal to the totalof transfers into a cost centre, so that the nettransfer is always zero .
C . Approved budget changes . Changes to theapproved budget which have been approved bythe NHS Executive subsequent to the FullBusiness Case .
D . Current control budget . The budget used forcomparison with the latest estimated cost (LEC),being the sum of columns A, B, and C .
E . LEC . The latest estimate of the total out-turncost, made up of commitments to date plus anestimate of uncommitted amounts required tocomplete (columns K+P) .
F . Net orders placed . The contract value of ordersplaced, before variations or claims, andexcluding discounts, uncommitted provisionaland prime cost sums, and VAT.
G . Variations - estimated . The cost of orderedvariations, for which the value has not yet beenagreed .
H . Variations - approved . The cost of orderedvariations, the value of which have been agreed .
1 . Provisional sums and dayworks - estimated . Thecost of ordered provisional sums and dayworks,the value of which have not yet been agreed .
J . Provisional sums and dayworks - approved . Thecost of ordered provisional sums and dayworks,the value of which have been agreed .
K . Total commitments . The total amount committedin respect of the project, being the sum ofcolumns F, G, H, 1, and J .
L . Future contracts . The estimated value ofcontracts which have not yet been committed .
M. Future variations . The estimated value ofcontract variations which have not yet beenordered .
N. Future provisional sums and dayworks . Theestimated cost of provisional sums anddayworks which have not yet been ordered oncommitted contracts .
O . Contract Claims . The estimated value of contractclaims received or anticipated .
P . Total uncommitted. The estimated value of thatpart of the total project cost which has not yetbeen committed, being the sum of columns L,M, N, and O.
Q . Paid to date . The total amount paid by the Trustin respect of the project .
R . Paid as a percentage of LEC . The proportion ofestimated out-turn cost paid to date .
S . Certified to date . The total amount in respect ofthe project cost which has been certified forpayment . This includes retention monies .
T. Certified as a percentage of LEC . The proportionof the estimated out-turn cost which has beencertified for payment .
A.7.5.5 The most important comparison isbetween the current control budget (column D)and the LEC (column E) . The total of commitments(column K) compared to the amount uncommitted(column P) gives a good indication of the riskwhich remains in the estimate . Columns Q and Sindicate cash flow, and the difference is theamount due to be paid in the following month .When expressed as percentages, they are a goodmeasure of progress for comparison with thephysical progress report .
Cash FlowA.7.6 .1 Cash flow is important in its own right,because of annualisation and the need for theTrust to manage its overall cash requirements . Itcan also serve as a useful guide to projectprogress . A report on cash flow should beincluded in the PPR .
InflationA.7.7 .1 For firm price contracts, the approvedbudget will normally be given in cash terms plus aseparate allowance for inflation up to tender date .
A.7.7.2 Approval of projects which will includevariation of price (VOP) clauses will, in addition tothe allowances for inflation up to tender date, alsoinclude an allowance for contract price variations .
A.7.7.3 Adjustments for inflation between the basedate of the approved budget and the date ofaccepted tenders are made by using a tender priceindex agreed in the Full Business Case .Adjustments after their tender dates are calculatedin accordance with the VOP clauses in thecontracts .
Mandatory Reports for the NHSExecutiveA.7.8.1 Reports in a form to be announced mustbe submitted to NHS Estates when specified eventsoccur or at the times stipulated in the proceduresfor all schemes exceeding the reporting threshold .
A.7.8.2 Reporting formats reflect the nature of theinformation and the purpose for which it iscollected and are of two broad types :
- basic static information, which becomesavailable when particular events occur, andthen remains largely unchanged for theduration of the scheme ; and
- dynamic information, which changes overtime and requires updating on a regular basis(normally monthly) for progress reportingthroughout the scheme duration .

A.7.8.3 Reports of type (a) include the following :
- basic information which identifies theproject, its purpose and function and forms abaseline for performance monitoring of costand time . These are required at Full BusinessCase approval and any subsequent re-approvals, and show approved cost estimateand programme dates for agreed milestoneevents ;
- information on consultant fee bids whencommissioned and consultant performance atpre-determined intervals ;
- Information on contractor's tenders atacceptance and contractor's performance oncompletion ; and
- elemental cost analyses of successful tenders .
A.7.8.4 Reports of type (b) include the following :
- progress against scheme event milestonescompared to baseline ;
- comparison between current estimate andbaseline, together with reasons for changesclassified in accordance with the CUPguidance No-38 `Approval of Works Projects' ;
- contract information to allow prediction oftime and cost outcome at an early stage ;
- cash flow comparison for the scheme .
A.7.8.5 The project director should obtain all thedata necessary for the mandatory NHS Executivereports from the project manager, who shouldprepare the report forms for the approval of theproject director .
A.7.8.6 Trusts must also notify the NHS Executiveif, at any time during the course of design andconstruction :
- the re-approval criteria are breached ; or- any fundamental criteria established in the
Full Business Case have changedsignificantly .
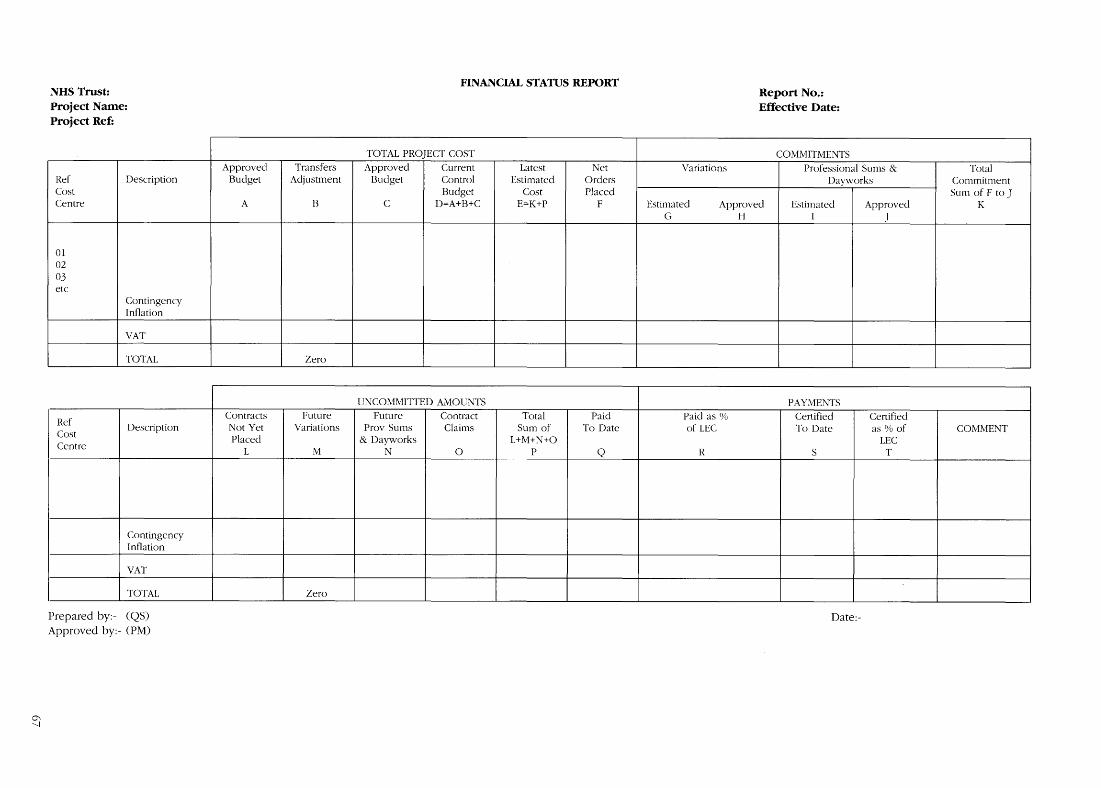
FINANCIAL STATUS REPORTNHS Trust:
Report No. .Project Name:
Effective Date :Project Ref:
TOTAL PROJECT COST
COMMITMENTSApproved
Transfers
Approved
Current
Latest
Net
Variations
Professional Sums &
TotalRef Description Budget Adjustment Budget Control Estimated Orders
Dayworks
CommitmentCost
Budget
Cost
Placed
Sum of F to JCentre
A B C D=A+B+C E=K+P F Estimated Approved Estimated Approved KG
H
I
J
010203etc
ContingencyInflation
VAT
TOTAL
Zero
UNCOMMITTED AMOUNTS
PAYMENTS
Ref
Contracts
Future
Future
Contract
Total
Paid
Paid as %
Certified
CertifiedDescription
Not Yet
Variations
Prov Sums
Claims
Sum of
To Date
of LEC
To Date
as % of
COMMENTCostCentre
Placed
& Dayworks
L+M+N+O
LECL
M
N
0
P Q
R
S
T
ContingencyInflation
VAT
TOTAL
Zero
Prepared by :- (QS)
Date:-Approved by:- (PM)
Appendix 8 : MandatoryReports to the NHSExecutiveA.8.1.1 The chief executive of the NHS Executiveis accountable to Parliament for the NHS capitalprogramme . Also Treasury require information tobe regularly returned about the progress ofschemes and contracts . To fulfil these obligations, itis necessary for units to return the information asoutlined below .
A.8.1.2 These returns were previously known asCONCISE forms . The content and layout of theforms been radically revised, so that only theminimum data is returned to the centre .
A.8.1.3 The project director is responsible for thereturn, on time, of the appropriate forms and isrequired to sign his or her authorisation . Fullguidance on the completion of the forms will beissued separately . An exemplar will also beprovided .
Schemes and Contracts Which MustBe Reported
A.8.2 .1 A separate circular gives details of thevarious reporting and approval thresholds . Thougha scheme may not require approval it may still bethe subject of regular reports to the NHS Executive .The scheme reporting threshold refers to the totalscheme sum as shown on the form FBI . Onlythose contracts which are part of a scheme overthat threshold and with a contract value in excessof the contract reports threshold are reportedseparately . The contract value includes the maincontract with any associated fees and sub-contracts .
A.8.2.2 Where a scheme which was below thereporting threshold increases in cost to above thethreshold it will not become subject to thesereporting procedures until the cost increase is 5%or more of the original Full Business Case .
Reporting Timetable
A.8.3.1 Those schemes over the approvalthreshold require Full Business Case approval .Returns are due, as identified below, from thatdate . Reports are made for other schemes abovethe scheme reporting threshold from the date onwhich the NHS Executive, chief executive orproject director, as appropriate, approves the FullBusiness Case .
A.8.3.2 It is important that forms are receivedwithin seven days of the due date .
Forms and Frequency of Return
MCP 100 - SCHEME MONTHLY AND THREE-MONTHLY REPORTA.8.4.1 This form is used for all schemes abovethe scheme reporting threshold .
A.8.4.2 This is returned at monthly intervals fromthe date of the Full Business Case until the monthafter the date of the Final Certificate of PracticalCompletion (or the equivalent completion pointfor management, and design and build contracts)is issued . After that, quarterly returns are requireduntil the project director certifies that the schemeidentified in the Full Business Case has beencompleted . This will be after the settlement of allfinal accounts .
A.8.4.3 As the scheme develops through stage 2,the Full Business Case sum will be allocated morefirmly to the various categories . Where schemesrequire Full Business Case approval, this is givenfor cost, time and functional content .
FORM MCP 200 - PRE-TENDER AND POST-TENDERING REPORTINGA.8.4.4 The information is only required for thosecontracts which at the end of stage 2 have abudget in excess of the contract reportingthreshold . This form is in two parts and is returnedtwice . The first return is made when the Certificateof Readiness to Proceed to Tender is issued . Thesecond return is when the certificate to proceed tocontract is issued .
FORM MCP 300 - CONTRACT MONTHLY ANDTHREE-MONTHLY REPORTA.8.4 .5 The information is only required for thosecontracts which at the end of stage 3 have acontract sum in excess of the contract reportingthreshold . The report is returned monthly from thedate of start on site until the month after theCertificate of Practical Completion (or itsequivalent for other forms of contract) is issued . Itis then returned quarterly until the Certificate ofFinal Account is issued .
FORM MCP 700 - ELEMENTAL COST ANALYSISA.8.4.6 An elemental cost analysis is a breakdownof the capital cost of building work only intostandard elements of the structure, such as floors,roof, walls, partitions, etc . Once the main contracthas been placed for a scheme containing asubstantial proportion of new building work, anelemental cost analysis should be prepared by the

quantity surveyor and submitted to NHS Estates,Leeds . An elemental cost analysis forms theprimary source of cost data which can be used forthe following :
- as a basis for creating an estimate and costplan for a future scheme of a similar nature .Computer programmes such as CONCISE 5facilitate the manipulation of such data andenable the rapid assembly of an estimate andcost plan that can be used to control costsduring the design stage of a scheme ; or
- as a source of data for checking the validityof departmental cost allowances againstactual schemes or as a source of data for thecreation of new or revised departmental costallowances .
A.8.4.7 An elemental cost analysis is normallyprepared from the data contained in a Bill ofQuantities . Where schemes are let without Bills ofQuantity, there is generally insufficient detailedcost data to enable an elemental cost analysis tobe prepared . With the advent of computer-basedsystems for the preparation of Bills of Quantities,the preparation of an elemental cost analysis is arelatively simple task involving little extra workduring the preparation of tender documents andthe completion of the analysis, once the tendersum has been established .
Full details of how to prepare an elemental costanalysis can be found in the CONCISE 3 users'manual Appendices 1-4 .

FIGURE 2: USING THE SCHEME AND CONTRACT MONITORING REPORTS
01311 - CAPITAL COST SUMMARYOB2 - DEPARTMENTAL COSTS
OUTLINE BUSINESS CASEAND EQUIPMENT COSTS
FB1 - CAPITAL COSTSSUMMARYFB2 - DEPARTMENTAL COSTS
FULL BUSINESS CASE
AND EQUIPMENT COSTSFB3 - ON- COSTSFB4 - FEES AND OTHER COSTS
DESIGN
MCP 200 - CONTRACTPRE-TENDER REPORT
MCP 200 - CONTRACT
TENDER AND CONTRACT
POST-TENDER REPORTMCP 700- CONTRACT COSTANALYSIS
CONSTRUCTION ANDEQUIPMENT SUPPLY
MCP 100 - SCHEME
MCP 300 - MONTHLYMONTHLY REPORT
CONTRACT REPORT
HANDNOVER ANDCOMMISSIONING
POSTCOMPLETION
MCP 300 - THREE MONTHLYCONTRACT REPORT
MCP 100 - SCHEME THREEMONTHLY REPORTS
SCHEME COMPLETIONCERTIFICATE
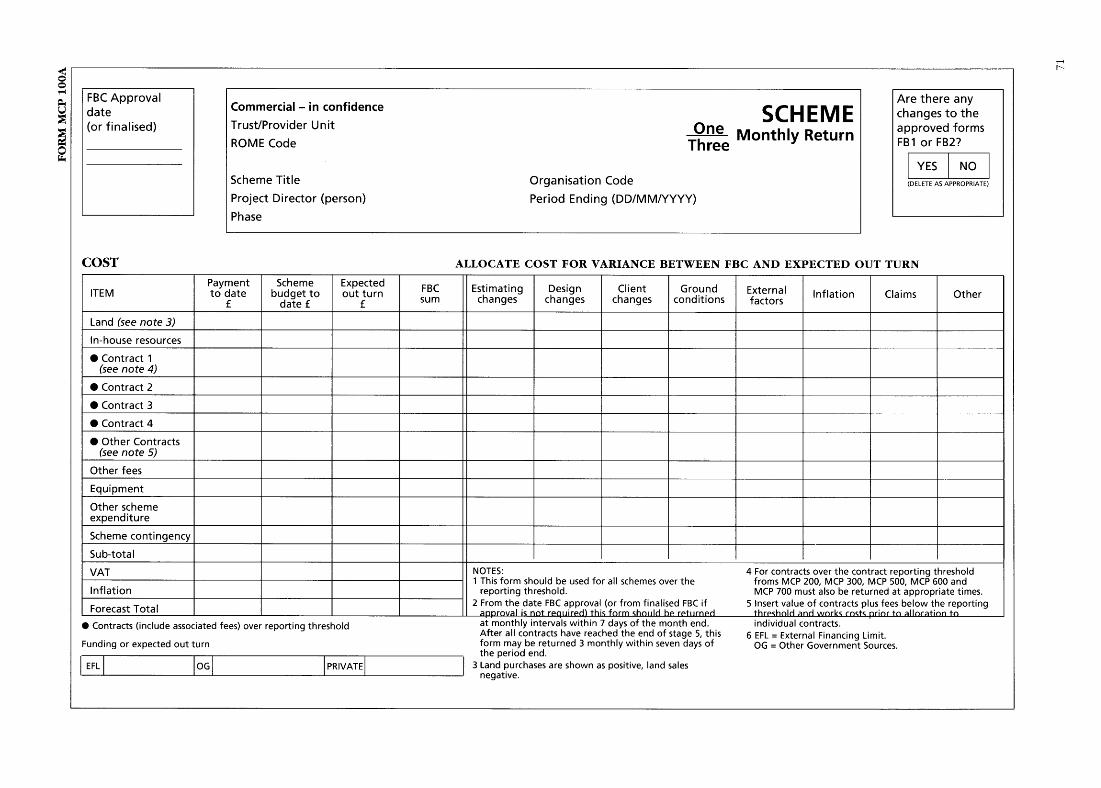
FBC Approval
Are there anydate
Commercial - in confidence
SCHEME(or finalised)
Trust/Provider Unit
changes to theOne Monthly Return
approved formsROME Code
Three
y
FB1 or FB2?
YES IVOScheme Title
Organisation Code
(DELETE AS APPROPRIATE)
Project Director (person)
Period Ending (DDIMMIYYYY)
Phase
COST
ALLOCATE COST FOR VARIANCE BETWEEN FBC AND EXPECTED OUT TURNPayment Scheme Expected FBC Estimating Design Client Ground ExternalITEM
to date
budget to
out turn
sum
changes
changes
changes
conditions
factors
Inflation
Claims
Otherf
date f
fLand (see note 3)
In-house resources" Contract 1
(see note 4)
" Contract 2" Contract 3
" Contract 4
" Other Contracts(see note 5)
OtherfeesEquipment
Other schemeexpenditure
Scheme contingencySub-total
IVAT
NOTES:
4For contracts over the contract reporting threshold1 This form should be used for all schemes over the
froms MCP 200, MCP 300, MCP 500, MCP 600 andInflation
reporting threshold.
MCP700 must also be returned at appropriate times.
Forecast Total
2 From the date FBC approval (or from finalised FBC if
5 Insert value of contracts plus fees below the reporting
"approval *~ not rpquor,-d) this form Should he ri-ttirned
thrPshold and works rosts priar to allocation toContracts (include associated fees) over reporting threshold
at monthly intervals within 7 days of the month end.
individual contracts.After all contracts have reached the end of stage 5, this
6 EFL = External Financing Limit .Funding or expected out turn
form may be returned 3 monthly within seven days of
OG = Other Government Sources.the period end .
EFL
OG
PRIVATE
3 Land purchases are shown as positive, land salesnegative .
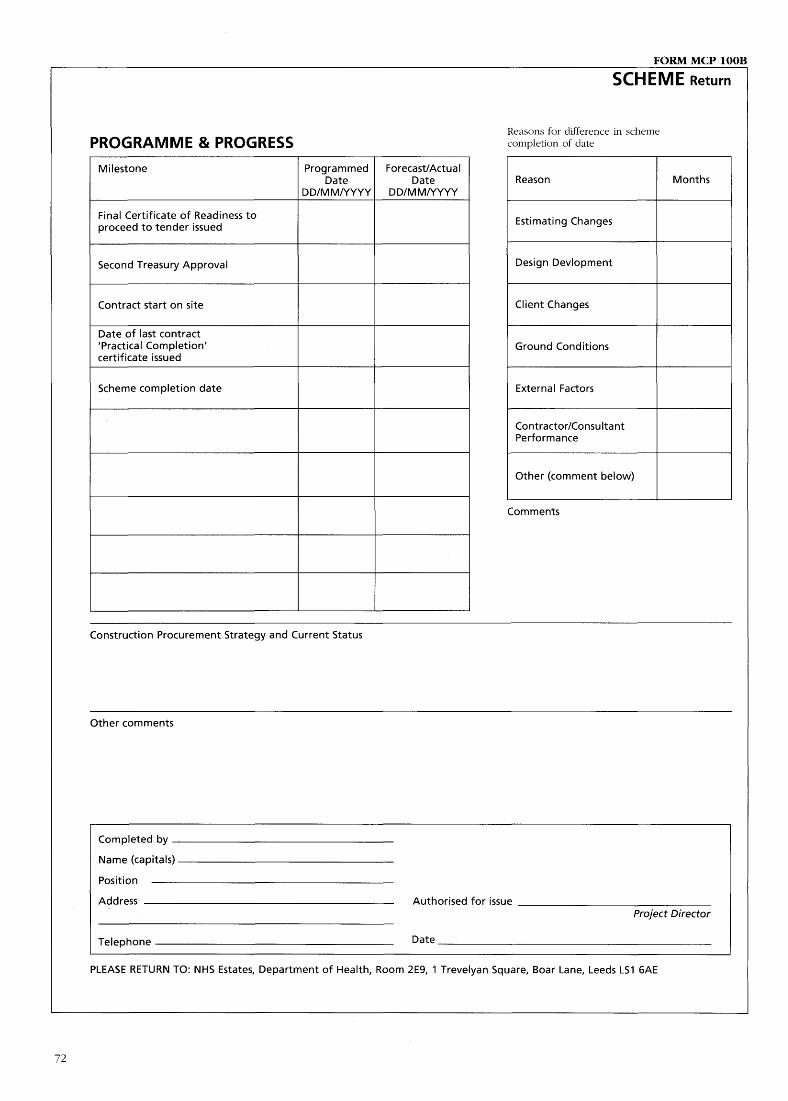
FORM MCP 100B
SCHEME Return
Reasons for difference in schemePROGRAMME & PROGRESS
completion of date
Milestone
Programmed Forecast/ActualDate Date
Reason
MonthsDD/MM/YYYY DD/MM/YYYY
Final Certificate of Readiness toproceed to tender issued
Estimating Changes
Second Treasury Approval
Design Devlopment
Contract start on site
Client Changes
Date of last contract'Practical Completion'
Ground Conditionscertificate issued
Scheme completion date
External Factors
Contractor/ConsultantPerformance
Other (comment below)
Comments
Construction Procurement Strategy and Current Status
Other comments
Completed by
Name (capitals)
Position
Address
Authorised for issueProject Director
Telephone
Date
PLEASE RETURN TO : NHS Estates, Department of Health, Room 2E9, 1 Trevelyan Square, Boar Lane, Leeds LS1 6AE

FORM MCP 200A
Commercial - in confidence
CONTRACTTrust/Provider Unit
ROME Code
Pre-Tender Report
Scheme Title
Contract Title
Organisation Code
Project Director (person)
Information valid at
PART A: Section A:1
Professional Services
Consultant's name
2
Type of Accommodation
a Architect
3
Functional Content
b Structural Engineer
4
Class of Work
c Mechanical Engineer
5
From/Type of Construction
d Electrical Engineer
6
Project Funding
e Quantity Surveyor
a EFL
b OG
c Priv
f Project Management
7
Date of Certificate of Readinessto Proceed to Tender
8
Date of EC Official Journal Notice
PART A: Section B:1
Contract Information
Target Start Date
Target Completion Date
Tendering Procedure
Type of Contract
Form of Contract
Fluctuating/Fixed Price*
2
Cost Information
MIPS Index
Indices Base : 1975 = 100
Pre-Tender Estimate
Budget Allocation
Variance
Contract
Associated Fees
VAT
Total
PART A: Section C: Notes
'Delete as appropriate .
Completed by
Name (capitals)
Position
Address
Authorised for issueProject Director
Telephone
Date
PLEASE RETURN TO: NHS Estates, Department of Health, Room 2E9, 1 Trevelyan Square, Boar Lane, Leeds LS1 6AE

FORM MCP 200H
Commercial - in confidence
CONTRACTTrust/Provider Unit
ROME Code
Post-Tender Report
Scheme TitleContract Title
Organisation Code
Project Director (person)
Information valid at
PART B: Contract Information :
1 Contractors
(i)(ii)
(iii)
(iv)Prime Cost
Unadjusted
AdjustedName
Sums (£)
Main Tender (O
Tender (I)
a Main Contractor(including Management Contractor, Designand Build Contractor, Consortium)
h Mechanical
c Electrical
d Lifts
e All other adjustments to the main contract
2
Tender date
7
Approved tender sum
3
Date awarded
8
Contingency sums in tender
4
Tender base date
9
Net tender
5
Index of approved tender
10 Fees
(Base 1975=100)
11 VAT
6
Contract dates - start :
complete :
12 Overall Cost at Tender
NOTES
Completed by
Name (capitals)
Position
Address
Authorised for issueProject Director
Telephone
Date
PLEASE RETURN TO : NHS Estates, Department of Health, Room 2E9, 1 Trevelyan Square, Boar Lane, Leeds LS1 6AE
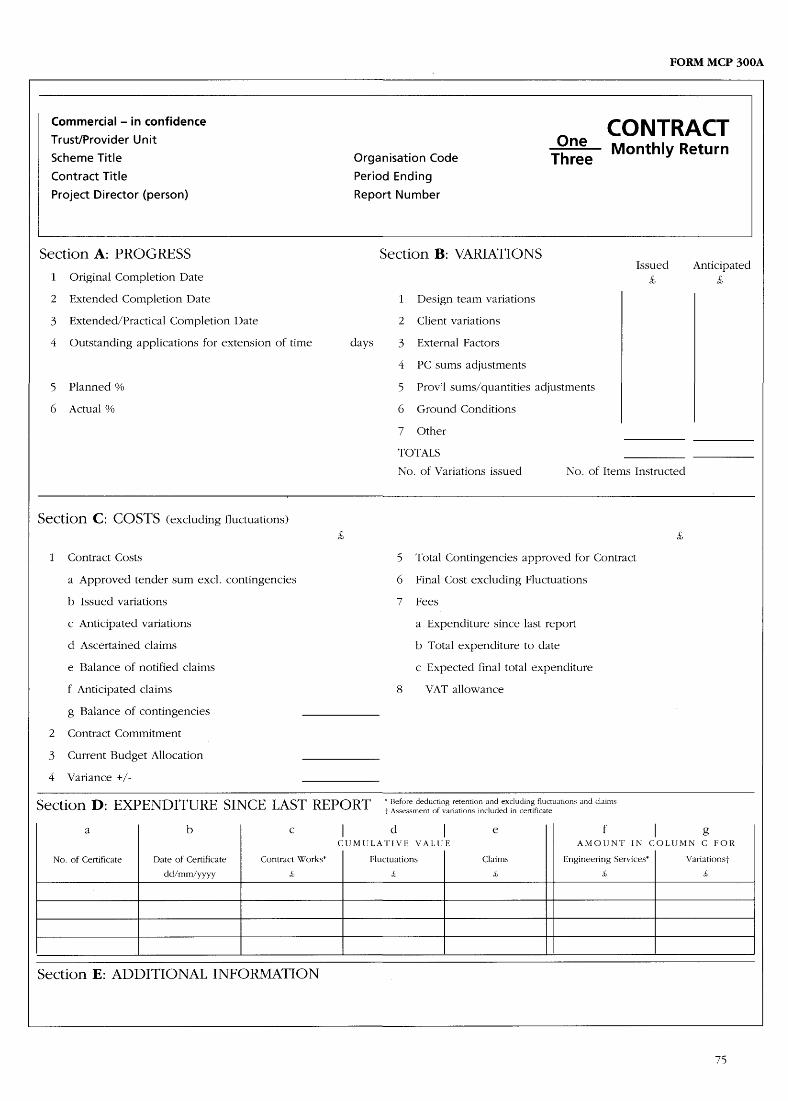
FORM MCP 300A
Commercial - in confidence
CONTRACTTrust/Provider Unit
OneScheme Title
Organisation Code
Three
Monthly Return
Contract Title
Period Ending
Project Director (person)
Report Number
Section A: PROGRESS
Section B: VARIATIONSIssued Anticipated
1
Original Completion Date
2
Extended Completion Date
1
Design team variations
3
Extended/Practical Completion Date
2
Client variations
4
Outstanding applications for extension of time
days
3
External Factors
4
PC sums adjustments
5
Planned %
5
Prov'l sums/quantities adjustments
6
Actual %
6
Ground Conditions
7 Other
TOTALS
No . of Variations issued
No. of Items Instructed
Section C: COSTS (excluding fluctuations)£,
£,
1
Contract Costs
5
Total Contingencies approved for Contract
a Approved tender sum excl . contingencies
6
Final Cost excluding Fluctuations
b Issued variations
7
Fees
c Anticipated variations
a Expenditure since last report
d Ascertained claims
b Total expenditure to date
e Balance of notified claims
c Expected final total expenditure
f Anticipated claims
8
VAT allowance
g Balance of contingencies
2
Contract Commitment
3
Current Budget Allocation
4 Variance +/-
Section D : EXPENDITURE SINCE LAST REPORTt' Asseore
dsss
dement
ofingvariations
retentionincluded
incertificate
cate
ti°ns and `aims
a
b
c
I
d
I
e
f
I
gCUMULATIVE VALUE
AMOUNT IN COLUMN C FOR
No . of Certificate
Date of Certificate
Contract Works*
Fluctuations
Claims
Engineering Services*
Variationst
dd/mm/yyyy
£
£
£
Section E: ADDITIONAL INFORMATION

FORM MCP 300B
COMMENTS AND ASSESSMENTS
CONTRACTOne
Monthly ReturnThree
By
Physical Progress and Programme
Costs
General State of Contract (delays, claims, other)
Completed by
Name (capitals)
Position
Address
Authorised byProject Director
Telephone
Date
PLEASE RETURN TO : NHS Estates, Department of Health, Room 2E9, 1 Trevelyan Square, Boar Lane, Leeds LS1 6AE
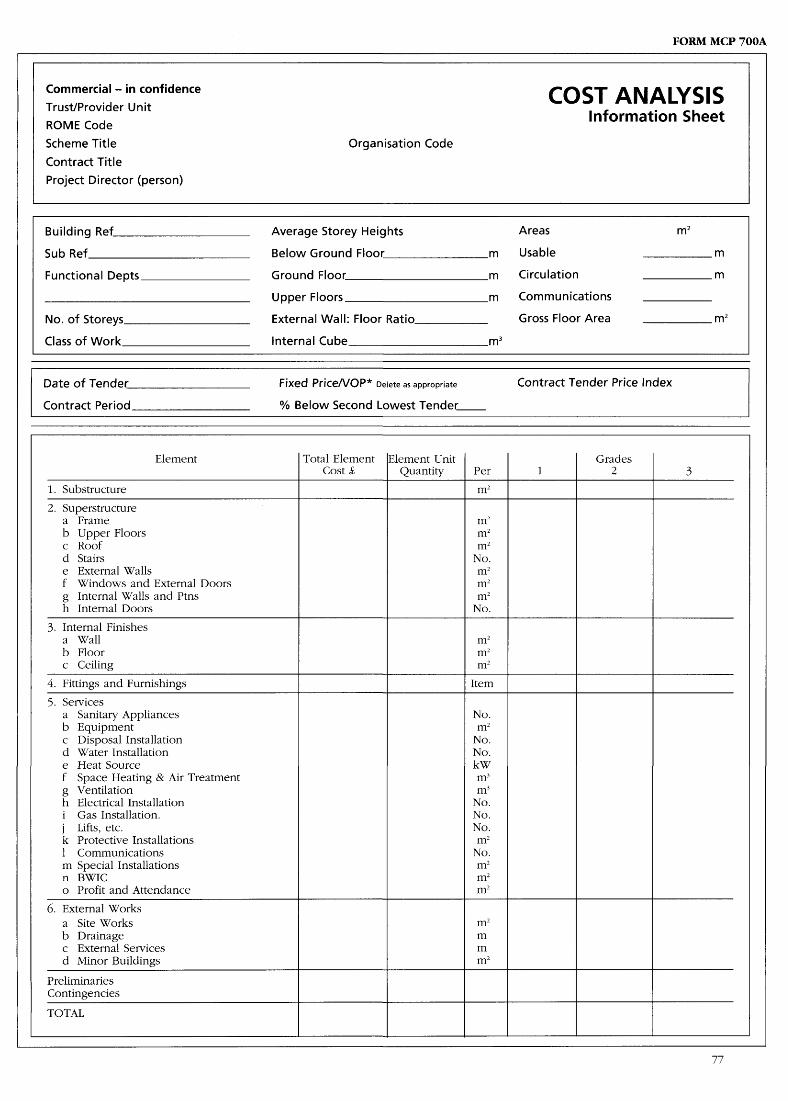
FORM MCP 700A
Commercial - in confidence
COST ANALYSISTrust/Provider Unit
Information SheetROME CodeScheme Title
Organisation CodeContract TitleProject Director (person)
Building Ref
Average Storey Heights
Areas
m2
Sub Ref
Below Ground Floor
m
Usable
m
Functional Depts
Ground Floor
m
Circulation
m
Upper Floors
m
Communications
No . of Storeys
External Wall : Floor Ratio
Gross Floor Area
mz
Class of Work
Internal Cube
m3
Date of TenderFixedPriceNOP* Delete as appropriate
Contract Tender Price Index
Contract Period
% Below Second Lowest Tender
Element
Total Element
Element Unit
GradesCost S'
Quantity
Per
1
2
3
1. Substructure
m2
2. Superstructurea Frame
m2b Upper Floors
m2c Roof
m2d Stairs
No.e External Walls
m2f Windows and External Doors
m2g internal Walls and Ptns
m2h internal Doors
No.
3 . Internal Finishesa Wall
m2b Floor
m2c Ceiling
m2
4. Fittings and Furnishings
Item
5 . Servicesa Sanitary Appliances
No.b Equipment
m2c Disposal Installation
No.d Water Installation
No.e Heat Source
kWf
Space Heating & Air Treatment
m3g Ventilation
m3h Electrical Installation
No.i
Gas Installation .
No.j Lifts, etc .
No.k Protective installations
m21 Communications
No.m Special Installations
m2n BWIC
m2o Profit and Attendance
m2
6. External Worksa Site Works
m2b Drainage
mc External Services
md Minor Buildings
m2
PreliminariesContingencies
TOTAL
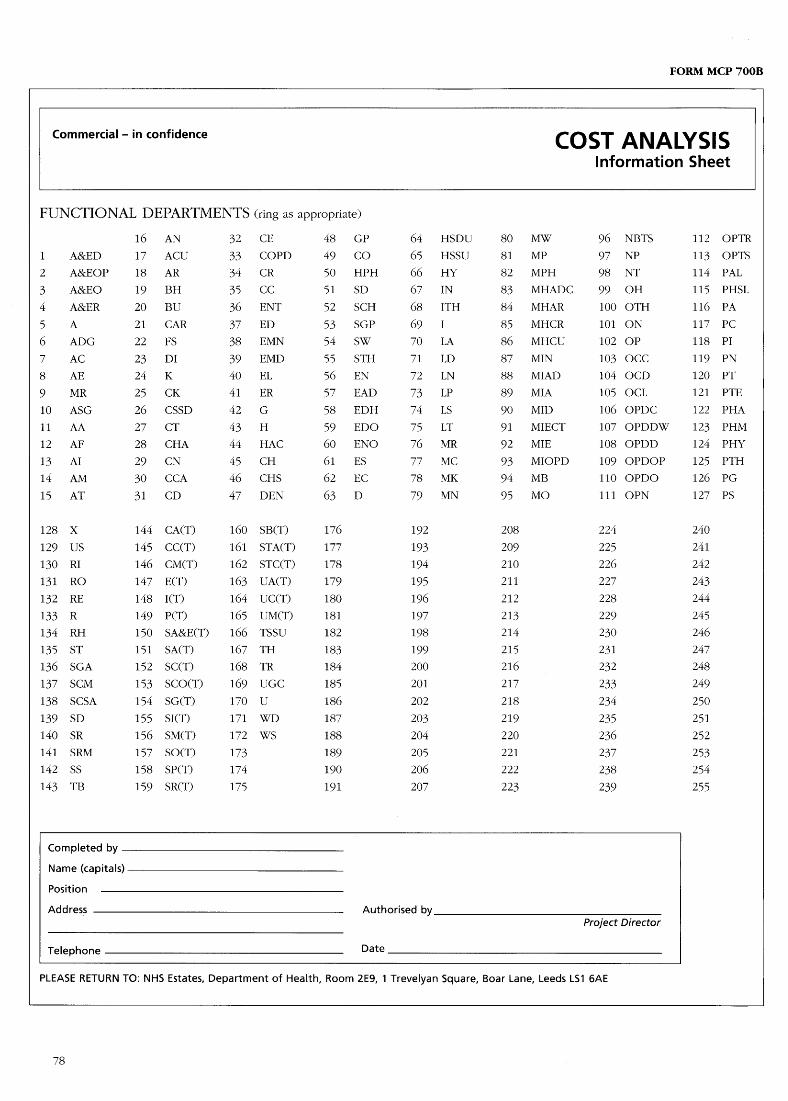
FORM MCP 700B
Commercial- in confidence
COST ANALYSISInformation Sheet
FUNCTIONAL DEPARTMENTS (ring as appropriate)
16 AN
32 CE
48 GP
64 HSDU 80 MW
96 NBTS
112 OPTR1 A&ED
17 ACU
33 COPD
49 CO
65 HSSU 81 MP
97 NP
113 OPTS2 A&EOP 18 AR
34 CR
50 HPH
66 HY
82 MPH
98 NT
114 PAL3 A&EO
19 BH
35 CC
51 SD
67 IN
83 MHADC 99 OH
115 PHSL4
A&ER
20 BU
36 ENT
52 SCH
68 ITH
84 MHAR
100 OTH
116 PA
5
A
21 CAR
37 ED
53 SGP
69 1
85 MHCR
101 ON
117 PC6
ADG
22 FS
38 EMN
54 SW
70 LA
86 MHCU
102 OP
118 PI
7
AC
23 DI
39 EMD
55 STH
71 LD
87 MIN
103 OCC
119 PN8
AE
24 K
40 EL
56 EN
72 LN
88 MIAD
104 OCD
120 PT9
MR
25 CK
41 ER
57 EAD
73 LP
89 MIA
105 OCL
121 PTE
10 ASG
26 CSSD
42 G
58 EDH
74 LS
90 MID
106 OPDC
122 PHA11 AA
27 CT
43 H
59 EDO
75 LT
91 MIECT
107 OPDDW
123 PHM12 AF
28 CHA
44 HAC
60 ENO
76 MR
92 MIE
108 OPDD
124 PHY13 AI
29 CN
45 CH
61 ES
77 MC
93 MIOPD
109 OPDOP
125 PTH14 AM
30 CCA
46 CHS
62 EC
78 MK
94 MB
110 OPDO
126 PG15 AT
31 CD
47 DEN
63 D
79 MN
95 MO
111 OPN
127 PS
128 X
144 CA(T)
160 SB(T)
176
192
208
224
240129 US
145 CC(T)
161 STA(T) 177
193
209
225
241
130 RI
146 CM(T)
162 STC(T) 178
194
210
226
242131 RO
147 E(T)
163 UA(T)
179
195
211
227
243
132 RE
148 I(T)
164 UC(T)
180
196
212
228
244
133 R
149 P(T)
165 UM(T)
181
197
213
229
245134 RH
150 SA&E(T) 166 TSSU
182
198
214
230
246
135 ST
151 SA(T)
167 TH
183
199
215
231
247136 SGA
152 SC(T)
168 TR
184
200
216
232
248137 SCM
153 SCOT) 169 UGC
185
201
217
233
249138 SCSA
154 SG(T)
170 U
186
202
218
234
250139 SD
155 SI(T)
171 WD
187
203
219
235
251140 SR
156 SM(T)
172 WS
188
204
220
236
252141 SRM
157 SO(T)
173
189
205
221
237
253142 SS
158 SP(T)
174
190
206
222
238
254143 T13
159 SR(T)
175
191
207
223
239
255
Completed by
Name (capitals)
Position
Address
Authorised byProject Director
Telephone
Date
PLEASE RETURN TO : NHS Estates, Department of Health, Room 2E9, 1 Trevelyan Square, Boar Lane, Leeds L51 6AE
Appendix 9 : Assessmentof Consultants' andContractors' PerformanceAs part of their obligations to manage every aspectof the building process, NHS Trusts and authoritiesare required to complete financial and technicalchecks of all firms being considered for inclusionon tender lists .
The information supplied to NHS Estates on theperformance of contractors and consultants will bemade available to NHS Trusts and authorities toassist them in formulating their tender lists . Theseforms are required for all schemes above theScheme Reporting Threshold.
Consultants MCP 500
NHS trusts and authorities will be able to ascertainthe current levels of fee bids, to allow them tocompare the competitiveness of bids as well as theperformance of consultants . Notification of detailsof bids for all consultants should be returned nolater than seven days after notification to thesuccessful consultant . The assessment of theconsultant's performance should be returned at theend of each of the following appropriate stages ofthe service
- design (issue of the Readiness to Proceed toTender Certificate) ;
- construction (issue of Practical CompletionCertificate) ; and
- commission .
Contractors MCP 600
Information on the performance,of contractors willhighlight areas of poor performance, which mayinfluence the decision to short-list firms for ascheme . The information on tender results oncontractors and subcontractors will show howcompetitive they have been in previous tendersand how well they have performed on otherhealth schemes . The results of all tenders forcontractors and subcontractors shall be returnedon the date of tender acceptance . Theperformance report on the contractors' andsubcontractors' performance shall be returned atpractical completion.
Forms NICP 500 and MCP 600 are set out on thefollowing pages .
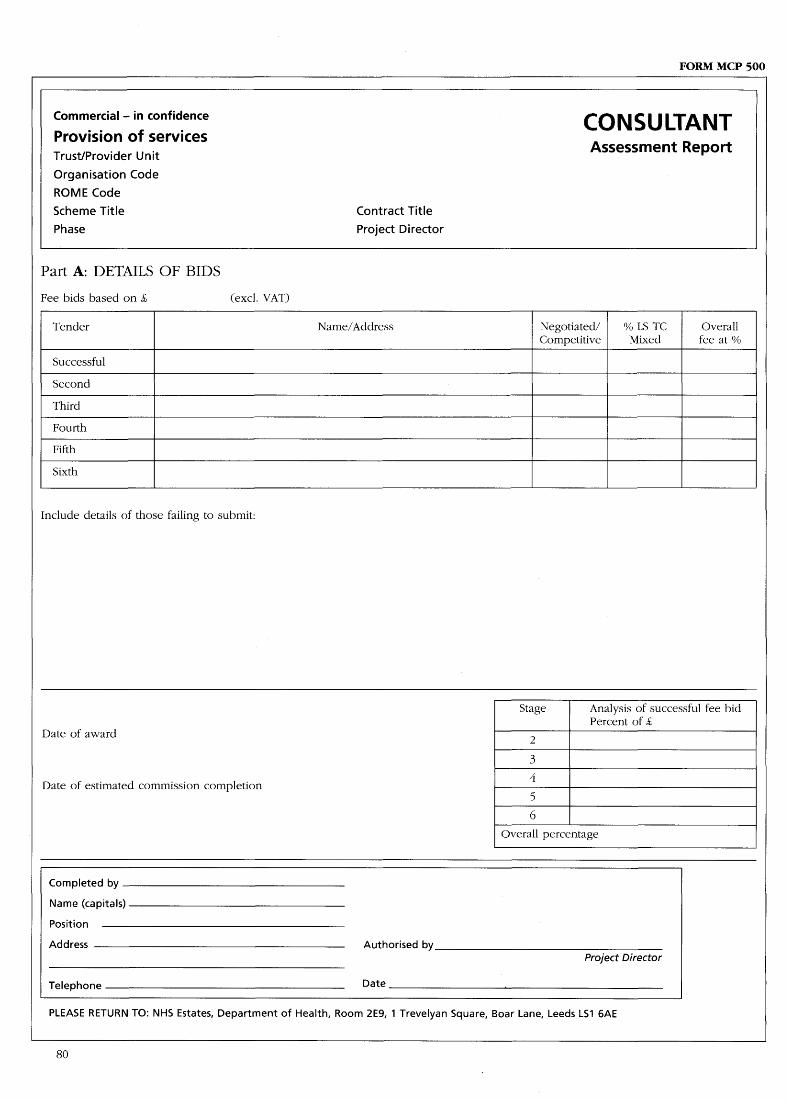
FORM MCP 500
Commercial- in confidence
CONSULTANTProvision of servicesTrust/Provider Unit
Assessment Report
Organisation CodeROME CodeScheme Title
Contract Title
Phase
Project Director
Part A: DETAILS OF BIDS
Fee bids based on £,
(excl . VAT)
Tender
Name/Address
Negotiated/
% LS TC
OverallCompetitive
Mixed
fee at
Successful
Second
Third
Fourth
Fifth
Sixth
Include details of those failing to submit :
Stage
Analysis of successful fee bidPercent of S,
Date of award
3
Date of estimated commission completion
4
5G
Overall percentage
Completed by
Name (capitals)
Position
Address
Authorised byProject Director
Telephone
Date
PLEASE RETURN TO : NHS Estates, Department of Health, Room 2E9, 1 Trevelyan Square, Boar Lane, Leeds LS1 6AE

FORM MCP 500 (CON'I7
QUALITY OF SERVICE
PART B: AT END OF DESIGN STAGEMarking : ~ See below
Actual/Expected Completion Date of Commission
Form completed by
Name (capitals)
Position
Address
Date
Telephone
Authorised for issue
Project Director
PART C: AT END OF CONSTRUCTION STAGEMarking : El See below
Actual/Expected Completion Date of Commission
Form completed by
Name (capitals)
Position
Address
Date
Telephone
Authorised for issue
Project Director
PART D: AT END OF COMMISSIONMarking : 11 See below
Actual Completion Date of Commission
Form completed by
Name (capitals)
Position
Address
Date
Telephone
Authorised for issue
Project Director
Stage
Analysis of out-turn fee bidPercent of £,
MARKING :2
1
Would hesitate to recommend for3
future commissons .4
2
Below average3 Average4
Above averageG
Overall percentage
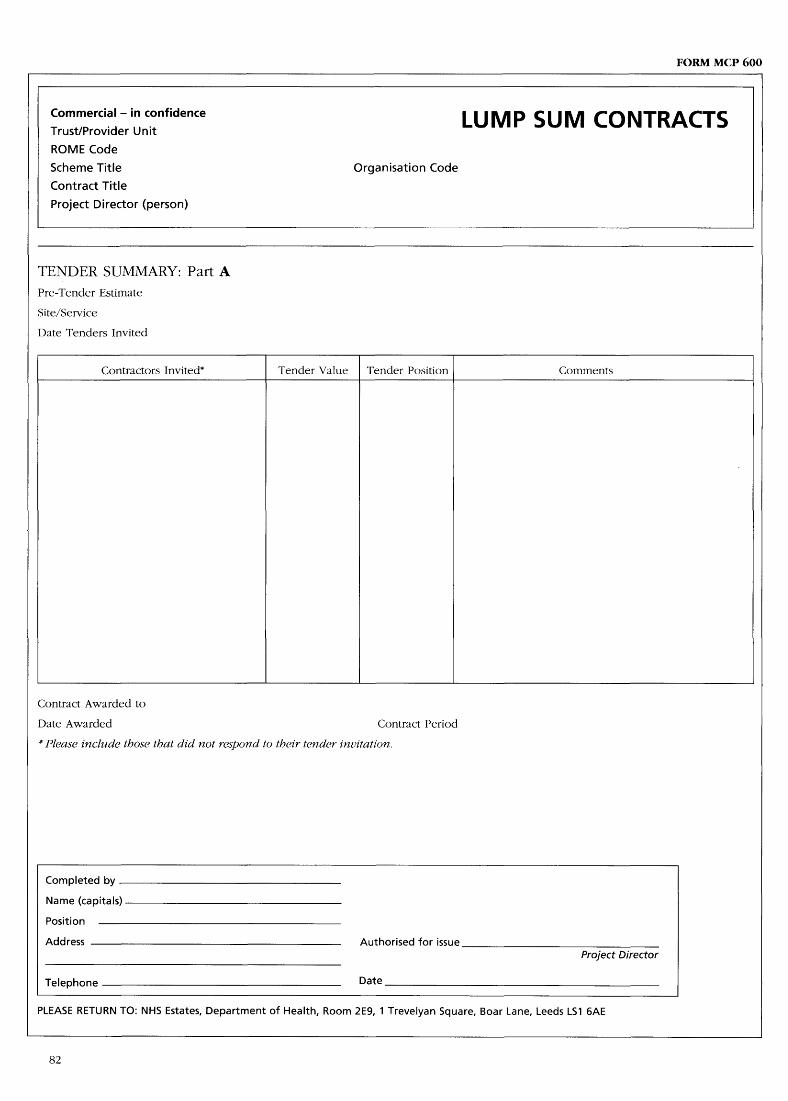
FORM MCP 600
Commercial- in confidence
LUMP SUM CONTRACTSTrust/Provider Unit
ROME Code
Scheme Title
Organisation CodeContract Title
Project Director (person)
TENDER SUMMARY: Part APre-Tender Estimate
Site/Service
Date Tenders Invited
Contractors Invited*
Tender Value
Tender Position
Comments
Contract Awarded to
Date Awarded
Contract Period
* Please include those that did not respond to their tender invitation .
Completed by
Name (capitals)
Position
Address
Authorised for issueProject Director
Telephone
Date
PLEASE RETURN TO : NHS Estates, Department of Health, Room 2E9, 1 Trevelyan Square, Boar Lane, Leeds LS1 6AE

FORM MCP 600 (cont)
Commercial - in confidence
PERFORMANCE REPORT BY TH ETrust/Provider Unit
CONTRACT ADMIN ISTRATORROME Code
Your Assessment of the Contractor's PerformanceScheme Title
Contract Title
Organisation Code
Project Director (person)
TENDER SUMMARY: Part B
Aspects of the Contract
Mark
A Above averageB Average
1 WorkmanshipC
Below average2 Speed
D Would hesitate to recommend for future
3 Organisation
contracts (this MUST be substantiated bywriting a separate report and attaching copies
4 Health and Safety
of all relevant correspondence with the
5 General Operation
contractor) .
COMMENTS :
Completed by
Name (capitals)
Position
Address
Authorised for issueProject Director
Telephone
Date
PLEASE RETURN TO : NHS Estates, Department of Health, Room 2E9, 1 Trevelyan Square, Boar Lane, Leeds LS1 6AE

Appendix 10 :Glossary of TermsActivity Database (ADB)A computerised briefing guide for design teamsand health administrators . ADB assists by definingspecific activities which have to be accommodatedin health building space and design, by listing thefunctional requirements and their relatedcomponents .
Approved BudgetThe capital cost of the project in the Full BusinessCase approved by the NHS Executive, or anychanges to it approved subsequently .
BriefThe document which defines the Trust'srequirements and which forms the basis of allsubsequent design, procurement, and construction .
Business Case Guide for Capital Investments(Business Case Guide)The document issued by the Executive detailingthe procedures necessary to obtain approval ofand funding for a new capital investment projectin the NHS .
CEOThe chief executive officer of a Trust .
CONCISECONCISE is a software system for the NHS capitalprogramme . It comprises a suite of programmesdesigned to assist project managers, financemanagers and construction specialists . NHS Estatescan provide more information on CONCISE .
CONCODEGuidance on the procurement of and contractualarrangements for NHS building and engineeringwork and on the commissioning of consultants .Issued by NHS Executive .
ContingencyAn allowance in a project budget or cost estimate,over and above the base estimate, to provide themost likely outcome of time and cost after takingrisks into account, and assuming that managementaction is taken to minimise their effect .
Contract AdministratorThe person named in a construction contract withresponsibility for administering it and for givingdecisions in respect of it .
Contract Procurement StrategyA planned strategy of arranging for the project tobe designed and constructed . It determines thenumber, scope, and types of contracts to beplaced .
Departmental Cost Allowance (DCA)A reference cost issued by NHS Executive for theprovision of a defined amount of functionalaccommodation based on Health Building Notes(HBHs) . (See also on-costs .) Used to assistestimating .
Design TeamThe professional architects and engineersresponsible for the design of a project .
EFLExternal financing limit - the amount provided to aTrust for capital expenditure .
EPCEstimate of prime cost based on preliminarydesign proposals under a management contract .
Final AccountThe final cost of a contract after taking intoaccount any re-measurement, variations,provisional and prime cost sums, and claims.Agreed by the quantity surveyor .
Financial Status Report (FSR)A report prepared monthly by the quantitysurveyor and the project manager for submissionto the Trust which shows the financial position ofthe project. Terms used in the FSR are defined inAppendix 6 .
Fixed price (FP) tendersSee Median Index of Public Sector (MIPS) BuildingTender Prices .
Full Business Case (FBC)The document prepared by a Trust in accordancewith the Business Case Guide and approved bythe Outpost which defines the criteria for aproject .
Health Building Notes (HBNs)Documents prepared by NHS Executive which setthe standards of accommodation andenvironmental services for health buildings .
Health Building ProceduresThese and other related procedures relating to themanagement of health care building projectsissued by the Executive .
Health Technical Memoranda (HTMs)Documents prepared by NHS Executive whichgive guidance on specific health building subjects,mainly in the field of engineering and safetystandards .
InflationThe change in the estimated cost of a project dueto increases or decreases in general price levels .The adjustment made to a cost estimate, which isbased upon price levels at the date of theestimate, in order to provide a proper comparisonof actual cost with the Approved Budget .
Investment Decision Maker (IDM)The project specific role of the CEO .
Latest Estimated CostThe estimated out-turn cost of the project at thedate of the report .
Median Index of Public Sector (MIPS) BuildingTender PricesA quarterly series of indices calculated from ratesfor measured work contained in Bills of Quantitiesfor accepted tenders for a range of public sectorbuilding works, including those for the healthservice . MIPS is the Department of Health acronymfor the Public Sector (PUBSEC) unweighted indexseries produced by the Department of theEnvironment . The index series is sub-divided intoTenders let on a Firm Price (FP) - generally thosewith a contract period not exceeding two yearsand Variation of Price (VOP) tenders - generallythose with a contract period exceeding two years .Unlike FP tenders where the tenderer has to makean allowance for increased costs in the originaltender, VOP tenders are net of increased costs,which are reimbursed separately - usually bymeans of a formula applied to a breakdown of theoriginal tender. NHS Estates can provide furtheradvice on these indices and forms of tender .
NHS EstatesAn Executive Agency of the Department of Healthwhich undertakes a range of central responsibiltiesin relation to capital projects on behalf of the NHSExecutive .
NHS ExecutiveThe Executive of the NHS .
NHS TrustA Health Care organisation within the NHS, whichhas been given Trust status and responsibilities .
NucleusA system for hospital planning and design,supported by comprehensive information,including standardised briefing material andplanning documentation .
Outline Business Case (OBC) - (see BusinessCase Guide) .
On-costsThat part of the capital cost of a building arisingfrom the interaction of departments within abuilding and the building with its site .
Post-tender EstimateThe estimated capital cost of a project when bidsfor the main construction contract have beenreceived, based on the accepted price .
Pre-tender EstimateThe estimated capital cost of the project when thetender documents for the main constructioncontract have been completed, but before bidshave been received .
ProjectA programme of activity to deliver a scheme forcapital investment in a health care buildingscheme and associated facilities and equipment . Itmay be a part of a wider scheme with theobjective of enabling a Trust to improve healthcare more generally, including other activities suchas staff resources and training, operatingprocedures, and the like .
Project BoardA board comprising senior Trust personnel withresponsibilities for a project delegated to it by theIDM .
Project Director (PD)The individual appointed by a Trust to represent itand to take personal responsibility for thesuccessful outcome of a project . Reporting to theIDM and with delegated authority to manage theday to day issues of the project .
Project Execution Plan (PEP)A document prepared by the project managerunder the direction of the project director whichsets out the scope, objectives, relative priorities,control processes, and administrative arrangementsfor a project .
Project ManagerThe individual with professional capabilityappointed to manage the design, construction,procurement, and commissioning of a buildingproject . Generally, the senior person in charge ofthe resource provided by an externally appointedproject management firm and referred to as the`project manager' . Responsible to the projectdirector.
Project Progress Report (PPR)A monthly report, prepared by the projectmanager, for submission to the Trust which showsthe progress of the Project compared with theprogramme . The PPR incorporates the FinancialStatus Report .
Project TeamThe project manager, designers, quantitysurveyors, contractors, and other people appointedby the project director to manage, design, andbuild the project . All are usually externalappointments .
PSCRThe Public Supply Contracts Regulations (S .I .1991/2679) published by HMSO, or anysubsequent amendment to it .
PWCSThe Public Works Contract Regulations 1991 (S .I .1991/2Cí80) published by HMSO, or anysubsequent amendment to it .

siteThe place where the project building works are tobe carried out and the equipment installed .
User PanelA panel of end users established for the purpose ofdefining requirements for inclusion in the brief andmonitoring that those requirements have been met .This function may also be carried out by theproject board .
Value EngineeringA review of the design of a part of a project todetermine whether the objectives of the brief could
be achieved in a better way . The improvementmay be in its capital cost, in ease of construction,in co-ordination with other features, in ease orcost of operation, or in aesthetic appearance .
Variation of Price (VOP)A clause in a contract which provides for contractpayments to be adjusted to take account ofincreases or decreases in cost due to inflation . Theadjustments are usually made by reference topublished cost indices . (See Median Index ofPublic Sector (MIPS/Building Tender Prices) .

Appendix 11 :BibliographyOther documents in the CapitalInvestment Manual:Overviewfor ChiefExecutivesProject OrganisationNHS Business Case Guidefor Capital InvestmentsPrivate Finance Information PackIM&T GuidanceCommissioning a Health Care FacilityPostproject Evaluation
Treasury Central Unit on Procurement(CUP) Guidance :Project Sponsorship (No-33)Approval of Works Projects (No-38)Managing Risk and Contingencyfor Works Projects(No.41)Contract and Contract ManagementforConstruction Works (No . 12)Contract Strategy Selectionfor MajorProjects(No-36)The Selection and Appointment of WorksConsultants (No . 13)Selection of Works Contractors (Nos . 26a and b .)Post Tender Negotiations and PTV Update (Nos .1and 19)Estimatingfor Works Projects (No . 15)Cost Managementfor Works Projects (No.25)Life Cycle Costing (No.35)
NHS Estates PublicationsESTATECODE (Asset Management):
- Strategic Asset Management- Asset Maintenance- Estate Investment Planning- Analysis of Estate Performance- Environment for Quality Care
CONCODE :- Procurement and Contract Policy- Guidance on Contract and Commissioning
Procedures
- Guidance on Requirements of EC Directives- Guidance on Specific Standard Lead Forms
of' Contract
Quarterly Briefing : Investment Economics andConstruction Project Information
Health Building Notes :- various
Health Technical Memoranda :- various
Health Facilities Notes:- various
Firecode.- various
Other:Hospital Building in England:Treasury Minute on the Eighteenth Reportfrom theCommittee ofPublic Accounts 1989-90. Cm. 1150 .
The Chelsea and Westminster Hospital:Treasury Minute on the Twenty-sixth Reportfromthe Committee ofPublic Accounts 1992-93 .Cm.2186 .

Index
References are to paragraphs
Additional paymentsclaims for
4.9.1Administrative systems
Project Execution Plan
A.6.7 .1, A.6 .7 .2Briefchanges in
A.4.1 .2development of
1 .6.1,2 .2.1,A .4 .4 .1-A .4 .4 .7frozen 2.2 .2full A.4 .3 .1initial, contents of
A.4.2 .1meaning A.4 .1 .1preparation of
A.4.1.3Budget cost
approved 1.14.3capital expenditure and VAT, covering
1.14.2financial overspend, financing
1 .14.5inflation and VAT, additional amount for
1.14.4preparation of
1.14.1Certificate of Readiness to Proceed to Tender
assurances in
2.10.2requirement of
2.10.1Change
control of
A.3.3.1-A .3 .3 .5Construction and equipment supply
additional payments, claims for
4.9.1cost management
4.7 .1objective 4.1 .1payment 4.8 .1plans, development of
4.1.2programme management
4.5.1, A.6.6A-A.6 .6 .3progress monitoring
4.4.1, A.7 .1 .2quality control
4.6.1record keeping
4.10.1Consultantsemployment of
1 .4 .1Contingency managementprocedures A.3 .2 .1review A.3 .2 .2
Contractadditional payments, claims for
4.9.1payment 4.8 .1programme management
4.5.1, A.6 .6.1-A .6 .6 .3progress monitoring
4.4.1, A.7 .1 .2quality control
4.6.1Contract administrator
appointment of
4.2 .2production information
4.3.1role of
4.2.1Contract procurement strategy
construction and equipment supply
4.1.1managing contracts, general procedures for
4.1.4meaning 1.9 .1procedures 3.1 .3
Costconstruction, management during
A.3.9 .1continuous and stage estimates
A.3.6.1elemental planning
A.3.5.1-A.3 .5 .3management 4.7.1,A.6 .5 .1-A .6-5 .5monitoring A.7 .1 .2profiling A.3 .4 .1
Cost estimateupdating 2.3 .2
Cost managementobjectives of
A.3.1 .1principal areas of
A.3.1 .2Costing building schemes
contingency allowances, setting
A.2.13.1, A.2 .13.2contingency and risk exposure, estimating
A.2 .12.1,A.2 .12.2
departmental cost allowances
A.2.5.1-A .2 .5 .4equipment cost allowances
A.2.6.1, A.2 .6 .2
estimate classification
A.2.2.1-A .2 .2 .5estimate components
A.2.4 .1, A.2 .4 .2estimating A.2 .3 .1guidance on
A.2.1 .1potential risks, identification of
A.2.10.1, A.2 .10.2project base estimate, content of
A.2.8 .1risk analysis and contingency allowance
A.2.9 .1,A.2 .9 .2
risk assessment
A.2.11 .1-A .2 .11 .5statistical indicators
A.2.7 .1, A.2 .7 .2Defectspost-completion 6.2 .1
Deliverablessupply of
5 .4.1Design
brief development
2.2.1design development, control during
A.3.7.1outline 1.8 .1quality, importance of
2.1.3stage, purpose of
2.1 .1Design and build contract
versions of
4.11 .1Design detailprocedures 2.6 .2process of
2.6.1Design development
Certificate of Readiness to Proceed to DetailedDesign 2.4 .2
cost control during
A.3.7 .1procedures 2.4 .1
Design managementprocedures for
2.3.2purpose of
2.3 .1Design team
Certificate of Readiness to Proceed to Tender,assurances in
2.10.2leadership 2.1 .2NHS Estates standards, familiarity with
2.1 .4responsibility of
2.3.2Development Control Planmeaning 1 .11 .1
Equipmentadvice on
1 .12.3budget A.5 .4 .1-A .5 .4 .4groups A.5 .2 .1-A.5 .2 .7importance of
1.12.1purchase 4.13.1schedules 2.5 .1strategy
1 .12 .2, A.5 .3 .1tendering and award of contracts
3.1 .1Equipping
process, summary of
A.5 .5.1-A .5 .5 .4project director, role of
A.5.1 .1Full Business Case
entire scope, implementation of
6.4.2forms
App. lproject organisation arrangements, explanation of
1 .2 .1scope of work required
1 .1.2Health and safety regulationshaving regard to
4.1.5Internal project control organisation
1.2 .1
Management contractsEstimate of Prime Cost
4.12.3guidance on
4.12.1increase in tender costs, funding to meet
4.12.4monthly financial status reports
4.12.5reason for using
4.12.2
NHS Executiveapproval, obtaining
1.17.1completion of design stage, approval on
2.10.3

Outline Business Caseapproval of
1 .1 .1
Planning permissionlate discussions, effect of
1.10.3obtaining 2 .7 .1planning authority, consultation with
1.10.2requirement of
1 .10.1responsibility for
2.7.2Post-completion
claims
6.1 .1, A.3 .11 .1-A .3 .11 .5defects 6.2 .1final accounts
6.1.1,A .3 .10.1final certificates
6 .3.1stage completion
6.4.1Post-project evaluation
planning for
1.16 .1Preferred option
affordability and costs
1.3.2alternative, consideration of
1.3.3justification for
1 .3 .1Private sector
involvement, consideration of
1 .5.1Procurement
implementation of policies
3.2.2overall project programme, integration into
3.1.4public, policies relating to
3.2 .1Production informationmeaning 4 .3 .1
Progress monitoringsystems for
4.4.1Progress reports
accurate, consistent and on time, to be
A.7.1.6contents of
A.7.1 .4functions A.7 .1 .5monthly A.7 .2 .1requirement of
A.7.1 .1use of
A.7.1 .3Project certificates
App.1Project director
consultants, employment of
1 .4.1equipping, role in
A.5 .1 .1items charged against budget, approval of
3 .1.2role of
A.6 .4 .2Project Execution Plan
administrative systems and procedure
A.6.7 .1, A.6 .7 .2changing A.6 .1 .3content A.6 .2 .1cost management procedures
A.6.5 .1-A .6 .5 .5format A.6 .2 .1mandatory requirement of
A.6.1 .1programme management
A.6.6.1-A .6 .6 .3project cost plan
A.6.5.1-A .ó .5 .5project definition and brief
A.6.3 .1, A.ó .3 .2
project director, role of
A.6.4.2project organisation, outlining
A.6.4 .1responsibilities, definition of
A.6.4 .3, A.6 .4 .4statement of policies and procedures, as
A.6.1 .2technical standards
A.6.8.1, A.6 .8 .2Project manager
responsibility of
2.3 .2Project monitoring reportsNHS Estates, submission to
1.18.1Riskassessment 1 .13 .1contingency provision
1.13.1Running costs
estimates, importance of
1 .15.2model, design on
1.15.1Scheme name
consistency of
1.17.2Site investigations
extent of
1.7.2requirement of
1 .7.1Stage completion
contract, execution of
2.5.2process of
2 .5.1Strategic context
review of
1.3.1Technical commissioning and handover
Certificate of Practical Completion
5 .5.1characteristics 5 .1 .1deliverables, supply of
5.4 .1inspection and testing
5.3.1organisation 5 .2 .1stage completion
5.5.1Tender
assessment 2.3 .1CONCODE, advice in
3 .1.2documents 2.8 .1estimate before
2.9 .1general procedures for
3.1 .1lists 2.3 .1period for
2.3.1post-tender estimate
2 .4.1, 3.1 .5post-tender negotiation
2.3 .1Tenderingaward of contract, procedure after
2.5.3component parts
2.3.1CONCODE, reference to
2.3.1contract, execution of
2.5.2stage completion
2.5.1Treasury approvalrequirement of
1.17.1scheme above Treasury threshold
1.17.3Value engineering
A.3.8.1-A .3 .8 .3
Published by HMSO and available from:
HMSO Publications Centre(Mail, fax and telephone orders only)PO Box 276, London, SW8 5DTTelephone orders 0171-873 9090General enquiries 0171-873 0011(queuing system in operation for both numbers)Fax orders 0171-873 8200
HMSO Bookshops49 High Holborn, London, WC1V 6HB(counter service only)0171-873 0011 Fax 0171-831 132668-69 Bull Street, Birmingham B4 6AD0121-236 9696 Fax 0121-236 969933 Wine Street, Bristol, BS1 2BQ0117 9264306 Fax 0117 92945159-21 Princess Street, Manchester, M60 8AS0161-834 7201 Fax 0161-833 063416 Arthur Street, Belfast, BT1 4GD01232 238451 Fax 01232 23540171 Lothian Road, Edinburgh, EH3 9AZ0131-228 4181 Fax 0131-229 2734The HMSO Oriel BookshopThe Friary, Cardiff CFl 4AA01222 395548 Fax 01222 384347
HMSO's Accredited Agents(see Yellow Pages)
and through good booksellers
17.50 net