carcinoma cuniculatum of the nasal tip
TRANSCRIPT

Formosan Journal of Surgery (2016) 49, 39e44
brought to you by COREView metadata, citation and similar papers at core.ac.uk
provided by Elsevier - Publisher Connector
Available online at www.sciencedirect.com
ScienceDirect
journal homepage: www.e-f js .com
CASE REPORT
Carcinoma cuniculatum of the nasal tip
Chin-Jung Feng a,b, Wing-Yin Li c, Han-Nan Liu d, Hsu Ma a,b,Szu-Hsien Wu a,b,*
a Division of Plastic Surgery, Taipei Veterans General Hospital, Taipei, Taiwanb Department of Surgery, National Yang Ming University, Taipei, Taiwanc Department of Pathology and Laboratory Medicine, Taipei Veterans General Hospital, Taipei, Taiwand Department of Dermatology, Taipei Veterans General Hospital, Taipei, Taiwan
Received 10 April 2015; received in revised form 12 May 2015; accepted 11 June 2015Available online 11 February 2016
KEYWORDScarcinomacuniculatum;
cutaneous verrucouscarcinoma;
keratoacanthoma;nasal tip;squamous cellcarcinoma
Conflicts of interest: The authors d* Corresponding author. Division of P
Taiwan.E-mail address: [email protected]
http://dx.doi.org/10.1016/j.fjs.2015.1682-606X/Copyright ª 2016, TaiwanCC BY-NC-ND license (http://creativ
Summary Carcinoma cuniculatum, also known as cutaneous verrucous carcinoma, is a rare,low-grade, well-differentiated squamous cell carcinoma usually involving the foot. It is oftenlocally aggressive but rarely metastatic. Only 10 cases involving the skin of the face (exceptthe lips and scalp) have been reported. We describe a 74-year-old man who presented withcarcinoma cuniculatum on the nasal tip arising from a keratoacanthoma-like lesion. To ourknowledge, this is the first report of such a case in the literature. Literature related to carci-noma cuniculatum is also reviewed, and the challenges in diagnosis and choice of treatmentare also described. In this case, the patient initially presented with keratoacanthoma on thenasal tip, and rapid recurrence with a verrucous mass occurred 1 month following tumor exci-sion. Wide excision with 5-mm safe margins and full-thickness skin graft resurfacing were per-formed smoothly after recurrence. Histopathologic examination revealed carcinomacuniculatum. The patient recovered uneventfully, and no recurrence of the lesion was re-ported over a 62-month period of observation. Overall, the prognosis of carcinoma cunicula-tum is usually favorable. However, early diagnosis and treatment of carcinoma cuniculatumare crucial by clinicopathological standards. General clinical awareness of this entity contrib-uted to more appropriate and timely treatment.Copyright ª 2016, Taiwan Surgical Association. Published by Elsevier Taiwan LLC. This is anopen access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
eclare no conflicts of interest.lastic Surgery, Taipei Veterans General Hospital, Number 201, Section 2, Shih-Pai Road, Taipei 112,
.tw (S.-H. Wu).
06.005Surgical Association. Published by Elsevier Taiwan LLC. This is an open access article under theecommons.org/licenses/by-nc-nd/4.0/).

Figure 1 (A) Frontal view of the keratoacanthoma-like lesionon the nasal tip. (B) Histology of the lesion showing extensiveepidermal proliferation with a central crater that is composedof a keratin plug (arrow), compatible with keratoacanthoma(original magnification 40�).
40 C.-J. Feng et al.
1. Introduction
Carcinoma cuniculatum was first described by Aird et al in1954 as epithelioma cuniculatum.1e3 The name is derivedfrom the Latin word cuniculus, meaning “rabbit,” becauseof its rabbit-burrow-like architecture (appearance of thecomplex branching of keratin-filled crypts). It is regarded aseither a low-grade subtype of squamous cell carcinoma or avariant of verrucous carcinoma. It is characterized by aslow-growing, well-differentiated exo- and sometimesendophytic neoplasm that is often locally aggressive butrarely metastatic. Carcinoma cuniculatum most commonlyoccurs on the soles. However, lesions occurring in othercutaneous sites have also been reported, known as cuta-neous verrucous carcinoma.1e5 We are the first to report apatient with carcinoma cuniculatum on the nasal tip,showing the typical histological features of carcinomacuniculatum with the atypical clinical manifestation, withrapid progression, arising from keratoacanthoma. More-over, we review the clinicopathological and differentialdiagnoses of this unusual epithelial neoplasm.
2. Case report
A 74-year-old man presented with a reddish nodule on thenasal tip, exhibiting rapid enlargement within 1 month. Hehad a past history of hypertension under regular medicationcontrol for 6 years and benign prostatic hyperplasia. Hedenied any type of trauma or chronic inflammation in thisregion. He also reported no substantial personal or familyhistory of skin disease. On physical examination, the pa-tient was found to have a 1.5-cm well-marginated,erythematous rubbery nodule with central ulceration onthe nasal tip (Figure 1A). The clinical differential diagnosesincluded deep bacterial or fungal infection, keratoacan-thoma, basal cell carcinoma, and squamous cell carcinoma.
First, an incisional biopsy was performed by ourdermatologist, who suspected pilar sheath acanthoma. Thepatient was then referred to our plastic surgeon for furthersurgical intervention. An excisional biopsy and full-thickness skin graft resurfacing were performed smoothly.Histologic examination revealed hyperkeratosis, para-keratosis, and acanthosis, resulting in pseudoepithelioma-tous hyperplasia compatible with a keratoacanthoma(Figure 1B). However, the resection base margin was notfree. Owing to the benign skin lesion, the patient refusedfurther excision and agreed to regular follow-ups in ouroutpatient clinic. The postoperative wound condition wasnormal. However, rapid local recurrence with a 1.5-cmverrucous mass was found at the original site 1 monthlater (Figure 2). Although the appearance of the mass wasunlike a typical keratoacanthoma, recurrent keratoacan-thoma was suspected. Therefore, the patient underwentfurther excisional biopsy to determine the nature of themass. Reconstruction surgery was not performed until thepathology report was finalized. Histologic examinationrevealed a symmetric tumor consisting of a massively hy-perplastic and papillomatous-folded epidermis with markedhyperkeratosis and parakeratosis. The epithelial strandscontained numerous keratin-filled cysts, formed crypts,and rabbit-burrow-like, keratin-filled sinus formations
(Figure 3A). At deeper levels, the tumor was sharplydemarcated by an intact basement membrane compressingthe underlying collagen tissue. The keratinocytes appearedwell differentiated, without any signs of nuclear atypia.Loss of polarity and horn pearls were absent. However,some parts of the tumor indicated slight evidence of atypia,including nascent focal loss of polarity and nuclear atypiaof the keratinocytes, even though the basement membranein these areas remained intact (Figure 3B). All the featureswere compatible with carcinoma cuniculatum. Thus, wideexcision with 5-mm safe margins and full-thickness skingraft resurfacing were performed smoothly 1 week later.The peripheral and base margins were free. The patientrecovered uneventfully, and no recurrence of the lesionwas reported over a 62-month period of observation(Figure 4).
3. Discussion
Verrucous carcinoma of the skin and mucosa is an uncom-mon low-grade squamous cell carcinoma characterized
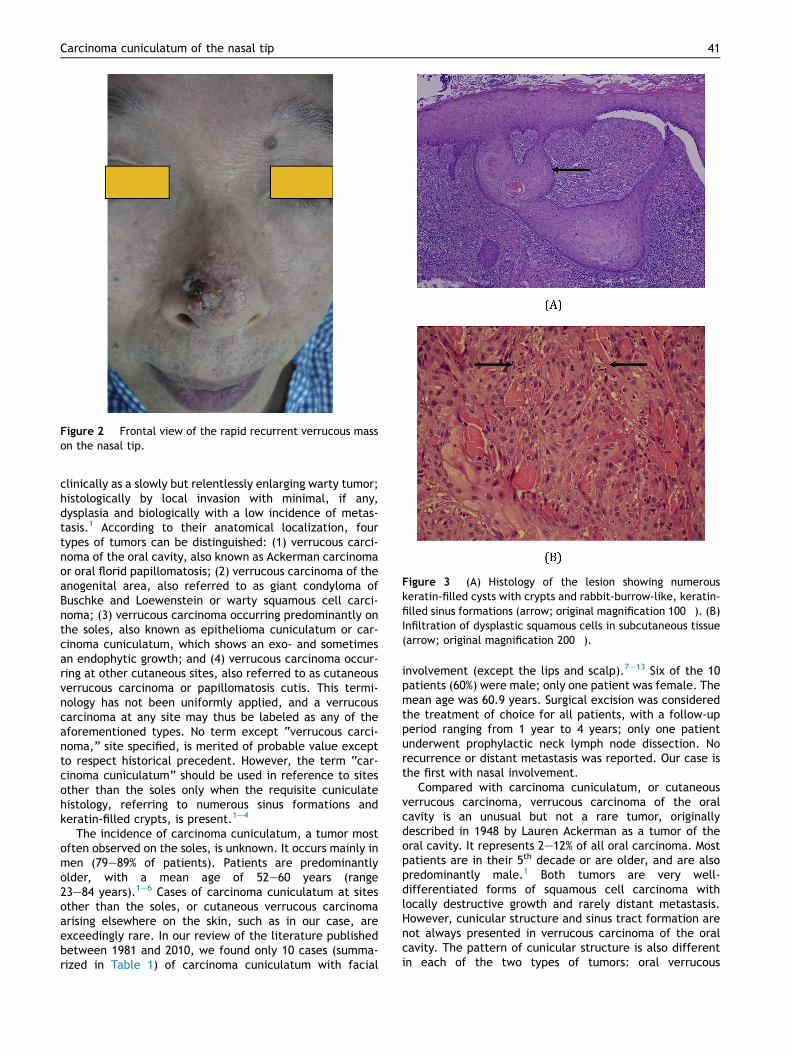
Figure 2 Frontal view of the rapid recurrent verrucous masson the nasal tip.
Figure 3 (A) Histology of the lesion showing numerouskeratin-filled cysts with crypts and rabbit-burrow-like, keratin-filled sinus formations (arrow; original magnification 100�). (B)Infiltration of dysplastic squamous cells in subcutaneous tissue(arrow; original magnification 200�).
Carcinoma cuniculatum of the nasal tip 41
clinically as a slowly but relentlessly enlarging warty tumor;histologically by local invasion with minimal, if any,dysplasia and biologically with a low incidence of metas-tasis.1 According to their anatomical localization, fourtypes of tumors can be distinguished: (1) verrucous carci-noma of the oral cavity, also known as Ackerman carcinomaor oral florid papillomatosis; (2) verrucous carcinoma of theanogenital area, also referred to as giant condyloma ofBuschke and Loewenstein or warty squamous cell carci-noma; (3) verrucous carcinoma occurring predominantly onthe soles, also known as epithelioma cuniculatum or car-cinoma cuniculatum, which shows an exo- and sometimesan endophytic growth; and (4) verrucous carcinoma occur-ring at other cutaneous sites, also referred to as cutaneousverrucous carcinoma or papillomatosis cutis. This termi-nology has not been uniformly applied, and a verrucouscarcinoma at any site may thus be labeled as any of theaforementioned types. No term except “verrucous carci-noma,” site specified, is merited of probable value exceptto respect historical precedent. However, the term “car-cinoma cuniculatum” should be used in reference to sitesother than the soles only when the requisite cuniculatehistology, referring to numerous sinus formations andkeratin-filled crypts, is present.1e4
The incidence of carcinoma cuniculatum, a tumor mostoften observed on the soles, is unknown. It occurs mainly inmen (79e89% of patients). Patients are predominantlyolder, with a mean age of 52e60 years (range23e84 years).1e6 Cases of carcinoma cuniculatum at sitesother than the soles, or cutaneous verrucous carcinomaarising elsewhere on the skin, such as in our case, areexceedingly rare. In our review of the literature publishedbetween 1981 and 2010, we found only 10 cases (summa-rized in Table 1) of carcinoma cuniculatum with facial
involvement (except the lips and scalp).7e13 Six of the 10patients (60%) were male; only one patient was female. Themean age was 60.9 years. Surgical excision was consideredthe treatment of choice for all patients, with a follow-upperiod ranging from 1 year to 4 years; only one patientunderwent prophylactic neck lymph node dissection. Norecurrence or distant metastasis was reported. Our case isthe first with nasal involvement.
Compared with carcinoma cuniculatum, or cutaneousverrucous carcinoma, verrucous carcinoma of the oralcavity is an unusual but not a rare tumor, originallydescribed in 1948 by Lauren Ackerman as a tumor of theoral cavity. It represents 2e12% of all oral carcinoma. Mostpatients are in their 5th decade or are older, and are alsopredominantly male.1 Both tumors are very well-differentiated forms of squamous cell carcinoma withlocally destructive growth and rarely distant metastasis.However, cunicular structure and sinus tract formation arenot always presented in verrucous carcinoma of the oralcavity. The pattern of cunicular structure is also differentin each of the two types of tumors: oral verrucous

Figure 4 Frontal view of the postoperative result at the 62-month follow-up.
42 C.-J. Feng et al.
carcinoma is an undulation from a verrucous surface, butcutaneous verrucous carcinoma descends from a flat sur-face. Other features that differ between the two tumorsrequire further investigation.14
The pathogenesis of carcinoma cuniculatum is still un-known. Human papillomavirus and chemical carcinogens,such as tobacco and betel quid, may play a critical role inthe development of specific tumors.6 Klima et al15
described previous chronic infection and long-standingscar tissue as crucial factors in the pathogenesis of cuta-neous verrucous carcinoma.
Table 1 Our review of the literature published between 1981 a
Authors Year Patient Age (y) Sex Location
Nguyen andMcMarlin8
1984 1 72 Male Right cheek andright lower eyelid
Takematsuet al12
1994 2 60 Male Left cheek
Vico et al13 1997 3 d d ColumellaVandeweyer
et al92001 4 82 Female Preauricular
regionVandeweyer
et al92001 5 64 Male Columella
Gallo et al11 2005 6 d d d
Shimizu et al7 2006 7 29 Male Chin
Shimizu et al7 2006 8 d d ForeheadGonzalez-Perez
et al102009 9 45 Male Left cheek
Gonzalez-Perezet al10
2009 10 74 Male Right temporalregion
FTSG Z full thickness skin graft; STSG Z split thickness skin graft.
At the histological level, all sites of verrucous carcinomaare characterized by a prominent papillomatous configu-ration with hyperkeratosis, parakeratosis, acanthosis,papillomatosis, and granular cell layer vacuolization. Thekeratinocytes show minimal or no dysplasia and no disrup-tion of the basement membrane. Blunt projections of awell-differentiated epithelium surrounded by edematousstroma and chronic inflammatory cells extend into thedermis, forming sinuses that are filled with keratin.1e3 Airdet al described a unique tumor, which they called epithe-lioma cuniculatum or carcinoma cuniculatum, consideringthe characteristic histological features of sinus formationsand keratin-filled crypts, which result in the rabbit-burrow-like architecture of the tumor.3
The differential diagnoses for carcinoma cuniculatuminclude verruca vulgaris, condylomata acuminata, kera-toacanthoma, pseudoepitheliomatous hyperplasia, typicalsquamous cell carcinoma, warty (condylomatous) squamouscell carcinoma, and papillary squamous cell carcinoma.Viral warts and condylomata acuminata do not present anyendophytic zones or significant nuclear atypia and showkeratohyaline granules. They do not usually grow overnumerous years, having a tendency toward spontaneousregression. Keratoacanthoma is never verrucous inappearance and has a rapid self-limited and self-healingcourse. Structurally, its multilocular crater of multi-follicular origin is clearly distinct. Histologically, the giantkeratoacanthoma may appear to be a well-differentiatedsquamous cell carcinoma; however, the prominent intra-cytoplasmic glycogen of the keratoacanthoma usuallyclarifies the distinction.
In the reactive or pseudoepitheliomatous hyperplasia,margins of the proliferating epidermis are often pointed orirregular rather than bulbous, with a more marked inflam-matory infiltrate than a mild-to-moderate one, which isassociated with carcinoma cuniculatum. In addition, thepresence of anaplastic cells suggests the diagnosis ofcutaneous squamous cell carcinoma, and not carcinoma
nd 2010.
Size (cm) Duration Treatment Follow-up Outcome
4 � 4.5 14 y Excision and STSG d d
d 3 y Excision and leftcervical lymphnode dissection
d d
d d d d d
4 � 3 3 mo Excision 1 y Diseasefree
d 1 y Excision 49 mo Diseasefree
d d d d d
8.5 � 8 4 y Excision and FTSG 1 y Diseasefree
d d d d d
2 6 mo Excision 2 y Diseasefree
4 2 y Excision 3 y Diseasefree

Carcinoma cuniculatum of the nasal tip 43
cuniculatum or verrucous carcinoma, even though the fociof conventional squamous cell carcinoma within a verru-cous carcinoma deserve special recognition as a hybridverrucousesquamous cell carcinoma. Therefore, histologicdiagnosis can be difficult. A deep biopsy of the lesion isnecessary to rule out other diagnoses.1e3,16,17
The standard treatments for carcinoma cuniculatum aresurgical excision and the Mohs technique (serial excision formicroscopic analysis), both of which are associated with ahigh cure rate and a low recurrence rate. Determination ofthe appropriate surgical margin in conventional surgicalexcision has often been an area of debate. By contrast,tissue sparing and complete margin control are two of thepotential benefits of the Mohs surgery. When the lesion ison the vital structure or face, Mohs surgery may play asubstantial role in preserving a functional or cosmeticoutcome, as in the case of our patient. Alternative treat-ments include curettage and electrodesiccation, cryosur-gery, alpha-interferon, systemic retinoids, chemotherapyusing methotrexate, bleomycin or 5-fluoruracil, carbon-dioxide laser therapy, and radiotherapy. Controversy per-sists concerning irradiation in managing carcinoma cunicu-latum. Despite reports describing the radiation-associatedanaplastic transformation of the tumor (a risk factor of10.7%), radiation therapy is frequently used in patients withextensive comorbidity that precludes surgery.1e3,16,17
Overall, the prognosis of carcinoma cuniculatum is usu-ally favorable. Typically, the tumor remains indolent forseveral years, but it may extend into the subcutaneoustissue or metastasize. As the course is characterized to beslow but with continuous local growth, morbidity resultsfrom the destruction of local skin and soft tissue and rarelyfrom perineural, muscle, or bone invasion. Painful nonma-lignant lymphadenopathy can be observed with concurrentinfection. The occurrence of distant metastases is rare, andtherefore, mortality is mostly due to local invasion, ratherthan metastatic spread. Recurrence is also rare aftercomplete treatment.1e3,16,17
To our knowledge, the present case, which involvedcarcinoma cuniculatum following keratoacanthoma at thenasal tip, is the first such report in the literature. Aninadequate margin and chronic inflammation after initialresection may cause further malignant change. In addition,balancing an adequate resection margin with an optimalcosmetic outcome is difficult when the tumor is located atthe nasal tip. Mohs surgery may play a substantial role whenthe tumor is located on the vital structure, as in the case ofour patient. It may also result in a lower local recurrencerate.6 However, because of the time-consuming nature ofthe procedure, false negative rate, and shortage of expe-rienced histotechnicians and pathologists, the patientrefused Mohs surgery and chose excisional biopsy to firstdetermine the nature of the tumor, followed by wideexcision with 5-mm safe margins. After wide excision,reconstruction with full-thickness skin graft was performedsmoothly in this patient. This process was undertaken toproduce a lower complication rate and for easier detectionof local recurrence. Reconstruction of the nasal tip is oftena complex process because of limited nearby tissue reser-voirs, highly contoured topography, and a conspicuouslocation. When reconstruction is approached empirically,an algorithm that is based on skin type, defect size, and
location is useful to determine the most appropriate repairfor a given patient. Local flaps, such as the bilobed andnasolabial flaps, have an excellent color and texture matchwith adjacent tissues but are suitable only for small nasaldefects. Other drawbacks of local flaps include a dramaticability to distort the symmetry of the distal nose and a highrisk of pin cushioning if design is not planned appropriately.Defects that exceed 1.5 cm in diameter, especially thosethat involve the entire tip subunit, are most amenable to aregional flap or staged paramedian forehead flap repair. Asthe forehead skin is thicker than the nasal skin, thinning ofthe flap is required. Compared with local or regional flapreconstruction, full-thickness skin grafting has a lowercomplication rate, and yields easier detection of localrecurrence but inferior coverage for cartilage exposure andworse appearance caused by color mismatch and contourdefects.18,19
Finally, early diagnosis and treatment of carcinomacuniculatum are crucial by clinicopathological standards.General clinical awareness of this entity contributes tomore appropriate and timely treatment.
References
1. Schwartz RA. Verrucous carcinoma of the skin and mucosa. JAm Acad Dermatol. 1995;32:1e21.
2. Assaf C, Steinhoff M, Petrov I, et al. Verrucous carcinoma ofthe axilla: case report and review. J Cutan Pathol. 2004;31:199e204.
3. Steffen C. Dermatopathology in historical perspective:epithelioma cuniculatum (Aird). Am J Dermatopathol. 2006;28:451e461.
4. Kruse AL, Graetz KW. Carcinoma cuniculatum: a rare entity inthe oral cavity. J Craniofac Surg. 2009;20:1270e1272.
5. Allon D, Kaplan I, Manor R, Calderon S. Carcinoma cuniculatumof the jaw: a rare variant of oral carcinoma. Oral Surg Oral MedOral Pathol Oral Radiol Endod. 2002;94:601e608.
6. Rudolph R, Zelac DE. Squamous cell carcinoma of the skin.Plast Reconstr Surg. 2004;114:82ee94e.
7. Shimizu A, Tamura A, Ishikawa O. Invasive squamous cell car-cinoma arising from verrucous carcinoma. Recognition of ver-rucous carcinoma of skin as an in situ carcinoma. Eur JDermatol. 2006;16:439e442.
8. Nguyen KQ, McMarlin SL. Verrucous carcinoma of the face.Arch Dermatol. 1984;120:383e385.
9. Vandeweyer E, Sales F, Deraemaecker R. Cutaneous verrucouscarcinoma. Br J Plast Surg. 2001;54:168e170.
10. Gonzalez-Perez R, Trebol I, Arregui A, et al. Verrucous carci-noma of the face: a report of two cases. Actas Dermosifiliogr.2009;100:160e162.
11. Gallo A, Fiorella ML, Simonelli M, Rocca CD, de Vincentiis M.Carcinoma cuniculatum: verrucous carcinoma of the skin of theface. Otolaryngol Head Neck Surg. 2005;133:640.
12. Takematsu H, Watanabe M, Matsunaga J, Ueno H, Tagami H.Verrucous carcinoma of the face with a massive neutrophilinfiltrate. Analysis of leukocyte chemotactic activity in thetumour extract. Clin Exp Dermatol. 1994;19:26e30.
13. Vico P, Nagypal P, Rahier I, Deraemaecker R. Verrucous carci-noma of the nasal septum and columella. Acta Chir Belg. 1997;97:50e51.
14. Kubik MJ, Rhatigan RM. Carcinoma cuniculatum: not a verru-cous carcinoma. J Cutan Pathol. 2012;39:1083e1087.
15. Klima M, Kurtis B, Jordan Jr PH. Verrucous carcinoma of skin. JCutan Pathol. 1980;7:88e98.

44 C.-J. Feng et al.
16. Lozzi GP, Peris K. Carcinoma cuniculatum. CMAJ. 2007;177:249e251.
17. Schein O, Orenstein A, Bar-Meir E. Plantar verrucous carcinoma(epithelioma cuniculatum): rare form of the common wart.IMAJ. 2006;8:885.
18. Konofaos P, Alvarez S, McKinnie JE, Wallace RD. Nasal recon-struction: a simplified approach based on 419 operated cases.Aesthetic Plast Surg. 2015;39:91e99.
19. Stigall L, Zitelli J. Reconstructing the nasal tip. Br J Dermatol.2014;171:23e28.