cardiac pacemakerspart iii
TRANSCRIPT

Cardiac Pace-Makers
Pacemaker Malfunctions, Part III
Salah Atta, MDProfessor of Cardiology,Cardiology Department

Potential Problems Identifiable on an ECG Can Generally Be Assigned to Five Categories:
• Noncapture • Undersensing• Oversensing• No output• (Pseudomalfunctions)

Pacing System Malfunction
Pacing system malfunction includes problems that might arise from any of the components of the system. The following is a description of the common PM malfunctions based on presence or absence of the pacing stimulus:
A) PM Stimuli Present + Loss of Capture
B) PM Stimuli Present + Loss of Sensing
C) PM Stimuli Absent.
D) Too much Pacing.

A) Pacing Stimulus Present with Loss of Capture
Noncapture or loss of capture1-Diagnosis:
Stimulus + NO subsequent paced P or QRS complex
2-Check spike
3-DD from fai lure to sense, and the spike is f ired but fal l in the physiological refractory period.
4-Consider the cause of loss of capture?

5
Noncapture/Failure to Capture
Pacer’s electrical stimulus (pacing) fails to depolarize (capture) the heart. SoPacing is simply unsuccessful at stimulating a contraction
ECG shows properly timed pacer spikes but no cardiac response
↓ CO occurs↓ Investigation: X-ray chest , PM check by
programmer, full lab work.

Problems with PacemakersFailure to Capture
Causes: • Threshold rise.• Lead dislodgement• Lead fracture

Less Common Causes of Noncapture May Include:
• Twiddler’s syndrome• Electrolyte abnormalities e.g.
hyperkalemia• Myocardial infarction• Drug therapy• Battery depletion• Exit block

B) Pacing Stimulus Present whenever unexpected Undersensing
1-Diagnosis of Undersensing:
Spontaneous P or QRS complex, followed by a Stimulus (which should not have been fired)
2-Check Set Sensit ivity.
3-Consider the Cause of Undersensing?
4-Increase Sensitivity Temporari ly Til l Cause is Treated .

9
Undersensing: Failure to sense
Pacer fails to detect an intrinsic rhythm
Paces unnecessarily (overpacing)
Patient may feel “extra beats”
If an unneeded pacer spike falls in the latter portion of T wave, dangerous tachyarrhythmias or V fib may occur (R on T).

non-sensed R-waves
Ventricular Undersensing

Causes of UndersensingDislodged Lead Insulation BreakToo low sensitivity
Problem Solving Program the sensitivity to a lower number
i.e increase the sensitivity.

C) Pacing Stimuli Absent
A
B

Problems with PacemakersFailure to Pace (Pauses)
Causes: • Oversensing• Battery failure• Internal insulation failure• Conductor coil fracture
Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, 7th ed., 2005.

C) Pacing Stimuli Absent
1-Diagnosis: NO pacing stimuli + NO P or QRS complex
2-Consider one of three possible system malfunctions:
1-Oversensing, 2-Open Circuit, 3-Defective Battery
3-DD between the three possible system malfunctions:
Magnet->stimulus->P or QRS=Oversensing
Magnet->no stimulus, or stimulus->No P or QRS=Open Circuit
4-Consider causes and manage accordingly

Oversensing
• Definition : The sensing of events other than P or R-
waves by the pacemaker circuit e.g T wave, A spiKe, Myopotentials
Detects extraneous signals such as those produced by electrical equipment or the activity of skeletal muscles (tensing, flexing of chest muscles)
So inhibits pacing as it would a true heart beat so causing pauses or underpacing.

Causes of Oversensing
• Too high sensitivity, • Insulation Break, Intermittent Lead
Fracture.• Myopotentials. -EMI.
• Program sensitivity to a higher number (↓sensitivity).
• Change polarity to bipolar
• Program the refractory period longer
Problem Solving

17
Pacer Failure
A. Earlyelectrode displacement/breakage
B. Failure > 6 monthsPremature battery depletion
Faulty pulse generator

Possible problems with DDD pacing1. Tracking of a too fast atrial rate may cause
serious ventricular response (e.g in case of atrial tachycardia, atrial flutter or atrial fibrillation) if no mode switch and high upper tracking rate.
2. Pacemaker mediated tachycardia.3. Ventricular inhibition 2ry to atrial pacing
may cause asystole (Cross talk).4. Others.
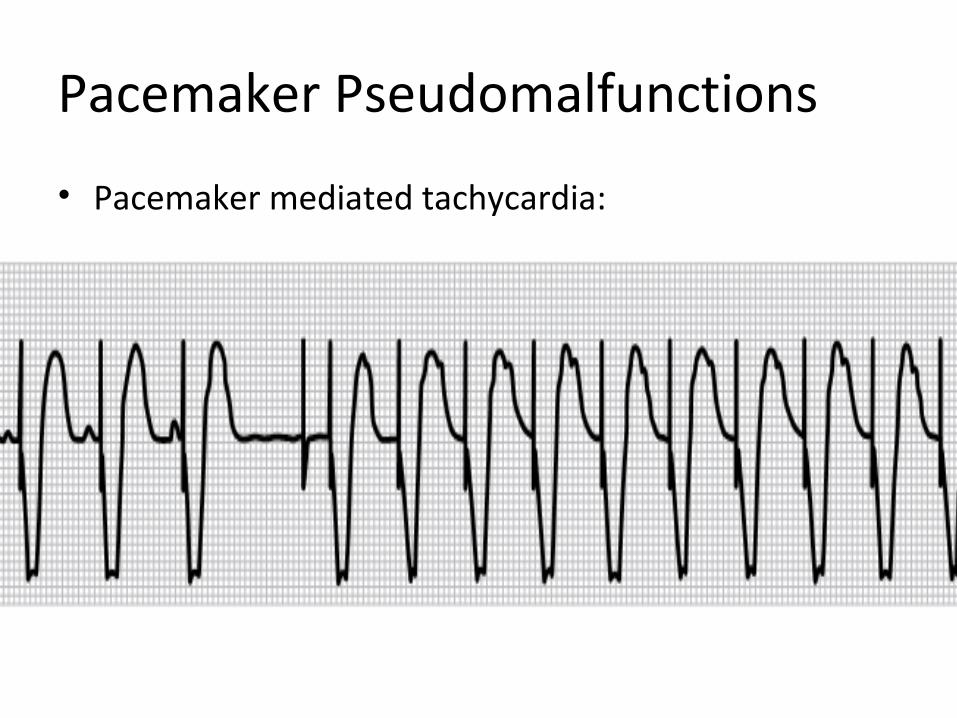
Pacemaker Pseudomalfunctions
Pacemaker Pseudomalfunctions
• Pacemaker mediated tachycardia:

Pacemaker Mediated Tachycardia (PMT)
Rapid ventricular pacing due to RETROGRADE CONDUCTION, sensed by the PM and responding by V pacing and
so on, most commonly at exactly the upper rate limit.

Retrograde Conduction• Propagation of an impulse from the ventricle back
to the atrium, Also known as VA conduction.
• 60 % of the population have the ability to conduct retrogradely
• 33 % of patients with complete heart block have the ability to conduct retrogradely
• Average retrograde conduction time= 235ms ± 55 ms

AVD
PVARP PVARP
Retrograde P waves
PVARP PVARP
PVC
Pacemaker Mediated Tachycardia

AVD
PVARP AREPVARP
AVD
PVARP
Retrograde P wavePVC
Prolong PVARP or Atrial Refractory Extension after a PVC
Pacemaker Mediated TachycardiaProblem Solving

Crosstalk• Sensing of the atrial output pulse by the ventricular sense
amplifier
• Inappropriate inhibition of the ventricular pacing due to sensing of the atrial output pulse by the ventricular sense amplifier.
• Crosstalk is only seen in dual chamber or biventricular pacemakers. Also called crosstalk inhibition, far-field sensing, or self-inhibition.

Problems with PacemakersFailure to Pace
Causes: • Crosstalk
Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, 7th ed., 2005.
Management by programming a ventricular blanking period

Factors Affecting Crosstalk
• Atrial pulse amplitude and pulse width
• Ventricular sensitivity
• Anatomical location of atrial and ventricular electrodes

Managing Crosstalk
• Atrial Pulse Energy
• Ventricular Sensitivity
• Ventricular Blanking Period

Ventricular Blanking Period (VB)
• A short (21-75 ms) period that begins simultaneously with an atrial output pulse and during which the ventricular sense amplifier is totally blind to incoming signals but it is modifiable only by the manifacturer.
AV delay
VB

Fusion and Pseudofusion beats

PM behaviour above ULI Pacemaker Wenckebach

Mode Switchingfrom DDD to DDI or VVI

Implantable Cardioverter Defibrillator (ICD)

ICD Implantation
• Secondary prevention: Prevention of SCD in patients with prior VF or sustained VT.
• Primary prevention: Prevention of SCD in individuals without a h/o VF or sustained VT.
Indications For ICD
• VF/sustained unstable VT not in the setting of a completely reversible cause.
• LVEF ≤ 35%, CHF NYHA class II, III.• Ischemic dilated cardiomyopathy, LVEF ≤ 40%,
NSVT and inducible sustained VT.• Syncope, LV dysfunction, inducible sustained VT.• High risk patients with: hypertrophic
cardiomyopathy, LQT syndrome, RV dysplasia, Brugada syndrome

• Impedance measurementImpedance measurement : 300 - 1000 : 300 - 1000 ohms.... calculated / displayedohms.... calculated / displayed
• SVC coil , RV coil impedence: 30-100 VSVC coil , RV coil impedence: 30-100 V• Sensing threshold (localy sensed intrinsic Sensing threshold (localy sensed intrinsic
electrogram)electrogram)• Amplitude (Minimum : “P” - 2mV , “R” - 5mV)Amplitude (Minimum : “P” - 2mV , “R” - 5mV)
• Pacing thresholdPacing threshold• (Measured amplitude at 0.5 ms.)(Measured amplitude at 0.5 ms.)• Paced rate > = 20 ppm above spontaneous ratePaced rate > = 20 ppm above spontaneous rate• Decrement variable output : Threshold < 1-1.5V @ 0.5ms.Decrement variable output : Threshold < 1-1.5V @ 0.5ms.
ICD ImplantationImplantation MeasurementsMeasurements

Dual Chamber ICD

Ellenbogen K A, 2007Ellenbogen K A, 2007

38
Shock
ICD interrogation revealed the following:
One shock was delivered, as above, with 9 other aborted shocks for long non-sustained VT (asymptomatic).

CRT Indications
• Age > 18 years, Sinus rhythm, EF less than 35%, NYHA class III-IV heart failure despite optimal medical treatment for at least 3 months.
• Indicator of dyssynchrony either:
Standard electrical criteria in the form of Wide QRS complex ≥130 ms, left bundle branch block (LBBB) with echo evidence of dyssynchrony in group 1 (or)

ECG of a wide QRS complex case
Before CRT implantation

LV lead position

After CRT implantation

Echo appearance before and 24 hours after CRT

FMR Before CRT implantation
24 hours after CRT implantation

Example 1
Atrial sensed, ventricular paced
Consistent with DDD or VDD pacing in VAT mode
The Alan E. Lindsay ECG Learning Center ; http://medstat.med.utah.edu/kw/ecg/

Example 2
Atrial paced
Consistent with AAI or DDD
The Alan E. Lindsay ECG Learning Center ; http://medstat.med.utah.edu/kw/ecg/

Example 3
Failure to Pace
The Alan E. Lindsay ECG Learning Center ; http://medstat.med.utah.edu/kw/ecg/

Example 4
Failure to Sense
The Alan E. Lindsay ECG Learning Center ; http://medstat.med.utah.edu/kw/ecg/

Thank you