cardiac ultrasound in emergency medicine anthony j. weekes md, rdms sarah a. stahmer md for the saem...
TRANSCRIPT

Cardiac Ultrasound in Cardiac Ultrasound in Emergency MedicineEmergency Medicine
Anthony J. Weekes MD, RDMSSarah A. Stahmer MD
For the SAEM US Interest Group

Primary IndicationsPrimary Indications
Thoraco-abdominal trauma
Pulseless Electrical Activity
Unexplained hypotension
Suspicion of pericardial
effusion/tamponade

Secondary IndicationsSecondary Indications
Acute Cardiac Ischemia
Pericardiocentesis
External pacer capture
Transvenous pacer placement

Main Clinical QuestionsMain Clinical Questions
What is the overall cardiac wall motion?
Is there a pericardial effusion?

Cardiac probe selectionCardiac probe selection
Small round footprint for scan between ribs
2.5 MHz: above average sized patient
3.5 MHz: average sized patient
5.0 MHz: below average sized patient or child
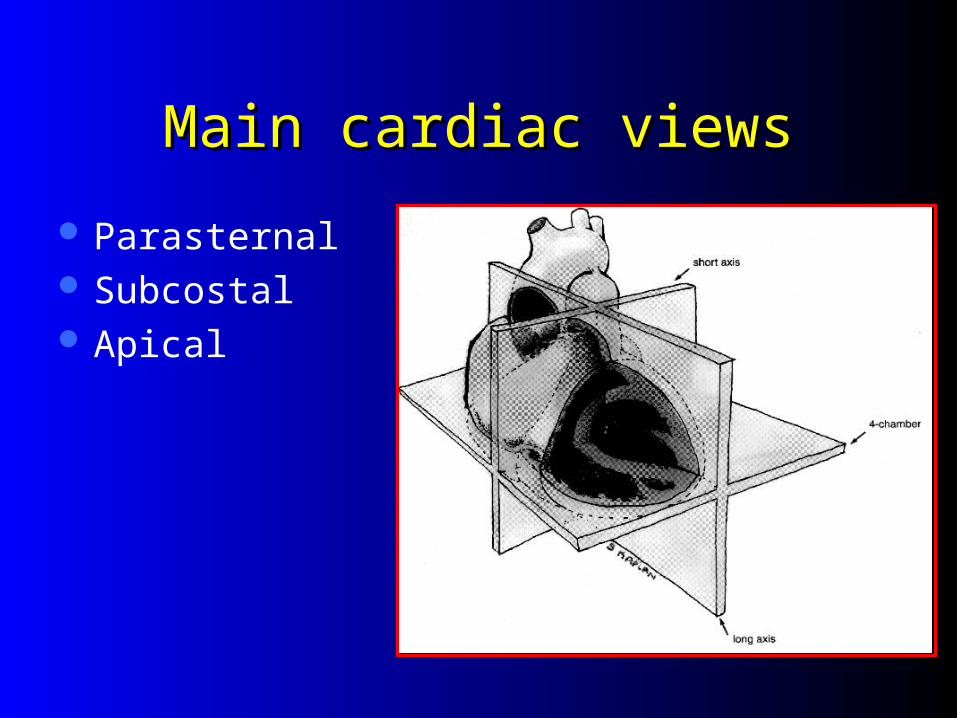
Main cardiac viewsMain cardiac views
Parasternal Subcostal Apical

Wall MotionWall Motion
NormalHyperkineticAkineticDyskinetic: may fail
to contract, bulges outward at systole
Hypokinetic

OrientationOrientation
Subcostal or subxiphoid viewBest all around imaging windowGood for identification of:
– Circumferential pericardial effusion– Overall wall motion
Easy to obtain – liver is the acoustic window\

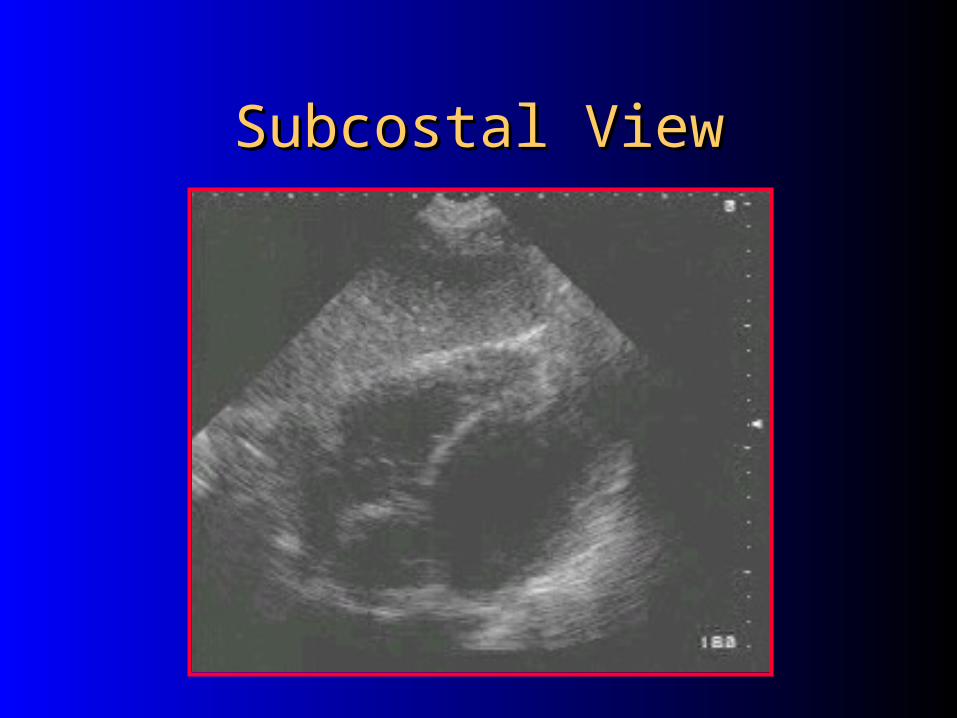
Subcostal ViewSubcostal View
Most practical in trauma setting
Away from airway and neck/chest procedures

Subcostal ViewSubcostal View
Liver as acoustic window
Alternative to apical 4 chamber view

Subcostal ViewSubcostal View
Subcostal ViewSubcostal View

Subcostal ViewSubcostal View
Angle probe right to see IVC
Response of IVC to sniff indicates central venous pressure
No collapse– Tamponade– CHF– PE– Pneumothorax

Parasternal ViewsParasternal Views
Next best imaging windowGood for imaging LVComparing chamber sizesLocalized effusionsDifferentiating pericardial from pleural
effusions

Parasternal Long AxisParasternal Long Axis
Near sternum3rd or 4th left intercostal spaceMarker pointed to patient’s right
shoulder (or left hip if screen is not reversed for cardiac imaging)
Rotate enough to elongate cardiac chambers

Parasternal Long AxisParasternal Long Axis

Parasternal Long Axis ViewParasternal Long Axis View

Parasternal Short Axis Parasternal Short Axis
Obtained by 90° clockwise rotation of the probe towards the left shoulder (or right hip)
Sweep the beam from the base of the heart to the apex for different cross sectional views

Parasternal Short Axis ViewParasternal Short Axis View

Parasternal Short AxisParasternal Short Axis

Apical ViewApical View
Difficult view to obtainAllows comparison of ventricular
chamber sizeGood window to assess septal/wall
motion abnormalities

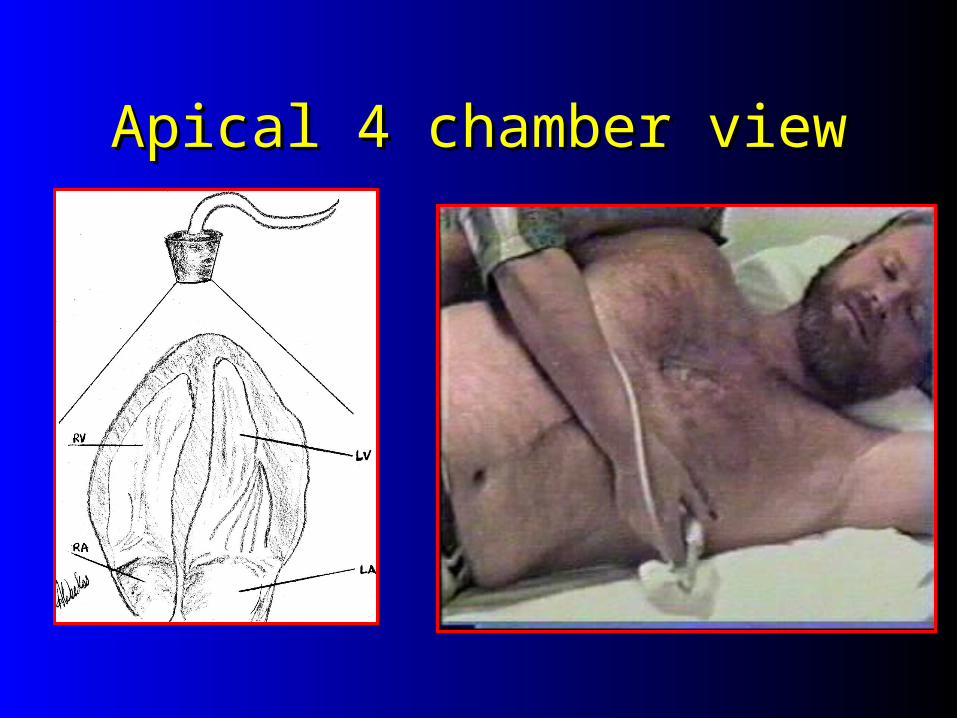
Apical ViewsApical Views
Patient in left lateral decubitus position
Probe placed at PMI
Probe marker at 6 o’clock (or right shoulder)
4 chamber view

Apical 4 chamber viewApical 4 chamber view Marker pointed to
the floor Similar to
parasternal view but apex well visualized
Angle beam superiorly for 5 chamber view
Apical 4 chamber viewApical 4 chamber view

Apical 2 chamber viewApical 2 chamber view
Patient in left lateral decubitus position
Probe placed at PMI
Probe marker at 3 o’clock
2 chamber view

Apical 2 chamber viewApical 2 chamber view Good look at inferior and anterior walls

Apical 2 chamber viewApical 2 chamber view
From apical 4, rotate probe 90° counterclockwise
Good view for long view of left sided chambers and mitral valve

Abnormal findingsAbnormal findings
Pericardial Effusion

Case PresentationCase Presentation
45 year old male presents with SOB and dizziness for 2 days. He has a long smoking history, and has complained of a non-productive cough for “weeks”
Initial VS are BP 88/palp, HR 140PE: Neck veins are distendedChest: Clear, muffled heart soundsBedside sonography was performed


Echo free space around the heartEcho free space around the heart
Pericardial effusionPleural effusionEpicardial fat (posterior and/or
anterior)Less common causes:
– Aortic aneurysm– Pericardial cyst– Dilated pulmonary artery

Size of the Pericardial Size of the Pericardial EffusionEffusion
Not PreciseSmall: confined to posterior space,
< 0.5cmModerate: anterior and posterior,
0.5-2cm (diastole)Large: > 2cm

Pericardial Fluid: Subcostal Pericardial Fluid: Subcostal

Clinical features of Clinical features of Pericardial effusionPericardial effusion
Pericardial fluid accumulation may be clinically silent
Symptoms are due to:– mechanical compression of adjacent
structures– Increased intrapericardial pressure

Pericardial Pericardial Effusion:AsymptomaticEffusion:Asymptomatic
Up to 40% of pregnant womenChronic hemodialysis patients
– one study showed 11% incidence of pericardial effusion
AIDSCHFHypoproteinemic states

Symptoms of Pericardial Symptoms of Pericardial EffusionEffusion
Chest discomfort (most common)Large effusions:
– Dyspnea– Cough– Fatigue– Hiccups– Hoarseness– Nausea and abdominal fullness

Cardiac TamponadeCardiac Tamponade
Increased intracardiac pressures
Limitation of ventricular diastolic filling
Reduction of stroke volume and cardiac output

Ventricular collapse in Ventricular collapse in diastolediastole

TamponadeTamponade

HypotensionHypotension

Abnormal findingsAbnormal findings
Is the cause of hypotension cardiac in
etiology?
Is it due to a pericardial effusion?
Is is due to pump failure?

Unexplained HypotensionUnexplained Hypotension
Cardiogenic shock – Poor LV contractility
Hypovolemia– Hyperdynamic ventricules
Right ventricular infarct/large pulmonary embolism– Marked RV dilitation/hypokinesis
Tamponade– RV diastolic collapse

Cardiogenic shockCardiogenic shock
Dilated left ventricle
Hypocontractile walls

HypovolemiaHypovolemia
Small chamber filling size
Aggressive wall motion
Flat IVC or exaggerated collapse
with deep inspiration

Massive PE or RV infarctMassive PE or RV infarct
Dilated Right ventricle
RV hypokinesis Normal Left
ventricle function Stiff IVC

Case presentation ? overdose Case presentation ? overdose
27 yo f brought in with “passing out” after night of heavy drinking.
Complaining of inability to breathe!PE: Obese f BP 88/60 HR 123 Ox
78% Chest: clearExt: No edemaBedside sonography was performed



Chest pain then codeChest pain then code
55 yo male suffered witnessed Vfib arrest in the ED
ALS protocol - restoration of perfusing rhythm
Persistant hypotensionED ECHO was performed



R sided leads

Non Traumatic Non Traumatic ResuscitationResuscitation

Direct VisualizationDirect VisualizationIs there effective myocardial
contractility?– Asystole– Myocardial “twitch”– Hypokinesis– Normal
Is there a pericardial effusion?

ECHO in PEAECHO in PEA
Perform ECHO during “quick look” and in pulse checks
Change management based on “positive” findings
Pericardial tamponade– Pericardiocentesis
Hyperdynamic cardiac wall motion– Volume resuscitate

ECHO in PEAECHO in PEA
RV dilatation– Hypoxic?? – Likely PE– ECG – IMI with RV infarct?
Profound hypokinesis– Inotropic support
Asystole– Follow ACLS protocols (for now)– Early data suggesting poor prognosis

ECHO in PEAECHO in PEA
False positive cardiac motion
– Transthoracic pacemaker
– Positive pressure ventilation

Case presentationCase presentation
Morbidly obese female with severe asthma Intubated for respiratory failure Subcutaneous emphysema developed Bilateral chest tubes placed Persistent hypotension at 90/palp Dependent mottling noted ECHO was performed

Ineffective cardiac Ineffective cardiac contractionscontractions

Optimizing PerformanceOptimizing Performance
Assessing capture by transthoracic pacemaker
Pericardiocentesis
Transvenous pacemaker placement

Optimizing PerformanceOptimizing Performance
Assessment of capture by transthoracic pacemaker
Ettin D et al: Using ultrasound to determine external pacer capture JEM 1999

Case PresentationCase Presentation
70 yo f collapsed in lobby. She was brought into the ED apneic, hypotensive. She was quickly intubated and volume resuscitation begun.
VS: BP 80/50 HR 50 Afebrile Physical exam : Thin, minimally responsive f.
Clear lungs, nl heart sounds, abdomen slightly distended with decreased bowel sounds. No HSM, ? Pelvic mass
ECG: SB, LVH, no active ischemia
Clinical questions?Clinical questions?
Why is she hypotensive?Volume loss
?Ruptured AAAPump failureBedside sonography was performed
while we were waiting for the “labs”

Increase HR with PM “on”Increase HR with PM “on”

What did this tell us?What did this tell us?
Normal wall motion
No pericardial/pleural effusion
Good capture with the transthoracic PM

Asystole w/ Transthoracic PMAsystole w/ Transthoracic PM

Optimizing performance Optimizing performance
Pericardiocentesis– Standard of care by cardiology/CT surgery
to use ECHO to guide aspiration

US Guided- US Guided- PericardiocentesisPericardiocentesis Subcostal approach
– Traditional approach– Blind– Increased risk of injury to liver, heart
Echo guided– Left parasternal preferred for needle entry
or…– Largest area of fluid collection adjacent to
the chest wall

Large pericardial effusionLarge pericardial effusion

TechniqueTechnique

Optimizing performanceOptimizing performance
Placement of transvenous pacemakerAguilera P et al: Emergency
transvenous cardiac pacing placement using ultrasound guidance. Ann Emerg Med 2000

Untimely end Untimely end
30 yo brought in after he “fell out”Ashen m with no spontaneous
respirationsVS: No pulse, agonal rhythm on monitorIntubated/CPRTransvenous pacemaker placed, no
capture.ECHO showed


Penetrating Chest TraumaPenetrating Chest Trauma

Penetrating Cardiac TraumaPenetrating Cardiac Trauma
Physician’s ability to determine whether there is a hemodynamically significant effusion is poor
Beck’s Triad – Dependent on patient cardiovascular status– Findings are often late
Determinants of hemodynamic compromise– Size of the effusion– Rate of formation

Penetrating Cardiac InjuryPenetrating Cardiac InjuryEmergency department
echocardiography improves outcome in penetrating cardiac injury.
Plummer D et al. Ann Emerg Med. 1992
28 had ED echo c/w 21 without ED echo Survival: 100% in echo, 57.1% in nonecho Time to Dx: 15 min echo, 42 min nonecho

Penetrating Cardiac InjuryPenetrating Cardiac Injury
The role of ultrasound in patients with possible penetrating cardiac wounds: a prospective multicenter study.
Rozycki GS: J Trauma. 1999
Pericardial scans performed in 261 patients Sensitivity 100%, specificity 96.9% PPV: 81% NPV:100% Time interval BUS to OR: 12.1 +/- 5.9 min

Emergency Department Echocardiography Improves Outcome in Penetrating Cardiac Injury
Plummer D, et al. Ann Emerg Med 21:709-712, 1992.
“Since the introduction of immediate ED two-dimensional echocardiography, the time to diagnosis of penetrating cardiac injury has decreased and both the survival rate and neurologic outcome of survivors has improved.”
Penetrating Cardiac TraumaPenetrating Cardiac Trauma

Stab wound to the chestStab wound to the chest

Echocardiographic signs of rising intrapericardial pressure– Collapse of RV free walls– Dilated IVC and hepatic veins
Goal: Early detection of pericardial effusion– Develops suddenly or discretely– May exist before clinical signs develop
Salvage rates better if detected before hypotension develops
Penetrating Cardiac TraumaPenetrating Cardiac Trauma

Technical ProblemsTechnical Problems
Subcutaneous airPneumopericardiumMechanical ventilation Scanning limited by:
– Pain/tenderness– Spinal immobilization– Ongoing procedures

Technical Problems Technical Problems
Narrow intercostal spacesObesityMuscular chest COPDCalcified rib cartilagesAbdominal distention

Sonographic PitfallsSonographic Pitfalls
Pericardial versus pleural fluid
Pericardial clot
Pericardial fat

Pericardial or Pleural FluidPericardial or Pleural FluidLeft parasternal long axis:
– Pericardial fluid does not extend posterior to descending aorta or left atrium
Subcostal: – No pleural reflection between liver and R
sided chambers– A pleural effusion will not extend between
to RV free wall and the liver

Pleural and Pericardial fluidPleural and Pericardial fluid

Pleural effusionPleural effusion

Blunt Cardiac TraumaBlunt Cardiac Trauma
Cardiac contusion
Cardiac rupture
Valvular disruption
Aortic disruption/dissection
Blunt Cardiac TraumaBlunt Cardiac Trauma
Pericardial effusionAssess for wall motion abnormality
– RV dyskinesis (takes the first hit)Assess thoracic aorta:
– Hematoma– Intimal flap– Abnormal contour
Valvular dysfunction or septal rupture

Cardiac ContusionCardiac Contusion
Akinetic anterior RV wall
Small pericardial effusion
Diminished ejection fraction

RV ContusionRV Contusion

Blunt Cardiac TraumaBlunt Cardiac Trauma
Assess thoracic aorta– Hematoma– Intimal flap– Abnormal contour– Requires TEE and expertise!
Valvular dysfunction or septal rupture– Requires expertise beyond our scope

SummarySummary
Bedside ECHO can help assess:– Overall cardiac wall motion– Identify clinically significant pericardial effusions
Useful in the assessment of the patient with:– Unexplained hypotension– Dyspnea– Thoracic trauma