cardio pulmonary resuscitation
TRANSCRIPT
Cardio-pulmonary resuscitation
Associate professorAhmed Elmadana
Dept. Anesthesiology and Intensive Care Medicine DSMA. 2013
http://www.erc.edu/index.php/guidelines_download_2005/en/

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
History of the resuscitation
The history of resuscitation comprises centuries. Else in 1543 year Vesalius described artificial ventilation of lungs with cycled positive pressure, however that program which can be called by cardiopulmonary resuscitation (CPR), was formed around the middle of XX century and up to the present time have not principle changes.

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
History of the resuscitationyears scientist Action
1513 Vesalius Artificial ventilation of lungs with cycled positive pressure
1530 Paracelsus Artificial ventilation by the forge furs
1878 R.Boehm (Germany) Non-direct massage of heart in animals
1892 Maass Non-direct massage of heart in humans
1900 J.L.Prevost, F.Batelli First experience of the electrical defibrillation in dogs
1901 K.Igelsrud (Norvey) Direct massage of heart in surgical patient
1906 G.V.Crile, D.H.Dolley Using of epinephrine in resuscitation in animals
1911 R.Drager First automatic lungs ventilator
1936 V.A.Negovsky Scientific justification of the possibility resuscitation of life.
1938-1947 N.L.Gurvich On- skin (external) defibrillation in animals
1947 C.S.Beck First direct (internal) defibrillation in patient
1956 P.M.Zoll First external defibrillation in human
1956 V.A.Negovsky First Intensive Care and Reanimation Unit (hospital named after Botkin, Moskow)
1958 P.Safar First Intensive Care Unit in USA
1961 P.Safar Complex of the cardiopulmonary resuscitation
1966 P.Safar Scientific justification of the importance of brain resuscitation

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
Definitions: life and death
There is no universal definition of life. To define life in unequivocal terms is still a challenge for scientists.
Life is a state of matter that distinguishes living organisms from non-living objects, such as non-life, and dead organisms.
Living organisms are capable of growth and reproduction, some can communicate and many can adapt to their environment through changes originating internally.
Death is the termination of the biological functions that define living organisms: homeostasis, metabolism, adaptation, response to stimuli, growth, reproduction, organization and other.
Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
Definitions: clinical, biological and social death
Clinical death is the termination of the biological functions with abilities to its recovery.
Biological death is the unrecoverable termination of biological function.
Social death is the state, that function of the central nervous system is terminated unrecoverable, but the heart still beating.

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
Demographics
Ischemic heart disease is the leading cause of death in the world. Sudden cardiac arrest is responsible for more than 60% of adult deaths from coronary heart disease. Based on data from Scotland and from five cities in other parts of Europe, the annual incidence of resuscitation for out-of-hospital cardiopulmonary arrest of cardiac etiology is 49.5-66 per 100,000 population.
The Scottish study includes data on 21,175 out-of-hospital cardiac arrests, and provides valuable information on etiology. The incidence of in-hospital cardiac arrest is difficult to assess because it is influenced heavily by factors such as the criteria for hospital admission and implementation of a do-not-attempt-resuscitation (DNAR) policy.
In a general hospital in the UK, the incidence of primary cardiac arrest (excluding those with DNAR and those arresting in the emergency department) was 3.3/1000 admissions; 21 using the same exclusion criteria, the incidence of cardiac arrest in a Norwegian University hospital was 1.5/1000 admissions.

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
Signs of the clinical death
Basic signs of the Clinical death: absence of pulse in coronary arteries of
victim absence of the breath of victim expansion of pupils
Additional signs of the Clinical death: No consciousness Pale or cyan color of victim’s skin Single convulsive reductions Absence of muscles tone and reflexes

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
Times limits for resuscitation
Diagnosis of clinical death must be identified as quick as possible!
This is very important because clinical death is limited 3, max 5 minute, but even in these limits – if we start resuscitation earlier, victim more chances
have for restore.
3 minute
34% 17%
Car
diac
arr
est

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
Contra-indications for resuscitation
1. Offensive of death because of exhausting disease, if all of modern methods of treatment are already utilized and death is not sudden, but only as continuation of dying.
2. Offensive of death because of incurable disease (cancer in terminal stage; trauma or stroke, not consonant with life).
3. Offensive of death for patients with initially heavy senile dementia.4. Patients which legalized the refuse of resuscitation before critical
illness.5. If it is exactly known that the stop of heart lasts more than 25
minutes at normothermia.6. If the signs of biological death is presence.

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
Signs of biological death
Eyes signs: softening influence of eyeballs (symptom –
“cats eye”) drying out of cornea dimness of cornea
Body signs: a spots of corpse a corpse becoming numb smoothing of body temperature with an
environment temperature

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
The Chain of Survival
The actions linking the victim of sudden cardiac arrest with survival are called the Chain of Survival. They include early recognition of the emergency and activation of the emergency services, early CPR, early defibrillation and early advanced life support.
Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
Complex cardiopulmonary and cerebral resuscitation
by P.SafarI stage – Basic life support (an elementary life support)
A.Air way open (renewal and control of respiratory tracts)
B.Breathe for victim (an artificial ventilation)C.Circulation his blood (an artificial blood circulation)
II stage – Advanced life supportD. Drug (a medicinal therapy of the cardiac arrest)E. Diagnostic of the kind of blood circulation stoppingF. Defibrillation
III stage – Protracted life supportG. Diagnostic of the “brain death”H. Treatment of the neurological and cognitive
dysfunctionI. Intensive care of violations and complications

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
I stage – Basic life support (BLS)

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
I stage – Basic life support (BLS)
BLS consists of the following sequence of actions:1.Make sure you, the victim and any bystanders are safe.2.Check the victim for a response. Gently shake his shoulders and ask loudly: ‘‘Are
you all right?’’3.a) If he responds:
• leave him in the position in which you find him provided there is no further danger• try to find out what is wrong with him and get help if needed• reassess him regularlyb) If he does not responds:• shout for help• turn the victim onto his back and then open the airway using head tilt and chin lift
4.Keeping the airway open, look, listen and feel for normal breathing:• Look for chest movement.• Listen at the victim’s mouth for breath sounds.• Feel for air on your cheek.
5.a) If he is breathing normally:• turn him into the recovery position (see Below)• send or go for help/call for an ambulance• check for continued breathingb) If he is not breathing normally:• send someone for help or, if you are on your own, leave the victim and alert the ambulance service; return and start chest compression

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
I stage – Basic life support (BLS)
The recovery position
Look listen and feel for normal
breathing
Shout for helpCheck the victim for a response
Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
I stage – Basic life support (BLS)
BLS consists of the following sequence of actions (continue):6. a) Combine chest compression with rescue breaths.
• After 30 compressions open the airway again using head tilt and chin lift.• Pinch the soft part of the nose closed, using the index finger and thumb of your hand on the forehead.• Allow the mouth to open, but maintain chin lift.• Take a normal breath and place your lips around his the mouth, making sure that you have a good seal.• Blow steadily into the mouth while watching for the chest to rise, taking about 1 s as in normal
breathing; this is an effective rescue breath.• Maintaining head tilt and chin lift, take your mouth away from the victim and watch for the chest to fall
as air passes out.• Take another normal breath and blow into the victim’s mouth once more, to
achieve a total of two effective rescue breaths. Then return your hands without delay to the correct position on the sternum and give a further 30 chest compressions.
• Continue with chest compressions and rescue breaths in a ratio of 30:2.• Stop to recheck the victim only if he starts breathing normally; otherwise do not interrupt resuscitation.
If your initial rescue breath does not make the chest rise as in normal breathing, then before your next attempt:
• check the victim’s mouth and remove any obstruction• recheck that there is adequate head tilt and chin lift• do not attempt more than two breaths each time before returning to chest
compressions

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
I stage – Basic life support (BLS)

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
I stage – Basic life support (BLS)
BLS consists of the following sequence of actions (continue):6. a) Combine chest compression with rescue breaths.
• After 30 compressions open the airway again using head tilt and chin lift.• Pinch the soft part of the nose closed, using the index finger and thumb of your hand on the forehead.• Allow the mouth to open, but maintain chin lift.• Take a normal breath and place your lips around his the mouth, making sure that you have a good seal.• Blow steadily into the mouth while watching for the chest to rise, taking about 1 s as in normal
breathing; this is an effective rescue breath.• Maintaining head tilt and chin lift, take your mouth away from the victim and watch for the chest to fall
as air passes out.• Take another normal breath and blow into the victim’s mouth once more, to
achieve a total of two effective rescue breaths. Then return your hands without delay to the correct position on the sternum and give a further 30 chest compressions.
• Continue with chest compressions and rescue breaths in a ratio of 30:2.• Stop to recheck the victim only if he starts breathing normally; otherwise do not interrupt resuscitation.
If your initial rescue breath does not make the chest rise as in normal breathing, then before your next attempt:
• check the victim’s mouth and remove any obstruction• recheck that there is adequate head tilt and chin lift• do not attempt more than two breaths each time before returning to chest
compressions

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
I stage – Basic life support (BLS)
BLS consists of the following sequence of actions (continue):6. b) Chest-compression-only CPR may be used as follows.
• If you are not able or are unwilling to give rescue breaths, give chest compressions only.
• do not attempt more than two breaths each time before returning to chest compressions.
• If chest compressions only are given, these should be continuous, at a rate of 100 min−1.
• Stop to recheck the victim only if he starts breathing normally; otherwise do not interrupt resuscitation.
7. Continue resuscitation until• qualified help arrives and takes over• the victim starts breathing normally• you become exhausted

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
I stage – Basic life support (BLS)Risk to the rescuer
The safety of both rescuer and victim are paramount during a resuscitation attempt. There have been few incidents of rescuers suffering watch for his chest to fall as air comes out adverse effects from undertaking CPR, with only isolated reports of infections such as tuberculosis and severe acute respiratory distress syndrome. Transmission of HIV during CPR has never been reported. There have been no human studies to address the effectiveness of barrier devices during CPR; however, laboratory studies have shown that certain filters, or barrier devices with one-way valves, prevent oral bacterial transmission from the victim to the rescuer during mouth-to-mouth ventilation. Rescuers should take appropriate safety precautions where feasible, especially if the victim is known to have a serious infection, such as TB or SARS. During an outbreak of a highly infectious condition such as SARS, full protective precautions for the rescuer are essential.

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
I stage – Basic life support (BLS)
Opening the airway
The jaw thrust is not recommended for lay rescuers because it is difficult to learn and perform and may itself cause spinal movement. Therefore, the lay rescuer should open the airway using a head tilt-chin lift maneuver for both injured and noninjured victims.

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
I stage – Basic life support (BLS)Opening the airway
“Triple method” by P.Safar
1. Head tilt2. Chin lift3. Mouth open

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
I stage – Basic life support (BLS)
VentilationDuring CPR the purpose of ventilation is to maintain adequate oxygenation.
The optimal tidal volume, respiratory rate and inspired oxygen concentration to achieve this, however, are not fully known. The current recommendations are based on the following evidence:1. During CPR, blood flow to the lungs is substantially reduced, so an adequate
ventilation perfusion ratio can be maintained with lower tidal volumes and respiratory rates than normal.
2. Not only is hyperventilation (too many breaths or too large a volume) unnecessary, but it is harmful because it increases intrathoracic pressure, thus decreasing venous return to the heart and diminishing cardiac output. Survival is consequently reduced.
3. When the airway is unprotected, a tidal volume of 1 l produces significantly more gastric distention than a tidal volume of 500 ml.51
4. Low minute-ventilation (lower than normal tidal volume and respiratory rate) can maintain effective oxygenation and ventilation during CPR. During adult CPR, tidal volumes of approximately 500—600 ml (6—7 ml kg−1) should be adequate.
5. Interruptions in chest compression (for example to give rescue breaths) have a detrimental effect on survival. Giving rescue breaths over a shorter time will help to reduce the duration of essential interruptions.

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
I stage – Basic life support (BLS)
Ventilation
Mouth-to-nose ventilation is an effective alternative to mouth-to-mouth ventilation.57 It may be considered if the victim’s mouth is seriously injured or cannot be opened, the rescuer is assisting a victim in the water, or a mouth-to-mouth seal is difficult to achieve.
There is no published evidence on the safety, effectiveness or feasibility of mouth-to-tracheostomy ventilation, but it may be used for a victim with a tracheostomy tube or tracheal stoma who requires rescue breathing.

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
I stage – Basic life support (BLS)
Chest compression
Chest compressions produce blood flow by increasing the intrathoracic pressure and by directly compressing the heart. Although chest compressions performed properly can produce systolic arterial pressure peaks of 60-80 mm Hg, diastolic pressure remains low and mean arterial pressure in the carotid artery seldom exceeds 40 mm Hg. Chest compressions generate a small but critical amount of blood flow to the brain and myocardium and increase the likelihood that defibrillation will be successful. They are especially important if the first shock is delivered more than 5 min after collapse.

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
I stage – Basic life support (BLS)
Chest compression
Chest compressions produce blood flow by increasing the intrathoracic pressure and by directly compressing the heart. Although chest compressions performed properly can produce systolic arterial pressure peaks of 60-80 mm Hg, diastolic pressure remains low and mean arterial pressure in the carotid artery seldom exceeds 40 mm Hg. Chest compressions generate a small but critical amount of blood flow to the brain and myocardium and increase the likelihood that defibrillation will be successful. They are especially important if the first shock is delivered more than 5 min after collapse.
There is insufficient evidence to support a specific hand position for chest compression during CPR in adults. Previous guidelines have recommended a method of finding the middle of the lower half of the sternum by placing one finger on the lower end of the sternum and sliding the other hand down to it. It has been shown that for healthcare professionals the same hand position can be found more quickly if rescuers are taught to ‘‘place the heel of your hand in the centre of the chest with the other hand on top’’, provided the teaching includes a demonstration of placing the hands in the middle of the lower half of the sternum. It is reasonable to extend this to laypeople.

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
I stage – Basic life support (BLS)
Chest compression
Compression rate refers to the speed at which compressions are given, not the total number delivered in each minute. The number delivered is determined by the rate, but also by the number of interruptions to open the airway, deliver rescue breaths and allow AED analysis. In one out-of-hospital study rescuers recorded compression rates of 100-120 min−1 but, the mean number of compressions was reduced to 64 min−1 by frequent interruptions.
100-120
60-70
ope
n th
e ai
rway
, de
liver
res
cue
brea
ths
AED or ECG analysis,
defibrillation

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
I stage – Basic life support (BLS)
Dependence of systolic and diastolic blood pressure level from the rate of compression
SBP
DBP
SBP
DBP100-120
60-70

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
I stage – Basic life support (BLS)
Compression—ventilation ratio
Insufficient evidence from human outcome studies exists to support any given compression:ventilation ratio. Animal data support an increase in the ratio above 15:2. A mathematical model suggests that a ratio of 30:2 would provide the best compromise between blood flow and oxygen delivery. A ratio of 30 compressions to two ventilations is recommended for the single rescuer attempting resuscitation on an adult or child out of hospital. This should decrease the number of interruptions in compression, reduce the likelihood of hyperventilation, simplify instruction for teaching and improve skill retention.

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
I stage – Basic life support (BLS)
Compression-only CPR
Healthcare professionals as well as lay rescuers admit to being reluctant to perform mouth-to-mouth ventilation in unknown victims of cardiac arrest. Animal studies have shown that chest compression-only CPR may be as effective as combined ventilation and compression in the first few minutes after non-asphyxial arrest. In adults, the outcome of chest compression without ventilation is significantly better than the outcome of giving no CPR. If the airway is open, occasional gasps and passive chest recoil may provide some air exchange. A low minute-ventilation may be all that is necessary to maintain a normal ventilation:perfusion ratio during CPR.
Laypeople should, therefore, be encouraged to perform compression-only CPR if they are unable or unwilling to provide rescue breaths, although combined chest compression and ventilation is the better method of CPR.

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
I stage – Basic life support (BLS+)Modern principles of BLS include using of automated external defibrillators:
(AED) More than 460,000 fatal heart attacks occur each year in the U.S. 95‰ of people who suffer a heart attack in the workplace do not survive Defibrillation within three minutes of the onset of a heart attack saves 7 out of 10 lives
2 8 year old man who died suddenly while wearing a cardiac monitor (cit. - Jeffrey P. Koplan, 2002)
0 mins
2 mins
10 mins
Time from Collapse
Likelihood of success with defibrillation
>90%
80%
<10%

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
I stage – Basic life support (BLS+)
Restoration rhythm after shock

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
I stage – Basic life support (BLS+)
Modern principles of BLS include using of automated external defibrillators: (AED)
AED machines, housed in plastic cases the size of a large purse, can be used to monitor a person’s heartbeat and determine if the heart’s rhythm is normal. Defibrillators can also deliver life-saving electric shocks to restart the heart or correct an irregular heartbeat. AEDs are designed to be used by non-medical personnel, so cardiac arrest victims don’t have to wait for emergency crews to arrive to receive potentially life-saving treatment.
Some models of AEDs
Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
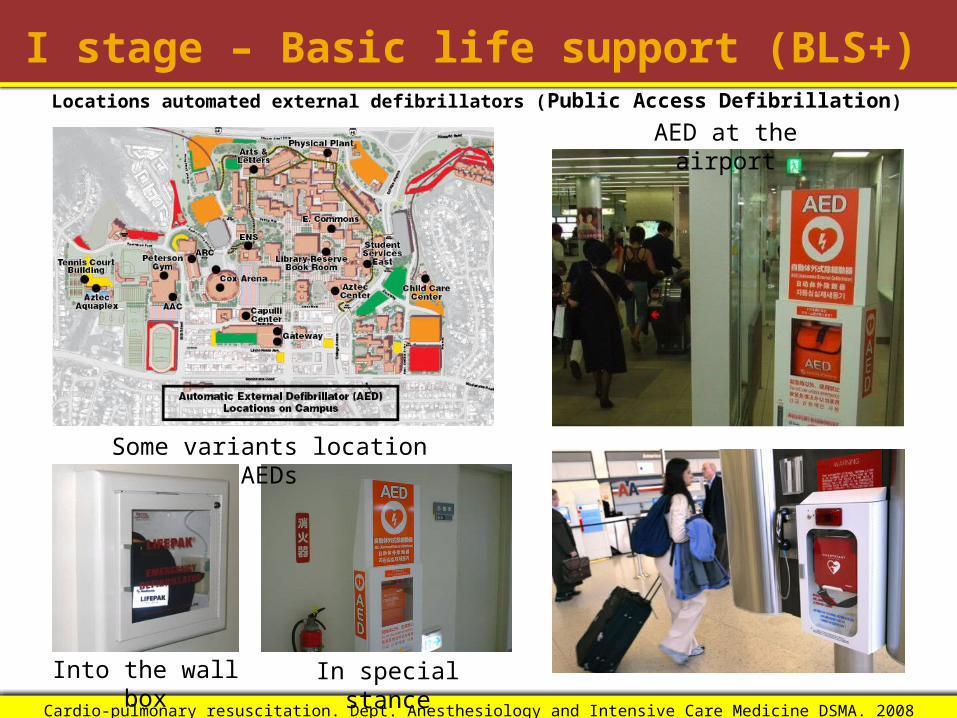
I stage – Basic life support (BLS+)Locations automated external defibrillators (Public Access Defibrillation)
Some variants location AEDs
Into the wall box In special stance
AED at the airport

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
I stage – Basic life support (BLS+)Sequence for use of an AED
As soon as the defibrillator arrives switch on the defibrillator and attach the electrode pads. If more than one rescuer is
present, CPR should be continued while this is carried out follow the spoken/visual directions ensure that nobody touches the victim while the AED is analyzing the rhythm
If a shock is indicated ensure that nobody touches the victim push shock button as directed (fully automatic AEDs will deliver the shock
automatically) continue as directed by the voice/visual prompts
If no shock indicated immediately resume CPR, using a ratio of 30 compressions to 2 rescue breaths continue as directed by the voice/visual prompts
Continue to follow the AED prompts until qualified help arrives and takes over the victim starts to breathe normally you become exhausted

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
I stage – Basic life support (BLS+)
Recent development in this direction – AED Plus from ZOLL Medical Corporation

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
I stage – Basic life support (BLS+)

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
II stage – Advanced life support (ALS)This stage usually is performed emergency
teambut any physician may, can and sometimes
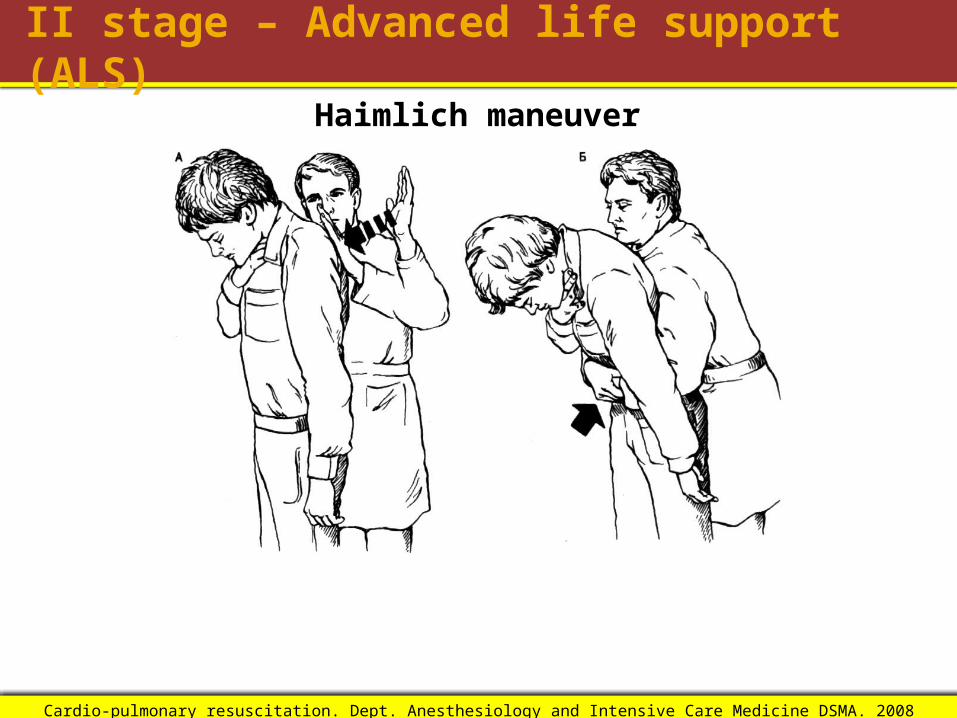
must do itAdvanced air way open procedures:
1. Haimlich maneuver2. Using vacuum-aspirator3. Aspiration bronchoscopy
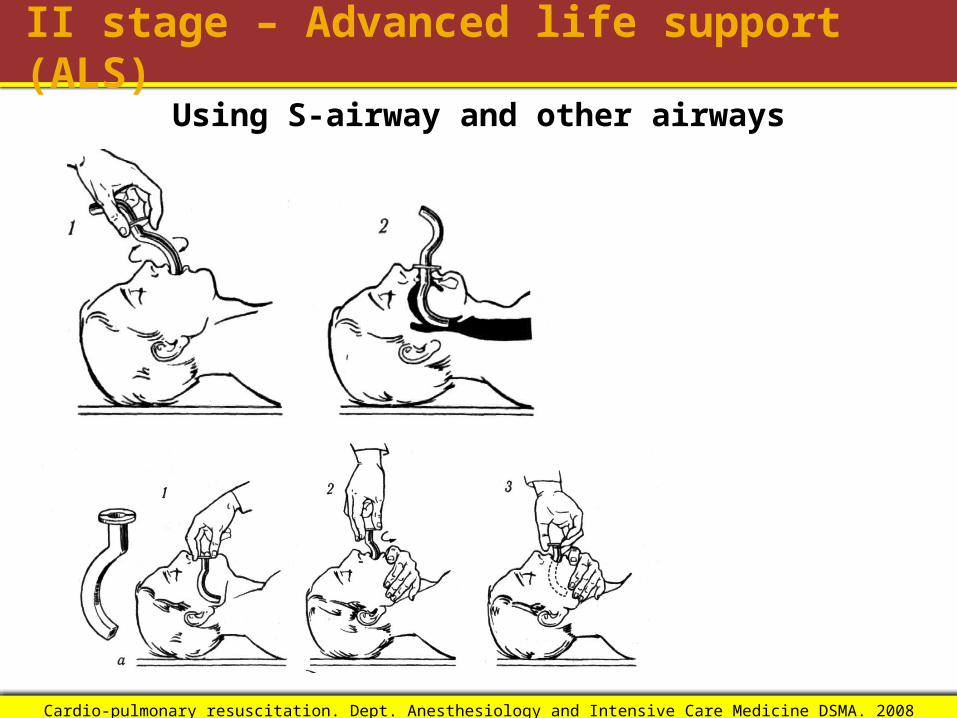
Advanced maintenance air way opened4. Using S-airway5. Using other airways6. Using laringeal mask7. Using oropharingeal tube (Combitube)8. Orotracheal or nasotracheal intubation
Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
II stage – Advanced life support (ALS)
Haimlich maneuver

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
II stage – Advanced life support (ALS)
Using vacuum-aspirator

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
II stage – Advanced life support (ALS)
Advanced maintenance air way opened1. Using S-airway2. Using other airways3. Using laringeal mask4. Using oropharingeal tube (Combitube)5. Orotracheal or nasotracheal intubation
Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
II stage – Advanced life support (ALS)
Using S-airway and other airways
Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
II stage – Advanced life support (ALS)
Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
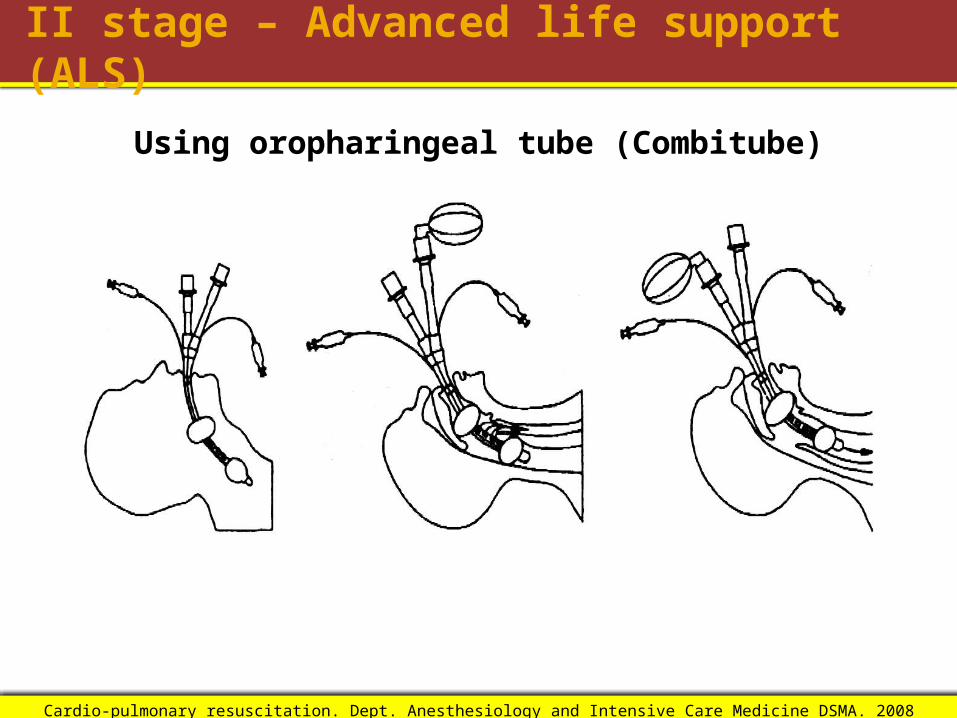
II stage – Advanced life support (ALS)
Using oropharingeal tube (Combitube)

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
II stage – Advanced life support (ALS)
Using laringeal mask

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
II stage – Advanced cardiac life support (ACLS)
Drugs and fluids for cardiac arrestThis topic is divided into:• drugs used during the management of a cardiac
arrest;• anti-arrhythmic drugs used in the peri-arrest period;• other drugs used in the peri-arrest period;• fluids;• routes for drug delivery.

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
II stage – Advanced cardiac life support (ACLS)
Drugs used during the management of a cardiac arrest:Epinephrine 1 mg every 3-5 min intravenously or 2 mg with 10 ml saline
endotrachealAtropine sulfate 3 mg intravenously or 6 mg with 10 ml saline endotracheal
one time on start drugs therapy cardiac arrestAmiodarone 300 mg intravenously, after third noneffective shock. It can
be retry every 10 min in dose – 150 mgLidocaine 100 mg (1-1.5 mg/kg) intravenously, further – 50 mg (max 3
mg/kg per hour). Using, if amiodaron is not available. Joint using both drugs is not recommended
Bicarbonate-Na 50 mmol (50 ml – 8.4% solution) if pH<7.1 or hyperkaliemia or overdose tricycle antidepressants
Aminophylline 5 mg/kg intravenously in case of asystolia and bradicardiaMagnesium sulfate 4 ml – 50% sol (8 mmol)Calcium chloride 10 ml – 10% sol in case of hyperkaliemia, hypocalciemia,
overdose blockader of calcium canal

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
II stage – Advanced cardiac life support (ACLS)
Fluids in CPR
Hypovolaemia is a potentially reversible cause of cardiac arrest. Infuse fluids rapidly if hypovolaemia is suspected. In the initial stages of resuscitation there are no clear advantages to using colloid, so use saline or Hartmann’s solution. Avoid dextrose, which is redistributed away from the intravascular space rapidly and causes hyperglycaemia, which may worsen neurological outcome after cardiac arrest.
There are no published human studies of routine fluid use compared to no fluids during normovolaemic cardiac arrest. Four animal studies of experimental ventricular fibrillation neither support nor refute the use of intravenous fluids routinely. In the absence of hypovolaemia, infusion of an excessive volume of fluid is likely to be harmful. Use intravenous fluid to flush peripherally injected drugs into the central circulation.

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
II stage – Advanced cardiac life support (ACLS)
Routes for drug delivery
• Intravenous• Intratracheal• Intraosseus

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
II stage – Advanced cardiac life support (ACLS)
Intraosseus line
If intravenous access cannot be established, intraosseous delivery of resuscitation drugs will achieve adequate plasma concentrations. Several studies indicate that intraosseous access is safe and effective for fluid resuscitation, drug delivery and laboratory evaluation. Traditionally, the intraosseous route is used mainly for children, but it is also effective in adults.

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
II stage – Advanced cardiac life support (ACLS)
Kinds of circulation arrest
Ventriculartachycardia (1%)
Ventricularfibrillation (58%)
Asystolia (31%)
Electromechanical dissociation (10%)

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
II stage – Advanced cardiac life support (ACLS)
www.mfi.ku.dk/PPaulev/chapter11/images/

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
II stage – Advanced cardiac life support (ACLS)
Defibrillation
Ventricular fibrillation is the condition when every myocardiocyte works in its own rhythm and synchronous action unavailable, therefore there is no systolic volume.
In this period different myocardiocytes have varying level of the sensitivities for electrical or mechanical stimuli, because its metabolism is depressed in varying degrees
Physical sense of defibrillation is: to make condition when every or main part of myocardiocytes are in the same phase cycle– phase of the refractory period.
This can be achieved through strong electrical shock.

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
II stage – Advanced cardiac life support (ACLS)
www.mfi.ku.dk/PPaulev/chapter11/images/

Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008Cardio-pulmonary resuscitation. Dept. Anesthesiology and Intensive Care Medicine DSMA. 2008
II stage – Advanced cardiac life support (ACLS)
Universal International AED sign (project)
Algorithm ofdefibrillation
Biphasic defibrillatorFirst shock – 150-200 J (biphasic truncatedexponential waveform) or 120 J (rectilinear biphasic waveform)Second shock – 250-300 J (BTE waveform) or Third shock – 360 J
Monophasic defibrillatorFirst and next – 360 J