cardiology board review august 30 th, 2011. test question the saints will win the superbowl this...
TRANSCRIPT
Cardiology Board Review
August 30th, 2011
Test Question
• The Saints will win the Superbowl this year.A. TrueB. False
CARDIAC HISTORY AND EXAM
Cardiac History
• Infants– Gestation– FHx– Neonatal status– Growth and development– Feeding patterns
• Children– Presence of palpitations– Chest pain– Lightheadedness or syncope– Activity level
Cardiac Exam
• Observation– Respiratory distress?– Central cyanosis?– Clubbing?– Syndromic appearance?
• Palpation– Hyperdynamic precordium?– Displaced PMI?– HSM?– Distal pulses equal? Bounding?
• Ausculatation
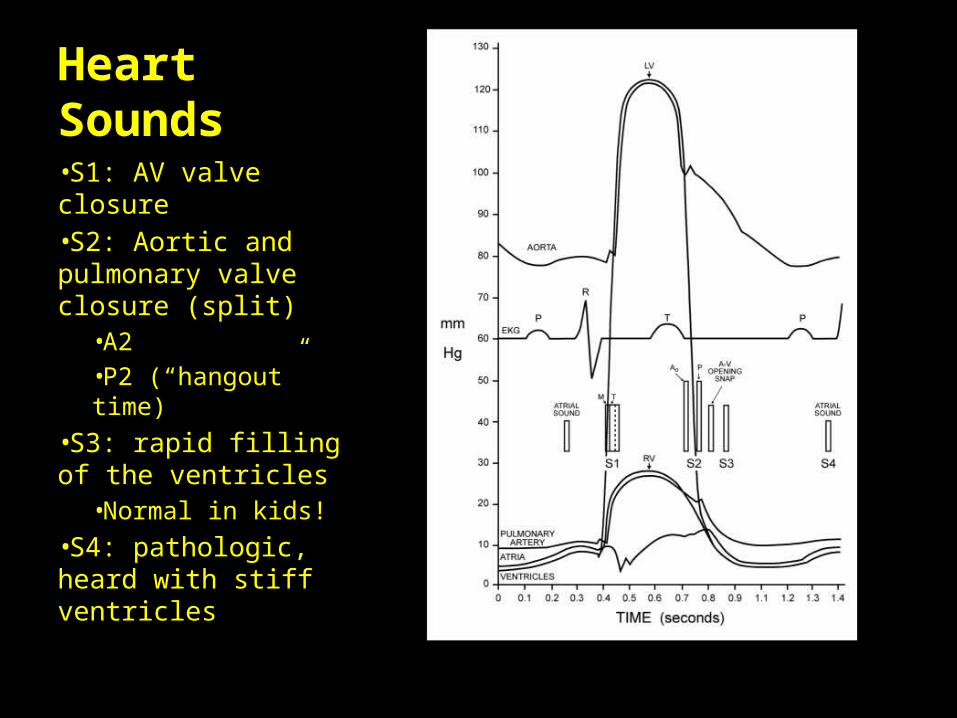
Heart Sounds•S1: AV valve closure•S2: Aortic and pulmonary valve closure (split)
•A2•P2 (“hangout” time)
•S3: rapid filling of the ventricles
•Normal in kids!•S4: pathologic, heard with stiff ventricles
Murmurs
Intensity• Grade 1: Barely audible• Grade 2: Audible and
constant• Grade 3: Loud without thrill• Grade 4: Loud with thrill• Grade 5: Heard with
stethoscope just touching the chest
• Grade 6: Heard with stethoscope off the chest
Placement in cardiac cycle• Systolic murmurs
– Pansystolic: begin with the first heart sound
– Ejection: begin after the first heart sound, have crescendo- decrescendo quality
• Diastolic murmurs– Immediate– Early or medium– Late

Question #1
• Which of the following accurately describes the Still murmur?– A: Mid-systolic murmur of low intensity heard at the base of
the heart, in the axillae, and over the back– B: Systolic or diastolic murmur heard in the infraclavicular
region (usually right sided); disappears when the patient is lying down
– C: Systolic murmur best heard above the clavicles, due to turbulence in the carotid artery
– D: Musical or vibratory quality at the mid-to-lower sternal border and toward the apex
– E: Loud continuous “machine-like” murmur
Innocent Murmurs
• Uniform characteristics– Early systolic ejection– Short duration– Low intensity (grade 1&2)– Vibrating or musical quality
• Examples– Still murmur– Venous hum– Supraclavicular bruit– PPS (peripheral pulmonary artery stenosis)
Pathologic Murmurs
• Longer and louder• All diastolic (except venous hum) and pansystolic
murmurs are pathologic• Systolic ejection murmur– Ejection click?– Is S2 widely split?– Does the S2 split move? Normally?– Hyperdynamic precordium?– Distended neck veins?– Peripheral pulses normal?
CONGENITAL HEART DISEASE IN NEONATE AND YOUNG INFANT
Clinical Presentations
• Recognize dysmorphic features as increased risk for CHD– Trisomy 21→ endocardial cushion defect– Trisomy 18→ VSD– Fetal alcohol syndrome→ ASD, VSD– 22q11 microdeltion→ interrupted aortic arch,
Tetralogy of Fallot, truncus arteriosus, atrial or ventricular septal defects, vascular rings
– 45 XO→ bicuspid aortic valve (16%), coarctation of aorta (11%)
Clinical Presentations
• Bicuspid aortic valve– Evaluated every 2 to 3 years– 70% develop some degree of stenosis or
insufficiency by age 30– Will require catheter-based or surgical
intervention at some point
Clinical Presentations
• Most have 1 of 4 presentations:– 1) Asymptomatic murmur– 2) Cyanosis (often without murmur)– 3) Gradually progressing symptoms of heart failure– 4) Catastrophic heart failure and shock
Asymptomatic with a Murmur
• Caused by regurgitant valves (mitral or tricuspid) or by lesions producing turbulence in a great artery (PS, AS, nonphysiologic peripheral pulmonary stenosis, supravalvular AS)
• Systolic murmur that obscures S1 is probably VSD or AV valve regurg
Asymptomatic with a Murmur
• ASD = fixed split S2 (increased flow across the pulmonary valve)
• Pulmonary stenosis = systolic click, heard best at left sternal border, radiates to back and axilla
• Aortic stenosis = ejection click (does not change with position), heard best at RUSB with radiation to neck
• PDA = continuous “machinery” murmur, loudest at left infraclavicular area
• VSD = holosystolic (if small, high-pitched and heard along sternal border)
Asymptomatic with murmur
• PDA– For preterm, can cause volume overload of right
heart– Hyperdynamic precordium and wide pulse
pressure– Dx by echo– Treat with indomethacin x 3– If fails to close, surgical ligation
Asymptomatic with murmur
• VSD– For moderate-to-large, systemic pressure in right
ventricle leads to systemic pulmonary pressure• CHF evolves over first 1 to 2 postnatal months
– Most surgical repair is at 4 to 6 months– If the normal decrease in pulmonary vascular
resistance does not occur→ no left-to-right shunt→ could develop Eisenmenger’s and irreversible pulmonary vascular changes→ now right-to-left shunt (right heart failure, valve dysfunction, arrhythmias)
Question #2• A 6-hour-old term male infant develops severe
cyanosis, but has no murmur on cardiac ausculatation. He is in no apparent distress, and CXR reveals prominent pulmonary vascular markings.
• The next MOST appropriate step is:A. Start oxygen via nasal canulaB. Prostaglandin infusionC. Atrial septostomy in cath labD. EchocardiogramE. IV Furosemide
Cyanotic CHD
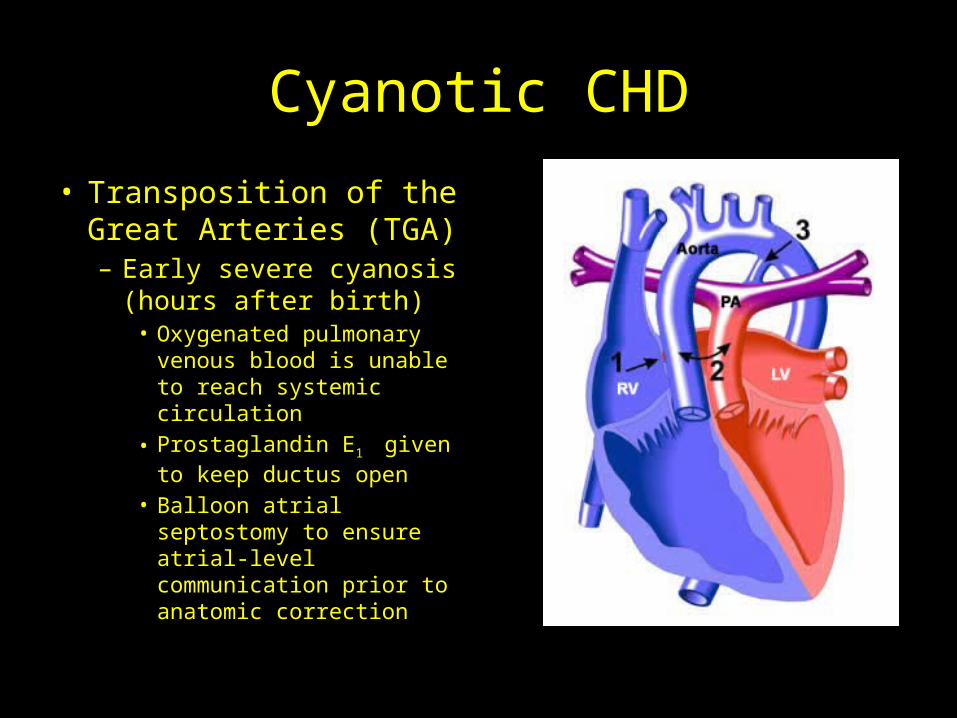
• Transposition of the Great Arteries (TGA)– Early severe cyanosis
(hours after birth)• Oxygenated pulmonary
venous blood is unable to reach systemic circulation
• Prostaglandin E1 given to keep ductus open
• Balloon atrial septostomy to ensure atrial-level communication prior to anatomic correction
Cyanotic CHD
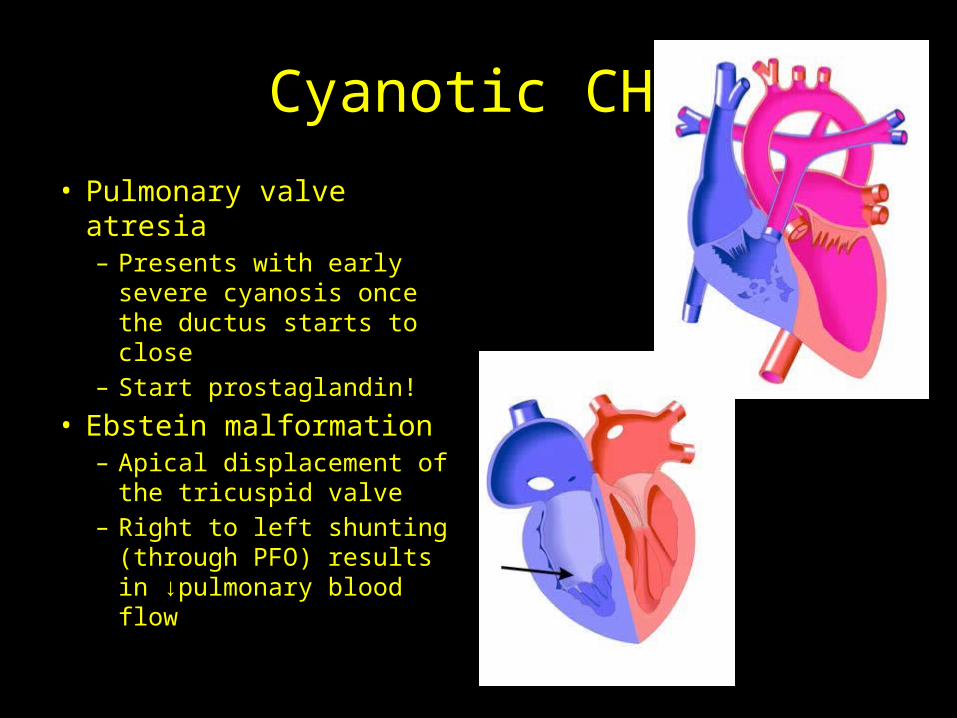
• Pulmonary valve atresia– Presents with early
severe cyanosis once the ductus starts to close
– Start prostaglandin!
• Ebstein malformation– Apical displacement of
the tricuspid valve– Right to left shunting
(through PFO) results in ↓pulmonary blood flow
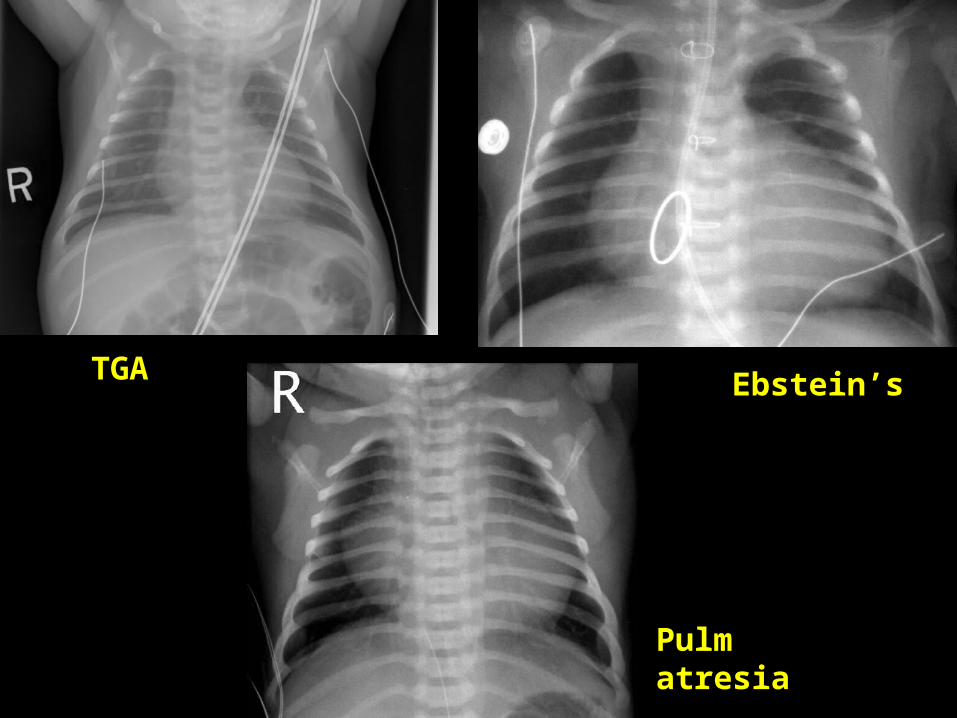
TGA Ebstein’s
Pulm atresia
Cyanotic CHD
• Most commonly, the presence of serious CHD is heralded by the identification of cyanosis in an infant who is not in respiratory distress (“happy cyanosis”)
Cyanotic CHD
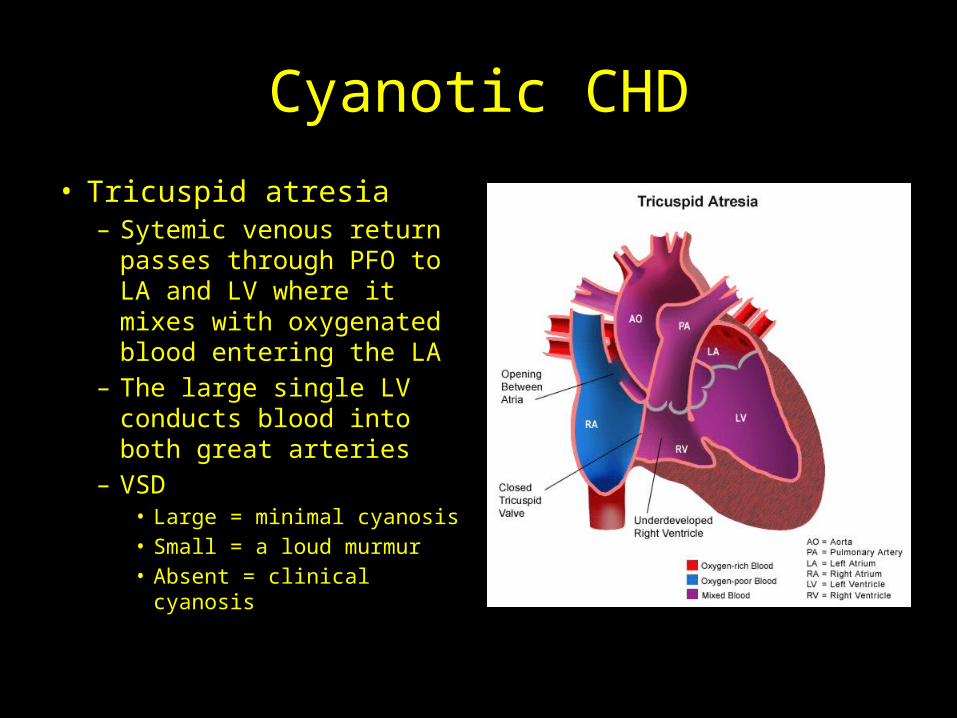
• Tricuspid atresia– Sytemic venous return
passes through PFO to LA and LV where it mixes with oxygenated blood entering the LA
– The large single LV conducts blood into both great arteries
– VSD• Large = minimal cyanosis• Small = a loud murmur• Absent = clinical cyanosis
Cyanotic CHD
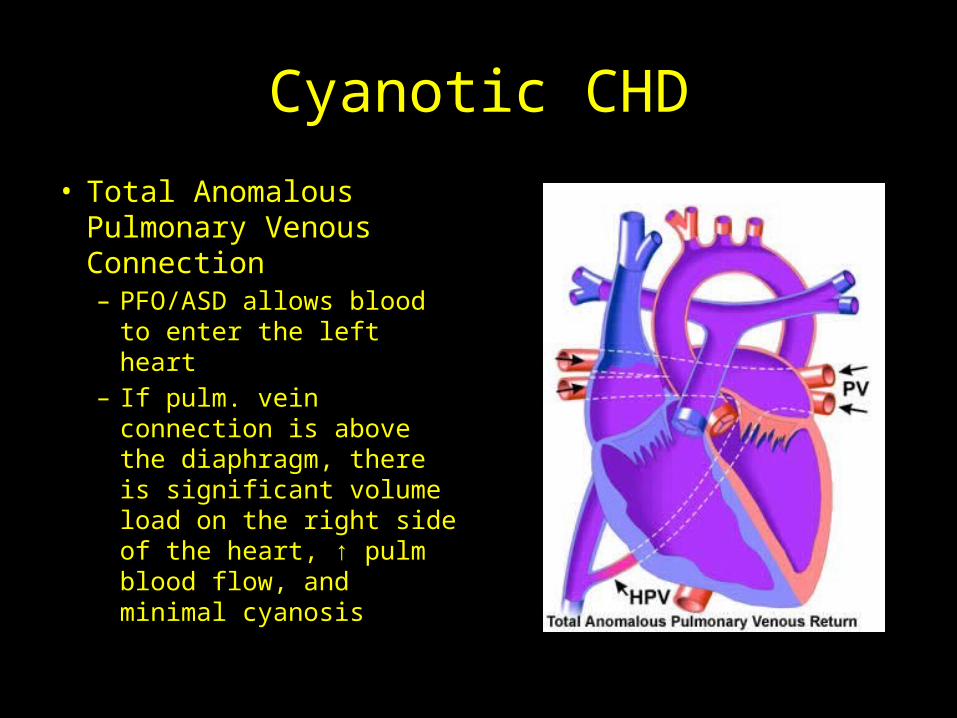
• Total Anomalous Pulmonary Venous Connection– PFO/ASD allows blood to
enter the left heart– If pulm. vein connection
is above the diaphragm, there is significant volume load on the right side of the heart, ↑ pulm blood flow, and minimal cyanosis
Cyanotic CHD
• TAPV can be difficult to distinguish from ASD– A palpable sternal lift, wide and fixed splitting of
S2 (due to RV overload), a pulmonary flow murmur, a tricuspid valve diastolic flow rumble, and tachypnea caused by pulm edema
– Only difference is presence of cyanosis• When connection is below the diaphragm– Infants are ill in newborn nursery with severe
pulm edema, pulm HTN, and cyanosis
Cyanotic CHD
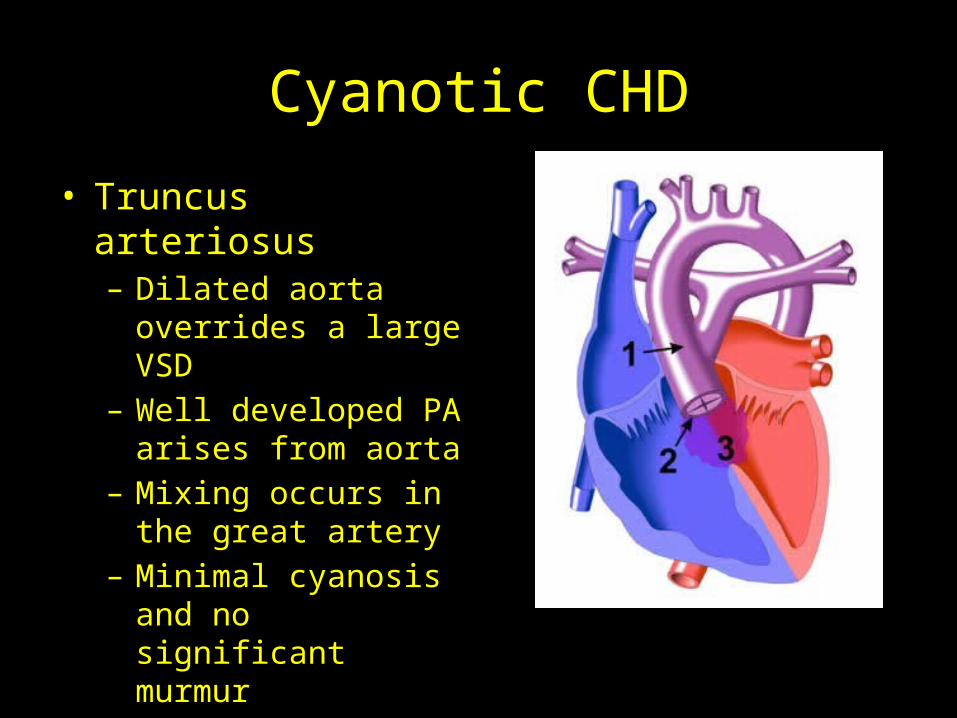
• Truncus arteriosus– Dilated aorta overrides a
large VSD– Well developed PA arises
from aorta– Mixing occurs in the
great artery– Minimal cyanosis and no
significant murmur
Cyanotic CHD
• S2 is loud due to anterior position of truncal aortic valve
• Ventricular lift is always palapable• Ejection click (or multiple clicks) caused by a
valve that can have as many as 6 leaflets• Commonly present with failure to thrive
several months after birth
Cyanotic CHD
• Review: Admixture lesions– Tricuspid atresia, TAPV, truncus arteriosus• Absence of pulmonary stenosis leads to minimal
cyanosis• Sometimes transient cyanosis on first postnatal day
– Pulse ox below 95% are never normal in otherwise healthy-appearing infants after the first 6 postnatal hours
Cyanotic CHD
• Hyperoxia test– Cyanosis typically present with sats ≤ 85%– Place the patient in a high-oxygen atmosphere
(FiO2 near 1.0)– No increase in sats or PaO2 (≥150), cyanotic
congenital heart disease should be considered
Question #3• A 4-month-old infant with unrepaired congenital
heart disease has had fever and URI symptoms since last evening. Her mother brings her to clinic, and on physical exam the patient is crying and unconsolable, has marked cyanosis, a decrease in the loudness of her murmur, and deep, rapid breathing.
• Of the following, the next MOST appropriate step is:A. EchocardiogramB. IVFsC. Sedation with MorphineD. AcetaminophenE. IV Furosemide
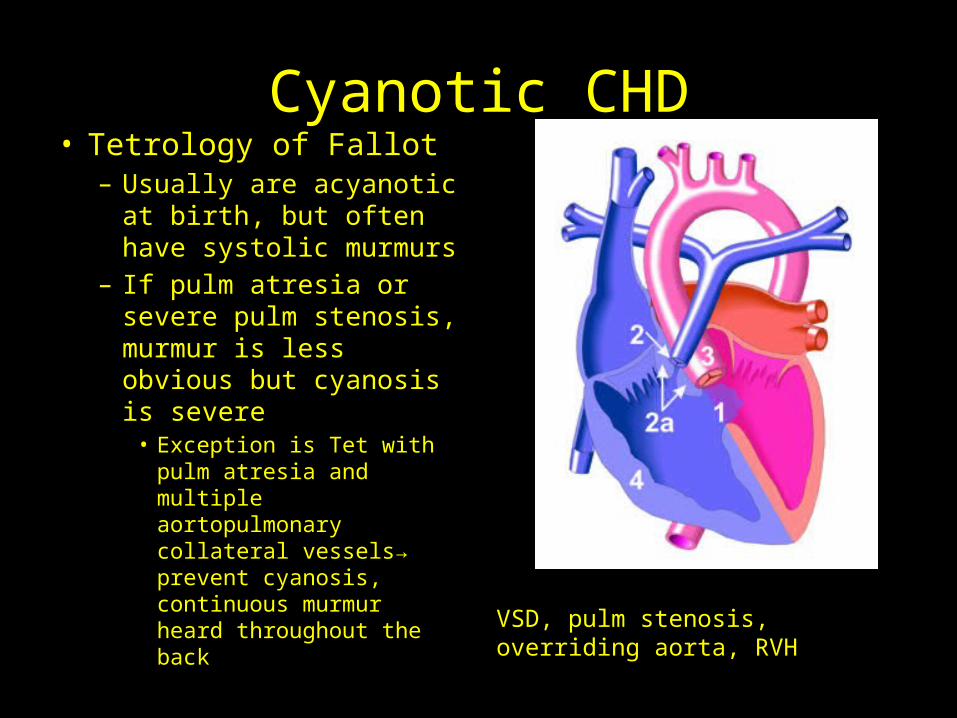
Cyanotic CHD• Tetrology of Fallot– Usually are acyanotic at
birth, but often have systolic murmurs
– If pulm atresia or severe pulm stenosis, murmur is less obvious but cyanosis is severe• Exception is Tet with pulm
atresia and multiple aortopulmonary collateral vessels→ prevent cyanosis, continuous murmur heard throughout the back
VSD, pulm stenosis, overriding aorta, RVH
Cyanotic CHD
• Hypercyanotic spells (“tet spells”)– Unusual in newborn period, but can happen any time in
an unrepaired tet– Intense cyanosis develops rapidly– Sudden decrease in loudness of murmur caused by ↓
systolic flow through the RV outflow tract– Deep, rapid respiratory pattern– Calming the infant (with or without sedation) may
resolve the spell

Cyanotic CHD
• Prognosis for TOF– Once infant develops progressive cyanosis, surgical
correction is indicated• Elective repair in first postnatal year
– Surgical survival of 95%– However, 10% of neonates requiring bypass surgery
have some element of neurodevelopmental delay or cognitive/school performance abnormality
– Speech and behavior disorders are common among those who undergo neonatal heart surgery
Cyanotic CHD
• Polycythemia– Desaturated arterial blood can cause increased erythropoetin
secretion– Increased blood viscosity– Risk for thrombosis to lungs, kidney, or brain– Risk for cerebrovascular accident
• Anemia– Chronic cyanotic heart disease pts. Are at risk for
cerebrovascular accident due to paradoxic emboli and a relative anemia
– Iron deficiency in the presence of polycythemia poses a greater risk for stroke
CHD with progressive heart failure
• Too much pulmonary blood flow or too little systemic blood flow
• When pulm vascular resistance falls, signs and symptoms start– Tachypnea, sweating, difficulty feeding, FTT, gallop
rhythm, hepatomegaly• Left-to-right shunt via VSD, atrioventricular septal
defect, or PDA causes pulm overcirculation• Most diseases causing heart failure in infants can
be treated surgically as soon as signs develop
Question #4• A 3-week-old infant presents to ER with tachypnea,
mottled gray skin, poor perfusion, decreased peripheral and central pulses, a gallop rhythm and hepatomegaly. CXR shows cardiomegaly. You suspect left heart obstructive disease and order prostaglandin.
• The MOST appropriate next step is:A. NS bolus 20ml/kgB. ElectrocardiogramC. Start oxygen via nasal canulaD. Captopril 0.01mg/kgE. Place patient in knee-to-chest position
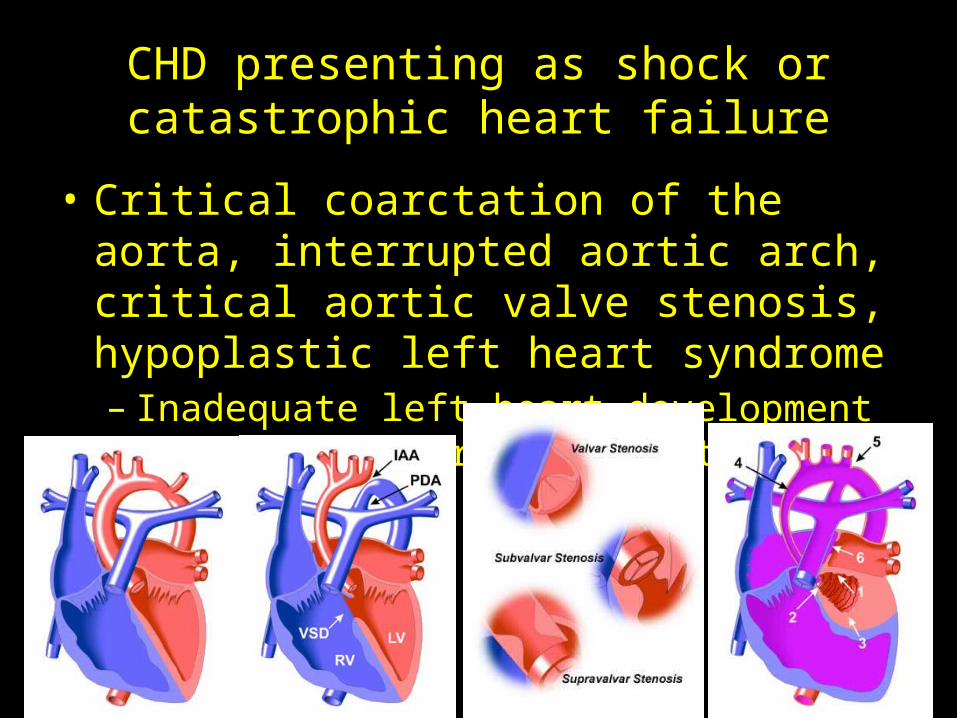
CHD presenting as shock or catastrophic heart failure
• Critical coarctation of the aorta, interrupted aortic arch, critical aortic valve stenosis, hypoplastic left heart syndrome– Inadequate left heart development compromises
cardiac output
CHD presenting as shock or catastrophic heart failure
• Potential for catastrophic deterioration due to inadequate systemic flow is greater in these lesions as the ductus undergoes spontaneous closure
• Oxygenated blood from the lungs is diverted across an atrial-level communication into right ventricle
• Mixing in right atrium→ increased sats of right heart blood→ minimizes the appearance of cyanosis
CHD presenting as shock or catastrophic heart failure
• In newborn nursery– A single and loud S2– Increase in RV activity on precordial palpation– Minimally abnormal postductal pulse ox– Decreased femoral pulses not present because
ductus is still large
CHD presenting as shock or catastrophic heart failure
• Check pre- and post-ductal sats– A postductal sat above 96-97% rule out a
completely ductal-dependent left heart obstruction
– High sats can occur in the setting of coarctation of the aorta
CHD presenting as shock or catastrophic heart failure
• Often present after discharge due to ductal patency– As ductus closes, decreased systemic blood flow,
oliguria, acidosis, pulmonary edema, and heart failure
– May mimic sepsis (tachypnea, mottled skin, poor perfusion)
– Critical clues: a gallop rhythm and marked hepatomegaly or cardiomegaly
CHD presenting as shock or catastrophic heart failure
• If suspect critical coarc or HLH, prostaglandin should be started immediately
• EKG and echo are part of evaluation for patient with possible cardiogenic shock
• Fluid resuscitation as well as respiratory and inotropic support are essential treatments
Follow-up for Coarc
• Recoarctation can occur as child grows• Higher incidence of hypertension– Frequent BP measurements by pediatrician
Question #5• A 4 week old infant born at term without complications presents
with poor feeding. He ate well for the first 3 weeks after birth and gained weight appropriately. For the past week, however, Mom reports that he appears hungry but fatigues with feeding (now taking twice as long to feed). He breathes fast during his feedings and stops frequently to “catch his breath.” Of the following, what is the most likely additional finding in this infant?– A. Lobar consolidation on CXR– B. Lipid laden macrophages on BAL– C. Elevated BNP– D. Positive RSV– E. Posterior esophageal indentation on barium swallow

HEART FAILURE
Definition
• HF results when cardiac output is insufficient to meet the metabolic demands of the body
• Triggers of HF in children:– Excessive preload– Excessive afterload– Abnormal rhythm– Decreased contractility
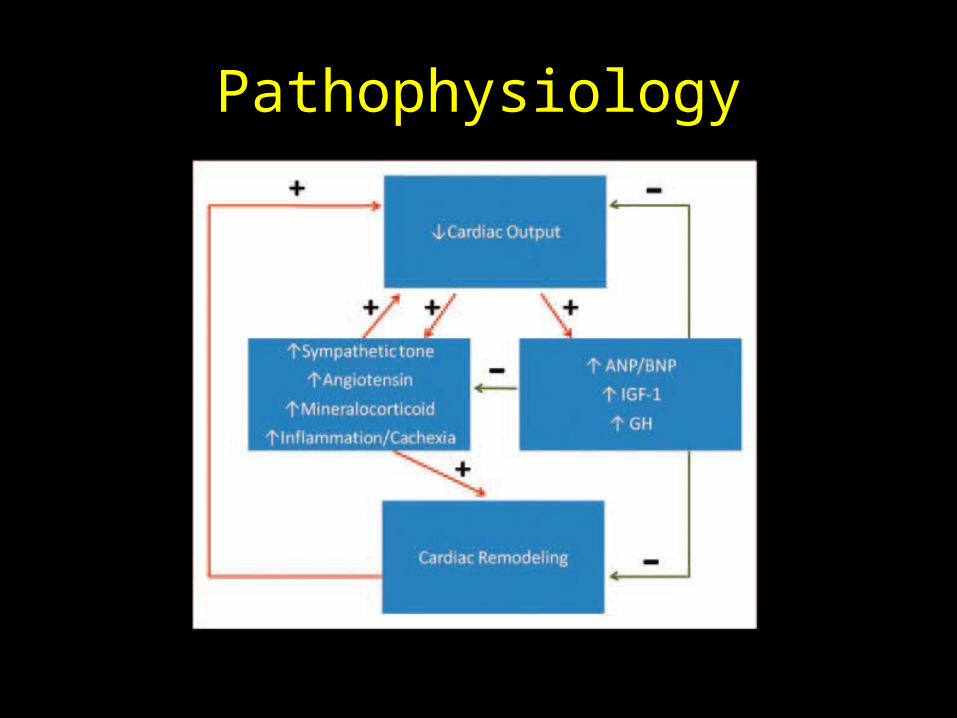
Pathophysiology
Clinical Manifestations
Infants• Feeding difficulties
– Volume and duration
• Increased fatigability• Mild to severe retractions• Tachypnea/ dsypnea• Grunting • Tachycardia• Gallop rhythm (S3,S4)• Hepatomegaly
Older Children• Exercise intolerance• Somnolence• Anorexia• Cough/wheezing• Crackles• Gallop rhythm• Hepatomegaly• JVD• Peripheral edema
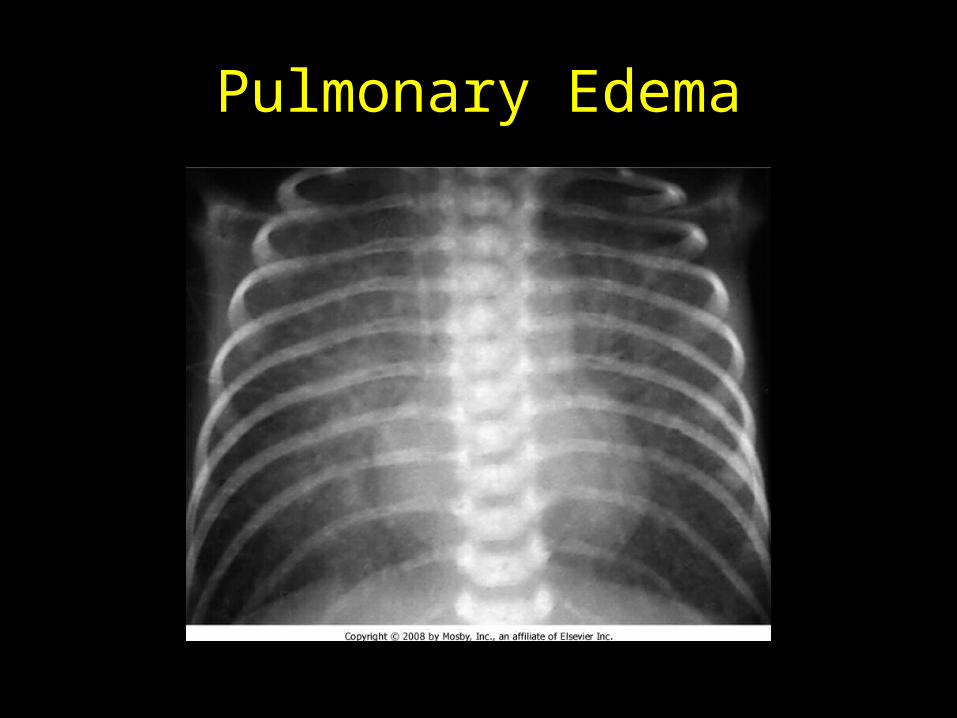
Pulmonary Edema
Common Causes- Excessive Preload
• L R shunts at the ventricular level– VSD, PDA– Present at 2-3 mos: pulmonary vascular
resistance pulmonary blood flow pulmonary venous return to the L atrium (excessive preload) cardiac filling pressure myofiber stretching and decreased contractility (HF)
Common Causes- Excessive Preload
• AVM– Divert blood from higher-resistance capillary beds
to low-resistance venous beds excessive venous return increased ventricular filling pressure (HF)
• Valvular regurgitation lesions– Most common mitral or aortic regurgitation
Common Causes- Excessive Preload
• R-sided volume loading can also HF– Rarely causes HF early in life• R ventricle highly compliant, so can accommodate
more volume without increasing filling pressures
– Examples:• Large ASD• TAPVR• Pulmonary regurgitation
Common Causes- Excessive Afterload
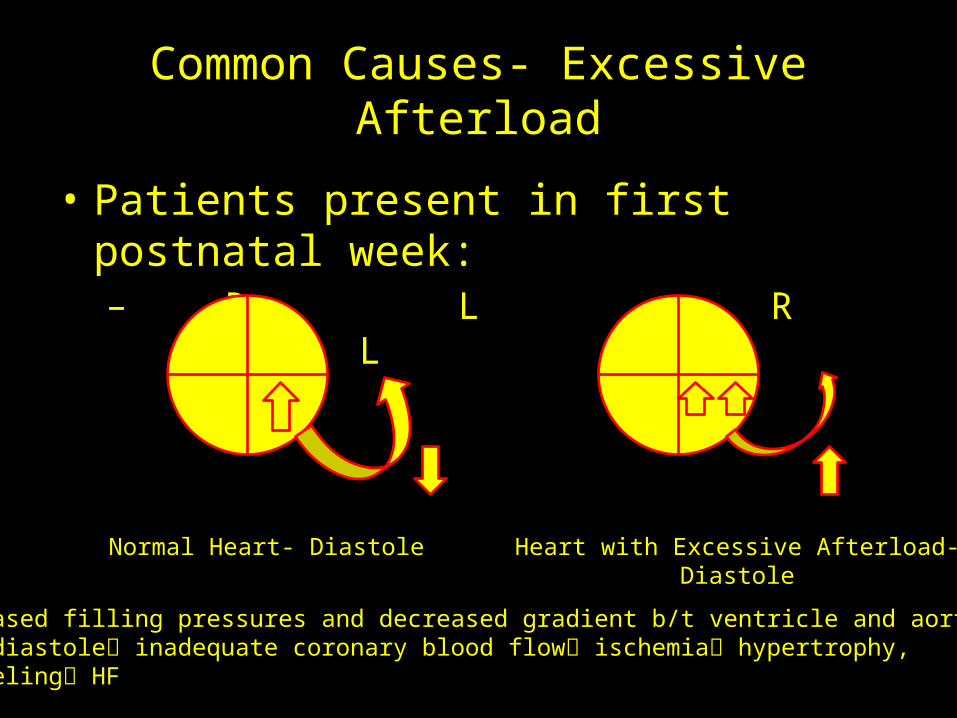
• Patients present in first postnatal week: – R L R L
Normal Heart- Diastole Heart with Excessive Afterload-Diastole
Increased filling pressures and decreased gradient b/t ventricle and aorta at end- diastole inadequate coronary blood flow ischemia hypertrophy,remodeling HF
Common Causes- Excessive Afterload
• Examples:– Mitral stenosis– Aortic stenosis– Coarctation of the aorta
Common Causes- Contractility
• Cardiomyopathy (HF presenting feature)– Dilated• Impaired systolic and diastolic function• Causes:
– Idiopathic– Infection (myocarditis)– Operative injury– Chemo (anthracyclines)– Metabolic/ degenerative diseases
Common Causes- Contractility
• Cardiomyopathy (con’t)– Restrictive• Abnormal diastolic function• Causes:
– Idiopathic– Infiltrative or storage diseases (hemochromatosis, Pompe dz)
– Hypertrophic• Not usually associated with pediatric HF
Common Causes- Arrhythmias
• Tachycardia- related diseases (SVT)– Decreased filling time Decreased CO HF
• Bradycardia- related diseases– Left ventricle enlarges to accommodate larger SV
significant chamber dilation HF
Evaluation
• Pulse oximetry• 12-lead EKG• CXR• Echocardiogram• HF biomarkers– BNP• Released in response to atrial stretching• Sensitive marker of cardiac filling pressure/ diastolic
dysfunction
Evaluation
• HF Biomarkers– BNP (con’t)• Can distinguish b/t primary respiratory and cardiac-
induced tachypnea
– CRP– TNF-alpha• Both correlate positively with worse outcome in HF
Question #6
• What is the role of ACE inhibitors in managing HF?– A. Preload reduction– B. Afterload reduction– C. Sympathetic inhibition– D. Increased contractility– E. Increased preload
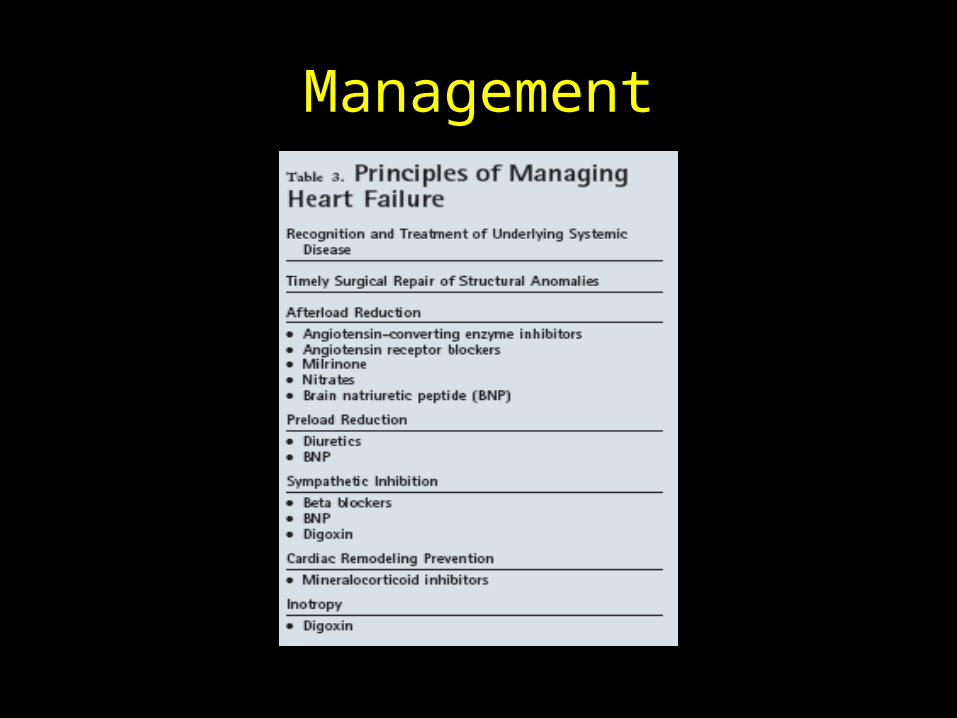
Management
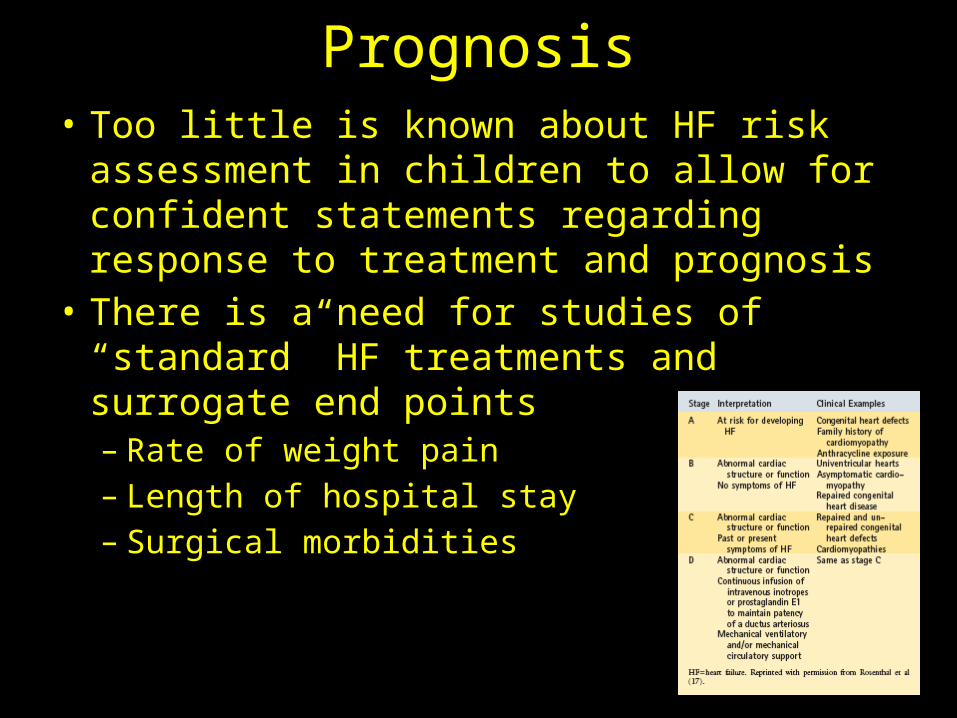
Prognosis• Too little is known about HF risk assessment in
children to allow for confident statements regarding response to treatment and prognosis
• There is a need for studies of “standard” HF treatments and surrogate end points– Rate of weight pain– Length of hospital stay– Surgical morbidities
ARRHYTHMIAS
Basic Principles
• Abnormality in regular heart conduction and rate• Spectrum of severity
– Benign• PAC• PVC
– Malignant• Atrial
– SVT– Atrial ectopic tachycardia– A. flutter– A. fibrillation
• Ventricular– V. tachycardia– V. fibrillation
Clinical Manifestations
Infants• Pallor • Diaphoresis• Respiratory distress• Poor feeding• Diminished perfusion• CHF• Shock
Children/ Adolescents• Palpatation
– Rapid, strong or irregular heart rate
• Shortness of breath• Dizziness • Light-headedness• Syncope
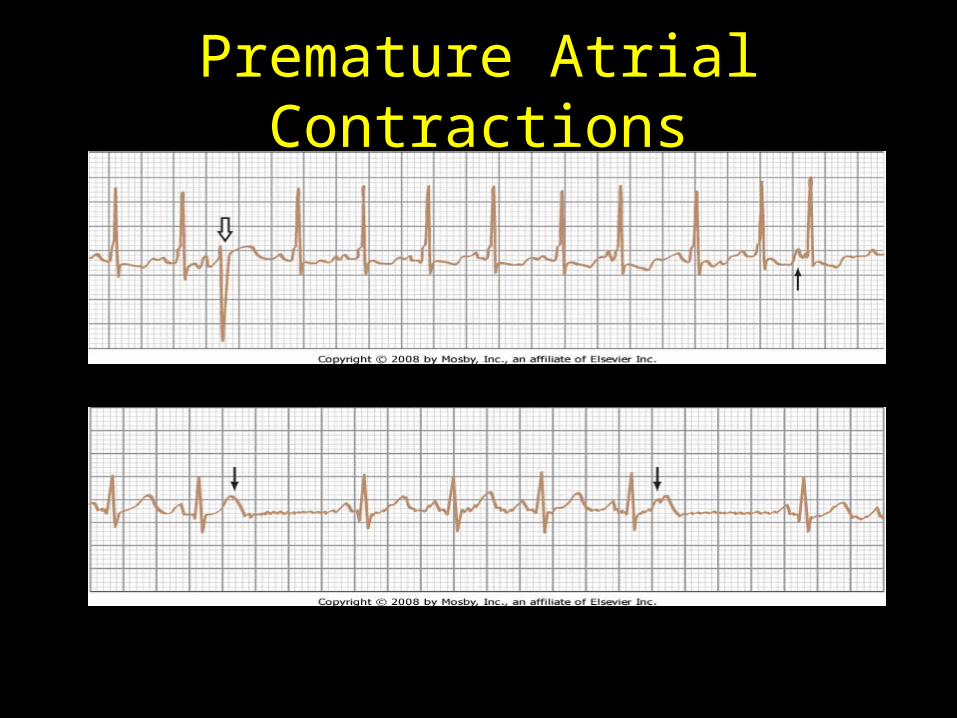
Premature Atrial Contractions
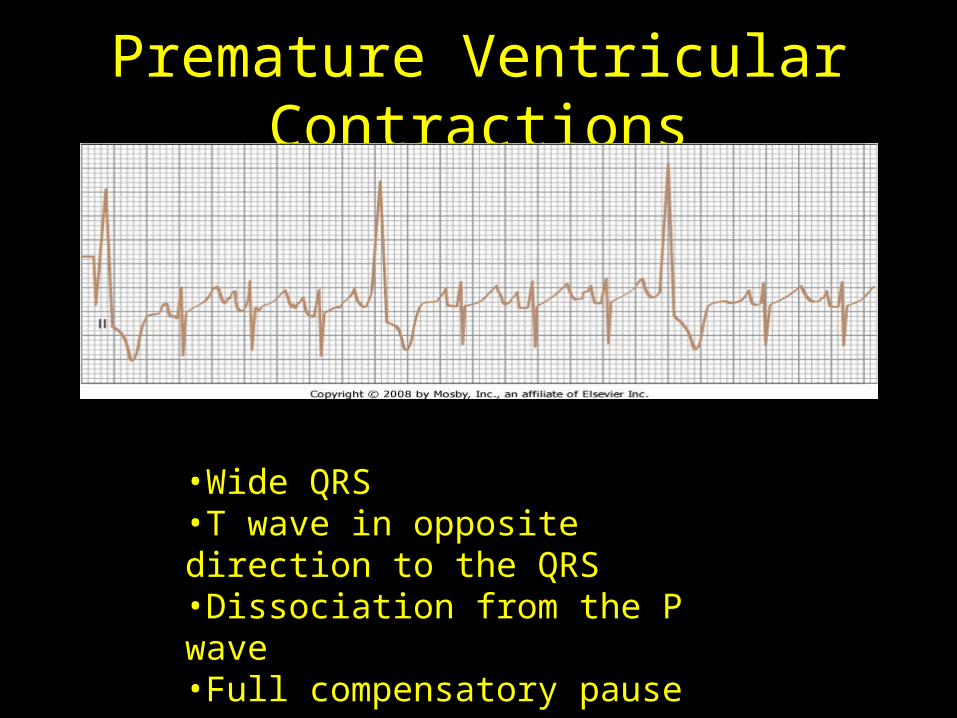
Premature Ventricular Contractions
•Wide QRS•T wave in opposite direction to the QRS•Dissociation from the P wave•Full compensatory pause
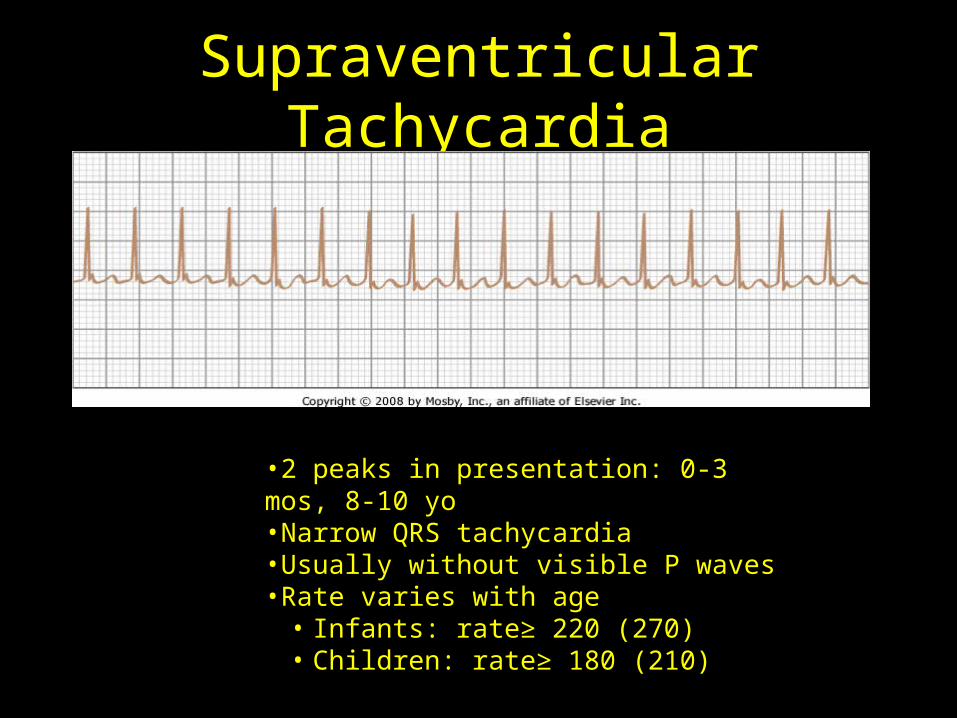
Supraventricular Tachycardia
•2 peaks in presentation: 0-3 mos, 8-10 yo•Narrow QRS tachycardia•Usually without visible P waves•Rate varies with age• Infants: rate≥ 220 (270)• Children: rate≥ 180 (210)
Treatment of SVT
• Acute management– Vagal maneuvers– Adenosine
• Transient complete AV block
– DC cardioversion• Chronic management– B-blocker (propranolol, atenolol)– Digoxin– Flecanide, sotalol, amiodarone– Radiofrequency catheter ablation
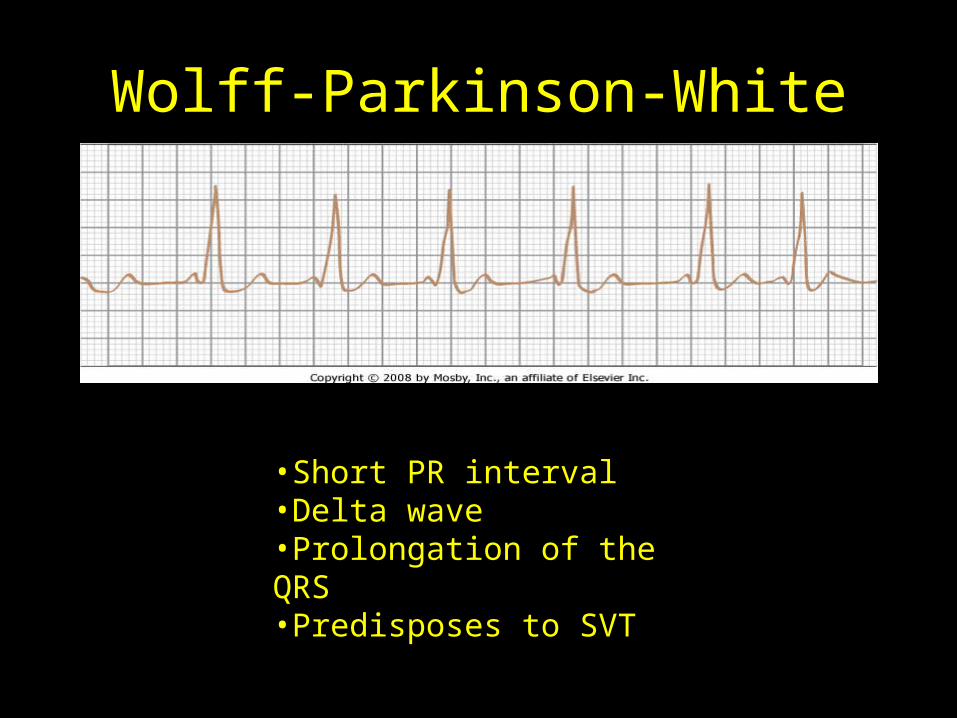
Wolff-Parkinson-White
•Short PR interval•Delta wave•Prolongation of the QRS•Predisposes to SVT
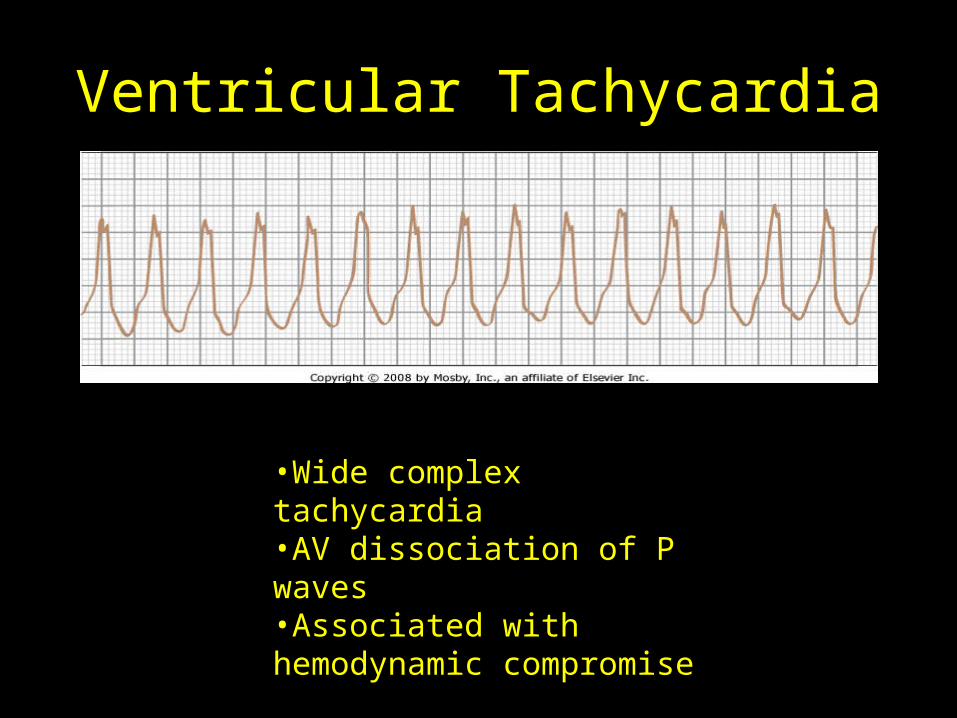
Ventricular Tachycardia
•Wide complex tachycardia•AV dissociation of P waves•Associated with hemodynamic compromise

Long QT Syndrome
•Must “correct” for patient’s HR: QTc=QT/Sq root of RR•QTc≥ 450 msec suggestive, QTc≥ 470 msec abnormal•Associated with development of torsades de pointes
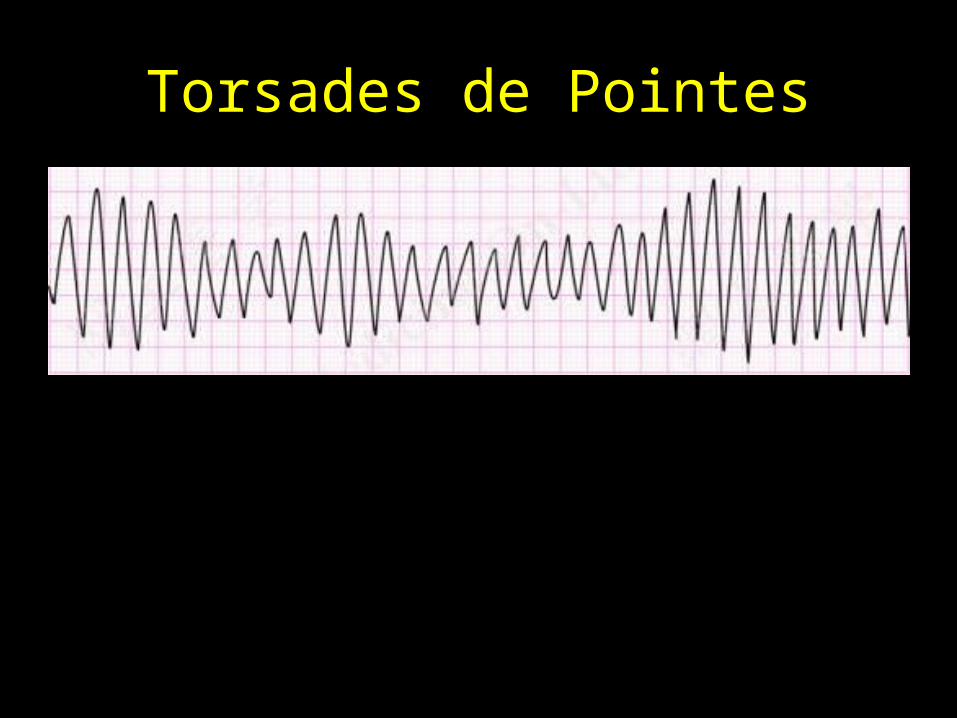
Torsades de Pointes
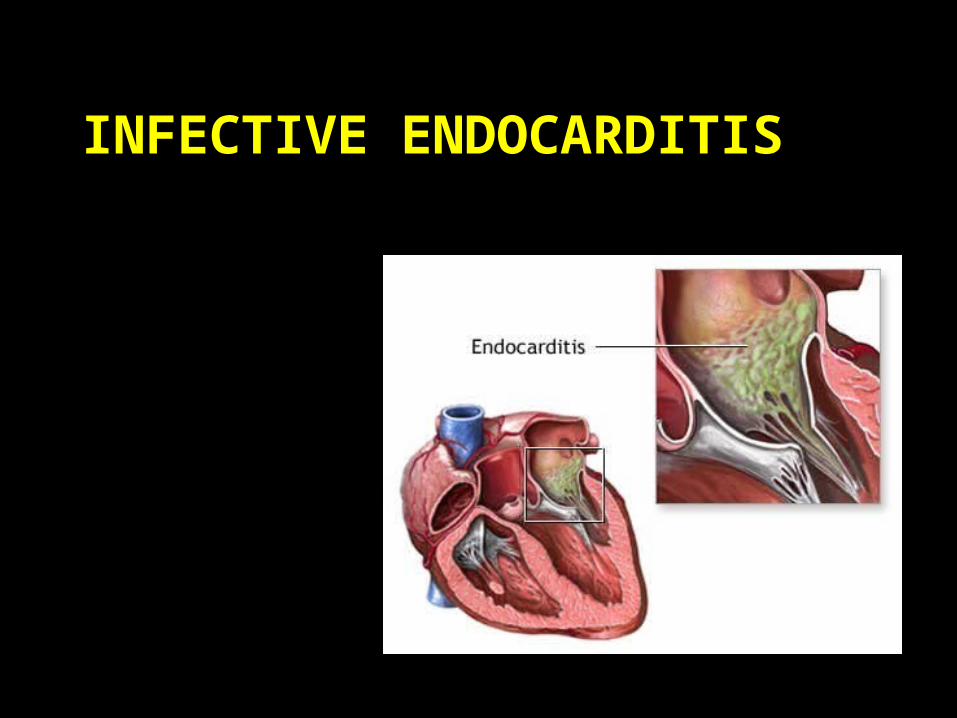
INFECTIVE ENDOCARDITIS
Definition and Epidemiology
• Definition: Inflammation of the valvular or mural endocardium, caused by microorganisms (bacteria or fungi), involving either the heart or the great vessels
• Epidemiology:– Rare diagnosis, but ?increasing
• Number of cases of ARF decreasing, but number of patients living beyond infancy with CHD increasing– 90% of cases occur in individuals with heart disease
• Increased use of invasive procedures in N/PICU are putting structually normal hearts at risk
Pathogenesis
• Damage to endothelium (or foreign materal) exposed fibronectin at the site of injury activation of the clotting cascade and fibrin deposition delivery of microbes to the clot by blood stream original nidus grows into a vegetation valve destruction/ HF/ embolization
• Gram positive cocci most likely pathogens– Predilection for fibronectin– S.viridans, S.aureus, S. epidermidis, B-hemolytic strep
Pathogenesis
• Gram negative organisms less common– Inability to bind fibronectin– “HACEK” organisms
• Fungi– Candida– Aspergillus
Clinical Manifestations
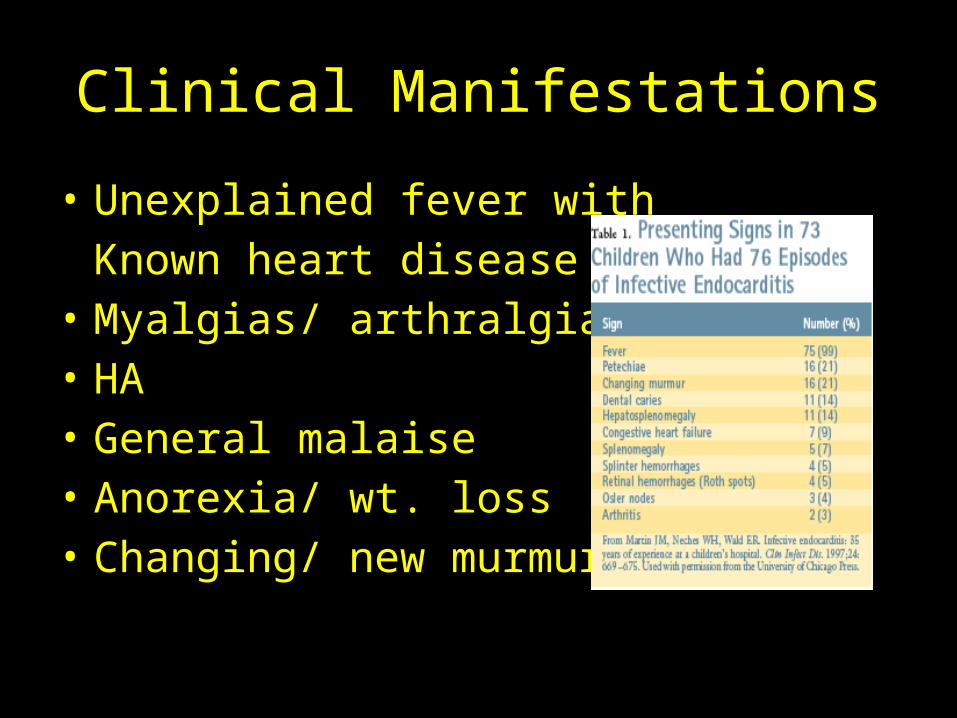
• Unexplained fever withKnown heart disease
• Myalgias/ arthralgias• HA• General malaise• Anorexia/ wt. loss • Changing/ new murmur

Clinical Manifestations
Janeway Lesions Osler Nodes

Clinical Manifestations
Hemorrhagic Lesions
Subungal splinter hemorrhages
Diagnosis
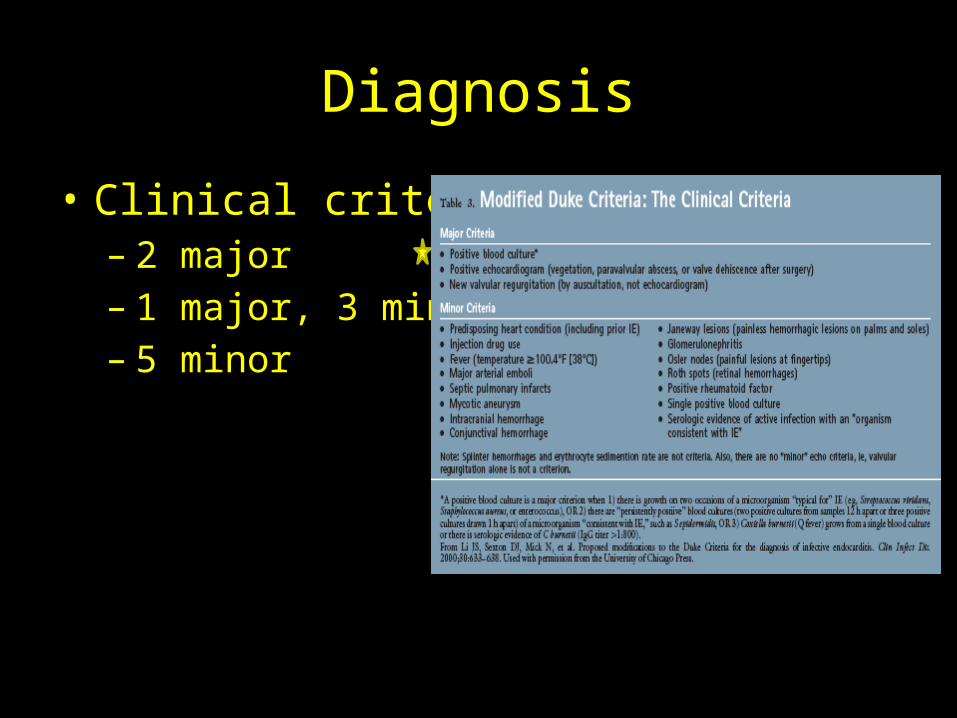
• Clinical criteria– 2 major– 1 major, 3 minor– 5 minor
Treatment
• Want to make sure BCxs have been obtained appropriately before starting ABx!
• If empiric treatment necessary:– Direct toward most common offenders
• Streptococci and Staphylococci
• IV Abx to attain high bactericidal concentrations• Ampicillin (Vancomycin) + Gentamicin
• Treatment x4-6 weeks– Longer with prosthetic valve
Complications
• Embolization!!• Abscess formation• Heart failure• Heart block• Mycotic aneurysms
Question #7
• You are referring one of your patients to have some teeth extracted. Mom mentions that she has a history of a “heart problem”. She asks if her daughter will need antibiotics prior to her dental procedure. Of the following, which cardiac lesion would require endocarditis prophylaxis?– A. Bicuspid aortic valve– B. Mitral valve prolapse– C. Hypertrophic cardiomyopathy– D. Pulmonary stenosis – E. Cardiac transplant with residual valvopathy
Endocarditis Prophylaxis: Who?
• 1. Prosthetic heart valves• 2. Previous IE• 3. Unrepaired cyanotic heart disease that includes
palliative shunts and conduits• 4. Completely repaired congential heart disease with
prosthetic material or device during the first 6 months following the procedure
• 5. Repaired congenitial heart disease with residual defects at the site or next to the site of the prosthetic device
• 6. Valvulopathy in a transplanted heart
Endocarditis Prophylaxis: When?
• Dental procedures– Involve manipulation of gingiva, perforation of the
oral mucosa• Tonsillectomy/ adenoidectomy• Operations involving the respiratory mucosa – Bronchoscopy with biopsy
• Surgical procedures on infected skin or musculoskeleton
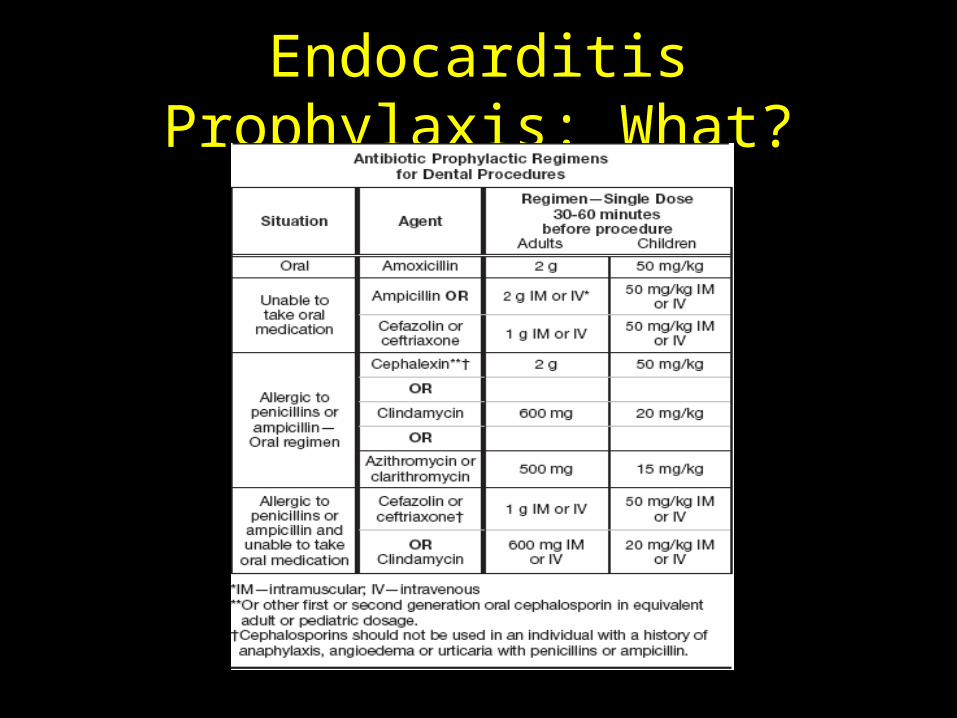
Endocarditis Prophylaxis: What?
Question #8• A 12 yo female with right knee swelling, pain, and
erythema presents to clinic. She had similar symptoms in left knee yesterday. She also complains of fatigue and fever. On PE she has a macular rash on trunk and arms and a 3/6 holosystolic murmur on ausculatation that radiates to the axilla. You suspect acute rheumatic fever, and are waiting on echo results. Her rapid strep antigen test is negative.
• What is the next most appropriate test?A. AntiDNAase BB. ESRC. CBCD. CRPE. Throat culture
ACUTE RHEUMATIC FEVER
Epidemiology
• Prevalence is 0.05 cases per 1,000 in US• Typically affects children 5 to 15 years old
Clinical Manifestations
• Delayed nonsuppurative complication of group A streptococcal (GAS) pharyngitis– A latent period of 2 to 4 weeks before symptoms
appear• Typically see polyarthritis (migratory), carditis,
subcutaneous nodules, erythema marginatum, or chorea
• Mitral regurgitation is the most common valvular lesion

Laboratory Findings
• Must establish the presence of a preceding GAS infection– Rapid strep antigen (95% specificity, 80% sensitivity)– Throat culture
• Negative in 75% of patients by the time ARF manifests
– Antistreptococcal antibody titers (antistreptolysin O, antiDNAse B, antihyaluronidase)• Peak around onset of ARF and are most useful
• Elevated ESR and CRP indicate ongoing inflammation
Carditis
• ARF can cause inflammation of pericardium, myocardium, and endocardium
• Good cardiac exam and echo are a must!– On exam most common murmurs:
• Apical, holosystolic murmur of mitral regurgitation (radiates to left axilla)
• Early diastolic decrescendo murmur of aortic regurgitation
• Cardiomegaly on CXR• ECG may reveal varying degrees of heart block
Treatment
• Treatment of GAS pharyngitis must be started within 9 days of onset to prevent ARF– Penicillin is drug of choice– Evaluate and treat all household contacts
• Long term prophylaxis to prevent additional GAS infection, recurrent ARF, and increased risk of developing rheumatic heart disease
• Short term high-dose Aspirin (100mg/kg/day) for arthritis
• Treat heart failure• Sedatives (haloperidol and pheonbarb) for chorea
Question #9• A 14 yo M cross-country runner comes to your office with c/o
difficulty breathing with exercise. Three days prior to his visit, he had been ill with fever, URI symptoms and sore throat. His fever resolved yesterday, so he went outside for a run, but couldn’t go more than ¼ mile due to SOB. In your office, he appears in NAD. T 98.2, HR 110, RR 26, Pox 96% RA. He has a II/VI holosystolic murmur @ LSB and his liver could be palpated ~2cm below the costal margin. Which organism is the MOST likely cause of his symptoms?– A. Adenovirus– B. Influenza A– C. S. aureus– D. Rhinovirus– E. Coronavirus
The Basics
• Inflammation of the cardiac myocytes• Clinically evident myocarditis infrequent• Follows a non-specific respiratory, flulike, or GI
illness with fever– Most common causes: Viruses!!• Adenovirus• Enterovirus (coxsackie B)
Clinical Manifestations
• Atypical chest pain• Fatigue and exercise intolerance• Dyspnea• Tachycardia• Arrhythmias
– Heart block– VT– SVT
• CHF• Cardiogenic shock• Sudden death

Evaluation
• ECG– Sinus tachycardia– Low-voltage QRS– T-wave inversion– ST-segment depression– Pathologic Q waves
• Echo– LV size and function
• Labs– Cardiac troponin levels– CK-MB
Treatment
• Supportive– Inotropes– Afterload reduction– Diuretics– Oxygen
• IVIg– Not proven to be of any benefit
Question #10
• A 14 yo female presents to ER with substernal chest pain, that she states is worse when she tries to take a breath. On PE, she looks toxic, she is leaning forward seated on the exam table, and has a fever of 40°C. You order a CXR, which reveals cardiomegaly and a right lower lobe pneumonia.
• The most likely etiology is:A. HIVB. InfluenzaC. Mycobacterium tuberculosisD. AdenovirusE. Staphylococcus aureus
PERICARDITIS
Pericarditis• Inflammatory condition that can arise from a wide variety of causes:• Infection• Autoimmune• Rheumatic fever• Uremia• Malignancy• Reaction to a drug• Post cardiac surgery• Idiopathic (30%)
Viral infection
• Most common cause• Prodrome of respiratory or GI illness– Coxackievirus– Echovirus– Adenovirus– EBV– Influenza– HIV
• Presentation = fever, chest pain, friction rub• Often accompanied by myocarditis
Bacterial pericarditis
• Less common, but higher mortality– Staph aureus– Haemophilus influenzae
• Presentation = toxic appearance, irritable, chest pain, cardiomegaly
• May be post-op or from another site (PNA)• TB pericarditis– Spread from lymph nodes or blood borne– Large effusions and cardiac tamponade common
Clinical Manifestations
• Chest pain tends to be substernal, sharp, worse with inspiration and relieved by sitting upright and leaning forward– Radiates to scapular ridge
• Pericardial friction rub– Scratchy, high-pitched to-and-fro sound– Heard best in 2nd and 4th intercostal space at LSB
midclavicular line
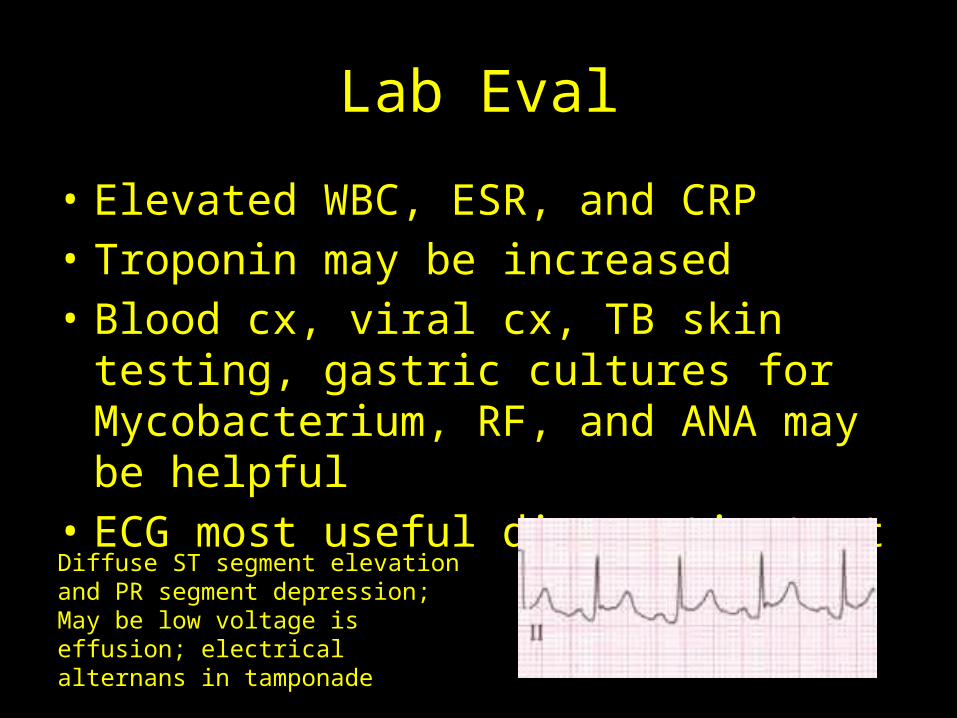
Lab Eval
• Elevated WBC, ESR, and CRP• Troponin may be increased• Blood cx, viral cx, TB skin testing, gastric
cultures for Mycobacterium, RF, and ANA may be helpful
• ECG most useful diagnostic test
Diffuse ST segment elevation and PR segment depression; May be low voltage is effusion; electrical alternans in tamponade
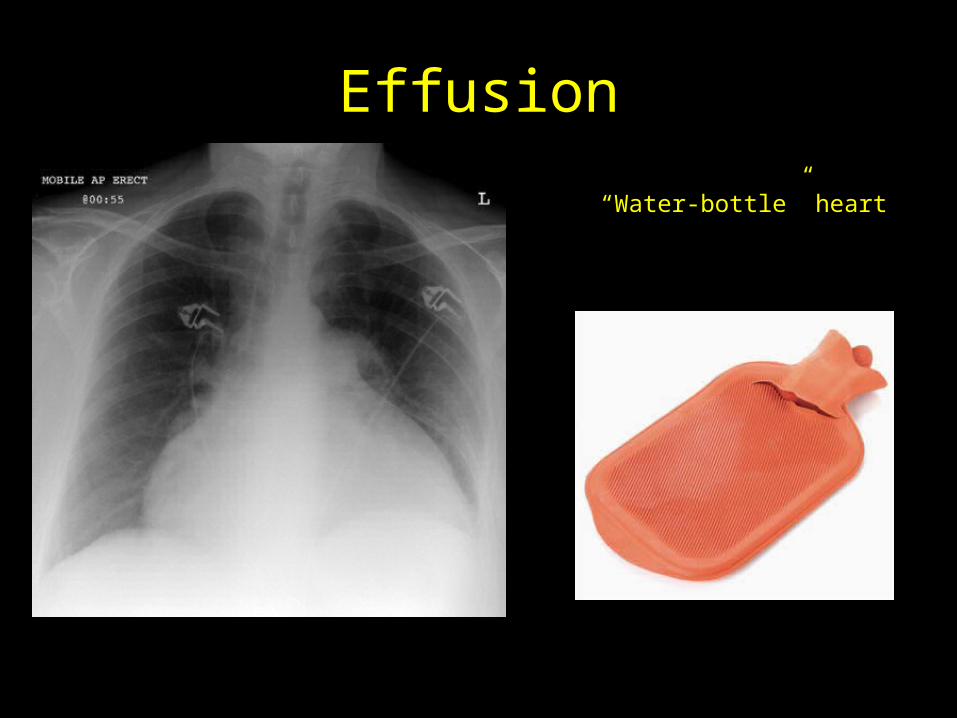
Effusion
“Water-bottle” heart
Management
• Treat the underlying cause• NSAIDS = to alleviate chest pain– If chest pain persists beyond 2 weeks, colchicine can be
added• Steroids = reserved for those unresponsive to
NSAIDS and colchicine or with a rheumatologic disease
• Pericardiocentesis = indicated with hemodynamic compromise, cardiac tamponade, purulent pericarditis, and suspected neoplastic pericarditis– Resistant cases→ pericardial window or pericardiectomy
KAWASAKI DISEASE
Cardiac complications• 20-25% of untreated children develop coronary
artery aneurysms• Other complications include:– Myocarditis– Pericarditis with effusion– Valvulitis (mitral valve)
• Aneurysms resolve 1 to 2 years after onset in 50%– Likelihood determined by size– Can rupture within first few months– Worst prognosis = giant aneurysms
• MI caused by thrombotic occlusion is cause of death– Occurs in first year
Echo
• Performed at diagnosis and 2 and 6 weeks after disease onset– Specifically look at all coronary artery segments– If aneurysms not identified in first 1 to 2 months,
unlikely to develop• Those with giant aneurysms need more
frequent imaging
Treatment
• Everyone gets IVIG and high-dose(80-100mg/kg/d) Aspirin to start– No coronary changes = Low-dose Aspirin (3-5mg/kg/d)
x 6-8wks– Transient coronary ectasia = Low-dose Aspirin x 6-8wks – Small to medium aneurysm = Low-dose Aspirin until
regression documented– >1 large or giant aneurysm (>8mm) = Low-dose Aspirin
+ Warfarin or LMWH– Coronary artery obstruction = Low-dose Aspirin +
Warfarin or LMWH
Other
• When refer to cardiology – *FHx HOCM, Marfan,
muscular dystrophy
• Marfan Syndrome– Due to risks of aortic root dilation and dissection,
NO participation in:• Contact or competitive sports• Isometric exercise• Avoid activities that increased risk of joint injury/ pain
Other
• Cholesterol Screening– Screen with fasting lipid panel:• Children/ adolescents with positive FHx for
dyslipidemia or premature CVD • Children/ adolescents with unknown FHx or with
additional risk factors– Overweight/obese– HTN– Smoking– Diabetes